hsda 03/02 done - · tasks each person must perform. many of them contain checklists of items such...
TRANSCRIPT

Sign up for your
FREE e-mail
newsletter at
www.healthsafetyinfo.com
and visit our online store,
www.hcmarketplace.com,
for daily discounts
and specials!
Training and drilling are effectiveways to make sure your staff knowwhat to do during a disaster, buttwo questions still nag safety andsecurity officers: How do you bestshow regulatory agencies your staffresponse to an emergency? And doeseveryone in your hospital knowwhat to do during an emergency?
The University of Utah Hospitalsand Clinics use a system that in-cludes role description cards and a72-hour disaster kit, says MurrayHayward, chief security officer forthe Salt Lake City-based system.
Surveyors cited the role cards as a“best practice” during the system’s
last survey in November 2001.
Role description cardsThe laminated role cards provideprinted instructions for staff to re-fer to and follow during a crisis.The cards, printed for both teamsand individual staff members, con-tain team member names, pagernumbers and codes, and assemblypoints for various team members.The role cards are based on thetasks each person must perform.Many of them contain checklistsof items such as status reports anddispatch and communicationsinstructions.
“Role cards define
Vol. 2 No. 11November 2001
Proven advice
Role cards and disaster kit earnJCAHO best practice seal
f o r
> p. 2
—INSIDE—
Need an HVA?The JCAHO wants you to complete a hazards vulnerability analysis as partof your disaster preparedness.Use this form with accompanying instructionsto take a good accounting of the hazards facing yourfacility, p. 4.
Looking for disaster dollars?Wondering where the funding is coming from? Act quickly if you want federal dollars for you hospital. Look here for thelatest updates, p. 9.
Questions and answersTwo experts answer questions during a recentaudioconference on bioterrorism preparedness,p. 10.
City prep digestOne Texas metropolitan area is making plans for acommunity-wide response toterrorism. Find out what it’sdoing on p. 12.
HEALTHCARE SECURITYAND DISASTER ALERTVol. 2 No. 3
March 2002
Ground Zero report:
Use daily information to monitorchemical, biological, or hazmat outbreaks
over a period of time to determinewhether a pattern or trend emerges,says Zachary Goldfarb, a NewYork–based management consultant.
On September 11, city officials keptan eye on these numbers, watchingfor spikes in the data indicating apresence of chemical or biologicalagents in the air.
Are you looking for a way totrack chemical, biological, or haz-ardous material (hazmat) informa-tion? Then adopt a process usedby New York City officials to alertyou to these situations.
City leaders there compare statis-tics such as ambulance calls andemergency room (ER) admissions > p. 8

Page 2 Healthcare Security and Disaster Alert—March 2002© 2002 Opus Communications, a division of HCPro
www.healthsafetyinfo.com
Role cards < p. 1
expectations by department and job description,”Hayward says. “They remind key people of thenecessary tasks to perform during infrequentand stressful events.” (See boxes below foran example of role card instructions.)
Disaster kits provide hardwareand survival items The hospital system patterned its disasterkits on the concept of assembling a 72-houremergency kit in the home. Staff place the kitsin large plastic toolboxes and inventory them for
expired contents every six months. The kits containduplicate role cards, facility and work area maps,
phone tree information, and other charts inpage protectors.
Emergency Planning Director DebbieKim instituted the disaster kit pro-
gram in 1990. For a detailed list of dis-aster kit items, see below. Each department
has its own set of kits stocked with enoughequipment for all personnel on duty at the time
of an emergency.
• Portable, battery-operated radio (see batterycomments above)
• Bag of hard candy or other snack items whichwill not deteriorate, such as instant powdereddrinks, coffee, etc.
• Gallon size Zip-loc baggies• Mortuary bags and tags or large bags which
could carry supplies if needed• Felt tip markers, pens, pencils and tape• A first aid kit (if you are far away from a clini-
cal area)• A whistle or other device that makes a loud
sound• Leather work gloves • Drinking water for patients and staff• One gallon of household bleach
Emergency management disaster box contents
The laminated role cards provide printed
instructions for staff to refer to and follow
during a crisis.
Role description card—Building systems operatorCode Yellow Alert and Code Yellow ActivateOutside of Normal Working Hours
The on-duty building operator notifies the follow-ing members of the facilities and engineering de-partment’s emergency response team:
1. Director of facilities and engineering
2. Manager for project control for the departmentof facilities and engineering
3. Supervisors of facilities and engineering4. Safety officer
The director or designee will determine additionalstaff requirements and whether to call-in more personnel.
Note: Encase copies of plans, or anything inpaper in a plastic page protector.
• Dated copy of hospital emergency manage-ment plan
• Dated copy of unit-specific emergency man-agement plan
• Dated list of telephone tree numbers for unit-based personnel
• Map of work area with exits, fire extinguisher,crash cart, and oxygen shut-off valve marked
• Copy of role description cards for each staffposition in unit or department
• One flashlight per staff member on duty • Flashlight batteries stored separately from the
flashlight in a plastic bag Source: Murray Hayward. Reprinted with permission.
Source: Murray Hayward. Reprinted with permission.

Make sure your facility is ready
for a disasterwith our
comprehensivepreparation
series at a savings of 40%!
Order the four-tape series of these recent audiocon-ferences and keep your facility one step ahead!
Tape #1 Disaster readiness in healthcare: Immediate steps to take
Tape #2 Preparing for bioterrorism: An action plan to strengthenyour existing staff's preparedness
Tape #3 Security planning for terrorism: staffing, steps, andpriorities
Tape #4 Decontamination during a mass casualty incident
The 4-tape series is yours for just $450—a savings of over 40%Call Customer Service at 800/650-6787 today.
Page 3Healthcare Security and Disaster Alert—March 2002 © 2002 Opus Communications, a division of HCPro
www.healthsafetyinfo.com
Code yellow alert and code yellow activate:• Director, facilities and engineering:1. Director reports to the command center (nor-
mally the boardroom).2. Director serves as liaison between command
center and the facilities and engineering emer-gency response team.
• Facilities and engineering staff (F&E):1. Facilities and engineering staff report to the fol-
lowing areas:
a. Emergency response team reports to the build-ing operator’s shack.
b. Alert manpower pool members and F&E car-penters and painters by group page number,555-1212. The pager code is nine ones,
Role description card—Director, facilities and engineering
(111111111). The pool members report to man-power pool in bldg. 200, level 1, near the eastentrance between the emergency room andradiology department, to await assignment.
c. Bio-medical personnel report to the bio-medshop for assignment to the critical care area.
d. Electricians report to the electrical shop. Twodesignated electricians will go to each of theemergency generator locations.
e. Office and storeroom personnel remain at theirnormal workstations.
f. Other F&E personnel report to the B-level bay,near the freight elevator, to await assignment.
g. After an event that threatens the structuralintegrity of building 521, all F&E staff meets atthe predesignated assembly area between Bldg.525 and the West Terrace.
Healthcare Security and Disaster AlertSubscriber Services Coupon
❑ Payment enclosed. ❑ Please bill me.❑ Please bill my organization using PO # ________________________Charge ❑ AmEx ❑ MasterCard ❑ VISASignature ____________________________________________________
Card # _____________________________________ Expires _________
Name & Title _________________________________________________Organization _________________________________________________Address _____________________________________________________City ________________________________ State ____ ZIP ___________Phone ( ) ___________________ Fax ( ) _______________________E-mail ________________________________
Mail to: Opus Communications, P.O. Box 1168, Marblehead, MA 01945
Call: 800/650-6787 Fax: 800/639-8511E-mail: [email protected]
(Required for authorization)
Your credit card bill will reflect a charge to “Opus Communications,”the publisher of Healthcare Security and Disaster Alert.
Source code:N0001
❑ Start my subscription to HSDA immediately. Please include a $15.00shipping and handling charge (option 1 or option 3 only). Deliveryoptions: (please select one only)
❑ Option 1: Print subscription (just $347 for 12 full issues) HSDAP ❑ Option 2: Electronic subscription (just $347 for 12 full issues) HSDAE❑ Option 3: Print and Electronic subscription (just $434 for 12 full issues
of each) HSDAPEOrder online at www.hcmarketplace.com and save 10%!
(Required for electronic subscriptions)
Special Offer!
Special Offer
MZ3568
Source: Murray Hayward. Reprinted with permission.

Page 4 Healthcare Security and Disaster Alert—March 2002© 2002 Opus Communications, a division of HCPro
www.healthsafetyinfo.com
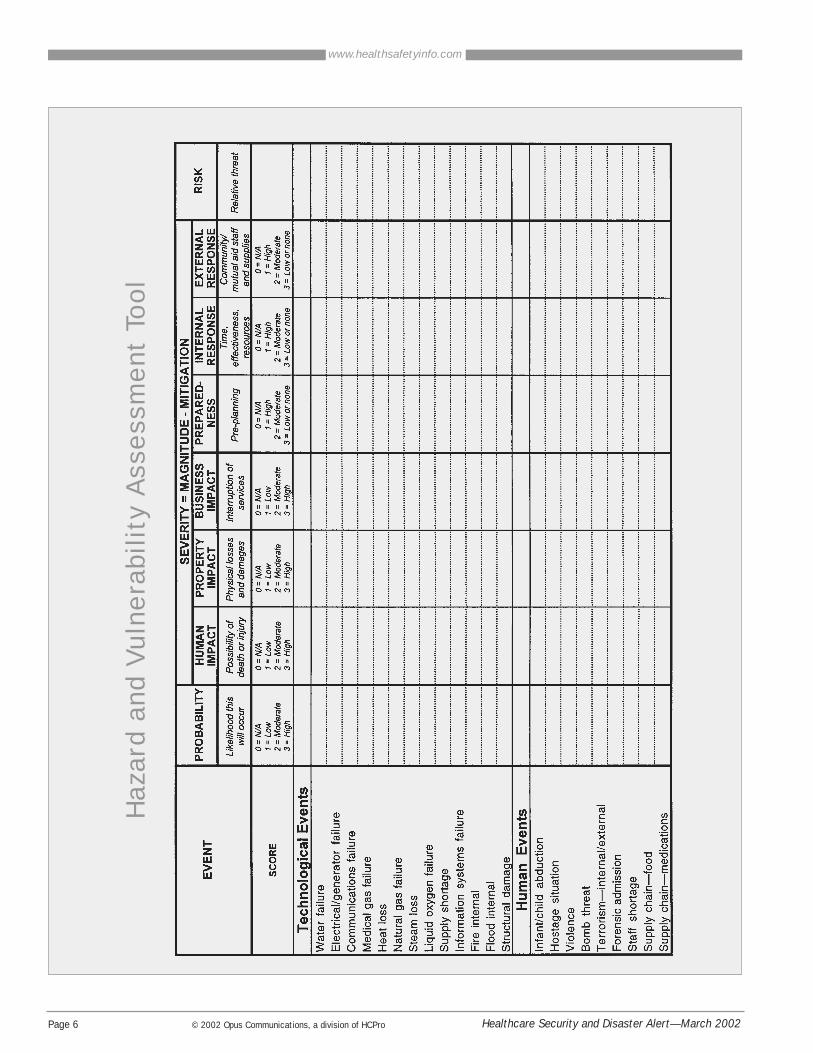
Everyone wants the hospital security director to pre-pare for every unforeseen event. But how do youknow whether you have looked at every possibility?
The Joint Commission on Accreditation of HealthCare Organizations wants you to use a hazards vul-nerability analysis (HVA). The HVA is a tool to helpyou identify, evaluate, and prioritize events that af-fect your facility’s abilities to provide services, saysSteve Bryant, practice director for accreditation atThe Greeley Company, a division of HCPro in Mar-blehead, MA. “Conducting an HVA gives you a morequantifiable scientific model to determine where to getthe best value for your resources and staff,” he says.
The JCAHO began requiring HVAs as part of its envi-ronment of care program when it revised the emer-gency management standards in January 2001.
The basicsUse a simple spreadsheet to set up your HVA. In theleft-hand column, list general categories of events thatcan happen followed by specific examples. Each eventwill get its own separate row on the spreadsheet. Forexample, consider the following categories andexamples:• Technological events—electrical, water, sewer, fire
alarm, and communication failures• Human-related events—mass-casualty incident (trau-
ma), mass-casualty incident (medical/infectious),infant abduction, civil disturbance, bomb threat
• Events involving hazardous materials—chemicalspill, hazardous material incident involving smallor mass casualties, external chemical exposure,terrorist chemical attack
✔ Tip: Use past incident reports, relevant local data,and experience to determine the different events toinclude in your HVA. Critical systems and utilities arealso good sources for determining events.
✔ Tip: As an alternative to the general topics listedabove, use the seven elements listed in EC.1 as thegeneral topics for your HVA. The standard says thathospitals plan for the following:• A safe environment
• A secure environment• Managing hazardous materials and waste• Addressing emergency management• Fire prevention• Managing medical equipment• Managing utilities
Using those topics shows surveyors that you ad-dressed the elements within the survey. Either way,give a good accounting of potential threats to yourhospital and how you will deal with them.
Severity and magnitude Once you develop a list of events that could affectyour hospital, determine the probability of the eventoccurring and its impact. To do this, label columnsacross the top of the spreadsheet with the following:
• Probability—Assess the likelihood of each eventoccurring. For example, a hospital in southernCalifornia has a higher probability of experienc-ing an earthquake than a hospital in Madison,WI. The hospital in Madison is more likely toface an ice storm.
• Human impact—Consider the possible amountof deaths or injuries if the event occurs.
• Property impact—Measure the potential physi-cal loss/damage to your building.
• Business impact—Evaluate the possible inter-ruption of service to patients.
Assign a numerical value between zero and threeaccording to the probability of the event occurringand its effects in the above categories. A “three” in-dicates a high chance that the event will happenand have a definite effect on the impact categories.For example, if your hospital is located in the South-eastern coastal regions, you’re probably no strangerto hurricanes. You would put a “three” under theprobability column. Likewise, a hurricane would doconsiderable damage to the human, property, andbusiness impact of the facility, so you would scorethose with a “three,” also.
MitigationThe next three columns deal with response scenar-
The nuts and bolts of a hazards vulnerability analysis
Page 5Healthcare Security and Disaster Alert—March 2002 © 2002 Opus Communications, a division of HCPro
www.healthsafetyinfo.com
ios and training that you should already have inplace. Label these columns with the following:
• Preparedness—How well you plan and train forthis event. Consider the resources available to you. • Internal response—The time it takes for yourstaff to react to the emergency. Do you have every-thing you need to handle the situation? • External response—The necessary contacts youneed with outside vendors. Do you have communityresources, such as contracts for external power gener-ators or snow removal? If so, how long will it takethem to respond?
For the mitigation columns, use a scale of one to three,with a “one” indicating the highest level of readiness.Using the example of the Southeastern coastal hospitaland the hurricane threat, you can say the hospital hasplans in place and experience because the facility hasbeen through this threat before. Therefore, mark a
“one” under each of the mitigation columns.
Determining riskOnce you assign numeric values to the prepared-ness, magnitude, and mitigation of each event, addthe columns up to determine the risk of the event toyour facility. A higher score indicates a higher riskto your facility. Using these scores, you can deter-mine where to apply resources for training andreadiness planning.
By taking a close look at the specific hazards thatyour facility faces based on past incidents and theprobability of future events, you can better focusyour training and resources.
“It forces you to think in a way that you haven’tthought of before,” Bryant says. “You are correlatingall the possibilities of events that could happen toyour facility to the level of preparedness.”
With current calls for heightened security through-out the industry, some health care security man-agers may jump to add more officers or upgradesecurity devices without taking into account theactual risk their facility faces.
But don’t be hasty. Determine what risks exist, howto mitigate them, and how to design good systemsto deal with them. “Putting additional resources inplace without thinking it through is a big mistakeand can create more difficulty in terms of credibil-ity and resources deployment in the future,” saysBonnie Michelman, CPP, CHPA, director of po-lice security and outside services at MassachusettsGeneral Hospital in Boston. Michelman’s com-ments came during last month’s audioconferenceon security planning for terrorism sponsored byThe Greeley Company. (See p. 3 to order.)
People are listeningAdvice from security directors is being sought out
more than ever since the September 11 attacks. “Ed-ucate people now because they are listening likethey have never listened before to . . . our indust-ry,” Michelman says.
In addition to education, efforts that should be un-der way for disaster planning and terrorism includereassessing facilities and doing risk assessments in anew, heightened, and frequent way, she says.
You can use other sources to assess the risk to yourfacility. “Certainly, we need to do a better job in co-ordinating with other agencies—law enforcement or-ganizations, federal, state, and local agencies, andother hospitals—to gather intelligence pertinent tous,” Michelman says.
Tip: Local law enforcement agencies and regionalbranches of federal agencies offer demographic infor-mation that you can use along with HVA data to helpyou accurately assess threats to your facilities.
Don’t change security systems without reassessing them first
Page 6 Healthcare Security and Disaster Alert—March 2002© 2002 Opus Communications, a division of HCPro
www.healthsafetyinfo.com
Haz
ard
and
Vuln
era
bility
Ass
ess
ment
Tool

Page 7Healthcare Security and Disaster Alert—March 2002 © 2002 Opus Communications, a division of HCPro
www.healthsafetyinfo.com
Sou
rce:
Ka
iser
Per
ma
nen
te.
Rep
rin
ted
wit
h p
erm
issi
on.

Page 8 Healthcare Security and Disaster Alert—March 2002© 2002 Opus Communications, a division of HCPro
www.healthsafetyinfo.com
Communities in the rest of the country can use a sim-ilar model for tracking an outbreak of disease gener-ated by chemical or biological agents, or Hazmatexposure.
First things first: Develop a baselineFind a database of information to use as a baseline.City and county health departments often have thisinformation already available. For example, if theaverage number of daily ambulance runs for a givenday is five, that number will become your baselinefor ambulance runs.
Next, develop a system to collect specific informa-tion from your area on a regular schedule. Includethe following elements in your reporting system:
1. A central source to cull information together—Designate a person or office within your hospital orhealth care community as a repository of the informa-tion. This person gathers information and monitors itfor any spike in the data indicating the presence ofa biological or chemical agent.
Ground Zero report
2. A system for reporting information that worksfor your facility or community—E-mail is the pre-ferred medium, but at the very minimum, a fax ma-chine will do the trick.
If your facility’s computer infrastructure allows you tosend spreadsheets by e-mail, you can send informa-tion that is already sorted.
3. A database of information—Use informationfrom the following sources to develop this database:• Emergency management system information in-
cluding pre-hospital fatalities, increased ambulanceruns, and ambulance run call types by category(breathing, flu, respiratory)
• Hospital information including diagnoses codes,ER admission statistics, and triage statistics
• Medical examiner office indicators including deathsby age group or influenza
• Commercial pharmacy information such as pur-chases of over-the-counter drugs
Monitor the information spikesOnce you’ve put the information-gathering system inplace, monitor it for any sharp increase in the data. Forexample, using the previous example of five ambu-lance runs in a day, you notice that your ambulanceteam has completed 15 runs before 11:00 a.m. Thisabnormality indicates that something is going on inthe field that may need further investigation.
✔ Tip: Remember, this is time-sensitive information,so you’ll need to process and act quickly on it.
Develop a protocol to react to information spikesUsing your hazards vulnerability analysis (HVA) as aguide, work out contingency plans to activate whendeviations or changes in data occur. Also, use theHVA and data to stock your medical and decontami-nation teams with proper equipment and medications.
For example, data indicating an outbreak of chemi-cal agents prompts you to activate your decontami-nation team and secure all entrances to your facility.As patients arrive, your staff directs them to theproper area and decontaminates them.
< p. 1
Has your hospital or health carefacility produced a video to helpeducate and train your staff? If so, it may be eligible for HCPro’s
inaugural Academy Awards®for staff training excellence. You and
your award-winning video will be profiled in one ofour publications and receive a $100 prize. Pleasesend in your business card along with a non-return-able copy of your video. Entries must be receivedby April 1, 2002. Winners will be notified in writ-ing by May 1, 2002.
And the nomineesare . . . ???

Page 9Healthcare Security and Disaster Alert—March 2002 © 2002 Opus Communications, a division of HCPro
www.healthsafetyinfo.com
Want federal dollars? Start writing letters nowAct fast if you want to get ahold of the federal dol-lars coming to states from the Department of Healthand Human Services (HHS).
Send a letter outlining your hospital’s needs to yourgovernor, state department of health, and state home-land security director, says John Hauser, safety offi-cer for the Nebraska Health System in Omaha.
“If you do not let them know your needs, I guaran-tee that others [first-responders, police, and fire agen-cies] will be at the table and will receive the most,”Hauser says.
Misconceptions abound about hospitals’ prepared-ness levels, he says.
“A few years ago some of the hospital safety folks[here] went to federal community training sessionsfor the first responders,” Hauser says. “They were tell-ing the fire, EMS, and police folks they didn’t needto worry about hospitals because all hospitals are re-quired to have plans to meet the accreditation require-ments,” he says. “We set them straight.”
FEMA seeks $6.4 billion budgetThe Bush administration asked Congress for $6.4billion in funding for the Federal Emergency Man-agement Agency (FEMA) in 2003. FEMA requested$3.5 billion to provide better training, equipment,and preparation for first responders including fire-fighters, police officers, and emergency medicaltechnicians. The agency also is asking for $1.8 bil-lion for the President’s Disaster Relief Fund to coverobligations for prior-year declarations and costs forfuture declared disasters. FEMA wants $300 millionfor a new, pre-disaster mitigation program that willprovide competitive grants for projects that reducefuture disaster risks.
FEMA’s budget request also includes:• $50 million for FEMA’s Office of National Pre-
paredness to work with states and localities onterrorism preparedness and administer the firstresponder grant program
• $117.4 million for financial and technical assistanceto improve mitigation techniques and planningprocesses for reducing damage from earthquakes,hurricanes, dam failures, and floods
• $300 million to update and digitize flood maps,and make them available over the Internet
Bush pushes for $5.9 billion in fiscal year 2003 bioterrorism prep spendingPreparing for future bioterrorist attacks is a major pri-ority in the Bush administration’s fiscal 2003 budgetproposal. It seeks $5.9 billion to finance improvementsin the nation’s public health system. The proposed in-crease is more than four times what the governmentspent on bioterrorism preparedness before the Sep-tember 11 terrorist attacks. The anthrax mail attacksraised concerns about the government’s ability torespond to such acts. The budget also includes
• $518 million to help hospitals plan for biologicalor chemical disasters
• $100 million to buy an antidote to treat peoplewho have reactions to the smallpox vaccine
• $98 million to hire more food inspectors to doublethe number of examinations of imported food
State bioterrorism preparedness funding announcedHHS last month detailed how it will distribute $1.1billion in bioterrorism preparedness funding for states.The funds are divided into three parts, with the firstportion provided by the Centers for Disease Controland Prevention and designated to support states deal-ing with bioterrorism, infectious diseases, and publichealth emergencies.
The Health Resources and Services Administrationprovides the second portion, which helps states createregional hospital plans to respond to a bioterrorismattack. The third part, supplied by the HHS Office ofEmergency Preparedness, supports the MetropolitanMedical Response System (MMRS), which improvesemergency responses to mass-casualty incidents. Thiswill add 25 new cities to those that received MMRSfunding in recent years. For a state-by-state break-down of the HHS funding, go to www.hhs.gov/news/press/2002pres /states.html
Trailing those disaster dollars . . .

AnswersAnswers&&QuestionsQuestionsIt’s probably worthwhile training some peo-ple with the hazmat team, because unless
the off-site team responds to a hazmat crisis, youmay have to deal with one. Create a plan to pro-tect your facility from contamination.
What should hospitals do with patients’relatives during an emergency?
Create a master list of patients’ whereaboutsfor family members. Here’s how it works:
Track patients by name within your communityresponse plan. The ideal place tostart this process is at the emer-gency management system levelwhere, as ambulances depart thescene with patients, a recorderdocuments what ambulance takeswhat patient (by name) to whatdestination.
Second, give or transfer this infor-mation to a call-taking center, which the
regional office of emergency management can bestorganize. All hospitals taking in patients can call thecenter with this information, so that it can compilea master list. A telephone number can then bepublished for family members to call in and findtheir loved ones.
If non-medical personnel decontaminatepatients, who determines which victims
get decontaminated or treated first? Shouldphysicians or registered nurses do that?
Non-medical personnel should perform theactual hands-on decontamination of patients.
Assign a triage person in the “hot zone” (the wait-ing area for contaminated victims) to direct whogoes through the decontamination line first. Once
Page 10 Healthcare Security and Disaster Alert—March 2002© 2002 Opus Communications, a division of HCPro
www.healthsafetyinfo.com
Q:
A:
A:
Q:
A:
Each month we ask emergency managementplanners questions related to security and disasterplanning in the health care environment. Thismonth’s questions come from the December 19,2001, HCPro audioconference, “Preparing for bioter-rorism: An action plan to strengthen your staff’s pre-paredness.” Zachary Goldfarb, BS, CEM, EMT-P,and Steve Oreck, MD, answered audience ques-tions. We paraphrased their remarks.
Who should serve as the incident com-mander during a hospital emergency?
First, make the incidentcommander a 24-hour-a-
day position. You don’t want toidentify the incident commanderby name but rather by title. Forexample, your plan might saythe following: “During businesshours, the chief nurse executiveserves as the incident comman-der. During off hours, the nursingsupervisor acts as the incident commander.” Thisway, the incident commander is always presentand can make instantaneous decisions.
The chief executive officer (CEO) is not a goodchoice as incident commander. During an emer-gency, a CEO tends to get out into the organiza-tion and touch base with staff, interact with media,and talk with patients. The incident commandermakes sure the operation is running smoothly andtackles problems as they arise.
We chose not to train our hospital per-sonnel at the [decontamination] opera-
tions level because we have a local certifiedhazmat team at our disposal. Do you thinkthis is a wise choice?
The chief executive officer(CEO) is not a good choice asincident commander. Duringan emergency, a CEO tends
to get out into the organization and touch
base with staff . . .
““
A:
Q:
Q:

Page 11Healthcare Security and Disaster Alert—March 2002 © 2002 Opus Communications, a division of HCPro
www.healthsafetyinfo.com
a victim gets into the “clean” area, you can per-form further triage.
How should a hospital deal with patientovercrowding during an emergency while
protecting its existing patient population?
First, separate the new patients from the cur-rent patients to avoid cross contamination of
diseases. Then, deal with overcrowding by lookingat where you can crowd patients into your facility.
No facility will have the excess capacity to handlenew patients without compromising the currentpatients in some way. Review your plans and fig-ure out where you can crowd people. Think aboutsuch things as using the cafeteria as a potential pa-tient care area. You may have to designate certainfloors for new patients, and try to transfer or dis-charge as many patients as possible during the crisis. Your plan should also include casualty col-lection points.
What is the role of the Red Cross in a disaster?
The Red Cross provides resources. It has ac-cess to logistic bases, experience with disaster
control, and can coordinate, and move informationaround the country to help find family membersoutside of town. It staffs shelters and will help sup-port an incident scene with rehabilitation resourcesand food. The Red Cross should be an externalresource of your disaster plan. Depending on thecommunity, it will also supply resources for theblood program. Other organizations within the com-munity perform this role, also. Within the communi-ty, look at the total pool of resources and determine
how best to allocate them.
Editor’s note: To obtain a copy of this audioconfer-ence, see our ad on p. 3 and call 877/727-1728 orvisit www.hcmarketplace.com.
About the speakers: Zachary Goldfarb, BS, CEM, EMT-P, is the prin-cipal of Incident Management Solutions, a NewYork–based emergency management consultingfirm that specializes in planning, training, and oper-ational leadership for emergencies and major disas-ter events. He is a member of the federal DomesticPreparedness Training Team, helping prepare firstresponders in the 120 largest cities in the countryto manage the medical consequences of terrorism.
Steve Oreck, MD, is clinical assistant professor ofsurgery at the University of Wisconsin School ofMedicine, Madison, WI. Oreck has extensive mili-tary experience, including five years in naval intelli-gence and more than 20 years as a medical officer.During his time in the service, he attended andplanned exercises around nuclear, biological, andchemical disasters.
Send us your questions!
If you have a question about health care sec-urity and disaster planning, pass it along to us and we’ll include it in one of HealthcareSecurity and Disaster Alert’s future Question& Answer columns. Send questions in writingto Ed Justen, associate editor, by✔mail to Healthcare Security and Disaster
Alert, 200 Hoods Lane, P.O. Box 1168,Marblehead, MA 01945
✔e-mail to [email protected] (put “Q&A” inthe subject line)
✔fax to 781/639-2982 (put your fax to theattention of Healthcare Security and Dis-aster Alert)
Q:
A:
A:
Q:
Telephone:781/639-1872,
Ext. 3432
E-mail:ejusten@
hcpro.com
Contact Associate Editor Ed Justen:
Questions? Comments? Ideas?

Page 12 Healthcare Security and Disaster Alert—March 2002© 2002 Opus Communications, a division of HCPro
Zachary Goldfarb, BS, CEM, EMT-PPresidentIncident Management Solutions, Inc.New York, NY
Mary Ann Leon-Graham, RN, MPH,CPHA-A, LHRMDirector of Risk ManagementPan American HospitalMiami, Florida
Steve MacArthurSafety consultantThe Greeley CompanyMarblehead, MA
Thom Clarke, RN, BSDirector Perioperative ServicesSt. Anthony HospitalPendleton, OR
Steven C. Dettman, BS, CHPADirector, Security and Visitor Support ServicesMayo Clinic HospitalPhoenix, AZ
Neal M. DrawasManaging director Kroll AssociatesNew York, NY
Sandra L. FreemanHR specialist Saint Vincent Health CenterErie, PA
Healthcare Security and Disaster Alert
Publisher/Vice President: Suzanne Perney
Group Publisher: Bob Croce
Associate Editor: Ed Justen, [email protected]
Healthcare Security and Disaster Alert is published monthly by Opus Communications, Inc., a division of HCPro, 200 Hoods Lane, Marblehead, MA 01945. Subscriptionrate: $347/year. • Postmaster: Send address changes to Healthcare Security and Disaster Alert, P.O. Box 1168, Marblehead, MA 01945. • Copyright 2002 Opus Communications, Inc., a division of HCPro. All rights reserved. Printed in the USA. Except where specifically encouraged, no part of this publication may be reproduced, in anyform or by any means, without prior written consent of Opus Communications or the Copyright Clearance Center at 978/750-8400. Please notify us immediately if you havereceived an unauthorized copy. • For editorial comments or questions, call 781/639-1872 or fax 781/639-2982. For renewal or subscription information, call customer serviceat 800/650-6787, fax 800/639-8511, or e-mail: [email protected]. • Visit our Web site at www.hcpro.com. • Occasionally, we make our subscriber list available toselected companies/vendors. If you do not wish to be included on this mailing list, please write to the Marketing Department at the address above. • Opinions expressed arenot necessarily those of HSDA. Mention of products and services does not constitute endorsement. Advice given is general, and readers should consult professional counselfor specific legal, ethical, or clinical questions. HSDA is not affiliated in any way with the Joint Commission on Accreditation of Healthcare Organizations.
Bonnie Michelman, CPP, CHPADirector of Police, Security and Outside ServicesMassachusetts General HospitalBoston, MA
Dr. Steven L. Oreck, MDUniversity of Wisconsin
Steve SchultzCorporate safety directorCape Fear Valley Health SystemFayetteville, NC
Earl Williams, HSPSafety CoordinatorBroMenn HealthcareBloomington, IL
Editorial Advisory Board
City preparation digestCity and county officials in San Antonio are seeking$66 million to finance their bioterrorism readinessplans, according to a report in the San Antonio Ex-press News. Officials consider the city a terrorist tar-get because it is the home to four military bases,many biomedical laboratories, and several trans-portation links to Mexico.
The proposal seeks the development of protocolsand cooperative agreements between local govern-ments, law enforcement agencies, and emergencyservice providers. Other plans call for the following:• A partnership among city, county, and suburban
communities to maintain a coordinated emergen-cy response office
• Appointment of a local homeland security chief
• The establishment of a suburban emergency op-erations center and a backup operations center
• The purchase of improved communicationsequipment
Keeping tabs on the statistics in Salt Lake City
Figure skating scores, ski jump distances, and lugetimes weren’t the only statistics under scrutiny atlast month’s Winter Olympic Games in Salt LakeCity.
Medical officials kept a close eye on influenza,gastrointestinal, neurological, and respiratory sta-tistics at the 35 primary care clinics throughoutthe fortnight using the Real-Time Outbreak Dis-ease Surveillance System. Scientists at the Bio-medical Security Institute, a joint association ofCarnegie Mellon University and the University ofPittsburgh, developed the system that shows ageographical display by ZIP code of the numberand types of symptoms reported.
Additionally, three epidemiological intelligenceofficers from the Centers for Disease Control andPrevention watched for unusual pathogens andoutbreaks of food-borne illnesses.