“immune therapy is a game changer. we need more research ... · pdf filebloomberg~kimmel...
TRANSCRIPT
“Immune therapy is a game changer. Weneed more research to take us the restof the distance, but we don’t think thereis a single cancer that the patient’s ownimmune system ultimately can’t beat.”
–Cancer Immunologist Drew Pardoll, M.D., Ph.D.
SPECIAL ISSUE
BL OOMBERG~KIMMEL INSTITUTE for CANCER IMMUNOTHERAPY
2 0 1 6 / 2 0 1 7
T H E S I D N E Y K I M M E LC O M P R E H E N S I V E
CA N C E R C E N T E R ATJ O H N S H O P K I N S

2 PROMISE & PROGRESS
JOHN RYAN IS AMONG THE MANY PATIENTSWHO HAVE BENEFITTED FROM A PROMISING NEW IMMUNE THERAPY CALLED ANTI-PD1.
THE SIDNEY KIMMEL COMPREHENSIVE CANCER CENTER at JOHNS HOPKINS 3
The Final Frontier?Immune Therapies Break Through Cancer’s Protective Barriers
Immune therapy is recognizably different from all conventional cancer therapies. Imagine acancer treatment that works without making patients sick or causing their hair to fall out.Doctors and nurses agree it is unlike anything they have ever witnessed in the world of cancermedicine. Gone are the iconic bald heads that immediately identified a person—inside oroutside of the hospital—as a cancer patient. Like no other disease, cancer has traumatizedthe human population with its lethality and toxic treatments. That’s all changing now, astherapies that empower the body’s own natural defenses are at last becoming a reality andproviding unparalleled, long-lasting responses across many cancer types, and even in themost advanced and treatment-resistant cancers.
cells. Researchers and clinicians at theKimmel Cancer Center have worked together with experts throughout JohnsHopkins, using science to follow theclues and bring the world what may be a universal treatment for cancer. Cancerimmunology and melanoma expertSuzanne Topalian calls immunotherapy“the common denominator.”
Immune-based therapies reflect a dif-ferent approach to treatment. Instead oftargeting cancer cells, the new therapiestarget immune cells in and around cancers.Some treatments increase the number ofimmune cells summoned to the tumor,
and others unleash the commands thatsend the immune cells to work against it.These types of immune therapies havehad success alone, but perhaps theirgreatest power will come in combiningthem and, through precision medicine,using the biological clues within each pa-tient’s cancer to guide treatment.
Leading the way are scientists, likeDrew Pardoll and Elizabeth Jaffee,who have been at work for more than 30years deciphering the mechanisms of theimmune system, how it works and why itall too often does not work against can-cer. As students of the immune system,Pardoll, Jaffee, and others understoodthat the characteristics of the immunesystem should make it the perfect anti-cancer weapon, but if the cancer cell wascomplex in its molecular construction,the intricacies of the immune systemwere equally complicated.
Unlike viruses and bacteria that areeasily recognized by our immune systembecause they are so different, cancer orig-inates from our own cells. As a result, ithas all of the cellular mechanisms thatare used by normal cells at its disposal.
PATIENTS ARE SAYING they don’t feellike they have cancer. Knowing whatcancer treatment is “supposed” to belike—many having already experiencedit—they worry that they feel too well. Manyask: “If I feel this healthy, could the treat-ment really be working?”
The answer, experts say, is a resound-ing “yes,” and the Kimmel Cancer Centeris leading the way with its unprecedentedfindings echoing through the laboratoriesand waiting rooms of medical institutions,community hospitals, and cancer clinicsall over the world.
“This is oncology of the future,” saysWilliam Nelson, Kimmel Cancer CenterDirector, “and the future is now.”
A Game Changer As long as cancer has been a recognizeddisease, doctors have believed the powerto eliminate it existed within the immunesystem, but attempt after attempt to unlock this potential has largely failed. The potential always existed, but the keyinformation needed to turn this promiseinto real treatments was locked away inside the DNA of tumor and immune
DREW PARDOLL AND ELIZABETH JAFFEE, CIRCA 1989.

4 PROMISE & PROGRESS
The secrets of the cancer cell’s ability to dodge an immune attack are being revealed, and the results, though admittedly early,are like nothing that has ever been seen in cancer medicine.
RESEARCHERS AND CLINICIANS AT THE KIMMEL CANCER CENTER HAVE WORKED TOGETHER WITH EXPERTS THROUGHOUT JOHNSHOPKINS, USING SCIENCE TO FOLLOW THE CLUES AND BRING THE WORLD WHAT MAY BE A UNIVERSAL TREATMENT FOR CANCER.CANCER IMMUNOLOGY AND MELANOMA EXPERT SUZANNE TOPALIAN CALLS IMMUNOTHERAPY “THE COMMON DENOMINATOR.”
Immune CheckpointBlockadesMore than 8000 practicing oncologistsand clinical cancer scientists from allover the world filled the lecture hall at the 2015 annual meeting of the AmericanSociety of Clinical Oncology (ASCO). It’s not the first time a standing-room-only crowd has come there to hear aKimmel Cancer Center cancer expertdiscuss one of the most promising newcancer therapies in decades—immunecheckpoint blockade. This time, cancerimmunology expert Suzanne Topalian wasthere as the David A. Karnofsky Memorial
ability to dodge an immune attack arebeing revealed, and the results, thoughadmittedly early, are like nothing that hasever been seen in cancer medicine. Utterdestruction of the most resistant, lethaltumors is occurring across many cancertypes and with few side effects. Patientswho were months, even weeks, fromdying are alive and well, some five yearsor more after treatment.
It was what Pardoll and Jaffee imag-ined three decades ago when they firstbegan studying the immune system—perhaps even better.
Cancer co-opts them selectively, usingthem like superpowers to grow, spread,and cloak themselves from the immunesystem.
It took time for the technology tocatch up with the scientific ideas, but the invincible cancer cell may have finallymet its match. This Kimmel Cancer Center team of multispecialty collabora-tors—seasoned investigators and youngclinician-scientists—has figured out howto reset the cellular controls hijacked bythe cancer cell and restore power to theimmune system. In a convergence of immunology, genetic, and epigeneticfindings, the secrets of the cancer cell’s
THE SIDNEY KIMMEL COMPREHENSIVE CANCER CENTER at JOHNS HOPKINS 5
types of therapy, oncologists wanted toknow more. Scholarly journals and thenews media alike were reporting ondrugs that caused lethal melanoma skincancers, kidney cancers, and lung can-cers to melt away and stay away.
The therapies are so new—first testedin patients in 2006—that the KimmelCancer Center immunology team readilyadmits there is much left to learn. “Wedon’t know yet what the ultimate survivalbenefit will be, but for some patients inthese first trials, the responses are still
“Cancer cells take control of a valuable immune response regulator and turn it on its head. The anti-PD-1 therapy allows us to seize that power back.”
BOB ANDERS
AMONG NORMAL CELLS, PD-1 IS NOT A BAD ACTOR, EXPLAINS BLOOD AND BONE MARROW CANCER EXPERT AND IMMUNOLOGYCOLLABORATOR JONATHAN POWELL. “IT’S ACTUALLY A GOOD THING. IT’S THE MEANS BY WHICH THE IMMUNE SYSTEM REGULATES ITSELF. IT MAKES SURE THE IMMUNE SYSTEM DOESN’T OVERDO ITS JOB.”
Award and Lecture recipient for “out-standing contributions to the research,diagnosis, and treatment of cancer.” In2012, Thoracic Oncology Program Direc-tor Julie Brahmer presented findings onan immune checkpoint blockade study inlung cancer. It marks a changing tide inclinical cancer research. Immunologystudies had never before received thislevel of attention at ASCO meetings.
With remarkable and lasting resultsin about 20 to 40 percent of patients withadvanced cancers that resisted all other
ongoing after many years,” says Pardoll.These long-lasting responses that contin-ued even after therapy was stopped andcaused few side effects are the reason the auditorium was filled to capacitywith doctors anxious to learn how andwhen they could get this new therapy fortheir patients.
The source of the excitement is animmune target called PD-1 and a relatedpartner protein on tumor cells calledPD-L1. PD-1 is what immunology expertscall an immune checkpoint. Pardoll stopsshort of calling it an immune systemmaster switch, but the results in labora-tory research and these early clinical trialspoint to it as one of the strongest influ-encers of an immune response to canceridentified so far. It—and likely some othersimilar proteins—is responsible for can-cer’s ability to avert an immune attack.
There are two main actions at playin an immune reaction. The first is a “go”signal. “Our cells are constantly present-ing our own proteins to our own immunesystem,” explains pathologistBob Anders.One can think of DNA as the blueprint ofa cell, and the proteins its genes encodeare its building blocks. A protein from amutated gene looks different than itsnormal counterpart. In the same way itrecognizes bacteria and viruses, the pa-trolling immune system can recognizeabnormal cells that don’t belong. “Whenimmune cells come upon something thatshouldn’t be there, they generate an im-mune reaction,” says Anders. This is the

6 PROMISE & PROGRESS
Lessons from theFirst Immune Therapy
SOME OF THE earliest research at theKimmel Cancer Center that focused onthe immune system was in blood andbone marrow cancers and bone marrowtransplantation. Cancers of the bloodand bone marrow, such as leukemia,lymphoma, and multiple myeloma, pro-vided a unique perspective of normalimmune cells, malignant ones, and themagnitude of the immune system’s power
In most cancers, the goal is to engagethe immune system, but in bone marrowtransplant, where the patient’s cancer-filled bone marrow is replaced withhealthy marrow from a donor, the goal isto disengage—well, at least a little. Thereason is a serious complication of bonemarrow transplant known as graft versushost disease (GVHD), a destructive im-mune attack against the patient’s organsand tissue. The transplanted marrowsees its new host as foreign and wages anassault that can be as lethal as cancer.
Veteran cancer immunology leaderDrew Pardoll first observed its wrath as an oncology trainee treating a younggirl dying from severe GVHD. It was a defining moment for the young physician-scientist. “I realized that theimmune system was probably the mostpowerful anticancer weapon we have,”says Pardoll. “If we learned how it workedand could focus it more precisely againstcancer, I believe it could be more power-ful than any drug.”
Pardoll decided to focus on deci-phering how the immune system worked,while Kimmel Cancer Center bone mar-row transplant experts began solving the problem of GVHD in what could be considered one of the first immunesuccess stories in cancer treatment.
Making Bone MarrowTransplant Safe andAvailable to All FOR DECADES GVHD prevented bonemarrow transplants from being performedon patients who did not have a donor witha nearly identically matching immune
system, usually found in a brother or sister. A large national registry matchedsome of these patients with unrelateddonors, but most grew sicker and manydied waiting for a match to be found. As a result, only about one-half of patientswere candidates for the potentially curative therapy. Minorities suffered the most. African-American patientswho did not have a match in their familyhad less than a 10 percent chance of finding a donor in the unrelated registry.
Pioneering discoveries led by Kimmel Cancer Center investigatorsRichard Jones, Ephraim Fuchs and Leo Luznik have now made it possiblefor almost any patient to receive a trans-plant. The research that led to this break-through focused on immune cells knownas T cells and technologies to removethese cells from the donor marrow. Clini-cal studies showed that when the T cellswere removed, patients did not get GVHDbut their cancers sometimes came back.It was one of the first observations of theimmune system’s ability to kill cancer cells.The challenge was to remove a preciseamount of T cells—small enough to avoidthe most severe cases of GVHD, yet a largeenough number to allow the immunesystem to keep the cancer from returning.
It turns out that the same drug usedto treat patients before bone marrowtransplant could be given post-transplantto limit GVHD without hampering the T cells’ ability to mop up any survivingcancer cells. This discovery led KimmelCancer Center experts to develop a newtype of bone marrow transplant, known asa haploidentical or half-identical transplant.
In this breakthrough approach developed at the Kimmel Cancer Center,
almost all parents, siblings, and childrenof patients—and sometimes even auntsand uncles, nieces and nephews, half-siblings, and grandparents or grandchil-dren—can safely serve as donors. Now,almost every patient who needs a bonemarrow transplant can find a matchingdonor. Since developing the treatmentmore than a decade ago, Kimmel CancerCenter experts have performed more than600 half-matched transplants for adultand pediatric leukemia and lymphoma.
These clinical studies have provenso successful, with safety and toxicitycomparable to matched transplants, thatthe therapy is now used to treat chronicbut debilitating noncancerous diseasesof the blood in adults and children, suchas sickle cell disease and severe autoim-mune disorders.
More recently, a revolutionary studyusing half-matched transplants to improvethe effectiveness and safety of solid organtransplants with living donors has begun.Kimmel Cancer Center researchers arecollaborating with transplant surgeonsto begin a combined kidney/half-identicalbone marrow transplant. Since the patient and donor would have the sameimmune system, it could essentiallyeliminate organ rejection and a lifetimeof antirejection drugs.
If successful, this important workwill conquer the transplantation barrier—rejection—and what is learned could beapplied to all solid organ transplants. Italso facilitates the research being done in regenerative medicine, where work togrow transplantable tissue and organswould ultimately be of no clinical usewithout the means to successfully andsafely transplant them into humans.
RICHARD JONES EPHRAIM FUCHS, LEO LUZNIK

THE SIDNEY KIMMEL COMPREHENSIVE CANCER CENTER at JOHNS HOPKINS 7
go signal. When the job is done and the invading cells are taken care of, theimmune system issues a “stop” signal.
These stop signals are controlled by immune checkpoints like PD-1. In cancer,malignant cells hijack the “stop” signal to maintain their own survival. They senda deceptive message to cancer-killing immune cells that there is no problem.Immune cells arrive at the tumor, butthey are duped with a false message thateverything is OK. “Essentially, they’retold to go home. There is nothing to seehere,” says pathologist Janis Taube.
Taube and Anders describe a sce-nario in which a tumor is spreading, andas immune cells come in to try to removethe cancer, the cancer turns up the volumeon PD-1, a signal that turns the immunecells off. “The tumor cells use our ownphysiology against us,” says Anders.
The “volume” of the PD-1 stop signalis controlled in the cancer cell by the expression of one or both of two partnerproteins called PD-L1 and PD-L2. Insolid tumors, like melanoma and lungcancer, PD-L1 has received the most attention today, but PD-L2 appears toplay an important role in cancers thatstart in the blood and lymphnodes, such as leukemia andlymphoma. “We see PD-L1frequently in melanoma,” saysTaube. “PD-L1 is expressed on the surface of the tumorcell. When you see it throughthe microscope, it looks likesomeone outlined the cellswith a marker. It forms anarmor that protects the cancer cell from the immune system.”
Giving patients a drug, known as ananti-PD-1 checkpoint blocker, for its abil-ity to interrupt PD-1 signaling as well asthe communication between PD-1 andPD-L1 and PD-L2, removes the stop sig-nal and re-engages the immune system.
Among normal cells, PD-1 is not abad actor, explains blood and bone
marrow cancer expert and immunologycollaborator Jonathan Powell. “It’s actually a good thing. It’s the means bywhich the immune system regulates itself.It makes sure the immune system doesn’toverdo its job,” he says. It’s the cancercell that once again assumes the role ofvillain. PD-1 is an immune mechanismthat has been usurped by the cancer cell.“Cancer cells take control of a valuableimmune response regulator and turn it on its head,” he says. “Anti-PD-1 therapyallows us to seize that power back.”
Unbelievable PatientResponsesJohn Ryan is among the many patientswho have benefited from the anti-PD-1therapy being discussed at ASCO.
Ryan, 71, began experiencing symp-toms in 2013 when he coughed up a smallamount of blood. The husband and fatherof eight thought it was strange, but withno pain or other symptoms he was stunnedto learn he had the most advanced stageof a common form of lung cancer knownas non-small cell lung cancer. The cancerhad already spread to a rib.
There are few diagnoses worse than late stage lung cancer. Thecancer kills more peoplethan any other type of cancer, and few patientssurvive once it has spread.At this stage, the cancer is treatment resistant, responding for a brieftime to chemotherapy or cancer-gene-targetedtherapies, but almost
always resurging even stronger.Medically speaking, Ryan’s diagnosis
was Stage 4 non small cell adenocarcinomaof the lung. “One of my sons was graduat-ing from college, and my daughter wasabout to leave for a study abroad. I wondered if I would live long enough tosee my son graduate or to welcome mydaughter back home,” Ryan recalls.
For a time the chemotherapy worked,but the treatment came at great physicalcost, and these side effects were worsen-ing. The simplest tasks became difficult.His body was weakening, and worse, he learned his cancer was no longer responding. Genetic testing of his tumordid not reveal any mutations that wouldmake him a candidate for targeted thera-pies. It seemed he was out of optionsuntil his doctor suggested he go to theKimmel Cancer Center and meet withlung cancer expert Julie Brahmer.
Brahmer was one of the lead investi-gators on an experimental clinical studyof the anti-PD-1 therapy in a variety ofadvanced cancers. Ryan’s form of lungcancer was among the cancers thatshowed unprecedented responses.
“Before I began treatment, I strug-gled to sit at my kitchen table. After justfour treatments, the tumor shrunk by 65percent, and I felt like a human beingagain,” says Ryan. A few more treatmentsand Ryan’s rapidly growing lung cancerwas nearly gone, and the cancer thatspread to his rib was eliminated. His onlyside effect was some minor skin irritationshe compared to a mosquito bite.
Anti-PD-1 is not the first checkpoint blockade therapy, but it is the first towork beyond melanoma in as many as 14 other cancer types, and that’sthe pivotal difference that has excited the cancer world.
PATHOLOGIST JANIS TAUBE SAYS THERE ARE BIOMARKERSTHAT CAN BE USED TO PREDICT RESPONSE TO IMMUNETHERAPY WITH ANTI-PD-1 CHECKPOINT INHIBITORS.TUMOR CELLS THAT EXPRESS PD-L1, HAVE MANY GENE MUTATIONS, AND ALREADY HAVE KILLER IMMUNE CELLSPRESENT ARE MOST LIKELY TO RESPOND. THE CANCER IMMUNOLOGY TEAM IS WORKING TO IDENTIFY OTHERCHARACTERISTICS, LIKE MISMATCH REPAIR ALTERATIONS,THAT WILL MAKE CANCER CELLS MORE VULNERABLE TOIMMUNE THERAPY.
JANIS TAUBE

8 PROMISE & PROGRESS
Ryan is not an isolated case. Topalianand Brahmer say about one-quarter ofthe lung cancer patients in their studiesresponded to the treatment. The num-bers are even higher for melanoma andkidney cancer patients.
Anti-PD-1 is not the first checkpointblockade therapy, but it is the first to workbeyond melanoma in as many as 14 othercancer types, and that’s the pivotal differ-ence that has excited the cancer world.
The Lung Cancer DifferenceThe first clinical reports of checkpointinhibitors in melanoma were excitingand peaked interest, but excitement wastempered because the few successes inimmune therapy over the last threedecades had also been primarily inmelanoma and kidney cancer. Therehave been documented cases of thesecancers occasionally going into sponta-neous remission, so experts long main-tained that, by nature, these types ofcancers had a way of engaging the immune system. No other type of cancerwas considered to be responsive to immune interventions. The new therapywas greeted with guarded optimism.
That all changed in 2012 when the Kimmel Cancer Center group publishedthe results of anti-PD-1 therapy in lung
cancer patients. Lung cancer had neverbefore responded to an immune therapy,and the remarkable activity of anti-PD-1in a small number of lung cancer patientsproved what Pardoll and other cancerimmunologists long believed—if under-stood, the immune system could be usedto fight any cancer. “Anti-PD-1 has be-come a cancer juggernaut,” says Pardoll.
Pardoll first became interested inthe protein in 2000, when he came uponPD-1’s second partner, PD-L2. LiepingChen, a collaborator of Pardoll’s at theKimmel Cancer Center who is now atYale, had just discovered PD-L1 andshowed that it’s expression in humanlung cancer cells was highly elevatedcompared to normal cells. Although lung cancers had not responded to otherpast immune therapy attempts, this discovery provided new evidence that it had the potential to work and was thereason the Kimmel Cancer Center teamincluded lung cancer patients in the firstanti-PD-1 trial.
Powell is excited about the successof PD-1 in patients, but he is also enthusi-astic about what he sees as a triumph ofscience. “What we have learned is so encouraging,” he says. “The mere factthat we can block a checkpoint and makea tumor go away is an incredibly impor-tant finding because it tells us that the
human body—even without help fromimmunologists—has an immune responseto cancer. The problem is that the responseis being blocked. That concept, and thefact that it is true in people, is exceedinglyimportant.”
“This is yet more evidence thatwell-thought-out, consistent and collab-orative research pays off,” says WilliamNelson, the Kimmel Cancer Center Director. “Anti-PD-1 is a triumph of teamscience.” It is this willingness to followleads and seek out other experts that can inform the process that continues to position Johns Hopkins as a leader in transitioning laboratory science intopioneering cancer therapies, he says.
“We developed this one from scratchat the Kimmel Cancer Center,” says Pardoll.As soon as the components of the PD-1pathway were discovered in 2000, Pardoll,Topalian, Brahmer, and immunology andgenitourinary cancer expert ChuckDrake saw the potential of blocking it.They began working with the smallbiotech company Medarex to developthe first anti-PD-1 antibody in the labora-tory and took it to patients. They toofound strong responses in melanoma, butit was Brahmer’s lung cancer patients thatwere game changers.
This was the moment Pardoll andTopalian, who are not only research part-ners but also husband and wife, werewaiting for. It was a belief Pardoll hadstaked his career on, and one that causedTopalian to change course from a careeras surgical oncologist to immunology. Sheworked as a National Cancer Institutescientist alongside cancer immunologypioneer Steven Rosenberg for 20 yearsbefore coming to the Kimmel Cancer Center.
Rosenberg’s research of interferonsand interleukins, cellular messengerscritical to immune responses, garneredsimilar excitement in the 1980s as a po-tential broad-based immune treatmentfor cancer. The cover of Timemagazineboasted the headline “Interferon: TheCure for Cancer.” When the celebratedtreatment failed to live up to expectations—most of which had been generated byan eager news media desperately waitingfor the grand-slam victory that had been
JULIE BRAHMER WAS ONE OF THE LEAD INVESTIGATORS ON AN EXPERIMENTAL CLINICALSTUDY OF THE ANTI-PD-1 THERAPY IN A VARIETY OF ADVANCED CANCERS.

Personalized Cell Therapy
T CELLS ARE THE foot soldiers of the im-mune system, and MILs are a type oftumor-specific T cell, a small subset ofimmune cells that recognize cancercells. In cancers of the blood, MILs arefound in the bone marrow where thecancer originates. In this new approach,our scientists retrieve patients’ ownMILs from their bone marrow, expandtheir numbers and coat the cells withimmune- activating antibodies in a spe-cial Cell Therapy Lab at Johns Hopkins,and then infuse them back into the patient’s bloodstream where they seekout and destroy cancer cells.
Borrello is using MILs therapy totreat patients with an incurable cancer ofthe blood plasma cells known as multiple
myeloma. In a first-of-its-kind clinicaltrial of the therapy, 22 patients withnewly diagnosed or recurrent multiplemyeloma received the therapy. Followingstandard treatment for multiple myeloma—high-dose chemotherapy to destroy thediseased bone marrow—and a stem celltransplant to repopulate the marrowwith normal blood and immune cells, patients were given their own MILs.
One year after MILs therapy, 13 pa-tients had at least a 50 percent reductionin their cancer. Their cancer remainedstable for nearly a year, and overall survival was close to three years. Sevenpatients saw a 90 percent reduction, andtheir cancer has remained in check formore than six years. There were no
serious side effects to the therapy. “This was a small trial, but we learned thatlarge numbers of activated MILs can selectively target and kill myeloma cells,” says Borello.
There is currently an ongoing clinicaltrial targeting myeloma patients withhigh risk features. Borrello and team hopeto determine if the approach can impactpatients where standard approaches areineffective. The trial will soon be extendedto other cancer centers.
Borrello and collaborator Kimberly Noonan, a research associate in theschool of medicine, say the studies shedlight on better ways to grown MILs. “In most of these trials, you see that themore cells you get, the better responseyou get in patients. Learning how to improve cell growth may improve theoutcomes of therapy,” says Noonan.
The research indicates that MILscould also be beneficial in the treatmentof a variety of other cancers, so Borrellohas involved a team of heavy hitters tohelp advance the science and clinicalreach beyond myeloma. Other plans include administering MILs in patientsthat have relapsed following an allogeneicbone marrow transplant, using MILsfrom the patient grown and expanded inthe laboratory, rather than immune cellsfrom the bone marrow donor. MILs arebeing developed to treat lung, esophageal,gastric, and prostate cancer in adults andneuroblastoma and Ewing’s sarcoma inpediatric patients. The team includes ofsome of the Kimmel Cancer Center’sleading experts in immunology, bloodand bone marrow cancer, and experts inspecific cancers, including Drew Pardoll,Carol Ann Huff, Leo Luznik, WilliamMatsui, Jonathan Powell, EphraimFuchs, Richard Ambinder, RichardJones, Ronan Kelly, Nate Brennan, and Brian Ladle.
THE SIDNEY KIMMEL COMPREHENSIVE CANCER CENTER at JOHNS HOPKINS 9
Kimmel Cancer Center immunology and bone marrow transplantexpert Ivan Borrello has developed a novel personalized cancertreatment approach called adoptive T cell therapy using the patients’ own immune cells to fight their cancer. This approachuses cells from the bone marrow known as marrow infiltratinglymphocytes, or MILs.
IVAN BORRELLO

10 PROMISE & PROGRESS
promised when the “war against cancer”was announced in 1971—the field of can-cer immunology was nearly crushed. To be fair, interleukin-2 treatment, while adifficult treatment for patients, continuesto be used occasionally today and ishighly effective in some patients withmelanoma and kidney cancer. However,instead of being the blockbuster immunetherapy people had hoped for, it was astart. “It was the first evidence that a drugthat acted only through the immune system could fight very advanced cancer,”says Topalian. “That was important because it told us we were on the righttrack with immunotherapy and neededto keep working on this.”
In fact, many outside the field ofcancer immunology had begun to doubtthe promise of immune treatments in cancer. Immunotherapy discussions at the large national cancer meetings weresparsely attended, and research fundingwas hard to come by. The Kimmel CancerCenter immunology team remained undeterred. They knew the power of theimmune system and their convictions werecemented in this truth. The challenge waschanneling this power into real therapies.
The promise of immune therapy ischanging the way new therapies arestudied and evaluated. Chemotherapypoisons cells dividing quickly, includingimmune cells. This toxic effect is thecause of the common side effects, likehair loss, nausea, and infection risk dueto a compromised immune system. Immune therapies appear to work moreslowly over time, and it’s looking nowlike they work better for longer. Some ofthis was learned almost serendipitously,as cancers that initially looked like theywere not responding to immune treat-ments, with more time, began to shrink.“The immune system has been livingwith cancer for years. To make it not beso happy living with the cancer takessome time,” says Drake.
Eventually, it all rested upon what was learned with science and technology—powerful new ways to look inside theDNA of cancer cells and computerizeddata mining that measures and quantifiesthe subtlest of changes and differencesamong seemingly similar cancers.
The mechanisms that make therapywork in one patient and not in another arenow being teased out. Treatments that
worked only in a small subset of patientswere once deemed failures. Now, in an eraof precision medicine that uses molecularmarkers to identify the right treatment foreach patient, the options are much broaderand the outlook is significantly brighter.
First, There Were Cancer VaccinesCancer vaccines were one of the first immune treatments studied by KimmelCancer Center investigators. Early research on cancer vaccines by immunol-ogist and pancreatic cancer expert Elizabeth Jaffee proved the ability tosuccessfully recruit immune cells to tumors, and even had some therapeuticbenefit. All too often, however, the immune cells—called to the tumor by the vaccine in large numbers—did notfully attack the cancer.
Vaccines can peak the immune re-sponse in days, calling immune cells tothe tumor site. To reverse tolerance ofthe cancer—characterized by immunecells flooding to the tumor site but nottaking action—can take time. It may alsorequire additional kinds of immune thera-pies. Some patients’ immune systems areon the edge, requiring just a vaccine tomake them respond. Others need more.
Jaffee andDaniel Laheru, co-direc-tors of the Skip Viragh Center for PancreasCancer Clinical Research and Patient Care,are leading the way in cancer vaccinetherapy, and their target is one of thedeadliest of cancers.
Jaffee began working on a pancreaticcancer vaccine more than two decades ago.To make vaccine therapy a reality, she became an expert in FDA regulations andvaccine manufacturing, and she opened a GMP (good manufacturing practices)facility at the Kimmel Cancer Center tomake vaccines for clinical studies.
Jaffee, Laheru, and young investiga-tors Dung Le, Lei Zheng, Erik Lutz
“Pancreatic cancer is notorious for being in areas outside of thepancreas, and the vaccine allows us to get ahead of the dis-ease and get microscopic cancer cells that surgery might miss.”
IMMUNOLOGY AND GENITOURINARY CANCER EXPERT CHUCK DRAKEHELPED DEVELOP THE FIRST ANTI-PD1 ANTIBODY IN THE LABORATORY.

THE SIDNEY KIMMEL COMPREHENSIVE CANCER CENTER at JOHNS HOPKINS 11
and others are testing various versions ofthe vaccine. It is built from pancreaticcancer cells that have been rendered dormant with radiation and engineeredto recruit immune cells to track and attack malignant cells anywhere in thebody and to continue to do it indefinitely.
In some patients, the original itera-tion of the vaccine has worked remark-ably. Patients like nearly 20-year survivorKathleen Dowell, 12-year survivor DonnaBender, and eight-year survivor NancyAmato were given months to live whentheir pancreatic cancers persisted aftersurgery, chemotherapy, and radiationtherapy. Jaffee’s vaccine continues tokeep their cancers in check.
Because it is perhaps one of the onlytreatments that make any real differencein long-term survival for this most aggressive of cancers, the vaccine has
attracted worldwide attention. Clinic coordinator and research nurse BarbaraBiedrzycki receives more than 60 callsper month from patients who want to getthe vaccine. Once after an appearance byJaffee on The Dr. Oz Show, the clinic wasflooded with more than 1,000 inquiriesfrom patients all over the country. “Thereis no other cancer center doing this kindof work,” say Zheng.
With funding from the Skip ViraghFoundation, Laheru, Zheng, Lutz, and Leare working with Jaffee to optimize theeffects of her pioneering vaccine. Theyare making tweaks in timing of vaccinationand changes to its composition and deliv-ery that they hope will boost its cancer-killing capabilities and make the vaccinea treatment option for many more patients.
One of their new approaches is togive the vaccine before surgery. “Pancre-
atic cancer is notorious for being in areasoutside of the pancreas, and the vaccineallows us to get ahead of the disease andget microscopic cancer cells that surgerymight miss,” says Laheru.
Other variations include combinedtreatments. In some patients, giving theimmune-modulating drug cyclophos-phamide before the vaccine causes im-mune structures to form inside tumorsthat help regulate immune cell activation.“These organized immune structures donot naturally appear in pancreatic cancers,”says Zheng. “This suggests that there hasbeen significant reprogramming of im-mune cells within the tumor.” There isevidence that adding a checkpoint block-ade like anti-PD-1 treatment to the mixcould further enhance immune activity.
Another combined approach adds a second kind of vaccine, a weakened
EARLY RESEARCH ON CANCER VACCINES BY IMMUNOLOGIST AND PANCREATIC CANCER EXPERT ELIZABETH JAFFEE PROVED THE ABILITY TO SUCCESSFULLY RECRUIT IMMUNE CELLS TO TUMORS AND EVEN HAD SOME THERAPEUTIC BENEFIT.

12 PROMISE & PROGRESS
version of the bacterium listeria. The listeria is genetically modified to be safefor humans but stimulates an immune response against the protein mesothelin.Ralph Hruban, pathologist and Directorof the Sol Goldman Pancreatic CancerResearch Center, found mesothelin inhigh levels on the surface of pancreaticcancer cells, and Jaffee and Le believethe protein helps pancreatic cancer cellsto grow and spread. “The combinationessentially trains the body to recognizeand attack pancreatic tumors,” says Le.
Ongoing research has revealed thatmesothelin is over-expressed in many
cancers, including about one-half of lungcancers, mesotheliomas, ovarian cancers,and stomach cancers. As a result, the vac-cine is now being tested in lung cancerand mesothelioma, and Kimmel CancerCenter immunology expert Leisha Emenswill lead a trial testing it in ovarian cancer.
Patient Perspective Sarasota internist Jonathan Greco, 58, isamong 90 patients enrolled in a clinicaltrial to test the effectiveness of a cyclophosphamide, GVAX, listeria, andanti-PD-1 quadruple combination.
After nine weeks of chemotherapy
at a cancer clinic near his home, Grecosays he felt worse than he ever had his life.He told himself it was worth it because,as bad as he felt, his doctors told him itwas causing his pancreatic cancer toshrink enough that it could be cut outwith surgery.
As a physician, Greco knew of JohnsHopkins expertise in the Whipple proce-dure, the primary surgical treatment forpancreatic cancer. Johns Hopkins sur-geons perfected the procedure, performmore of them, and train more new sur-geons how do the procedure than anyother institution in the world. With thisin mind, Greco scheduled a consultationat the Kimmel Cancer Center’s Skip Viragh Center.
At his consultation, he learned thechemotherapy hadn’t worked. In fact, hiscancer was quite advanced, and a Whip-ple procedure would not help him. “I’mso thankful I came to Johns Hopkins,”says Greco. “If I had listened to the doc-tors in Florida and went ahead with thesurgery, I’m certain I would have died.”
Greco continued to do his research.He was familiar with immune therapyand went to the National Cancer Insti-tute’s clinicaltrials.gov website to searchfor experimental treatments and infor-mation. “Johns Hopkins clearly had themost immunotherapy experience. It wasevident they had been doing this longerthan anybody,” says Greco.
IMMUNOLOGY EXPERT LEISHA EMENS IS STUDYING VACCINES FOR BREAST CANCER AND OVARIAN CANCER.
DANIEL LAHERU, CO-DIRECTOR OF THE SKIP VIRAGH CENTER FOR PANCREAS CANCER CLINICAL RESEARCH AND PATIENTCARE, IS HELPING LEAD THE WAY IN CANCER VACCINE THERAPY. HIS TARGET IS ONE OF THE DEADLIEST OF CANCERS.

THE SIDNEY KIMMEL COMPREHENSIVE CANCER CENTER at JOHNS HOPKINS 13
Immune Therapy Shows Promise for Breast Cancer
PRELIMINARY results of an early, multi-center study showed an experimentalimmune therapy drug was safe in patientswith metastatic, triple-negative breastcancer. These early findings offer newhope in the fight against this particularlyaggressive and difficult-to-treat disease.
The study involved 54 patients withadvanced triple-negative breast cancerfrom the Kimmel Cancer Center andother cancer centers. The patients received an experimental drug, known as a PD-1 blockade, designed to disrupt apathway that hides tumor cells from theimmune system.
“Early data in this trial show thatthe drug is generally safe and well-toler-ated, and it appears to be able to controldisease in some of these patients,” saysstudy leader Leisha Emens, M.D., Ph.D.“Now we’ll need to test it further in morepatients and compare it with standardtherapies to establish its therapeuticvalue.”
The drug binds to an immune-regu-lating protein known as PD-L1, disruptingan interaction between it and a relatedprotein known as PD-1, enabling an im-mune response against the cancer cells.The researchers determined that 37 ofthe 54 patients expressed the PD-L1 protein in some immune cells withintheir tumors, and 21 of these patients
were evaluated to assess the impact ofthe drug. Six patients survived at least 24 weeks without disease progression, an unusual result among patients withthis type of advanced and resistant cancer. Two patients saw their cancersdisappear, and tumors shrunk in another two patients.
Next steps include testing the drug’sbenefit in groups of patients and compar-ing it with standard treatments to deter-mine its therapeutic value. A large globalstudy to evaluate it as a possible standardtherapy is underway.
“Engaging the immune system tofight breast cancer is a game changer,”says Emens. “This is especially true fortriple-negative breast cancer, for whichchemotherapy is currently the only stan-dard treatment option outside of a clini-cal trial. Identifying a way to predictahead of treatment which patients aremore likely to respond is critically impor-tant, and there are ongoing efforts toidentify biomarkers for patients who aremore likely to respond to this therapy.”
ROISIN CONNOLLY, M.B.B.CH., WAS AWARDED A YOUNGINVESTIGATOR AWARD FROM THE NATIONAL COMPREHEN-SIVE CANCER NETWORK TO INVESTIGATE WHETHER THEIMMUNE SYSTEM CAN BE HARNESSED IN THE TREATMENTOF TRIPLE-NEGATIVE BREAST CANCER. TUMOR BIOPSIESAND BLOOD SAMPLES OBTAINED FROM PATIENTS WILL BE USED TO LEARN MORE ABOUT HOW THE IMMUNE SYSTEM ACTS IN PATIENTS WITH TRIPLE-NEGATIVE BREASTCANCER AND TO IDENTIFY BIOMARKERS THAT WILL HELPDISTINGUISH PATIENTS WHO WILL RESPOND BEST TOTHESE TREATMENTS.
He enrolled in a clinical trial designed and led by Elizabeth Jaffee andDung Le that is the centerpiece of aStand Up To Cancer pancreatic cancerdream team directed by Jaffee. It combines treatments with the vaccine-enhancing drug cyclophosphamide, theimmune-activating GVAX vaccine,mesothelin-targeting listeria, and theimmune checkpoint blockade with anti-PD-1. The pancreatic cancer GVAXvaccine was developed by Jaffee withViragh funding and is manufactured at a GMP facility in the Kimmel CancerCenter that she opened and directs.
The combined therapy represents aculmination of immunology laboratoryand clinical science, joining the strengthof several immune-targeted therapies inan attempt to topple one of the mostlethal cancers. Jaffee and Le hope thecombination will pack the immunepunch needed to break the resistance ofpancreatic cancer.
“I feel fortunate to be one of the 90 patients participating in this trial,”says Greco. Le says it’s too early in histreatment to measure the effect thetreatment is having on his cancer or toknow what the long-term impact will be.After his experience with chemotherapy,Greco says he is grateful for a treatmentthat doesn’t make him sick. “I feel likemyself again. I feel great. I swim every-day, and I’m still seeing patients. I feellike I’m cured.”
Then Came PD-1The first patients were treated with anti-PD-1 in 2006 as part of a small clinicaltrial led by Brahmer and funded byMedarex, now part of pharmaceuticalgiant Bristol- Myers Squibb. The scien-tific studies to better understand howanti-PD-1 was working were supportedby the Melanoma Research Alliance, theNational Cancer Institute, and facultysupport Susan Topalian received fromthe Kimmel Cancer Center and the Department of Surgery when she cameto Johns Hopkins.
Fast forward to 2015, and peoplewere getting very excited again about immunotherapy when the attention of

JONATHAN GRECO ISONE OF 90 PANCREATICCANCER PATIENTS PARTICIPATING IN A CLINICAL STUDY OF A VACCINE / ANTI-PD-1 COMBINATION.
THE SIDNEY KIMMEL COMPREHENSIVE CANCER CENTER at JOHNS HOPKINS 15
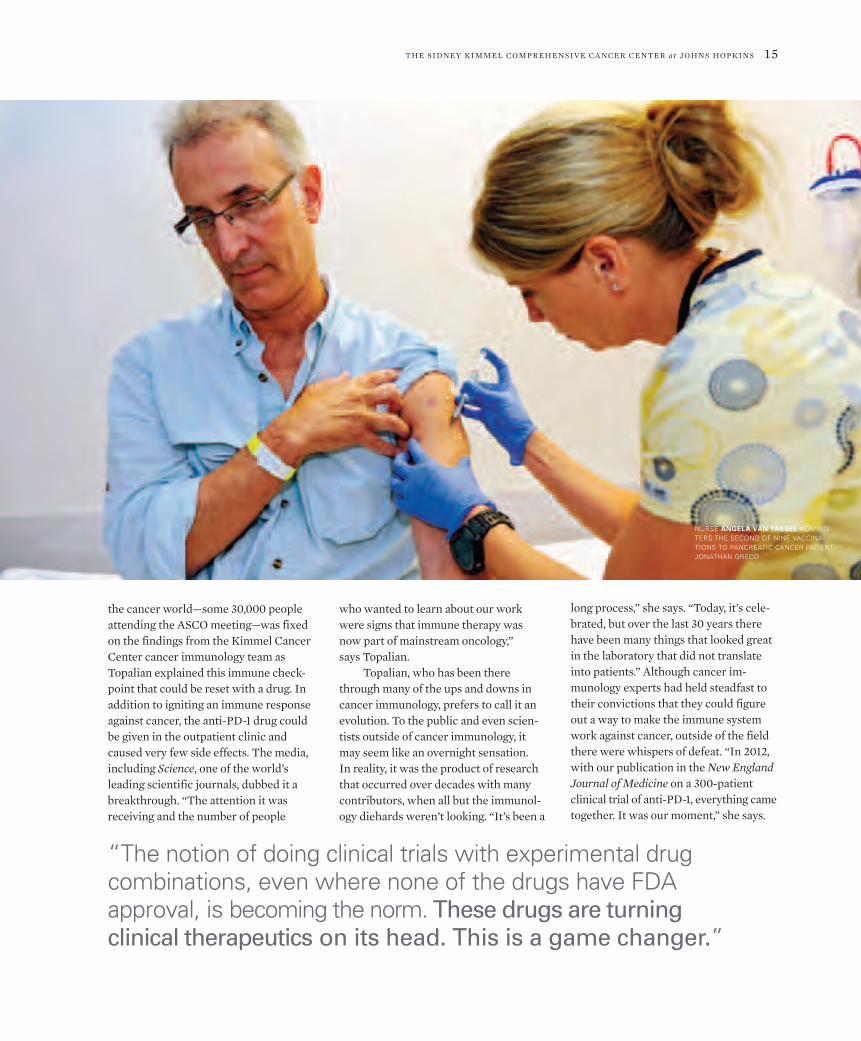
NURSE ANGELA VAN TASSEL ADMINIS-TERS THE SECOND OF NINE VACCINA-TIONS TO PANCREATIC CANCER PATIENTJONATHAN GRECO.
“The notion of doing clinical trials with experimental drug combinations, even where none of the drugs have FDA approval, is becoming the norm. These drugs are turning clinical therapeutics on its head. This is a game changer.”
the cancer world—some 30,000 peopleattending the ASCO meeting—was fixedon the findings from the Kimmel CancerCenter cancer immunology team asTopalian explained this immune check-point that could be reset with a drug. Inaddition to igniting an immune responseagainst cancer, the anti-PD-1 drug couldbe given in the outpatient clinic andcaused very few side effects. The media,including Science, one of the world’sleading scientific journals, dubbed it abreakthrough. “The attention it was receiving and the number of people
who wanted to learn about our workwere signs that immune therapy wasnow part of mainstream oncology,” says Topalian.
Topalian, who has been therethrough many of the ups and downs incancer immunology, prefers to call it anevolution. To the public and even scien-tists outside of cancer immunology, itmay seem like an overnight sensation. In reality, it was the product of researchthat occurred over decades with manycontributors, when all but the immunol-ogy diehards weren’t looking. “It’s been a
long process,” she says. “Today, it’s cele-brated, but over the last 30 years therehave been many things that looked greatin the laboratory that did not translateinto patients.” Although cancer im-munology experts had held steadfast totheir convictions that they could figureout a way to make the immune systemwork against cancer, outside of the fieldthere were whispers of defeat. “In 2012,with our publication in the New EnglandJournal of Medicine on a 300-patientclinical trial of anti-PD-1, everything cametogether. It was our moment,” she says.

16 PROMISE & PROGRESS
Immune Therapy forChildhood Cancers
WITH THEIR LOW toxicities, immunetherapies seem tailor-made for pediatriccancer patients where long-term effectscaused by conventional therapies are ofgreat concern. Childhood cancer patientscan suffer the consequences ofchemotherapy throughout their lifetime,including fertility issues, cardiac toxici-ties, learning impairment and more. Infact, many cancer immunology expertsbelieve immune therapies may be a para-digm changer, eventually replacingchemotherapy as the first-line treatmentin many pediatric cancers because of its ability to spare patients from thesedangerous toxicities.
Take, for example, Hodgkin’s lym-phoma. It is a common childhood cancerthat responds well to chemotherapy, but treatment is long and toxic, and thegrowing brains and bodies of childrenand adolescents are particularly susceptible to the damaging effects ofchemotherapy. New research showsHodgkin’s lymphoma may be one of thebest responders so far to anti-PD-1 im-mune checkpoint blockade therapy, withresponse rates approaching 90 percent.There have been excellent responses andlow toxicities even in patients whosecancer resisted standard drug treatment.
Researchers like pediatric oncolo-gists and cancer immunology expertsBrian Ladle andChristopher Gamper
say there is emerging evidence that im-mune therapies may be more effectiveagainst chemotherapy-resistant cancer.They offer new hope for pediatric pa-tients with cancers that currently cannotbe cured with standard treatments.
Ladle is excited about this less toxicapproach to destroying cancers. “It’s aprivilege to be able to cure kids of cancer,but right now, what we have to put themthrough to get them there is unaccept-able,” he says. “We have to do better forthem.”
While he doesn’t think immunetherapy will completely replace the needfor surgery and chemotherapy, he believes it has great potential to reducethe amount and duration of treatment.More importantly, since immune cellscan travel anywhere throughout thebody—inside bones and to organs and tissue—they have a unique ability to findand destroy lingering cancer cells thatoften result in the recurrence and spreadof cancers.
Ladle and Gamper are discoveringcrucial links between T cell behavior, the main cells activated in an immune response, and the epigenetic or chemicalenvironment of T cell DNA. Althoughthe DNA code of a T cell that has neverbeen activated is identical to that of Tcells engaged in an immune attack, sig-nificant changes occur in the chemicals
that surround the DNA that help signal itto remain dormant or go into action. As aresult, Ladle and Gamper are decipheringthe normal epigenetic activity of immuneT cells and exploring whether existingepigenetic-targeted treatments might beable to improve immune responses tocancer.
Ladle and Gamper believe epige-netic drugs may augment the effective-ness of other immune treatments, suchas cancer vaccines and immune check-point blockers. They are also looking forother proteins expressed by tumor cellsthat work like PD-1 to shut down an immune response to cancer. In addition,new pediatric oncology physician-scien-tist Nico Llosa is working on ways to usePD-1 blockade and other similar immuneagents to fight pediatric cancers.
While there have been significantadvances in cancer immune therapies inadults over the last few years, translatingthese findings to pediatric cancers lagsfar behind. “This is the main reason Iwanted to work in pediatric oncology,”says Ladle. “There is so much promise.We know that children’s immune systemsare much more responsive than adults’.”What Ladle envisions are treatments thatharness and deploy the body’s own natu-ral ability to fight cancer and decreasethe need for invasive surgeries and toxic,cell-poisoning drugs.
BRIAN LADLE CHRISTOPHER GAMPER

THE SIDNEY KIMMEL COMPREHENSIVE CANCER CENTER at JOHNS HOPKINS 17
Pioneering Patients
“I Don’t Feel Like I HaveCancer”Thomas Kotula, a patient with melanomabeing treated by Evan Lipson, is receivinga combination of two immune checkpointinhibitors, anti-PD-1 and anti-CTLA-4.He comes to the Kimmel Cancer Centerevery two weeks for the hourlong infusion.
“He was in pretty rough shape thefirst time I saw him,” says Lipson. Kotula’smelanoma had spread, including a soft-ball-size tumor in his thigh that made itdifficult to walk. By his third treatment,the tumors began to get smaller. A yearlater they have shrunk by more than half.The clinical trial he is on, headed bymelanoma expert William Sharfman,calls for two years of treatment.
“A major focus of our research in-volves understanding how to safely andeffectively use these new immune-basedmedications in as many patients as possi-ble,” says Lipson. “One of the potentialadvantages of immune therapy is that oncethe immune system is activated, it can keepcancer at bay for long periods of time.”
Kotula, a husband, father of six, andgrandfather of nine, says he came to theKimmel Cancer Center for a secondopinion at the encouragement of his chil-dren. His doctor at a community hospitalnear his home recommended surgery.Lipson had to deliver the bad news toKotula that surgery would be of littlevalue because the cancer had spread, buthe offered him an opportunity to partici-pate in Sharfman’s immune therapy trial.
Kotula has experienced relativelymild side effects from treatment, includ-ing a rash and some thyroid issues, says Lipson. He and his cancer immunology
collaborators are working to better un-derstand how to encourage the immunesystem to attack only tumors and leaveother parts of the body alone.
“He’s living his life,” says cancer immunology nurse Trish Brothers. “Immune therapy has offered real hope toMr. Kotula, both in terms of combating hiscancer and allowing him to avoid some ofthe debilitating side effects often associatedwith traditional cancer treatments.”
“I’m so glad I came here. I can’t sayenough about these doctors and nurses.They are like family,” says Kotula. “Whata difference from a year ago. I don’t evenfeel like I have cancer.”
GENE OGLE
THOMAS KOTULA (LEFT)AND EVAN LIPSON
“I Beat Pancreatic Cancer”When Gene Ogle’s doctor told him hehad pancreatic cancer, his first questionwas: “How long do I have to live?” Oglewas just 54 years old when he got the news,and his thoughts immediately turned tohis father, who died of the same disease30 years earlier at 63. Although manyyears had passed, his memory was clear.“My father died two months after he wasdiagnosed. My knowledge was that itwas incurable and killed quickly.”
Ogle’s doctor told him that there hadbeen many advances since his father’s diagnosis, and specifically referred todiscoveries at the Johns Hopkins KimmelCancer Center. He decided to make anappointment at its Skip Viragh Center forPancreas Cancer Clinical Research andPatient Care.
Despite the diagnosis, there wassome good news. His cancer was not asadvanced as his father’s, and he was acandidate for a Whipple procedure, acomplex pancreatic cancer surgery per-fected at Johns Hopkins. At the appoint-ment research nurse Carol Judkins also
talked to him about a clinical trial testingthe benefits of giving a pancreatic cancervaccine before surgery.
The pancreatic vaccine, developedby Elizabeth Jaffee, supercharged the immune system, drawing cancer-attackingkiller T cells to pancreatic tumors. Jaffeehad laboratory evidence that giving thevaccine before surgery gave the immunesystem a step up on the cancer and mighthelp it get at microscopic cancer cellsthat could cause the cancer to spread.She was working with two young clinicalinvestigators, Dung Le and Lei Zheng, to explore whether earlier use of the vac-cine would provide a clinical advantage.
Ogle was well aware of the high rateof pancreatic cancer spread and recur-rence. As an engineer, he is a numbersguy. He recalled a survival chart he sawaround the time of his surgery. “It peakedat one year and went down after that.Less than 5 percent of people survivedpast five years.” says Ogle.
“Enrolling in the vaccine trial wasan easy decision for me,” says Ogle. “Istill had no hope that I would survive,but I thought if I participated in the vaccine study, I might be able to helpdoctors move that survival curve far beyond five percent.”
That was nearly six years go, andcontrary to the statistics and his own per-sonal predictions, Ogle is alive and doingwell. It’s been almost four years since hisfinal vaccination. His cancer isn’t gone,but it’s not growing. With the boost fromthe vaccine, his immune system appearsto be keeping it in check. “I’m still here,and I want to be a message of hope toothers,” he says.
Ogle fully expected to become apancreatic statistic, but not a positiveone. “My perspective is changing,” hesays. He is certain the wonderful care hereceived, including surgery, chemotherapy,radiation therapy, and particularly thepancreatic cancer vaccine, allowed himto beat the odds. “I’m so proud to be apart of these studies. It’s a huge honor,”says Ogle. “Everyone who took care ofme—from the receptionist to the nursesand doctors—was top-notch. They allhad so much compassion.”

18 PROMISE & PROGRESS
tant events in their lives that he honestlymight not have otherwise lived to see,”says Drake.
On the other hand, there are can-cers, including prostate and pancreaticcancers, that remain largely resistant.“We need to address that on the researchside,” says Topalian. Drake does not get a good response in all bladder cancer pa-tients either. “In some patients, it worksquite well, but in others, the cancer con-tinues to grow,” he says. Understandingwhy some tumors do not respond is asimportant as learning why others do, hesays. “If we can figure out when it worksand how it works—what kinds of cells areinvolved and what is happening from animmunological standpoint—maybe wecan take non-responders and make themresponders,” Drake says.
There are currently about eight dif-ferent types of antibodies that block PD-1or PD-L1 on the market. The treatment isnow FDA-approved for melanoma andlung cancers, and Pardoll says approvalsfor kidney cancer, bladder cancer, andHodgkin’s lymphoma are anticipated bythe end of 2015 or early 2016. They aren’tcheap, costing about $100,000 or moreper year for each patient treated.
Although there have been many newsreports about the pricing of the drugs,immunology research nurseAlice Pons
and colleagues say pa-tients have not seemedconcerned about thecost. That could be be-cause some insurancecompanies are covering
them even before final FDA approval.Nurse practitioner and immunology expert Barbara Biedrzycki says other in-surance companies may resist approvingimmune therapy, requiring patients to firsttry less expensive drug therapies. To helpease the cost burden, the pharmaceuticalcompanies making anti-PD-1 drugs saythey have programs to provide free drugsfor patients who cannot afford them.
Immune therapies are outpatient treatments, and although there havebeen some serious side effects, in mostpatients they have so far proven to bevery safe. When hospitalizations, management of side effects, and the
A Milestone in Cancer MedicineRemarkable responses were occurring ina significant number of patients, puttingthe framework for a potentially broad-based treatment for cancer in place. Thisglimmer quickly ignited into a spark andcontinues to gain momentum as collabo-rations across many specialties at JohnsHopkins are expanding its benefit toother cancers.
This success revealed that the im-mune system could be employed againstcancers beyond melanoma and kidneycancer. As important, it provided defini-tive proof that there was a common forceat work to shut down an immune responseto cancer.
The most recent clinical study pro-vides clear evidence that for lung cancerpatients whose immune cells expressPD-1 or whose tumor cells express PD-L1,immune therapy works better than thebest chemotherapy drugs and with farfewer side effects. In addition, patientswith late-stage lung cancers frequentlybecome resistant to chemotherapy, butBrahmer says that patients who respondto immune therapy tend to continue responding. “In my 20 years in practice, Ihave never seen anything like this. We’rereporting three-year and more survivalrates in lung cancer patients who honestlywould not typically be around,” saysBrahmer. “This is truly a milestone incancer medicine.”
As for how long patients will continue to respond off treatment andwhether there are any long-term effectsof this type of immune therapy, it’s toosoon to know. Pardoll, Topalian and col-laborators are working to answer thesequestions. They also want to make senseof the varied responses. In some patients,tumors were held in check, neithergrowing nor shrinking. Other patients,like Ryan, experienced huge reductionsin the size of their tumors, but they didn’tgo away completely. Pardoll and Topalianhave gone back to the laboratory to betterunderstand the biology of these responses.In virtually all patients, however, the re-sponses appear to be long lasting. Somepatients from the original clinical studies
continue to do well. Such responses arevirtually unheard of in advanced cancers.“We don’t know yet what the ultimatesurvival benefit will be, but for these earlytrials and these patients, the responsesare lasting a long time,” says Pardoll. “We don’t have to intervene anymorewith therapy. The patients’ own immunesystems have taken over the battle.”
“It is a cyclical process,” says Topalian.“We need to continue working betweenthe laboratory and the clinic to advancethe science and understand more aboutresponses, how long the drugs need to be given, and how to make the treatmentwork in more patients.” To help gatherthese answers, she is turning to patholo-gists Anders, Taube, and Ed Gabrielson,who are uncovering the biomarkers, theunique cellular characteristics and signalsthat differentiate cancers that respond toanti-PD-1 from those that do not.
The list of responding cancers con-tinues to grow. Bladder cancer, Hodgkin’slymphoma and a few difficult-to-treatcancers, like triple-negative breast cancerand mesothelioma, are on it, with others,like certain ovarian, endometrial, colon,head and neck, stomach, liver, andesophageal cancers, expected to soon be added.
Drake tells of a patient referred tohim from fellow Greenberg Bladder Cancer Institute physician-scientistTrinity Bivalacqua. The patient was getting chemotherapy to shrink the sizeof his bladder cancer so that it could be removed with surgery. When Bivalacquaoperated, he found the cancer had alreadyspread. Surgery would not cure him, sohe left his bladder intact and referred thepatient to Drake.
The patient had lost his hair and was underweight from the chemotherapy, andnow it was no longer working. “He wasnot looking well when he came to see mein 2013,” says Drake. He recommendedimmune therapy with anti-PD-1. Almostimmediately, the patient regained his appetite and put some weight back onand reported just generally feeling better.Over time, his cancer shrank by 80 percent. His only side effect was a small,itchy rash on his shoulder. “He has threechildren and was able to witness impor-

THE SIDNEY KIMMEL COMPREHENSIVE CANCER CENTER at JOHNS HOPKINS 19
cost of drugs, are taken into consideration,Biedrzycki suspects the costs ofchemotherapy and immune therapy will become much more comparable.
With improved responses and lowertoxicities, which are clearly documentedin common cancers, such as non smallcell lung cancer, withholding immunetherapies from patients could intensifypublic ire aimed at the already batteredreputations of the pharmaceutical andinsurance industries.
“This research has completelychanged the slow, conservative approvalprocess for drugs,” says Pardoll. “Typicallyyou would have phase I and II clinicaltrials and then a big phase III trial, and ifa drug makes it all the way through, itgets approval.” Some of the anti-PD-1drugs are getting approved right out ofthe gate in phase I trials. “They havesuch remarkable therapeutic effects andlittle toxicity that we don’t need phaseIII studies. There is an obligation to getthe therapy to patients quickly,” he says.
Nelson says this is where Johns Hop-kins leadership in precision medicine
will play a leading role. The first anti-PD-1trials were open to all patients with advanced cancers that were resistant tostandard treatments, but as our scientistslearn more about what cancers respondand what cancers do not, they can beginto use biomarkers to identify the cancersand patients most likely to benefit fromimmune therapy. Pharmaceutical compa-nies have already begun developing bio-marker tests for PD-L1 based on the workof Anders and Taube that demonstratedPD-L1 expression was the best predictorof response to anti-PD-1 treatment. “PD-L1 on tumor cells is the cloak thatshields cancer from the immune system,”says Anders. “If the tumor is not express-ing PD-L1, it is not likely to respond to anti-PD-1 therapy.” Some clinical trialsalready require the biomarker test forPD-L1 before treatment, says Topalian.
At the same time, the cancer immunology team continues to work in the laboratory to find other immune“stop” signals and learn how to transformimmune therapy-resistant cancers intoresponsive cancers.
CANCER IMMUNOLOGY NURSING TEAM (LEFT TO RIGHT), BARB BIEDRZYCKI, ANGELA SCARDINA, BETH ONNERS,HOLLY KEMBERLING, MAUREEN BERG, SUSAN SARTORIUS-MERGENTHALER, KATRINA PURTELL, TIANNADAUSES, ANGIE VAN TASSEL, DENISE GALLAGHER, GALINA MELANCON, KATHY ELZA-BROWN
Expanding ResponsesOne of the ways cancer immunology experts are improving response is bycombining immune drugs. “The notionof doing clinical trials with experimentaldrug combinations, even where none ofthe drugs have FDA approval, is becom-ing the norm,” says Pardoll. “These drugsare turning clinical therapeutics on itshead,” he says. “This is a game changer.”
One of these combinations is anti-LAG-3 and anti-PD-1. LAG-3 was shownby Drake, Powell and others to shut downimmune responses to cancer cells, similarto PD-1. Unlike PD-1, however, inhibitingLAG-3 did not create the same robust response that occurred with anti-PD-1therapies. However, Drake found thatcombining two drugs—one that targetsPD-1 and another targeting LAG-3—worksin synergy to boost the immune responseagainst cancers. Combined approachesusing another checkpoint inhibitor knownas anti-CTLA-4 and anti-PD-1 drugs also have been studied, and Drake believesthat as more immune regulatory genesare identified, more combinations will be revealed.

20 PROMISE & PROGRESS
Micromanaging Colon Cancer
THERE IS A microscopic society livingwithin us. Our bodies are home to morethan 100 trillion microorganisms, morethan 10 times the number of human cellsin the body. Many of them reside in ourgut. Most of the time, this microsociety—which includes hundreds of species ofbacteria—and its human host coexist har-moniously. The “bugs” we live with aidin digestion, metabolism and immunity.
With such an overwhelming numbersadvantage, it may only take the activity ofa single organism to shift this harmoniousrelationship in a way that can promotecancer, says infectious disease expertCynthia Sears.
Of the trillions of possibilities, Searshas zeroed in on a population that appearsto be related to colon cancer development.
The entire colon is lined with a thickprotective layer of mucus, and, undernormal conditions, bacteria are excluded.In some colon cancers, however, Sears,researcher Christine Dejea, and teamhave found biofilms made up of a subsetof bacteria that has managed to invadethe mucus. “They invade the layer ofmucus that protects the epithelial cellslining the colon and upend the whole biology of the system,” says Sears.
With so many different forms ofbacteria colonized within the humanbody, it is a difficult task differentiatingthose that keep us healthy from thosethat contribute to disease. In this case,the association seems clear. The risk ofcolon cancer may be as much as five timesgreater in patients who have biofilms in their colons compared to those whohave none.
Sears doesn’t yet know how thesebiofilms develop, but she has a hunchabout their link to cancer. She speculatesthat they cause inflammation in the colon,which spurs genetic mutations that leadto cancer. “When we look at people whoundergo screening colonoscopy, we finda subset of people who have biofilms.
What happens in that tissue and cellsright under the biofilm, are the sameprocesses we see in cancer.” Anothermystery was related to the location of the biofilms. In her team’s study of 178surgery or colonoscopy patients treatedat either The Johns Hopkins Hospital orthe University of Malaya Medical Centrein Malaysia, the vast majority of biofilmswere located in the right colon. “It’s virtually a universal feature of tumorsthat appear in that section of the colon,although we don’t understand why,” says Sears.
To help answer some of these questions, Sears is working with cancerprevention and control expert ElizabethPlatz, cancer immunology expert DrewPardoll, and gastroenterologist FrancisGiardiello to establish a large multicentercolonoscopy study to define the naturalhistory of biofilms and their associationto changes in tissue. “When we detectbiofilms, where are they? How long dothey last, and what do they do? This iswhat we want to figure out,” says Sears.
The study will also establish a largebank of biofilm samples to integratecomplex microbial and immune analyses.“We want to understand how the immune
system responds to biofilms as well asthe gene expression of these bacterialcommunities and how they interact with other bacteria inside of the biofilm,”she says.
Biofilms are a new discovery, andSears and team are the first to systemati-cally explore them in colon cancer.
Patients with an inherited form ofcolon cancer, known as familial adeno-matous polyposis (FAP), may providesome early answers. The disease is char-acterized by large numbers of polyps inthe colon. Sears says FAP sufferers alsodevelop many biofilms, but instead ofbeing made up of many types of microor-ganisms, they primarily consist of twotypes of bacteria. “This is the best evidence so far that particular organismsmay be relevant, and it may help us zeroin on the bacteria that could be pushingthis process,” says Sears.
Among her long-term goals, Searshopes to use her findings to develop a non-invasive test to detect biofilms and predicta person’s risk of developing cancer. “Mostcolon cancers are known to develop slowlyover time,” she say. “It’s a disease that’scurable if diagnosed early, and maybebiofilms are an early warning sign.”
CYNTHIA SEARS

THE SIDNEY KIMMEL COMPREHENSIVE CANCER CENTER at JOHNS HOPKINS 21
“We know there are more check-points and that, in some cancers, wemight have to block more than one,” saysPowell. “Maybe in some patients, PD-1 isnot the relevant checkpoint, and we’llhave to find the one that is. In other can-cers, we may have to block more than onecheckpoint because both are relevant.”
Powell and colleagues are also havingsuccess using anti-PD-1 in combinationwith a drug that interferes with metabo-lism of cancer cells. Tumors kill by grow-ing, and they require nutrients—lots ofthem—to sustain this growth. Blockingcell pathways that enable this growth
by providing amino acids, glucose, andlipids that nourish tumor cells can havean antitumor effect.
“We think tumor cell metabolismcan be considered a kind of immunecheckpoint because it creates an environ-ment that turns off the immune response,”says Powell. Surprisingly, blocking thesenutrients is cancer specific. All cells neednutrients, but normal cells don’t requirethe extraordinarily high levels demandedby rapidly dividing cancer cells. “To be areally good cancer cell, it needs a hugeamount of these nutrients,” he says. Cutting off the biological supply line of
these nutrients slows the growth of cancer cells without harming normalcells. Adding a checkpoint blocker likeanti-PD-1 allows the immune system tosweep in and finish the job on the weak-ened cancer cells.
Powell is also studying a group offailed Parkinson’s disease drugs that target a pathway known as adenosinethat acts as an on/off switch for immuneT cells. Studies in Powell’s laboratoryfound that the drugs were remarkablyproficient at instigating an immune response against cancer cells. The drugshave already been studied in patients
“I have never seen anything like this. We’re reporting three-yearand more survival rates in lung cancer patients who honestlywould not typically be around. This is truly a milestone in cancer medicine.”
SUZANNE TOPALIAN

22 PROMISE & PROGRESS
with Parkinson’s disease and proved safe,so with funding, he hopes to be able tobring them to clinical trials for patientswith cancer in less than a year.
These new combinations will not be limited to immune agents. Animal research by radiation oncology fellow Andrew Sharabi and Drake found thatfocused radiation treatment, like thatused in radiosurgery, stimulates an immune response against the cancer.Sharabi says cell damage caused by radia-tion deploys immune cells to the tumorsite, and combining anti-PD-1 with radio-surgery unleashes an immune assault onthe cancer. “Radiation opens the door,and anti-PD-1 therapy allows the immunecells to get to work,” says Sharabi.
Radiation oncologist Joseph Herman,Anders, and Taube find evidence that radiosurgery may be activating immunecells in pancreatic cancer as well, a cancerthat currently does not respond well toanti-PD-1 treatment. Combining radio-surgery with the right immune-targeteddrugs may increase responses in a varietyof cancers. Anders is examining tumorsthat are traditionally treated with radia-tion, including head and neck cancersand esophageal cancers to look for expression of PD-L1 in tumor cells, an indicator that they might respond to ananti-PD-1 checkpoint blockade/radiationtherapy combination.
JOSEPH HERMAN
THE ROAD TO CANCER IMMUNITY “IF A CAR IS SITTING AT THE TOP OF A HILL WITH THE FRONT POINTING DOWNHILL, ITMAY ONLY NEED THE PARKING BRAKE RELEASED TO START MOVING. ANOTHER CAR SITTING ON A FLAT ROAD MAY NEEDTHE BRAKE RELEASED AND A PUSH TO GET GOING. A CAR SITTING AT THE BOTTOM OF A HILL AND FACING UPHILL WILLNEED THE BRAKE RELEASED AND A LOT OF GAS TO GET MOVING,” SAYS DREW PARDOLL.
Pardoll and Topalian are hopefulthat combination therapies may be thekey to converting currently nonrespond-ing cancers like prostate cancer into responders. Similar to Sharabi andDrake’s work, Topalian believes that giving another kind of therapy up front,including radiation, chemotherapy ortargeted therapies, and following withanti-PD-1 could provoke an immune response in currently resistant cancers.
She is working in her laboratory tosee what therapies incite an inflammatoryresponse in the tumor, because inflam-mation draws the attention of immune
cells. These are the situations whereadding anti-PD-1 has the potential tocause a synergistic immune response.She and others are compiling this labora-tory evidence. This component is critical,she says. “There are endless possibilitiesof potential treatment combinations. We can’t test them all, and we can’t simply do combinations of convenience,”says Topalian. “We have to let the research lead us, and then move to theclinic only with combinations supportedby scientific evidence.”
Some cancers will respond to anti-PD-1, but others will need more to getthe immune system working. Pardoll isconfident that working together overtime Johns Hopkins experts will be ableto figure out the right combinations toget the immune therapy moving againstalmost any cancer.
The Learning CurveWith Ryan’s cancer stable—no longershrinking, but not growing either—Brahmer has decided to stop anti-PD-1treatment. “We think that over time the immune system creates a memory.The T-cell remembers how to attack the cancer and stop the cancer fromshielding itself from the immune cells.We think the immune system can keepthe cancer under control now, even without treatment,” says Brahmer.

THE SIDNEY KIMMEL COMPREHENSIVE CANCER CENTER at JOHNS HOPKINS 23
“I feel like this is about more than just me. Immune therapysaved my life, and I want to bring this message of hope to others. I know how fortunate I was to have this wonderful teamof doctors and nurses at Johns Hopkins. They are my heroes.”
If Ryan’s cancer begins to grow, shewill start therapy again. Other patientswhose tumors began to grow again afteranti-PD-1 treatment was stopped haveresponded with treatment that wasreinitiated. It’s all part of the learningcurve. Ryan continues his regular tripsfrom his home near Middleburg, Virginia, to the Kimmel Cancer Centerto have his cancer monitored. He alsoparticipates in a Stand Up To Cancer-funded study providing blood samplesthat help researchers understand moreabout how immune checkpoint blockadetherapy works against cancer. Not everypatient whose immune cells expressPD-1 or whose tumor cells express PD-L1 respond to immune therapy. Patients like Ryan are helping investi-gators solve those mysteries and leadingthem to ways to help more patients.
“I feel like this is about more thanjust me,” says Ryan. “Immune therapysaved my life, and I want to bring thismessage of hope to others. I know howfortunate I was to have this wonderfulteam of doctors and nurses at JohnsHopkins. They are my heroes,” he says.“Two years ago, in a very short period oftime, I went from feeling fine to beingin serious trouble. I thought I mighthave only months to live and that Iwould miss so many important momentsin my children’s lives. Time was critical,and I was fortunate to get in the righthands quickly.”
Today, Ryan says, he feels better thanhe has in years. He recently providedaround-the-clock logistical support as acrew chief to his son as he participated in a grueling 100-mile ultra-marathonthrough the Vermont mountains. “Myfriends and family were worried when Itold them I planned to do this. They wereshocked by how much energy I had.”
Pardoll sees the therapy as a truebreakthrough in cancer medicine. This is not just hyperbole; he actually did the math. With 14 different cancer types responding at rates of between 15 and 40 percent, early studies in Hodgkin’slymphoma reporting response rates ofnearly 90 percent, and enduring cancerremissions, immune checkpoint block-ade therapy has distinguished itself fromchemotherapy and gene-targeted thera-pies. “By a factor of 30,” he says, “anti-PD-1 is the most powerful single agent in the history of cancer therapeutics.”
Another Road Leads to PD-1Forty years ago as efforts to decipher thecauses and cures for cancer intensified,many began looking to the laboratories of the fledgling cancer center at JohnsHopkins. From the beginning, the National Cancer Institute had named it a center of excellence. Among the mainareas of research were laboratories focused on immunology, genetics, andepigenetics. One of them, experts hoped,would lead to a discovery that would
JOHN RYAN

developed a model for cancer initiationand progression that became the paradigmfor much of modern cancer research.
Pardoll continued to pursue cancer immunology, in part inspired by themonthly meetings with Coffey. With hisand Vogelstein’s encouragement, he soonjoined the faculty and started his owncancer immunology laboratory. But thatwas not the end of the Vogelstein/Pardoll collaboration. As Vogelstein focused on the cancer genome, Pardollbegan to explore the genetic mechanismsof immune cells. Neither anticipated anintersection of the two laboratories thatwould lead to an unusual discovery.
“This kind of collaboration is whatmakes us Hopkins,” says Vogelstein.“People share their ideas and results here.Drew [Pardoll] and Suzanne [Topalian]showed us what they found and askedfor our ideas.”
Pardoll and Topalian were trying tofigure out why one of the first colon cancerpatients ever treated with anti-PD-1 hada complete response—with no detectabletumor six years later—but another 32colon cancer patients did not respond.They hoped that the Vogelstein team’sexpertise in colon cancer could shedlight on what was unique about that patient and maybe what they learned
could be used to turn the tide of strikinglypoor responses for that disease. “We werehappy to share any of our research thatcould help,” says Vogelstein. “It’s all donein the service of patients. There is no discussion of the usual academic kinds ofthings. We don’t do that in the KimmelCancer Center.”
The Mystery of the Single Responder Cancer is a disease of genetic mistakes, sofor all intents and purposes, the signalssent out by mutated genes should be anannouncement to the immune systemthat they don’t belong. “Ironically, thisvery mechanism that the tumor uses toaccelerate its genetic diversity creates anAchilles heel for immunotherapy,” saysLuis Diaz, investigator in the KimmelCancer Center’s Ludwig Center. Themore mutations that exist in the cancer,the louder the signal and the more likely it is that the immune system willtake notice.
TOP: IN 1977, BERT VOGELSTEIN, (RIGHT) A YOUNG SCIENTISTCONCENTRATING ON THE NEARLY IMPOSSIBLE TASK OFCRACKING CANCER’S GENETIC CODE, AND DREW PARDOLL,(CENTER) HIS GRADUATE STUDENT AT THE TIME, METMONTHLY WITH SENIOR CANCER RESEARCHER DONALDCOFFEY (LEFT) TO TOSS AROUND IDEAS ABOUT HOW TOCURE CANCER. BOTTOM: SOME 35 YEARS LATER, THE RESEARCH TRIO IS STILL COLLABORATING.
conquer cancer. No one, including Pardoll,ever imagined the interconnection ofthese three areas of research or that itwould result in some of the most signifi-cant cancer discoveries of our time.
In 1977, Bert Vogelstein, a youngscientist concentrating on the nearly im-possible task of cracking cancer’s geneticcode, and Pardoll, his graduate student atthe time, met monthly with senior cancerresearcher Donald Coffey to toss aroundideas about how to cure cancer. Ideaswere about all anyone had at that time.Coffey remains an iconic figure at theKimmel Cancer Center. The consummateteacher with an enthralling Southerndrawl challenged talented young investi-gators then—as he continues to do today—to work together and look for creative solutions to a tough problem. Usually,they would talk casually over tea. Eventhen, the immune system was on theirshort list of ideas. Vogelstein continuedto pursue genetics, convinced it wouldyield greater insights into the cellularprocesses that result in cancer.
Vogelstein, the Clayton Professor of Oncology and co-director of the KimmelCancer Center’s Ludwig Center, went on to define cancer as a genetic disease.Starting with colon cancer, he, KennethKinzler, and their Ludwig Center team
24 PROMISE & PROGRESS
DREW PARDOLL

THE SIDNEY KIMMEL COMPREHENSIVE CANCER CENTER at JOHNS HOPKINS 25
Healing Cancer
BIOMEDICAL ENGINEER JenniferElisseeff was working on a way to pro-mote healing in trauma patients when a friend of a cancer patient visiting Elisseeff’s lab told her that similar ap-proaches were reported to fight cancer.
A few years later, Elisseeff began re-search that promised to bridge the fieldsof immunology and biomedical engineer-ing. She called the emerging field regen-erative immunology. It led her to a newuse for her trauma-targeted therapy.
Elisseeff works with biologically en-gineered animal and tumor tissues thatare implanted locally at the site of an in-jury. “The immune system is a first re-sponder when trauma to tissue and cellsoccur,” says Elisseeff, the Jules Stein Professor in the Translational Tissue Engineering Center. Her engineered biologic materials give it an extra nudge.“They trigger immune cells, particularlyT cells, to direct other immune cells toheal the injury,” she says.
Elisseeff and team are collaboratingwith the U.S. military to study in people,including servicemen and women injured in combat, the safety and activity of her biomaterials. The engineered materials are made in the Kimmel Cancer Center’s GMP facility. If humanstudies are successful, it creates a frame-work for eventually transferring thetechnology to an experimental clinicaltrial for cancer patients.
The first step was to test the ostensi-ble cancer fighting potential in her labo-ratory. Elisseeff injected her biomaterialsin mice engrafted with human melanomaskin cancer cells, and it hampered thegrowth of the cancer. “We’ve looked atthe lymph nodes near the injection siteand lymph nodes in other parts of thebody and have identified immune changesdirectly related to the biomaterials,” shesays. These observations indicated thatthe treatment has the ability to chasedown cancer cells that have broken offfrom the primary tumor and spread toother parts of the body.
Just as important, Elisseeff andteam’s findings challenge the commonperception that regenerative medicine iscancer promoting. “This has been a nag-ging concern in our field, but we’ve neveractually seen it occur,” she says. “Our research provides evidence that this maynot be a concern.”
The promising anticancer activity inanimal models occurred using biomateri-als alone. Elisseeff says adding immunetherapies, such as anti-PD1 blockades,may make it work even better. To findout she is collaborating with cancer im-munology experts Drew Pardoll andJonathan Powell, who have worked with her to establish this fledgling fieldof regenerative immunology.
Elisseeff met Pardoll when theyworked together on Johns Hopkins Uni-versity President Ronald Daniels’ innova-tion hub committee aimed at promotinginnovation translation to bring life-changing technologies to market. It ledto the current collaboration focused oncombined biomaterials/immune therapyanimal and clinical studies, and Powell ishelping decipher the biologic mechanisms.He has provided laboratory models thatreveal the specific immune T cells essen-tial to the healing immune response.
“This is the first therapeutic model,”says Elisseeff. “No one has ever beforebridged the fields of immune-engineeringand regeneration.”
She says they have only begun toscratch the surface of this new type oftherapy and admits there is much theyneed to learn. Still, early findings point tothe therapy she has created as a way toheal both wounds and disease. A patientundergoing cancer surgery could havethe biologic material injected during theoperation to promote healing of the sur-gical wound and to simultaneously gen-erate a cancer-fighting immune response.
Nanoparticle TherapyGene therapy may be an effective treat-ment option for the deadly brain cancerglioma, but getting the right genes tocancer cells in the brain has proven diffi-cult. Now, for the first time, Johns Hop-kins researchers used biodegradablenanoparticles filled with genes to turn an inactive prodrug into a potent braincancer cell killer. The nanoparticles, encoding a special gene, were injectedinto brain tumors in rats and followed by treatment with the drug ganciclovir. The treatment successfully killed cancercells and extended survival in this animalmodel.
“Our nanoparticles penetrated com-pletely throughout the tumor following asingle injection,” says biomedical engineerJordan Green. “When combined withsystematic administration of ganciclovir,rats with malignant glioma lived signifi-cantly longer than rats that did not receive treatment.”
Nanoparticles are ultra tiny struc-tures that are about 20 times larger thana molecule but 100 times smaller than acell, so they can be loaded with genesand small molecules, including immunetherapies, and guide and deploy thesetherapeutics inside cells. These nanopar-ticles are able to penetrate tumors anddeliver immune-system-activating drugsand antibodies that cause immune cellsto specifically attack cancer cells. Thistype of therapy kills cancer cells more effectively and with far few side effects.
On the Web: READ MORE ABOUT THE KIMMEL CANCER CENTER’S COLLABORATIONS WITH THEENGINEERING EXPERTS IN OUR SPECIAL ISSUE OF PROMISE & PROGRESS , ENGINEERING CURES

26 PROMISE & PROGRESS
immune system should work, ignoringthose things that are “self” and noticingthose things that are different. This iscalled immune recognition; the next stepis action. That’s the role of anti-PD-1,which works by shutting down the can-cer cell’s ability to send false signals tocommandeer and divert immune cellsfrom reacting. With anti-PD-1, the immunecells alerted by the high number of genemutations were put into action to killcancer cells.
“For other treatments, includingchemotherapy, the changing tumor biology due to accumulating mutationscauses treatments to stop working, but itseems to make immune therapies workbetter,” says Le. It’s likely more about thequantity of mutations than the specifictype of mutation. The investigators be-lieve the good responses to anti-PD-1that occur in a subset of melanoma andlung cancers are also related to the accu-mulating gene mutations caused by sunexposure in melanoma and smoking inlung cancer. “In theory, you only needone mutation to get the immune system’sattention, but larger numbers of mutations,shift the odds in your favor,” he says.
The only way to prove the hypothesis
Kinzler, and Papadopoulos developed atest for mismatch repair gene mutations,so that families with a history of Lynchsyndrome could be screened and theircolon cancers detected in an early and curable stage.
They could have never envisionedthe clinical application that Diaz and another young immunology investigator,Dung Le, would have for the test. Itwould prove instrumental. “What is thepatient’s mismatch repair status?” Diazasked Pardoll and Topalian about the single colon cancer responder. Using thetest Vogelstein, Kinzler, and Papadopoulosdeveloped two decades earlier, theyproved their suspicion was spot on. Thepatient’s tumor was positive for mismatchrepair alterations. The large number ofmutations common to mismatch repairserved as an alert to immune cells becausethey make the tumor look much moredifferent from normal colon cells thatdon’t have this large number of mutations.
Imagine a crowd of people in aroom. If one person is speaking a lan-guage different from the rest, it might go unnoticed. If many of them are speakinga different language, it will likely garnerattention. In principle, this is the way the
So it was not surprising when KimmelCancer Center investigators, includingDiaz, had an idea. “It’s mutations,” theysuggested, suspecting that the single patient who responded to anti-PD-1treatment had Lynch Syndrome, an inherited form of colon cancer character-ized by abnormally large numbers of mutations.
The research that formed the basisfor their conclusion occurred some 20years earlier, remarkably from the sameLudwigCenter laboratory. In 1993, Vogel-stein, Kinzler, andNickolas Papadopoulosof the Kimmel Cancer Center and Albertde la Chapelle from The Ohio State University identified a genetic alterationlinked to Lynch syndrome, a hereditaryform of colon cancer that is caused bymistakes in mismatch repair genes.
The job of mismatch repair is to correct copying errors that occur whenDNA replicates and cells divide. Peoplewho inherit a defective copy of the geneexperience high rates of mutations andare at increased risk of developing coloncancer. Colon cancers in patients withmismatch repair deficiency have morethan 1,000 mutations while those withouttypically have less than 100. Vogelstein,
LUIS DIAZ (LEFT ), AND DUNG LE (RIGHT ) ARE TWO OF THE YOUNG RISINGSTARS OF THE KIMMEL CANCER CENTER. LE IS A VIRAGH SCHOLAR FOCUSEDON IMMUNOLOGY AND PANCREATIC CANCER VACCINES, AND DIAZ IS A GICANCER AND GENETICS EXPERT AND DIRECTOR OF THE SWIM ACROSSAMERICA LABORATORY.

THE SIDNEY KIMMEL COMPREHENSIVE CANCER CENTER at JOHNS HOPKINS 27
“Immune therapy is a game changer. We need more researchto take us the rest of the distance, but we don’t think there is asingle cancer that the patient’s own immune system ultimatelycan’t beat.”
mistakes—including some rare, difficult-to-treat cancers—and the treatmentworked. “If you have the mismatch repair signature, you should be treatedwith a checkpoint inhibitor,” says Diaz.“Defects in mismatch repair genes arefound in a small percentage of many can-cer types,” says Le. Vogelstein estimatesthat 2 to 4 percent of all cancers havemismatch repair mistakes, and when thatis calculated across every cancer type,the potential to help a lot of people is veryreal. Le believes that similar biomarkersfor immunotherapy response could beapplied to cancers with errors in otherDNA repair genes.
“There is a tsunami coming,” saysAnders, who believes the mismatch repairtest is the first of many that will be usedto predict response to immune therapy.
This is what excites Diaz and Le.They witnessed it firsthand, and Diazbrims with enthusiasm when he speaksparticularly of two young patients whowere part of the clinical study.
Stephanie Joho, who has Lynch syn-drome, had just graduated from collegewhen she was diagnosed with colon can-cer. Surgery and two different types ofchemotherapy did nothing to avert theaggressive cancer. Out of options and in excruciating pain, Joho searched desperately for other treatments and had reached out to Diaz, who until themismatch repair discovery had triedeverything available. Recognizing Johowould be a perfect candidate for his newstudy, he called her. She was distraught,sitting in a waiting room at another com-prehensive cancer center after one morefailed search for an experimental therapy,when she got Diaz’s call. “Come downhere. We’ll cure you,” he told her. Aftertreatment with anti-PD-1, Joho’s tumor
was to test it in patients, but these trialsare expensive and a huge undertaking foryoung investigators. Diaz and Le wereundeterred. Merck agreed to donate thedrug, but it was the generosity of privatefunders—Swim Across America, theLustgarten Foundation, the Skip ViraghFoundation, the Banyan Gate Foundation,the Commonwealth Fund, and the SolGoldman Pancreatic Cancer ResearchCenter—that allowed Diaz and Le to makeit happen.
Le and Diaz are two of the youngrising stars of the Kimmel Cancer Center.Le is a Viragh Scholar focused on im-munology and pancreatic cancer vaccines,and Diaz is a GI cancer and genetics expert and director of the Swim AcrossAmerica Laboratory. The balance of cancer genetics/cancer immunology expertise each brought to the table wasperfectly suited to this study.
“The success of the Kimmel CancerCenter is inextricably tied to our abilityto attract the best and brightest talent,”says Nelson. “This trial is an example ofthe depth of talent we have in our younginvestigators. Unfortunately, as thisstudy illustrates, it can be a challenge forthem to find funding for their sciencebecause they may not yet have a largebody of work or the notoriety of moresenior investigators. It is one of thegreatest shortcomings in research but apriority at the Kimmel Cancer Center. It was our benefactor Sidney Kimmel’svision—a vision he brought to lifethrough the Kimmel Scholars Program—and vitally important to the future ofcancer medicine.”
With funding in place and the drugacquired, Le and Diaz began a clinicaltrial in 48 patients. Le, the more subduedof the research duo, speaks calmly and
straightforwardly about the significanceof their findings. Even before accrual tothe study was completed, the results
were so dramatic thatthey were viewed as amajor finding, warrant-ing publication in theprestigious New Eng-land Journal of Medicinein 2015, featured at theAmerican Society of
Clinical Oncology, and setting the stage forFDA breakthrough status for anti-PD-1immune therapy in patients with mis-match repair deficiency.
Roughly 60 percent of patients withmismatch repair deficiencies respondedto treatment, pointing to the presence ofother checkpoint blockades that worksimilarly to PD-1. This will be the focusof additional laboratory research. As crit-ical of a finding, however, was that noneof the 25 patients with normal mismatchrepair responded to treatment. The investigators will need to replicate theirfindings in a larger number of patients, butit provides clear evidence that mismatchrepair alterations in tumors predictswhich patients are good candidates forimmune therapy with anti-PD-1.
Additional laboratory research atthe Kimmel Cancer Center has pointedto other immune checkpoints in these tumors, which could be targeted in com-bination with anti-PD-1. Frank Housseauand pediatric cancer expert Nico Llosafound high expression of LAG-3 in mismatch repair deficient tumors.
Beyond colon cancer, the clinicalstudy demonstrated that mismatch repair deficiency is a universal biomarkerof response to immune therapy. Theytested the treatment in a small number ofother cancers marked by mismatch repair
NICO LLOSA
28 PROMISE & PROGRESS
“Throughout my career as a clinician and scientist and nowas cancer center director, I cannot recall another timewhen so many opportunitieswere within our grasp.”
—William Nelson, DirectorSidney Kimmel ComprehensiveCancer Center at Johns Hopkins

THE SIDNEY KIMMEL COMPREHENSIVE CANCER CENTER at JOHNS HOPKINS 29
shrank, and her pain subsided. “I haven’tfelt this well in four years,” says Joho,now 25.
Another patient was weeks fromdying and being encouraged to enter hos-pice care when Diaz and Le learned histumor was positive for mismatch repair.He was so sick that they had to get a spe-cial exception to get him enrolled in thetrial. “Without any doubt, this youngman’s life was saved by this treatment,”says Diaz.
Diaz recalls more patients. “Wecould fill this room with people who havebenefited,” says Diaz. The two recognizetheir study was small, and in science,numbers matter. Still, they have metevery one of the patients in their study,and they also recognize that medicine ismore than numbers. Behind every statis-tic is a human being.
“It is rare to get a response in coloncancer patients who have not respondedto other standard therapies, and most ofthem had just months to live,” says Le.She is hopeful this discovery will verysoon benefit thousands, but nonetheless,at this moment, they celebrate Joho andthe 20 other lives that were saved.
“One of the things that put us at theforefront of clinical breakthroughs incancer immunology is that we never for-got the science,” says Pardoll. “Havingthe leading epigenetics and genetics researchers here gives us an edge. At mostinstitutions, the different laboratoriesdon’t interact at all. At Johns Hopkins,interaction among different disciplines is the norm, and these types of collabora-tions have led to some exciting immunol-ogy advances. There is no other place I know of with these deep, intellectualroots in genetics and immunology andthe support of the institution to carry outinvestigator-initiated trials,” says Vogel-stein. “You can’t create that environmentfrom scratch. It has to be built in from
the ground up, and we’re very fortunateto have it here.”
“Dung and I are standing on theshoulders of many giants,” says Diaz.
The Epigenetic ConnectionA number of the controls that turn theimmune system on and off are epigeneticin nature. These chemically mediated onand off switches alter the function ofgenes without mutating the DNA, usuallyby adding chemical groups to the signal-ing portion of genes or by tightening orrelaxing how the DNA is packaged withinthe cell. Epigenetic therapies that targetthese control mechanisms, can reactivategenes that have been turned off.
Stephen Baylin is one of the world’sforemost epigenetics experts. He, Vogel-stein, and Pardoll have independently in-formed some of the most vexing problemsof cancer initiation, spread, and treatmentresistance. Their combined knowledge is the cancer world’s triple threat. By deci-phering the inter-related complexities ofgenetics, epigenetics, and immunology,they are bringing forth some of the mostencouraging cancer treatment strategies of our time.
As Baylin explored the effects ofepigenetic-targeted drugs on lung cancer
cells in his laboratory, he found thatsome of the genes that were being reacti-vated were connected to immune re-sponses. Among them was PD-L1 whichinteracts with a key molecule on immunecells, PD-1.
Baylin and young investigator Cynthia Zahnow,working with him aspart of the Stand Up To CancerEpigeneticsDream Team, shared their findings withPardoll. In some lung cancer cells, thePD-L1 gene was already active, and epigenetic therapy made its signal evenstronger. Pardoll believed that addinganti-PD-1 therapy in conjunction withepigenetic therapy could activate an im-mune response right within the tumor.
Treated with epigenetic drugs, the ability of cancer cells to evade the immune system is broken and they sendnew signals, beckoning immune cells tocome and get them. At the same time,they begin to express PD-L1 to shieldagainst immune attack. Anti-PD-1 breaksoff that communication, unleashing theimmune system on the cancer cells.
Baylin, Zahnow, and team wentback to the laboratory to decipher theimmune evasion signature for lung,breast, colon, and ovarian cancers. To do this, they looked at all of the genes inlung, breast, and ovarian cancers that got turned on in cancer cells with epige-netic-targeted therapies. Lots of geneswere switched on, they found, but whatstood out were the 20 percent or so related to immune regulation. These
By deciphering the inter-related complexities of genetics, epigenetics, and immunology, they are bringing forth some of themost encouraging cancer treatment strategies of our time.
STEPHEN BAYLIN
CYNTHIA ZAHNOW

30 PROMISE & PROGRESS
genes were studied in depth by post-doc-toral fellow Kate Chiappinelli and foundto be epigenetically programmed toevade detection by the immune system.
They are now looking at tumor sam-ples from patients receiving combinedepigenetic and anti-PD-1 immune therapy to see if the epigenetic therapyturned on immune genes that wouldcause the cancer cells to respond to anti-PD-1 treatment. “Epigenetic therapydoes not break immune tolerance, but ithas the potential to sensitize cancers toan immune anti-PD-1 checkpoint block-ade treatment,” says Baylin. “We think it brings in immune cells, so if we followit with anti-PD-1, we can cause an im-mune reaction against cancer cells.” Thistheory is currently being studied in clini-cal trials funded by Stand Up To Cancer.
Baylin continued his research ofepigenetic controls of immune response,collaborating with another epigeneticsresearch giant, Peter Jones, director ofresearch at the Van Andel Institute.Working together as co-leaders of theStand Up To Cancer Epigenetics DreamTeam, they uncovered a viral defensemechanism in tumors that mimics a viralinfection. Epigenetic drugs cause it tosimulate an infection and summon im-mune cells to tumors.
“Epigenetic drugs upregulate the viral defense pathway, activating interferon signaling, and this brings in immune cells,” says Chiappinelli.“When epigenetic therapy is followed by anti-PD-1 checkpoint blockade immunetherapy, the immune cells go into actionagainst the cancer.”
The viral defense pathway is an an-cient human biological mechanism thatallows cells to recognize when they havebeen infected by a virus and helps acti-vate an immune response to the viral in-vader. Our DNA retain a record of ourviral exposure, creating a history that be-comes integrated into the genome. Thisviral record is rendered dormant throughepigenetic signaling, but as Baylin andChiappinelli found, it can be reactivatedwhen epigenetic-targeted therapies aregiven. Since it reactivates just a memoryof viruses, it only mimics an infection intumor cells, but fake infection is enoughto generate an immune response.
When they examined the DNA of a variety of cancer types, including ovariancancer, colon cancer, and melanoma, theyfound that tumors with high expression ofthe viral defense pathway were morelikely to respond to immune therapy withanti-PD-1. Tumors with low viral defenseexpression could be coaxed into responseif epigenetic-targeted drugs were givenbefore immune therapy. The FDA-ap-proved epigenetic drug 5-azacityidine(Aza) converted low viral defense expression to high expression.
“Our research findings are consistentwith the previous notion that silencingviral sequences in the human genome isa major function controlled epigeneti-cally,” says Baylin. Using drugs like Azato remove the epigenetic controls that silence the noninfectious viral memorylocked away within tumor cells activatesinterferon, a signal to the immune sys-tem released by cells when they are in-vaded by bacteria or viruses. In essence,
Aza makes tumor cells think they are infected with a virus and causes them tosound the alarm to alert the immune system. In laboratory experiments whereBaylin and Chiappinelli blocked inter-feron in tumor cells, the Aza-induced immune response stopped.
To further test their theory, the twocollaborated with experts at MemorialSloan Kettering Cancer Center in NewYork to examine cancer cells frommelanoma patients treated with anti-CTLA-4, another checkpoint blockadeimmune therapy similar to anti-PD-1.They determined the viral defense pathway expression for each tumor andmatched it back to the patients. High viraldefense expression matched with all ofthe patients who responded to immunetherapy, and low expression matched with those who did not respond.
In a mouse model of melanoma,adding an epigenetic drug to cancers thatwere not responding to immune check-point blockade triggered an immune response. Baylin says the true test willcome from clinical studies, but he is energized by these laboratory results.
“This is the most exciting time ofmy entire career,” says Baylin. “KimmelCancer Center scientists have made sem-inal contributions to the basic science, andnow what is happening is almost magical aswe make the unbelievable transformationto harness the immune system to attacktumors. Our latest findings further decipher the mechanisms that lead tothis immune reaction and offer a novelway to potentially boost the success ofimmune therapies in cancer patients.”
“Kimmel Cancer Center scientists have made seminal contribu-tions to the basic science, and now what is happening is almost magical as we make the unbelievable transformation to harness the immune system to attack tumors. Our latestfindings further decipher the mechanisms that lead to this immune reaction and offer a novel way to potentially boost thesuccess of immune therapies in cancer patients.”

THE SIDNEY KIMMEL COMPREHENSIVE CANCER CENTER at JOHNS HOPKINS 31
Baylin, like all of the Kimmel CancerCenter researchers and clinicians whoheld firm to their belief in immune therapy, is most excited by the safe anddurable responses it delivers.
“Many people still view cancer as aterminal disease, particularly advancedcancers, and look what we have to putpatients through to treat them,” saysBaylin. “Immunotherapy promises tochange that. It’s already made a huge difference. We have patients now who,against all odds, are alive and living well even when we have not completelyeliminated their cancer. I can only imag-ine what the next 10 years will bring. You have to be excited about this.”
Whispers of a CureThese combined approaches are thenewest adaptation of cancer immunologytherapies. Pardoll, Topalian, Drake, Jaffeeand their immunology teams are opti-mistic that the power of immune therapyand the right combinations will continueto expand the numbers of cancer pa-tients who will see their immune systems engaged against their cancers. For thefirst time in the history of cancer, expertsand patients alike are beginning to see in immune therapy, the potential for a universal cure for cancer.
Through the convergence of awealth of expertise, the advancement of
technology and in an environment wherebench-to-bedside research flourishes,Kimmel Cancer Center experts havesolved the puzzle of cancer immune resistance, or at least they have identifiedmany of the pieces. The critical compo-nent—immune resistance, how the can-cer cell escapes an immune attack—wasrevealed and therapies to undo cancer’sability to manipulate the immune cells toits own benefit can now be developed.
“The success we have had so far isunlike anything we have ever seen incancer, and consider that we have onlymined about 5 percent of what the im-mune system can do in cancer. This isjust the beginning,” says Pardoll. “As welearn about other immune signals andcombined approaches, we think it willonly start to look better. In 20 years, possibly less, immune therapy has thepromise to completely change the face of cancer and make almost all cancerscurable or controllable.”
Patients, even those who are notcurrently on immune therapy, seem tosense the changing tide, says veteran immunology nurse practitioner TiannaDauses. “Every day, we get calls fromcancer patients who want to come to the Kimmel Cancer Center for immunetherapy. Current patients, including manywho are on other types of therapies, express the hopefulness they feel from
being at a cancer center that is engaged inthis kind of paradigm-shifting research.”Her immunology nursing colleagues con-cur. “I’ve worked in oncology for a longtime. It’s an exciting time to see these newtherapies that work in the worst cancersand don’t cause terrible side effects,” saysresearch nurse Beth Onners. “One of thefirst questions I typically get from patientsis, ’Will it make my hair fall out? It’s sonice to be able to tell them it won’t.”
The patients who were on chemo-therapy before treatments like anti-PD-1were discovered say they feel likechemotherapy kept them alive, but immune therapy gave them their livesback, says Biedrzycki. “It is so exciting to be a part of this,” she says.
After decades of research, it is the patients that matter most to the KimmelCancer Center immunology researchersand clinicians. It is not seeing their scientific theories proven correct thatthey finds most gratifying. The real sat-isfaction, they say, comes from seeingthese scientific theories actually helppatients and without the terrible side ef-fects that have defined cancer treatmentfor decades. “Immune therapy is a gamechanger,” says Pardoll. “We needmore re-search to take us the rest of the distance,but we don’t think there is a single cancer that the patient’s own immunesystem ultimately can’t beat.”•
CYNTHIA ZAHNOW AND STEPHEN BAYLIN