implementing work-based assessments professor t.masud nottingham university hospitals nhs trust
TRANSCRIPT
Implementing Work-Based Implementing Work-Based AssessmentsAssessments
Professor T.MasudProfessor T.Masud
Nottingham University Hospitals Nottingham University Hospitals NHS TrustNHS Trust
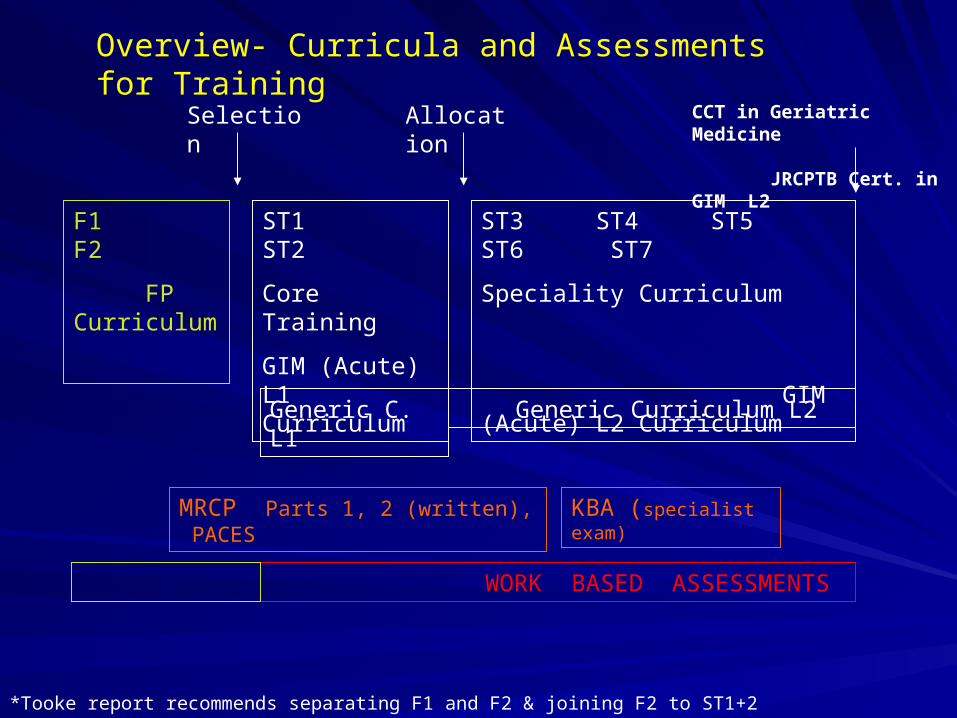
ST1 ST2
Core Training
GIM (Acute) L1 Curriculum
F1 F2
FP Curriculum
ST3 ST4 ST5 ST6 ST7
Speciality Curriculum
GIM (Acute) L2 Curriculum
Generic C. L1 Generic Curriculum L2
CCT in Geriatric Medicine JRCPTB Cert. in GIM L2
Selection Allocation
MRCP Parts 1, 2 (written), PACES KBA (specialist exam)
WORK BASED ASSESSMENTS
Overview- Curricula and Assessments for Training
*Tooke report recommends separating F1 and F2 & joining F2 to ST1+2
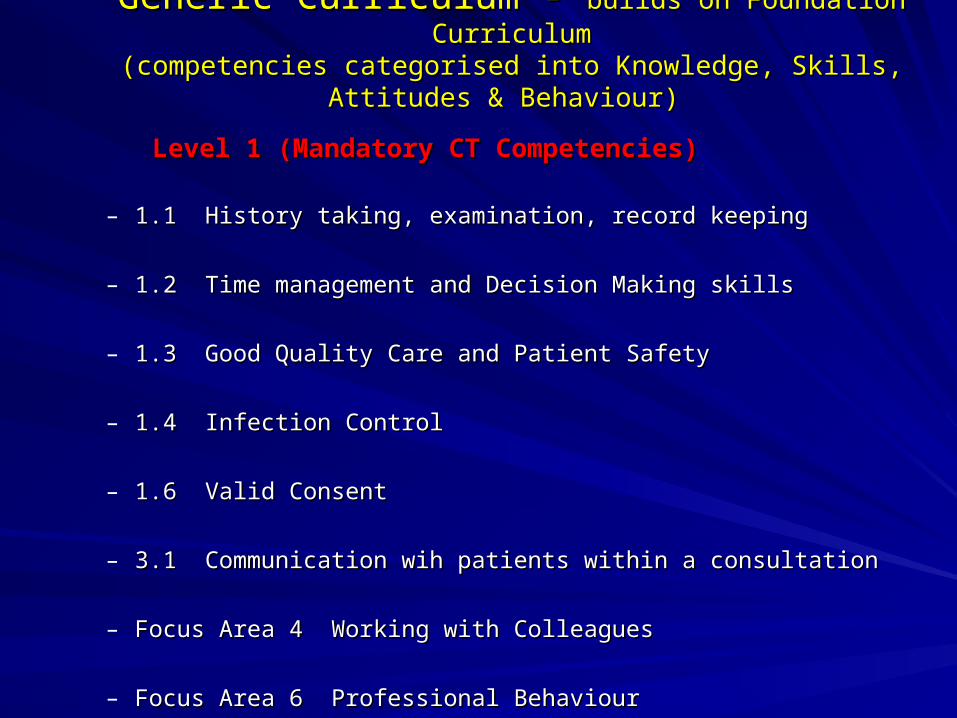
Generic Curriculum - Generic Curriculum - builds on Foundation Curriculumbuilds on Foundation Curriculum(competencies categorised into Knowledge, Skills, Attitudes & Behaviour)(competencies categorised into Knowledge, Skills, Attitudes & Behaviour)
Level 1 (Mandatory CT Competencies)Level 1 (Mandatory CT Competencies)
– 1.1 History taking, examination, record keeping1.1 History taking, examination, record keeping
– 1.2 Time management and Decision Making skills1.2 Time management and Decision Making skills
– 1.3 Good Quality Care and Patient Safety1.3 Good Quality Care and Patient Safety
– 1.4 Infection Control1.4 Infection Control
– 1.6 Valid Consent1.6 Valid Consent
– 3.1 Communication wih patients within a consultation3.1 Communication wih patients within a consultation
– Focus Area 4 Working with ColleaguesFocus Area 4 Working with Colleagues
– Focus Area 6 Professional Behaviour Focus Area 6 Professional Behaviour
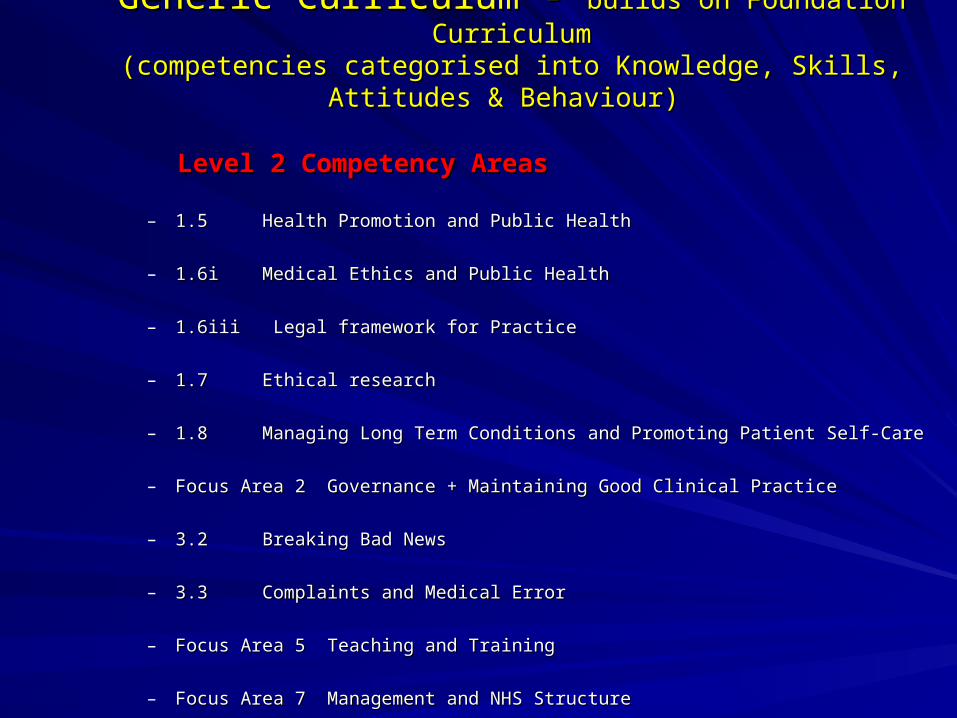
Generic Curriculum - Generic Curriculum - builds on Foundation Curriculumbuilds on Foundation Curriculum(competencies categorised into Knowledge, Skills, Attitudes & Behaviour)(competencies categorised into Knowledge, Skills, Attitudes & Behaviour)
Level 2 Competency AreasLevel 2 Competency Areas
– 1.5 Health Promotion and Public Health1.5 Health Promotion and Public Health
– 1.6i Medical Ethics and Public Health1.6i Medical Ethics and Public Health
– 1.6iii Legal framework for Practice1.6iii Legal framework for Practice
– 1.7 Ethical research1.7 Ethical research
– 1.8 Managing Long Term Conditions and Promoting Patient Self-Care1.8 Managing Long Term Conditions and Promoting Patient Self-Care
– Focus Area 2 Governance + Maintaining Good Clinical PracticeFocus Area 2 Governance + Maintaining Good Clinical Practice
– 3.2 Breaking Bad News3.2 Breaking Bad News
– 3.3 Complaints and Medical Error3.3 Complaints and Medical Error
– Focus Area 5 Teaching and TrainingFocus Area 5 Teaching and Training
– Focus Area 7 Management and NHS StructureFocus Area 7 Management and NHS Structure
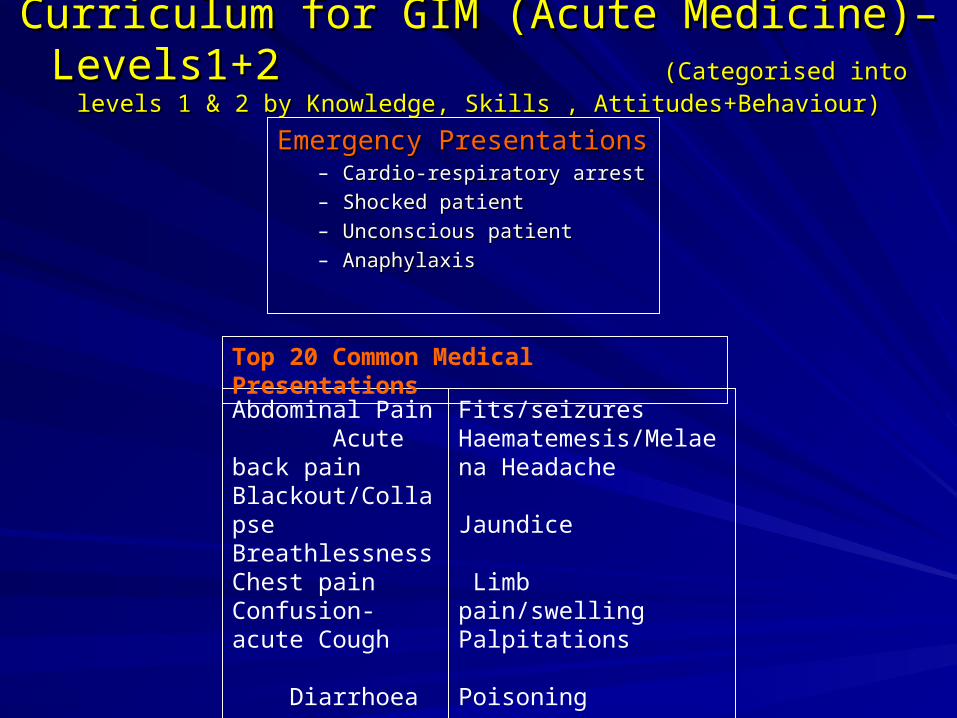
Curriculum for GIM (Acute Medicine)– Levels1+2 Curriculum for GIM (Acute Medicine)– Levels1+2 (Categorised into levels 1 & 2 by Knowledge, Skills , Attitudes+Behaviour)(Categorised into levels 1 & 2 by Knowledge, Skills , Attitudes+Behaviour)
Emergency PresentationsEmergency Presentations– Cardio-respiratory arrestCardio-respiratory arrest
– Shocked patientShocked patient
– Unconscious patientUnconscious patient
– AnaphylaxisAnaphylaxis
Abdominal Pain Acute back pain Blackout/Collapse Breathlessness Chest pain Confusion- acute Cough Diarrhoea Falls Fever-
Fits/seizures Haematemesis/Melaena Headache Jaundice Limb pain/swelling Palpitations Poisoning Rash Vomiting /nausea Weakness/Paralysis
Top 20 Common Medical Presentations
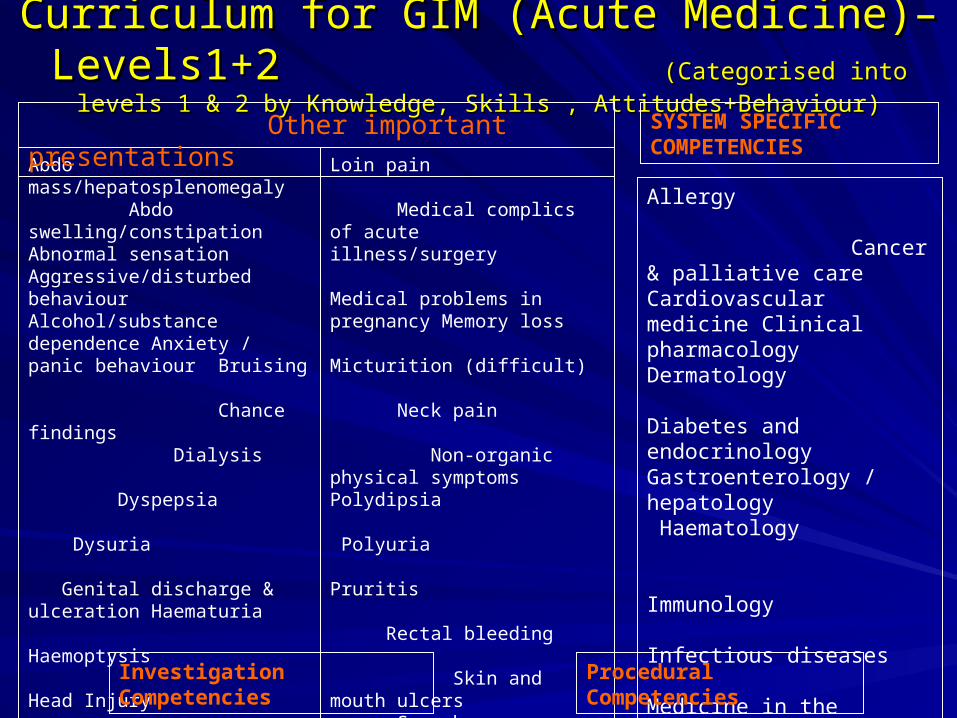
Curriculum for GIM (Acute Medicine)– Levels1+2 Curriculum for GIM (Acute Medicine)– Levels1+2 (Categorised into levels 1 & 2 by Knowledge, Skills , Attitudes+Behaviour)(Categorised into levels 1 & 2 by Knowledge, Skills , Attitudes+Behaviour)
Abdo mass/hepatosplenomegaly Abdo swelling/constipation Abnormal sensation Aggressive/disturbed behaviour Alcohol/substance dependence Anxiety / panic behaviour Bruising Chance findings Dialysis Dyspepsia Dysuria Genital discharge & ulceration Haematuria Haemoptysis Head Injury Hoarseness and stridor Hypothermia Immobility Involuntary movements Joint swelling Lymphadenopathy
Other important presentations SYSTEM SPECIFIC COMPETENCIES
Loin pain Medical complics of acute illness/surgery Medical problems in pregnancy Memory loss Micturition (difficult) Neck pain Non-organic physical symptoms Polydipsia Polyuria Pruritis Rectal bleeding Skin and mouth ulcers Speech disturbances Suicidal ideation Swallowing difficulties Syncope and presyncope Unsteadiness /balance problems Visual disturbance Weight loss
Allergy Cancer & palliative care Cardiovascular medicine Clinical pharmacology Dermatology Diabetes and endocrinology Gastroenterology / hepatology Haematology Immunology Infectious diseases Medicine in the Elderly Musculoskeletal system Neurology Psychiatry Public Health / H.Promotion Renal medicine Respiratory medicine
Investigation Competencies Procedural Competencies
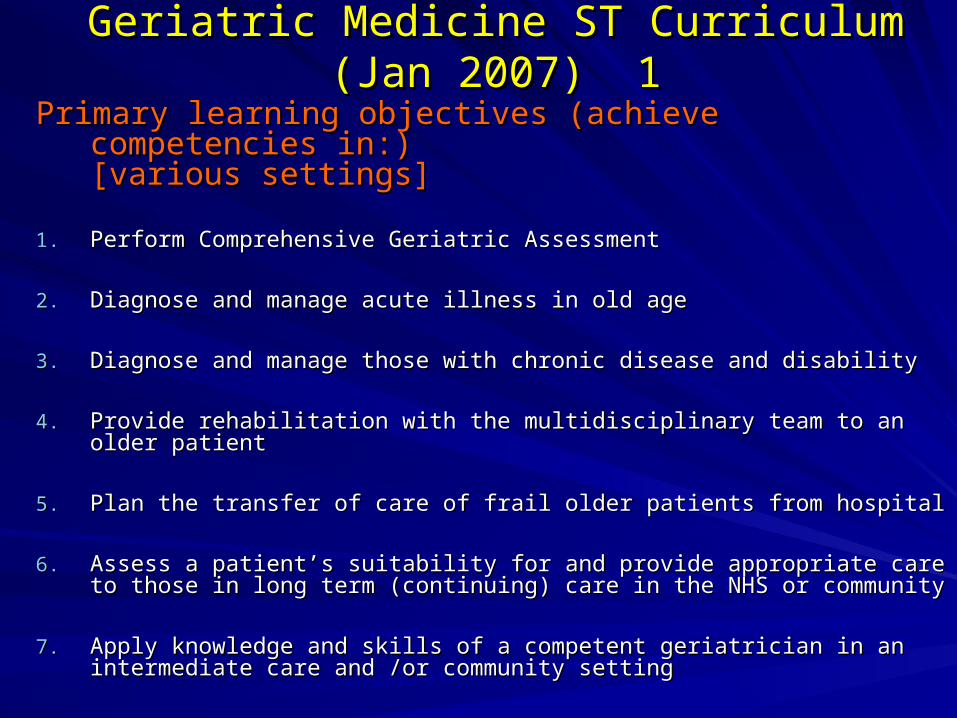
Geriatric Medicine ST Curriculum (Jan 2007) 1Geriatric Medicine ST Curriculum (Jan 2007) 1
Primary learning objectives (achieve competencies in:) Primary learning objectives (achieve competencies in:) [various [various settings]settings]
1.1. Perform Comprehensive Geriatric AssessmentPerform Comprehensive Geriatric Assessment
2.2. Diagnose and manage acute illness in old ageDiagnose and manage acute illness in old age
3.3. Diagnose and manage those with chronic disease and disabilityDiagnose and manage those with chronic disease and disability
4.4. Provide rehabilitation with the multidisciplinary team to an older patientProvide rehabilitation with the multidisciplinary team to an older patient
5.5. Plan the transfer of care of frail older patients from hospitalPlan the transfer of care of frail older patients from hospital
6.6. Assess a patient’s suitability for and provide appropriate care to those Assess a patient’s suitability for and provide appropriate care to those in long term (continuing) care in the NHS or communityin long term (continuing) care in the NHS or community
7.7. Apply knowledge and skills of a competent geriatrician in an Apply knowledge and skills of a competent geriatrician in an intermediate care and /or community settingintermediate care and /or community setting
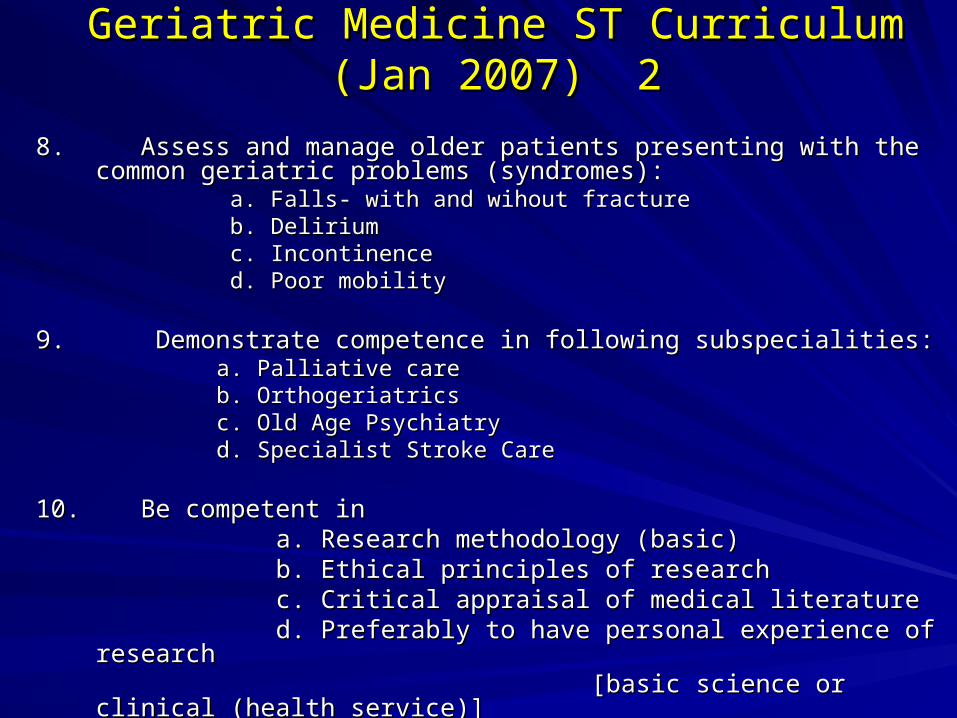
Geriatric Medicine ST Curriculum (Jan 2007) 2Geriatric Medicine ST Curriculum (Jan 2007) 2
8. Assess and manage older patients presenting with the common geriatric 8. Assess and manage older patients presenting with the common geriatric problems (syndromes):problems (syndromes):
a. Falls- with and wihout fracturea. Falls- with and wihout fracture b. Deliriumb. Delirium c. Incontinencec. Incontinence d. Poor mobilityd. Poor mobility
9. Demonstrate competence in following subspecialities:9. Demonstrate competence in following subspecialities: a. Palliative carea. Palliative care b. Orthogeriatricsb. Orthogeriatrics c. Old Age Psychiatryc. Old Age Psychiatry d. Specialist Stroke Cared. Specialist Stroke Care
10. Be competent in 10. Be competent in a. Research methodology (basic)a. Research methodology (basic) b. Ethical principles of researchb. Ethical principles of research c. Critical appraisal of medical literaturec. Critical appraisal of medical literature d. Preferably to have personal experience of researchd. Preferably to have personal experience of research [basic science or clinical (health service)][basic science or clinical (health service)]
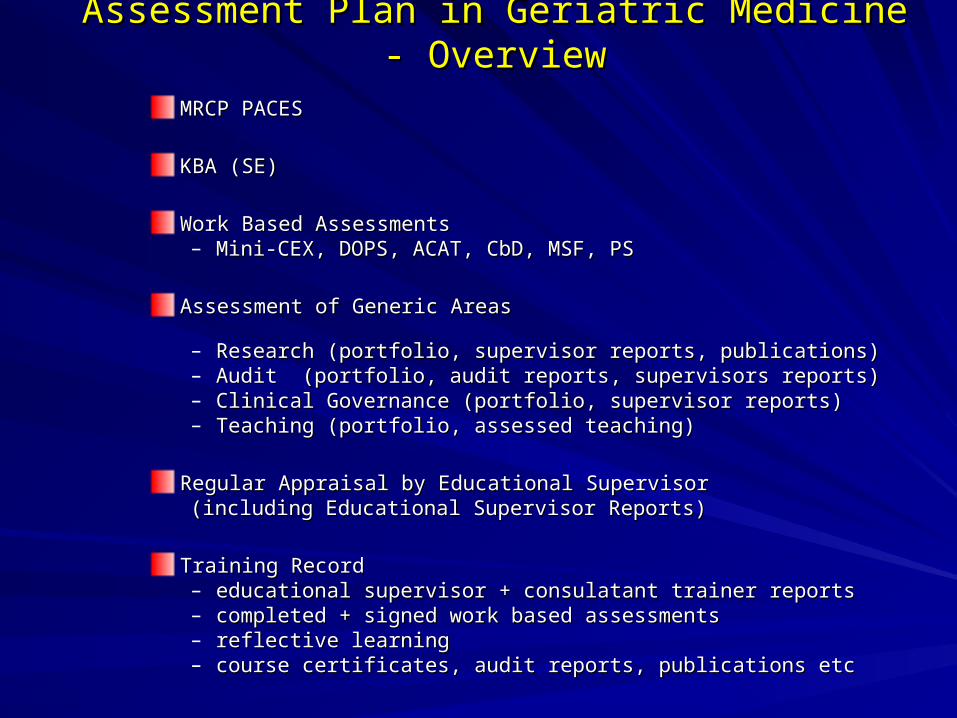
Assessment Plan in Geriatric Medicine - OverviewAssessment Plan in Geriatric Medicine - Overview
MRCP PACESMRCP PACES
KBA (SE)KBA (SE)
Work Based AssessmentsWork Based Assessments– Mini-CEX, DOPS, ACAT, CbD, MSF, PSMini-CEX, DOPS, ACAT, CbD, MSF, PS
Assessment of Generic Areas Assessment of Generic Areas – Research (portfolio, supervisor reports, publications)Research (portfolio, supervisor reports, publications)– Audit (portfolio, audit reports, supervisors reports)Audit (portfolio, audit reports, supervisors reports)– Clinical Governance (portfolio, supervisor reports)Clinical Governance (portfolio, supervisor reports)– Teaching (portfolio, assessed teaching) Teaching (portfolio, assessed teaching)
Regular Appraisal by Educational Supervisor Regular Appraisal by Educational Supervisor (including Educational Supervisor Reports)(including Educational Supervisor Reports)
Training RecordTraining Record– educational supervisor + consulatant trainer reportseducational supervisor + consulatant trainer reports– completed + signed work based assessmentscompleted + signed work based assessments– reflective learningreflective learning– course certificates, audit reports, publications etccourse certificates, audit reports, publications etc

Work Based Assessment MethodsWork Based Assessment Methods
Mini-Clinical Evaluation Exercise (mini-CEX)Mini-Clinical Evaluation Exercise (mini-CEX)
Direct Observation of Procedural Skills (DOPS)Direct Observation of Procedural Skills (DOPS)
Multi-Source Feedback (MSF)Multi-Source Feedback (MSF)
Case-Based Discussions (CbD)Case-Based Discussions (CbD)
Patient Survey (PS)Patient Survey (PS)
Acute Care Assessment Tool (ACAT)Acute Care Assessment Tool (ACAT)
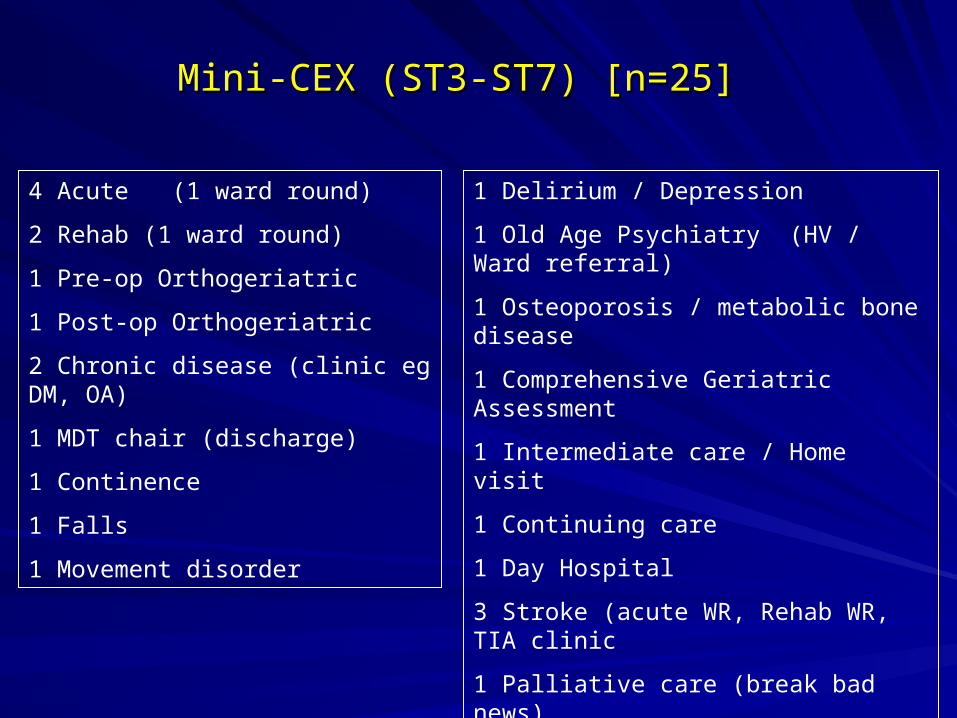
Mini-CEX (ST3-ST7) [n=25]Mini-CEX (ST3-ST7) [n=25]
4 Acute (1 ward round)
2 Rehab (1 ward round)
1 Pre-op Orthogeriatric
1 Post-op Orthogeriatric
2 Chronic disease (clinic eg DM, OA)
1 MDT chair (discharge)
1 Continence
1 Falls
1 Movement disorder
1 Delirium / Depression
1 Old Age Psychiatry (HV / Ward referral)
1 Osteoporosis / metabolic bone disease
1 Comprehensive Geriatric Assessment
1 Intermediate care / Home visit
1 Continuing care
1 Day Hospital
3 Stroke (acute WR, Rehab WR, TIA clinic
1 Palliative care (break bad news)
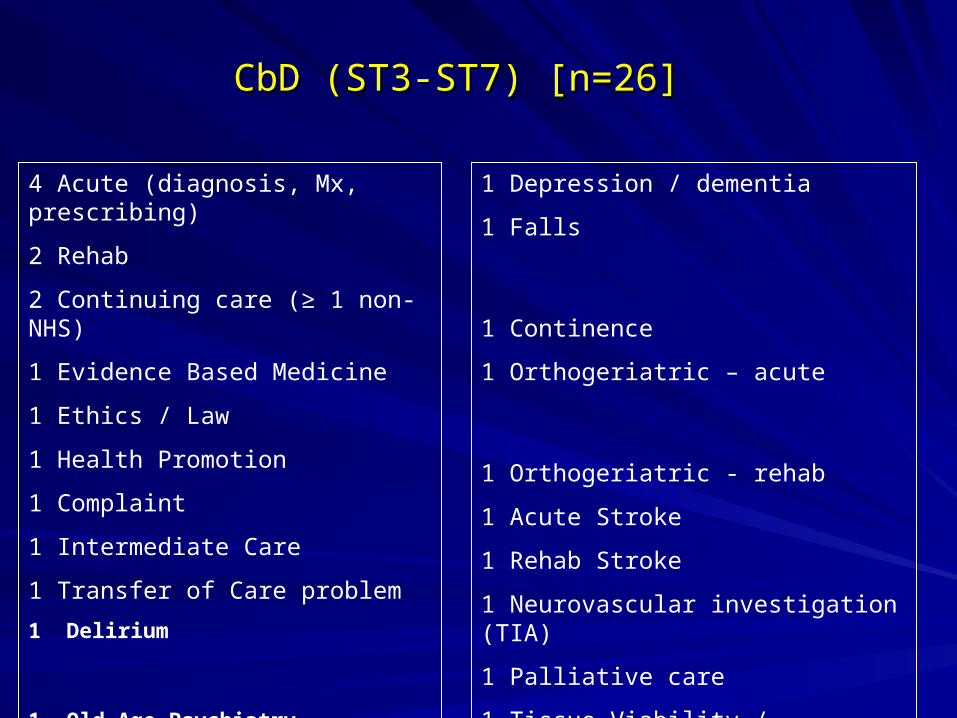
CbD (ST3-ST7) [n=26]CbD (ST3-ST7) [n=26]
4 Acute (diagnosis, Mx, prescribing)
2 Rehab
2 Continuing care (≥ 1 non-NHS)
1 Evidence Based Medicine
1 Ethics / Law
1 Health Promotion
1 Complaint
1 Intermediate Care
1 Transfer of Care problem
1 Delirium
1 Old Age Psychiatry
1 Depression / dementia
1 Falls
1 Continence
1 Orthogeriatric – acute
1 Orthogeriatric - rehab
1 Acute Stroke
1 Rehab Stroke
1 Neurovascular investigation (TIA)
1 Palliative care
1 Tissue Viability / Hypothermia

Mid-Trent Experience of MSF (360 degree appraisals for SPRS)
Overview of Earlier PilotOverview of Earlier Pilot
• Early pilot June-August 2004
• 18 SPRs in 6 NHS Trusts
• Then 13 SPRs (1 abroad, 1 maternity leave)
• 11 SPRs performed 360 degree appraisals
• Minimal guidance
• Experience discussed at RITAs Sept 2004 (subjective)
• Questionnaire sent to SPRs in Jan 2005 (objective)
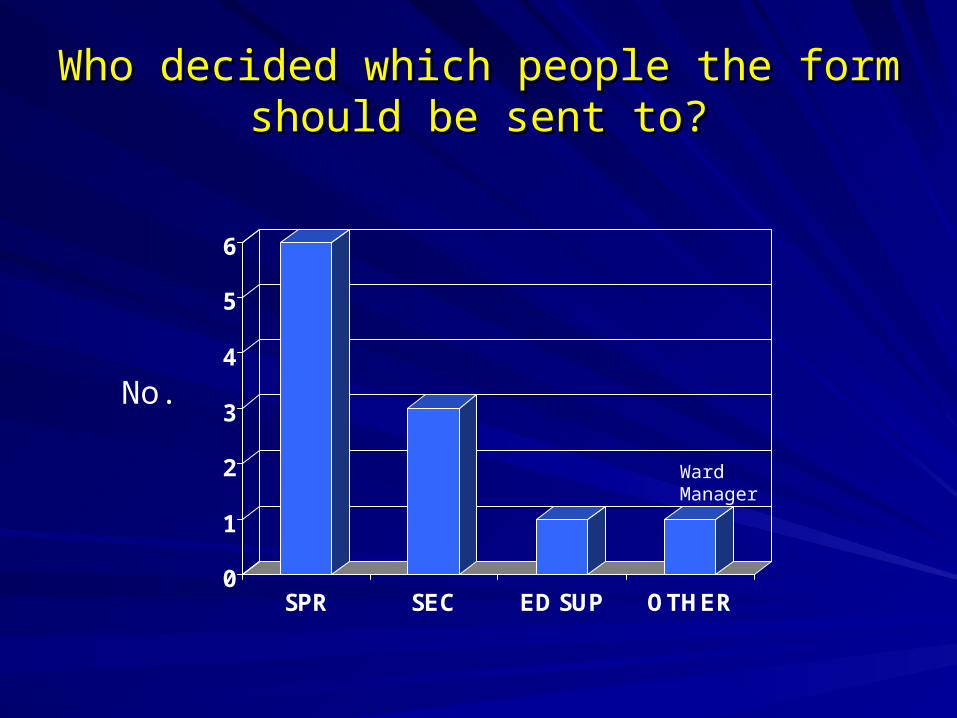
Who decided which people the form should Who decided which people the form should be sent to?be sent to?
0
1
2
3
4
5
6
SPR SEC ED SUP OTHER
No.
Ward Manager

Did you find the exercise useful?Did you find the exercise useful?
Yes- extremely usefulYes- extremely useful 11
Yes- quite usefulYes- quite useful 44
Not sureNot sure 33
No- not that usefulNo- not that useful 22
No- waste of timeNo- waste of time 11
Comments: Those who found process Comments: Those who found process usefuluseful
• Gave useful feedback on how I am performing on the ward
• I think it is a great way of assessing clinicians
• Getting positive feedback improved my confidence.
• The process informed the appraisal meeting with my
educational supervisor
Comments: Those who found process Comments: Those who found process notnot usefuluseful
• Other people should distribute the forms so the SPR does not know who has been asked to complete them (x2)
• Meetings with the educational supervisor more important than the 360 degree appraisal
Further analysisFurther analysis
• Of the 5 SPRs who found the process useful, for 3 of them “others” decided who to send the forms to.
• Of the 6 SPRS who who did not find the process useful or were not sure, all 6 SPRs chose the people to send the forms to

Conclusion of the Early pilotConclusion of the Early pilot
Main hypothesis generated:
The process is more useful if educational supervisor / consultant trainer decides to whom the questionnaires are sent to.
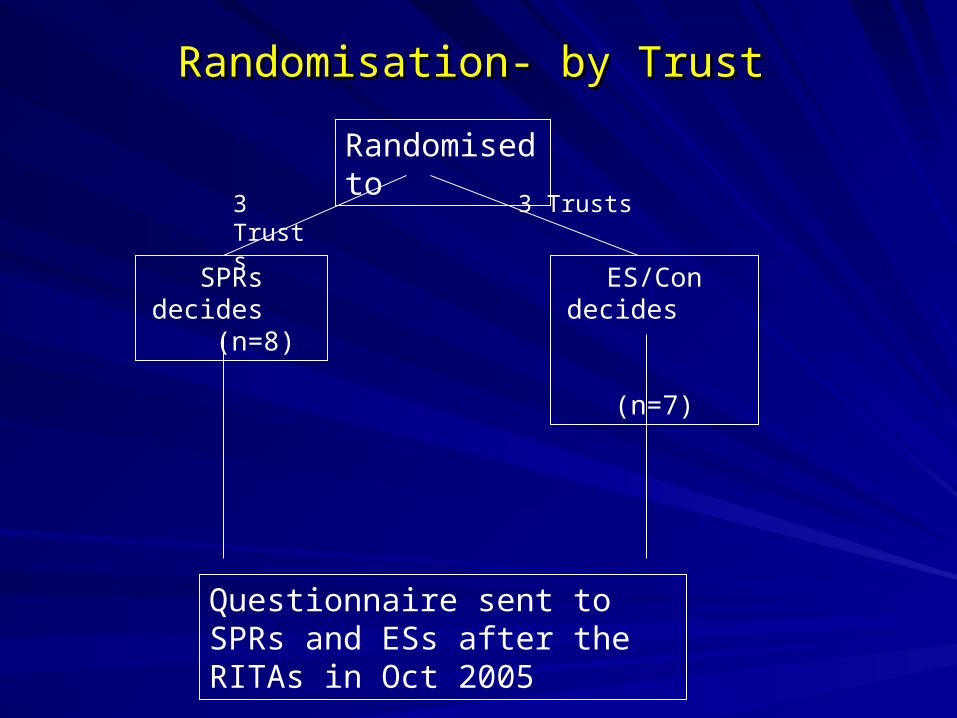
Randomisation- by TrustRandomisation- by Trust
Randomised to
SPRs decides (n=8)
ES/Con decides
(n=7)
3 Trusts 3 Trusts
Questionnaire sent to SPRs and ESs after the RITAs in Oct 2005
Mean no of Qs sent 17.8 (range 10-20)Mean no of Qs sent 17.8 (range 10-20)
Mean returns 15.1 (range 10-20)Mean returns 15.1 (range 10-20)
Mean response rate 85% (range 55%-Mean response rate 85% (range 55%-100%)100%)
No difference between the 2 groupsNo difference between the 2 groups
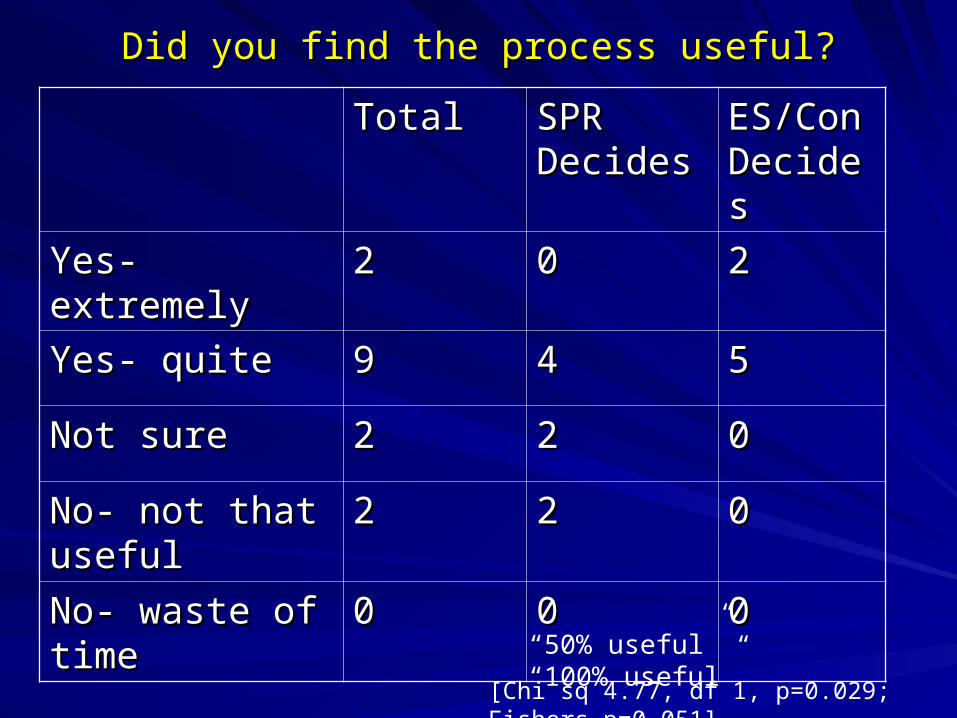
Did you find the process useful?Did you find the process useful?
TotalTotal SPR SPR DecidesDecides
ES/Con ES/Con DecidesDecides
Yes- extremelyYes- extremely 22 00 22
Yes- quiteYes- quite 99 44 55
Not sureNot sure 22 22 00
No- not that No- not that useful useful
22 22 00
No- waste of No- waste of timetime
00 00 00
“50% useful” “100% useful”
[Chi sq 4.77, df 1, p=0.029; Fishers p=0.051]

Mini-CEXMini-CEX
12 SPRs had performed at least 1 Mini-CEX12 SPRs had performed at least 1 Mini-CEX
9 found them useful, 3 not9 found them useful, 3 not
Egs - Ward round (x4); MDM (x2); Tilt (x1) Egs - Ward round (x4); MDM (x2); Tilt (x1) - Rest not stated - Rest not stated

DOPS + Patient Satisfaction QsDOPS + Patient Satisfaction Qs
4 SPRs had performed at least 1 DOPS4 SPRs had performed at least 1 DOPS
3 found them useful (Temp pacing, OGD, not stated)3 found them useful (Temp pacing, OGD, not stated)
1 not useful (LP)1 not useful (LP)
1 SPR performed a patient satisfaction Q- useful1 SPR performed a patient satisfaction Q- useful

Feedback from Educational supervisors Feedback from Educational supervisors (5 returns from 7) (5 returns from 7)
2 found the 360 degree process extremely 2 found the 360 degree process extremely usefuluseful
2 found it quite useful2 found it quite useful
1 not sure1 not sure
Feedback from Educational supervisorsFeedback from Educational supervisors
Was the process time-consuming?
No- 4
Yes–slightly 1
Yes – very 0

Assessment Plan For Speciality Training in Assessment Plan For Speciality Training in Geriatric Medicine Geriatric Medicine
MRCPMRCP KBEKBE(SE)(SE)
Mini-Mini-CEXCEX
CbDCbD MSFMSF ACATACAT PSPS ES+CTES+CTReportsReports
Audit / Audit / ResearchResearch
Teach Teach AssesAsses
CertCert
ST3ST3 ** 6 6 AcuteAcute
6 6 AcuteAcute
11 ** ALSALS
ST4ST4 66 66 ** 11 ** ** Acute Acute Audit Audit
ALS ALS Res. Res. Meth.Meth.
ST5ST5 ** 66 66 11 ** Audit Audit (eg rehab)(eg rehab)
** ALS ALS TeachTeach
ST6ST6 66 66 ** ** * * PYA PYA
Audit (eg IC) Audit (eg IC) Res. present.Res. present.
ALSALS
ST7ST7 11 22 11 ** PublicationPublication ALS ALS Manag.Manag.
TOTTOT 25 25 2626 22 44 22
Summative Formative

EducationalAppraisal
Annual Review of
Competence Progression
Outcome
Annual Planning
1. Learning agreement:aims & intended learning outcomesbased on specialty curriculum2. Advice on portfolio3. Regular feedback (2 way)4. Personal Development Plan5. Trainer’s structured report
6. Workplace based (NHS) appraisal
Educational supervisor and/or TPD meet with trainee toreview competence outcome with trainee plan next part of training
Based on a paper from PMETB’s Workplace Assessment Group (2005)
Workplace based (NHS)
appraisal
ARCPA. Evidence1 Assessment of performance e.g.workplace based assessments and observational methods E.g. mini-CEX, DOPS, video, CBDexaminationsstructured report
2. Assessment of experience, e.g.portfolio/log bookauditresearchcritical incidents
B. Annual Competence Review Appropriately constituted panel considers evidence Outcome of review
Role of the ARCP
ChallengesChallenges
Overlap between SpRs and StRsOverlap between SpRs and StRs
StRs – proactiveStRs – proactive
Educational supervisors – proactiveEducational supervisors – proactive
Consultant Trainers – proactiveConsultant Trainers – proactive
New documentation – structuredNew documentation – structured
Time in Job plansTime in Job plans
Useful process or tick-box exercise?Useful process or tick-box exercise?
Some Suggestions
• StRs and CTs to have forms for CbDs, Mini-CEX
handy
• 2 CbDs and 2 Mini-CEX per 4 month attachment
• 3 CbDs and 3 Mini-CEX per 6 month attachment
• Importance of Meeting with Education Supervisor
about 1 month before ARCP
• Regular half day / full day teaching sessions
mapped to curricula
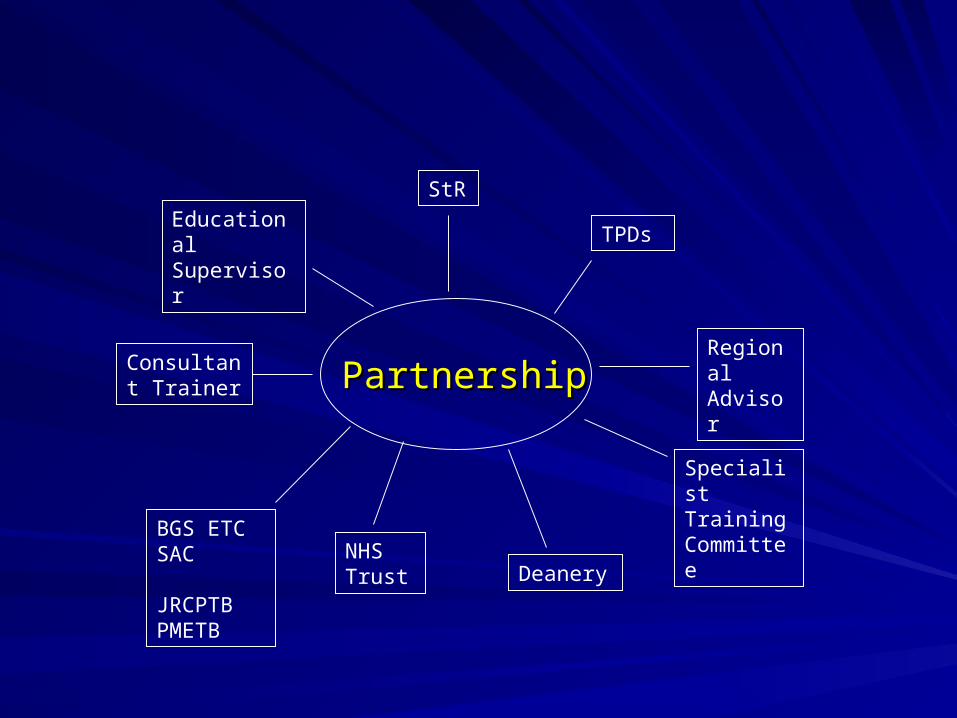
PartnershipPartnership
StR
Educational Supervisor TPDs
Consultant Trainer
Specialist Training Committee
Deanery
BGS ETC SAC JRCPTB PMETB
NHS Trust
Regional Advisor

Assessments! Assessments!More Work Based Assessments