identifying the characteristics of optimum practice: findings from a survey of practice experts in...
TRANSCRIPT
Journal of Advanced Nursing, 1995,22, 24-32
Identifying the characteristics of optimumpractice: findings from a survey of practiceexperts in nursing, midwifery and health visiting
Tony Butterworth PhD MSc RGN RMN RNT DipNQueens Nursmg Institute Professor of Community Nursmg, The University ofManchester, Manchester
and Veronica Bishop PbD MPbil RGNNursmg Officer, NHSE and Professor of Nursing, Anglia Polytechnic University,Chelmsford, Essex, England
Accepted for publication 28 September 1994
BUTTERWORTH T & BISHOP V (1995) Journal of Advanced Nursing 22, 24-32Identifying the characteristics of optimuin practice* findings from a survey ofpractice experts in nursmg, midwifery and health visitingIn a questionnaire survey m England of 1221 practising nurses, midwives andhealth visitors, 18 key characteristics of optimum practice, made up from 77sub-Item categories, were identified by respondents Five open-ended questionsasked respondents to consider various aspects of optimum practice and tocomment on factors which encouraged those m practice to deliver care of thehighest quality Consensus of view was obtained through a Delphi approachThe researchers offer commentary on the implications of this research forcommissioners, providers and the professions and suggest action for thoseconcerned with the provision of health care
TNTTRnnTIPTTniVr '^ ^^ Umted Kingdom, clmical areas which demon-strate positive characteristics have been designated as
The need for information to estahlish and maintain opti- nursing development units They have been supported bymum practice in nursing, midwifery sind health visiting is central funding initiatives and reported widely (Vaughanof paramount importance in the development and main- 1992) There are also likely to be other centres where worktenance of high quality care The reasons for this are many, of the highest quality from nurses, midwives and healthnot least the 'flattened' professional management struc- visitors is to he found hut will have gone unreported Withtures and the introduction of an internal market system increasing demeuids for attention to issues of quality andwhich has forced renewed attention on the practice settmg clinical leadership it is important to describe those mattersGaptured in a senes of policy target statements in the docu- which enable centres to carry out nursmg, midwifery andment A Vision for the Future (NHSME 1993), it is sug- health visiting which is of the highest standard Glearly,gested that optimum practice is linked with matters of quality and
standards of careprofessional leaders should be able to demonstrate the existence ~, , i. , , > , . . , , ., , r , , The interpretations ot quality identified by Attree
of networks for sharing good practice , „, , i , , , , , ,(1993) are held to be central to this research In her review
and that of the literature Attree suggests that excellence, ldealness,, , , . . . , , , , , , fitness for purpose and conforming to standards, meeting
providers should be able to demonstrate three areas where chmcal , ,. , ,, , , „ , the customers requirements, satisfying need and customer
practice has changed as a result of research findings , i i n 7 i r. i i i . , . ^value could all be identified, but she notes the lack of
Correspondence Professor T Buttenvorth, Tbe School of Nursmg Stud.es clarity and the Conceptual COnfusiOn whlch SUrrounds theUmversity of Manchester, Coupland 3 Building Oxford Road Manchester debate ahout Standards, lSSUes of quality Care and whatM13 9PL England could be defined as optimum practice
24 © 1995 Blackwell Science Ltd

Charactenstics of optimum practice
The research
The research descnbed in this paper also has roots in per-sonal attnbution (Kitson 1986) and matters of structure(Taylor & Haussman 1991) It seeks to inform the pro-fession further about those matters which are seen asimportant by those in practice
The complex nature of nuismg, midwifery and healthvisiting does not make description an easy task However,there are research methods available which can provideimportant insights This is an account of one such exerciseWhile the document A Vision for the Future (NHSME 1993)set an agenda for the professions, and the subsequent docu-ment Targeting Practice The Contribution of Nurses, Mid-wives and Health Visitors (Department of Health 1993)earned this forward by describing examples of good prac-tice, the research descnbed m this paper presents the viewsof chmcally active and expert nurses, midvnves and healthvisitors on what constitutes and supports good practice
AIMS OF THE RESEARCH
The research was funded by the Department of Health,England, and took place over a 12-month period
The agreed aims of the research project were
1 to provide intelligence on those matters which establish,maintain and develop optimum practice m nursing,midwifery and health visiting, and
2 to gather information from, and generate correspon-dence between, expert nurses, midwives and healthvisitors
It was agreed that these questions should be addressed tonurses, midwives and health visitors in practice
DEVELOPING THE METHODOLOGY
The task of generating discussion, achieving agreementand consequently making policy decisions which canclaim to represent the view of a professional group,IS methodologically difficult Delphi survey researchattempts to overcome some of these problems and wasselected as the method of choice for this exercise TheDelphi research technique was developed as a method-ological response to counter those problems identified mgetting collective opinions from expert groups It is a wayof eliciting and refining the opimons of a group of peoplewho, in practice, are usually experts or knowledgeableindividuals m the substantive area of interest
The advantages claimed (Linstone & Turoff 1975) for tbetechnique over other ways of elicitmg judgemental datainclude its ability to reduce the tendency to 'follow theleader' and its ability to lessen the bandwagon effect,common m group settings It allows 'experts' who have nohistory of communicating to do so It reduces, or ehmm-
ates completely, the possibility of a dominant personalitycontrolhng the outcome of the group, produces a threat-free environment for an individual to state a personal opi-mon and provides a communication structure m whicheveryone has a chance to be heard equally
In common with all research methods, the DelphiTechnique has limitations eind these (see Sadonan 1975,Goodman 1986) are acknowledged The method does notclaim to cover unexpected, spectacular and unanticipatedbreakthroughs or to remove the uncertamty of the future
There are examples of this technique being used by earl-ier researchers for the purpose of definmg matters relatedto nursmg and midwifery practice Farrell & Shearer (1983)used the Delphi techmque to explore indicators of qualitynursmg care Four major groups were selected to representthe nursing population administrators, educators,researchers and clinical nurses From this, nurses gave opi-nions on what constituted quality nursing care Bond &Bond (1982) used a Delphi research method to identifyclinical nursing research priorities In work for the EnglishNational Board for Nursmg, Midwifery and Health Visiting(ENB 1993), researchers at the University of Manchesterused the method to determine views on educationalexpenences vnth community nurses
There are examples where Delphi research has beenused to gather an informed view on likely developmentsm psychiatnc nursing m the United Kingdom (White1991), nursing m Europe (Butterworth 1991), nursing edu-cation (Crotty 1993) and the role of front line managers(Duffield 1993)
THE PROGRAMME OF RESEARCH
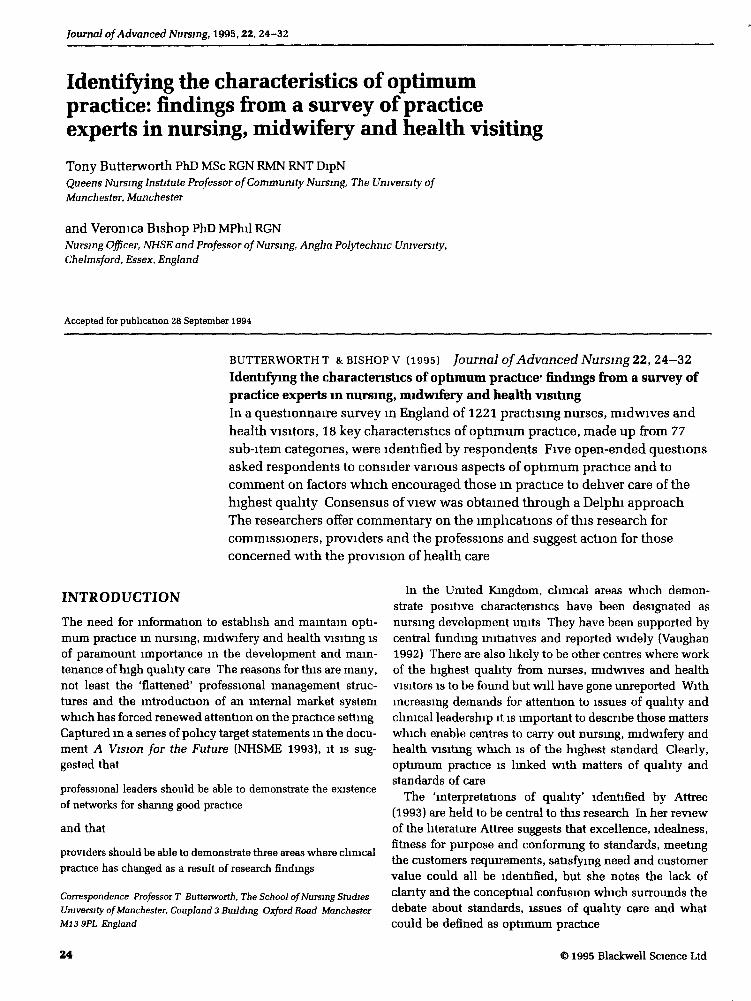
The research took the following fairly typical sequence ofseven steps The timetable is shown m Figure 1
1 A panel of methodology and practice experts was estab-lished This group (group A) identified the key questionsto be asked and considered how to derive and then com-municate with a panel of expert respondents (group B)
AprilJuly
AugustSeptemberOctoberNovemberJanuary
July
Establishment of the methods group |1 Establishment ofthe expert respondent group
First questionnaire to expert group
1 Analysis of data from round 1
Second questionnaire to expert group
1 Analysis of data from round 2
1 May 1
Third communication to expert group
1Final data analysis and presentationof fmdings to Department of Health
Figure 1 The timetable of research
© 1995 Blackwell Science Ltd, Journal of Advanced Nursing, Z2, 24-32 25
T Butterworth and V Bishop
2 The first round questionnaire was given to the expertrespondent group (group B)
3 Data from the first questionnaire were analysed and thenconsidered by group A A second questionnaire wasdeveloped
4 The second questionnaire was given to the expertrespondent group (group B)
5 Data from the second questionnaire were analysed andthen considered by group A No third questionnaire wasdeveloped as a high meetsure of agreement had beenreached
6 A third communication was sent to the expert respon-dent group (group B)
7 A draft report was produced
The expert methodology group (group A)
This group consisted of methodology and subject expertsand was facilitated by the Department of Health Member-ship of the group can be found at the end of this paper
The expert respondent group (group B)
The methodology group debated ways of locatmg a groupof experts who could parbcipate in the research exerciseFollowmg investigation, three possible avenues for gather-mg respondents were explored the live Register of theUnited Kingdom Central Council for Nursing, Midwiferyand Health Visiting (UKGG), the Department of Health(DOH), England, and the English National Board forNursmg, Midwifery and Health Visiting (ENB) These pos-sibilities were rejected as their databases were either toodifficult to sample, or focused on an inappropriate groupof respondents
It was agreed that expert nurse, midwife and heedth visi-tor respondents could be identified through nurse advisorsfor each providing authority in England All regional nurseadvisors m regional health authorities m England werecontacted by letter and the names of nurse executives forall provider units were obtained Four hundred and forty-one nurse executives were identified Each of these wassent a letter and requested to supply the names of up tofive nurses, midwives or health visitors who
1 had at least 5 years clinical experience and were cur-rently m clinical practice,
2 had a post within the clmical grading structure of F, G,or H or, exceptionally, were clinical specicJists atgrade I, and
3 were nurses, midwives or health visitors whom thenurse advisors could descnbe as skilled clinicians ofFer-mg optimum care
These criteria were established so that those involvedwith clmical activity on a day-to-day basis would be at theheart of the study Inevitably, respondents were drawn
from a group which, m the judgement of the nurse execu-tives, consisted of practitioners whom they beheved to beboth expert and offering optimum care The selection wastherefore subject to the biases and limitations that thisimposes The response rate from nurse executives reached89% and they named 2006 nurses, midwives or healthvisitors who fulfilled the necessary criteria and could becategorized as suitable respondents
The nurses, midwives and health visitors as a'sample'
National figures for nurses, midwives and health visitorsm England have been supplied by the statistics and man-agement division ofthe Department of Health m order thatthe respondent group csm be seen m the context of work-force figures (Table 1) This mformation has limited useful-ness m that it mcludes some commimity nurses withoutspecific preparation and does not always discmmnatebetween level one and level two nurses Also, numbers ofschool nurses emd practice nurses cannot be qusuitifiedeasily from existing DOH data sets
Nurses, midwives and health visitors identified for thissurvey by provider authority nurse executives cannot beseen m the context of these data, as the study asked forparticular characteristics in the respondent groupNonetheless it is helpful to consider overall numbers memployment It is important to note that the expert respon-dent group cannot be considered as a representative strati-fied sample of nurses, midwives and health visitors memployment m England Equally they will not be a pro-portionate group mirronng nationed figures The commonal-ity that they share rests solely with criteria set out m thequestionnaire to nurse advisors m providing authonties
Designing questions for the expert respondentgroup
The expert methodology group considered construction ofa first questionnaire A first version was locally pilotedand refined and a final version was sent to the identified
Table 1 Whole time equivalent qualified staff m employment
District nursesHealth visitorsMidwivesCommumty midwivesCommunity mental handicap nursesMental handicap nursesCommunity psychiatnc niu:sesMental illnessChildren's nursesAdult general nursesTotal
1980012 07015660
42001580
301503600
5317010 550
161030311810
26 © 1995 Blackwell Science Ltd, Journal of Advanced Nursing, 22, 24-32
Charactensttcs of optimum practice
expert respondent group The questioruiEtire asked a senesof questions to establish the characteristics of the res-pondent group, followed by five open-ended questionsRespondents were asked to give an opinion on each Theopen-ended questions were
1 What IS It ahout your care that has led one of yourmanagers to consider you as someone who providesoptimum/best practice'
2 How would you describe optunum/best practice'3 What facihtates optimum/best practice in the place
where you work'4 If you were starting from the beginnuig and creating a
centre providing optimum/best nursing practice, whatingredients would need to be present'
5 Are there any further comments you may have aboutoptimum/best practice'
The expert respondent group and their willingnessto participate
The 2006 nurses identified by nurse executives becamethe expert respondent group and received the first ques-tionnaire After a period of 3 weeks non-respondersreceived a reminder letter and a second copy of the ques-tionnaire, 1221 members replied to the questionnairewhich meant a response rate of 61% This can be con-sidered a respectable response rate for a questionnairesurvey but is lower than some other surveys A sample ofnon-responders was contacted by telephone to try anddetermine their reasons for non-completion It was vari-ously ascnbed to pressures of work and the considerablechanges being introduced by managers There were somecomplaints of questionnaire fatigue produced by other sur-veys and the constant demand for information
The project did not allow time to pursue another cohortof respondents and a decision was made to proceed withthe group who had replied
ANALYSIS OF THE FIRST QUESTIONNAIRE
The characteristics of expert respondents
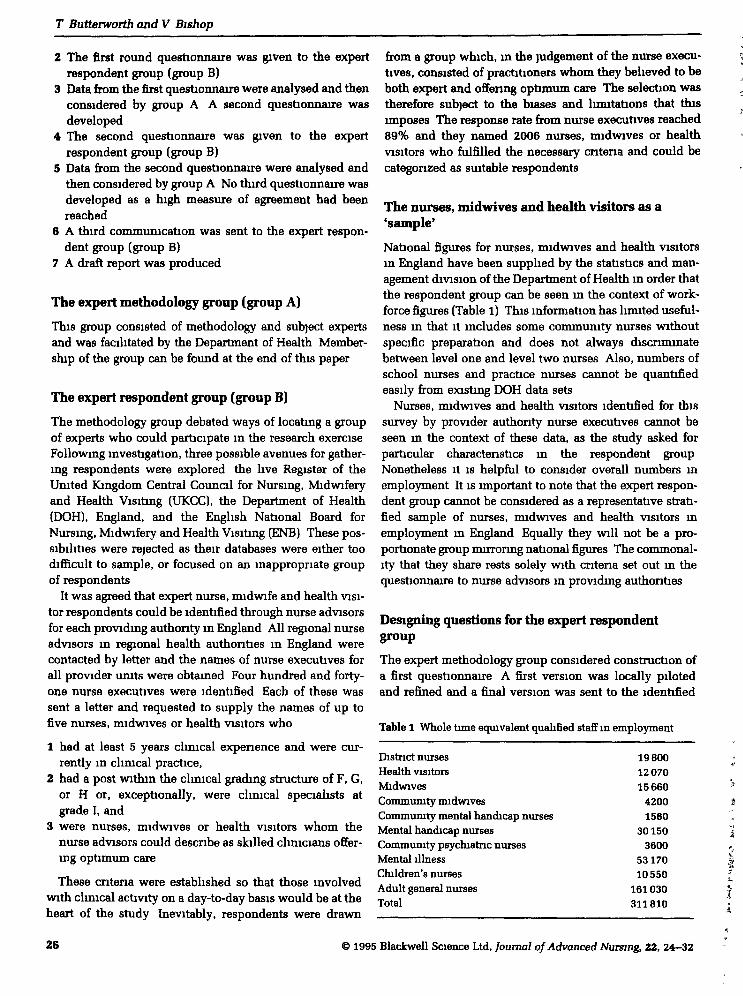
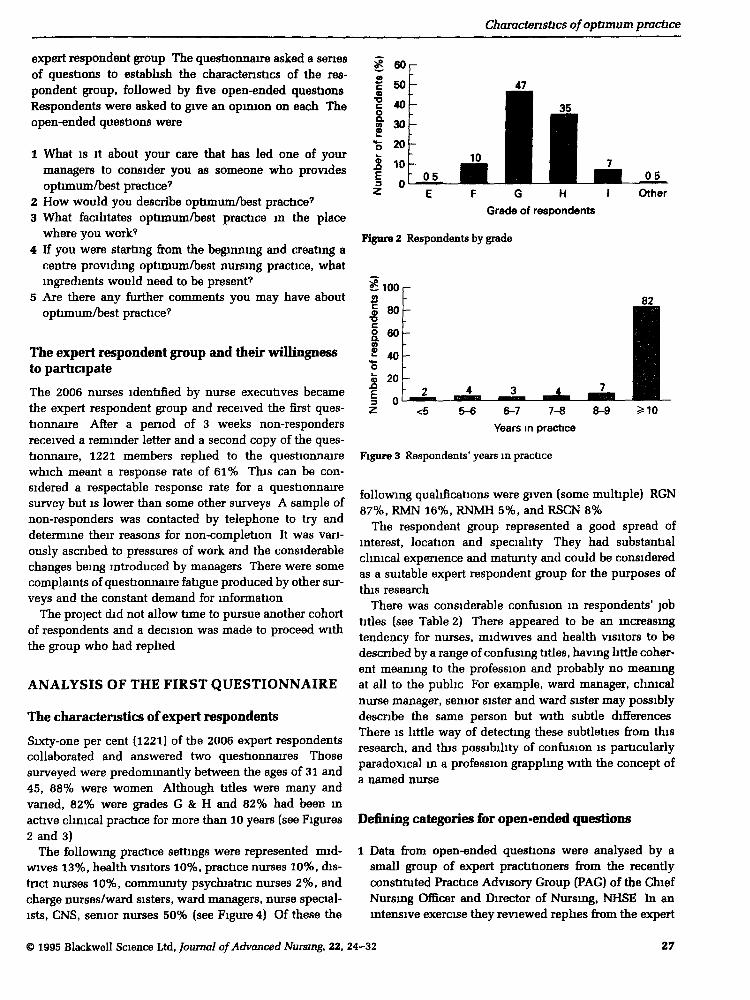
Sixty-one per cent (1221) of the 2006 expert respondentscollaborated and answered two questionnaires Thosesurveyed were predominantly between the ages of 31 and45, 88% were women Although titles were many andvaried, 82% were grades G & H and 82% had been mactive clinical practice for more than 10 years (see Figures2 and 3)
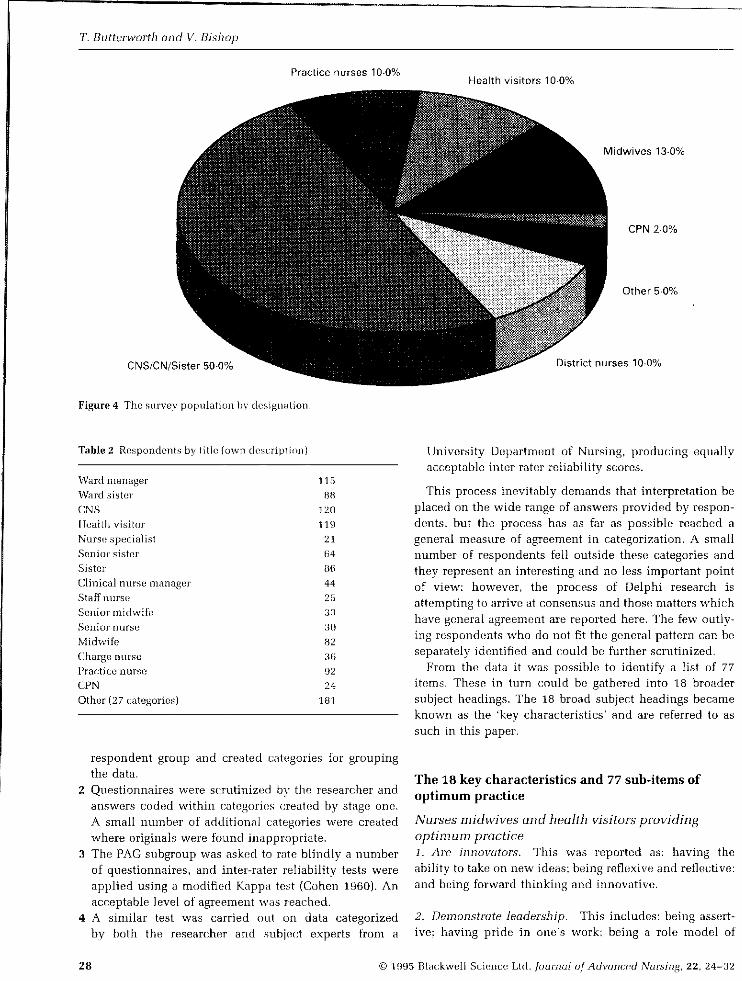
The following practice settings were represented mid-wives 13%, health visitors 10%, practice nurses 10%, dis-tnct nurses 10%, community psychiatric nurses 2%, andcharge nurses/ward sisters, ward managers, nurse special-ists, CNS, semor nurses 50% (see Figure 4) Of these the
a?
onde
nts
1
jmb
er o
f r
z
60
50
40
30
20
10nU
-
-
-
- 05
E
10
F
^M 35• •1 ^H ^H ^ ^
G H 1
Grade of respondents
05
Other
Figure 2 Respondents by grade
82
6-7 7-8 8-9Years in practice
Figure 3 Respondents' years in practice
following qualifications were given (some multiple) RGN87%, RMN 16%, RNMH 5%, and RSCN 8%
The respondent group represented a good spread ofinterest, location and speciality They had substantialclinical experience and maturity and could be consideredas a suitable expert respondent group for the purposes ofthis research
There was considerable confusion m respondents' jobtitles (see Table 2) There appeared to be an increasingtendency for nurses, midwives and health visitors to bedescribed by a range of confusing titles, having httle coher-ent meaning to the profession and probably no meaningat all to the public For example, ward manager, clinicalnurse manager, senior sister and ward sister may possiblydescribe the same person but with subtle differencesThere is httle way of detecting these subtleties firom thisresearch, and this possibility of confusion is particularlyparadoxical m a profession grappling with the concept ofa named nurse
Defining categories for open-ended questions
1 Data from open-ended questions were analysed by asmall group of expert practitioners from the recentlyconstituted Practice Advisory Group (PAG) of the ChiefNursing Officer and Director of Nursmg, NHSE In anintensive exercise they reviewed rephes from the expert
© 1995 Blackwell Science Ltd, Journal of Advanced Nursing, 22, 24-32 27
T. Butt^rworth and V. Bishop
Practice nurses 10-0%Health visitors 10-0%
Midwives 13-0%
CNS/CN/Sister50-0%
Figure 4 The survey population by desigiuition.
CPN 20%
Other 5-0%
District nurses 10-0%
Table 2 Respondents by litlc (iiwn
Ward managerWard .siHtcirCNSHealth visitorNurse .speciaiistSenior sisterSisterClinical nurse managerStaiT nurseSenior midwifeSenior nurseMidwifeCharge nursePractice nurseCPNOther (27 categories)
115
BH
120
119
21
64
86
44
25
33
30
82
36
92
24
181
respondent groLip and created uategories for groupingthe data.
2 Questionnaires were scrutinized hy the researcher andanswers coded within categories created by stage one.A small number of additional categories were createdwhere originals were found ijiappropriate.
3 The PAG subgroup was asked to rate blindly a numberof questionnaires, and inter-rater reliability tests wereapplied using a modified Kappa test (Cohen 1960). Anacceptable level of agreement was reached.
4 A similar test was carried out on data categorizedby both the researcher and .subject experts from a
University Department of Nursing, producing equallyacceptable inter-rater reliability scores.
This process inevitably demands that interpretation beplaced on the wide range of answers provided by respon-dents, but the process has as far as possible reached ageneral measure of agreement in categorization. A smallnumber of respondents fell outside these categories andthey represent an interesting and no less important pointof view; however, the process of Delphi research isattempting to arrive at consensus and those matters whichhave general agreement are reported here. The few outly-ing respondents who do not fit the general pattern can beseparately identified and could be further scrutinized.
From tbe data it was possible to identify a list of 77items, Tbese in turn could be gathered into 18 broadersubject headings. Tbe 18 broad subject headings becameknown as the 'key characteristics' and are referred to assuch In this paper.
The 18 key characteristics and 77 suh-items ofoptimum practice
Nurses midwives and health visitors providingoptimum practice1. Are innovators. This was reported as: having theability to take on new ideas; being reflexive and reflective:and being forwai'd thinking and innovative.
2. Demonstrate leadership. This includes: being as.sert-ive; having pride in one's work; being a role model of
28 © 1995 Blac:kweli Si:ienct! Ltd. Journcil of Advancpd Nursing, 22, 24-32
Charactenstics of optimum practice
leadership, giving respect to colleagues, and being forwardthinking
3 Have key personal qualities Key personal qualitiesLacluded having a positive attitude, keeping calm underpressure, giving attention to detail, being approachable,and giving commitment
4 Can demonstrate positive communication skills Thiswas descnbed as bemg able to give tune, bemg skilled inwritten euid verbal commumcation, bemg an available andinformed source for expert mformation, and having anability to commumcate effectively in a multi-disciplmaryteam
5 Can demonstrate expertise This was defLaed ashaving a broad experience which allows the demonstrationof expert practice, having competence, being up to date,being a model of expert practice, and bemg able to teachadvanced practice skills to other nurses
6 Are able to work in a multi-disciphnary team Thiswas expressed through being able to share work with otherdisciplines, articulating and makmg an equal effort to teameffort, having a clearly stated role, and being able to givemutual respect to other colleagues
Requirements for optimum practice7 A supportive environment for clinical activity and per-sonal development This is achieved by having an activemodel of clinical supervision, being able to give andreceive support, bemg able to give and receive criticism,encouraging peer review, and providing mentorship fornew staff
8 Management which allows its development and givesit support This IS expressed through managementwhich respects optimum practice and shows this throughactive support, allows support to be returned from thosem practice, encourages involvement m decision making,and allows practitioners to take responsibility
9 Active involvement with education This is achievedby providing the opportunity to be a teaching resourcefor students, active involvement with centres of edu-cation, bemg a provider of ln-service education, and pro-vidmg expenence for students undertaking clmicalexperience
10 Active involvement m patient teaching/educationActive involvement was characterized by providingknowledge to patients/clients, makmg opportumty forhealth education and heedth promotion, bemg an expertsource of knowledge, and active involvement with teach-mg patients and chents
11 That standards be set and issues of quality beaddressed This is shown through mvolvement with set-ting standards, havmg and using protocols, being mvolvedwith quality imtiatives, and being aware of the scope ofprofessional practice available to nurses
12 Political awareness This is obtamed throughknowledge of influential groups and mdividuals at a locallevel and national level, and by bemg able to debate andpersuade withm a multi-disciplmary setting
13 A need to be aware of and involved m researchactivity This requires access to appropriate hbrarymaterials, being able to use theory in practice, enablingresearch in practice, and using research findmgs as a basefor, and to change, practice
Requirements fornurses, midwives and healthvisitors to provide optimum practice14 Suitable service support This is expressed throughreasonable clerical support, having an appropriately struc-tured skill mix, and having well-designed information sys-tems that provide mtelligent and useable data
15 The right milieu This is achieved by creatmg anatmosphere which is conducive to givmg nursing, mid-wifery or health visitmg care and allows both carers andpabents/clients a sense of ownership, having some controlover the throughput of patients/clients, and nurses, mid-wives and health visitors pla3nLng a part in devismg theexpectations of service delivery
16 Careful attention from the human support servicesThis IS effected through careful staff selection processes,regular motivational support, frequent, well-nm staff meet-mgs, suitable staffing levels, and support from emd supportfor managers
17 User involvement and chent/patient ownership ThisIS expressed through preserving patient/client dignity,acting to sustain patient/client advocacy, giving openaccess to service-specific mformation, encouraging con-sumer feedback, and encouraging patient/client-heldrecords
18 To work within a system of holistic care Thismvolves individualized patient/client care, care based ona system of pnmary nursing, care which has well-orgamzed discharge planmng, and contmmty of care
THE SECOND QUESTIONNAIRE ANDOBTAINING CONSENSUS
FoUowmg analysis of the first questionnaire, a secondquestionnaire was developed and sent to the expert
© 1995 Blackwell Science Ltd, Joumal ofAdvanced Nursing, 22, 24.-32 29

T Butterworth and V Bishop
respondent group in order to ascertain a measure of con-sensus on the defined characteristics Expert respondentswere presented with a questionnaire showing the categor-ies which had been developed and were asked to give eacha measure of agreement or disagreement by using a 5-pomtLikert scale
Duffield (1993) reports on a Delphi study, giving particu-lar attention to the requirements for consensus This wasequally important m this study, which reached a strongmeasure of agreement The data in this research demon-strate that all categones were seen to have a measure ofagreement which fell mto either the 'totally agree' or'agree' elements of the scale While this does not imply acomplete measure of consensus, most respondents wereable to agree with the categones m 29 cases and totallyagree m 48 These data indicate 'good enough' agreementand there seemed little pomt in attempting further agree-ment through a third questionnaire It was thereforedecided that the third commvmication to respondentswould be an information giving exercise only
THE USEFULNESS OF THE KEYCHARACTERISTICS: CONCLUSIONS ANDPOINTS FOR ACTION
When the 18 key characteristics are considered m detailIt becomes possible to see their value as ingredients whichmight be built uito quality controls Some are clearlyperson- and possibly personality-focused, and others haveto do with the culture of the clmical environment and howIt IS managed Some are therefore open to influence eindcheinge and others less so The key characteristics are con-sidered further m the context of what they unply for thedelivery of optimum health care On occasions they aretaken together as the implications and issues are commonIn the following text there are some verbatim quotes fromrespondents which make telling observations
Optimum nursing practice should be aimed at what the clientsneed and want, not what we think they want A great deal needsto be done to equalize the partnership between practitioners andclients so that optimum nursmg care can be given
Giving support
The power to provide support rests with provider man-agers Although simple enough m concept it is seen bysome respondents to be vanable m quality, and to requirerenewed attention Clinical supervision has been rec-ommended as a device which is necessary for the supportand development of practice (Butterworth & Faugier 1992)In the document A Vision for the Future (NHSME 1993)clinical supervision is singled out for special attentionand undoubtedly provides a vehicle for sustaining anddevelopmg the profession
Recommendation for actionTarget ten from the document A Vision for the Future(NHSME 1993) which refers to clinical supervision isendorsed by this research, and information on clinicalsupervision should be extended by estabhshing ongoingtnals of different models of chnical supervision
I'm surpnsed that I've been nominated as an expert, no one hasbothered to tell me before
Being innovative
Innovation requires that attention be given to the develop-ment needs of staff providing optimum practice Numberof years m practice is no guarantee of continued excellenceand expertise There are cost implications which can bepeirtly met by mdividual nurses but which also requiretangible support from employers
Recommendations for action1 Providers sbould attend to the development needs of
staff by ldentifymg a relevant programme of continuingeducation through individual performance review
2 Commissioners need to identify a programme ofcontmumg development of staff in their contractingspecifications
Having expertise
Respondents m this survey could claim a great depth ofexpenence This expenence has as much vahdity m thedelivery of care as does the skill of the general mannerHealth care dehvery requires a mutual respect which recog-mzes and values both organizational and clinical skills
Experts are often deferred to and referred to by otherprofessions as the source of optimum practice It is evidentfrom this research that the hard won status which clinicalexcellence confers should be more openly acknowledgedand fostered
Recommendations for action1 The status of clinical excellence should be defended by
making sure that titles given to non-practitioners do notsuggest that they are clinically active
2 Titles given to clmical staff should be unambiguous andclearly imderstood by patients/clients in particular
Communicating
Opportunities to communicate properly were deimaged bypressure of work euid an inability of some managers tosee casework discussions as a legitimate part of workIntelligent nursing, midwifery and health visiting requiresintelligent debate and management Optimum practicerequires skills m wntten and verbal presentation
30 © 1995 Blackwell Science Ltd, Journal of Advanced Nursing, 22, 24-32
dharactenstics of optimum practice
Recommendation for actionOpportunities for communication must be allowed toflourish Managers should identify time to be made avail-able for proper communication
Personal qualities
Key personal qualities are thought of as important for theprovision of optimum practice Their importance lieswithin the area of role modelling for students and otherstaff It IS clear fi-om this study that personal qualities ratehighly with experts in practice
Recommendation for actionThere should be further work to explore the importanceof key personal qualities in the provision of optimumpractice
Patient care is only as good as the nurse who provides it Goodpatient care comes from a nurse who is motivated, happy at workand has good communication skills, has the relevant knowledge,IS willing to question and change her practice as required Theabove nurse functions well imder management with the samemotivation and skills with the foresight to empower staff
Working with other professions
Multi-discipIinary work is ofiered by many as a key to theprovision of effective care, and was clearly important tothe expert respondents m this study Collaborativeworking should be encouraged dunng first-level prep-aration, regardless of profession Experts m this study hadsufficient confidence to engage m an equal dialogue withmedical colleagues and could both take and give infor-mation and advice The combined product of a multi-disciplinary team is a powerful one and this power restsnot only in its combmed force but also m defining healthyboundaries and professional responsibilities
Recommendation for actionImtial and continumg education should include oppor-tunities for multi-disciplinary study This should be ident-ified when purchasing education
Practice is facilitated in the place where I work by a nurse edu-cation centre that is interested m nursmg care m the clinical areas
Sustaining and developing expertise
In order to maintain optimum practice there must beaccess to hbrary materials and resources Equally, although
I experts have displayed a great willingness to attend totheir own ongoing educational development, employerscarry some responsibility There is clear evidence of dim-lmshing opportumties for attending courses and studydays More particularly, such help as there is available is
often directed at short-term corporate requirements, to theexclusion of personal development There should beopportunibes for both
Extremes of provision have been seen in this researchThe report on a Strategy for Research in Nursing, Mid-wifery and Health Visiting (Department of Health 1992)provides good advice for research action, and the enthusi-asm for research-based practice shown by expert respon-dents m this exercise finds support and expression in thatdocument
Recommendations for action1 Centres of climcal practice should be linked to databases
and libranes in order to allow expert practiboners accessto research-based information
2 Continumg education should not only be a matter ofthecorporate need but should relate to individual develop-ment Appraisal schemes can locate both corporate andpersonal need and should be implemented at all levels
Working with people who use services
This study has highlighted the importance of workingalliances between service users and nurses, rmdwives andheedth visitors Where optimiun practice is provided thereIS often a working alliance between users and pro-fessionals It IS necessary to go beyond the simple gestureswhich have often been given as evidence of user involve-ment It IS quite possible to empower users still further bymvolving them as equal partners m curriculum com-mittees, research design and quahty measures
Recommendation for actionThe views and opinions of people who use services mustbe included m the provision of optimum practice by estab-lishing a series of workshops and debates designed toencourage a new partnership between user groups andnurses, nudwives and heedth visitors
I don't bog down my manager with tnvia, but I do talk to her andinvolve her m my cases if appropnate
Being well managed
Simple matters were reported as frustratingly absent andeasily rectifiable It was clear that some individu£ds werestruggling without clencal support and were often usingunintelligible and hopeless information systems There isevidence that the peirtnership between managers andexperts m this study is central to the provision of opti-mum practice
Support fi'om some managers was not always evidentand simple gestures of praise or encouragement were notgiven to balance the demands for change Staff meetingswere sometimes badly run, without agendas or discussion.
© 1995 Blackwell Science Ltd, Journal of Advanced Nursmg, 22, 24-32 31
T Butterworth and V Bishop
and human support services were seen by some asunskilled m selectmg new staff
Interestmgly, experts recognized the pressures uponmanagers and on occasions wanted to give recognition andsupport where it was due This was not always possiblebecause managers did not make themselves available toreceive it
Recommendation for actionThere should be a clear statement to purchasers whichdescribes and demonstrates the active mvolvement of thehuman support services in the clinical arena emd thenature of motivational support available for climcal staff
I have a wonderfully supportive senior nurse and general managerwho have enabled me to do all this work They have been therewhen and if I need them — but not breathing down my neck
The Expert Methodology Group
Professor Veronica Bishop, Department of Health,England Dr Senga Bond, Umversity of Newcastle,England Professor Christopher Maggs, Umversity ofWales, College of Medicme, Wales Dr Donna Mead,Umversity of Swansea, Wales Dr Sue Armitage (nowProfessor of Nursmg, Umversity of Sydney, Australia) MsBarbara Vaughan, Kmg's Fimd Centre, London, England
Disclaimer
The views expressed m this paper are those ofthe authorsand do not claim to represent the funding agency — TheDepartment of Health, England
References
Attree M (1993) An analysis of the concept of quality as it relatesto contemporary nursmg care Intemational Joumal of NursingStudies 30(4). 355-369
Bond S & Bond J (1982) Chmcal nursmg research pnonties
Unpublished monc^raph. Health Care Research Umt,Umversity of Newcastle upon Tyne, Newcastle upon Tyne
Butterworth T (1991) Meetmg the challenge of Europe NursingStandard 5(15), 24-28
Butterworth T 4 Faugier J (1992) Chnical Supervision andMentorship m Nursing Chapman and Hall, London
Cohen J (1960) Coefficient agreement for ordinal scalesEducation and Psychological Measurement 20, 37-46
Crotty M (1993) Clmical role activities of nurse teachers m Project2000 programmes Joumal ofAdvanced Nursing 18, 460—464
Department of Health (1992) Report of the Taskforce on theStrategy for Research m Nursing, Midwifery and HealthVisiting HMSO, London
Department of Health (1993) Targeting Practice The Contributionof Nurses, Midwives and Health Visitors HMSO, London
Duffield C (1993) The Delphi technique a comparison of resultsobtamed usmg two expert panels Intemational Joumal ofNursing Studies 30(3), 227-237
ENB (English National Board for Nursmg, Midwifery and HealthVisiting) (1993) The Provision of Learning Expenence m theCommunity for Students Undertaking Project 2000 ResearchHighlights Number 2 ENB, London
Farrell P & Shearer K (1983) The Delphi technique as a methodfor selecting criteria to evaluate nursing care Nursing Papers15(1), 51-60
Goodman C (1986) The Delphi technique a critique Joumal ofAdvanced Nursmg 12, 729-734
Kitson A (1986) Indicators of quality in nursing care — an alterna-tive approach Joumal ofAdvanced Nursing 11, 133-144
Linstone H & Turoff M (1975) The Delphi Method Techniquesand Applications Addison-Wesley, Readii^, Massachusetts
NHSME (National Health Service Management Executive) (1993)A Vision for the Future The Nursmg, Midwifery and HealthVisiting Contnbution to Health and Health Care Departmentof Health, London
Sackman H (1975) Delphi Critique Lexington Books, Boston,Massachusetts
Taylor A & Haussman G (1991) Meaning and measurement ofquality nursmg care Applied Nursmg Research 1(2), 84-88
Vaughan B (1992) The pursuit of excellence Nursmg Times88(31), 26-28
White E (1991) The Future of Psychiatric Nursing by the Year2000 A Delphi Study School of Nursmg Studies, Umversity ofManchester, Manchester
32 © 1995 Blackwell Science Ltd, Joumal ofAdvanced Nursmg, 22, 24-32
