impact of a pilot walking school bus intervention on children's pedestrian safety behaviors: a...
TRANSCRIPT

Health & Place 18 (2012) 24–30
Contents lists available at SciVerse ScienceDirect
Health & Place
1353-82
doi:10.1
n Corr
1100 Ba
fax: þ1
E-m1 Pr
Prevent
Tucker
journal homepage: www.elsevier.com/locate/healthplace
Impact of a pilot walking school bus intervention on children’s pedestriansafety behaviors: A pilot study
Jason A. Mendoza a,b,c,n, Kathy Watson a,1, Tzu-An Chen a, Tom Baranowski a,c, Theresa A. Nicklas a,c,Doris K. Uscanga a, Marcus J. Hanfling b,d
a USDA/ARS Children’s Nutrition Research Center, 1100 Bates St, Houston, TX 77030-2600, USAb Academic General Pediatrics, 6701 Fannin St, Suite 1540, Houston, TX 77030, USAc Dan L Duncan Cancer Center, Baylor College of Medicine, One Baylor Plaza, Suite 45A, Houston TX 77030, USAd Ben Taub General Hospital, 1504 Taub Loop, Houston TX 77030, USA
a r t i c l e i n f o
Keywords:
Walking school bus
Safe routes to school
Injury prevention
Active commuting to school
Pedestrian safety
Neighborhood safety
92/$ - see front matter & 2011 Elsevier Ltd. A
016/j.healthplace.2011.07.004
esponding author at: USDA/ARS Children’s
tes St, Houston, TX 77030-2600, USA. Tel.: þ
713 798 7098.
ail address: [email protected] (J.A. Me
esent address: Division of Nutrition, Phy
ion of the Centers for Disease Control and
Rd, Atlanta, GA 30341, USA.
a b s t r a c t
Walking school buses (WSB) increased children’s physical activity, but impact on pedestrian safety
behaviors (PSB) is unknown. We tested the feasibility of a protocol evaluating changes to PSB during a
WSB program. Outcomes were school-level street crossing PSB prior to (Time 1) and during weeks 4–5
(Time 2) of the WSB. The protocol collected 1252 observations at Time 1 and 2548 at Time 2. Mixed
model analyses yielded: intervention schoolchildren had 5-fold higher odds (po0.01) of crossing at the
corner/crosswalk but 5-fold lower odds (po0.01) of stopping at the curb. The protocol appears feasible
for documenting changes to school-level PSB.
& 2011 Elsevier Ltd. All rights reserved.
1. Introduction
Encouraging physical activity among youth is important foraddressing the rising rates of childhood obesity worldwide (Wangand Lobstein, 2006; World Health Organization, 2010). Reports onchildren’s active commuting to school (walking or cycling toschool, henceforth termed active commuting) to improvechildren’s physical activity appear promising. Epidemiological studiesfrom multiple countries have reported positive associationsbetween children’s active commuting and total daily physicalactivity including from England (Cooper et al., 2003), Scotland(Alexander et al., 2005), Australia (Spinks et al., 2006), Germany(Landsberg et al., 2007), Canada (Loucaides et al., 2007), and theUnited States (Mendoza et al., 2011; Saksvig et al., 2007; Sirardet al., 2005). Active commuting is the main behavior of interest forthe Safe Routes to School (SRTS) Program, which originated inDenmark (Brown et al., 2007), and in the US promotes walking andbicycling to school safely by primary and middle school studentsthrough improvements to schools’ walking environments andpromotional activities (Brown et al., 2007).
ll rights reserved.
Nutrition Research Center,
1 713 798 7055;
ndoza).
sical Activity, and Obesity
Prevention, 3005 Chamblee
The ‘‘walking school bus’’ (WSB) program is an integral part ofSRTS programs (National Center for Safe Routes to School, 2006).A WSB is a group of children that walks to and from school withparents or other adults, in which the children are picked upthroughout the neighborhood. WSB programs have the potentialto improve children’s pedestrian safety behaviors through twomain mechanisms: (1) walking with an adult decreases children’spedestrian risk by almost 70% (Roberts, 1995) and (2) adultleaders can teach and model safe street crossing behaviors onthe way to and from school. Children’s pedestrian safety isimportant to promoting active commuting, since it influencesparents’ decisions on their children’s active commuting (Dellingerand Staunton, 2002; Martin and Carlson, 2005). Moreover, pedes-trian injuries are an important contributor of pediatric uninten-tional injuries, which are the leading cause of mortality amongchildren aged 1–19 years (National Center for Injury Preventionand Control, 2010). Improving children’s pedestrian safety beha-viors could be an additional important benefit of WSBs, besidesincreasing children’s active commuting and physical activity.A previous systematic review of randomized controlled trials(RCTs) on pedestrian safety programs concluded that theseeducation programs, some that directly targeted children andothers that targeted parents, have shown promise for increasingknowledge and pedestrian behaviors (Duperrex et al., 2009).While preliminary evaluations of WSB and similar walk to schoolprograms in Scotland (McKee et al., 2007) and the US (Heelanet al., 2009; Mendoza et al., 2009; Sirard et al., 2008; Stauntonet al., 2003) have reported improving rates of children’s active

J.A. Mendoza et al. / Health & Place 18 (2012) 24–30 25
commuting, WSB studies evaluating pedestrian safety behaviorsare lacking. As recommended for pilot studies, in which the maingoal is to test feasibility of a research protocol (Arain et al., 2010;Kraemer et al., 2006; Leon et al., 2011), the goal of this pilot studywas to evaluate the feasibility of a protocol to measure changes tochildren’s pedestrian safety behaviors at the school-level asso-ciated with a WSB program. A secondary goal was to evaluate thepotential influence of the WSB program, neighborhood safety, andintersection characteristics on children’s pedestrian safety beha-viors at the school-level.
2. Methods
2.1. Design
This pilot study on children’s pedestrian safety behaviors wasconducted as part of a cluster RCT of a WSB program amonglow-income 4th grade elementary schoolchildren, in which sig-nificant increases in children’s active commuting and moderate-to-vigorous physical activity were reported elsewhere (Mendozaet al., 2011). A full description of methods for that study includingthe related CONSORT flow diagram have been reported in detail(Mendoza et al., 2011; Mendoza et al., 2010b). Briefly, 4th gradechildren were enrolled (26.1% of all 4th graders) and baselineoutcomes were assessed prior to random assignment of schools toa study condition. All enrolled 4th grade children agreed toparticipate in the WSB program if their school was randomlyassigned to the intervention condition. During the 4–5 weekintervention period, the intervention children made 20.9713.4trips by active commuting (Mendoza et al., 2011). For the presentstudy, children’s pedestrian safety behaviors assessed at majorschool intersections were the primary outcome of interest andanonymously measured among all child pedestrians (regardless ofgrade-level) approaching study schools as described below. Schoolswere matched by race/ethnicity and socioeconomic status (percentof children who qualified for the US federal free/reduced pricelunch program) and then randomly assigned within school pairs tointervention (n¼4) or control (n¼4) conditions. Time 1 measure-ments occurred prior to both random assignment and implemen-tation of the intervention in March 2009. Time 2 measurementsoccurred during weeks 4–5 of the intervention. Participants andresearch staff at Time 2 were not blinded to the assignment ofschools to the intervention, since it was a behavioral program. Thisstudy received approval through the Institutional Review Board ofBaylor College of Medicine and the Department of Research andAccountability of the Houston Independent School District. Thisstudy was registered on clinicaltrials.gov and the identifier numberis NCT00758615.
2.2. Setting
The setting was elementary schools from the Houston Indepen-dent School District (HISD) located in Houston, TX, which is the 4thlargest city in the US (Planning and Development Department,2003). Schools were recruited from HISD based on having 475% ofchildren qualified for the free/reduced lunch program (a proxy forschool socioeconomic status), responding to a district-wide letterdescribing the study, and informal observations on the schools’walking environments, i.e. street connectivity, road traffic/presenceof arterial roads, and sidewalk conditions.
2.3. Intervention
The walking school bus program at each intervention schoolwas based on publicly available guidelines issued by the US
National Center for Safe Routes to School (National Center forSafe Routes to School, 2006). Intervention schools had one tothree WSB routes organized around children’s home residences.Study staff walked the 4th grade participants to and from schoolup to five days per week, although the children and parentsdecided when the children participated. Study staff underwent a4-h classroom and field-based training on the WSB and pedes-trian safety led by the study investigators. Staff members wereexpected to model, teach, and be evaluated on teaching thefollowing pedestrian safety behaviors during the walk to andfrom school: (1) crossed at a corner or crosswalk, (2) crossed withan adult or safety patrol, (3) stopped at the curb, (4) looked left-right-left, and (5) walked and did not run across the street. Thesebehaviors were selected from previous child pedestrian injuryprevention studies (Rivara et al., 1991; Rosenbloom et al., 2008;Zeedyk and Kelly, 2003; Zeedyk et al., 2002) and were theorizedto be related to pedestrian injuries, although direct links have notbeen established. Children were postulated to learn the pedes-trian safety behaviors through observational learning (Bandura,1976), i.e. by observing staff members properly crossing a street,and by direct teaching and reinforcement of those behaviors bythe staff to the children. Direct teaching and reinforcementoccurred by having the children take turns co-leading the walkinggroups and helping the adult staff to decide when to cross thestreet safely. Siblings who attended the same school as the 4thgrade WSB participants were allowed to walk with the WSBs as apractical measure. Parents were encouraged but not required towalk with the WSBs. Study staff and WSB children wore brightfluorescent safety vests during the intervention period. WSBroutes had approximately 8–12 children for every two staffmembers and averaged 0.8 miles in total length. No interventionwas conducted at the control schools, which only received theusual information provided by HISD on school transportationoptions. The intervention and control conditions were launchedsimultaneously in March 2009, after Time 1 assessments, andcontinued for five weeks.
2.4. Outcome variables
Crossing a street is one of the most vulnerable acts for childpedestrians (Hotz et al., 2009), and children’s pedestrian safetybehaviors related to crossing a street were measured by trainedresearch assistants using a previously validated observationalinstrument (Mendoza et al., 2010a). Children of all grade levelswere unobtrusively observed at major intersections at eachschool for completion (yes/no) of five street crossing behaviorslisted in the Intervention subsection above. Each of the five streetcrossing behaviors (yes¼1; no¼0) and a composite score (thesum from 0 to 5 of the five behaviors) were determined for eachschool. Among low-income elementary schoolchildren in HISD,this instrument had acceptable sensitivity (85%), specificity (83%),high percent agreement (91%), and moderate reliability (for thecomposite score, r¼0.55, po0.01) comparing trained researchassistants with an expert observer (Mendoza et al., 2010a). Thepedestrian safety behaviors were observed during Time 1 (beforethe intervention) and Time 2 (during weeks 4 and 5 of theintervention) before the start of the school day. Research assis-tants were instructed not to interact with the child pedestrians,which precluded the collection of individual-level sociodemo-graphic data including names. Therefore the pedestrian safetydata reflect child pedestrians of any grade level (kindergar-ten—5th grade) approaching the study schools; i.e. these wereschool-level, cross-sectional observations, and were not limited to4th grade children enrolled in the WSB study.

Table 1School demographics by intervention and control conditionsa.
Enrollment Hispanic
(%)
African-
American (%)
Free/reduced
price lunch (%)
Academic
rating
Intervention schools
A 701 78 13 84 Exemplary
B 935 94 4 95 Recognized
C 471 8 92 94 Recognized
D 580 43 50 84 Exemplary
Control schools
A 490 92 8 93 Exemplary
B 506 93 5 97 Exemplary
C 492 7 92 95 Recognized
D 521 59 41 98 Exemplary
a Provided by the Houston Independent School District (HISD) for the 2008–
2009 school year. Academic ratings were based on the Texas Education Agency
Accountability System, which rated schools according to four categories (Exemp-
lary, Recognized, Acceptable, and Unacceptable) based on school-wide perfor-
mance on standardized test scores, rates of completing grades, and dropouts.
Paired schools share the same letter in lieu of their actual names, as requested by
HISD.
J.A. Mendoza et al. / Health & Place 18 (2012) 24–3026
2.5. Covariates
At each of the major intersections where research assistantsscored the child pedestrians’ street crossing behaviors, researchassistants also noted the number of lanes of traffic, defined aslanes that pedestrians may cross and where motor vehicles eithercontinue through the intersection or turn left or right. A weightedaverage of the number of lanes of traffic for each school was usedin analyses, based on the numbers of children observed at thatintersection. As an exploratory hypothesis, we believed thattraffic lanes would be inversely associated with pedestrian safetybehaviors. We based this hypothesis on the postulation that withgreater traffic lanes, the complexity of crossing the street wouldincrease and thereby result in greater opportunities for error.
Parents of the 4th grade children enrolled in the WSB study atthe intervention and control schools completed questions on theirperceptions of neighborhood safety using the Disorder subscale ofthe Neighborhood Environment for Children Rating Scales at Time1. This subscale was composed of items on which parents ratedthe family’s neighborhood for safety, violence, drug traffic, andchild victimization (Coulton et al., 1996). Among previous urbansamples, the subscale had acceptable internal consistency (Cron-bach’s alpha¼0.95), reliability (generalizability coefficient¼0.84),and discriminated between high and low risk neighborhoods(po0.01) with regard to child maltreatment rates (Coultonet al., 1996). The subscale was reported to be inversely relatedto children’s television viewing in a large national US study(Burdette and Whitaker, 2005). The parents’ scores for thissubscale were combined and averaged for each school to producea school-level rating. As an exploratory hypothesis, we believedthat neighborhood disorder would be inversely associated withpedestrian safety behaviors.
2.6. Statistical analysis
Frequencies and percentages were used to describe schoolcharacteristics and the prevalence of the pedestrian safety beha-viors. To assess the feasibility of the protocol for measuringchanges to children’s pedestrian safety associated with the WSBprogram, we expected to conduct pedestrian safety observationson at least ½ of all active commuters at the study schools, i.e. 17%of weekly trips (Mendoza et al., 2011). Therefore, the protocol wasconsidered feasible if we collected observational data on at least798 children/week crossing a major school intersection each atTime 1 and Time 2. For the unadjusted bivariate analyses betweenchildren’s pedestrian safety behaviors and the average number oftraffic lanes for the intersections or parents’ perceptions ofneighborhood safety, we used: (1) the point-biserial correlationfor the relationship between binary (the individual item scores forthe pedestrian safety behaviors) and interval variables (trafficlanes or neighborhood safety) and (2) the Pearson correlation todetermine the relationship between interval variables (the com-posite pedestrian safety behaviors score, traffic lanes, and neigh-borhood safety). To compare intervention versus control schoolsfor each of the children’s pedestrian safety behaviors and thecomposite pedestrian safety scores, we used generalized mixedmodel analyses and mixed model analyses, respectively. Becausechildren in the same school shared similar characteristics, theoutcomes of interest could be influenced by the schools them-selves. Therefore, children (level one) were considered nestedwithin schools (level two). In addition, since the data wascollected on different groups of children at each assessmentpoint, we cannot match Time 1 and Time 2 data at the child-level. Hence, time was treated as a between groups factor. Forthese models, school was a random and time was a fixed effect.The average number of traffic lanes for the intersections observed
and parents’ perception of neighborhood safety were school-levelcovariates.
3. Results
The eight study schools were selected from a total of 15 HISDelementary schools that expressed initial interest in the studyafter a district-wide solicitation announcement. Schools wereexcluded based on the following criteria: inability to accommo-date the study and measurements (n¼3) or poor walking envir-onments, e.g. no sidewalks, low street connectivity, and majorarterial roads/highways adjacent to the school (n¼4). All eightschools completed the study. School-level characteristics pro-vided by the district are reported in Table 1 (InformationServices, 2009).
As the main indication of the feasibility of the protocol tocollect data on children’s pedestrian safety behaviors, we success-fully recorded 1252 observations at Time 1 and 2548 observationsat Time 2. Both were well above the threshold of 798 observationsthat was based on observing at least ½ of all child pedestrians’weekly trips at Time 1.
In unadjusted analyses at Time 1, there were no differences inthe prevalence of the pedestrian safety behaviors at the interven-tion compared to the control schools (all p40.05). Also at Time 1,the number of traffic lanes at each intersection was negativelyassociated with the composite score of children’s pedestriansafety behaviors (r¼�0.14, po0.01, Table 2). Examining thebehaviors individually, with increasing traffic lanes, fewer chil-dren stopped at the curb (r¼�0.26, po0.01). The number oftraffic lanes was not significantly associated with any of the otherpedestrian safety behaviors (all p40.05).
In unadjusted analyses at Time 1, parents’ perceptions ofneighborhood safety, measured by the Disorder subscale, wasnot related to the composite score of children’s pedestrian safetybehaviors (Table 2, p40.05). Examining the pedestrian safetybehaviors individually, with greater neighborhood disorder, morechildren crossed at a corner or crosswalk (r¼0.08, po0.01), morecrossed with an adult or safety patrol (r¼0.08. po0.01), andfewer children stopped at the curb (r¼�0.09, po0.01).
The intracluster correlation coefficients for the pedestriansafety behaviors ranged from 0.02 to 0.53 (Table 3), which reflectswide variability in the clustering of the behaviors within schools.The generalized mixed model analyses yielded significant group
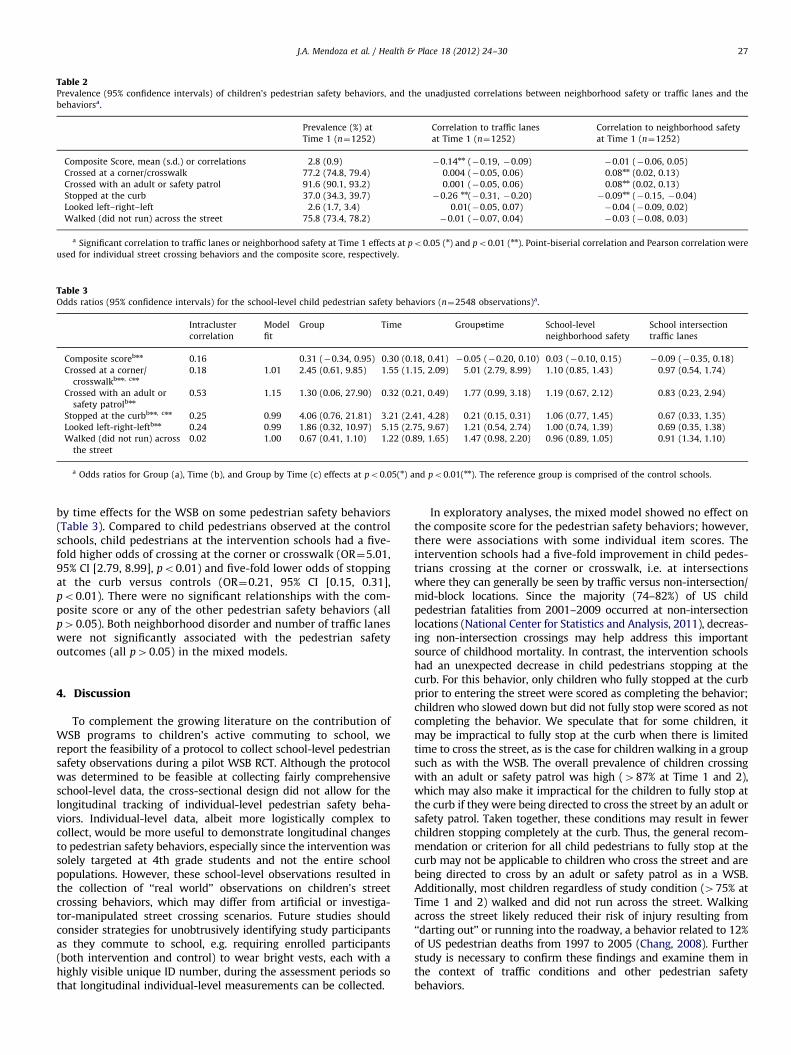
Table 2Prevalence (95% confidence intervals) of children’s pedestrian safety behaviors, and the unadjusted correlations between neighborhood safety or traffic lanes and the
behaviorsa.
Prevalence (%) at
Time 1 (n¼1252)
Correlation to traffic lanes
at Time 1 (n¼1252)
Correlation to neighborhood safety
at Time 1 (n¼1252)
Composite Score, mean (s.d.) or correlations 2.8 (0.9) �0.14nn (�0.19, �0.09) �0.01 (�0.06, 0.05)
Crossed at a corner/crosswalk 77.2 (74.8, 79.4) 0.004 (�0.05, 0.06) 0.08nn (0.02, 0.13)
Crossed with an adult or safety patrol 91.6 (90.1, 93.2) 0.001 (�0.05, 0.06) 0.08nn (0.02, 0.13)
Stopped at the curb 37.0 (34.3, 39.7) �0.26 nn(�0.31, �0.20) �0.09nn (�0.15, �0.04)
Looked left–right–left 2.6 (1.7, 3.4) 0.01(�0.05, 0.07) �0.04 (�0.09, 0.02)
Walked (did not run) across the street 75.8 (73.4, 78.2) �0.01 (�0.07, 0.04) �0.03 (�0.08, 0.03)
a Significant correlation to traffic lanes or neighborhood safety at Time 1 effects at po0.05 (n) and po0.01 (nn). Point-biserial correlation and Pearson correlation were
used for individual street crossing behaviors and the composite score, respectively.
Table 3Odds ratios (95% confidence intervals) for the school-level child pedestrian safety behaviors (n¼2548 observations)a.
Intracluster
correlation
Model
fit
Group Time Groupntime School-level
neighborhood safety
School intersection
traffic lanes
Composite scorebnn 0.16 0.31 (�0.34, 0.95) 0.30 (0.18, 0.41) �0.05 (�0.20, 0.10) 0.03 (�0.10, 0.15) �0.09 (�0.35, 0.18)
Crossed at a corner/
crosswalkbnn, cnn
0.18 1.01 2.45 (0.61, 9.85) 1.55 (1.15, 2.09) 5.01 (2.79, 8.99) 1.10 (0.85, 1.43) 0.97 (0.54, 1.74)
Crossed with an adult or
safety patrolbnn
0.53 1.15 1.30 (0.06, 27.90) 0.32 (0.21, 0.49) 1.77 (0.99, 3.18) 1.19 (0.67, 2.12) 0.83 (0.23, 2.94)
Stopped at the curbbnn, cnn 0.25 0.99 4.06 (0.76, 21.81) 3.21 (2.41, 4.28) 0.21 (0.15, 0.31) 1.06 (0.77, 1.45) 0.67 (0.33, 1.35)
Looked left-right-leftbnn 0.24 0.99 1.86 (0.32, 10.97) 5.15 (2.75, 9.67) 1.21 (0.54, 2.74) 1.00 (0.74, 1.39) 0.69 (0.35, 1.38)
Walked (did not run) across
the street
0.02 1.00 0.67 (0.41, 1.10) 1.22 (0.89, 1.65) 1.47 (0.98, 2.20) 0.96 (0.89, 1.05) 0.91 (1.34, 1.10)
a Odds ratios for Group (a), Time (b), and Group by Time (c) effects at po0.05(n) and po0.01(nn). The reference group is comprised of the control schools.
J.A. Mendoza et al. / Health & Place 18 (2012) 24–30 27
by time effects for the WSB on some pedestrian safety behaviors(Table 3). Compared to child pedestrians observed at the controlschools, child pedestrians at the intervention schools had a five-fold higher odds of crossing at the corner or crosswalk (OR¼5.01,95% CI [2.79, 8.99], po0.01) and five-fold lower odds of stoppingat the curb versus controls (OR¼0.21, 95% CI [0.15, 0.31],po0.01). There were no significant relationships with the com-posite score or any of the other pedestrian safety behaviors (allp40.05). Both neighborhood disorder and number of traffic laneswere not significantly associated with the pedestrian safetyoutcomes (all p40.05) in the mixed models.
4. Discussion
To complement the growing literature on the contribution ofWSB programs to children’s active commuting to school, wereport the feasibility of a protocol to collect school-level pedestriansafety observations during a pilot WSB RCT. Although the protocolwas determined to be feasible at collecting fairly comprehensiveschool-level data, the cross-sectional design did not allow for thelongitudinal tracking of individual-level pedestrian safety beha-viors. Individual-level data, albeit more logistically complex tocollect, would be more useful to demonstrate longitudinal changesto pedestrian safety behaviors, especially since the intervention wassolely targeted at 4th grade students and not the entire schoolpopulations. However, these school-level observations resulted inthe collection of ‘‘real world’’ observations on children’s streetcrossing behaviors, which may differ from artificial or investiga-tor-manipulated street crossing scenarios. Future studies shouldconsider strategies for unobtrusively identifying study participantsas they commute to school, e.g. requiring enrolled participants(both intervention and control) to wear bright vests, each with ahighly visible unique ID number, during the assessment periods sothat longitudinal individual-level measurements can be collected.
In exploratory analyses, the mixed model showed no effect onthe composite score for the pedestrian safety behaviors; however,there were associations with some individual item scores. Theintervention schools had a five-fold improvement in child pedes-trians crossing at the corner or crosswalk, i.e. at intersectionswhere they can generally be seen by traffic versus non-intersection/mid-block locations. Since the majority (74–82%) of US childpedestrian fatalities from 2001–2009 occurred at non-intersectionlocations (National Center for Statistics and Analysis, 2011), decreas-ing non-intersection crossings may help address this importantsource of childhood mortality. In contrast, the intervention schoolshad an unexpected decrease in child pedestrians stopping at thecurb. For this behavior, only children who fully stopped at the curbprior to entering the street were scored as completing the behavior;children who slowed down but did not fully stop were scored as notcompleting the behavior. We speculate that for some children, itmay be impractical to fully stop at the curb when there is limitedtime to cross the street, as is the case for children walking in a groupsuch as with the WSB. The overall prevalence of children crossingwith an adult or safety patrol was high (487% at Time 1 and 2),which may also make it impractical for the children to fully stop atthe curb if they were being directed to cross the street by an adult orsafety patrol. Taken together, these conditions may result in fewerchildren stopping completely at the curb. Thus, the general recom-mendation or criterion for all child pedestrians to fully stop at thecurb may not be applicable to children who cross the street and arebeing directed to cross by an adult or safety patrol as in a WSB.Additionally, most children regardless of study condition (475% atTime 1 and 2) walked and did not run across the street. Walkingacross the street likely reduced their risk of injury resulting from‘‘darting out’’ or running into the roadway, a behavior related to 12%of US pedestrian deaths from 1997 to 2005 (Chang, 2008). Furtherstudy is necessary to confirm these findings and examine them inthe context of traffic conditions and other pedestrian safetybehaviors.

J.A. Mendoza et al. / Health & Place 18 (2012) 24–3028
These exploratory short-term results are consistent withseveral previous randomized controlled trials of child pedestriansafety programs that reported modest or mixed results from asystematic review updated in 2009 (Duperrex et al., 2009).Present results also build upon other child pedestrian safetystudies, many of which had larger effects, but were not rando-mized controlled trials (Barton et al., 2007; Demetre and Lee,1992; Glang et al., 2005; Gresham et al., 2001; Hotz et al., 2004;Preusser and Lund, 1988; Rivara et al., 1991; Rothengatter, 1984;Young and Lee, 1987) or relied on children’s self-reports of theirpedestrian safety rather than on observations of the behaviors(Berry and Romo, 2006; Gresham et al., 2001; Morrongiello andKiriakou, 2006).
While most parents agree that children should be taughtpedestrian safety skills, few parents actually teach those skillsto their children while crossing the street (Morrongiello andBarton, 2009; Zeedyk and Kelly, 2003). The WSB provides anopportunity for parents and other adults to repeatedly teach andmodel pedestrian safety to children on the walk to and fromschool. There are several safety-related advantages to the WSBprogram in addition to promoting active commuting to school:(1) pedestrian safety education occurs during the children’scommute to school, which provides for practical, frequent, realworld lessons; (2) the intervention specifically targets childrenwho walk to and from school and who are thereby at risk forpedestrian injuries, and (3) the intervention takes place beforeand after school and does not interfere with classroom time. Themain disadvantages are related to (1) program implementation,which can be logistically difficult among low-income families orlow-resource schools; (2) program availability, which can belimited since only a proportion of children regularly participatedin WSB programs (Mendoza et al., 2009); however, the WSBprogram could be used with other promising pedestrian safetyprograms to improve child pedestrian safety, such as computer-based or virtual reality programs that potentially have wide reach(McComas et al., 2002; Schwebel and McClure, 2010; Thomsonet al., 2005; Tolmie et al., 2005); and (3) the potential for childrento become reliant on adults to safely cross the street. This relianceon adults may be mitigated by allowing children to co-lead thewalking groups and encouraging older children to independentlywalk to school when developmentally appropriate, i.e. olderchildren ‘‘graduate’’ from the WSB program.
In unadjusted analyses, the number of traffic lanes at schoolintersections was negatively associated with the composite score ofchildren’s pedestrian safety behaviors. This relationship was entirelydriven by the negative association between traffic lanes and childrenstopping at the curb: with more traffic lanes, fewer children fullystopped at the curb before crossing the street, perhaps due to thegreater distance involved in crossing the street, greater traffic volumeassociated with larger streets, and the constraint of crossing a largerdistance during a time-limited opportunity. Similarly, in unadjustedanalyses, parents’ perceptions of neighborhood safety were signifi-cantly but weakly correlated with children’s pedestrian safetybehaviors: with greater neighborhood disorder, children wereslightly more likely to cross at a corner or crosswalk and cross withan adult or safety patrol, but slightly less likely to stop at the curb.Given the very small associations, these findings are likely notclinically significant. To our knowledge, this is the first study toexamine the relationship between parents’ perception of neighbor-hood safety and children’s pedestrian safety behaviors. Thesepreliminary bivariate results are informed by parallel studies con-ducted in Australia and the US examining neighborhood builtenvironment or safety and childhood obesity or physical activityoutcomes (Carver et al., 2010; Grow et al., 2008; Lumeng et al., 2006;Molnar et al., 2004; Timperio et al., 2005), and suggest the need forfurther study with additional environmental variables and adequately
powered samples. Neither traffic lanes nor neighborhood safety weresignificantly associated with child pedestrian safety outcomes in thegeneralized mixed model from the present study. These null findingssuggest that environmental influences on children’s pedestrian safetybehaviors may be less important than the influence of otherpedestrians, whether peers or adults, or the safety patrol.
Like most pilot studies, this study has limitations. First, weused cross-sectional school-level data on child pedestrians of anygrade level and not longitudinal data on the 4th grade WSB studyparticipants due to logistic complexity. This design likely dilutedthe impact of the intervention since many of the child pedestriansobserved at intervention schools were not directly involved in theWSB program. However, this school-wide assessment approachhas been used previously to examine pedestrian behaviors in the‘‘real world’’ (Hotz et al., 2004). Second, generalizability may belimited since all schools were low-income, composed primarily ofethnic minority children, and located in urban settings in Hous-ton. Third, although establishing changes to pedestrian safetybehaviors during the intervention was an important first step,we do not know if the changes are generalizable outside of thewalking school bus intervention. Future studies should measurepedestrian safety behaviors post-intervention, to determinesustainability of the potential behavior change. Finally, althoughwe included data on the number of traffic lanes at each intersec-tion and parents’ perception of neighborhood safety, we had onlylimited data on the neighborhood built environment, which hasbeen associated with pedestrian injuries (LaScala et al., 2004;Newbury et al., 2008; Schuurman et al., 2009). Despite theselimitations, this pilot study has a number of strengths: (1) thedesign was a randomized controlled trial, (2) it is among the firstWSB studies to examine children’s pedestrian safety, (3) it usedvalidated measures of pedestrian safety (Mendoza et al., 2010a) toassess children’s pedestrian safety behaviors in the field ratherthan relying on children’s self-reported behaviors or their safetyknowledge, and (4) we conducted the study among underrepre-sented ethnic minority schoolchildren who have a disproportion-ate risk for unintentional injuries in the US (Pressley et al., 2007).
5. Conclusion
This pilot study demonstrated the feasibility of collectingschool-level pedestrian safety behavior outcomes and changesto those outcomes during a WSB program study. In exploratoryanalyses, the WSB was associated with more children crossing atan intersection, but fewer children fully stopping at the curb.These mixed results suggest modification to the WSB programmay be necessary in order to improve children’s pedestrian safetybehaviors on the walk to and from school. Further WSB studies,preferably fully powered experimental trials that longitudinallyfollow participants’ pedestrian safety behaviors in the long term,should be conducted in a variety of settings among diversepopulations to formally evaluate pedestrian safety and physicalactivity outcomes. Moreover, studies that examine the influenceof the built environment, use objective measures of neighborhoodsafety, and consider vehicular traffic are also necessary to evalu-ate their influences on the WSB and children’s pedestrian safety.
Acknowledgments
We are grateful to the children and parents who participated inthis study and the reviewers who provided many helpful com-ments to improve this work. We thank the teachers, principals,administrators, and staff of HISD, for their support and partnershipin this study. This work was supported, in part, by Active Living

J.A. Mendoza et al. / Health & Place 18 (2012) 24–30 29
Research of the Robert Wood Johnson Foundation (63773), theNational Cancer Institute (1R21CA133418), and the Harris CountyHospital District Foundation. The first author was supported, inpart, by a career development award from the National CancerInstitute (1K07CA131178). This work was also supported by and isa publication of the US Department of Agriculture/AgriculturalResearch Service (USDA/ARS) Children’s Nutrition Research Center,Department of Pediatrics, Baylor College of Medicine, Houston,Texas, and was funded with federal funds from the USDA/ARSunder Cooperative Agreement No. 58-6250-6001. The funders hadno role in the study design; in the collection, analysis andinterpretation of data; in the writing of the report; and in thedecision to submit the paper for publication. The contents of thispublication do not necessarily reflect the views or policies of thefunders or Baylor College of Medicine, nor does mention of tradenames, commercial products, or organizations imply endorsementfrom the funders or Baylor College of Medicine.
References
Alexander, L.M., Inchley, J., Todd, J., Currie, D., Cooper, A.R., Currie, C., 2005. Thebroader impact of walking to school among adolescents: seven day accel-erometry based study. BMJ 331, 1061–1062.
Arain, M., Campbell, M., Cooper, C., Lancaster, G., 2010. What is a pilot or feasibilitystudy? A review of current practice and editorial policy. BMC MedicalResearch Methodology 10, 67.
Bandura, A., 1976. Social Learning Theory, 1st ed. Prentice Hall, Englewood Cliffs, NJ.Barton, B.K., Schwebel, D.C., Morrongiello, B.A., 2007. Brief report: increasing
children’s safe pedestrian behaviors through simple skills training. Journal ofPediatric Psychology 32, 475–480.
Berry, D.S., Romo, C.V., 2006. Should ‘Cyrus the Centipede’ take a hike? Effects ofexposure to a pedestrian safety program on children’s safety knowledge andself-reported behaviors. Journal of Safety Research 37, 333–341.
Brown, A., Marchetti, L., Pullen, N., Scully, M., Zegeer, C., 2007. Safe Routes toSchool Guide. National Center for Safe Routes to School, Chapel Hill, NC.
Burdette, H.L., Whitaker, R.C., 2005. A national study of neighborhood safety,outdoor play, television viewing, and obesity in preschool children. Pediatrics116, 657–662.
Carver, A., Timperio, A., Hesketh, K., Crawford, D., 2010. Are safety-related featuresof the road environment associated with smaller declines in physical activityamong youth? Journal of Urban Health 87, 29–43.
Chang, D., 2008. National Pedestrian Crash Report. In: US Department of Trans-portation (Ed.). National Center for Statistics and Analysis, Washington, DC.
Cooper, A.R., Page, A.S., Foster, L.J., Qahwaji, D., 2003. Commuting to school: arechildren who walk more physically active? American Journal of PreventiveMedicine 25, 273–276.
Coulton, C.J., Korbin, J.E., Su, M., 1996. Measuring neighborhood context for youngchildren in an urban area. American Journal of Community Psychology 24, 5–32.
Dellinger, A., Staunton, C.E., 2002. Barriers to children walking and biking toschool—United States, 1999. MMWR Morbidity and Mortality Weekly Report51, 701–704.
Demetre, J.D., Lee, D.N., 1992. Errors in young children’s decisions about trafficgaps: experiments with roadside simulations. British Journal of Psychology 83,189.
Duperrex, O.J.M., Roberts, I.G., Bunn, F., 2009. Safety education of pedestrians forinjury prevention. Cochrane Database of Systematic Reviews.
Glang, A., Noell, J., Ary, D., Swartz, L., 2005. Using interactive multimedia to teachpedestrian safety: an exploratory study. American Journal of Health Behavior29, 435–442.
Gresham, L.S., Zirkle, D.L., Tolchin, S., Jones, C., Maroufi, A., Miranda, J., 2001.Partnering for injury prevention: evaluation of a curriculum-based interven-tion program among elementary school children. Journal of Pediatric Nursing16, 79–87.
Grow, H.M., Saelens, B.E., Kerr, J., Durant, N.H., Norman, G.J., Sallis, J.F., 2008.Where are youth active? Roles of proximity, active transport, and builtenvironment. Medicine & Science in Sports & Exercise 40, 2071–2079(2010.1249/MSS.2070b2013e3181817baa).
Heelan, K.A., Abbey, B., Donnelly, J., Mayo, M., Welk, G.J., 2009. Evaluation of awalking school bus for promoting physical activity in youth. Journal ofPhysical Activity and Health 6, 560–567.
Hotz, G., Cohn, S., Castelblanco, A., Colston, S., Thomas, M., Weiss, A., Nelson, J.,Duncan, R., 2004. WalkSafe: a school-based pedestrian safety interventionprogram. Traffic Injury Prevention 5, 382–389.
Hotz, G.P., Kennedy, A.M.P.H., Lutfi, K.M.P.H., Cohn, S.M.M.D.F., 2009. Preventingpediatric pedestrian injuries. Journal of Trauma Injury Infection & Critical Care66, 1492–1499.
Information Services, 2009. Facts and Figures 2008–2009. Houston IndependentSchool District, Houston, TX.
Kraemer, H.C., Mintz, J., Noda, A., Tinklenberg, J., Yesavage, J.A., 2006. Cautionregarding the use of pilot studies to guide power calculations for studyproposals. Archives of General Psychiatry 63, 484–489.
Landsberg, B., Plachta-Danielzik, S., Much, D., Johannsen, M., Lange, D., Muller, M.J.,2007. Associations between active commuting to school, fat mass and lifestylefactors in adolescents: the Kiel Obesity Prevention Study (KOPS). EuropeanJournal of Clinical Nutrition 62, 739–747.
LaScala, E.A., Gruenewald, P.J., Johnson, F.W., 2004. An ecological study of thelocations of schools and child pedestrian injury collisions. Accident Analysis &Prevention 36, 569–576.
Leon, A.C., Davis, L.L., Kraemer, H.C., 2011. The role and interpretation of pilotstudies in clinical research. Journal of Psychiatric Research 45, 626–629.
Loucaides, C.A., Plotnikoff, R.C., Bercovitz, K., 2007. Differences in the correlates ofphysical activity between urban and rural canadian youth. Journal of SchoolHealth 77, 164–170.
Lumeng, J.C., Appugliese, D., Cabral, H.J., Bradley, R.H., Zuckerman, B., 2006.Neighborhood safety and overweight status in children. Archives of Pediatricsand Adolescent Medicine 160, 25–31.
Martin, S., Carlson, S., 2005. Barriers to children walking to or from school—UnitedStates, 2004. MMWR Morbidity and Mortality Weekly Report 54, 949–952.
McComas, J., MacKay, M., Pivik, J., 2002. Effectiveness of virtual reality for teachingpedestrian safety. CyberPsychology & Behavior 5, 185–190.
McKee, R., Mutrie, N., Crawford, F., Green, B., 2007. Promoting walking to school:results of a quasi-experimental trial. Journal of Epidemiology and CommunityHealth 61, 818–823.
Mendoza, J., Levinger, D., Johnston, B., 2009. Pilot evaluation of a walkingschool bus program in a low-income, urban community. BMC Public Health9, 122.
Mendoza, J., Watson, K., Baranowski, T., Nicklas, T., Uscanga, D., Hanfling, M.,2010a. Validity of instruments to assess students’ travel and pedestrian safety.BMC Public Health 10, 257.
Mendoza, J.A., Watson, K., Baranowski, T., Nicklas, T.A., Uscanga, D.K., Hanfling,M.J., 2011. The walking school bus and children’s physical activity: a pilotcluster randomized controlled trial. Pediatrics 128, e537–e544.
Mendoza, J.A., Watson, K., Baranowski, T., Nicklas, T.A., Uscanga, D.K., Nguyen, N.,Hanfling, M.J., 2010b. Ethnic minority children’s active commuting to schooland association with physical activity and pedestrian safety behaviors. Journalof Applied Research in Children 1 (Article 4).
Mendoza, J.A., Watson, K., Nguyen, N., Cerin, E., Baranowski, T., Nicklas, T.A., 2011.Active commuting to school and association with physical activity andadiposity among US youth. Journal of Physical Activity & Health 8, 488–495.
Molnar, B.E., Gortmaker, S.L., Bull, F.C., Buka, S.L., 2004. Unsafe to play?: neighbor-hood disorder and lack of safety predict reduced physical activity among urbanchildren and adolescents. American Journal of Health Promotion 18, 38–46.
Morrongiello, B.A., Barton, B.K., 2009. Child pedestrian safety: parental super-vision, modeling behaviors, and beliefs about child pedestrian competence.Accident Analysis & Prevention 41, 1040–1046.
Morrongiello, B.A., Kiriakou, S., 2006. Evaluation of the effectiveness of single-session school-based programmes to increase children’s seat belt and pedes-trian safety knowledge and self-reported behaviours. International Journal ofInjury Control and Safety Promotion 13, 15–25.
National Center for Injury Prevention and Control, 2010. Web-based InjuryStatistics Query and Reporting System. Centers for Disease Control andPrevention, Atlanta, GA.
National Center for Safe Routes to School, 2006. The walking school bus:combining safety, fun and the walk to school, Chapel Hill, NC.
National Center for Statistics and Analysis, 2011. Traffic Safety Fact Sheets.National Highway Traffic Safety Administration of the US Department ofTransportation, Washington, DC.
Newbury, C., Hsiao, K., Dansey, R., Hamill, J., 2008. Paediatric pedestrian trauma:the danger after school. Journal of Paediatrics and Child Health 44, 488–491.
Planning and Development Department, 2003. Houston Almanac: August 2003,4th edition City of Houston, Texas, Houston.
Pressley, J.C., Barlow, B., Kendig, T., Paneth-Pollak, R., 2007. Twenty-year trends infatal injuries to very young children: the persistence of racial disparities.Pediatrics 119, e875–884.
Preusser, D.F., Lund, A.K., 1988. And keep on looking: a film to reduce pedestriancrashes among 9 to 12 year olds. Journal of Safety Research 19, 177–185.
Rivara, F.P., Booth, C.L., Bergman, A.B., Rogers, L.W., Weiss, J., 1991. Prevention ofpedestrian injuries to children: effectiveness of a school training program.Pediatrics 88, 770–775.
Roberts, I., 1995. Adult accompaniment and the risk of pedestrian injury on theschool–home journey. Injury Prevention 1, 242–244.
Rosenbloom, T., Ben-Eliyahu, A., Nemrodov, D., 2008. Children’s crossing behaviorwith an accompanying adult. Safety Science 46, 1248–1254.
Rothengatter, T., 1984. A behavioural approach to improving traffic behaviour ofyoung children. Ergonomics 27, 147–160.
Saksvig, B.I., Catellier, D.J., Pfeiffer, K., Schmitz, K.H., Conway, T., Going, S., Ward, D.,Strikmiller, P., Treuth, M.S., 2007. Travel by walking before and after schooland physical activity among adolescent girls. Archives of Pediatrics andAdolescent Medicine 161, 153–158.
Schuurman, N., Cinnamon, J., Crooks, V., Hameed, S.M., 2009. Pedestrian injury andthe built environment: an environmental scan of hotspots. BMC Public Health9, 233.
Schwebel, D.C., McClure, L.A., 2010. Using virtual reality to train children in safestreet-crossing skills. Injury Prevention 16, e1–e5.

J.A. Mendoza et al. / Health & Place 18 (2012) 24–3030
Sirard, J.R., Alhassan, S., Spencer, T.R., Robinson, T.N., 2008. Changes in physicalactivity from walking to school. Journal of Nutrition Education and Behavior40, 324–326.
Sirard, J.R., Riner Jr., W.F., McIver, K.L., Pate, R.R., 2005. Physical activity and activecommuting to elementary school. Medicine and Science in Sports and Exercise37, 2062–2069.
Spinks, A., Macpherson, A., Bain, C., McClure, R., 2006. Determinants of sufficientdaily activity in Australian primary school children. Journal of Paediatrics andChild Health 42, 674–679.
Staunton, C.E., Hubsmith, D., Kallins, W., 2003. Promoting safe walking and bikingto school: the Marin County success story. American Journal of Public Health93, 1431–1434.
Thomson, J.A., Tolmie, A.K., Foot, H.C., Whelan, K.M., Sarvary, P., Morrison, S., 2005.Influence of virtual reality training on the roadside crossing judgments of childpedestrians. Journal of Experimental Psychology: Applied 11, 175–186.
Timperio, A., Salmon, J., Telford, A., Crawford, D., 2005. Perceptions of localneighbourhood environments and their relationship to childhood overweightand obesity. International Journal of Obesity 29, 170–175.
Tolmie, A., Thomson, J.A., Foot, H.C., Whelan, K., Morrison, S., McLaren, B., 2005.The effects of adult guidance and peer discussion on the development ofchildren’s representations: Evidence from the training of pedestrian skills.
British Journal of Psychology 96, 181–204.Wang, Y., Lobstein, T., 2006. Worldwide trends in childhood overweight and
obesity. International Journal of Pediatric Obesity 1, 11–25.World Health Organization, 2010. Global Recommendations on Physical Activity
for Health. Global Strategy on Diet, Physical Activity and Health. World HealthOrganization, Geneva, Switzerland.
Young, D.S., Lee, D.N., 1987. Training children in road crossing skills using a
roadside simulation. Accident Analysis & Prevention 19, 327–341.Zeedyk, M.S., Kelly, L., 2003. Behavioural observations of adult–child
pairs at pedestrian crossings. Accident Analysis and Prevention 35, 771–776.
Zeedyk, M.S., Wallace, L., Spry, L., 2002. Stop, look, listen, and think? What youngchildren really do when crossing the road. Accident Analysis and Prevention
34, 43–50.