incorporating radiology into medical gross anatomy: does the use of cadaver ct scans improve...
TRANSCRIPT

RESEARCH REPORT
Incorporating Radiology Into Medical Gross Anatomy: Doesthe Use of Cadaver CT Scans Improve Students’ Academic
Performance in Anatomy?
Rebecca S. Lufler,1* Ann C. Zumwalt,1 Carla A. Romney,2 Todd M. Hoagland1
1Department of Anatomy and Neurobiology, Boston University School of Medicine, Boston, Massachusetts2Division of Graduate Medical Sciences, Boston University School of Medicine, Boston, Massachusetts
Radiological images show anatomical structures in multiple planes and may be effectivefor teaching anatomical spatial relationships, something that students often find difficultto master. This study tests the hypotheses that (1) the use of cadaveric computed tomog-raphy (CT) scans in the anatomy laboratory is positively associated with performance inthe gross anatomy course and (2) dissection of the CT-scanned cadaver is positively asso-ciated with performance on this course. One hundred and seventy-nine first-year medicalstudents enrolled in gross anatomy at Boston University School of Medicine were pro-vided with CT scans of four cadavers, and students were given the opportunity to choosewhether or not to use these images. The hypotheses were tested using logistic regressionanalysis adjusting for student demographic characteristics. Students who used the CTscans were more likely to score greater than 90% as an average practical examinationscore (odds ratio OR 3.6; 95% CI 1.4, 9.2), final course grade (OR 2.6; 95% CI 1.01,6.8), and on spatial anatomy examination questions (OR 2.4; 95% CI 1.03, 5.6) thanwere students who did not use the CT scans. There were no differences in performancebetween students who dissected the scanned cadavers and those who dissected a differentcadaver. These results demonstrate that the use of CT scans in medical gross anatomy ispredictive of performance in the course and on questions requiring knowledge of anatom-ical spatial relationships, but it is not necessary to scan the actual cadaver dissected byeach student. Anat Sci Educ 3:56–63, 2010. © 2010 American Association of Anatomists.
Key words: gross anatomy; medical education; radiology; CT scans; cadaver CT scans;spatial relationships
INTRODUCTION
Given the pervasive use of imaging in multiple medical spe-cialties and the need for every medical student to be able tointerpret basic radiographs, a thorough understanding ofthree-dimensional (3D) anatomical relationships is a crucial
skill for medical students to develop. It is routine to viewimaging modalities such as computed tomography (CT) andmagnetic resonance (MR) imaging as sagittal and coronal sli-ces, reinforcing the need for medical professionals to have athorough understanding of anatomical spatial relationships inmultiple planes (Bassett and Squire, 1985; Lanier and Kaude,1993; Clough and Lehr, 1996).
Studies have shown that incorporating radiological imagesinto medical gross anatomy courses provides valuable learn-ing opportunities for students to learn anatomical relation-ships (Bassett and Squire, 1985; Squire and Novelline, 1985;Berman et al., 1993; Shepherd et al., 2003; Shaffer, 2004;Gunderman and Wilson, 2005). Teaching radiological inter-pretation significantly improves students’ abilities to identifyanatomical structures on diagnostic images (Erkonen et al.,1990, 1992). Teaching cross-sectional anatomy with radiolog-ical images has also been shown to facilitate interpretation ofCT images; however, this was tested after students partici-
*Correspondence to: Rebecca S. Lufler, Department of Anatomy andNeurobiology, Boston University School of Medicine, 72 EastConcord St., Boston, MA 02118, USA. E-mail: [email protected]
Grant sponsor: Lippincott Williams & Wilkins/American Association ofAnatomists, Education Research Scholarship.
Received 23 November 2009; Revised 4 February 2010; Accepted 9February 2010.
Published online 8 March 2010 in Wiley InterScience (www.interscience.wiley.com). DOI 10.1002/ase.141
© 2010 American Association of Anatomists
Anat Sci Educ 3:56–63 (2010) MARCH/APRIL 2010 Anatomical Sciences Education

pated in a radiology course (de Barros et al., 2001). Thesestudies demonstrate that students’ abilities to identify ana-tomical structures in radiological images improve wheninstructed using the same images or modalities. Conversely,Khalil et al. (2005) found that there was no difference in theability of students who were exposed to both cross sectionsand MR images and students only exposed to MR images toidentify anatomical structures in radiological images. It isunclear whether students’ understanding of anatomy and ana-tomical spatial relationships improves when they view speci-mens or images that are different from those used for the ini-tial instruction.
One approach to integrating radiology into gross anatomyeducation is through the use of cadaveric radiographs in thegross anatomy laboratory. Correlating premortem radio-graphs from the medical records of the donor with dissectioncan help students find anatomical variations and pathology,surgically altered anatomy, and compare and contrast grossanatomical structures with radiologic structures (Pantojaet al., 1984, 1985). Given the importance of incorporating ra-diology into anatomy, providing CT scans of students’ cadav-ers may be a pedagogically sound investment. Giving studentsthe opportunity to examine radiologic images of their cadavershould improve their understanding of anatomical spatialrelationships. Indeed, McNiesh et al. (1983) found that theuse of postmortem cadaver plain films in gross anatomyassisted first-year medical students during dissection becauseit helped them to understand complex anatomical spatialrelationships and allowed them to conceptualize the cadaveras their first patient. However, no quantitative data werereported by these investigators to augment the subjective stu-dent responses.
Although the educational research literature is replete withretrospective studies that show the effect of a curriculumchange on students’ performance, medical education studiescommonly depend on the assumption that medical studentsare a homogeneous group. However, students enter medicalschool with a variety of backgrounds and experiences. Thesecharacteristics, if not adjusted for, may affect the interpreta-tion of data on an educational intervention. For example, astudent with prior experience interpreting radiological imageswill likely be more successful in identifying anatomical struc-tures on an image than a student with no prior radiology ex-perience. Therefore, to determine the effect of a pedagogicalintervention, such as radiology instruction, on students’ abil-ities to identify structures on radiological images, previous ra-diology experience must be included in statistical analysis.Further, Medical College Admission Test (MCAT) scores areconsidered to be a predictor of medical school academic per-formance. Boston University School of Medicine studentshave a wide range of MCAT scores, and this further illus-trates the diversity of the medical student population. Thisstudy adjusts for students’ background characteristics todetermine the effect of a change in pedagogy on students’ per-formance in medical gross anatomy.
In this study, we investigated the utility of cadaveric CTscans as a pedagogical tool to enhance learning in gross anat-omy. We examined the relationship between students’ per-formance on spatial anatomy questions and laboratoryexaminations and their use of the radiological images,because these examinations require students to visualizestructures from various views to identify anatomical struc-tures. Subjective data have shown that students find learningradiological analogs to gross structures during gross anatomy
courses is not only enjoyable but also prepares them for radi-ology rotations during the third and fourth years of medicalschool (Sullivan et al., 1987; Lanier and Kaude, 1993; Shep-herd et al., 2003; Branstetter et al., 2007, 2008). However, todate, there have not been any rigorous studies to determinethe effect of incorporating radiological images into medicalgross anatomy on students’ understanding of anatomical andstructural relationships. In this study, we tested two hypothe-ses: Our first hypothesis was that the use of cadaver CT scansin the gross anatomy laboratory is positively associated withperformance in the gross anatomy course as measured bypractical examination scores, spatial anatomy examinationquestions, and final course grade; the second hypothesis wasthat dissecting the cadaver that was CT scanned is positivelyassociated with performance on spatial anatomy examinationquestions and practical examination scores. We also identifiedstudent demographic characteristics that may affect perform-ance on examinations and on the utilization of CT scans.
METHODS
All Boston University School of Medicine first-year medicalstudents enrolled in Gross Anatomy in 2008 were informedof the study during the course orientation. Participation wasvoluntary and did not contribute to students’ final grades inthe course. Students could withdraw from the study at anytime during the semester; however, no students elected to doso. This study was granted exempt status by the Boston Uni-versity School of Medicine Institutional Review Board.
Cadaver Scanning
Four previously embalmed cadavers were CT scanned in theRadiology Department at Boston Medical Center (BMC).Whole-body CT scans were acquired using a General Electric(GE) Lightspeed 16 detector VCT scanner (GE Medical Sys-tems, Milwaukee, WI) in the axial projection at 1.25-mmslice thickness with coronal and sagittal reconstructions. Theimages were separated into four series: (1) head and neck, (2)thorax, (3) abdomen and pelvis, and (4) lower limb. Theupper limbs were included in both the thorax and abdomenseries, since the arms of the cadavers remained at their sides.The CT scout images from which the axial slices were pre-scribed in frontal and lateral projections accompanied eachseries of CT images. The CT images with the PacsCubeDicom Viewer (Version 2.1.0, Merge Healthcare, Milwaukee,WI) were provided by the BMC Radiology Department andloaded onto four computers in the gross anatomy laboratory,one cadaver per computer. The Dicom Viewer softwareallowed students to scroll through the axial, sagittal, and cor-onal images freely and to enable a reference line on the scoutimage while locating anatomical structures and their relation-ships. Worksheets were provided in the laboratory on how touse the Dicom Viewer, interpret the images, and locate spe-cific structures on the images. Structures were not labeled onthe CT scans, and students could confirm their findings withgross anatomy faculty who circulated within the laboratory.
Laboratory Setup
The Boston University School of Medicine first-year curricu-lum is subject based, and the medical gross anatomy course istaught by region. The medical gross anatomy course consistsof 128 contact hours, with 54 hr allocated to lecture time
Anatomical Sciences Education MARCH/APRIL 2010 57

and 74 hr allocated to laboratory time. The course is com-prised of three major units: back and limbs; thorax, abdo-men, and pelvis; and head and neck. In the gross anatomylaboratory, eight students are assigned to each cadaver. Theteams of eight are further divided into two groups of four,and each group is required to explain their dissection to theother group on their team. During dissection, all students dis-sected their assigned cadaver with assistance from faculty,graduate teaching assistants, and fourth-year medical studentprosectors.
The axial cadaver CT images with coronal and sagittalreconstructions were available to all students on computersplaced equidistant from both the scanned cadaver and a non-scanned cadaver. To access the CT scans, students had to loginto the computer using a username and password. TheWorkTime Professional edition computer tracking program(Version 4.11, NesterSoft, Woodbridge, ON, Canada) docu-mented the amount of time each student viewed the scans,yielding data on use of the scans. Students discovered whichcadaver had been scanned by matching their anatomical find-ings from their dissection and the CT scans.
Assessment
Students completed the mental rotations test (MRT) to gatherbaseline data on each student’s ability to mentally manipulateobjects in 3D, a questionnaire to provide investigators withinformation about their background preparation, and theVARK assessment of learning styles. The MRT was adaptedby Vandenberg and Kuse in 1978 and is a validated tool tomeasure visual-spatial ability (Vandenberg and Kuse, 1978).This version of the test was administered according to its pro-tocol at two points, during orientation in August 2008 andjust before completing the final examination in December2008. The MRT was scored by assigning each item two timepoints, requiring the correct choice of both comparison stim-uli. No points were given for one correct and one incorrectanswer. If only one answer was chosen and it was correct,one point was given. The questionnaire specifically addressedgender, undergraduate major and minor, previous gross anat-omy and radiology experience, path to medical school entry,and course load while taking gross anatomy.
The VARK questionnaire (Fleming, 2009) to assess indi-vidual learning styles was used with permission from Neil D.Fleming, Copyright Version 7.0 (2006) held by Neil D. Flem-ing, Christchurch, New Zealand and Charles C. Bonwell,Green Mountain Falls, CO. The acronym VARK stands forvisual, aural, read/write, and kinesthetic sensory modalitiesthat are used for learning information. Fleming and Mills(1992) suggested that these four categories reflect the experi-ences of students and teachers. Students can score mild,strong, or very strong in each of the individual modalities aswell as in any combination of two to four of the modalities.Combinations are referred to as multimodal, and the mild,strong, and very strong categories were collapsed into onegroup. The VARK questionnaire was administered on thepassword-protected course website.
Practical and written examinations were given followingeach unit of the course, so there were six examination grades.There were 41 questions on each practical examination. In thisstudy, students’ understanding of anatomical spatial relation-ships was evaluated by their performance on both spatial anat-omy questions and practical examinations from each of thethree units in the course. Spatial anatomy questions included
cross-sectional, CT, and plain film X-ray questions on the writ-ten and practical examinations, totaling 25questions (11 cross-sectional and 14 radiographic). The practical examinationsrequired an in-depth understanding of anatomical spatial rela-tionships to answer each question. These examinationsincluded identification of bony landmarks on articulated anddisarticulated skeletons as well as structures tagged withincadavers and marked on cross sections and radiographicimages. The cadavers were presented in various positions, someorgans were removed and not placed in anatomical position,and limbs were disarticulated. This forced students to know the3D orientation of every structure. Students were not allowed totouch anything during the examination, so this reinforced theneed to understand structural relationships within the body.Each examination was graded out of 100%, and the percentageof questions answered correctly was used in data analyses.Questions that used cross-sectional, CT, and X-ray images werealso evaluated separately.
Data Analysis
Logistic regression (Logit link, SAS version 9.1, SAS Institute,Cary, NC) was used to determine the relationships betweenpredictors and outcomes for the two hypotheses while con-trolling for students’ individual background demographiccharacteristics. The outcome variables included practical ex-amination scores for each unit of gross anatomy, averagescores on the three practical examinations, correct answerson spatial anatomy questions on written and practical exami-nations, and final course grade in medical gross anatomy. Allperformance outcome variables were dichotomized at 90%,which was considered the level of proficiency. This cutoff waschosen because students who earn scores at this level aremore likely to have a full understanding of the spatial rela-tionships among anatomical structures than students whoscore below 90%. A score below 90% may represent compe-tency, but this is less likely to indicate that students havemastered the anatomical structural relationships. We alsoconsidered generalized linear models on the continuous scoresand found the results to be comparable to the logistic regres-sion results presented here. However, logistic regression wasprimarily used to provide a cutoff that represents the proba-bility that a student has attained the defined level of profi-ciency or understanding of the material. Odds ratios and95% confidence intervals were used to interpret the logisticregression models. The predictor variable considered in thisstudy was CT scan use (minutes) during the course section ofinterest, which was dichotomized into CT scan use (use forgreater than 10 min) and no CT scan use (use for less than10 min). Students who used the CT scans were comparedwith students who did not use the CT scans.
Covariate variables were also studied in the logistic regres-sion models. Gender, previous anatomy experience, previousradiology experience, undergraduate major, undergraduateminor, VARK learning preference, path to medical schoolentry, course load while taking gross anatomy, MRT score,and MCAT scores were evaluated as covariates (Table 1).When these covariates were included in the logistic regressionanalysis models, their impact on the parameter estimates ofthe predictor variable of interest was assessed individually.If the parameter estimate changed by more than 10% in ei-ther the positive or negative direction, the covariate was con-sidered a confounder and was included in the final model. Allcovariates were categorical, except MRT and MCAT scores.
58 Lufler et al.
Variables were categorized as follows: gender (male orfemale); previous anatomy and radiology experience (yes orno); VARK learning preferences (visual, aural, read/write,kinesthetic, the multimodal combination of all four sensorymodalities VARK, or any other multimodal combination ofsensory modalities); undergraduate major (biology, chemistry,engineering, or other); undergraduate minor (biology, chemis-try, engineering, other, or none); path to medical school entry(students who matriculated directly from an undergraduateinstitution or those who matriculated from a different path);and course load (students who were taking the full first se-mester course load or students who were exempted from bio-chemistry). Confounding variables, covariates that affectedboth the predictor and outcome variables, differed amonganalyses. However, if a covariate was considered to be a con-founding variable in one analysis, it was included in all anal-yses. Therefore, all odds ratios were adjusted for MCATscores, gender, previous anatomy and radiology experience,VARK learning preferences, undergraduate major, path tomedical school entry, and course load. MRT scores andundergraduate minor were not deemed to be confounders andtherefore were not included in any model.
RESULTS
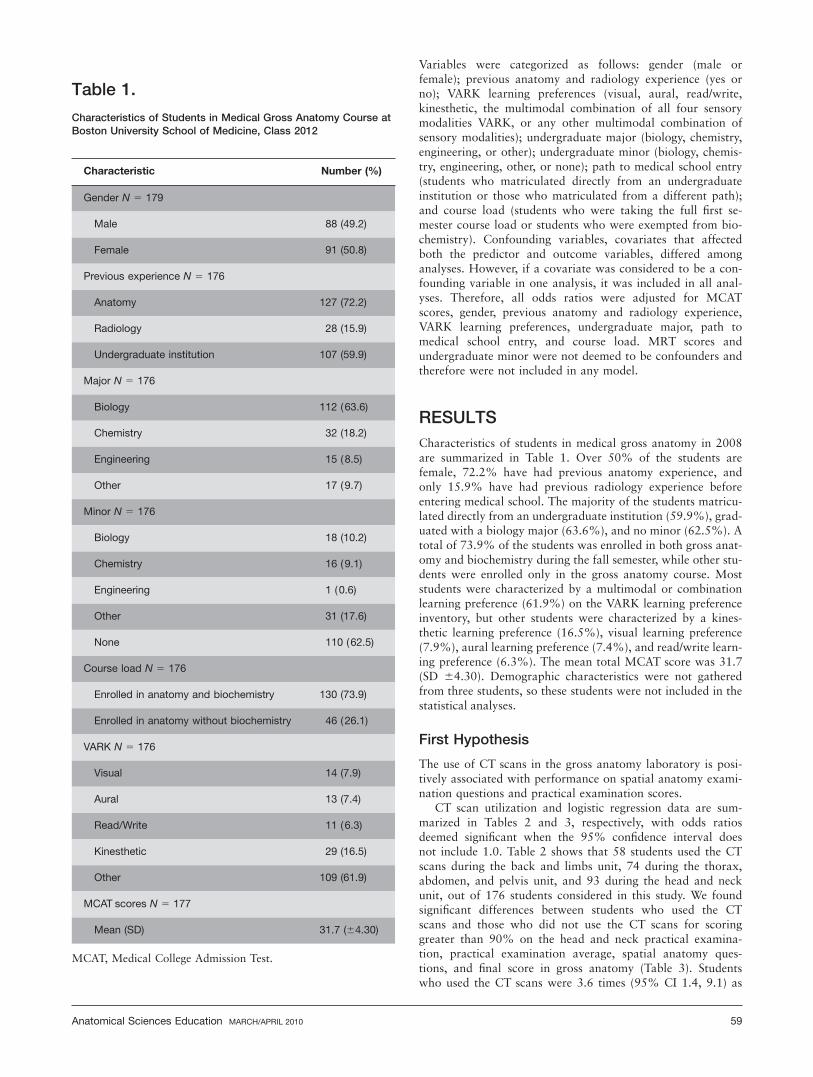
Characteristics of students in medical gross anatomy in 2008are summarized in Table 1. Over 50% of the students arefemale, 72.2% have had previous anatomy experience, andonly 15.9% have had previous radiology experience beforeentering medical school. The majority of the students matricu-lated directly from an undergraduate institution (59.9%), grad-uated with a biology major (63.6%), and no minor (62.5%). Atotal of 73.9% of the students was enrolled in both gross anat-omy and biochemistry during the fall semester, while other stu-dents were enrolled only in the gross anatomy course. Moststudents were characterized by a multimodal or combinationlearning preference (61.9%) on the VARK learning preferenceinventory, but other students were characterized by a kines-thetic learning preference (16.5%), visual learning preference(7.9%), aural learning preference (7.4%), and read/write learn-ing preference (6.3%). The mean total MCAT score was 31.7(SD 64.30). Demographic characteristics were not gatheredfrom three students, so these students were not included in thestatistical analyses.
First Hypothesis
The use of CT scans in the gross anatomy laboratory is posi-tively associated with performance on spatial anatomy exami-nation questions and practical examination scores.
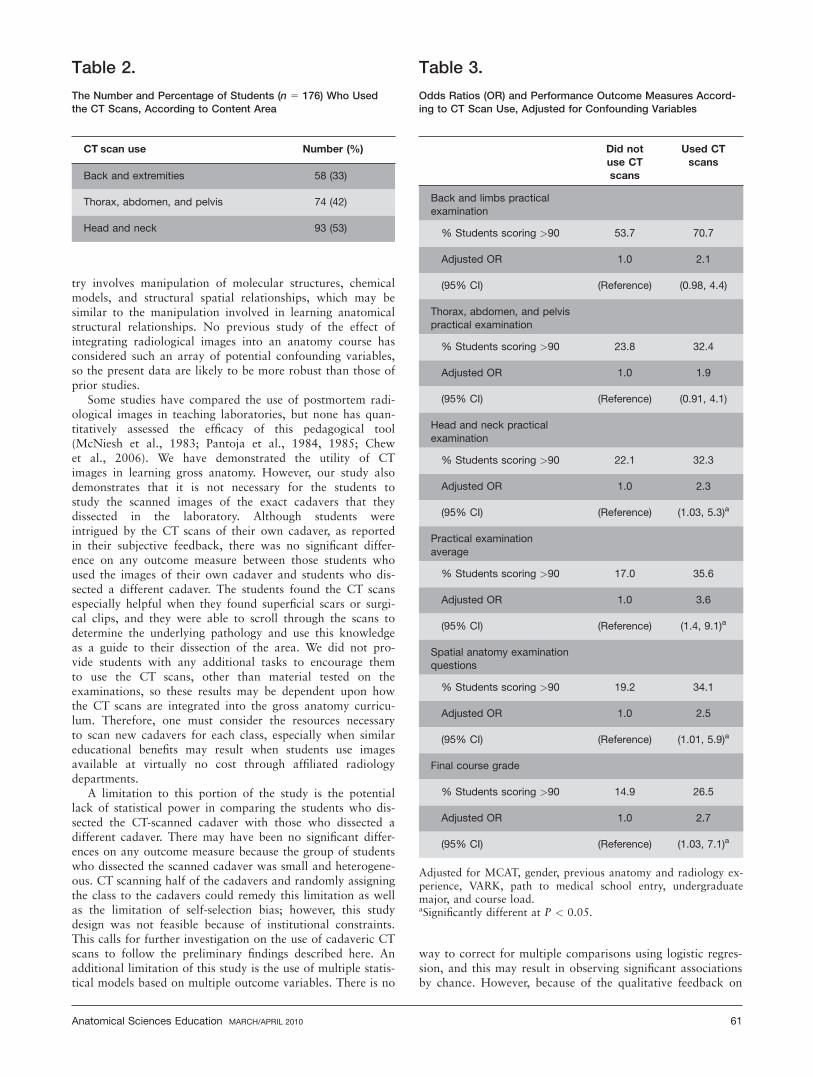
CT scan utilization and logistic regression data are sum-marized in Tables 2 and 3, respectively, with odds ratiosdeemed significant when the 95% confidence interval doesnot include 1.0. Table 2 shows that 58 students used the CTscans during the back and limbs unit, 74 during the thorax,abdomen, and pelvis unit, and 93 during the head and neckunit, out of 176 students considered in this study. We foundsignificant differences between students who used the CTscans and those who did not use the CT scans for scoringgreater than 90% on the head and neck practical examina-tion, practical examination average, spatial anatomy ques-tions, and final score in gross anatomy (Table 3). Studentswho used the CT scans were 3.6 times (95% CI 1.4, 9.1) as
Table 1.
Characteristics of Students in Medical Gross Anatomy Course atBoston University School of Medicine, Class 2012
Characteristic Number (%)
Gender N 5 179
Male 88 (49.2)
Female 91 (50.8)
Previous experience N 5 176
Anatomy 127 (72.2)
Radiology 28 (15.9)
Undergraduate institution 107 (59.9)
Major N 5 176
Biology 112 (63.6)
Chemistry 32 (18.2)
Engineering 15 (8.5)
Other 17 (9.7)
Minor N 5 176
Biology 18 (10.2)
Chemistry 16 (9.1)
Engineering 1 (0.6)
Other 31 (17.6)
None 110 (62.5)
Course load N 5 176
Enrolled in anatomy and biochemistry 130 (73.9)
Enrolled in anatomy without biochemistry 46 (26.1)
VARK N 5 176
Visual 14 (7.9)
Aural 13 (7.4)
Read/Write 11 (6.3)
Kinesthetic 29 (16.5)
Other 109 (61.9)
MCAT scores N 5 177
Mean (SD) 31.7 (64.30)
MCAT, Medical College Admission Test.
Anatomical Sciences Education MARCH/APRIL 2010 59

likely to score greater than 90% as an average practical ex-amination grade as students who did not use the CT scans.These students were also 2.5 times (95% CI 1.03, 5.9) aslikely to answer greater than 90% of spatial anatomy exami-nation questions correctly and 2.7 times (95% CI 1.01, 7.1)as likely to score greater than 90% as a final course grade ingross anatomy.
Confounding variables that had an effect on both the pre-dictor and outcome variables in all analyses were gender andprevious anatomy experience; the remaining confounding var-iables were included in all analyses because they affected atleast one of the models. Surprisingly, students’ visual-spatialability did not have an effect on their use of the CT scans.Students with a kinesthetic learning preference used the CTscans the most, followed by those with visual, multimodalVARK, other multimodal combinations of modalities, read/write, and aural learning preferences. Additionally, within themodels producing the results above, a few confounding varia-bles were also significantly associated with the outcomes.MCAT scores were associated with performance on the backand limbs practical examination and final course grade, whilecontrolling for the other covariates in the model and the CTscan use predictor variable. The odds ratio estimate was 1.1for both of these continuous outcome variables, which meansthat for every unit increase in MCAT score, there is a 10%increase in back and limbs practical examination score andfinal course grade. Students with an undergraduate chemistrymajor were 7.8 times (95% CI 1.6, 39.0) as likely to scoregreater than a 90% as their practical examination average asstudents with any other undergraduate major. Finally, whenadjusting for CT scan use, female students were 2.2 times(95% CI 1.01, 4.8) and 2.8 times (95% CI 1.2, 6.6) as likelyto score greater than 90% on the head and neck practical ex-amination and as a final course grade as were their malecounterparts.
Second Hypothesis
Dissecting the cadaver that was CT scanned is positively asso-ciated with performance on spatial anatomy examinationquestions and practical examination scores.
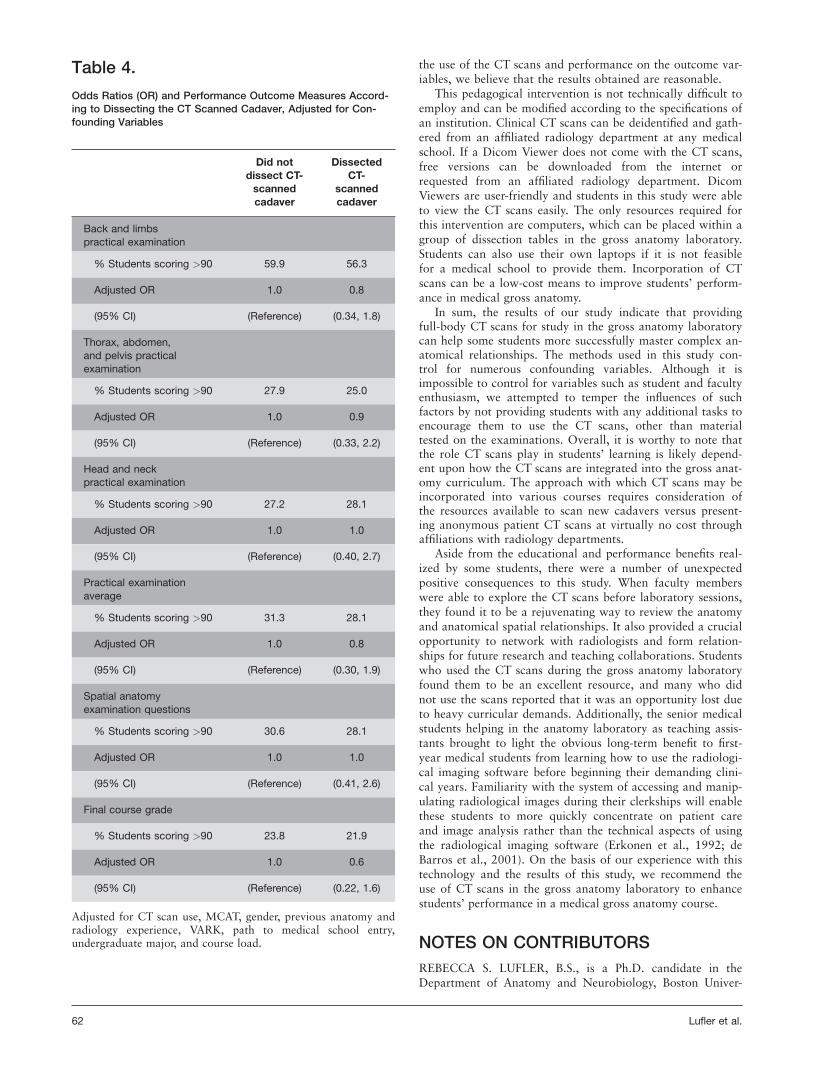
Logistic regression data for dissecting the CT-scannedcadaver and all outcome measures are summarized in Table4. Thirty-two students were assigned to a CT-scannedcadaver and 147 students were assigned to a differentcadaver. These models also adjusted for students’ CT scan useas a confounding variable based on the results presentedabove. Although the use of CT scans was associated withpractical examination average grades, performance on spatialanatomy questions, and final grades in gross anatomy, therewas no association between using cadaver-specific CT scansand all of the aforementioned outcome measures. Studentswho dissected the specific cadaver that was CT scanned werenot more likely to score greater than 90% on the outcomemeasures than were students who dissected a differentcadaver (Table 4).
DISCUSSION
The overall objective of this study was to examine the effec-tiveness of using cadaveric CT images to facilitate the learn-ing of anatomy and anatomical spatial relationships. Specifi-cally, we investigated the relationship between the use of CT
scans in the medical gross anatomy laboratory and perform-ance on spatial anatomy examination questions and practicalexamination scores. We also investigated the effect of dissect-ing a scanned cadaver on learning anatomical spatial relation-ships.
As instruction in radiological image interpretation contin-ues to infiltrate medical curricula, the need to validate it asan effective pedagogical tool has become paramount. Thisprospective study assesses the impact of using CT scans in thegross anatomy laboratory on students’ performance on practi-cal examinations, on questions that assess their understandingof spatial anatomy, and overall anatomy course grade. Thisstudy is also unique in that demographic characteristics wereconsidered as potential confounding variables in statisticalanalyses. Our data show no significant association betweenCT scan use and practical examination score for the backand limbs and thorax, abdomen, and pelvis portions of theanatomy course. However, there was a significant associationbetween CT scan use and performance on the head and neckunit of gross anatomy. This is often a difficult section for stu-dents to master because they must visualize the course of thecranial nerves through the skull and understand how thenerve fibers intermingle without directly seeing them. UsingCT scans in multiple planes may have helped students to de-velop a better three-dimensional understanding of the anat-omy of the head and neck. Not only are structures in theback and limbs and thorax, abdomen, and pelvis portions ofthe course larger, but they are also more visually accessiblethan structures in the head and neck. Our data also show asignificant association between CT scan use and performanceon questions that required identification of anatomical struc-tures in the axial, sagittal, and coronal planes. This indicatesthat students who used the CT scans are better able to inte-grate the multiple views in which anatomical structures areshown throughout the course and identify them when pre-sented in different ways.
This is the first prospective study to quantitatively demon-strate the association of incorporating CT scans into a grossanatomy course. Earlier studies have not had an appropriatecontrol group or they have relied on pretest/posttest analyses.A pretest/posttest design typically shows improvement afterexposure to an instructional method, since the tests examinematerial directly related to the intervention. This studyincluded a control group of students who did not use the CTscans in the gross anatomy laboratory. This design helps toisolate the effect of the intervention on the learning outcomesof interest. This study also considers students’ previous expe-riences and background demographics. As students learn ma-terial in different ways, the VARK learning preference inven-tory was given to all students to control for these intrinsicdifferences. Previous anatomy experience and gender wereshown to have confounding effects in all analyses. Studentswho had already participated in an anatomy course mayhave been more comfortable with the material and able toexplore the CT scans more easily. Within the models used totest the hypotheses, gender was also significantly associatedwith two outcome variables: performance on the head andneck practical examination and final course grade. It is notclear why females tend to outperform males, but this obser-vation provides an opportunity for future research on under-standing the role of students’ background demographics onperformance in medical gross anatomy. Interestingly, studentswho majored in chemistry as undergraduates also tended tooutperform their peers. This is not surprising because chemis-
60 Lufler et al.
try involves manipulation of molecular structures, chemicalmodels, and structural spatial relationships, which may besimilar to the manipulation involved in learning anatomicalstructural relationships. No previous study of the effect ofintegrating radiological images into an anatomy course hasconsidered such an array of potential confounding variables,so the present data are likely to be more robust than those ofprior studies.
Some studies have compared the use of postmortem radi-ological images in teaching laboratories, but none has quan-titatively assessed the efficacy of this pedagogical tool(McNiesh et al., 1983; Pantoja et al., 1984, 1985; Chewet al., 2006). We have demonstrated the utility of CTimages in learning gross anatomy. However, our study alsodemonstrates that it is not necessary for the students tostudy the scanned images of the exact cadavers that theydissected in the laboratory. Although students wereintrigued by the CT scans of their own cadaver, as reportedin their subjective feedback, there was no significant differ-ence on any outcome measure between those students whoused the images of their own cadaver and students who dis-sected a different cadaver. The students found the CT scansespecially helpful when they found superficial scars or surgi-cal clips, and they were able to scroll through the scans todetermine the underlying pathology and use this knowledgeas a guide to their dissection of the area. We did not pro-vide students with any additional tasks to encourage themto use the CT scans, other than material tested on theexaminations, so these results may be dependent upon howthe CT scans are integrated into the gross anatomy curricu-lum. Therefore, one must consider the resources necessaryto scan new cadavers for each class, especially when similareducational benefits may result when students use imagesavailable at virtually no cost through affiliated radiologydepartments.
A limitation to this portion of the study is the potentiallack of statistical power in comparing the students who dis-sected the CT-scanned cadaver with those who dissected adifferent cadaver. There may have been no significant differ-ences on any outcome measure because the group of studentswho dissected the scanned cadaver was small and heterogene-ous. CT scanning half of the cadavers and randomly assigningthe class to the cadavers could remedy this limitation as wellas the limitation of self-selection bias; however, this studydesign was not feasible because of institutional constraints.This calls for further investigation on the use of cadaveric CTscans to follow the preliminary findings described here. Anadditional limitation of this study is the use of multiple statis-tical models based on multiple outcome variables. There is no
way to correct for multiple comparisons using logistic regres-sion, and this may result in observing significant associationsby chance. However, because of the qualitative feedback on
Table 2.
The Number and Percentage of Students (n 5 176) Who Usedthe CT Scans, According to Content Area
CT scan use Number (%)
Back and extremities 58 (33)
Thorax, abdomen, and pelvis 74 (42)
Head and neck 93 (53)
Table 3.
Odds Ratios (OR) and Performance Outcome Measures Accord-ing to CT Scan Use, Adjusted for Confounding Variables
Did notuse CTscans
Used CTscans
Back and limbs practical
examination
% Students scoring >90 53.7 70.7
Adjusted OR 1.0 2.1
(95% CI) (Reference) (0.98, 4.4)
Thorax, abdomen, and pelvispractical examination
% Students scoring >90 23.8 32.4
Adjusted OR 1.0 1.9
(95% CI) (Reference) (0.91, 4.1)
Head and neck practical
examination
% Students scoring >90 22.1 32.3
Adjusted OR 1.0 2.3
(95% CI) (Reference) (1.03, 5.3)a
Practical examination
average
% Students scoring >90 17.0 35.6
Adjusted OR 1.0 3.6
(95% CI) (Reference) (1.4, 9.1)a
Spatial anatomy examinationquestions
% Students scoring >90 19.2 34.1
Adjusted OR 1.0 2.5
(95% CI) (Reference) (1.01, 5.9)a
Final course grade
% Students scoring >90 14.9 26.5
Adjusted OR 1.0 2.7
(95% CI) (Reference) (1.03, 7.1)a
Adjusted for MCAT, gender, previous anatomy and radiology ex-perience, VARK, path to medical school entry, undergraduatemajor, and course load.aSignificantly different at P < 0.05.
Anatomical Sciences Education MARCH/APRIL 2010 61
the use of the CT scans and performance on the outcome var-iables, we believe that the results obtained are reasonable.
This pedagogical intervention is not technically difficult toemploy and can be modified according to the specifications ofan institution. Clinical CT scans can be deidentified and gath-ered from an affiliated radiology department at any medicalschool. If a Dicom Viewer does not come with the CT scans,free versions can be downloaded from the internet orrequested from an affiliated radiology department. DicomViewers are user-friendly and students in this study were ableto view the CT scans easily. The only resources required forthis intervention are computers, which can be placed within agroup of dissection tables in the gross anatomy laboratory.Students can also use their own laptops if it is not feasiblefor a medical school to provide them. Incorporation of CTscans can be a low-cost means to improve students’ perform-ance in medical gross anatomy.
In sum, the results of our study indicate that providingfull-body CT scans for study in the gross anatomy laboratorycan help some students more successfully master complex an-atomical relationships. The methods used in this study con-trol for numerous confounding variables. Although it isimpossible to control for variables such as student and facultyenthusiasm, we attempted to temper the influences of suchfactors by not providing students with any additional tasks toencourage them to use the CT scans, other than materialtested on the examinations. Overall, it is worthy to note thatthe role CT scans play in students’ learning is likely depend-ent upon how the CT scans are integrated into the gross anat-omy curriculum. The approach with which CT scans may beincorporated into various courses requires consideration ofthe resources available to scan new cadavers versus present-ing anonymous patient CT scans at virtually no cost throughaffiliations with radiology departments.
Aside from the educational and performance benefits real-ized by some students, there were a number of unexpectedpositive consequences to this study. When faculty memberswere able to explore the CT scans before laboratory sessions,they found it to be a rejuvenating way to review the anatomyand anatomical spatial relationships. It also provided a crucialopportunity to network with radiologists and form relation-ships for future research and teaching collaborations. Studentswho used the CT scans during the gross anatomy laboratoryfound them to be an excellent resource, and many who didnot use the scans reported that it was an opportunity lost dueto heavy curricular demands. Additionally, the senior medicalstudents helping in the anatomy laboratory as teaching assis-tants brought to light the obvious long-term benefit to first-year medical students from learning how to use the radiologi-cal imaging software before beginning their demanding clini-cal years. Familiarity with the system of accessing and manip-ulating radiological images during their clerkships will enablethese students to more quickly concentrate on patient careand image analysis rather than the technical aspects of usingthe radiological imaging software (Erkonen et al., 1992; deBarros et al., 2001). On the basis of our experience with thistechnology and the results of this study, we recommend theuse of CT scans in the gross anatomy laboratory to enhancestudents’ performance in a medical gross anatomy course.
NOTES ON CONTRIBUTORS
REBECCA S. LUFLER, B.S., is a Ph.D. candidate in theDepartment of Anatomy and Neurobiology, Boston Univer-
Table 4.
Odds Ratios (OR) and Performance Outcome Measures Accord-ing to Dissecting the CT Scanned Cadaver, Adjusted for Con-founding Variables
Did notdissect CT-scannedcadaver
DissectedCT-
scannedcadaver
Back and limbs
practical examination
% Students scoring >90 59.9 56.3
Adjusted OR 1.0 0.8
(95% CI) (Reference) (0.34, 1.8)
Thorax, abdomen,
and pelvis practical
examination
% Students scoring >90 27.9 25.0
Adjusted OR 1.0 0.9
(95% CI) (Reference) (0.33, 2.2)
Head and neckpractical examination
% Students scoring >90 27.2 28.1
Adjusted OR 1.0 1.0
(95% CI) (Reference) (0.40, 2.7)
Practical examination
average
% Students scoring >90 31.3 28.1
Adjusted OR 1.0 0.8
(95% CI) (Reference) (0.30, 1.9)
Spatial anatomy
examination questions
% Students scoring >90 30.6 28.1
Adjusted OR 1.0 1.0
(95% CI) (Reference) (0.41, 2.6)
Final course grade
% Students scoring >90 23.8 21.9
Adjusted OR 1.0 0.6
(95% CI) (Reference) (0.22, 1.6)
Adjusted for CT scan use, MCAT, gender, previous anatomy andradiology experience, VARK, path to medical school entry,undergraduate major, and course load.
62 Lufler et al.

sity School of Medicine, Boston, MA. This research is part ofher doctoral dissertation.
ANN C. ZUMWALT, Ph.D., is an assistant professor inthe Department of Anatomy and Neurobiology, Boston Uni-versity School of Medicine, Boston, MA. She teaches medicalgross anatomy and various clinical anatomy courses to medi-cal students.
CARLA A. ROMNEY, D.Sc., is an assistant dean ofGraduate Medical Sciences, Boston University School ofMedicine, Boston, MA. She is responsible for the design andevaluation of K-12, undergraduate, and medical educationinitiatives.
TODD M. HOAGLAND, Ph.D., is an assistant professorin the Department of Anatomy and Neurobiology, BostonUniversity School of Medicine, Boston, MA. He is the coursedirector of medical gross anatomy.
ACKNOWLEDGMENTS
The authors thank Laura White, Ph.D., Assistant Professor ofBiostatistics at Boston University School of Public Health, forher assistance with the statistical analyses presented in thisstudy.
LITERATURE CITEDBassett LW, Squire LF. 1985. Anatomy instruction by radiologists. InvestRadiol 20:1008–1010.
Berman MC, Miller JA, Chase LM, Anthony A. 1993. Teaching sectional anat-omy. Acad Med 68:548–549.
Branstetter BF IV, Faix LE, Humphrey AL, Schumann JB. 2007. Preclinicalmedical student training in radiology: The effect of early exposure. AJR Am JRoentgenol 188:W9–W14.
Branstetter BF IV, Humphrey AL, Schumann JB. 2008. The long-term impactof preclinical education on medical students’ opinions about radiology. AcadRadiol 15:1331–1339.
Chew FS, Relyea-Chew A, Ochoa ER Jr. 2006. Postmortem computed tomog-raphy of cadavers embalmed for use in teaching gross anatomy. J ComputAssist Tomogr 30:949–954.
Clough RW, Lehr RP. 1996. Testing knowledge of human gross anatomy inmedical school: An applied contextual-learning theory method. Clin Anat9:263–268.
de Barros N, Rodrigues CJ, Rodrigues AJ Jr, de Negri Germano MA, CerriGG. 2001. The value of teaching sectional anatomy to improve CT scan inter-pretation. Clin Anat 14:36–41.
Erkonen WE, Albanese MA, Smith WL, Pantazis NJ. 1990. Gross anatomyinstruction with diagnostic images. Invest Radiol 25:292–294.
Erkonen WE, Albanese MA, Smith WL, Pantazis NJ. 1992. Effectiveness ofteaching radiologic image interpretation in gross anatomy. A long-term follow-up. Invest Radiol 27:264–266.
Fleming ND. 2009. VARK: A Guide to Learning Styles. Christchurch, NewZealand. URL:http://www.vark-learn.com/english/page.asp?p5questionnaire[accessed 20 November 2009]
Fleming ND, Mills C. 1992. Not another inventory: Rather a catalyst forreflection. To Improve the Academy 11:137–149.
Gunderman RB, Wilson PK. 2005. Viewpoint: Exploring the human interior:The roles of cadaver dissection and radiologic imaging in teaching anatomy.Acad Med 80:745–749.
Khalil MK, Payer AF, Johnson TE. 2005. Effectiveness of using cross-sectionsin the recognition of anatomical structures in radiological images. Anat Rec283B:9–13.
Lanier L, Kaude JV. 1993. Radiologic anatomy—A credit course for first-yearmedical students. Acta Radiol 34:414–416.
McNiesh LM, Madewell JE, Allman RM. 1983. Cadaver radiography in theteaching of gross anatomy. Radiology 148:73–74.
Pantoja E, Nagy F, Zambernard J. 1984. Cadaver radiographs. J Med Educ59:536–537.
Pantoja E, Nagy F, Zambernard J. 1985. Clinical radiographs of the cadaver asa teaching aid in anatomy. Radiology 155:28.
Shaffer K. 2004. Teaching anatomy in the digital world. N Engl J Med351:1279–1281.
Shepherd SM, Dudewicz DM, Hindo WA. 2003. Immediate and long-termeffects of a sophomore radiology elective. Acad Radiol 10:786–793.
Squire LF, Novelline RA. 1985. Radiology should be a required part of themedical school curriculum. Radiology 156:243–244.
Sullivan DC, Effmann EL, Chen JT. 1987. Experience with an alternative cur-riculum. Invest Radiol 22:246–249.
Vandenberg SG, Kuse AR. 1978. Mental rotations, a group test of three-dimen-sional spatial visualization. Percept Mot Skills 47:599–604.
Anatomical Sciences Education MARCH/APRIL 2010 63