how can we make health homes work for the homeless?
DESCRIPTION
How can we make Health Homes work for the Homeless? Lessons from NYC HHC ’ s Chronic Illness Demonstration Project Maria Raven, MD, MPH, MSc Supportive Housing Network of New York Sept 23, 2011. Hospital to Home (H2H). SDOH-sponsored Chronic Illness Demonstration Project - PowerPoint PPT PresentationTRANSCRIPT

How can we make Health Homes work for the Homeless?Lessons from NYC HHC’s Chronic Illness Demonstration Project
Maria Raven, MD, MPH, MSc
Supportive Housing Network of New YorkSept 23, 2011

2
Hospital to Home (H2H)• SDOH-sponsored Chronic Illness Demonstration Project
– HHC holds one of six State Department of Health contracts
• Intensive care management and coordination for fee-for-service Medicaid patients at high risk for frequent hospitalization
• Care Management Teams based at three HHC Hospitals:• Bellevue, Woodhull, Elmhurst
• Enrolling patients since August of 2009– 368 currently enrolled (540 cumulative)– 51% enrollees homeless or precariously housed
Hospital to Home’s task
• Find and enroll SDOH identified high-risk, high-cost patients
• Intervene with the goal of reducing Medicaid expenditures (read: hospital admissions)
• Improve health and social outcomes• All for $291.50 per patient, per month• “Supportive housing without the housing”*
*John Billings

How we do what we do
• Outreach, find, enroll• Conduct in-depth assessment• Develop care plan with patient using
motivational interviewing techniques• Staff begin to work with patient, first on
immediate, then long-term goals– Social Workers supervise Community Based Care
Managers (1:25 patient ratio), full-time housing coordinator, some dedicated primary care
Homelessness and H2H
• We knew from pilot work that significant numbers of eligible patients would be homeless
• Partnerships with homeless services providers a priority
• SDOH/NYSHF monies used to fund fulltime Housing Coordinator
• No ability to have H2H enrollees prioritized for housing

Most H2H patients are homeless or unstably housed
• 37 % Housed– 2/3 rent/own, 1/3 in supportive housing
• 22% Homeless• 29% Non-permanent situation
– Institutionalized– Staying temporarily with friends/family or in transitional housing
• 12% did not report
• Of 99 Housing Coordinator referrals:• 16 housed• 20 stabilization bed/safe haven • 41 shelter/drop-in center • 52 HRA 2010Es submitted

Health system-housing partnerships are key to this work
• We need you and you need us. Patients need us both.
• Health system is entry (and underused intervention point) for homeless– Many have spent more time with us that you know!
• Partnerships improve communication, reduce care fragmentation, improve outcomes
• Poor planning and communication leads to PREVENTABLE re-admissions, higher health care costs, poor outcomes including death for most vulnerable.
• Un-housed patients delay getting care they need

H2H Partnerships
• Traditionally, health care folk have not intersected with housing folk: increasingly this is a necessity
• All parties came readily to the table– DHS, CUCS, Project Renewal, Common Ground, BRC
among others
• Targeted interventions tailorable to the individual patient, incorporate patient input
• For the homeless, housing generally top priority

H2H Case Study: Ms. W• Patient Overview:• 44 year old PR female, enrolled 9/09• Morbid obesity, IDDM w/
complications, HCV, HTN, CHF, renal insufficiency, asthma, tobacco, prior IVDU, depression, suicide attempts
• Homeless in shelter at enrollment – moved into supportive housing 12/8/09
• Frequent hospital admissions for high blood sugars and related infections
• Difficulty remembering to take all of her medications, depression impacted motivation for tx and attending appointments
• Post-Enrollment Activity:• Mobile phone, appointment
reminders, transportation assistance, moral support.
• Connected to H2H PMD, sub-specialists
• Mental health, substance abuse treatment & Smoking Cessation
• H2H Housing Coordinator assisted with housing placement
• SSI appeal and PA workforce decision• Home care referral and services
advocacy• Monthly H2H support groups,
Recovery Clinic and at her residence• Encouraged self care – not putting
others’ needs first• Active listening – validating her
feelings and experiences
Comparing 12 months pre-enrollment to 12 months post: 3 hospitalizations vs. 1, over 60K in Medicaid savings
Hospital to Home’s immediate future
• Originally, a demo slated to end in March 2012. – Evaluation would guide program’s future (or lack
thereof)• Now: anticipated Health Home conversion
November 2011• Eligibility criteria broadened, will no doubt
include even greater numbers of homeless and precariously housed
Translating H2H into HH for the homeless
• Mobile phone technology• Aggressive contribution to and tracking of
housing applications• Formal partnerships with housing organizations
to enable:– Bi-directional data sharing with patient
consent/assent– Patient tracking before and after housing placement– Patient co-management (what can we take off your
plate that makes sense?)– Group meetings for difficult cases
What we need to (really) move ahead
• More flexibility around housing qualifications and eligibility• Advocacy pre and post housing application submission:
maximize chance for success• More permanent housing stock with liberal criteria around
chronicity and co-morbidities• Private sector anyone?
• Formal connections and communication between the health and housing delivery systems– For both homeless AND those already in supportive housing
units– On-site services investments for some
• Better health care system integration

What do these patients cost…and are we making a dent?
• 263 H2H patients • Minimum of 6 months pre-enrollment data
and 6 months post-enrollment data• Average pre-enrollment cost to Medicaid, all
claims– $5,928.85– PER MONTH– $71,146 per patient per year

Are we making a dent?• Average post-enrollment costs to Medicaid
– $4,755.36 per person per month– $57,064.32 per person annually
• Annual per-person Medicaid savings if numbers hold:– $14,081.68 (20%)– Over $3.7 million total for 263 patients (includes program costs)
• If costs decreasing, likely that hospitalizations and ED are decreasing• Matters as risk shifts from Medicaid (under FFS) to MCOs• Matters because it’s likely a proxy for improved health

Homeless H2H patients
• Patient defined as homeless if referred to H2H housing coordinator– Only those currently homeless on street or in shelter
• 53 patients with at least 6 months of before and after data
• $4,281.99 per month pre-enrollment• $3,426.43 per month post-enrollment• $855.56 per month in per-person Medicaid
savings (20% savings)

Where do the savings come from?
• Reduction in inpatient visits– 0.68 per month to 0.36 per month– 47% decrease (a 27% decrease in inpatient costs)
• Reduction in ED visits (T&R)– 1.13 month to 0.53 per month – 53% decrease (a 30% decrease in ED costs)
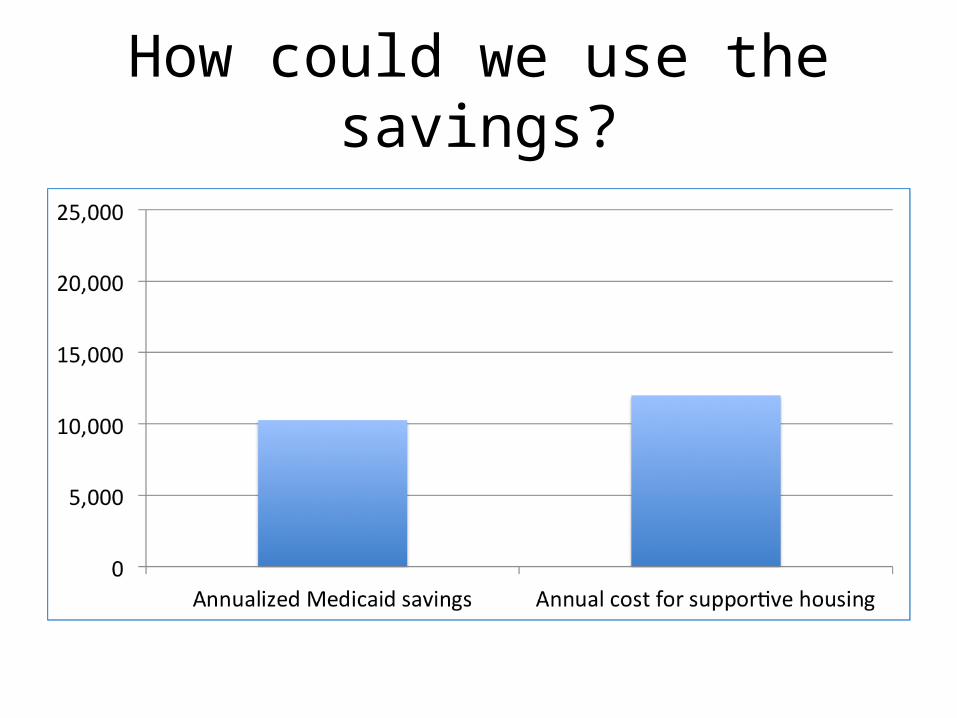
How could we use the savings?


Many Thanks• Supportive Housing Network of New York• Bellevue, Elmhurst and Woodhull Teams• The New York State Department of Health• John Billings, NYU• Common Ground Community• NYC Department of Homeless Services• New York State Health Foundation• United Hospital Fund• New York Community Trust• HHC Central Office leadership• Krista Olson and Yuriy Libster
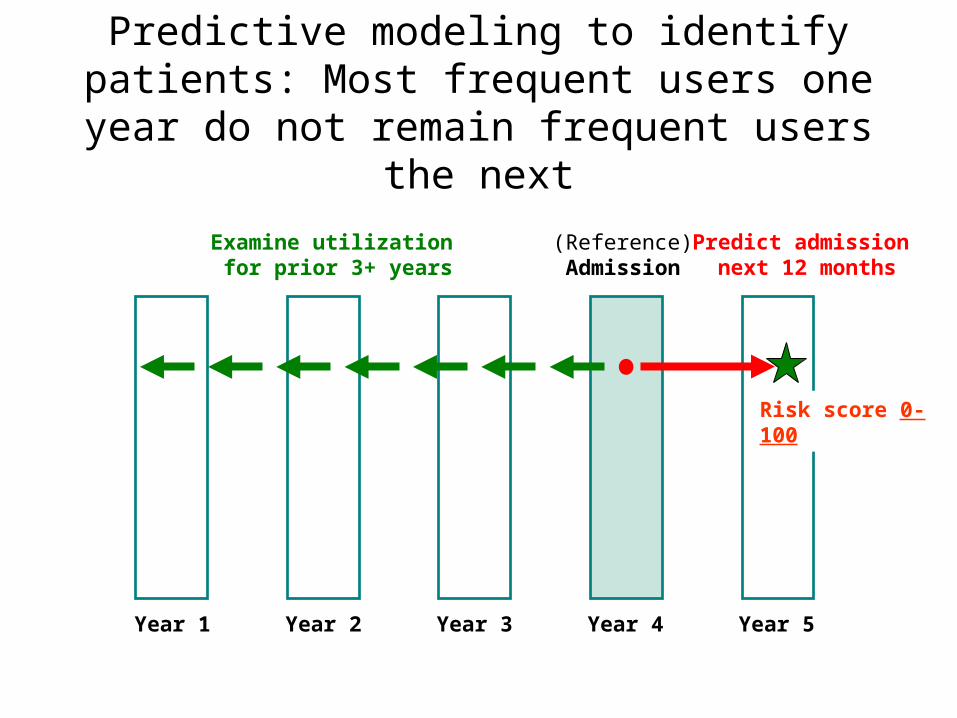
Predictive modeling to identify patients: Most frequent users one year do not remain frequent
users the next
(Reference)Admission
Examine utilization for prior 3+ years
Predict admission next 12 months
Year 4 Year 5Year 3Year 2Year 1
Risk score 0-100
Health Care?• Linkages to medical care• Accompany individual to appointments• Collaborate on discharge planning with inpatient teams
• Cell phone provision, support• Transportation assistance• Entitlements enrollment• Facilitate housing • Home visits/safety assessments• Reminder calls, alarm clocks, pill boxes• Support groups• 24- hour call line with our staff on other end• “Patient Necessities Fund”