improving anaesthetists' communication skills
TRANSCRIPT

SPECIAL ARTICLE
Improving anaesthetists’ communication skills
C. Harms,1 J. R. Young,5 F. Amsler,2 C. Zettler,3 D. Scheidegger4 and C. H. Kindler1
1 Staff Anaesthetist, 2 Consultant Psychologist, 3 Resident, 4 Professor and Chairman, Department of Anaesthesia,
University Clinics Basel, 5 Biostatistician, Basel Institute of Clinical Epidemiology, University Clinics Basel,
Kantonsspital, CH-4031 Basel, Switzerland
Summary
The attitude, behaviour and communication skills of specialised doctors are increasingly recognised
as important and they have been identified as training requirements. We designed a programme to
teach communication skills to doctors in a University Department of Anaesthesia and evaluated its
effect on patient outcomes such as satisfaction and anxiety. The 20 h programme was based on
videotaped reviews of actual pre-operative visits and role-playing. Effects on patient satisfaction and
pre-operative anxiety were assessed using a patient questionnaire. In addition, all participating
anaesthetists assessed the training. We provide evidence that the training increased patient satis-
faction with the pre-operative anaesthetic visit. Training also decreased anxiety associated with
specific aspects of anaesthesia and surgery, but the effect was rather small given the intense pro-
gramme. The anaesthetists agreed that their interpersonal skills increased and they felt better
prepared to understand patients’ anxieties. Communication skills training can increase patient
satisfaction and decrease specific anxieties. The authors conclude that in order to better demon-
strate the efficacy of such a training programme, the particular communication skills of anaesthetists
rather than indirect patient outcome parameters should be measured.
Keywords Patient satisfaction. Anxiety. Pre-operative care. Physician-patient relations. Communication.
Clinical competence. Education.
........................................................................................................
Correspondence to: C. H. Kindler
E-mail: [email protected]
Accepted: 31 August 2003
Effective communication between doctor and patient
improves patient satisfaction, patient recall of information
and medical outcome, and can even protect doctors
against malpractice litigation [1]. Although interest in
teaching communication skills in medical schools has
increased over the years, most postgraduate medical
education still focusses on the technical and biomedical
aspects of medicine [2]. However, the importance of
non-technical skills in the daily work of doctors is now
increasingly recognised, even in subspecialties such as
anaesthesia [3]. Anaesthesia residency review committees
in different countries now demand documentation of
training in communication skills. For example, the Royal
College of Anaesthetists requires an assessment of com-
munication skills, attitudes to patients and behaviour for
its Certificate of Completion of Specialist Training [4].
The American Accreditation Council for Graduate
Medical Education (ACGME) has endorsed six general
competencies including interpersonal and communica-
tion skills for residents in all specialties [5]. The ACGME
and the American Board of Medical Specialties are now
collaborating to implement and evaluate these general
competencies. The impact of doctors’ personal skills has
therefore become an area of clinical interest and research.
Most medical training programmes that teach communi-
cation skills are designed for general practitioners, but a
few have been designed for surgeons [1] or for Accident
and Emergency Department doctors [6].
Apart from personal observations, there are no data
available on how anaesthetists communicate with their
patients [7, 8]. We designed a programme to teach
communication skills to anaesthetists using videotaped
reviews of their pre-operative visits and role-play. Com-
munication skills that are effective for general practitioners
are not necessarily effective for other specialists [1]. Our
programme was therefore tailored to the particular
Anaesthesia, 2004, 59, pages 166–172.....................................................................................................................................................................................................................
166 � 2004 Blackwell Publishing Ltd

situation of the anaesthetist and patient in the pre-
operative setting. The objectives of the training pro-
gramme were to improve the receptive and affective
behaviour and interpersonal skills of anaesthetists and to
increase patient participation in informed or shared
decision-making with respect to the planned anaesthetic
technique. Despite the resources invested in communica-
tion skills training, few programmes seem to have been
assessed in terms of patient outcome [2, 9]. Using a patient
questionnaire, we assessed whether our training pro-
gramme increased patient satisfaction and decreased
patient anxiety before surgery. In addition, the training
programme was assessed by a questionnaire distributed to
all participating anaesthetists.
Methods
The Local Research Ethics Committee of the University
of Basel approved the communication skills training
programme and its assessment by questionnaires. A
clinical psychologist (F.A.) led the training. Anaesthetists
in a University Department of Anaesthesia were trained in
small groups of 7–10 with a similar mixture of residents
and faculty within each group. Each group received 10
training sessions, one each month, and each session lasted
about 2 h. Participation in the training was mandatory for
all 59 anaesthetists involved in patient care during the
study period, although not all received the full 20 h of
training.
Training started with a short theoretical introduction to
interpersonal communication and its effect on patient
outcomes such as patient satisfaction. After this, training
consisted firstly of reviewing videotaped pre-operative
visits. Each trainee had to record two of his ⁄ her pre-
operative visits and these videos were discussed and
analysed within each group. Trainees were asked to
observe themselves, recognise their own emotions, rec-
ognise their patients’ expressions and listen actively to
what their patients were saying. Second, role-playing was
used to prepare for difficult situations. Trainees were
asked to apply four behaviours of effective clinicians,
adapted to the pre-operative situation:
1 establish a welcoming atmosphere for the pre-operative
visit and agree with the patient on an agenda;
2 elicit the patient’s concerns about anaesthesia and
surgery;
3 demonstrate empathy both verbally and non-verbally;
4 actively involve the patient in making decisions about
the planned anaesthetic technique whenever possible, and
appropriately conclude the visit by reassuring the patient
of ongoing care.
The training programme was assessed using a pre- and
postintervention design. Patient satisfaction and patient
pre-operative anxiety were defined as appropriate meas-
ures of improvement in communication skills. We
constructed a questionnaire using a modified Delphi
procedure [10] to measure patient satisfaction with the
pre-operative visit, patient pre-operative anxiety [11] and
patient perception of the anaesthetist [12]. The final
version of the questionnaire contained 86 items. Inclusion
criteria for patients were: age over 18 years; fluency and
literacy in the German language; written informed
consent. Patients with a seriously impaired mental status
were excluded. Anaesthetists were informed verbally and
in writing about the purpose of the study and asked
to participate. They were told that they did not have to
distribute questionnaires to patients if they did not wish to
do this and they also signed a physician questionnaire
containing patient and physician demographic data. Pre-
intervention data were collected for a period of 3 months
from all patients undergoing elective surgery, the inter-
vention consisted of training in communication skills for a
period of 10 months using videotape reviews and role-
playing, and postintervention data were collected for a
3-month period after the training finished. At the end
of the programme, all participating anaesthetists also
assessed it.
Summary response variables
Six response variables were used to summarise patients’
satisfaction with the pre-operative anaesthetic visit and
pre-operative anxiety. Satisfaction with the pre-operative
anaesthetic visit was summarised by ‘overall satisfaction’ in
the form of each patient’s response to a general question
on overall satisfaction, and by ‘median satisfaction’ in the
form of each patient’s median response to 10 specific
questions on satisfaction with different aspects of the pre-
operative anaesthetic visit. All 11 questions used the same
five ordered categories (insufficient, fair, appropriate, very
good, excellent). Pre-operative anxiety was summarised
by using the German version of the Spielberger-State-
Anxiety-Score (STAI-G Form X1) [13], by ‘overall
anxiety about anaesthesia’ and ‘overall anxiety about
surgery’ in the form of each patient’s response to two
general questions on overall anxiety, and by ‘median
anxiety’ in the form of each patient’s median response to
10 specific questions on different aspects of anxiety about
anaesthesia and surgery [11]. These 12 questions on
anxiety all used a 10-cm visual analogue scale (VAS).
Predictor variables
The predictor variables used to model each summary
response variable were: age, gender, level of education,
prior experience of anaesthesia, whether or not pati-
ents felt they were involved in choosing the type of
anaesthesia they would receive, planned duration of
Anaesthesia, 2004, 59, pages 166–172 C. Harms et al. Æ Improving anaesthetist communication skills......................................................................................................................................................................................................................
� 2004 Blackwell Publishing Ltd 167

surgery, the anaesthetist and the number of hours of
training the anaesthetist had received before the anaes-
thetic visit. Age, planned duration of surgery and the
number of hours of training were continuous variables; all
other variables were categorical. The patients’ level of
education was coded as one of three categories: at most
primary or secondary school, apprenticeship or high
school, college or university. Prior experience of anaes-
thesia was also coded as one of three categories: none,
prior experience, prior bad experience.
Models and model fitting
The six summary response variables were modelled using
analysis of covariance. ‘Mixed’ models were fitted with
the anaesthetist as a random effect and all other predictors
as fixed effects. As a fixed effect, each predictor variable or
category of a predictor variable is represented by a single
parameter. As a random effect, each anaesthetist is said to
form a cluster; responses from patients with the same
anaesthetist are correlated but responses from patients
with different anaesthetists are independent. A single
parameter, the between-cluster variance, describes the
differences between clusters; cluster effects are assumed to
be normally distributed with a mean of zero. In this way,
variability between anaesthetists is modelled without
needing additional predictor variables to describe the
differences between them.
Different distributions were assumed for the six sum-
mary response variables. For both overall and median
satisfaction, < 1% of responses were ‘fair’ and none was
‘insufficient’. The lower three categories were therefore
combined and renamed ‘standard’. Overall and median
satisfaction were assumed to follow underlying normal
distributions, although each was measured on an ordinal
scale [14]; the Spielberger score was assumed to follow a
normal distribution; and the other anxiety responses were
assumed to follow exponential distributions (Fig. 1).
Models were fitted using the NLMIXED, MIXED and
GENMOD procedures in SAS version 8.2. (SAS Institute
Inc., Cary, NC). The NLMIXED procedure fits non-
linear models with both fixed and random effects; the
MIXED procedure fits linear models with both fixed and
random effects; the GENMOD procedure fits non-linear
models with only fixed effects. Where possible, therefore,
parameter estimates from NLMIXED were checked
against estimates from other procedures: the MIXED
procedure reproduced estimates for the Spielberger score
with the random effect, the GENMOD procedure
reproduced estimates for the other anxiety responses
without the random effect.
When using NLMIXED, models were first fitted
without the random effect to provide suitable starting
values for fitting with the random effect. Optimisation in
NLMIXED was by the trust region method or, if this
failed to converge, by quasi-Newton methods. The trust
region method uses both first and second order partial
derivatives and often provides stable estimates when a
model has a small number of predictor variables. When
a model has more variables, the trust region method
may fail to converge, but quasi-Newton methods may
converge as these use only the first order partial derivatives
[15]. All confidence intervals were approximate 95%
%
0
10
20
30
40
Anxiety - anaesthesia
0 -<1
1 -<2
2 -<3
3 -<4
4 -<5
5 -<6
6 -<7
7 -<8
8 -<9
9 -10
%
0
5
10
15
20
Spielberger score
20 -<25
25 -<30
30 -<35
35 -<40
40 -<45
45 -<50
50 -<55
55 -<60
60 -<65
65 -<70
70 -<75
75 -80
%
0
10
20
30
40
50
Satisfaction - overallStandard Very good Excellent
%
0
10
20
30
40
Anxiety - median
0 -<1
1 -<2
2 -<3
3 -<4
4 -<5
5 -<6
6 -<7
7 -<8
8 -<9
9 -10
%
0
10
20
30
40
Anxiety - surgery
0 -<1
1 -<2
2 -<3
3 -<4
4 -<5
5 -<6
6 -<7
7 -<8
8 -<9
9 -10
%
0
10
20
30
40
50
Satisfaction - medianStandard Very good Excellent
Figure 1 The six summary responsevariables for patient satisfaction withthe pre-operative anaesthetic visit andpre-operative anxiety expressed as apercentage of patients in each category.Anxiety-surgery, anxiety-anaesthesia,and anxiety-median are represented on a10 cm visual analogue scale.
C. Harms et al. Æ Improving anaesthetist communication skills Anaesthesia, 2004, 59, pages 166–172......................................................................................................................................................................................................................
168 � 2004 Blackwell Publishing Ltd
confidence intervals based on the Wald statistic. All
significance tests were based on the likelihood ratio
statistic.
Results
A total of 1338 patients completed the survey. Of these,
1228 patients were included in the statistical analysis: 905
were patients of anaesthetists without training in com-
munication skills and 323 were patients of anaesthetists
who received at least some training. Patients were
included in the analysis if their data were available for
all predictor variables and if their anaesthetist saw at least
10 surveyed patients. Missing values for response variables
further reduced the sample size for specific models; the
lowest sample size was 902 for the Spielberger score.
Patients seen by anaesthetists with or without training
were similar in age, education and prior experience of
anaesthesia (Table 1). However, patients seen by anaes-
thetists without training were more likely to be male;
those seen by anaesthetists with training were more likely
to be female. Both the expected duration of surgery and
the length of the pre-operative visit were similar for
patients seen by anaesthetists with or without training.
Overall satisfaction with the pre-operative visit was
high. With and without training, 79% and 78% of
patients, respectively, felt that their anaesthetic visit had
been ‘very good’ or ‘excellent’. Overall pre-operative
anxiety was low. On a 10-cm VAS, overall anxiety about
anaesthesia scored a median [IQR] of 2.0 [0.5–4.8] both
with and without training, while overall anxiety about
surgery was 2.3 [0.8–5.1] with training and 2.4 [0.4–2.6]
without (Table 1).
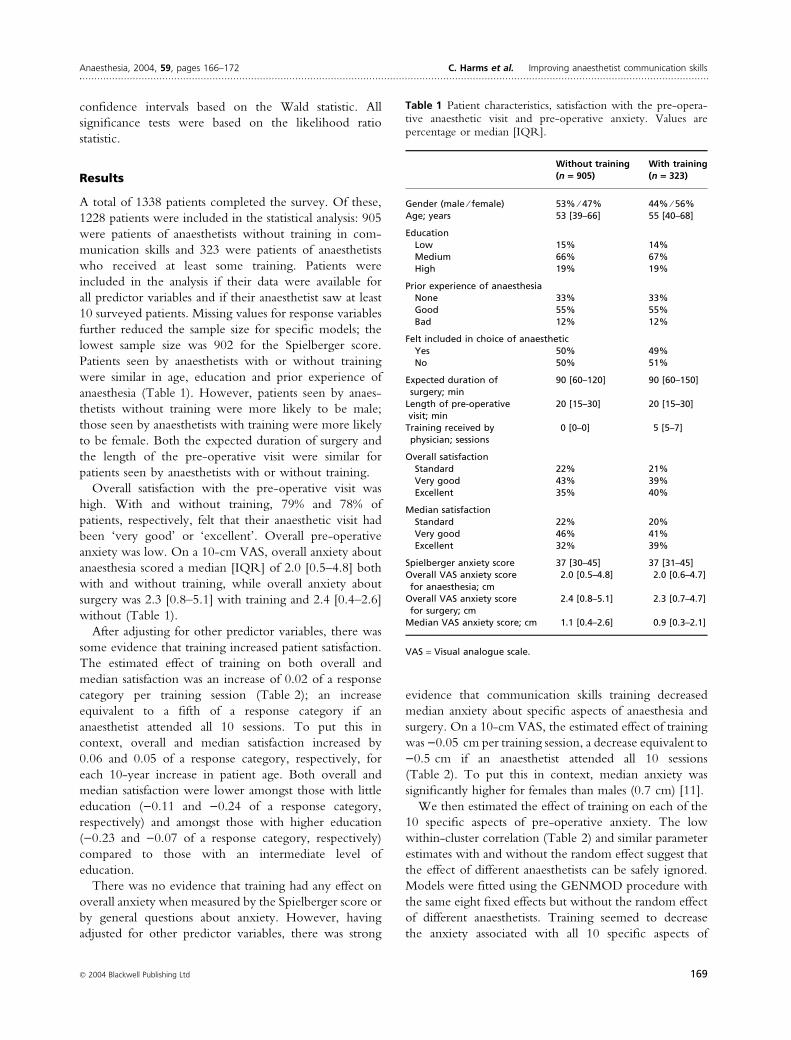
After adjusting for other predictor variables, there was
some evidence that training increased patient satisfaction.
The estimated effect of training on both overall and
median satisfaction was an increase of 0.02 of a response
category per training session (Table 2); an increase
equivalent to a fifth of a response category if an
anaesthetist attended all 10 sessions. To put this in
context, overall and median satisfaction increased by
0.06 and 0.05 of a response category, respectively, for
each 10-year increase in patient age. Both overall and
median satisfaction were lower amongst those with little
education ()0.11 and )0.24 of a response category,
respectively) and amongst those with higher education
()0.23 and )0.07 of a response category, respectively)
compared to those with an intermediate level of
education.
There was no evidence that training had any effect on
overall anxiety when measured by the Spielberger score or
by general questions about anxiety. However, having
adjusted for other predictor variables, there was strong
evidence that communication skills training decreased
median anxiety about specific aspects of anaesthesia and
surgery. On a 10-cm VAS, the estimated effect of training
was )0.05 cm per training session, a decrease equivalent to
)0.5 cm if an anaesthetist attended all 10 sessions
(Table 2). To put this in context, median anxiety was
significantly higher for females than males (0.7 cm) [11].
We then estimated the effect of training on each of the
10 specific aspects of pre-operative anxiety. The low
within-cluster correlation (Table 2) and similar parameter
estimates with and without the random effect suggest that
the effect of different anaesthetists can be safely ignored.
Models were fitted using the GENMOD procedure with
the same eight fixed effects but without the random effect
of different anaesthetists. Training seemed to decrease
the anxiety associated with all 10 specific aspects of
Table 1 Patient characteristics, satisfaction with the pre-opera-tive anaesthetic visit and pre-operative anxiety. Values arepercentage or median [IQR].
Without training(n = 905)
With training(n = 323)
Gender (male ⁄ female) 53% ⁄ 47% 44% ⁄ 56%Age; years 53 [39–66] 55 [40–68]
EducationLow 15% 14%Medium 66% 67%High 19% 19%
Prior experience of anaesthesiaNone 33% 33%Good 55% 55%Bad 12% 12%
Felt included in choice of anaestheticYes 50% 49%No 50% 51%
Expected duration ofsurgery; min
90 [60–120] 90 [60–150]
Length of pre-operativevisit; min
20 [15–30] 20 [15–30]
Training received byphysician; sessions
0 [0–0] 5 [5–7]
Overall satisfactionStandard 22% 21%Very good 43% 39%Excellent 35% 40%
Median satisfactionStandard 22% 20%Very good 46% 41%Excellent 32% 39%
Spielberger anxiety score 37 [30–45] 37 [31–45]Overall VAS anxiety scorefor anaesthesia; cm
2.0 [0.5–4.8] 2.0 [0.6–4.7]
Overall VAS anxiety scorefor surgery; cm
2.4 [0.8–5.1] 2.3 [0.7–4.7]
Median VAS anxiety score; cm 1.1 [0.4–2.6] 0.9 [0.3–2.1]
VAS = Visual analogue scale.
Anaesthesia, 2004, 59, pages 166–172 C. Harms et al. Æ Improving anaesthetist communication skills......................................................................................................................................................................................................................
� 2004 Blackwell Publishing Ltd 169
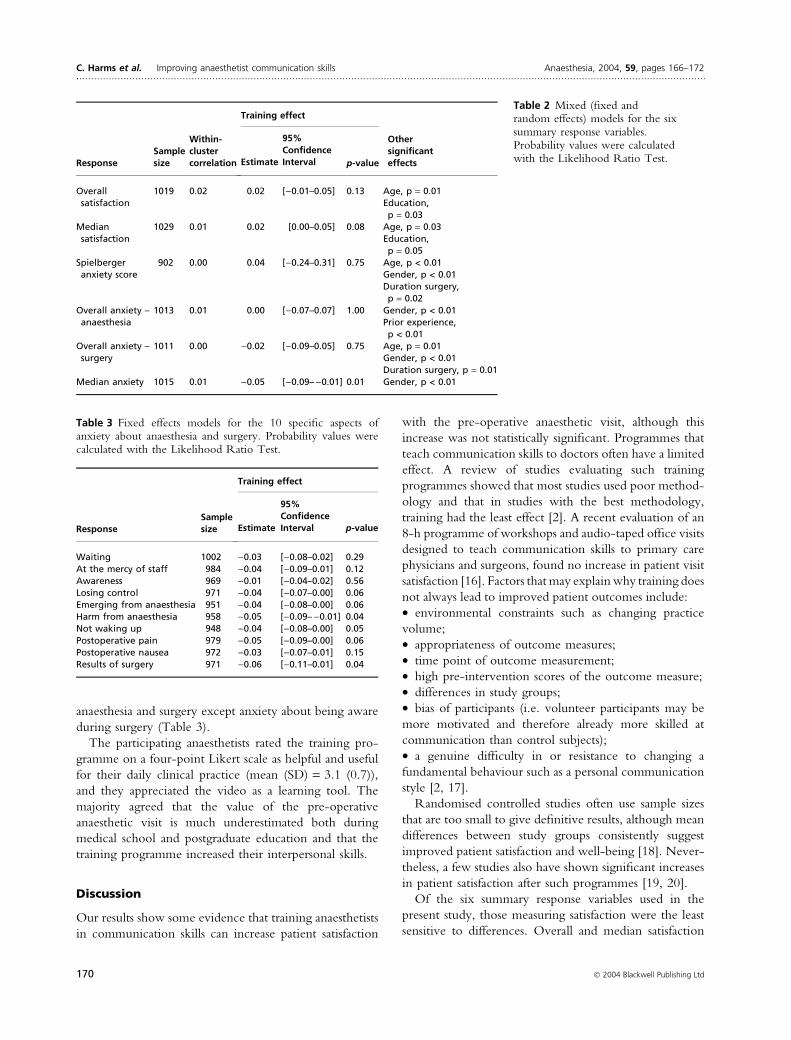
anaesthesia and surgery except anxiety about being aware
during surgery (Table 3).
The participating anaesthetists rated the training pro-
gramme on a four-point Likert scale as helpful and useful
for their daily clinical practice (mean (SD) = 3.1 (0.7)),
and they appreciated the video as a learning tool. The
majority agreed that the value of the pre-operative
anaesthetic visit is much underestimated both during
medical school and postgraduate education and that the
training programme increased their interpersonal skills.
Discussion
Our results show some evidence that training anaesthetists
in communication skills can increase patient satisfaction
with the pre-operative anaesthetic visit, although this
increase was not statistically significant. Programmes that
teach communication skills to doctors often have a limited
effect. A review of studies evaluating such training
programmes showed that most studies used poor method-
ology and that in studies with the best methodology,
training had the least effect [2]. A recent evaluation of an
8-h programme of workshops and audio-taped office visits
designed to teach communication skills to primary care
physicians and surgeons, found no increase in patient visit
satisfaction [16]. Factors that may explain why training does
not always lead to improved patient outcomes include:
• environmental constraints such as changing practice
volume;
• appropriateness of outcome measures;
• time point of outcome measurement;
• high pre-intervention scores of the outcome measure;
• differences in study groups;
• bias of participants (i.e. volunteer participants may be
more motivated and therefore already more skilled at
communication than control subjects);
• a genuine difficulty in or resistance to changing a
fundamental behaviour such as a personal communication
style [2, 17].
Randomised controlled studies often use sample sizes
that are too small to give definitive results, although mean
differences between study groups consistently suggest
improved patient satisfaction and well-being [18]. Never-
theless, a few studies also have shown significant increases
in patient satisfaction after such programmes [19, 20].
Of the six summary response variables used in the
present study, those measuring satisfaction were the least
sensitive to differences. Overall and median satisfaction
Table 2 Mixed (fixed andrandom effects) models for the sixsummary response variables.Probability values were calculatedwith the Likelihood Ratio Test.Response
Samplesize
Within-clustercorrelation
Training effect
OthersignificanteffectsEstimate
95%
ConfidenceInterval p-value
Overallsatisfaction
1019 0.02 0.02 [)0.01–0.05] 0.13 Age, p = 0.01Education,p = 0.03
Mediansatisfaction
1029 0.01 0.02 [0.00–0.05] 0.08 Age, p = 0.03Education,p = 0.05
Spielbergeranxiety score
902 0.00 0.04 [)0.24–0.31] 0.75 Age, p < 0.01Gender, p < 0.01Duration surgery,p = 0.02
Overall anxiety –anaesthesia
1013 0.01 0.00 [)0.07–0.07] 1.00 Gender, p < 0.01Prior experience,p < 0.01
Overall anxiety –surgery
1011 0.00 )0.02 [)0.09–0.05] 0.75 Age, p = 0.01Gender, p < 0.01Duration surgery, p = 0.01
Median anxiety 1015 0.01 )0.05 [)0.09–)0.01] 0.01 Gender, p < 0.01
Table 3 Fixed effects models for the 10 specific aspects ofanxiety about anaesthesia and surgery. Probability values werecalculated with the Likelihood Ratio Test.
ResponseSamplesize
Training effect
Estimate
95%ConfidenceInterval p-value
Waiting 1002 )0.03 [)0.08–0.02] 0.29At the mercy of staff 984 )0.04 [)0.09–0.01] 0.12Awareness 969 )0.01 [)0.04–0.02] 0.56Losing control 971 )0.04 [)0.07–0.00] 0.06Emerging from anaesthesia 951 )0.04 [)0.08–0.00] 0.06Harm from anaesthesia 958 )0.05 [)0.09–)0.01] 0.04Not waking up 948 )0.04 [)0.08–0.00] 0.05Postoperative pain 979 )0.05 [)0.09–0.00] 0.06Postoperative nausea 972 )0.03 [)0.07–0.01] 0.15Results of surgery 971 )0.06 [)0.11–0.01] 0.04
C. Harms et al. Æ Improving anaesthetist communication skills Anaesthesia, 2004, 59, pages 166–172......................................................................................................................................................................................................................
170 � 2004 Blackwell Publishing Ltd

were measured on an ordinal scale and only three of the
five categories were commonly chosen. A VAS scale
would have had more power to detect the effect of
training on satisfaction. Patient satisfaction with the pre-
operative anaesthetic visit was already high before the
training programme. In a previous analysis of 10 811
patients, the overall level of satisfaction with anaesthetic
care was also very high (96.8%) and only 0.9% of patients
were ‘dissatisfied’ [21]. Patient satisfaction questionnaires
may therefore have a limited value as an evaluation tool in
the doctor–patient relationship because patient satisfaction
is usually very high before an intervention [22]. In such a
situation, the modest improvements we have seen may be
all we can reasonably expect.
In addition to a modest increase in patient satisfaction,
our results show good evidence that teaching communi-
cation skills to anaesthetists significantly decreased patient
anxiety associated with specific aspects of anaesthesia and
surgery. However, the training had no effect on overall
pre-operative anxiety. These two results are not neces-
sarily inconsistent. General questions about overall anxi-
ety may be more of a measure of ‘irrational anxiety’,
whereas specific questions may be more of a measure of
‘rational anxiety’. The former is probably more difficult
to influence and may reflect the ‘trait’ of the personality.
Consistent with this idea is the finding that training had
no effect on overall anxiety about surgery but decreased
anxiety about the results of surgery. The general questions
on overall anxiety about anaesthesia and surgery were
asked before the 10 specific questions on anxiety; the
specific question on the results of surgery was the last
question asked. Therefore, general questions were asked
before patients thought about specific issues; having
thought about such issues, patients may have been more
‘rational’ about their anxiety.
The within-cluster correlation gives the ratio of
random effect variation to total variation. Hence, the
variability associated with different anaesthetists is at most
2% of the total variability in a response. This low
percentage suggests that patient-dependent predictor
variables are more important than anaesthetist-dependent
predictor variables in modelling patient satisfaction with
the anaesthetic visit and pre-operative anxiety. As a
consequence, changing the anaesthetist’s behaviour may
have little impact on a patient’s perceptions.
In the present study, essential environmental factors
such as the anaesthetist’s workload remained constant pre-
and postintervention. The length of the pre-operative visit
was also constant (median = 20 min). The training ses-
sions were always held in the afternoon during regular
working hours and the participants were relieved of their
clinical responsibilities in the operating theatres by nurse
anaesthetists and by those anaesthetists not in training on
that day. While this format increased the cost of training, it
maintained the mandatory aspect of the programme so as
to minimise participant bias. It was also a change from
clinical routine work and it was not surprising that most
participants enjoyed these training sessions, although some
faculty members complained about disruption to their
non-clinical responsibilities and schedules. Anaesthetists
found their empathy developed so that they could
perceive the needs and anxieties of their patients better,
although the transfer of the newly acquired techniques to
the actual patient encounter seems for many to be difficult.
As a teaching hospital, we have a considerable turnover
of residents and faculty. This makes a longitudinal study
over a 16-month period difficult, and only 10 out of
59 physicians were present for the full 16 months. A
randomised design with intervention and control groups
might have been easier to organise and more successful in
detecting significant differences. However, given the costs
and effort involved, we wanted to offer communication
training to all anaesthetists in the department. It also
might have been easier to detect significant differences by
measuring anaesthetists’ behaviour directly, but we felt it
was more relevant to measure behaviour indirectly in
terms of patient outcome. Finally, while our anxiety
measures have been validated [11], our measures of
satisfaction with the pre-operative visit have unknown
reliability and validity.
Despite efforts by the American Board of Internal
Medicine to understand patient expectations of doctors’
behaviour [23], it is still not clear which communication
skills should be taught to the different medical specialties.
Recently, a group of experts identified seven essential
tasks of medical communication: building a relationship,
opening the discussion, gathering information, under-
standing the patient’s perspective, sharing information,
reaching agreement on problems and plans, and providing
closure. Our communication training programme inclu-
ded, at least in part, all seven of these elements, which are
published as ‘The Kalamazoo Consensus Statement’ [24].
Such effective communication between doctors and
patients is an important factor in the quality of clinical
care as well as a determinant of patient satisfaction, and
both of these are important markers for health plans in a
competitive health care environment [16]. Therefore, we
encourage Departments of Anaesthesia to continue to
teach communication skills to their anaesthetists and to
investigate the effects of such programmes further.
References
1 Levinson W, Chaumeton N. Communication between
surgeons and patients in routine office visits. Surgery 1999;
125: 127–34.
Anaesthesia, 2004, 59, pages 166–172 C. Harms et al. Æ Improving anaesthetist communication skills......................................................................................................................................................................................................................
� 2004 Blackwell Publishing Ltd 171
2 Hulsman RL, Ros WJ, Winnubst JA, Bensing JM. Teaching
clinically experienced physicians communication skills.
A review of evaluation studies. Medical Education 1999; 33:
655–68.
3 Fletcher GC, McGeorge P, Flin RH, Glavin RJ, Maran NJ.
The role of non-technical skills in anaesthesia: a review of
current literature. British Journal of Anaesthesia 2002; 88:
418–29.
4 The Royal College of Anaesthetists. The Certificate of
Completion of Specialist Training (CCST) in Anaesthesia,
Part I. General Principles, Appendix 2: 23–8. http://
www.rcoa.ac.uk/docs/ccstptied2.pdf.
5 ACGME. American Accreditation Council for Graduate
Medical Education (ACGME). General Competencies, Vers. 1.3.
http://www.acgme.org/outcome/comp/compFull.asp.
6 Lau FL. Can communication skills workshops for emergency
department doctors improve patient satisfaction? Journal of
Accident and Emergency Medicine 2000; 17: 251–3.
7 Smith AF, Shelly MP. Communication skills for anesthe-
siologists. Canadian Journal of Anaesthesia 1999; 46: 1082–8.
8 Kopp VJ, Shafer A. Anesthesiologists and perioperative
communication. Anesthesiology 2000; 93: 548–55.
9 Henwood PG, Altmaier EM. Evaluating the effectiveness of
communication skills training: a review of research. Clinical
Performance and Quality Health Care 1996; 4: 154–8.
10 Fung D, Cohen MM. Measuring patient satisfaction with
anesthesia care: a review of current methodology. Anesthesia
and Analgesia 1998; 87: 1089–98.
11 Kindler CH, Harms C, Amsler F, Ihde-Scholl T, Scheidegger
D. The visual analog scale allows effective measurement of
preoperative anxiety and detection of patients’ anesthetic
concerns. Anesthesia and Analgesia 2000; 90: 706–12.
12 Kindler CH, Harms C, Alber C. The patients’ perception of
the anaesthetist in a Swiss University hospital. Anaesthesist
2002; 51: 890–6.
13 Spielberger CD, Gorsuch RL, Lushene R, Vagg PR, Jacobs
GA. Manual for the State-Trait Anxiety Inventory. Palo Alto:
Consulting Psychologists Press, 1983.
14 Hedeker D, Gibbons RD. A random-effects ordinal
regression model for multilevel analysis. Biometrics 1994;
50: 933–44.
15 SAS Institute Inc. SAS ⁄ STAT User’s Guide, Version 8. Cary:
SAS Institute, 2000.
16 Brown JB, Boles M, Mullooly JP, Levinson W. Effect of
clinician communication skills training on patient satisfac-
tion. A randomized, controlled trial. Annals of Internal
Medicine 1999; 131: 822–9.
17 Cleary PD. Changing clinician behavior: necessary path
to improvement or impossible dream? Annals of Internal
Medicine 1999; 131: 859–60.
18 Smith RC, Lyles JS, Mettler J et al. The effectiveness of
intensive training for residents in interviewing. A random-
ized, controlled study. Annals of Internal Medicine 1998; 128:
118–26.
19 Smith RC, Lyles JS, Mettler JA et al. A strategy for
improving patient satisfaction by the intensive training of
residents in psychosocial medicine: a controlled, randomized
study. Academic Medicine 1995; 70: 729–32.
20 Roter D, Rosenbaum J, de Negri B, Renaud D, DiPrete-
Brown L, Hernandez O. The effects of a continuing medical
education programme in interpersonal communication skills
on doctor practice and patient satisfaction in Trinidad and
Tobago. Medical Education 1998; 32: 181–9.
21 Myles PS, Williams DL, Hendrata M, Anderson H, Weeks
AM. Patient satisfaction after anaesthesia and surgery: results
of a prospective survey of 10,811 patients. British Journal of
Anaesthesia 2000; 84: 6–10.
22 Langewitz W, Keller A, Denz M, Wossmer-Buntschu B,
Kiss A. The Patient Satisfaction Questionnaire: a suitable
tool for quality control in the physician-patient relationship?
Psychotherapie Psychosomatik Medizinische Psychologie 1995; 45:
351–7.
23 Carter WB, Inui TS. Humanistic Behavior of Physicians as
Rated by Patients. Guide to Awareness and Evaluation of
Humanistic Qualities in the Internist. Technical Report.
Philadelphia: American Board of Internal Medicine,
1992.
24 Makoul G. Essential elements of communication in medical
encounters: the Kalamazoo consensus statement. Academic
Medicine 2001; 76: 390–3.
C. Harms et al. Æ Improving anaesthetist communication skills Anaesthesia, 2004, 59, pages 166–172......................................................................................................................................................................................................................
172 � 2004 Blackwell Publishing Ltd