improved long-term outcomes after renal transplantation associated with blood pressure control
TRANSCRIPT
American Journal of Transplantation 2005; 5: 2725–2731Blackwell Munksgaard
Copyright C© Blackwell Munksgaard 2005
doi: 10.1111/j.1600-6143.2005.01093.x
Improved Long-Term Outcomes After RenalTransplantation Associated with Blood PressureControl
Gerhard Opelz∗ and Bernd Dohler for the
Collaborative Transplant Study
Department of Transplantation Immunology, Institute ofImmunology, University of Heidelberg, Germany∗Corresponding author: Gerhard Opelz,[email protected]
Hypertension has a negative impact on long-term out-comes after renal transplantation. We investigated theeffect of a recent decline in blood pressure amongrenal transplant patients in the Collaborative Trans-plant Study (CTS) database on long-term graft and pa-tient survival. CTS data were used to evaluate trans-plant outcomes in relation to recipient systolic bloodpressure (SBP) for 24 404 first cadaver kidney recip-ients transplanted between 1987 and 2000. Patientswhose SBP was >140 mmHg at 1 year posttransplan-tation but controlled to ≤140 mmHg by 3 years hadsignificantly improved long-term graft outcome com-pared with patients with sustained high SBP to 3 years(RR 0.79; CI 0.73-−0.86; p < 0.001). Additional exam-ination at 5 years showed that SBP lowering afteryear 3 was associated with improved 10-year graft sur-vival (RR 0.83; CI 0.72–0.96; p = 0.01), whereas evena temporary increase in SBP at 3 years was associ-ated with worse survival (RR 1.37; CI 1.19–1.58; p <0.001). Changes in SBP were paralleled by changes inthe incidence of cardiovascular death among recipi-ents younger than 50 but not in older recipients. Low-ering SBP, even after several years of posttransplanta-tion hypertension, is associated with improved graftand patient survival in renal allograft recipients.
Key words: Blood pressure control, hypertension,long-term transplant outcomes, renal transplantation
Received 18 April 2005, revised and accepted for pub-lication 30 July 2005.
Introduction
Chronic allograft nephropathy is the main factor contribut-ing to late renal allograft loss (1). As immunologic causesof chronic kidney graft failure have been increasinglycontrolled through effective immunosuppression, nonim-munologic mechanisms are being targeted as important
mediators of reduced long-term renal function. In the non-transplant setting, elevation of blood pressure (BP) plays asignificant role in the production of progressive renal dam-age (2–5). Although the deleterious effect of hypertensionon graft function has been a long-standing observation, thelarge retrospective study from the Collaborative TransplantStudy (CTS) first demonstrated a strong, graded relation-ship between posttransplant BP and renal allograft failure(6), and subsequent studies demonstrated that this find-ing was independent of acute rejection and baseline renalfunction, thus suggesting that progressive renal dysfunc-tion was the result of elevated BP (7,8).
BP is a modifiable determinant of renal function, and theimprovement in renal function in primary renal disease withantihypertensive agents is well documented (9,10). By ex-tension, adequate control of BP in the transplant settingshould help preserve allograft function and improve long-term outcomes. However, our study in 1998 found that inclinical practice, BP control is suboptimal and as many as50% of patients have a systolic blood pressure (SBP) >140mmHg, a finding confirmed in another recent study (8). Abeneficial effect of BP lowering in preventing renal allograftdeterioration has been difficult to demonstrate, althoughevidence suggests that satisfactory control of hyperten-sion was associated with renal protection to 2.5 years offollow-up (11).
The extent to which the finding linking worse allograft func-tion with poorly controlled BP has translated into morerigorous control of BP in clinical practice remains uncer-tain. A recent large single-center study that examined theprevalence of hypertension found only a slight improve-ment in BP control in recent years (1993–2000) comparedwith previous years (1976–1992) (8). PosttransplantationBP has been documented in the CTS database since 1987,and our data show little change in SBP between 1987 and1997, which remained consistently high at a median of140–141 mmHg. Although some improvement did occurbefore 1998, a significant decline in the fraction of patientswith SBP >140 mmHg has occurred only after 1997. It hasnot been determined whether lowering BP after severalyears of exposure to high BP can impact long-term graftoutcomes. In this large retrospective study, we examinedthe relationship of BP control in transplant recipients tolong-term graft and patient survival. We present results for
2725

Opelz and Dohler
a patient population receiving mainly a CYA-based immuno-suppressive regimen and show evidence suggesting thataggressive BP management can provide significant long-term benefits after renal transplantation.
Methods
Patients
A total of 24 404 adult first cadaver renal transplant recipients (age≥20 years) reported to the CTS by 258 transplant centers were includedin the analysis (12). Outpatient BP measurements and clinical follow-up in-formation were obtained at yearly intervals after transplantation. The trans-plants were performed between 1987 and 2000. The primary outcomeswere patient and graft survival up to 10 years. Functional graft survival wasalso determined after censoring patients dying with a functioning graft. Graftloss was determined by return to dialysis or death. Rates of cardiovasculardeath during follow-up were calculated from the cause of death indicationsreported to the CTS database.
Our analysis was limited to SBP because we showed previously that theprimary deleterious effect was due to systolic and not diastolic pressure (6).In accordance with the WHO standard and previously published studies,we chose a cutoff value of 140 mmHg and included all patients in whomSBP at 1 and 3 years posttransplant was reported to the study center; noexclusions were made. For evaluation of the recent changes in SBP, weincluded 3571 patients transplanted in 2001 and 2002 for whom 1-yearvalues were available. In additional analyses, we included 5-year SBP tostudy the effect of long-standing hypertension, as well as that of temporarydecreases or increases of SBP on long-term outcomes.
Statistical analysis
The Kaplan–Meier method was used to estimate graft and patient survivalas well as the rate of cardiovascular death. To control for the confoundinginfluence of demographic differences in patient populations, multivariateanalysis was performed with a Cox regression model using the follow-ing variables: recipient and donor gender; race and age (stratified by 10-year intervals); year of transplantation; geographical location of transplantcenter (continent); cause of end-stage renal disease; cold ischemic preser-vation time; percent panel-reactive antibodies; number of HLA-A+B+DRmismatches; immunosuppressive regimen (intention to treat); use of anti-lymphocyte antibodies for induction; acute rejection episodes; serum cre-atinine and administration of antihypertensive medication. Cox regressionresults are indicated as relative risk (RR) and 95% confidence interval (CI).The Mantel–Haenzel test was used to analyze the decrease in SBP duringrecent years and the log-rank test was used for pairwise comparison of sur-vival curves. Chi-square analysis was used to test for differences in patientdemographics. p-Values <0.05 were considered significant.
Results
Study population
BP measurements at 1 and 3 years were available for24 404 first cadaver kidney recipients. Demographic char-acteristics of the patients are shown in Table 1. As ex-pected, patients with SBP >140 mmHg differed fromthose with SBP ≤140 mmHg with respect to most vari-ables examined; because of the large numbers of trans-plants studied, even small numerical differences resultedin statistically significant p-values. This was the basis for
conducting a Cox regression analysis in which these fac-tors were specifically considered.
Prevalence of hypertension 1 and 3 years
posttransplantation
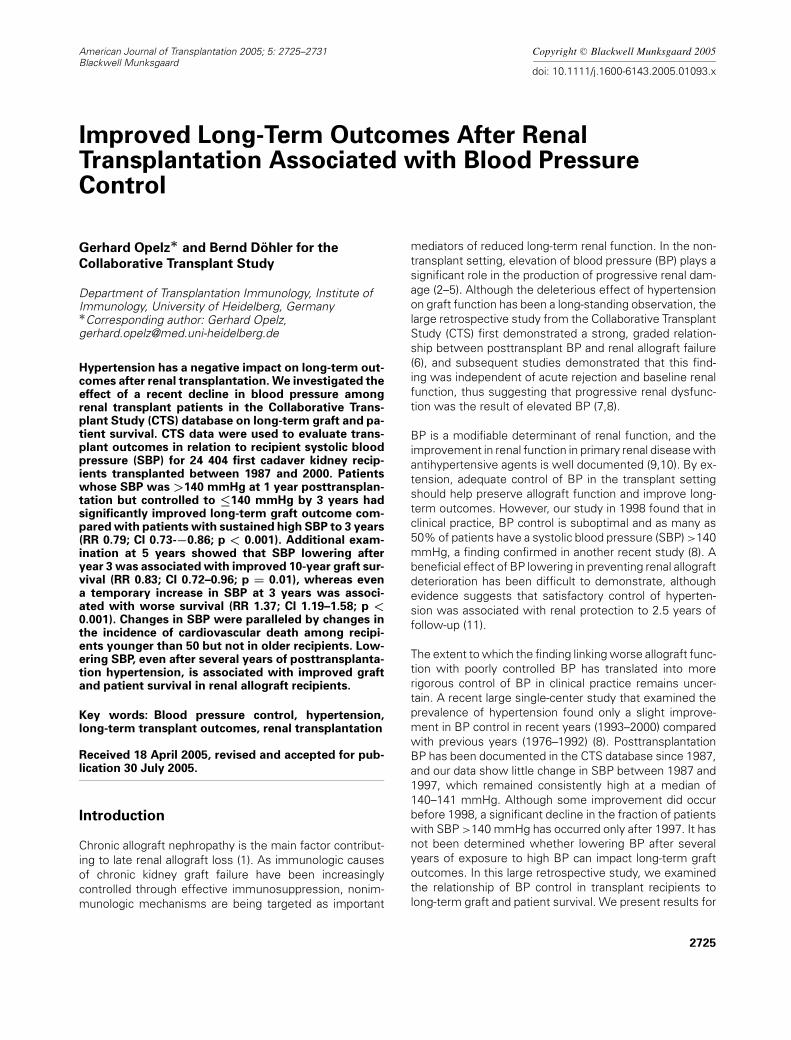
The fraction of patients with SBP >140 mmHg at 1 and3 years posttransplantation from 1990 to 2003 (transplantyears 1987–2000) is shown in Figure 1. The percentage ofpatients with SBP >140 mmHg decreased only modestlyup to the year 1997 (Mantel–Haenzel test: p = 0.10 andp = 0.17 for year 1 and 3, respectively), but improvementin SBP accelerated from 1998 onward (p < 0.001 at both1 and 3 years). At 1 year posttransplant, the difference inthe fraction of patients with SBP >140 mmHg betweenthe periods 1990–1991 and 1996–1997 was a mere 1.5%(38.5% vs. 37.0%), whereas it increased to 10.6% (37.0%vs. 26.4%) when the intervals 1996–1997 and 2002–2003were compared. Similarly, at 3 years posttransplant, the dif-ference between the intervals 1990–1991 and 1996–1997was 0.9% (39.5% vs. 38.6%) whereas the difference be-tween the intervals 1996–1997 and 2002–2003 was 11.4%(38.6% vs. 27.2%).
BP control during the first 3 years posttransplantation
and transplant outcomes
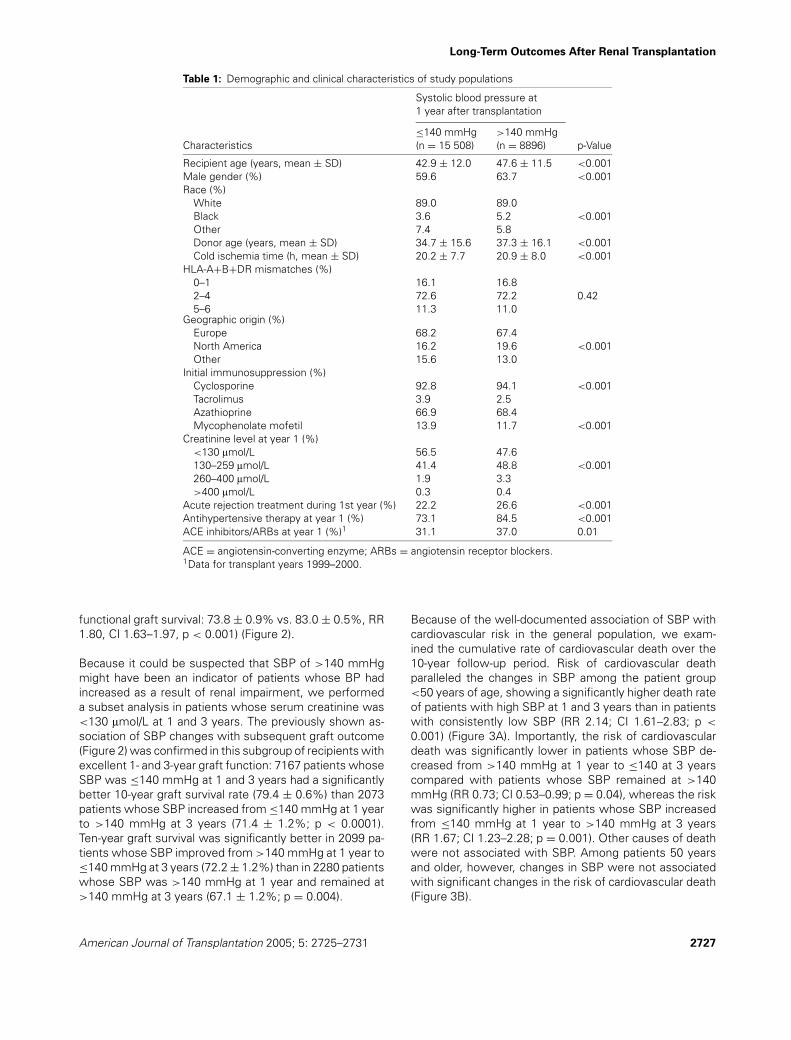
We next examined the influence of different levels of BPcontrol between 1 and 3 years posttransplantation on graftand patient outcomes at 10 years (Figure 2). The best10-year graft and patient survival rates were obtained whenthe SBP was maintained at ≤140 mmHg between 1 and3 years (72.2 ± 0.5% and 85.4 ± 0.4%, respectively) andworst when the SBP exceeded 140 mmHg at both times(54.1 ± 0.9% and 72.8 ± 0.8%, respectively). Cox regres-sion analysis confirmed that higher SBP at 1 and 3 yearswas associated with increased risk of graft failure (RR 1.61;CI 1.50–1.72; p < 0.001) and death (RR 1.35; CI 1.23–1.48;p < 0.001). Importantly, patients who had a high SBP at1 year posttransplantation but whose SBP was subse-quently controlled to ≤140 mmHg by 3 years, showedsignificantly better 10-year graft survival compared withpatients in whom SBP remained high, indicating that low-ering of pressure even after at least 1 year of increasedposttransplant pressure was beneficial to graft outcome(62.2 ± 1.0% vs. 54.1 ± 0.9%; RR 0.79; CI 0.73–0.86;p < 0.001). Death-censored functional survival also wassignificantly better (77.9 ± 0.9% vs. 70.6 ± 0.9%; RR 0.70;CI 0.63–0.77; p < 0.001). However, the small improve-ment in patient survival did not reach statistical significance(77.1 ± 0.8% vs. 72.8 ± 0.8%; RR 0.93; CI 0.84–1.03;p = 0.15). Conversely, patients whose SBP increased from≤140 mmHg at 1 year to >140 mmHg at 3 years showed10-year graft and patient survival rates that were strikinglylower than those in patients whose SBP remained consis-tently low (graft survival: 59.7 ± 1.0% vs. 72.2 ± 0.5%,RR 1.52, CI 1.41–1.63, p < 0.001; patient survival: 78.2 ±0.8% vs. 85.4 ± 0.4%, RR 1.27, CI 1.15–1.40, p < 0.001;
2726 American Journal of Transplantation 2005; 5: 2725–2731
Long-Term Outcomes After Renal Transplantation
Table 1: Demographic and clinical characteristics of study populations
Systolic blood pressure at1 year after transplantation
≤140 mmHg >140 mmHgCharacteristics (n = 15 508) (n = 8896) p-Value
Recipient age (years, mean ± SD) 42.9 ± 12.0 47.6 ± 11.5 <0.001Male gender (%) 59.6 63.7 <0.001Race (%)
White 89.0 89.0Black 3.6 5.2 <0.001Other 7.4 5.8Donor age (years, mean ± SD) 34.7 ± 15.6 37.3 ± 16.1 <0.001Cold ischemia time (h, mean ± SD) 20.2 ± 7.7 20.9 ± 8.0 <0.001
HLA-A+B+DR mismatches (%)0–1 16.1 16.82–4 72.6 72.2 0.425–6 11.3 11.0
Geographic origin (%)Europe 68.2 67.4North America 16.2 19.6 <0.001Other 15.6 13.0
Initial immunosuppression (%)Cyclosporine 92.8 94.1 <0.001Tacrolimus 3.9 2.5Azathioprine 66.9 68.4Mycophenolate mofetil 13.9 11.7 <0.001
Creatinine level at year 1 (%)<130 lmol/L 56.5 47.6130–259 lmol/L 41.4 48.8 <0.001260–400 lmol/L 1.9 3.3>400 lmol/L 0.3 0.4
Acute rejection treatment during 1st year (%) 22.2 26.6 <0.001Antihypertensive therapy at year 1 (%) 73.1 84.5 <0.001ACE inhibitors/ARBs at year 1 (%)1 31.1 37.0 0.01
ACE = angiotensin-converting enzyme; ARBs = angiotensin receptor blockers.1Data for transplant years 1999–2000.
functional graft survival: 73.8 ± 0.9% vs. 83.0 ± 0.5%, RR1.80, CI 1.63–1.97, p < 0.001) (Figure 2).
Because it could be suspected that SBP of >140 mmHgmight have been an indicator of patients whose BP hadincreased as a result of renal impairment, we performeda subset analysis in patients whose serum creatinine was<130 lmol/L at 1 and 3 years. The previously shown as-sociation of SBP changes with subsequent graft outcome(Figure 2) was confirmed in this subgroup of recipients withexcellent 1- and 3-year graft function: 7167 patients whoseSBP was ≤140 mmHg at 1 and 3 years had a significantlybetter 10-year graft survival rate (79.4 ± 0.6%) than 2073patients whose SBP increased from ≤140 mmHg at 1 yearto >140 mmHg at 3 years (71.4 ± 1.2%; p < 0.0001).Ten-year graft survival was significantly better in 2099 pa-tients whose SBP improved from >140 mmHg at 1 year to≤140 mmHg at 3 years (72.2 ± 1.2%) than in 2280 patientswhose SBP was >140 mmHg at 1 year and remained at>140 mmHg at 3 years (67.1 ± 1.2%; p = 0.004).
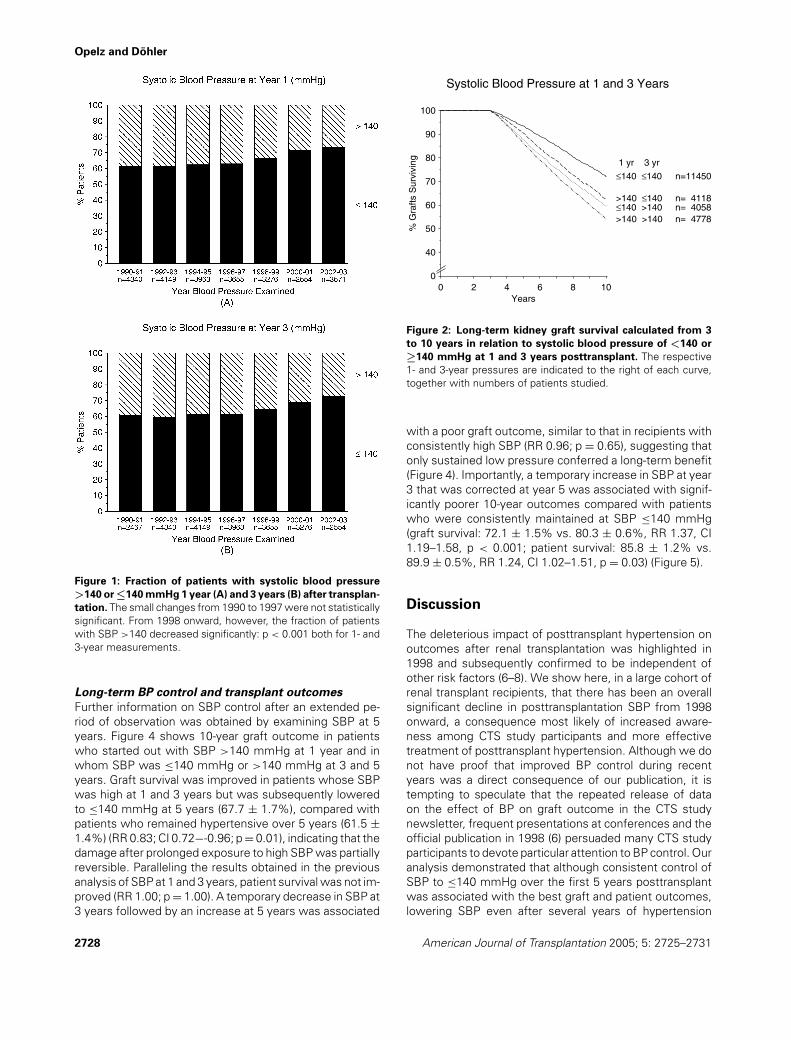
Because of the well-documented association of SBP withcardiovascular risk in the general population, we exam-ined the cumulative rate of cardiovascular death over the10-year follow-up period. Risk of cardiovascular deathparalleled the changes in SBP among the patient group<50 years of age, showing a significantly higher death rateof patients with high SBP at 1 and 3 years than in patientswith consistently low SBP (RR 2.14; CI 1.61–2.83; p <
0.001) (Figure 3A). Importantly, the risk of cardiovasculardeath was significantly lower in patients whose SBP de-creased from >140 mmHg at 1 year to ≤140 at 3 yearscompared with patients whose SBP remained at >140mmHg (RR 0.73; CI 0.53–0.99; p = 0.04), whereas the riskwas significantly higher in patients whose SBP increasedfrom ≤140 mmHg at 1 year to >140 mmHg at 3 years(RR 1.67; CI 1.23–2.28; p = 0.001). Other causes of deathwere not associated with SBP. Among patients 50 yearsand older, however, changes in SBP were not associatedwith significant changes in the risk of cardiovascular death(Figure 3B).
American Journal of Transplantation 2005; 5: 2725–2731 2727
Opelz and Dohler
Figure 1: Fraction of patients with systolic blood pressure
>140 or ≤140 mmHg 1 year (A) and 3 years (B) after transplan-
tation. The small changes from 1990 to 1997 were not statisticallysignificant. From 1998 onward, however, the fraction of patientswith SBP >140 decreased significantly: p < 0.001 both for 1- and3-year measurements.
Long-term BP control and transplant outcomes
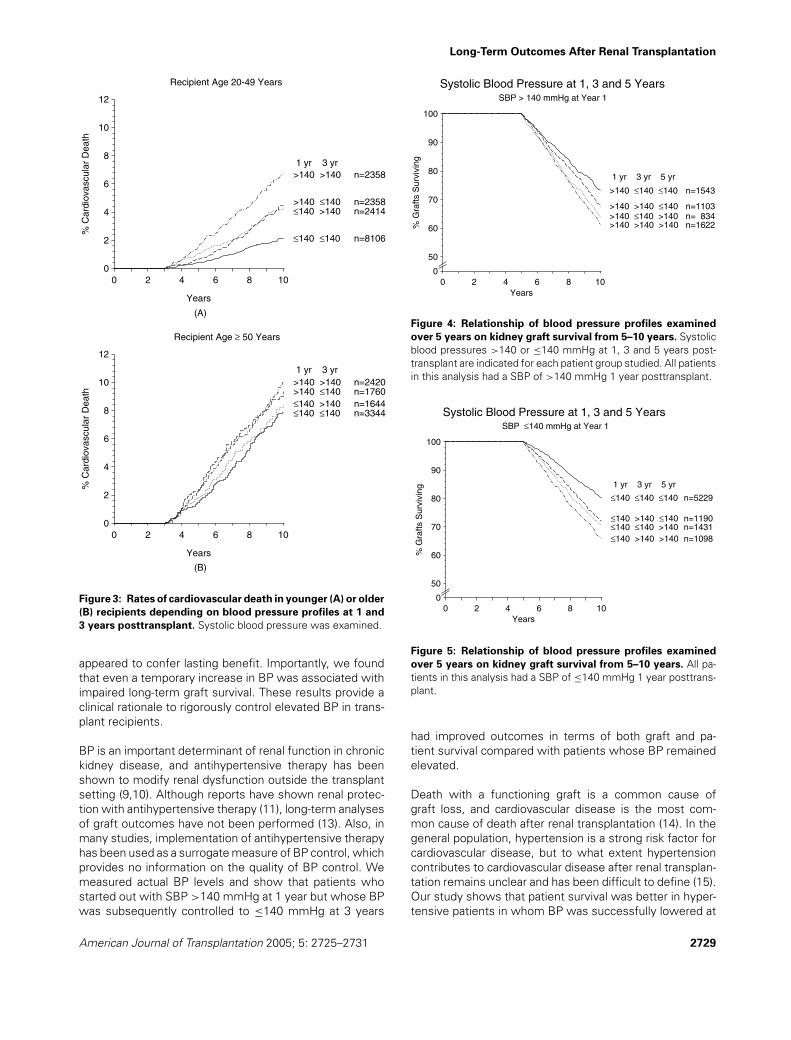
Further information on SBP control after an extended pe-riod of observation was obtained by examining SBP at 5years. Figure 4 shows 10-year graft outcome in patientswho started out with SBP >140 mmHg at 1 year and inwhom SBP was ≤140 mmHg or >140 mmHg at 3 and 5years. Graft survival was improved in patients whose SBPwas high at 1 and 3 years but was subsequently loweredto ≤140 mmHg at 5 years (67.7 ± 1.7%), compared withpatients who remained hypertensive over 5 years (61.5 ±1.4%) (RR 0.83; CI 0.72−-0.96; p = 0.01), indicating that thedamage after prolonged exposure to high SBP was partiallyreversible. Paralleling the results obtained in the previousanalysis of SBP at 1 and 3 years, patient survival was not im-proved (RR 1.00; p = 1.00). A temporary decrease in SBP at3 years followed by an increase at 5 years was associated
Systolic Blood Pressure at 1 and 3 Years
0
100
90
80
70
60
50
40
% G
rafts
Sur
vivi
ng
0 2 4 6 8 10Years
11450 n=≤140 ≤140
4118 n=>140 ≤140 4058 n=≤140 >140 4778 n=>140 >140
1 yr 3 yr
Figure 2: Long-term kidney graft survival calculated from 3
to 10 years in relation to systolic blood pressure of <140 or
≥140 mmHg at 1 and 3 years posttransplant. The respective1- and 3-year pressures are indicated to the right of each curve,together with numbers of patients studied.
with a poor graft outcome, similar to that in recipients withconsistently high SBP (RR 0.96; p = 0.65), suggesting thatonly sustained low pressure conferred a long-term benefit(Figure 4). Importantly, a temporary increase in SBP at year3 that was corrected at year 5 was associated with signif-icantly poorer 10-year outcomes compared with patientswho were consistently maintained at SBP ≤140 mmHg(graft survival: 72.1 ± 1.5% vs. 80.3 ± 0.6%, RR 1.37, CI1.19–1.58, p < 0.001; patient survival: 85.8 ± 1.2% vs.89.9 ± 0.5%, RR 1.24, CI 1.02–1.51, p = 0.03) (Figure 5).
Discussion
The deleterious impact of posttransplant hypertension onoutcomes after renal transplantation was highlighted in1998 and subsequently confirmed to be independent ofother risk factors (6–8). We show here, in a large cohort ofrenal transplant recipients, that there has been an overallsignificant decline in posttransplantation SBP from 1998onward, a consequence most likely of increased aware-ness among CTS study participants and more effectivetreatment of posttransplant hypertension. Although we donot have proof that improved BP control during recentyears was a direct consequence of our publication, it istempting to speculate that the repeated release of dataon the effect of BP on graft outcome in the CTS studynewsletter, frequent presentations at conferences and theofficial publication in 1998 (6) persuaded many CTS studyparticipants to devote particular attention to BP control. Ouranalysis demonstrated that although consistent control ofSBP to ≤140 mmHg over the first 5 years posttransplantwas associated with the best graft and patient outcomes,lowering SBP even after several years of hypertension
2728 American Journal of Transplantation 2005; 5: 2725–2731
Long-Term Outcomes After Renal Transplantation
Recipient Age 20-49 Years
0
12
10
8
6
4
2
% C
ardi
ovas
cula
r D
eath
0 2 4 6 8 10
Years
2358 n=>140 >140
2358 n=>140 ≤140 2414 n=≤140 >140
8106 n=≤140 ≤140
1 yr 3 yr
Recipient Age ≥ 50 Years
0
12
10
8
6
4
2
% C
ardi
ovas
cula
r D
eath
0 2 4 6 8 10
Years
2420 n=>140 >140 1760 n=>140 ≤140 1644 n=≤140 >140 3344 n=≤140 ≤140
1 yr 3 yr
(A)
(B)
Figure 3: Rates of cardiovascular death in younger (A) or older
(B) recipients depending on blood pressure profiles at 1 and
3 years posttransplant. Systolic blood pressure was examined.
appeared to confer lasting benefit. Importantly, we foundthat even a temporary increase in BP was associated withimpaired long-term graft survival. These results provide aclinical rationale to rigorously control elevated BP in trans-plant recipients.
BP is an important determinant of renal function in chronickidney disease, and antihypertensive therapy has beenshown to modify renal dysfunction outside the transplantsetting (9,10). Although reports have shown renal protec-tion with antihypertensive therapy (11), long-term analysesof graft outcomes have not been performed (13). Also, inmany studies, implementation of antihypertensive therapyhas been used as a surrogate measure of BP control, whichprovides no information on the quality of BP control. Wemeasured actual BP levels and show that patients whostarted out with SBP >140 mmHg at 1 year but whose BPwas subsequently controlled to ≤140 mmHg at 3 years
SBP > 140 mmHg at Year 1
Systolic Blood Pressure at 1, 3 and 5 Years
0
100
90
80
70
60
50
% G
rafts
Sur
vivi
ng
0 2 4 6 8 10Years
1543 n=>140 ≤140 ≤140
1103 n=>140 >140 ≤140834 n=>140 ≤140 >140
1622 n=>140 >140 >140
1 yr 3 yr 5 yr
Figure 4: Relationship of blood pressure profiles examined
over 5 years on kidney graft survival from 5–10 years. Systolicblood pressures >140 or ≤140 mmHg at 1, 3 and 5 years post-transplant are indicated for each patient group studied. All patientsin this analysis had a SBP of >140 mmHg 1 year posttransplant.
SBP ≤ 140 mmHg at Year 1
Systolic Blood Pressure at 1, 3 and 5 Years
0
100
90
80
70
60
50
% G
rafts
Sur
vivi
ng
0 2 4 6 8 10Years
5229 n=≤140 ≤140 ≤140
1190 n=≤140 >140 ≤1401431 n=≤140 ≤140 >1401098 n=≤140 >140 >140
1 yr 3 yr 5 yr
Figure 5: Relationship of blood pressure profiles examined
over 5 years on kidney graft survival from 5–10 years. All pa-tients in this analysis had a SBP of ≤140 mmHg 1 year posttrans-plant.
had improved outcomes in terms of both graft and pa-tient survival compared with patients whose BP remainedelevated.
Death with a functioning graft is a common cause ofgraft loss, and cardiovascular disease is the most com-mon cause of death after renal transplantation (14). In thegeneral population, hypertension is a strong risk factor forcardiovascular disease, but to what extent hypertensioncontributes to cardiovascular disease after renal transplan-tation remains unclear and has been difficult to define (15).Our study shows that patient survival was better in hyper-tensive patients in whom BP was successfully lowered at
American Journal of Transplantation 2005; 5: 2725–2731 2729

Opelz and Dohler
3 years compared with those who continued to be hyper-tensive at 3 years. Considering the potentially confoundingfactors listed in Table 1, multivariate Cox regression anal-ysis demonstrated that this effect was attributable to adecrease in the rate of cardiovascular death. The findingthat the cardiovascular death rate did not improve in olderpatients may reflect a more severe impact of pretransplantchronic kidney disease in older recipients.
Although we observed a decrease in overall posttransplan-tation BP since 1998 compared with earlier time periods, ahigh percentage of transplant patients continue to be main-tained at BP values associated with an increased incidenceof graft failure. A recent report documented that as manyas 46% of renal recipients have a SBP >140 mmHg after1 year (8). Our study suggests that the window of opportu-nity to derive a benefit from BP lowering is wide and thatBP lowering undertaken even several years after transplan-tation can still confer significant benefits for graft survival.Thus patients whose hypertension was poorly controlledat 1 or 3 years posttransplantation had better outcomes iftheir 5-year SBP was controlled to ≤140 mmHg than thosewho continued to have hypertension to 5 years. Our find-ings further highlight the importance of sustained controlof hypertension, as patients derived little benefit from tem-porary control. Conversely, a temporary increase in SBP at3 years was detrimental to 10-year graft survival, comparedwith graft survival in patients whose SBP was consistently≤140 mmHg.
Earlier studies argued that increased BP is not the causebut is simply a marker of chronic allograft dysfunction thatmight develop as a consequence of other risk factors ofpoor allograft outcomes (16,17). Our analysis showed thatimproved BP control was beneficial even in patients withexcellent graft function. Further supporting the indepen-dent beneficial effect of reduced BP is that our Cox regres-sion analysis showed improved BP control to be associatedwith better graft outcome irrespective of serum creatinineand the occurrence of acute rejection episodes.
Poor control of hypertension in renal transplant recipientsmay stem from insufficient treatment, refractoriness totreatment or patient noncompliance. Currently, there areno guidelines on the optimal level of BP control in re-nal transplant recipients or on the most appropriate an-tihypertensive agents (18,19). It may be argued that be-cause newer antihypertensive agents such as ACE in-hibitors have renoprotective effects independent of BP(20,21), improved long-term outcomes may have been aresult of these other renal benefits. However, we havefound a similar beneficial effect of BP control in the groupof patients transplanted from 1987 to 1990 when only fewpatients received the new agents (6) (not shown).
A weakness of our study is the lack of randomization, whichwould have guaranteed that patients with good or poor BPcontrol were clinically similar. However, because of ethi-
cal considerations, such a trial is unlikely to be performed.Our data, although derived retrospectively, are the mostconvincing to date suggesting that control of BP, even if in-stituted late after transplantation, improves outcomes. An-other drawback is that we were unable to determine howmany patients were managed with particularly intensiveBP treatment. Data on the high prevalence of transplantpatients with SBP >140 mmHg suggest that BP reductionoften is not being undertaken vigorously. It is thereforelikely that with more aggressive measures, the benefits oflower BP would be evident in a higher percentage of pa-tients. Our study provides an estimate of the magnitudeof the improvement that can be attained when BP is suc-cessfully lowered. It should be noted that the trend towardimproved BP was documented in the centers reporting tothe CTS who also had provided the data for our initial studyon posttransplant hypertension and thus were aware ofthis issue (6); it is uncertain whether the data can be gen-eralized to centers not participating in the CTS. Becauseonly a small fraction of the patients analyzed were non-Caucasian, the results are not representative for patientsof African or African American origin.
In conclusion, there has been a decline in posttransplanta-tion hypertension among transplants reported to the CTSstudy in recent years, in all likelihood because of a height-ened awareness of the deleterious effects of hypertensionon renal allografts and consequently more vigorous inter-vention. The observed improvements in long-term graftand patient outcomes underscore the potential value of ag-gressively controlling BP after transplantation, particularlybecause our data suggest that the benefits of lowering BPcan be realized even after several years of hypertension.With the current paucity of donor kidneys the need to op-timize graft outcomes is greater than ever, and risk factorssuch as hypertension that are amenable to interventionmust be actively controlled.
Acknowledgment
We thank the 258 transplant centers for generously providing the data onwhich this analysis was based.
References
1. Hariharan S. Long-term kidney transplant survival. Am J KidneyDis 2001; 38 (Suppl 6): S44–S50.
2. Klag MJ, Whelton PK, Randall BL et al. Blood pressure and end-stage renal disease in men. N Engl J Med 1996; 334: 13–18.
3. Chobanian AV, Bakris GL, Black HR et al. Seventh report of theJoint National Committee on Prevention, Detection, Evaluation,and Treatment of High Blood Pressure. Hypertension 2003; 42:1206–1252.
4. Whitworth JA. World Health Organization, International Societyof Hypertension Writing Group. 2003 World Health Organization(WHO)/International Society of Hypertension (ISH) statement onmanagement of hypertension. J Hypertens 2003; 21: 1983–1992.
2730 American Journal of Transplantation 2005; 5: 2725–2731

Long-Term Outcomes After Renal Transplantation
5. Lewington S, Clarke R, Qizilbash N, Peto R, Collins R. Prospec-tive Studies Collaboration. Age-specific relevance of usual bloodpressure to vascular mortality: A meta-analysis of individual datafor one million adults in 61 prospective studies. Lancet 2002; 360:1903–1913.
6. Opelz G, Wujciak T, Ritz E. Association of chronic kidney graft fail-ure with recipient blood pressure. Collaborative Transplant Study.Kidney Int 1998; 53: 217–222.
7. Mange KC, Cizman B, Joffe M, Feldman HL. Arterial hypertensionand renal allograft survival. JAMA 2000; 283: 633–638.
8. Kasiske BL, Anjum S, Shah R et al. Hypertension after kidneytransplantation. Am J Kidney Dis 2004; 43: 1071–1081.
9. Walker WG, Neaton JD, Cutler JA, Neuwirth R, Cohen JD. Renalfunction change in hypertensive members of the Multiple RiskFactor Intervention Trial. Racial and treatment effects. The MRFITResearch Group. JAMA 1992; 268: 3085–3091.
10. Peterson JC, Adler S, Burkart JM et al. Blood pressure control,proteinuria, and the progression of renal disease. The Modifica-tion of Diet in Renal Disease Study. Ann Intern Med 1995; 123:754–762.
11. Mourad G, Ribstein J, Mimran A. Converting-enzyme inhibitor ver-sus calcium antagonist in cyclosporine-treated renal transplants.Kidney Int 1993; 43: 419–425.
12. Collaborative Transplant Study. http://www.ctstransplant.org. Ac-cessed March 1, 2005.
13. Raine AEG. Does antihypertensive therapy modify chronicallograft failure? Kidney Int 1995; 48 (Suppl 52): S107–S111.
14. Ojo AO, Hanson JA, Wolfe RA, Leichtman AB, Agodoa LY, PortFK. Long-term survival in renal transplant recipients with graftfunction. Kidney Int 2000; 57: 307–313.
15. Kasiske BL. Cardiovascular disease after renal transplantation.Semin Nephrol 2000; 20: 176–187.
16. Sanders CE, Curtis JJ. Role of hypertension in chronic re-nal allograft dysfunction. Kidney Int 1995; 48 (Suppl 52): S43–S47.
17. Curtis JJ. Distinguishing the causes of post-transplantation hy-pertension. Pediatr Nephrol 1991; 5: 108–111.
18. Midtvedt K, Hartmann A. Hypertension after kidney transplanta-tion: Are treatment guidelines emerging? Nephrol Dial Transplant2002; 17: 1166–1169.
19. Zeier M, Mandelbaum A, Ritz E. Hypertension in the transplantedpatient. Nephron 1998; 80: 257–268.
20. Barnett AH, Bain SC, Bouter P et al Diabetics Exposed to Telmisar-tan and Enalapril Study Group. Angiotensin-receptor blockade ver-sus converting-enzyme inhibition in type 2 diabetes and nephropa-thy. N Engl J Med 2004; 351(19): 1952–1961.
21. Coyle JD, Gardner SF, White CM. The renal protective effects ofangiotensin II receptor blockers in type 2 diabetes mellitus. AnnPharmacother 2004; 38: 1731–1738.
American Journal of Transplantation 2005; 5: 2725–2731 2731