hypospadias, epispadias and bladder exstrophy
TRANSCRIPT

HYPOSPADIAS
DR. SUDHIR KUMAR JAIN
M.B.B.S, M.S, M.B.A, F.R.C.S, F.A.C.S, F.I.C.S
DIRECTOR PROFESSOR
DEPARTMENT OF SURGERY
MAULANA AZAD MEDICAL COLLEGE

HYPOSPADIAS
• Definition- urethral opening proximal (ventral) to the normal granular location
• Caused due to arrested penile development
• Characterised by:
• Ventral meatus
• Ventral curvature (Chordee)
• Dorsal hood of prepuce
• Other defects:
• Downward glans tilt
• Deviation of the median penile raphe
• Ventral curvature
• Midline scrotal cleft
• Scrotal encroachment onto the penile shaft

NORMAL DEVELOPMENT
• Genital Tubercle elongation and enlargement + fusion of urethral folds
Testosterone
Penis

DEVELOPMENT
• Cloacal endoderm primitive urethral plate, ventrally
• Medial endoderm male urethra, ventrally
• Lateral ectoderm skin of penile shaft and prepuce
• Layers fuse posteriorly to anteriorly, forming median raphe
• Arrest in fusion HYPOSPADIAS
• Abnormal development of growth plate, disproportionate corpora and fibrosis leads
to penile curvature

• Main differential diagnosis is: Chordee without hypospadias aka Congenital Ventral
Curvature
• Characterised by asymmetrical preputial development but normal granular meatus
• Another variant termed as

• Incidence: 1: 300 males
• Risk is 13 fold in 1st degree relatives
• 8% patients have father with hypospadias, 14% have male siblings with hypospadias
• Risk of hypospadias in next child, when one child is affected with hypospadias:
• 12% with negative family history
• 19% if cousin or uncle has hypospadias
• 26% if father or sibling has hypospadias
• 8.5 times more risk in monozygotic twins

Other risk factors:
• Placental dysfunction
• Low birth weight
• Preterm birth
• Pre-pregnancy maternal obesity
• Extremes of maternal age ( <24 and >40)
• Assistive Reproductive techniques

ASSOCIATED ANOMALIES
• Undescended testes- 9%
• Inguinal hernias- 9%
• Upper urinary tract anomalies 1-3%
• Utriculus masculinus- Incomplete mullerian duct regression
• Cryptorchidism- intersexuality needs to be ruled out especially in cases of non
palpable testis

TIMELINE
• 100-200 AD
• Heliodorus and Antyllus
• Amputation distal to meatus
• 1838
• Dieffenbach
• Pierced glans to meatus with stenting
• 1869
• Thiersch
• Local tissue flaps
• Hook
• Multistage repairs
• One stage repair

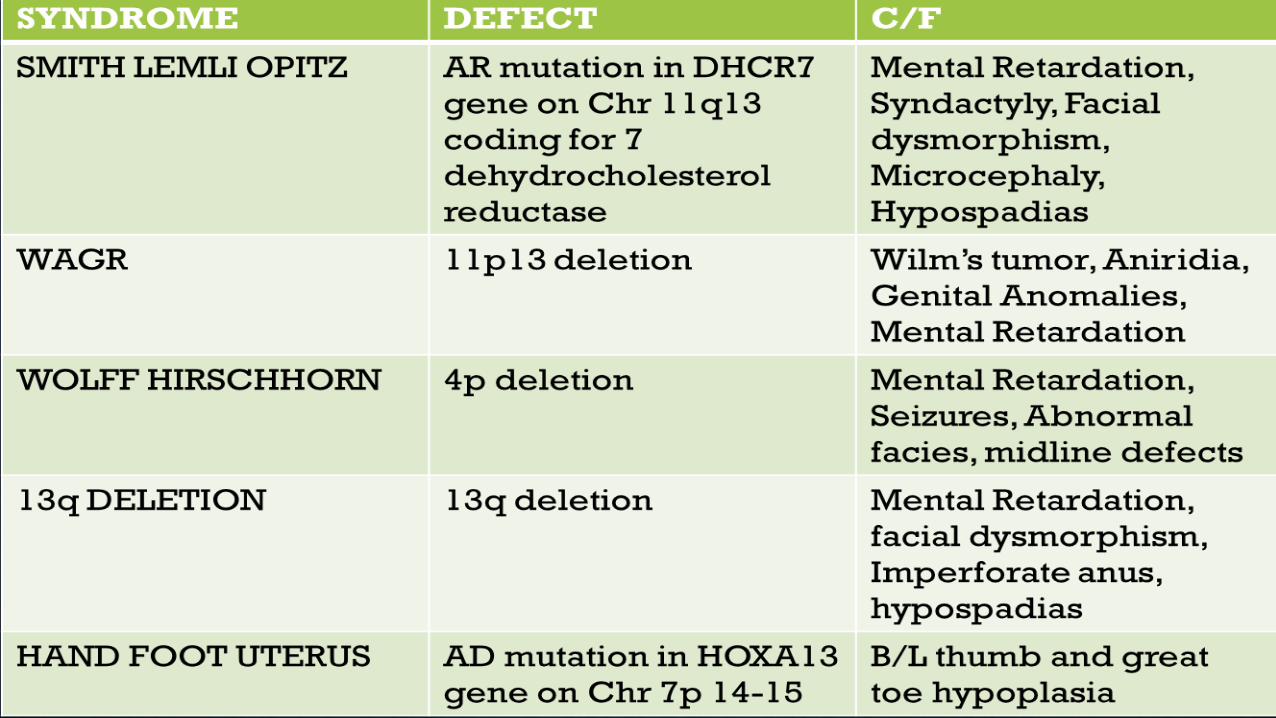
SYNDROMES
• 90% are isolated penile defects. Rest are syndromic namely:
• Smith Lemli Opitz syndrome
• WAGR syndrome
• Wolf Hirschhorn syndrome
• 13p deletion syndrome
• Hand foot Uterus syndrome

CLASSIFICATION
•ANTERIOR
•GRANULAR
•CORONAL
•SUBCORONAL
MIDDLE
DISTAL PENILE
MID SHAFT
PROXIMAL PENILE
POSTERIOR
•PENOSCROTAL
•SCROTAL
•PERINEAL

• Anterior hypospadias is the most common: 50-70%
• Posterior: 10-15%

TYPES OF HYPOSPADIAS
Coronal Hypospadias Peno-scrotal
HypospadiasPerineal Hypospadias with
Scrotal transposition

DIAGNOSIS AND TREATMENT
• Diagnosis is clinical
• Imaging not required in cases of isolated hypospadias, regardless of severity
• Surgery is the treatment of choice
• Performed at the age of 3 months or older

ALGORITHM FOR HYPOSPADIAS URETHROPLASTY
PROXIMALDISTAL RE-OPERATION
TIP
VC<30˚
2 STAGE
GRAFT
Urethral plate
maintained, no gross scar
VC>30˚
2 STAGE ORAL GRAFT
• BXO
• GROSS
SCARRING
• VC>30˚
• HAIR IN
URETHRA
INLAY ORAL GRAFT
previously
excised skin
strip
without
scar
PREPUCIAL FLAP
Sufficient
skin, no
BXO

TUBULARISED INCISED PLATE (TIP) REPAIR FOR
DISTAL HYPOSPADIAS
• A: Circumscribing skin incision
• B: Incisions along the visible junction of the
glans wings to the urethral plate
• C: Incision of the urethra plate extending
to near the underlying corpora
• D: Tubularising the urethral plate from
distally to proximally. Note that the first
stitch is about 3 mm proximal to the end of
the plate creating an oval opening
• E: The neourethra is covered with a dartos
flap
• F: Glansplasty creating the neomeatus and
continuing down to the corona
• G: Repair and circumcision completed

• Alternative methods for distal hypospadias repair:
• MAGPI- Meatal Advancement and Granuloplasty Incorporation
• Mathieu or Flip Flap technique

MAGPI
• Urethral plate is cut in dorsal midline, and meatus advanced distally
• Ventral lip of meatus is pulled distally and glans closed beneath it.
• Indications:
• Granular or coronal hypospadias
• Flat or convex glans
• Narrow meatus
• Skin and mucosa proximal to meatus thick and healthy
• No chordee or mild chordee

MATHIEU REPAIR
• Rectangular flap is outlined proximally on the ventral penile shaft, elevated and
sutured distally to the urethral plate

PROXIMAL HYPOSPADIAS REPAIR
• Choice of repair depends upon the extent of ventral curvature after degloving and
excision of scrotal extensions onto the penile shaft
• VC<30- TIP, preputial flap
• VC>30- single stage tubularised preputial flaps, 2 stage preputial flaps or 2 stage
preputial graft repair

TIP IN PROXIMAL HYPOSPADIAS
• A: Circumscribing incision preserves
urethral plate in patient desiring
circumcision.
• B: After degloving, glans wings are separated
from the urethral plate. Corpus spongiosum is
dissected from the cavernosal bodies and
released distally from the glans wings for
later spongioplasty. At this point artificial
erection is performed and ventral curvature
straightened as discussed in the text.
• C: Midline urethral plate incision.
• D: Two-layer urethral plate tubularization
using interrupted subepithelial 7-0
polyglactin followed by running 7-0
polydioxanone.
• E: Spongioplasty approximates divergent
corpus spongiosum over the neourethra,
before a tunica vaginalis barrier flap is added.
2 STAGE GRAFT
• Indication- VC>30˚
• Choice of flap depends whether patient undergoes circumcision or urethroplasty
• Urethral plate is transected as a part of straightening procedures followed by
preputial or buccal mucosa graft
• If circumcision is preferred, then discarded prepuce is used for graft
• If urethroplasty is desired, then oral mucosa from lower lip is preferred

1st stage consists of transecting the urethral plate to correct the ventral curvature followed by substitution of urethral bed
by using free preputial graft and creation of proximal urethrostomy.
A. Defect to be grafted after the urethral plate has been excised, glans wings developed, and proximal urethrostomy
created.
B. Graft secured to glans, shaft skin, and scrotum at the perimeter of the defect and then quilted to the corpora first along
the midline and then to either side at approximately 1-cm intervals.
C. Detail showing the graft extending to either side of the urethrostomy before quilting.
D. Tie-over dressing gently compresses the graft to reduce possibility for seroma or hematoma to accumulate beneath it.
E. Healed graft.

• 2nd stage consists of creating a
neomeatus by tubularising the
artificially created urethral bed over a
feeding tube and creating a distal
meatus.
• 2nd stage is usually carried out after 6
months of 1st stage
• Tunica vaginalis flap is placed over the
newly created urethra.
Tunica vaginalis flap covering the neourethra
PREPUTIAL FLAPS
• Onlay and tubularised flaps are single stage alternatived to TIP and 2 stage grafts.

ONLAY PREPUTIAL FLAP
• A. Lines of incision to create the preputial flap and preserve the urethral plate.
• B. Preputial flap mobilized on its vascular pedicle.
• C. Flap sewn to the urethral plate

TUBULARISED PREPUTIAL FLAPS
• After degloving and release of ventral
dartos, persisting ventral curvature
greater than 30 degrees led to excision of
the urethral plate. An inner preputial flap
approximately 10 mm wide is dissected on
its dartos vascular pedicle and transposed
ventrally. This flap can be tubularized,
with the proximal end anastomosed to the
spatulated native urethra and the distal
end to the glans wings.
• Alternatively, one edge of the flap can be
fixed with interrupted sutures to the
corpora cavernosa from the proximal
meatus distally into the glans. Then the
flap is trimmed and the opposite edge
sutured along the first to create a tube
with uniform caliber. Glansplasty and skin
closure are similar to that described for
onlay preputial flaps.

SALIENT FEATURES
• 90 % hypospadias are isolated, only 10% are syndromic
• Urinary tract imaging is not required for isolated cases.
• Surgery is the treatment of choice, performed at the age of 3 months or older
• Penile blocks are considered superior to caudal blocks for surgery owing togreater
risk of penile engorgement
• Ventral curvature <30- corrected by dorsal plication, >30 by degloving and dissection
• Tubularised preputial flaps have better outcomes as compared to onlay flaps
• For distal repairs, follow up is desired at 2 months and 8 months post-operatively,
while for proximal repairs, annual follow up is recommended till puberty.
SALIENT FEATURES• Risk factors for complications:
• Proximal meatus
• Re-operation
• Glans width <14mm
• Complications include:
• Fistula
• Glans dehiscence
• Meatal stenosis
• Neourethral stricture
• Diverticulum at the flap site
• BXO
• Graft contractures
• Obstructive urinary symtoms
• Sexual dysfunction
EPISPADIAS

• Defect in the dorsal wall of urethra
• Normal urethra is replaced by a strip of mucosa
• Associated Defects:
• Dorsally placed meatus
• Dorsal chordee
• Sphincter incontinence
• Pubic bone diastasis
• Unilateral renal agenesis
• VUR in cases of complete epispadias
• Male: Female =3-5:1
• Incidence is 1:1,00,000

TREATMENT
• Treatment goals include:
• Cosmetically acceptable genitalia
• Preservation of urinary continence
• Prevention of reflux
• Urethroplasty and penile elongation procedures are carried out before bladder neck
reconstruction
• Bladder capacity is the eventual indicator of continence and therefore is increased upto 95cc
in 18 months post epispadias repair before carrying out bladder neck reconstruction
procedures to have better functional outcomes
• Yound-dees-leadbetter and Marshall-Marchetti-Krantz suspension and ureteric
reimplantation are performed usually between 4-5 years of age
• Meticulous repair of urethra, appropriate selection of patients and surgical expertise form the
cornerstone for success

FEMALE EPISPADIAS
• Rare anpomaly
• Incidence 1;480,000
• Davis classification used for severity
• Mild: urethral orifice patulous
• Moderate: urethra dorsally split along most of the urethra
• Severe: cleft along entire urethra + incontinence
• Genital defect includes bifid clitoris, depressed mons with underdeveloped labia minora
• Vagina and internal genitalia usually normal

• Deficient ureterovesical junction wity
resultant reflux
• Small and thin bladder with limited capacity

• A. Normal female anatomy.
• B. Vesicular epispadias—urethra mainly normal but relation to clitoris altered.
• C. Subsymphyseal epispadias—defect in anterior wall of urethra for about one half its length.
• D. Retrosymphyseal epispadias—defect in anterior wall of entire urethra. Sphincter is usually involved

TREATMENT
• Objectives:
• Reconstruction of functionally and cosmetically acceptable genitalia
• Achievement of continence
• Preservation of upper urinary tract

A. Typical appearance of female epispadias with initial incisions outlined.
B. Excision of the glabrous skin of the mons.
C. Tapering of the urethra with a dorsal resection of a wedge of tissue.
D. Reconstruction of the urethra over a catheter with running suture.
E. and F, Medial aspect of the labia minora and clitoris.
G. Initial layer of mons closure.
H. Approximation of the labia minora over the urethral reconstruction.
I. Second layer of mons closure.
J. Creation of clitoral hood.
K. Completion of mons closure.

BLADDER EXSTROPHY

EXSTROPHY-EPISPADIAS COMPLEX
• Bladder exstrophy generally occurs as a complex of meatal defects alongwith
genitourinary malformations termed as exstrophy-epispadias complex
• Incidence 2.2 per 100,000 live births
• Risk is 500 times more in offsprings of affected parents
• Increased incidence in mothers who received large doses of progesterone in the early
part of 1st trimester
• Disruption in the 5’ region of CASPR3 gene on chromosome 9

SPECTRUM OF EXSTROPHY-EPISPADIAS
COMPLEX:
1. SUPERIOR VESICAL FISSURE
2. CLASSICAL BLADDER EXSTROPHY
3. MALE EPISPADIAS
4. FEMALE EPISPADIAS

EMBRYOLOGY
Allantoic ductMidgut
Cloacal
membrane
Tailgut
Midgut
Hindgut
Cloacal
membrane Incompletely
divided cloaca
Urorectal
septumGenital tubercle
Bladder
anlage
Cloacal
membrane
Genital
tubercle
Bladder
Hindgut
Urorectal
septum
Anal
canal
Peritoneum
Peritoneum
Hindgut
Rectum
Anal
membrane
Urogenital
membrane
Urogenital
sinus
Bladder
Urachus
The theory of embryonic maldevelopment in
exstrophy held by Marshall and Muecke (1968) is
that the basic defect is an abnormal
overdevelopment of the cloacal membrane during
the 4th week of gestation, which prevents medial
migration of the mesenchymal tissue and proper
lower abdominal wall development.4th Week 8th Week

• Classical exstrophy >50% of this complex
• Closure of lateral body wall folds results in exstrophy
• If failure of fusion in abdominal and pelvic regions both Cloacal exstrophy
• If failure of fusion in pelvis alone Bladder exstrophy
• Other theories:
• Abnormal development of genital hillocks
• Abnormal caudal insertion of body stalk with failure of mesenchyme interposition
• Maldevelopment of bony pelvis

CLASSICAL EXSTROPHY
• Rotational Defects include:
• external rotation of the posterior pelvis/iliac wings;
• external rotation of the anterior pelvic segment
• Coronal rotation of the sacroiliac joint
• acetabular retroversion
• convergence of iliac wings
• femoral retroversion.
• Dimensional anomalies include:
• increased pubic diastasis
• shortened anterior pubic segment
• increased intertriradiate cartilage distance

• These defects lead to short, pendular penis
• Bony defects also lead to bony deformities and waddling gait

PELVIC FLOOR DEFECTS
• Pelvic floor muscles particularly levator ani group is positioned more posteriorly and
outwards leading to a more flattened puborectal ling leading to exstrophy
PubococcygeusPuborectalis Pubococcygeus
PAUCITY OF ANTERIOR PELVIC FLOOR MUSCULATURE
ABDOMINAL WALL DEFECTS
• Premature rupture of cloaca causes triangular defect being taken up by bladder and
posterior urethra
• Associated indirect inguinal hernias can be seen owing to persistent processus
vaginalis, large superficial and deep rings, and lack of obliquity of inguinal canal
• The perineum is short and broad and the anus is situated directly behind the
urogenital diaphragm. Patient has varying degrees of anal incontinence and rectal
prolapse due to deficient anterior pelvic musculature

MALE GENITAL DEFECTS
• Male genital defects included:
• Corporeal bodies separated and triangular in shape
• Long convex ventral surface and short wedge shaped dorsal surface
• Varying length of neurovascular supply
• Prostate and accessory sex organs remain unaffected
• Autonomic innervation of corpora are displaced but maintained functionally
• Testis remain normal and descend normally without the need for orchiopexy

FEMALE GENITAL DEFECTS
• Female genital defects:
• Vagina is shorter in length, ≤6cm, but calibre normal
• Vaginal opening stenotic
• Clitoris bifid, and labia, mons and clitoris are divergent
• Cervix enters the vagina more superiorly, lying in the anterior vaginal wall near introitus

URINARY SYSTEM DEFECTS
• The most common malformation was a duplicated collecting system
• Others included:
• hypoplastic or absent kidney
• pelvic kidney
• ureteropelvic junction obstruction
• Multicystic dysplastic kidney.
• Reflux in the closed exstrophy bladder occurs in 100% of patients, and reimplantation surgery
is required at bladder neck reconstruction. If excessive outlet resistance is gained at the time
of either initial closure or combined epispadias and bladder exstrophy closure, and recurrent
infections are a problem even with suppressive antibiotics, ureteral reimplantation or Deflux
injections are required before bladder neck reconstruction.

DIAGNOSIS
• Clue to prenatal diagnosis can be provided by high resolution obstetric ultrasound.
• Features observed:
• Absence of bladder filling
• A low-set umbilicus
• Widening pubis ramus
• Diminutive genitalia
• A lower abdominal mass that increased in size as the pregnancy progressed and as the
intra-abdominal viscera increased in size
• Fetal MRI is reserved for patients in whom 3D ultrasonography is not sufficient to
differentiate satisfactorily between classic and cloacal exstrophy, or when other severe
anomalies are suspected.

MANAGEMENT
• Management is surgical with medical management playing a supportive role
• Previously exstrophy-epispadias complex was managed via surgery in a staged
manner with B/L iliac osteotomies being oerformed 4-6 days prior to bladder closure
and epispadais repair performed separately.
• In the current scenario, management include:
• bladder closure, abdominal wall closure, and posterior urethral closure well onto the penis in
the newborn period
• bilateral innominate and vertical iliac osteotomy, if indicated
• epispadias repair at 6 months to 1 year of age
• bladder neck reconstruction along with antireflux procedure at age 4 to 5 years, when the child
has achieved an adequate bladder capacity for bladder neck reconstruction and is motivated to
participate in a postoperative voiding program

• Osteotomy:
• Diastasis>4cm
• Malleability of the pelvis poor
• If the patient is younger than 72 hours and examination under anesthesia reveals that the pubic bones are
malleable and able to be brought together easily in the midline by medial rotation of the greater trochanters, the
patient can undergo closure without osteotomy.
• Complications of inadequate immobilization include:
• Failure of the closure
• bladder prolapse
• loss of suprapubic tubes, and ureteral stents.
• inadequate pain and movement control.
• Main role of osteotomy to be relaxation of tension on the bladder, posterior urethra, and abdominal
wall repair during healing.

BLADDER REPAIR TECHNIQUES
• Surgical treatment of choice is MSRE (Modern Staged Repair of Exstrophy)
• Other repairs include:
• Warsaw
• Kelly
• Complete
• Mainz
• Erlangen
• The primary objective in functional closure is to convert the bladder exstrophy into a complete
epispadias with the urethra well up onto the proximal shaft or midshaft of the penis

A. Initial incision around the bladder plate in the male.
B. Initial incision around the bladder plate in the female.
C. Incision follows the bladder template and includes the umbilicus.
D. Dissection of the lateral aspect of the bladder from the abdominal wall.

E. Dissection of the crura from the symphysis pubis.
F. Division of the urogenital (UG) diaphragm fibers.
G. Initial layer of the bladder closure. Urethral meatus is calibrated to 14-Fr size. Stents are
brought out of the bladder.
H. Pubic approximation is performed with No. 2 nylon mattress suture (see inset). Abdominal wall closure
is completed. Suprapubic tube and stents are brought out through the neoumbilicus.