housestaff training and consortium operations manual … · housestaff training and consortium...
TRANSCRIPT
HOUSESTAFF
TRAINING
and
CONSORTIUM
OPERATIONS
MANUAL
July 1, 2014
This manual supersedes all previously issued training manuals.
Core Manual July 2014 page 2
Table of Contents
FROM THE REGIONAL DIRECTOR OF MEDICAL EDUCATION ........................................................... 4
MEDICAL EDUCATION STAFF ............................................................................................................... 5
MISSION AND VALUES STATEMENT .................................................................................................... 6
HONOR AND INTEGRITY....................................................................................................................... 7
CHAIN OF COMMAND ............................................................................................................................ 8
INTRODUCTION TO THE TRAINING PROGRAM ................................................................................. 9
1. THE PBCGME CONSORTIUM: ................................................................................................... 10 2. THE HCA-AFFILIATED BASE FACILITIES OF THE PBCGME ....................................................... 10 3. OTHER AFFILIATED INSTITUTIONS ............................................................................................. 11
I. POLICY ON NONDISCRIMINATION; PROCESS AND CRITERIA FOR SELECTION OF
RESIDENTS/ORIENTATION............................................................................................................. 12
1. NONDISCRIMINATION: ................................................................................................................ 12 2. RECRUITMENT: .......................................................................................................................... 12 3. PROCESS: ................................................................................................................................... 13 4. ORIENTATION ............................................................................................................................. 13
II. GENERAL INFORMATION AND REGULATIONS ............................................................. 13
1. INTRODUCTION........................................................................................................................... 13 2. REQUIREMENTS .......................................................................................................................... 14 3. PROGRAM/CONTRACTS .............................................................................................................. 14 4. TRANSITIONS OF CARE ............................................................................................................... 15 5. ALERTNESS MANAGEMENT/FATIGUE MITIGATION .................................................................... 16 6. CLINICAL RESPONSIBILITIES ...................................................................................................... 16 7. TEAMWORK................................................................................................................................ 18 8. MOONLIGHTING ......................................................................................................................... 18 9. DEPARTMENTAL MEETINGS/COMMITTEES ................................................................................ 18 10. DIDACTIC PROGRAM .............................................................................................................. 18 11. NUTRITIONAL SERVICES/CAFETERIA/DOCTORS DINING ........................................................ 19 12. ELECTRONIC ACCESS ............................................................................................................. 19
III. EMPLOYMENT ....................................................................................................................... 19
1. SALARY.................................................................................................................................... 19 2. BENEFITS ................................................................................................................................ 20 3. TIME OFF: ABSENCES/LEAVE/HOLIDAYS/VACATIONS ............................................... 22
IV. PROFESSIONAL CONDUCT.................................................................................................. 25
1. PROFESSIONALISM, PERSONAL RESPONSIBILITY, AND PATIENT SAFETY.................................... 25 2. CONFIDENTIALITY...................................................................................................................... 28 3. SOCIAL MEDIA-HCA GUIDELINES ............................................................................................. 29 4. DRESS CODE ............................................................................................................................... 32 5. COMMUNITY SERVICE ................................................................................................................ 32
V. RESIDENT DOCUMENTATION ............................................................................................ 33
1. GENERAL ................................................................................................................................ 33 2. PORTFOLIO ............................................................................................................................ 34 3. CHARTING RESPONSIBILITIES/PATIENT MEDICAL RECORD ............................................ 34
VI. RESEARCH .............................................................................................................................. 39
VII. ADMINISTRATIVE MATTERS ............................................................................................. 40
1. DEFERMENT FORMS ................................................................................................................... 40 2. PAGERS/PARKING....................................................................................................................... 40 3. MAJOR DISASTER PLAN, HURRICANE PLAN AND FIRE PLAN ...................................................... 40 4. EVIDENCE-BASED MEDICINE ............................................................................................. 41
Core Manual July 2014 page 3
5. INTERNAL REVIEW............................................................................................................... 42 6. THE MEDICAL LIBRARY ...................................................................................................... 44 7. VISITING STUDENTS AND RESIDENTS .............................................................................. 45
VIII. ORGANIZATION ................................................................................................................. 46
1. LEADERSHIP .......................................................................................................................... 46 2. COMMITTEES......................................................................................................................... 47
IX. LEGAL STATUS OF HOUSESTAFF; HOUSESTAFF EVALUATION PROCESS; ............ 49
1. GENERAL INFORMATION ................................................................................................... 49 2. TERMINATION WITHOUT THE RIGHT TO APPEAL: ...................................................... 49 3. ACADEMIC DEFICIENCIES .................................................................................................. 51
APPENDIX I: CRITERIA FOR FACULTY APPOINTMENT FOR THE ASSUMPTION OF
TEACHING RESPONSIBILITIES ..................................................................................................... 54
APPENDIX II: RESIDENT WORK HOURS POLICY .................................................................... 56
APPENDIX III: RESIDENT SUPERVISION POLICY.................................................................... 57
APPENDIX IV: CODE OF CONDUCT .............................................................................................. 60
APPENDIX V: SUBSTANCE ABUSE POLICY ................................................................................. 63
APPENDIX VII: ENDIX VI: INSTITUTIONAL CORE COMPETENCY PLAN ............................ 67
Core Manual July 2014 page 4
FROM THE REGIONAL DIRECTOR OF MEDICAL EDUCATION Like Dr. Andrew Taylor Still, the founders of our originating institution, West Palm Hospital, believed that physical healing by itself is not enough. They believed, as we do today, that a person’s physical health is closely linked with his/her spiritual, emotional and mental well-being; and they sought to provide a place where each of these aspects of the whole person could find both healing and nurture. Today, more than 40 years later, the Palm Beach Consortium for Graduate Medical Education (PBCGME) is a multi-facility academic medical center and AOA-recognized consortium, with a passion for medical education. The faculty, staff and administration of PBCGME are committed to these same values, as well as to providing excellent medical care through state-of-the-art services, equipment and training. We are committed to the quality of care rendered to our patients, the quality of medical education provided to our students and housestaff and the quality of care that will be rendered to the patients of our students and housestaff, once they are independent practicing physicians. As a result of this commitment, the osteopathic Residency Training Programs at the Palm Beach Consortium for Graduate Medical Education, which includes West Palm Hospital, Palms West Hospital, St. Lucie Medical Center and University Hospital and Medical Center, offer the opportunity to treat our patients as a whole; and provide high quality, compassionate, cost-effective healthcare responsive to the needs of our patients, and community. At the PBCGME, we believe in evidence-based learning, competency-based evaluation and the philosophy that education, not service, is paramount to the success of our programs. We treat our housestaff first and foremost as learners, and provide education in settings that render the highest quality of care. We believe our Residency Programs – as well as our Externship Rotations – are among the finest available. We welcome you to the “PBCGME Team”, as you join a heritage of rigorous, challenging and high quality training, and become part of the success of our ongoing medical education endeavors. As part of our Team, you will enjoy the strong support of our company, hospital administration, program leadership and faculty. Many of programs’ attendings, DMEs, and even the Regional DME, are ourselves graduates of our training program. To us, this is more than “a job”; this is where we trained; this is family; this is home. As you embark on this year of training, we hope that every morning when you wake up the first thing you think of is how lucky you are to be able to help at least one patient that day, a person you encounter some manner of pain or suffering, and that you as a physician are uniquely positioned to help make their life better. This manual will acquaint you with the policies and procedures pertaining to PBCGME residency programs. It is important that all Housestaff review these pages and promptly address any questions you may have with your Program Director (PD), Director of Medical Education (DME), Chief Resident, Administrative DME, Regional Medical Education Coordinator, or me. With warm welcome,
Bradley S. Feuer, DO, JD, FCLM, FACFEI, FACOFP Regional Director of Medical Education (RDME) The Palm Beach Consortium for Graduate Medical Education (PBCGME)
Core Manual July 2014 page 5
Palm Beach Consortium for Graduate Medical
Education MEDICAL EDUCATION STAFF
Dept. of Medical Education Dept. of Medical Education Dept. of Medical Education Dept. of Medical Education PBCGME/West Palm Hospital PBCGME/Palms West Hosp PBCGME/St. Lucie Medical Center University Hosp & Med Center 2201 45
th Street 13001 Southern Boulevard 1800 SE Tiffany Drive 7425 N. University Drive
West Palm Beach, FL 33407 Loxahatchee, FL 33470 Port St. Lucie, FL 34952 Tamarac, FL 33321 561-863-3910 (phone) 561-784-3127 (phone) 772-398-1990 (phone) 954-724-6540 (phone) 561-881-4365 (fax) 561-784-3134 (fax) 772-398-1925 (fax) 954-724-6258 (fax)
Regional Director of Medical Education, PBCGME: Bradley Feuer, DO, JD, FCLM, FACFEI, FACOFP Director of Medical Education, PBCGME/West Palm Hospital: David Stern, DO, FACOI Associate Director of Medical Education, PBCGME/West Palm Hospital: Hal Bashein, DO, FACOS Director of Medical Education, PBCGME/St. Lucie Med Center: Thomas Matese, Jr., DO, FACP, FACEP Director of Medical Education, PBCGME/University Hospital & Medical Center: Marlene Caraballo,
DO, FAAHPM Program Director, PBCGME/Internal Medicine: David Stern, DO, FACOI Associate Director, PBCGME/Internal Medicine: Minerva Ellis, DO, FACOI Program Director, PBCGME/Dermatology: Robin Shecter, DO, FAOCD Associate Program Director, PBCGME/Dermatology: Andleeb Usmani, DO, FAOCD Chief Trainer, VAMC, PBCGME/Dermatology: Gabriela Lemoine, MD Program Director, PBCGME/Pediatrics: Alberto Marante, MD, FAAP Program Director, PBCGME/Emergency Medicine: Thomas Matese Jr., DO, FACP, FACEP Associate Program Director, PBCGME/Emergency Medicine: Josephin Mathai, DO Program Director, PBCGME/Family Practice: Robert Anderson, DO Program Director, PBCGME/Psychiatry: Ethan Kass, DO Administrative DME: PBCGME/Palms West Hospital, Consortium GME Coordinator: Joanne Guccio Administrative Director of Student Education, PBCGME: Francessca DellaSala Administrative DME, PBCGME/West Palm Hospital: Cara Cataldo Administrative DME: PBCGME/St. Lucie Medical Center: Crystal Raines Administrative DME, PBCGME/University Hospital and Medical Center: Ashley Zeidman, MSW Medical Education Coordinator, PBCGME/St. Lucie Medical Center: Monica Leighton Chief Executive Officer, PBCGME/West Palm Hospital: Dana Oaks Chief Executive Officer, PBCGME/Palms West Hospital: Eric Goldman Chief Executive Officer, PBCGME/St. Lucie Medical Center: Jay Finnegan Chief Executive Officer, PBCGME/University Hospital & Medical Center: Joseph Melchiode Chief of Residents; Chair, Resident Council: Jamie Bosma Groh, DO, FACOI Coordinator, PBCGME CISM Team: Shana Rissmiller, DO, FACOI Coordinator, PBCGME Community Service Programs: Tina Steinmetz, FACOI Coordinator, PBCGME Disaster Response: Jamie Groh, DO, FACOI Coordinator, PBCGME Resident Activities: Sarah Ferrer, DO, FACOI Palm Beach County Medical Society Liaison: Brent Schillinger MD
Core Manual July 2014 page 6
Palm Beach Consortium for Graduate Medical
Education
MISSION AND VALUES STATEMENT
Above all else, we are committed to the care that is rendered to the patients of our attendings, as well as that which will be provided to the patients of our graduates. In recognition of this commitment, we will strive to deliver high quality, cost-effective graduate medical education programs utilizing the resources of our hospitals, affiliated facilities, faculty and community. In pursuit of our mission, we believe the following value statements are essential and timeless:
• We recognize and affirm the obligation to our community to graduate the most highly-qualified physicians possible. • We will not graduate any individual whom we would not feel comfortable referring a loved one to. • We act with absolute honesty, integrity and fairness in the way we conduct our business and the way we live our lives. • We trust our colleagues as valuable members of our education team and pledge to treat one another with loyalty, respect, and dignity.
Core Manual July 2014 page 7
Palm Beach Consortium for Graduate Medical
Education
HONOR AND INTEGRITY
What is Expected of a PBCGME Graduate: Displays absolute integrity
Maintains clinical competence
Takes care of subordinates
Respects others
Is goal-oriented
Sets high standards for self
Possesses supreme confidence
Shows superb “people skills”
Chooses leadership over “managership”
Has high physical and mental drive
Holds the ability to choose the “harder right” over the “easier wrong”
PBCGME Principles of Leadership: Seek responsibility and take responsibility for your actions
The value of looking for more work-work of increased volume, accountability, and dependability
Resident's mission, simply put, is to find areas of additional responsibility
Residency is stressful, fun, emotional, hilarious, tiring and overall, unforgettable
PBCGME Honor Code: A resident will not lie, cheat, steal or tolerate those who do
Weigh all actions against:
Does this action attempt to deceive anyone or allow anyone to be deceived?
Does this action gain or allow the gain of a privilege or advantage to which I or someone else
would not otherwise be entitled?
Would I be satisfied by the outcome if I were on the receiving end of the action?
The Harder Right over the Easier Wrong: People frequently do not respond well to actions of pure integrity
Choose to say and do ethical things, rather than things people want to hear and see
Reap the benefits of pay me now or pay me later
A lie very often comes back to haunt you later on, in magnified form. End result is accusation,
criticism, and embarrassment much worse than anything that could have come from doing the
appropriate, truthful thing in the first place
Being Less Than Truthful is Addictive
Mentoring: Best “pearls” and most reassuring words are shared between residents of different levels.
No accomplishment is more rewarding than steering a younger resident through academic or
anxiety-relating hardship and seeing that resident make it into the next year.
Upperclassman takes underclassman as a friend and disciple, serving as trainer, listening post
and career advisor.
Core Manual July 2014 page 8
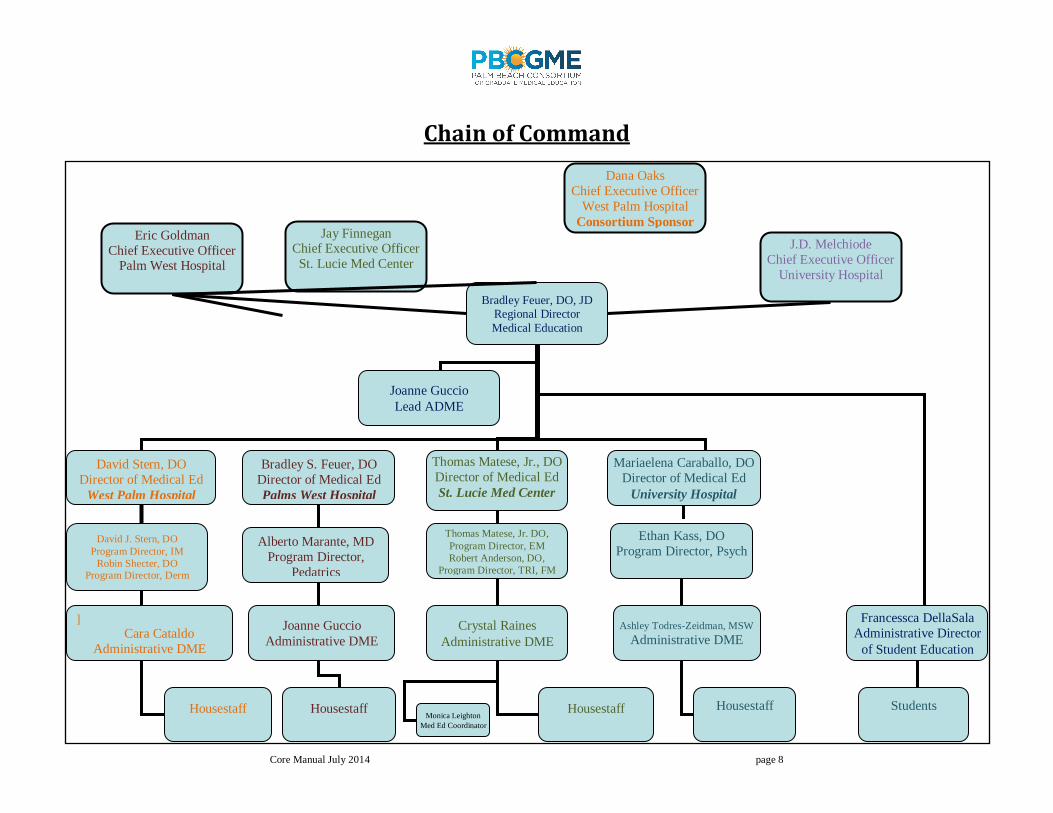
Chain of Command
Bradley Feuer, DO, JD Regional Director
Medical Education
David Stern, DO
Director of Medical Ed
West Palm Hospital
Bradley S. Feuer, DO
Director of Medical Ed
Palms West Hospital
Housestaff
Thomas Matese, Jr., DO
Director of Medical Ed
St. Lucie Med Center
Thomas Matese, Jr. DO,
Program Director, EM
Robert Anderson, DO,
Program Director, TRI, FM
Housestaff
Crystal Raines
Administrative DME
Mariaelena Caraballo, DO
Director of Medical Ed
University Hospital
Ethan Kass, DO
Program Director, Psych
Housestaff
Ashley Todres-Zeidman, MSW
Administrative DME
Francessca DellaSala
Administrative Director
of Student Education
David J. Stern, DO
Program Director, IM
Robin Shecter, DO Program Director, Derm
]
Cara Cataldo
Administrative DME
Housestaff
J.D. Melchiode
Chief Executive Officer
University Hospital
Eric Goldman
Chief Executive Officer Palm West Hospital
Joanne Guccio
Lead ADME
Students
Jay Finnegan Chief Executive Officer
St. Lucie Med Center
Alberto Marante, MD
Program Director,
Pedatrics
Joanne Guccio
Administrative DME
Monica Leighton
Med Ed Coordinator
Dana Oaks
Chief Executive Officer
West Palm Hospital
Consortium Sponsor
Core Manual July 2014 page 9
This is the Training and Operations Manual of the Palm Beach Consortium for Graduate Medical Education. Together with the program-specific material that follows, this document delineates the
policies of the Consortium and Training Programs. Unless otherwise stated herein, the only exceptions to these policies are those specifically authorized by the Consortium Graduate Medical
Education Committee.
INTRODUCTION TO THE TRAINING PROGRAM WELCOME TO THE PBCGME and to what we know will be rewarding years for you as a member of the housestaff team, as well as for those of us on the administration and faculty who have prepared these hospitals to be the finest osteopathic patient care and educational facilities in South Florida. Our goal is excellence in medical education, excellent quality of care of our patients, and excellent quality of care of your future patients. To this end, we aim to create knowledgeable, skilled, and compassionate physicians; your role in putting forth genuine effort to obtaining this goal is essential. Since the start of PBCGME training in 1982, the rule has been that the interns/residents are not to be over-worked and not to be exhausted. It is expected that the residents will have ample supervision to make sure that this exposure is an educational and not just a service program. From its inception, our programs have worked on the idea that, within a given year and across all years of training, collegiality was to be supportive. The residents are encouraged to help all their colleagues do the best and be the best that they can. The Department of Medical Education has an open door policy for residents to have access to leadership in addition to their assigned supervisors and attendings. These traits - faculty accessibility and attention to supervision of residents - have been stressed since the start of the program. Graduates from our training programs are highly sought after by fellowships, academic departments, employers, and colleagues nationwide. An outstanding, nearly perfect success rate on Part III of NBOME as well as in-service examinations and board-certification examinations attests to the goals of the training. PBCGME-trained physicians are regional, national, and international leaders in patient care, administration, education, and research. In the following pages of this manual, you will find the guidelines which the Department of Medical Education has established to help make these years an educational experience that we feel will properly prepare you for the practice of your chosen specialty. Since this manual cannot cover all situations with which you will be faced during the coming years, we expect you will approach these situations with mature and sound judgment. When in doubt, do not hesitate to ask a member of this Department, the Regional Director of Medical Education, Director of Medical Education, Program Director, ADME or the Chief Executive Officer. We are ready and willing to give you whatever assistance is necessary. The first year of residency training is the year in which medical school graduates learn to apply basic knowledge in the clinical practice of medicine. New Housestaff will find that during the first weeks they will be under rather complete supervision but as the year progresses the responsibilities will expand and individual initiatives will be encouraged in concert with demonstrated abilities. During the advanced years of training, Housestaff are expected to assume an ever expanding role in the care of our patients. This requires a continuous refining of skills to develop into the most highly-qualified physicians possible. This Manual is based on the PBCGME’s commitment to excellent patient care. It must be remembered that a resident program is a dynamic process which changes as the maturation of the physician occurs and as our hospitals and programs grow. It is recognized that the osteopathic concept and theory of practice provide the sound foundation upon which a successful professional career is constructed. To assure that all osteopathic residency programs are committed to and capable of delivering uniquely osteopathic postdoctoral training, the AOA requires affiliation with, and sponsoring by, an Osteopathic
Core Manual July 2014 page 10
Postgraduate Training Institute (OPTI). PBCGME is affiliated with the Consortium for Excellence in Medical Education, the OPTI of Nova Southeastern University. The Palm Beach Consortium for Graduate Medical Education is comprised of acute inpatient hospitals affiliated with HCA Healthcare, the nation’s leading provider of healthcare services. HCA is composed of locally managed facilities that include approximately 190 hospitals and 91 outpatient surgery centers in 23 states, England and Switzerland. 1. The PBCGME Consortium:
a. PBCGME is an osteopathic consortium consisting of a group of HCA East Florida Division
hospitals engaged in AOA approved training in multiple specialties. The involved training
hospitals are related in the same health system and each specialty functions only as a single
program with a single program description and program director in compliance with AOA
standards and is reviewed at on-site reviews as a single program. The programs and program
sites evolved initially as multiple individually approved programs at various sites within a
system, and came together as a consortium following approval by AOA.
b. PBCGME is a multiple specialty consortium with trainee groups based at separate institutions
in the consortium and with a rotation pattern for each group.
c. WEST PALM HOSPITAL is the one identified AOA accredited entity (HFAP accredited base
institution) that is ultimately responsible for the oversight and management of the
consortium.
d. Owned, operated and located within HCA’s East Florida Division, the organizational structure,
size and geographic area of the consortium lends itself to appropriate oversight and
supervision with a clearly identified structure for oversight and accountability. Each program
director has responsibility for the oversight of all aspects of the program, especially the
training and evaluation of all trainees.
e. Trainee contracts, benefits, academic requirements, and resources are standard for every
trainee within the consortium.
f. All participants in the consortium abide by AOA Basic Documents and Specialty College
Standards without exception.
g. All institutions active in the consortium as training sites belong to the same Osteopathic
Postdoctoral Training Institution.
h. Required program approval documentation and applications are filed for all sites as a total
program. Site specific information i.e. faculty, training conducted/objectives of training at each
site and department segregated totals are available to specialty colleges upon request.
i. Site reviews of multiple sites of consortia programs will be inspected reviewed
jointly/concurrently and citations at one site apply to the consortium as a whole.
j. Site directors are associate program directors located at each consortium training site for the
respective specialty. They are responsible to the approved osteopathic specialty program
director and must be certified in the respective specialty. Flexibility in credentials may be
allowed by the Specialty College and PTRC provided that the program director and DME meet
all the requirements.
k. To ensure the quality of the educational experience of the trainee in programs with multiple
sites, there are at least two residents in rotations at each training site.
2. The HCA-affiliated base facilities of the PBCGME include:
a. PBCGME/West Palm Hospital: West Palm Hospital is the HFAP-accredited AOA entity that is
ultimately responsible for the oversight and management of the consortium. The roots of PBCGME’s
passion for medical education stem from the long standing tradition of training excellence founded at
Core Manual July 2014 page 11
West Palm Hospital. West Palm Hospital is a 250-bed acute care facility (with an 88-bed psychiatric
Pavilion) accredited by the AOA as well as the Joint Commission. The first teaching hospital between
Miami and Orlando, West Palm Hospital has been actively involved in osteopathic medical education
since it was founded, in 1975. With an experienced, motivated, and energetic teaching staff, West
Palm Hospital boasts excellent didactics in addition to strong clinical rotations with ample opportunity
for “hands-on” experience. West Palm Hospital is the base for Internal Medicine residency training,
and fellowship in Dermatology.
b. PBCGME/Palms West Hospital: Palms West Hospital is a 204 bed acute care facility located in a
younger population area of Palm Beach County, which is among one of the fastest growing
communities in the country. Palms West Hospital and the Children’s Hospital at Palms West currently
host premier residency training in Pediatrics.
c. PBCGME/St. Lucie Medical Center: Located a few miles inland from The Treasure Coast beaches,
St Lucie Medical Center serves Florida’s vibrant and rapidly growing Treasure Coast community. SLMC
is a 229-bed acute-care, full service medical center which is the first teaching hospital on the Treasure
Coast. With a high emergency room volume and outstanding staff, this prestigious medical center is
accredited for osteopathic residency training in Emergency Medicine, Family Practice and a Traditional
Rotating Internship.
d. PBCGME/University Hospital and Medical Center: University Hospital’s is a 317-bed hospital with
a free standing state of the art behavioral health facility. The Pavilion features four units with 30 semi-
private patient rooms, cafeteria, gym, pool, and indoor and outdoor group areas. In partnership with
the West Palm Beach VA Medical Center, University Hospital and Medical Center hosts PBCGME’s
Psychiatry Residency Training Program.
To enhance the quality of care rendered in our facilities, as well as the academic programs offered to our students and Housestaff, The Palm Beach Consortium for Graduate Medical Education has formed strategic alliances with some of the area and world’s finest healthcare organizations. All institutions participating in the training of Housestaff have an affiliation agreement with the Palm Beach Consortium for Graduate Medical Education.
3. Other Affiliated Institutions include: a. NSUCOM/Consortium for Excellence in Medical Education (OPTI): High-tech compressed video
equipment provides our programs with real-time access between each of our facilities, as well as between our hospitals and Nova Southeastern University’s College of Osteopathic Medicine and the other hospitals within NSUCOM’s Consortium. NSUCOM students may spend their third year of training in core clinical rotations at PBCGME.
b. Kansas City University of Medicine and Biosciences: A primary affiliate for core medical student rotations, PBCGME is an affiliate member of KCUMB’s OPTI.
c. Philadelphia College of Osteopathic Medicine: A primary affiliate for core medical student rotations, PBCGME accepts core medical students from GA-PCOM for their entire third year of training.
d. Veterans Administration Medical Center: The West Palm Beach VA provides health care to eligible veterans in a seven-county area along Florida's Gold and Treasure Coasts. Comprehensive services include medical, surgical and psychiatric inpatient care and outpatient services in each specialty. In addition, extended care services offer community residential care, adult day health care, respite and hospice in addition to nursing home care. The VA Medical Center has partnered with PBCGME to support our Internal Medicine, Dermatology, and Psychiatry.
e. JFK Medical Center: An HCA-affiliate, JFKMC hosts ACGME-residencies through the University of Miami, providing outstanding didactic opportunities for our housestaff.
f. Plantation General Hospital: An HCA-affiliate, PGH offers inpatient opportunities to PBCGME including Neonatal Intensive Care.
Core Manual July 2014 page 12
g. Lawnwood Regional Medical Center: Lawnwood Regional Medical center has the only Level II Trauma Center, Level III Neonatal Intensive Care Unit as well as the most experienced Heart Center on the Treasure Coast. Soon to be opening the only Pediatrics Emergency Department, Lawnwood is the site of Trauma training for our emergency medicine residency.
h. Miami Children’s Hospital: A world-renowned facility, Miami Children’s is affiliated with PBCGME for the purpose of training Pediatrics and Dermatology residents.
i. Florida Atlantic University: Recently accredited for a new four-year allopathic medical school, Florida Atlantic University’s high-tech Simulation Laboratory provides training for our Housestaff in Advanced Life Support, and Pediatric Advanced Live Support.
j. Florida Community Health Centers: Florida Community Health Centers (FCHC) provides continuity of care training sites for some of our pediatrics residents. FCHC is a leader in Florida’s primary and preventive health services, providing services through a network of health centers surrounding Lake Okeechobee in South-Central Florida. FCHC is designated as a Federally Qualified Health Center (FQHC) and is accredited by The Joint Commission.
k. Treasure Coast Community Health: Also a Federally-Qualified Community Health Center, Treasure Coast provides accessible, cost-effective, high quality, comprehensive healthcare to all persons, regardless of socio-economic circumstances, throughout Indian River County. Serving in excess of 15,000 patients, Treasure Coast provides outpatient rotations to our family medicine residents.
l. Foundcare: Foundcare, Inc. is a community health center located in the heart of Palm Beach County. The Health Center began operations in January 2004 and has since grown rapidly in response to the high level of community need for accessible, affordable, high-quality healthcare. Foundcare provides opportunity for clinical training in our Pediatrics and Dermatology programs.
I. POLICY ON NONDISCRIMINATION; PROCESS AND CRITERIA FOR
SELECTION OF RESIDENTS/ORIENTATION
1. Nondiscrimination: Equal employment opportunities are provided to all employees and applicants for employment without regard to race, color, religion, sex, national origin, age, disability, sexual orientation, genetic information or status as a Vietnam-era or special disabled veteran in accordance with applicable federal laws. This policy applies to all terms and conditions of employment, including, but not limited to, hiring, placement, promotion, termination, layoff, transfer, leaves of absence, compensation, and training. Genetic information includes information about an individual’s genetic tests, genetic tests of a family member, and family medical history. Genetic information does not include information about the sex or age of an individual or the individual’s family members, or information that an individual currently has a disease or disorder. Genetic information also does not include tests for alcohol or drug use. This policy expressly prohibits any form of unlawful employee harassment based on race, color, religion, sex, national origin, age, disability, sexual orientation, genetic information, status as a Vietnam-era or special disabled veteran, or status in any group protected by state or local law. Improper interference with the ability of employees to perform their expected job duties is not tolerated. The interpretation of this or any Human Resource policy rests with the PBCGME facility’s Human Resource Department which-o reserves the right to modify change or discontinue the policy at any time. 2. Recruitment: Recruitment is conducted following the policies and procedures of the AOA Match Registration Program. All appointments are made through that program. PBCGME does not attempt to impose local requirements to supersede the AOA Matching Program. Housestaff are accepted into the program following an application through the Electronic Residency Application System (ERAS) and a successful interview process.
Core Manual July 2014 page 13
Admission to PBCGME training programs is not influenced by race, color, sex, religion, creed, national origin, age, or handicap. The program only enrolls graduates of AOA-Accredited Colleges of Osteopathic Medicine. They must be and remain members in good standing of the AOA. 3. Process: a) Submission of a resident application through ERAS and the required documentation which will include,
but not be limited to, two letters of recommendation, transcripts from an approved College of
Osteopathic Medicine, dean's letter of recommendation, and scores from the National Board of
Osteopathic Medical Examiners.
b) Periodic review by the program of files and notification of prospective resident regarding his/her
required document status.
c) Interview of selected resident candidate by the Regional Director of Medical Education, Director of
Medical Education, Program Director and/or one or more members of the Medical Education or
Curriculum and Advancement Committee.
d) Evaluation of resident based upon all available objective and subjective material and impressions. A
written evaluation is completed.
e) Selection of the most capable and competent candidates as determined by the Regional Director of
Medical Education, Director of Medical Education, Program Director and/or Medical Education
Committee. Applicants who have not passed both Part II sections of the NBOME COMLEX
examination should not be eligible for ranking.
f) Completion of the match rank form for the Registration Program of the AOA (First-year residents only). g) Submission of all forms to the National Match Registry by deadline (First-year residents, only). h) Execution of the residency contract in accordance with the terms and time requirements of the AOA
and National Residency Match Program.
i) PBCGME will execute the contract and forward an original back to the resident.
j) If all funded positions are not filled through the match program, then PBCGME will attempt to fill those
positions from a listing of non-matched students.
4. Orientation The orientation program exposes the resident to the culture and functions of the PBCGME System and is conducted prior to the first day of the residency. The resident will be introduced to various individuals such as administration officials, representatives of affiliated facilities and managers of various patient care disciplines. The hospital’s rules and regulations, benefits, human resources policies, advanced directives information, health sciences (library) services, risk management procedures, and health information management (medical records) systems will be explained. Orientation is mandatory for existing and incoming residents.
II. GENERAL INFORMATION AND REGULATIONS
1. Introduction Residency is an essential dimension of the transformation of the medical student to the independent practitioner along the continuum of medical education. It is physically, emotionally, and intellectually demanding, and requires longitudinally‐concentrated effort on the part of the resident. The specialty education of physicians to practice independently is experiential, and necessarily occurs within the context of the health care delivery system. Developing the skills, knowledge, and attitudes leading to proficiency in all the domains of clinical competency requires the resident physician to assume personal responsibility for the care of individual patients. For the resident, the essential learning activity is interaction with patients under the guidance and supervision of faculty members who give value, context, and meaning to those interactions. As residents gain experience and demonstrate growth in their ability to care for patients, they assume roles that permit them to exercise those skills with greater independence. This concept—graded and progressive responsibility—is one of the core
Core Manual July 2014 page 14
tenets of American graduate medical education. Supervision in the setting of graduate medical education has the goals of assuring the provision of safe and effective care to the individual patient; assuring each resident’s development of the skills, knowledge, and attitudes required to enter the unsupervised practice of medicine; and establishing a foundation for continued professional growth.
2. Requirements All Housestaff must:
a) Abide by the rules, regulations, and policies established by PBCGME, its hospitals, departments, affiliates, the residency program director, and the director of medical education throughout the course of the training program. This includes, but is not limited to, the provisions of this manual including the Code of Conduct.
b) Observe the curriculum requirements as designated by the AOA, specialty college and PBCGME, performing all duties assigned by the Institution to him or her to the best of his or her ability, maintaining standards of professional competence as determined by the PBCGME and the Residency Program, and conducting himself or herself in a professional manner at all times.
c) Attend and participate in all rotations, lectures, educational experiences, and other assigned responsibilities, tasks and schedules. This includes participation at “out rotation sites” at the discretion of the Program Director and DME.
d) To maintain current registration with the State of Florida as an Osteopathic Physician in Training, certification as required by the program (such as CPR and ACLS), and membership in Florida Osteopathic Medical Association, AOA, and national and state specialty societies (of the field in training). The fees required to maintain such registration or membership requirements will be paid directly by the Institution or reimbursed to the Intern/Resident/Fellow upon submission of satisfactory documentation of payment by Intern/Resident/Fellow. To register for Medicare, Medicaid, and other required third party payment programs if/when requested.
e) Be available for rotations during regularly scheduled rotation hours. Further be available to do alpha/bravo 12-24 hour shifts in the event of natural or other disasters.
f) Complete and submit monthly logs, annual report, scientific paper and all other documentation in the time frames required by the program.
g) Document osteopathic biomechanical examinations on all assigned patients of osteopathic physicians, and to regularly provide patients with osteopathic manipulative treatment, when indicated.
h) Sign an Agreement of Extension of Training for maternity leave, illness, or any other extenuating circumstance that would prevent the Resident from completing the required fifty-two (52) weeks of training during the contract period. Part of this Agreement would include preference of receiving all pay during the extension period and none during the leave. This assumes the extension would be anticipated to last no greater than one hundred twenty (120) days.
i) Reside within thirty (30) minutes driving time of the resident training program’s base hospital. j) Engage, during the term of the residency, only in such activities of a professional nature as are
approved by the PBCGME and the AOA, it being understood that such activities shall include compliance with institutional and AOA work hour policies to include all policies regarding moonlighting. To refrain during the entire term of the residency from engaging or participating in any nonprofessional activities that would potentially or actually interfere with the Resident/Fellow’s effective performance of their contract.
k) Attend/complete annual hospital in-service updates (presented during our department’s annual orientation of new Housestaff, as well as online); attend annual Ethics refresher courses (offered during the academic year) and have annual history and physical exams including PPD (unless contraindicated) prior to start of new academic year.
l) Put his/her full efforts into his/her residency program. When permitted by program policy, outside remunerative work must not interfere with his/her residency program activities.
m) To further fulfill any and all obligations as stipulated in the resident/fellow agreement.
3. Program/Contracts The terms and length of residency training programs are in accordance with AOA and specialty
Core Manual July 2014 page 15
college basic standards. The term and length of the residency contract is one (1) year. Factors that
will be taken into consideration for a resident to be given a contract for any successive year
include, but are not limited to:
a) Academic Performance
b) Professionalism
c) Teamwork
d) Performance on annual in-service exam
e) Compliance with terms of this residency manual
4. Transitions of Care
PBCGME programs design clinical assignments to minimize the number of transitions in patient care. Accordingly, programs ensure and monitor effective, structured hand‐over processes to facilitate both continuity of care and patient safety, ensure that residents are competent in communicating with team members in the hand‐over process, and ensure the availability of schedules that inform all members of the health care team of attending physicians and residents currently responsible for each patient’s care. In addition to resident-to-resident patient transitions, residents must care for patients in an environment that maximizes effective communication among all individuals or teams with responsibility for patient care in the healthcare setting. Policy a) Each training program will review call schedules at least annually to minimize transitions in patient
care within the context of the other duty hour standards. Whenever possible, transitions in care
should occur at a uniform daily time to minimize confusion. Documentation of the process involved in
arriving at the final schedule should be included in the minutes of the annual program review
meeting.
b) Each residency training program that provides in-patient care is responsible for creating a templated
patient checklist and is expected to have a documented process in place to assure complete and
accurate resident-to-resident patient transitions. At a minimum, key elements of this template should
include:
-rays;
sues with a "to do" list including follow up on laboratory and X-rays;
d depending upon the specialty.
c) There must be a structured face-to-face, phone-to-phone, or secure intra-hospital electronic handoff
that occurs with each patient care transition. At a minimum this should include a brief review of each
patient by the transferring and accepting residents with time for interactive questions. All
communication and transfers of information should be provided in a manner consistent with
protecting patient confidentiality.
d) Each training program is responsible for notifying their hospital’s telephone operators about its call
schedule so that the entire health care team (staff physicians, residents, medical students, and
Core Manual July 2014 page 16
nurses) know how to immediately reach the resident and attending physician responsible for an
individual patient's care.
e) Each residency training program is responsible for assuring its residents are competent in
communicating with all caregivers involved in the transitions of patient care. This includes members
of effective interprofessional teams that are appropriate to the delivery of care as defined by their
specialty residency review committee. Methods of training to achieve competency may include GME
orientation sessions, annual review of the program-specific policy by the program director with the
residents, departmental and GME conferences, and on-line training activities.
5. Alertness Management/Fatigue Mitigation PBCGME programs, faculty and residents: a) Are vigilant to the signs of fatigue and sleep deprivation;
b) Consider fatigue mitigation processes to manage the potential negative effects of fatigue on
patient care and learning, such as naps or back‐up call schedules.
c) Have processes, formal or informal, to ensure continuity of patient care in the event that a
resident may be unable to perform his/her patient care duties, and provide adequate sleep facilities
and/or safe transportation options for residents who may be too fatigued to safely return home.
6. Clinical Responsibilities a) The clinical responsibilities for each resident are based on OGME‐level, patient safety, resident
education, severity and complexity of patient illness/condition and available support services.
b) Resident services to patients at the Hospital are provided without cost or obligation to such
patients. Housestaff may not accept payment for services, nor tips or gifts from patients or faculty.
c) Housestaff are responsible for seeing that their patients are receiving medications/treatments
which are ordered and that other aspects of management are not being neglected.
d) Housestaff should see that their patients are comfortable, able to sleep, and that complaints of
patients and their family members are conveyed to the attending physician and proper personnel.
e) Housestaff are to evaluate patients immediately when notified by the nurse of a change in the
condition of the patient.
f) Housestaff may institute emergency treatment in an emergency situation as outlined above. This
should be noted in the progress notes of the patient chart. Housestaff are responsible for notifying
the attending physician of any complications or change in patient condition. Conversations with
attendings regarding patients seen on house coverage should be documented in the medical
record. Remember, “If it’s not documented; it’s not done!”
g) Housestaff should be familiar with their patients so that they anticipate the development of
complications or unusual occurrences and notify the attending physician immediately.
h) Housestaff should give osteopathic treatments when indicated and appropriate, and approved by
the attending physician. All OMT procedures should have an appropriate order, and be recorded in
the progress notes.
i) When on duty, housestaff must immediately see all patients after admission and make a suitable
examination to ascertain the severity and nature of each patient's condition.
j) Complete and appropriate examinations, including rectal examination when indicated and
appropriate, must be performed on all patients. A witness must be present for rectal and vaginal
examinations.
k) Housestaff are expected to review all radiographic images as well as radiographic reports, reports
all other reports and consultations, and laboratory work on their own patients once those reports
and findings are available. Housestaff must strive to be proficient in performing venipunctures and
other procedures pertinent to the rotation and specialty. This proficiency is best achieved by
performing a number of these procedures... Housestaff should keep in mind that, once they are in
Core Manual July 2014 page 17
private practice, allied medical personnel are likely to turn to them for help with “difficult sticks”!
l) Housestaff are expected to visit other services to review interesting cases as they develop. An
updated “most interesting finding” and/or “most interesting patient” list should be maintained in
the housestaff lounge always being cognizant of patient and medical information confidentiality.
m) Housestaff are not to leave until the work for the day has been completed or turned over to a
colleague. It is expected that housestaff will assist each other as workloads and duty-hour limits
vary. Each Housestaff member is primarily responsible for the entire chart on his or her service.
Over weekends, service admissions (as defined by the DME and/or Program Director), history and
physicals may be performed by the housestaff on call.
n) Housestaff should be located at their assigned service at all times. Housestaff should not leave the
building or rotation during assigned time without specific permission from the Program Director or
his/her designee. When leaving the building during an inpatient rotation, housestaff should inform
the attending and other residents, so that there will not be unnecessary paging or delay in patient
care. Whether in or out of the house (other facility or physician’s office) residents must notify the
office of Medical Education when they will not be located at their assigned service. This includes
times when attendings have off, Housestaff become sick, or other pressing matters arise.
o) When a death occurs and an autopsy is to be performed, housestaff are expected to attend the
autopsy if in house, and encouraged to attempt arrangements to attend if at the medical examiner.
Housestaff are expected to assist in speaking with family members and obtaining permission for
organ donation or performance of the autopsy.
p) The position of house staff physician entails provision of care commensurate with the house staff
physician’s level of advancement and competence, under the general supervision of appropriately
privileged attending staff. Specifically, the Housestaff are expected to:
i. Develop a personal program of self-study and professional growth with guidance from teaching
staff.
ii. Participate in safe, effective and compassionate patient care under supervision.
iii. Participate completely in the educational activities of the program and, as required, assume
responsibility for teaching and supervising junior Housestaff, and medical students.
iv. Participate in institutional programs and activities involving the medical staff and adhere to
established practices, procedures and policies of the institution.
v. Participate in institutional committees and councils, especially those that relate to patient care
review activities.
vi. Develop an understanding of ethical, socioeconomic and medical legal issues that affect health
care practice and of how to apply cost containment measures in the provision of patient care.
vii. Work harmoniously with other members of the health care team.
viii. Complete, in a timely manner, all responsibilities with respect to medical records
q) If covering house and called to an accident or unusual occurrence within the Hospital, it is
imperative that housestaff who receive the call see the patient immediately, and determine,
through actual examination, the extent of the injury.
r) In the event of an accident to a patient, visitor, or employee, proper incident reports must be
completed. Included on this report should be an accurate description of the accident, time,
location, circumstances, etc. The patient's primary physician should be notified of the situation.
This is normally initiated through the nursing station but remains your obligation.
s) Attending physicians are to be contacted one week prior to the start of all rotations
i. In the case of two-week or half-month rotations, both attendings are to be called prior to the start of the month.
ii. If the attending is on vacation, or otherwise unavailable, the medical education office is to be notified for rotation assignment.
Core Manual July 2014 page 18
7. Teamwork Residents must care for patients in an environment that maximizes effective communication. This includes the opportunity to work as a member of effective interprofessional teams that are appropriate to the delivery of care in the specialty.
8. Moonlighting
The Residency Programs at PBCGME are full time employment commitments that challenge the resident to grow and mature in medical knowledge, clinical experience, and personal skills that are necessary for the capable practice of medicine. Accordingly, with the exception of housestaff who have already achieved primary care certification and are enrolled in a PBCGME fellowship program, residents are not permitted to moonlight. While still a privilege, in order to maintain competency skills moonlighting will be allowed for fellows, who have already achieved primary care certification, to moonlight only in the field of their primary certification, not the fellowship in which they are currently training. This privilege will be limited to fellows who are performing very well in their current program. At no time may moonlighting activities conflict with or diminish the fellow’s responsibilities to the residency program. Outside employment (moonlighting) by fellows may be done only with approval of the Program Director who will assure that no conflicts exist with the program requirements. Approval further requires the endorsement of the DME and Regional DME. Professional liability coverage provided to residents does NOT extend to moonlighting activities.
9. Departmental Meetings/Committees Housestaff may be invited, on an individual and/or rotating basis, to attend hospital committee meetings involved with patient care review; e.g. issue/Tumor/Transfusion Committee, ER Committee, ICU Committee, Medical Education Committee, Quality Assurance, Osteopathic Methods & Concepts Committee, Medical Records Committee.
Housestaff will attend all department meetings of their specialty training, All Housestaff are required to attend and sign in. Housestaff may be excused if the Chair deems that an issue or topic is sensitive and inappropriate for discussion in the presence of Housestaff. Housestaff should refrain from commenting at these meetings unless directly addressed by the Chair. Since these meetings may address patient care, QA or other matters dealing with protected speech, Housestaff must refrain from outside conversations pertaining to these meetings
10. Didactic Program While it may vary from program to program, lectures are generally held weekdays at 7:15 AM and at 12:30 PM. Various journal clubs, book clubs and grand rounds are held monthly. Other lectures, including those given consortium-wide, will cover various aspects of outpatient and inpatient medicine and other aspects of medical practice in today’s health care arena. This will include, OMM, Managed Care, Behavioral Medicine, Office Management, Finances, Billing, and Computers. ALL Housestaff are expected to attend ALL lectures for their program when rotating in house or nearby. If mitigating circumstances warrant an absence or tardiness, such must be reported to the Administrative DME and the Chief Resident. Absences will be addressed by the Program Director and DME, and may require extra call to be taken, or papers to be written. An official sign-in sheet is to be completed and signed by all of those in attendance. This sheet is to be returned to the Medical Education Office. The lecture schedule will be prepared, distributed, and posted by the Medical Education Office. Penalties for unexcused absences from didactics include:
i. 1st
unexcused absence: present a PowerPoint lecture (topic assigned by chief resident or Program Director)
ii. 2nd
unexcused absence: extra night of call or extra work shift
Core Manual July 2014 page 19
iii. 3rd unexcused absence: fail rotation NOTE: Three unexcused absences will result in failure of the current rotation. Programs should also develop a resident-led, backup lecture policy, in case an attending does
not show for scheduled lecture. For example: i. 1st 6 months: Administrative resident with 1st-year resident
ii. 2nd
6th
months: Administrative resident with 1st
year resident or student
11. Nutritional Services/Cafeteria/Doctors Dining The primary objective of the Hospital's Nutritional Services Department is the preparation and distribution of patient diets. Its secondary obligation is to serve meals to the employees and professional staff of the Hospital while on duty (this does not include family members). The cafeteria is open to employees, professional staff, house staff, and Housestaff according to the schedule posted in the department. Meals are provided at no charge to all Housestaff while on duty in the hospital. This is a privilege that should not be abused. All food is to be consumed in the cafeteria, with the exception that food may be brought into classrooms during lecture, and under mitigating circumstances. It is the responsibility of the person bringing the food in to remove all debris. No food is to be taken out of the hospital or distributed to other family, friends, or staff members. Family members are not provided food. One helping per meal-time is provided. Specialty items, such as bottled beverages and frozen desserts are not complimentary. In the event of an unavoidable delay in adhering to Cafeteria time schedule (i.e., delayed in Emergency Room, Surgery, or with a critical case), it is recommended that housestaff contact (or have someone contact) the Nutritional Services Department prior to closing time and request that a tray be prepared and set aside. Arrangements should be made for meals, for night duty, through the medical education department. Doctors Dining Areas:
i. Housestaff may obtain their food through the doctor’s dining room, without eating there, in the rare case that they are late for a lecture and there is a substantial line in the main cafeteria.
ii. If there is no lecture at that time, Housestaff are allowed to sit and dine in the company of, and at the request of attending physician in the physician dining room.
iii. Senior residents (final year of training) and Fellows are allowed to dine in the physician dining room.
12. Electronic Access Work related electronic login information is to be considered CONFIDENTIAL. At no time may Interns/Residents/Fellows share any work-related login information, (including, but not limited to CPOE, Meditech and Outlook access) with anyone else, or use another’s information. Sharing of one’s login information, use of another’s login information is grounds for immediate dismissal from the program.
III. EMPLOYMENT
1. SALARY OGME-1 salary is $46,500 per year, OGME-II salary is $48,000 per year, OGME-III salary is $50,000 per
year and OGME-IV (emergency medicine and Psychiatry) is $52,000 per year. Fellowship salary is
program-dependent.
Core Manual July 2014 page 20
2. BENEFITS a) GENERAL: PBCGME will provide the resident with:
i. Two (2) white medical lab coats, or two (2) sets of scrubs, or one coat and one
set of scrubs. Note: The Graduate Medical Education Committee may, from
time to time, elect to purchase additional attire for residents in order to serve
the needs of our program or hospitals.
ii. A pager and on-call system if required by program needs.
b) EXPENSES: An annual continuing education allowance, subject to advance approval by the
DME, as follows:
1. Traditional Intern $0.00
2. OGME-1 $300.00
3. OGME 2-4* $1,000.00
*Dermatology Fellows are not eligible for Education Allowance
i. CME allowance of $300 for OGME-1 (excluding Traditional Rotating Interns),
$1000.00 for OGME-2 and above residents will be reimbursed for CME expenses,
approved medical reference texts approved by the DME, professional society
membership, licensure (State of Florida), DEA registration or attendance at
approved CME conferences. Other educational references or tools may be
approved at the discretion of the Regional DME. Traditional Rotating Interns do
not get reimbursed for CME expenses. Expenses must be approved by the DME
and Program Director in advance to qualify for CME reimbursement. ORIGINAL
RECEIPTS are required. If scheduling travel, it is important that housestaff
contact the Medical Education Office for information regarding reimbursement.
AIR TRAVEL ARRANGEMENTS MUST BE BOOKED BY YOUR ADME IN
ACCORDANCE WITH HCA TRAVEL POLICY. Accounting will not issue
reimbursement checks without the required documentation and approval of the
Medical Education Department. Submit to the Department of Medical Education
all receipts, airline ticket stubs (ordinarily, all air travel should be made through
our corporate travel partner, and will be paid directly), hotel bill, meeting
registration form (with cost of conference on it), mileage, car rental (if
appropriate and necessary), and agenda of conference as soon as possible after
returning. Allow four to six weeks for payment.
ii. Funds may not accumulate from the one year to the next, and all funds must be
expended no later than sixty (60) days prior to completion of the academic
training year.
iii. In the normal course of training, there may be occasions in which the Director of
Medical Education desires the resident to incur an expense, such as attendance
at a conference, or purchase of study material, which will inure to the benefit of
the overall program, and/or educational experience. In such circumstance, and
with prior direction from and approval by the Director of Medical Education, the
resident will be eligible for reimbursement of that expense, without having to
use their allowance, upon submission of proper documentation.
c) MEMBERSHIP: Housestaff are required to become a member of the American Osteopathic
Association, and the specialty college of their field of training. Program Directors, with the
consent of the Regional DME, may require further memberships. Dues for these
memberships will be provided by the residency programs’ PBCGME base facility. Failure to
hold membership in the AOA and the osteopathic specialty college during residency will
result in loss of credit for training. Therefore these must be applied for immediately upon
Core Manual July 2014 page 21
entering the program. As soon as they are in receipt of these membership cards, housestaff
should provide a copy to the Office of Medical Education. This will be kept in the housestaff ’s
personal credentials file and available to the AOA Office of Hospital Affairs. Fees required to
maintain membership in the Florida Osteopathic Medical Association, AOA, and national
and state specialty societies (of the field in training) will be paid directly by the Institution
or reimbursed to the Intern/Resident/Fellow upon submission of satisfactory
documentation of payment by Intern/Resident/Fellow. Receipt of documentation of
membership should also be made a part of the personal credentials file.
d) HEALTH INSURANCE: As an employee of a PBCGME facility, group health insurance coverage
will be offered pursuant to Hospital policy for elective benefits.
e) MALPRACTICE INSURANCE: The hospital will cover housestaff for all work assumed within the
institution and on assigned rotations and for all activities required as a participant in the
resident training program while working in the PBCGME base facility, affiliated hospitals,
clinics and required or elective rotations sites which are part of the approved training
program. Professional liability insurance is NOT provided for any moonlighting activities
even if participation is approved by the Director of Medical Education or Medical
Education Office.
f) LIFE INSURANCE: As an employee of a PBCGME facility, group life insurance will be offered
pursuant to Hospital policy for elective benefits.
g) HOUSING: Housestaff (and their families) will need to provide for their own accommodations.
h) EXAMINATIONS: Housestaff will not be advanced into the OGME-2 year unless they have
passed Part III of the NBOME COMLEX examination. OGME-1s must sit for (and pass)
COMLEX III no later than December 31 of the OGME-1 year. Housestaff will not be offered a
contract for an OGME-II position unless proof of passing COMLEX Level III is provided to the
medical education office by April 30.
i) Reimbursement for the cost of Level III of the COMLEX exam will be made to those
continuing onto their OGME-2 within PBCGME, after proof of passing that exam is
provided to the Office of Medical Education. All housestaff will be required to sit for their
specialty college annual in-service examination.
i. Any member of the housestaff scoring below the mean/median for their
class year will be required to document and prove a plan of study prior to being
considered for advancement into the next year.
j) SPECIALTY BOARDS: Reimbursement for specialty board certification examinations is not
provided and will be the responsibility of the resident. For those Housestaff eligible to sit
for the exam during training, CME money may be used for the examination.
k) PRO-RATION: Reimbursement of all membership expenses will be prorated to cover only
the time spent in training.
l) WORKERS' COMPENSATION: Each Housestaff member is protected in accordance with the
Workers' Compensation Law of the State of Florida. The Hospital's Emergency Department
provides initial physician services for Housestaff injured in connection with duty. Housestaff
are required to immediately report the incident to the Director of Medical Education and to
the Emergency Medicine Physician for any necessary treatment.
m) MILEAGE: House Staff may be reimbursed for travel to rotations and program-required
didactics, when travel is greater than 40 miles from the resident’s base facility, or home
(whichever is less). Amount and procedure for reimbursement shall be in accordance
with HCA policy.
.
Core Manual July 2014 page 22
3. TIME OFF: ABSENCES/LEAVE/HOLIDAYS/VACATIONS a) ABSENCES
i. Because of the urgent nature of healthcare work, and essential nature of training, regular attendance by each intern/resident/fellow is mandatory. If the intern/resident/fellow employee is going to be unable to report for work as assigned, the intern/resident/fellow employee must personally notify his/her attending, and the medical education office. Such notice must be given as far in advance (at least 2 hours) of the time assigned for reporting to work as possible. An intern/resident/fellow absent because of illness should advise his/her attending and the medical education office of his/her status and estimated date of return on a daily basis. In cases of absence due to illness, interns/residents/fellows must provide documentation from a local physician indicating that they are under their care for an illness that precluded them from reporting for duty (specifics of the illness are not required to be provided). In the alternative, the intern/resident/fellow may have a direct verbal communication with the Director of Medical Education, detailing the specifics of the illness and why they are unable to report for duty.
ii. The HCA Time Away From Work Program combines Paid Time Off, Short-Term Disability benefits, Long-Term Disability coverage and Leaves of Absence. To submit or view claims, visit the Time Away From Work Service Center. In addition to contacting your attending and the medical education office, you must contact the Time Away From Work Service Center at 1-855-858-7557 if you will be absent from work for four or more days due to a non-work-related personal illness or injury, or You need to take ANY leave of absence — continuous or intermittent — regardless of the duration or reason for the leave.
iii. Attendings will take vacation, days off for holidays, personal business, and even regularly schedule office hours for less than five full days per week. If an intern/resident/fellow is assigned to a service (other than inpatient hospitalist or house-based rotation) and the attending takes off a half-day or greater, it is the intern/resident/fellow’s responsibility to report such to the Director of Medical Education for program-specific re-assignment during that time. Failure to do so will constitute TIME AWAY FROM WORK and an UNEXCUSED ABSENCE. The only exceptions allowed will be when prior approval is received, in writing, from the Program Director.
iv. Any time away from work will be deducted from allotted vacation time. Unexcused absences from any rotation or clinic will be deducted from vacation time and may result in disciplinary action and/or extension of training. Housestaff are NOT TO LEAVE THE HOSPITAL OR ROTATION DURING DUTY unless so granted by the Director of Medical Education, Program Director or their designee. Personal affairs must be attended to during off hours. In the event of illness, special holidays, or the need for educational programs, a time will be determined by the DME on a one-on-one basis since it is impossible to make provisions for all situations that may occur. If approved, any absences from the training program in excess of the allowed vacation and academic time must be made up.
b) LEAVE i. Subject to Hospital policy, The Program Director with the concurrence of the
Director of Medical Education and Regional Director of Medical Education may have the prerogative, for educational purposes, of granting a total of ninety (90) days leave for any academic year, which time must be made up on a day for day basis. In the event that more than ninety (90) days leave is required in one year, a new contract must be negotiated. For details regarding statutory eligibility and hospital regulations for other types of leave, please contact the Human Resources Department.
Core Manual July 2014 page 23
ii. Any absences from the training program in excess of the allowed vacation and academic time must be made up. If a resident takes FMLA leave, the resident will be required to use accrued vacation time at the beginning of the FMLA leave period. The paid leave will be substituted for unpaid FMLA leave, and counted against the 12-week FMLA leave entitlement. If an Intern/Resident/Fellow is absent for a period longer than that allowed above, and this would preclude the Intern/Resident/Fellow from completing the required fifty-two (52) weeks of training within the term of the Intern/Resident/Fellow Agreement, the Institution will evaluate how this absence may be accommodated within the scope of the program. Any extension of the training period that may be made available is with the understanding that Intern/Resident/Fellow will receive compensation only during the extension of the training period, and not during the period of time that the leave exceeds the time allowed as delineated, herein. This extension shall be limited by, and in compliance with the terms of the Institution’s employee policy. If made available, residency training may be extended by a maximum of twelve (12) weeks to successfully meet requirements of the resident. Residency training requiring extension beyond twelve weeks must receive approval by the AOA Committee on Postdoctoral Training.
iii. Time Away from Work and Workers’ Compensation Process, house staff are to contact the Time Away from Work Service Center (TAFWSC) when they are going to miss four days or more due to leave. This can be coordinated with the ADME/Medical Education Office and Human Resources.
c) Vacation i. First year Intern and Residents are provided with up to three weeks of time away
from duty (e.g., vacation, illness, bereavement, interviews). Two separate weeks (five days each) is allowed continuous; the other five days should be taken separately (no more than two continuous weekdays).
ii. Residents and Fellows beyond the first year are provided with up to four weeks (20 business days, Monday through Friday) of time away from duty for vacation, professional, sick or other leave. Three separate weeks (five days each) is allowed continuous; the other five days should be taken separately (no more than two continuous weekdays). No more than 20 business days of leave may be granted for any purpose, without extending the program.
iii. Vacation days that are taken separately (not continuous days) should be scheduled on days other than those in which may be primarily didactic in nature.
iv. These days may not be accumulated from one year to the next. ONLY the Regional Director of Medical Education, Director of Medical Education, or Program Director may permit exceptions, as contracts are annual, only. These days are not to be taken in the last two (2) weeks of the Internship or Residency Program and will not be paid out at the end of the residency.
v. Housestaff may not have vacation time during the last two weeks of their contract period without special permission from the DME.
vi. Interns seeking to leave early should request permission within the first half of the academic year, and budget their time off, accordingly. As per AOA policy, “No more than 20 business days per contract year of leave may be granted for any purpose without extending the program.” Interns will be required to attend the graduation ceremony, and should seek to complete a minimum of three (3) weeks of the June rotation. If an intern’s residency program requires that they depart prior to this time, special circumstances will be considered after documentation is provided from that program.
vii. Days off should not be taken during rotations which may be deemed, by the Program Director or DME to be essential, such as inpatient internal medicine, inpatient pediatrics, VA rotations, block nights, or critical care rotation months. These months vary by program, and are at the discretion of the program director. ONLY the DME may permit exceptions. Vacation time for holiday
Core Manual July 2014 page 24
periods must be worked out between the Housestaff so as to ensure that no more than ½ the housestaff scheduled for any half-day are absent from the clinic.
viii. Sick leave counts towards vacation. ix. All leave must be approved by ADME, Chief Resident, DME, program director,
and attending physician (s), including continuity of care clinic. x. LEAVE HAS NOT BEEN APPROVED UNTIL WRITTEN CONFIRMATION (e.g., email or
calendar invitation) HAS BEEN RECEIVED FROM THE ADME. d) Suspension of Duties for Resident Activities
i. Residents will be excused from patient care responsibilities, and house coverage shall be suspended during certain resident activities as follows:
a. Residents Day Out: House coverage shall be suspended from 12 am prior to 12 am following the activity. Residents will be responsible to round on their patients prior to reporting to Resident’s Day Out activities. However, residents shall be excused from patient rounds and all patient care responsibility no later than 9AM.
ii. Resident Graduation: House coverage and all patient care responsibility shall be suspended from 5 pm the evening of graduation until normal time for day shift, the following day.
e) Procedure i. Except in cases of emergency, requests for leave, or changes in call and clinic
schedules must be made in writing to the Medical Education Office. When a resident desires vacation time, or finds it necessary to switch on call or clinic responsibilities, the following procedure is to be followed:
a. In case of call switch, arrange the switch with a fellow housestaff member. Unless urgent, no vacation requests which would involve a call switch will be approved after call schedule has been finalized. When urgent, it is the responsibility of the resident to provide coverage for shifts if assignments have already been made.
b. Complete a “Request for Time Off” form with dates and/or explaining the switch and have the covering resident sign.
c. Obtain approval and signature from the Attending Faculty and the Clinic Director (if applicable).
d. Requests for NON-URGENT leave should be turned in at least thirty (30) days in advance of the scheduled rotation. Requests for call switches should be turned in at least thirty (30) days in advance of the scheduled rotation.
e. Hand the form in to the Medical Education Office for approval by the ADME and Program Director no less than 21 days in advance.
f. All attendings, including those in clinic, as well as other Housestaff, affected by the time off must be informed and reminded of the change in coverage. It is the responsibility of the requesting resident to do this.
g. Vacation requests for the next contract period should be turned in to the office of Medical Education by May 15 to facilitate scheduling of core rotations for the next contract period.
h. Requests for vacation time must be approved the Clinic Director (if applicable), Program Director and DME. When necessary or appropriate, Housestaff must find their own coverage.
ii. All requests are subject to staffing requirements prior to approval. No request is approved until the Medical Education office obtains the signature of the Program Director; you will be notified via email by the ADME if/when your request is approved.
iii. Residents must consider and deal with impact of time off on clinic patients’ care. Whether for vacation time or organized PBCGME activities, residents are to work with office managers and personnel at the continuity of care site to alter patient appointments in effort minimize the impact as much as possible.
Core Manual July 2014 page 25
IV. PROFESSIONAL CONDUCT 1. Professionalism, Personal Responsibility, and Patient Safety
More courtesy and understanding are required in the practice of medicine than in any other field of work.
Misconduct while on duty, or on personal time can subject the Hospital and its employees to criticism.
Accordingly, the following codes should be observed at all times:
a) It is essential that residents and faculty members understand the professional responsibilities
of physicians to appear for duty appropriately rested and fit to provide the services required by
their patients. PBCGME is committed to and responsible for promoting patient safety and
resident well‐being in a supportive educational environment.
b) PBCGME DMEs and program directors will ensure that residents are integrated and actively
participate in interdisciplinary clinical quality improvement and patient safety programs. The
learning objectives of the program will be accomplished through an appropriate blend of
supervised patient care responsibilities, clinical teaching, and didactic educational events; and,
not be compromised by excessive reliance on residents to fulfill non‐physician service
obligations.
c) PBCGME fosters a culture of professionalism that supports patient safety and personal
responsibility. Residents and faculty members must demonstrate an understanding and
acceptance of their personal role in the following:
i. Assurance of the safety and welfare of patients entrusted to their care;
ii. Provision of patient‐ and family‐centered care;
iii. Assurance of their fitness for duty;
iv. Management of their time before, during, and after clinical assignments;
v. Recognition of impairment, including illness and fatigue, in themselves and in their
peers;
vi. Attention to lifelong learning;
vii. The monitoring of their patient care performance improvement indicators; and,
viii. Honest and accurate reporting of duty hours, patient outcomes, and clinical experience
data.
d) All residents and faculty members must demonstrate responsiveness to patient needs that
supersedes self‐interest. Physicians must recognize that under certain circumstances, the best
interests of the patient may be served by transitioning that patient’s care to another qualified
and rested provider.
e) Housestaff are not to address each other by given names while in the presence of patients.
Members of the medical staff are not to be addressed, by their given names, at any time. They are
to be addressed as Dr. Jones, etc. Members of the health care team should ALWAYS be addressed
and treated with respect.
f) Housestaff are to maintain order and decorum at all times. The dignity of the profession shall
remain above reproach.
g) Housestaff are not to perform operations of any kind except under the supervision of a medical
staff member.
h) Housestaff may question the attending physician privately regarding anything that they do not
understand.
i) When appropriate under HIPAA guidelines, Housestaff may discuss diagnosis, treatment or
other aspects of the patient’s care with the family members or hospital personnel, after
discussion with the attending physician.
j) Housestaff are not to write any prescriptions for students, housestaff or faculty members
unless a proper physician/patient relationship has been established including completion of a
Core Manual July 2014 page 26
medical record. Housestaff medical liability insurance does not offer protection for care
rendered outside the scope of the residency.
k) Any questions, comments or concerns regarding rotations, fellow housestaff, students,
attendings, or the program should be addressed by following the chain of command, found
earlier in this manual. If satisfaction is not achieved, or if the resident does not feel that it is
appropriate to discuss at that level, the issue should be brought to the attention of the next
level of the chain. If the resident still has not achieved satisfaction, or if there is a matter
which compels privacy or other special circumstances, the issue may be brought directly to the
attention of the Regional DME or hospital CEO. There are no exceptions to this chain of
command.
l) Housestaff are expected to be on time for lectures, clinic and rotations.
m) Housestaff are not only the recipients of education, they are also teachers. Anyone who teaches
also learns and those who are most knowledgeable are sought out to teach. It is the responsibility
of Housestaff to teach medical students as well as to thoroughly review their notes and H&P’s,
and review assignments.
n) Housestaff are to check email daily and immediately notify the Department of Medical
Education of any changes in preferred email address.
o) No students or attending are allowed in the housestaff call rooms unless accompanied by a
housestaff member. Accordingly, computers in the call rooms are for housestaff use, only.
p) Call rooms, libraries and classrooms are to be kept clean at all times.
q) Housestaff shall comply with all rules pertaining to HIPAA. Housestaff are not to discuss
patients in public areas, and patient lists, or paper with PHI should not be left unattended.
r) During hours off, personal activities are the housestaff member’s own concern. However,
housestaff should keep in mind that their actions are a reflection upon our profession and this
institution. Accordingly egregious behavior may subject the resident to disciplinary action.
s) When visiting a patient, housestaff should introduce themselves, explain who they are, and ask
permission to obtain a history and physical examination. Housestaff must learn to properly
introduce themselves to all patients, and work out a routine without difficulty. Most patients who
are cheerfully approached will cooperate after a suitable introduction. If housestaff should
experience difficulty in securing patient cooperation, they should not press the issue themselves,
but notify the attending physician who will decide how to proceed. If the patient is a young child
or otherwise incapable of providing a history, housestaff should try to secure the history and
physical from another reliable source e.g. family or caregiver, nursing staff, EMS personnel,
nursing home staff etc. If a reliable source is not available, the housestaff should ask the charge
nurse to notify them when someone comes to visit the patient from whom they can obtain the
needed information. The record must indicate whom the history is provided by and an assessment
of the historian’s reliability. If there is a language barrier to obtaining a history, do not rely on a
family member to provide translation. A certified medical translator should be used. HCA facilities
employ a language line for these purposes. Privacy matters must be considered.
t) HOUSESTAFF SHOULD WASH THEIR HANDS BEFORE AND AFTER EXAMINATION OF EACH PATIENT
and in the presence of the patient if possible.
u) Research suggests that when doctors sit when visiting hospitalized patients, they build a better
rapport and patient confidence; patients perceive them as being present longer and also
express greater overall satisfaction with their medical care. In addition to increasing patient
comfort and satisfaction, this enhances patient compliance, and lowers levels of litigation. As
patient quality of care is one of the pillars of PBCGME, students and housestaff are expected to
sit down when talking to patients.
Core Manual July 2014 page 27
v) Relatives of Patients: Housestaff will often be called upon by relatives to render an opinion as to
the diagnosis, progress, or prognosis of the patient. THIS IS NOT A HOUSESTAFF RESPONSIBILITY.
The attending physician knows the patient and his/her family history and may have an entirely
different idea about talking to the patient and family members as well as a good reason for this
approach. Housestaff should be courteous but non-committal, or simply refer the patient or
family member to the attending physician unless the attending physician specifically directs them
to provide information to the patient and/or family member.
w) Nursing Staff: The nursing staff is an integral and essential part of the medical team. Physicians
can learn a great deal from our nursing colleagues; Treat them with respect. At all times,
housestaff must maintain a professional manner and efficient working relationship with the
nursing staff. Respond promptly to a call from a nurse. If any problems arise with the nursing
service, housestaff are not to take it upon themselves to try to correct the situation. Issues in this
regard will be handled through the Director of Medical Education, the Hospital's Chief Executive
Officer, and the Chief Nursing Officer.
x) ANCILLARY MEDICAL SERVICES include Laboratory, Radiology, Respiratory Therapy, Physical
Therapy, EEG, EKG, etc. Housestaff should learn and comply with the rules of each of these
departments. When housestaff display a proper professional interest, the staff of these services
will do their utmost to make available the opportunity to learn. Housestaff should also remember
that if they "request" assistance or services rather than "demand," they will receive the respect
and cooperation of the ancillary medical services personnel.
y) It is wise not to argue with patients. If difficulties should arise with a patient, the Nursing
Supervisor, Department Head, or Attending Physician should be called to handle the situation.
z) The facilities of the PBCGME are all non-smoking environments. Smoking is not permitted in
private offices, public/non-public areas, cafeterias, patient rooms, elevators, nursing stations, or in
hallways. These are non-smoking hospitals.
aa) Personal conversations are not to be carried out in the presence of patients or visitors and
personal affairs or problems are not to be discussed with patients.
bb) Housestaff should show evidence of loyalty to the Hospital, PBCGME and training programs by
not criticizing program or Hospital policies either publicly or to fellow residents, attendings,
medical staff, nursing staff or medical students. When issues arise, the chain-of-command
should be followed to bring the matter to light and seek resolution
cc) THEFT/LOST AND FOUND: Because the hospital is open at all times, Housestaff are urged to be
alert to the presence of strangers. The cooperation of everyone is needed in order to minimize
theft and ensure safety. Valuables and excessive sums of money should not be brought to work as
the Hospital cannot be responsible for loss of personal items. All articles should be properly stored
in the vehicle trunks, or covered in cargo areas. Nothing should be left in plain view in parked cars.
Found articles are to be promptly turned in to the Security Department where they may be
claimed upon proper identification.
dd) LECTURES COME FIRST; CLINICS COME SECOND: Housestaff attendance at all lectures is
mandatory (refer to program-specific lecture schedules and exceptions).Housestaff have a
primary obligation to clinic. Both attendings and patients rely on housestaff in the clinic stetting. If
Housestaff cannot make clinic due to excused absence, post-call or other reasons, they must
notify their clinic attending as far in advance as possible. In addition, please make sure that your
rotation attending understands when your clinic day/hours are, in order that they may anticipate
your absence from their service.
ee) ELECTIVE ROTATIONS: Housestaff may be assigned elective rotations. All rotations must be
approved by the DME and Program Director sixty (60) days in advance. Failing to make
request in a timely manner may result in having an elective assigned. The elective form found
Core Manual July 2014 page 28
in this manual should be completed by the preceptor’s office and faxed to the Medical
Education Office for approval. The resident needs to have the approval letter signed by the
preceptor and returned to the Medical Education Office prior to the beginning of the rotation.
Electives using resources out of PBCGME may be permitted, on a case-by-case basis, at the
discretion of the DME/PD, based upon intern/resident performance and documented need for
exposure to a program to which they are applying for a residency or fellowship. Generally, a
maximum of one such elective will be permitted, during training, at another hospital facility.
Additional electives at another hospital facility may only be scheduled based upon
recommendation of the program director with approval of the Regional DME and hospital CEO.
ff) TEACHING BY RESIDENTS: PBCGME is committed to the philosophy that an effective physician
is a good teacher. On each clinical service, residents participate actively in the clinical
instruction of third year and fourth year medical students. Residents also teach other
physicians and professional staff through interactions and formal presentations.
Resident’s non-compliance with any of these stipulations or other responsibilities of the residency will result in disciplinary action according to the Medical Education Department’s disciplinary policy as published in this Manual.
2. Confidentiality a) The most important rule of Hospital ethics is to respect the confidential nature of information
pertaining to the patient. Housestaff are not to discuss patient or Hospital affairs with
employees or outsiders.
b) Housestaff should refer questions regarding patient diagnosis, prognosis or other
information to the attending physicians.
c) Keep all medical records strictly confidential. Housestaff should not discuss
confidential information in the cafeteria, hallways, elevators or other areas where
patients or visitors can overhear them. All information from current or past medical
records/charts is to be considered confidential.
d) Housestaff should not speak to the media. All questions or requests from the media
should be referred to the Director of Marketing.
e) Financial questions from patients should be referred to the Nursing Station or
Business Office.
f) Computer Confidentiality: Hospital personnel share in the responsibility of
maintaining the confidentiality of the medical record information accessed by
computer for inpatients and outpatients.
g) Computer accessed Medical Record information includes but is not limited to the
following:
a. Patient order, both current and future b. Order results c. Documentation d. Previous hospital records e. Current face sheet information f. Billing information
h) Hospital personnel that currently have a right to review the patient’s manual medical
record may access computer generated information, on-line and printed, strictly
during their tour of duty and within their area(s) of responsibility. This includes:
a. Nursing staff members directly responsible for the care of the patient (RN,
LPN, NA, NT, Psych Tech, US, SN, SPN)
b. Primary physician
c. Consulting physician(s)
Core Manual July 2014 page 29
d. Allied health personnel
e. Ancillary personnel directly responsible for the care of the patient
f. Personnel from authorized departments (i.e., HIM, QA, RM) for the purpose
of data collection.
i) Any question regarding the appropriateness of a request to access computer
information is to immediately be referred to the supervisor/director for assessment of
this request.
j) Any inappropriate or unauthorized retrieval/review/sharing of private patient
information by or with hospital personnel (or with the assistance of hospital
personnel) is considered a breach of confidentiality and will be considered just cause
for immediate termination of employment.
k) Paper Destruction: Copies of confidential information may be taken to Medical
Records or the Medical Education office to be shredded. NEVER discard copies of
confidential information in a trash can or where it may be picked up or read by
unauthorized personnel or visitors.
l) Patients’ Health Information: Preventative Measures
i. Always ensure the correct patient’s information is accessed, provided to
patients, etc., by using appropriate identifiers (e.g., verify the patient name
on the discharge paperwork, match the date of birth).
ii. Keep PHI secure and do not leave it unattended in patient rooms, restrooms,
public areas, library, classroom, etc.
iii. Do not discuss PHI in public areas such as elevators and cafeterias.
iv. Always verify the mailing address, email address, or fax number before
sending.
v. When faxing, use pre-programmed numbers when feasible and use a cover
sheet.
vi. Ensure pre-programmed fax numbers are correct.
vii. Ask the patient for permission to discuss PHI when family/visitors are in the
room and ensure the facility’s policy (e.g., “Passcode” policy) is followed.
viii. Never discuss PHI with individuals who are not authorized or permitted to
receive the information.
ix. Only access PHI when there is a legitimate need to know and it is within the
scope of the workforce member’s job duties.
x. Ensure reasonable safeguards are implemented when permissibly discussing
PHI such as lowering voices, and drawing curtains between beds.
xi. For internal uses of PHI using email, ensure the appropriate recipient is
chosen from the directory.
xii. When printing PHI, verify that the correct printer is mapped to the computer
and/or chosen before printing.
xiii. Housestaff should not assume the patient has agreed to have PHI verbally
shared in front of their family members, friends or other visitors just
because the patient did not request these individuals to leave when the
intern/resident began speaking.
3. Social Media-HCA Guidelines
These social media guidelines apply to Company-authorized users of social media, as well as
HCA-affiliated employees’ personal use of social media. For purposes of these guidelines,
Company refers to HCA and its affiliated entities. Individuals seeking to engage in social media
Core Manual July 2014 page 30
activity must adhere to these guidelines as well as the Company’s Appropriate Use of
Communications Resources and Systems Policy, EC.026.
Blogging and other forms of social networking include but are not limited to video or wiki postings, sites such as Facebook and Twitter, chat rooms, personal blogs or other similar forms of online journals, and diaries or personal newsletters not affiliated with HCA.
Unless specifically authorized, employees are restricted from speaking on behalf of HCA or their affiliated employer. Employees are expected to protect the privacy of patients, employees and other stakeholders and are prohibited from disclosing patient information and any other proprietary or confidential information to which they have access.
a) Monitoring
Employees are reminded that they should have no expectation of privacy while posting
information to social networking sites. Postings often can be reviewed by anyone,
including HCA and/or its affiliates. As described in EC.026, HCA and affiliated employers
reserve the right to use content management tools to monitor comments or discussions
about the Company, its employees, its patients and the industry posted on the Internet.
b) Reporting and Discipline for Violations
i. Reporting Violations
HCA and its affiliates strongly urge employees to report any violations or possible
or perceived violations to supervisors, managers or the HR department, to the
Facility Privacy Official (if patient information is involved) or to the Ethics Line (1-
800-455-1996).
ii. Discipline
HCA and/or its affiliates investigate and respond to reports of violations of
EC.026, these Social Media Guidelines and other related policies. Violations may
result in disciplinary action.
c) Authorized Use of Social Media
i. The goal of authorized social media is to enhance the exchange of information
between the organization and its constituents in order to drive business results
and support our long-term success. Authorized use of social networking
media is purposeful in conveying information about Company services,
promoting and raising awareness of HCA and its affiliated entities,
communicating with employees, patients, business associates and the media,
and discussing activities and events.
ii. When social networking, blogging or using other forums, HCA must ensure that
use of these communications is consistent with and supportive of the mission
and values of HCA and its affiliated entities, and maintains their brand
identities, integrity and reputation while minimizing risks inside or outside the
workplace.
iii. The following rules and guidelines apply to social networking when authorized
by your employer and done on working time. The rules and guidelines apply to
all employer-related blogs and social networking entries, including employer
subsidiaries or affiliates.
iv. Content. Only authorized employees can prepare and modify content for Company-sponsored blogs and/or Company-authorized social networking entries. Content must be relevant, add value and meet at least one of the specified goals or purposes developed by HCA and/or its affiliates. If uncertain about any information, material or conversation, discuss the content with your manager and/or the Marketing Director.
Core Manual July 2014 page 31
v. Unauthorized Content. Business units and departments are responsible for ensuring all blogging and social networking information complies with the written policies of HCA and/or the applicable affiliate. The Marketing Department and senior management are authorized to remove any content that does not meet the rules and guidelines of this policy or that may be illegal or offensive. Removal of such content may be done without permission of the blogger or advance warning. Contact the Marketing Department or follow the chain of command to report unauthorized or questionable content.
vi. Identification. Employees must identify themselves as employees of the appropriate HCA affiliate when posting comments or responses on the employer’s blog or a social networking site.
vii. Copyright. The use of copyrighted content cannot be posted on any HCA-affiliated blog without first obtaining written permission from the copyright owner.
viii. Guest Bloggers. HCA and its affiliates expect all guest bloggers to abide by these guidelines. HCA and its affiliates reserve the right to remove, without advance notice or permission, all guest bloggers’ content considered inaccurate or offensive. HCA and its affiliates also reserve the right to take legal action against guests who engage in prohibited or unlawful conduct.
ix. Media. If contacted by the media or press about a post that relates to the business of HCA and/or any of its affiliates, employees are required to speak with their manager and the Marketing/Public Affairs Department before responding.
d) Personal Use of Social Media
HCA and its affiliates respect the right of employees to participate in blogs and use social networking sites during non-working hours and does not discourage self-publishing or self-expression. Employees are expected to follow these guidelines and policies to provide a clear distinction between you as an individual and you as an employee.
Personal Responsibility. You are personally responsible for your commentary on social media. You can be held personally liable for commentary that is considered defamatory, obscene, proprietary or libelous by any offended party, not just HCA.
Non-threatening. Employees should not use blogs or social networking sites to harass, threaten, discriminate or defame employees or anyone associated with or doing business with HCA or its affiliates.
Disclaimer. When you identify yourself as an employee of HCA or an affiliate, some readers may view you as a spokesperson for HCA and/or that affiliate. Because of this possibility, you must state that the views expressed by you through social media are your own and not those of the Company, nor of any organization affiliated or doing business with HCA and/or an affiliate.
Privileged or Confidential Information. Employees cannot post on personal blogs or other sites the trademark or logo of HCA, its affiliates, or any business with a connection to HCA or its affiliates. Employees cannot post Company-privileged or confidential information, including copyrighted information, Company-issued documents, or patient protected health information.
Workplace photographs. Employees must follow the Company’s policy regarding photos taken in the workplace.
Advertising. Except as authorized or requested by HCA or an affiliate, employees may not post on personal blogs and social networking sites any advertisements or photographs of Company products, nor sell Company products and services.
Patient Information. Do not use your personal social media account to discuss or communicate patient information with one of your patients, even if the patient initiated the contact or communication. Always use Company-approved communication methods when communicating with patients about their health or treatment.
Core Manual July 2014 page 32
Security. Consult the Information Security site on Atlas for social media information security tips. If you have any questions relating to these guidelines , a personal blog or social networking, ask your ADME, PD or DME.
4. Dress Code
a. All Housestaff will adopt Professional dress. Housestaff must appear neat and observe
the dress code at all times while on duty in the hospital, on rotations, at continuity of care
clinic, or any other clinical site.
b. A white jacket and name tag (provided by the hospital) are to be worn at all times while
on duty at the hospital, on rotations, or continuity of care clinic. Male Housestaff are to
wear dress shirt and clean, unwrinkled slacks that comply with a professional appearance.
Ties are encouraged but optional, and when worn should be covered by a closed lab coat
when examining or treating patients. Female Housestaff are to wear a dress or pants
consistent with a professional appearance. Hosiery, shoes and socks conducive to
comfort and a professional appearance are to be worn (no sandals, athletic footwear
(unless wearing scrubs), or open shoes).
c. Scrubs are not to be worn by Housestaff as dress in the Hospital except in those areas so
designated (a white jacket must be worn over the greens when outside of those areas).
Designated areas are (1) operating room or (2) areas where special procedures are carried
out and sterile dress is required (ED, ICU, OB, Night rotations). Athletic footwear may be
worn in the hospital if the Housestaff are wearing surgical scrubs. Scrubs are obtained
daily as needed and returned to the OR, or Linen Department. Scrubs should not be left
at home. When worn, scrubs must be the color issued as standard by the hospital the
intern/resident is rotating in, or be dark blue with PBCGME logo.
d. Housestaff are not, at any time, permitted to see patients while wearing other than the
above-described attire.
e. PBCGME reserves the right to decide whether an individual’s mode of dress and grooming
are satisfactory. The Regional DME, DME or CEO will interpret PBCGME dress codes to
determine what constitutes a professional appearance.
f. Hair will be clean and well groomed. Males’ hair will be above the collar, over the ears,
and without long sideburns. Jewelry, piercing and tattoos will be limited and discreet as
defined by PBCGME interpretation, as per above. Acrylic nails may not be worn. Use of
perfumes, colognes, etc should be limited and subtle to avoid overwhelming
environmental scents. Masks are to be discarded only in the sterile areas. In the OR, all
facial hair (i.e., mustache, beard) is to be covered by the appropriate mask and head gear.
Shoes are to be maintained in clean condition with proper covering in sterile and non-
conductive areas. These coverings are not to be worn outside the areas of surgery.
5. Community Service a. The leadership of PBCGME is firmly committed to the support of community service, and
residents and fellows are expected to volunteer service or activity for the benefit of the community. Continuous community service activities are preferred, as are those which are medically related; a minimum of two “major” acts of community service, or four “minor” acts of community service are required each year. Activity beyond this requirement is encouraged, but will not accrue in successive years. These activities will be reviewed with the program director on a quarterly basis, reported at C&A Committees, and documented in the residents’ portfolio.
i. “Major acts” of community service are defined as those which include ongoing responsibilities, such as the organization of an event; leadership role in
Core Manual July 2014 page 33
county/state/national medical or specialty organization; or participating in an event which lasts eight (8) hours or more. (One full day.)
ii. “Minor acts” are defined as those which require individual participation for at least four hours (such as participating in a walk or run). (One half-day.)
iii. One significant/extensive activity, such as participating in a four-day medical outreach trip to an underserved country, may satisfy the entire annual requirement.
b. A great deal of research has been done on the subject of volunteering and community service, resulting in evidence for multiple kinds of benefits. Among the most significant gains reported are the psychological, social, and cognitive benefits experienced by those who provide it.
i. Psychological Benefits: Overall, sources indicate that those who get involved in community service have shown more life satisfaction with increases in positive feelings and mental health, and decreases in depression and stress.
ii. Social Benefits: By “giving back” through participating in service projects, housestaff forge bonds with each other, as well as other members of the community. These bonds enhance Trust, Cooperation, and Citizenship; and Improved Communication Skills;
iii. Cognitive Benefits: The life-lessons learned from volunteering frequently support and enrich understandings of how the community is set up to function. By learning about the people for whom they volunteer, housestaff may develop attitudes of social responsibility and other cognitive gains including Political and Civic Awareness, Exposure to Diversity, Multiculturalism, and Different Ways of Thinking, and Critical Thinking and Problem Solving Skills.
c. Volunteering community service does not include any obligations of your normal training program, such as working in a community health clinic. Examples of true voluntary community service, as performed previously by housestaff members include:
i. Doing screenings at community health fairs ii. Getting involved with national organizations such as Habitat for Humanity iii. Organizing “Poker Runs” iv. Responding to disasters, such as earthquakes or hurricanes v. Working with local police organizations to educate the public on proper seatbelt
usage vi. Speaking to underprivileged students about the benefits of healthy habits
vii. Assuming a leadership role in a county, state or national medical or specialty society
d. Medical Missions: PBCGME may, on occasion, sponsor medical missions. Participation in these missions, or permission to participate in any other medical mission, is contingent upon successful standing within our program. Approval for participation depend upon factors including, but not limited to, residency class, performance on in-service exams, absence of any quality, performance or academic issues, absence of any remediation, etc.
V. RESIDENT DOCUMENTATION 1. GENERAL
a. During the training program, the resident must:
a. Submit an annual report to the specialty college, if so required in the area of
training.
b. Keep a log of each procedure and case assigned.
b. All evaluations, procedure logs, and summaries are to be submitted BY THE 3RD DAY OF
THE MONTH FOLLOWING COMPLETION OF THE ROTATION.
c. Failure to have rotation documentation submitted in a timely fashion (3 days following
completion of rotation) may result in administrative suspension, and extension of
program training.
Core Manual July 2014 page 34
2. PORTFOLIO a. All Housestaff will maintain a learning portfolio, which is a collection of materials that
represents resident’s progress and achievements in multiple areas of the curriculum
throughout their training, as part of their file in the Medical Education Office. The purpose
of a learning portfolio is to facilitate improvement in abilities and contribute to the
lifelong learning process. A portfolio is a method to encourage Housestaff to reflect on
their experiences and learn from them. A portfolio is a place to store and keep work
products of the residency and would include: (a) Collection of personal work, i.e.
PowerPoint slides, handouts, exhibits, effort, progress, achievement; (b) Serves as an
ongoing diary of their learning experiences. A portfolio will help mentors and coaches use
the system to help Housestaff gain insight into their education.
b. By creating a portfolio the resident takes an active role in his/her achievements during
training.
c. A portfolio is a record of growth, achievement and professional attributes that illustrate
progression toward competence over time and to self-directed, lifelong learning. During
the years of training the resident will construct a portfolio with evidence of growing
competency. Upon graduation the portfolio will be given to the trainee and will give them
documentation that will enhance their marketability and serve as proof to others as well
as the trainee that they are a competent physician. A portfolio provides the opportunity
for Housestaff to learn and demonstrate skills needed to develop an approach to self-
directed, lifelong learning because the Housestaff are responsible for its creation.
d. At a minimum, portfolios will contain:
i. Rotation Schedules
ii. Conference Attendance
iii. In-service Exam Results
iv. Procedures Logs/Clinical Patient Logs/Continuity of Care Patient
Logs/OMM logs
v. Quarterly Performance Reviews (Competency Log)
vi. Research Paper Progress Report
vii. Presentations Given at Conferences, Grand Rounds, etc (include
slides/handouts)
viii. Attendance at National Meetings
ix. Community Service
x. Medical Organization Memberships and Activities
3. CHARTING RESPONSIBILITIES/Patient Medical Record a. Verbal orders are expressly discouraged, unless in case of emergency. Any time a verbal
order is given, it must be countersigned/authenticated immediately once the emergency
condition has been stabilized, and the Housestaff is no longer providing emergent care.
Under no circumstances should housestaff leave the hospital at the end of a shift prior to
authenticating all verbal orders.
b. Students are NOT permitted to write any orders at any time. Students are NOT permitted to
enter notes into the electronic medical record. Students should produce written notes,
absent any patient identifiers, for review by residents and/or attendings. Following such
review, those notes should be destroyed.
c. Any documents dictated by housestaff (e.g., H&P, discharge summary) must be
authenticated by the housestaff as soon as the document is available. It is incumbent upon
the housestaff to monitor such availability and assure timely compliance.
Core Manual July 2014 page 35
d. Under no circumstances are medical records to be removed from the hospital by housestaff
or given to anyone to be removed from the hospital.
e. All housestaff progress notes and orders must be co-signed/authenticated by an
attending physician within 24 hours.
f. When dictating on the hospital system, housestaff must be sure to state their name, as
well as the name of the physician for whom they are dictating, at the beginning and end
of the dictation. Also, they should spell the name of the patient, and give the medical
record number.
g. Housestaff must ensure that all records of patients admitted to the teaching service of
osteopathic patients contain full osteopathic structural examinations, with correlation of
structural findings to admitting diagnosis. Housestaff are encouraged to perform OMT on
all such patients, as indicated. Housestaff must include the medical record numbers of
patients on whom OMT was given, in their monthly summaries. In the case of primary
care residencies, two OMT procedures must be performed and documented
appropriately by housestaff on months that they are on the service of an osteopathic
physician attending. An order and short procedure note must be entered in the record.
Housestaff are to submit the patient’s initials, medical record number and date of
admission/date of OMT at the end of the month.
h. All medical records should be addressed in a timely manner. If a Housestaff are >30 days
delinquent they will not be allowed to return to their rotation until the records are
completed. This may result in extension of training.
i. Each Housestaff are responsible for the following items on his or her charts:
HISTORY AND PHYSICAL EXAMINATION On all critical and/or emergency cases, a pertinent history and physical must be
completed within 4 hours of admission or before emergency surgery is performed. All
other history and physicals are to be completed within 24 hours
Housestaff will be responsible for H&Ps (either combined admit note/H&P or separate
dictated H&P) on ALL patients that they admit. If dictated, a progress note must be
written indicating "H&P dictated". Housestaff also have responsibility of all patients on
their service that they don't admit (i.e., admitted on nights or weekends). If a night or
weekend H&P is performed by another member of the housestaff, the housestaff on
service shall co-sign the documentation. If the H&P is initially done by a medical student, it
must be repeated and dictated by the housestaff on the service. Responsibility for H&Ps
on services without housestaff on a particular month will remain with the attending
physician (except for those patients admitted at night on unassigned medicine call, in
which case the housestaff will document an H&P).
OSTEOPATHIC STRUCTUAL DIAGNOSIS FORMS MUST BE COMPLETED ON ALL ADMISSIONS
OF OSTEOPATHIC ATTENDINGS.
Only approved PBCGME facility abbreviations are to be used during dictation and in the
chart. (Please refer to the attached abbreviation list.)
All adult patients admitted to the hospital must be told that a breast, pelvic/pap and
rectal examination are part of the physical examination unless contraindicated. If the
patient refuses this part of the exam, it must be documented on the chart and the H&P as
Core Manual July 2014 page 36
“Patient refused the _____ for the following reason _____.” Obviously, ICU and PCU
patients confined to bed cannot have the most complete physical exam, but breast,
bimanual pelvic, and rectal exams can be performed on patients confined to bed rest. If
items on the H&P are deferred, they must be completed as soon as possible. In addition,
the patient must be told to follow up with their family doctor or a specialist.
The History & Physical must be completed within 24 hours of a patient's admission to the
Hospital except in the case of an emergency (shock, coma, emergency surgery, obstetrical
cases, severe pain, and all other non-elective cases) when it should be completed as soon
as possible. Assistance may be obtained from the medical students. The pertinent
portions of the H&P must be written immediately upon admission to the hospital and
the chart completed within 4 hours before any surgical procedure.
Pertinent portions of the H&P include those areas that are related to the patient's chief
complaint. This will vary with the individual case, but should include all items which may
be concerned with differential diagnosis. The complete History & Physical is, as the name
applies, intended to be a complete analysis of the medical history of the patient and an
effort to investigate and ascertain other related or unrelated pathology or symptoms.
This will, of necessity, vary in its completeness depending upon the type of case, but, in no
event, is it to be strictly limited to the brief printed instructions on the forms.
An accurate blood pressure by the resident is part of every History & Physical (this also
includes pediatric patients). The patient's temperature, weight, and height are normally
taken by the registered nurse although housestaff should be aware of these findings and
submit them as part of the H&P or if not available from the nurse, obtain the information
themselves.
Osteopathic structural findings MUST be accurately recorded on every patient of
osteopathic attendings in a manner that is understandable and follows the outline of the
Musculoskeletal Biomechanical Examination Form. Approved osteopathic nomenclature
must also always be used. Handwriting must be legible and the H&P must be signed by
the resident followed by the printed name and pager number.
The word Negative or abbreviations, such as WNL (for Within Normal Limits), are not
acceptable on a History & Physical.
Housestaff may do an interim H&P on patients who have been admitted within 30 days
with the same or related chief complaint IF a complete H&P was done with the most
recent prior admission. The interim H&P must consist of cc, Hx, CC, PMHx, PSHx,
medications, allergies, and PE. The rest of the interim H&P should read “as per previous
admission. Please see past medical record.”
RE-ADMISSION HISTORY AND PHYSICAL If a patient is readmitted for the same complaint within a 30-day period (which can be verified by
obtaining the previous chart from the Medical Records Department) an interim history must be
completed. The pertinent portion of the physical should be repeated with particular reference to
the previous positive findings or important negative findings. If the patient is readmitted for
another complaint, a complete H&P must be obtained unless the previous record entirely covers
Core Manual July 2014 page 37
the case. In either event, there must be a reference on the new chart to the old record and a
description of the interim course.
PROGRESS NOTES
Daily progress notes are mandatory for all services. A note must also be written any time that
housestaff is called to evaluate or provide an order for a patient. All notes require a:
Title (H+P, Cardiology Resident, House Resident, etc.)
Signature with printed name and beeper number
Printed attending physicians name
ALL PROGRESS NOTES ARE TO INCLUDE DATE AND TIME.
Progress notes should describe any change in the patient's clinical course of any procedure or treatment rendered by the housestaff member. This includes such procedures as the insertion of nasal gastric tubes, catheterization cut downs, subclavian sticks, etc. Housestaff will also write a note describing any change in the patient's condition, impression, and subsequent actions taken. Housestaff responsible for a patient will write a progress note at least once every day and additionally when the patient's condition warrants. All progress notes should be complete and comprehensive and should be done before the housestaff shift is over.
A useful, meaningful progress record of a patient's chart shows a flowing progressive unfolding of
the patient's hospital stay, reflects diagnostic thinking about the chief complaint, the plan of
diagnostic investigation, an outline of treatment, description of the conclusions reached, and the
disposition of the case at discharge.
A progress note should represent the "thinking" of those concerned with the patient's care. It
should portray the facts about the case as they may develop during the hospitalization period as
substantiated by the chart. The progress record, in many respects, represents the "philosophy of
the case management." The progress note is not the appropriate venue to argue with other care
providers about the patient’s management or diagnosis.
Any change in the diagnostic thinking or the treatment should be reflected in the progress
record. Wherever possible and whenever indicated, the reasoning for such change should be
stated.
Notations may be necessary several times a day in order to adequately reflect the progress of the
case. Conversely, unless there is some specific change or notation to be made, progress notes
might only appear once a day.
The progress record:
is a place where the doctor "thinks out loud."
is a mirror reflecting for the hospital inspector the professional stature of the staff of a
given teaching institution.
FINAL PROGRESS NOTE The final progress note or paragraph is very important and shares prominence with the opening
or admission paragraph. Here is where the physician:
describes the termination of his or her responsibility for the hospitalized patient;
determines, for the record, whether or not the admission chief complaint has been
answered;
Core Manual July 2014 page 38
discusses, in review, complications which may have been developed during the
hospitalization;
justifies the diagnosis and treatment;
discusses his or her inability to reach a diagnosis, successfully, if such is the case;
indicates what disposition has been made of the case and the patient’s status;
In case of a death, the matter of autopsy should be discussed in the final progress notes. If an
autopsy was refused, the reason(s) for such refusal should be stated. [This will serve the staff later
when the death is reviewed by the Mortality Review Committee and the staff and physician is called
upon to explain why the case was not posted.] Also, the steps and techniques utilized in an attempt
to procure an autopsy should be stated.
If an autopsy was done and pertinent information was made available in a fairly immediate post-
mortem period, such information should, likewise, be in the final progress note. If such information
is not immediately available, it would be considered good judgment to make an addendum to the
notes at some later date in order that the chart may be as complete as possible. Such an addendum
would be of further assistance as a basis upon which a case abstract should be more easily made.
The final entry on the progress record should constitute a case summary.
The chart is the responsibility of the resident on the service until the patient leaves. If the resident
changes services during a patient's stay, he or she must complete the chart up to the time that he
leaves the service and document a summarizing “off-service note” which includes progress to this
point and plans for the remainder of the hospitalization. If a chart is not completed, it will be placed
into the resident's box in the Medical Records Department. It must be completed within 72 hours.
Failure to comply with this may result in the loss of time off.
In the event of unusual situations where housestaff are over-burdened with work and cannot
complete charts within this period of time, the Director of Medical Education must be notified of this
fact and request an extension of time. Completion of charts refers to quantity, quality, and accuracy.
In completion of the chart, the final diagnosis in particular and the entire chart in general must be
reviewed and signed by the attending physician. If there is disparity between the laboratory,
radiology, pathology findings and the final diagnosis, this should be explained in the summary. The
Housestaff are encouraged to speak with the attending physician in regard to the charts.
ORDERS
All orders should be written in a clear and understandable language. ALL ORDERS ARE TO INCLUDE
DATE AND TIME, HOUSESTAFF NAME AND PAGER NUMBER, AND ATTENDING NAME. The
Housestaff are to write the necessary initial orders if, at the time of the patient's admission, they
have not been given or the attending physician is unavailable. Housestaff will be responsible for
calling the physician for the orders if they have not been received. No abbreviations or chemical
formulas should be used. The name of the drug should be fully written out as it appears on the label.
All orders must be written on the proper form and signed with a double signature (attending
physician and housestaff). Housestaff should print his/her name legibly under his signature and
include his/her pager number. Verbal orders are not to be used by housestaff covering the house
except in an emergency situation. Housestaff must, without exception, visit any patient before any
order for medication is given. Only the drugs in the Hospital Formulary are to be ordered, unless
directed by the attending.
Core Manual July 2014 page 39
STUDENTS ARE NOT TO WRITE ORDERS AT ANY TIME.
MANAGEMENT AND CONSULTATION OF CASES
The admitting physician shall be responsible for the patient until the patient is transferred or
discharged. The proper methodology for writing for management of a case or consultation is as
follows:
If an order is written, "Dr. may participate in management." This allows both the
admitting physician and the named physician to write orders. [This would ordinarily pertain to
partnerships, coverage on weekends, etc.] In this instance, the admitting physician still has
overall chart responsibility.
If an order is written, "Dr. for management," the admitting physician may no longer
write orders.
If an order is written, "Dr. for management of a specific entity or procedure," (e.g.,
diabetes, cystoscopy, etc.), the responsibility for other management remains with the admitting
physician.
If an order is written, "Dr. for consultation," the consultant may not write orders on the
chart. The specific reason for consultation should be included in the order.
If an order is written, "Dr. for consultation and management," the admitting physician
may no longer write orders. Again the order should include the specific reason for the
consultation.
VI. RESEARCH a) Residents and Fellows are required to participate in research projects and original research.
Research can be accomplished by any of the following means:
i. Research projects within the Department of their specialty training.
ii. Institutional research programs, in which the Department of their specialty training is actively
involved.
iii. Area-wide or multi-centered research projects involving PBCGME Hospitals and the
Department in which the Housestaff are being trained.
b) While individual programs may require more (in accordance with, or in additional to that required
by the corresponding specialty college), during the course of training, all PBCGME residents and
fellows are required to prepare, present and submit at least one unpublished scientific or research
paper during the course of their training. This paper must in a form acceptable for publication in
the Journal of the American Osteopathic Association, or other peer-reviewed journal approved by
the program director and followed through to either acceptance or rejection. This paper must be
ready for presentation to the C&A Committee, Medical Education Committee and/or meeting of
the clinical department of general medical staff no later than six months prior to graduation.
Papers must be accompanied by an abstract.
c) Any research done must be in accordance with any and all applicable federal, state and local laws
and rules, as well as HCA policy and policies of the resident’s base hospital, pertaining to clinical
research, as well as appropriate guidance.
d) In addition, each PBCGME resident/fellow will be required to prepare one scientific poster each
year, to be presented at the specialty college, OPTI, other recognized/organized medical
conference, and/or PBCGME, which may sponsor an annual Research Day. Note that individual
hospital departmental, peer review, and educational meetings do not meet the requirements for
submission. Posters should be reviewed by the Program Director prior to submission. Failure to
prepare/present such poster will prevent advancement to the following year of training. Under
extenuating circumstances, the DME and Program Director may permit the resident to advance,
Core Manual July 2014 page 40
with the understanding that they will do two presentations the following year, as well as provide a
well-annotated lecture (based upon current peer-reviewed literature) on a topic chosen by the
Program Director, to a facility “Grand Rounds” with mandatory attendance by all other residents in
their program.
e) Residents and fellows may choose to do an annual paper, in a form acceptable for publication in
the Journal of the American Osteopathic Association, or other peer-reviewed journal approved by
the program director and followed through to either acceptance or rejection, in lieu of the annual
poster requirement.
f) Residents and fellows will review the status of their poster presentations and research papers at
each quarterly meeting held with their program director.
g) Residents and fellows who do not submit their completed research papers or posters and abstracts
by the date of their expected graduation will not be allowed to graduate and will not be given the
diploma. The diploma will be conferred upon the receipt of the Program Director approved paper
or poster and abstract by the Office of Medical Education.
VII. ADMINISTRATIVE MATTERS
The Medical Education Department is open Monday through Friday from 8:30 a.m. to 5 p.m. and closed on weekends and holidays. In cases of emergency, the Administrative DME may be reached on the emergency line, information for which may be found on the outgoing message of the Department’s voicemail. 1. Deferment Forms
The Medical Education office will assist housestaff with loan deferment forms. The office is generally open 8:30 – 5:00 pm, Monday through Friday, and closed on weekends and holidays. The procedure is as follows: a) Complete all sections of the forms for borrower information. Please be sure to fill in
correctly all necessary dates.
b) Present the form to the Administrative DME. The ADME, DME or Program Director will
sign them and a copy will be made for file. Housestaff should also keep a copy for their
personal records.
c) The Medical Education Office will then mail the original form out. Be sure the correct
mailing address appears on the form.
2. Pagers/Parking Each Housestaff member may be provided with a pager. The pager is to be returned to the hospital at the end of the program. There is a charge of $100 for lost or damaged pagers.
In addition to each resident’s individual pager, there may be one pager that is always carried by the resident “on-call.” This enables attending physicians, the nursing staff and nursing homes to easily contact this resident. This pager should never be left with anyone other than another member of the housestaff, nursing supervisor or operator. Special circumstances MUST be approved by the DME. Employee parking is restricted to certain areas. Please park only in areas designated for employees. RESIDENTS MAY NOT park in the emergency room parking areas or physician parking.
3. Major Disaster Plan, Hurricane Plan and Fire Plan
Housestaff are responsible for evaluating PBCGME’S Disaster Plan, as well as the Major Disaster Plan, Hurricane Plan, and Fire Plan of their base institution, and to be knowledgeable of his or her role in the event of a major disaster, hurricane, or fire. a. Emergency Code System
Core Manual July 2014 page 41
As adopted by the Florida Hospital Association, the following is the Emergency Code System in place at PBCGME facilities:
In case of Fire:
Remember the word "RACE"
Rescue patients in immediate danger
Alarm - Activate pull station and call 3911
Contain the fire
Extinguish the fire
or
Evacuate when ordered
Remember the word "PASS"
Pull pin
Aim at base of fire
Squeeze handles together
Sweep from side to side
4. EVIDENCE-BASED MEDICINE
The most common definition of EBM is taken from Dr. David Sackett. EBM is "the conscientious, explicit and judicious use of current best evidence in making decisions about the care of the individual patient. It means integrating individual clinical expertise with the best available external clinical evidence from systematic research." (Sackett D, 1996)
EBM is the integration of clinical expertise, patient values, and the best evidence into the decision making process for patient care. Clinical expertise refers to the clinician's cumulated experience, education and clinical skills. The patient brings to the encounter his or her own personal and unique concerns, expectations, and values. The best evidence is usually found in clinically relevant research that has been conducted using sound methodology. (Sackett D, 2002)
The evidence, by itself, does not make a decision for you, but it can help support the patient care process. The full integration of these three components into clinical decisions enhances the opportunity for optimal clinical outcomes and quality of life. The practice of EBM is usually triggered by patient encounters which generate questions about the effects of therapy, the utility of diagnostic tests, the prognosis of diseases, or the etiology of disorders.
Event Standard Code List
MEDICAL EMERGENCY – Cardiac Arrest CODE Blue
FIRE CODE Red
INFANT / CHILD ABDUCTION CODE Pink
MASS CASUALTY / DISASTER CODE Green
HOSTAGE SITUATION CODE White
BOMB THREAT CODE Black
ACTIVE SHOOTER CODE Silver
HAZ MAT SPILL CODE Orange VIOLENCE OR SECURITY ALERT CODE Grey
FACILITY LOCKDOWN CODE Yellow
SEVERE WEATHER CODE Brown
DECONTAMINATION CODE Purple
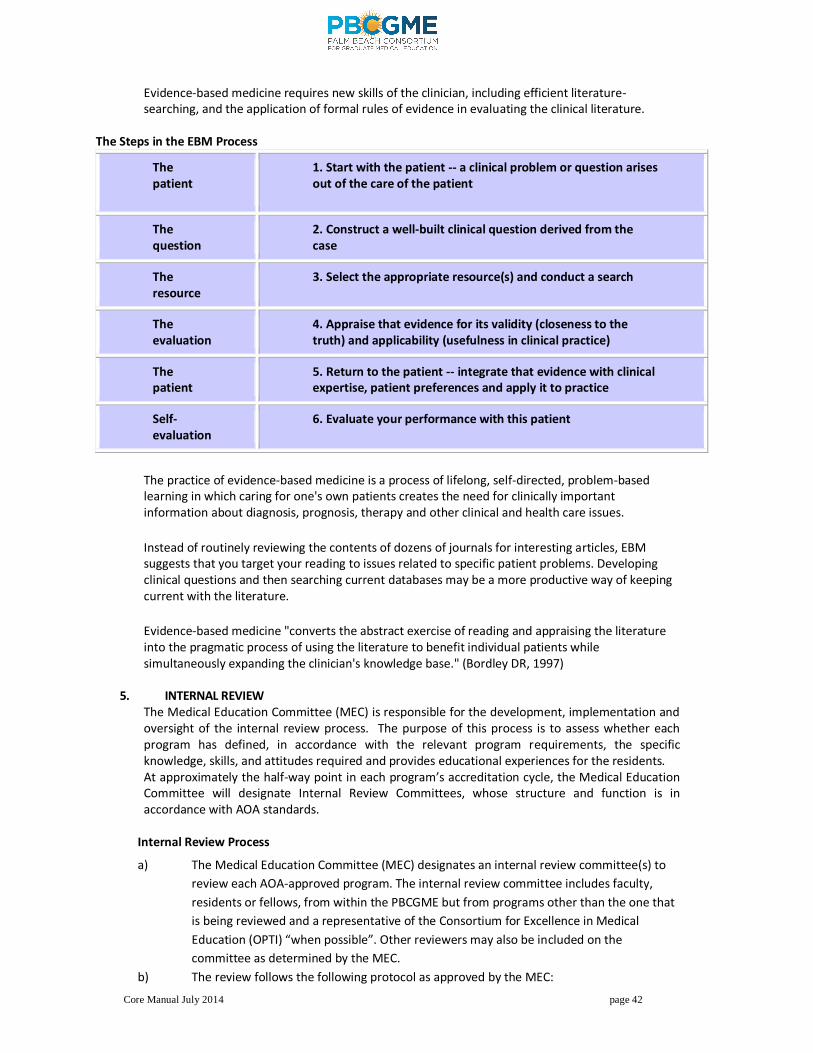
Core Manual July 2014 page 42
Evidence-based medicine requires new skills of the clinician, including efficient literature-searching, and the application of formal rules of evidence in evaluating the clinical literature.
The Steps in the EBM Process
The patient
1. Start with the patient -- a clinical problem or question arises out of the care of the patient
The question
2. Construct a well-built clinical question derived from the case
The resource
3. Select the appropriate resource(s) and conduct a search
The evaluation
4. Appraise that evidence for its validity (closeness to the truth) and applicability (usefulness in clinical practice)
The patient
5. Return to the patient -- integrate that evidence with clinical expertise, patient preferences and apply it to practice
Self-evaluation
6. Evaluate your performance with this patient
The practice of evidence-based medicine is a process of lifelong, self-directed, problem-based learning in which caring for one's own patients creates the need for clinically important information about diagnosis, prognosis, therapy and other clinical and health care issues.
Instead of routinely reviewing the contents of dozens of journals for interesting articles, EBM suggests that you target your reading to issues related to specific patient problems. Developing clinical questions and then searching current databases may be a more productive way of keeping current with the literature.
Evidence-based medicine "converts the abstract exercise of reading and appraising the literature into the pragmatic process of using the literature to benefit individual patients while simultaneously expanding the clinician's knowledge base." (Bordley DR, 1997)
5. INTERNAL REVIEW
The Medical Education Committee (MEC) is responsible for the development, implementation and oversight of the internal review process. The purpose of this process is to assess whether each program has defined, in accordance with the relevant program requirements, the specific knowledge, skills, and attitudes required and provides educational experiences for the residents. At approximately the half-way point in each program’s accreditation cycle, the Medical Education Committee will designate Internal Review Committees, whose structure and function is in accordance with AOA standards.
Internal Review Process
a) The Medical Education Committee (MEC) designates an internal review committee(s) to
review each AOA-approved program. The internal review committee includes faculty,
residents or fellows, from within the PBCGME but from programs other than the one that
is being reviewed and a representative of the Consortium for Excellence in Medical
Education (OPTI) “when possible”. Other reviewers may also be included on the
committee as determined by the MEC.
b) The review follows the following protocol as approved by the MEC:
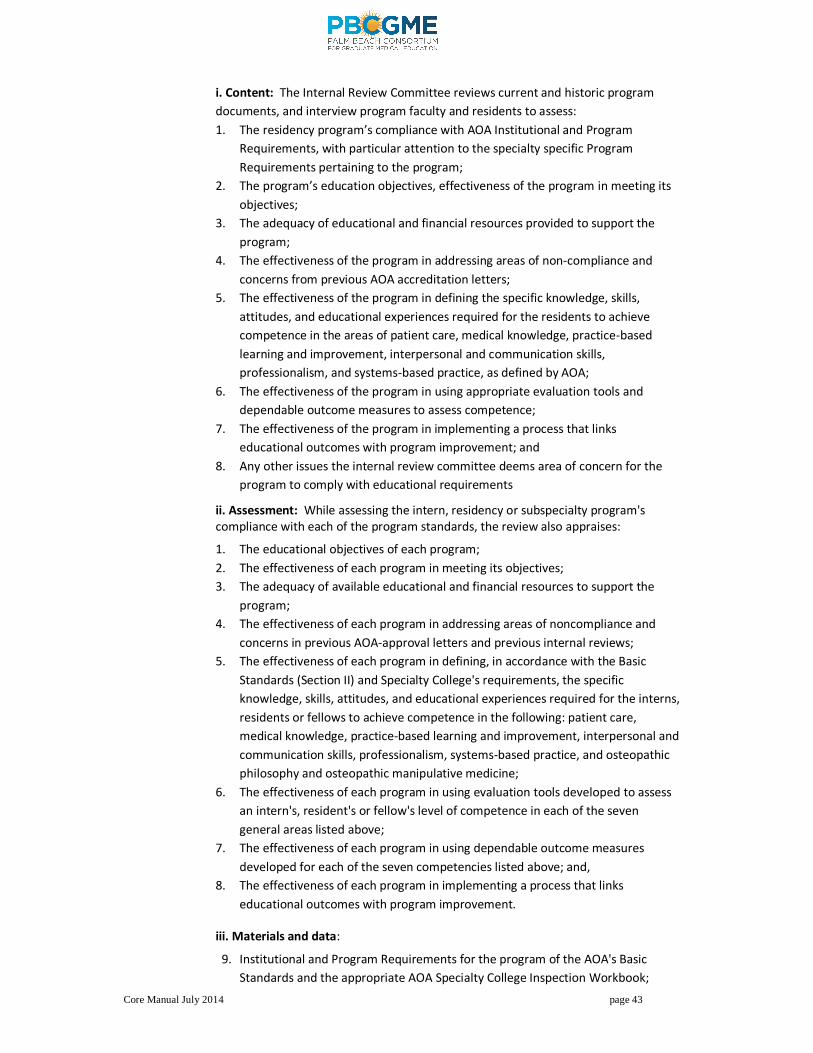
Core Manual July 2014 page 43
i. Content: The Internal Review Committee reviews current and historic program
documents, and interview program faculty and residents to assess:
1. The residency program’s compliance with AOA Institutional and Program
Requirements, with particular attention to the specialty specific Program
Requirements pertaining to the program;
2. The program’s education objectives, effectiveness of the program in meeting its
objectives;
3. The adequacy of educational and financial resources provided to support the
program;
4. The effectiveness of the program in addressing areas of non-compliance and
concerns from previous AOA accreditation letters;
5. The effectiveness of the program in defining the specific knowledge, skills,
attitudes, and educational experiences required for the residents to achieve
competence in the areas of patient care, medical knowledge, practice-based
learning and improvement, interpersonal and communication skills,
professionalism, and systems-based practice, as defined by AOA;
6. The effectiveness of the program in using appropriate evaluation tools and
dependable outcome measures to assess competence;
7. The effectiveness of the program in implementing a process that links
educational outcomes with program improvement; and
8. Any other issues the internal review committee deems area of concern for the
program to comply with educational requirements
ii. Assessment: While assessing the intern, residency or subspecialty program's compliance with each of the program standards, the review also appraises:
1. The educational objectives of each program;
2. The effectiveness of each program in meeting its objectives;
3. The adequacy of available educational and financial resources to support the
program;
4. The effectiveness of each program in addressing areas of noncompliance and
concerns in previous AOA-approval letters and previous internal reviews;
5. The effectiveness of each program in defining, in accordance with the Basic
Standards (Section II) and Specialty College's requirements, the specific
knowledge, skills, attitudes, and educational experiences required for the interns,
residents or fellows to achieve competence in the following: patient care,
medical knowledge, practice-based learning and improvement, interpersonal and
communication skills, professionalism, systems-based practice, and osteopathic
philosophy and osteopathic manipulative medicine;
6. The effectiveness of each program in using evaluation tools developed to assess
an intern's, resident's or fellow's level of competence in each of the seven
general areas listed above;
7. The effectiveness of each program in using dependable outcome measures
developed for each of the seven competencies listed above; and,
8. The effectiveness of each program in implementing a process that links
educational outcomes with program improvement.
iii. Materials and data:
9. Institutional and Program Requirements for the program of the AOA's Basic
Standards and the appropriate AOA Specialty College Inspection Workbook;
Core Manual July 2014 page 44
10. Accreditation letters from previous AOA reviews, corrective action plans and
progress reports approved by the MEC and sent to the AOA; and,
11. Reports from previous internal reviews of the program.
12. The written report of each internal review is presented to and reviewed by the
MEC to monitor the areas of noncompliance and recommend appropriate action.
13. Reviews are conducted at approximately the midpoint between the AOA
program surveys.
14. The internal review committee conducts interviews with the program director;
representatives from the faculty; intern, residents or fellows training in the
program (no less than fifty percent) and other individuals deemed appropriate by
the committee.
15. A written report of each internal review is presented to and reviewed by the MEC
to monitor the areas of noncompliance and recommend appropriate action. The
OPTI receives a copy of the report. The report contains:
a. The name of the program or subspecialty program reviewed and the
date of the review;
b. the names and titles of the internal review committee members to
include the resident(s) and an OPTI representative;
c. a brief description of how the internal review process was carried out,
including the list of the groups/individuals who were interviewed;
d. sufficient documentation or discussion of the program's requirements
and the AOA's Institutional Requirements to demonstrate that a comprehensive
review was conducted and was based on the MEC's internal review protocol;
e. A list of the areas of noncompliance or any concerns or comments from
the previous AOA-approval letter with a summary of how the program and /or
institution addressed each one.
6. THE MEDICAL LIBRARY
The purpose of the Health Science Library Resource Centers within the facilities of the PBCGME is to provide information for patient care, continuing education, management, and research. PBCGME/Palms West Hospital is also a “Classic” affiliate of the Calder Library at the University of Miami Jackson Memorial Medical Center. This affiliation gives the staff, Housestaff, and medical students access to the entire Calder collection, along with full borrowing, research and multi-media privileges. All Housestaff and teaching faculty also have access to full on-line texts through Nova Southeastern University’s library.
Each hospital’s in-house resource center contains carefully selected texts, the latest editions of medical journals and other appropriate publications, in various branches pertaining to the training of Housestaff, and personal computers with internet access. Housestaff are required to practice the tenets of a professional which include the constant discipline of professional reading. A comprehensive library of journals and textbooks is available to all members of the medical staff and the resident group. When removing books from the shelves, please return them in the same order/location it was removed from. BOOKS AND JOURNALS ARE NOT TO BE REMOVED FROM THE RESOURCE CENTER.
The individual training departments maintain a small library of textbooks in the Housestaff’ call room for use by the house staff. These textbooks are to be considered as part of the hospital’s Resource Center collection and must be treated and returned as is required with all other library books.
Core Manual July 2014 page 45
LIBRARY POLICY 1. Journals (bound or single issues) may be used in the Resource Center only, and not
checked out. 2. Books may NOT be removed from the Resource Center. Failure to comply will result in
failure of the rotation and a fine up to $200. 3. It is the responsibility of Housestaff to become familiar with copyright law and fully obey
all such laws. Likewise, any plagiarism by housestaff will be grounds for disciplinary action including, but not limited to, dismissal from the program.
4. The following policy is in effect for admittance to the PBCGME Resource Centers outside of regular library operating hours: a. Housestaff will be assigned key codes for entry to the Resource Center. b. All Housestaff and medical students must have their ID badge visible at all times
when in the Resource Center, as in other parts of the hospitals. c. Unauthorized removal of any materials from the Resource Center will result in
failure of the current rotation and a fine of up to $200.
Contact the Department of Medical Education with any problems or questions.
7. VISITING STUDENTS AND RESIDENTS In order to appropriately manage limited resources within our facilities, all requests for student electives must be processed through the PBCGME Administrative Director of Medical Education. No students will be allowed to accompany physicians in PBCGME facilities, even to observe, without verification of enrollment, criminal background check, medical student orientation as well as any other HCA requirements for students, and approval of the facility’s Director of Medical Education. PBCGME may accept visiting residents from other osteopathic residency programs which are part of the same OPTI and from other programs affiliated with HCA. Any other visiting residents will only be permitted to observe within PBCGME facilities. In either case, visitor must be supervised by a member of the PBCGME faculty, and rotation is subject to the approval of the individual facility’s CEO. a. Observer Responsibility:
Observers will need sign and abide by the terms of the PBCGME Agreement for Observer; the Statement of Responsibility; the Non-Employee observer Agreement; complete applicable Visiting Resident or Student Application Form, and provide the following prior to start of observership:
i. Registration with the Florida Board of Osteopathic Medicine for rotation at PBCGME (Residents only)
ii. Completion of PBCGME background check (fee paid by Observer) iii. Documentation that Observer is in good standing at an existing program or school iv. Is paid a salary and by whom (Resident) v. Has paid malpractice insurance, by whom, effective in the State of Florida
vi. Has paid health insurance and by whom vii. Is up to date on all required vaccines and TB testing
b. Supervising Physician Responsibility:
The Observer shall be under the direct supervision of Supervising Physician for the entire Observation Period. The Supervising Physician will be responsible for the direct supervision of Observers at Hospital. Such responsibilities shall include, but not be limited to, the following:
i. Orientation and direct personal supervision of Observers and his/her performance and
activities at Hospital as well as adherence to the standards of conduct as set forth in
accordance with the all applicable rules, regulations, laws, protocols, bylaws and policies of
the Hospital and its professional or medical staff, as well as PBCGME including but not
limited to the Health Insurance Portability and Accountability Act (HIPAA);
Core Manual July 2014 page 46
ii. Securing and documenting written authorization from Hospital’s patients with whom
Observers may come in contact for personal interaction or observation, or for observation of
procedures performed in Hospital using the Consent for Observation attached hereto as
Exhibit D;
iii. Assuring that Observers shall not at any time become personally involved in the rendering of
care to Hospital’s patients;
iv. Prohibiting Observers from accessing patient medical records in written or electronic form, and limiting access to other protected health information to the minimum necessary, in compliance with HIPAA;
v. Performing such other supervisory duties as may from time to time be required by Hospital
and/or PBCGME.
The Supervising Physician will notify PBCGME sufficiently in advance of the start of the Observation Period to allow PBCGME to provide the Observer with necessary orientation and HIPAA training. Neither the Supervising Physician nor the Supervising Physician’s practice may receive any remuneration from Observer or Observer’s program for providing supervision of Observer’s rotation. c. Observers/Shadows
Pursuant to HCA Policy, only authorized individuals are observing or shadowing within the facility. It is not appropriate to allow unauthorized observers or shadows to view procedures, enter patient rooms, etc. The following frequently asked questions provide guidance on when it may or may not be appropriate from a privacy perspective:
May we allow high school students to “shadow” health care workers or participate in “take your son/daughter to work days”? It depends. If the observer is not going to enter a patient room, review records or observe surgeries, etc., we believe that the disclosures are incidental. No authorization would be needed. If the observer does enter a room, observe a surgery, etc., individual patient authorization is required. Many facilities across the country have discontinued these types of activities altogether.
May a physician or other health care worker bring a “shadow” (e.g., during rounds)? HIPAA allows an individual who is a part of a formalized training program or part of a formal agreement with the facility, where they are learning under supervision to practice or improve their skills, to receive PHI. It does not allow for an individual who is a friend or acquaintance to receive PHI. If the “shadow” does not enter a patient room, review records or observe surgeries/procedures, any observations would be incidental.
What documentation is needed when the individual is part of a formalized training program or part of a formal agreement with the facility, where they are learning under supervision to practice or improve their skills? PBCGME will be responsible for the HIPAA compliance training as part of orientation.
VIII. ORGANIZATION
1. LEADERSHIP The Program Directors are directly responsible for the day-to-day operation of the residency programs, and report to the DME, who reports to the Regional DME. The Regional DME is an employee of the Palm Beach Consortium for Graduate Medical Education and reports directly to the Chief Executive Officers of the hospitals, who are ultimately responsible for all aspects of the graduate medical education programs.
Core Manual July 2014 page 47
2. COMMITTEES a) CURRICULUM AND ADVANCEMENT COMMITTEES: Resident performance is monitored
regularly by various evaluation tools, including monthly competency-based evaluation forms. Faculty performance and rotation effectiveness is monitored regularly by various evaluation tools, including monthly competency-based evaluation forms. All such performance is reviewed at the programs’ Curriculum and Advancement Committees, which meet at least quarterly. Based upon these reviews, these committees make recommendation to the Medical Education Committee pertaining to resident advancement, appointment and maintenance of faculty teaching responsibilities, and curriculum planning. Minutes are reported to the Medical Education Committee
i. MEMBERSHIP: Membership of the Curriculum and Advancement Committees is through appointment by the Director of Medical Education, based upon recommendation of the Program Directors. In addition to the Regional DME, DME (both who sit ad-hoc) and the Program Director (who chairs), Committee members include key faculty. A representative of administration is a nonvoting member. The Administrative DME serves as committee secretary.
b) MEDICAL EDUCATION/GOVERNANCE COMMITTEE: The Medical Education/Governance Committee of the Palm Beach Consortium for Graduate Medical Education is organized to assist the Regional DME and DMEs in developing and implementing a high-quality educational program for Housestaff. The committee, in cooperation with the DMEs, develops a curriculum and methods to evaluate the educational experience of the Housestaff during training. The committee participates in program, faculty, resident evaluations, as well as program modification as needed in accordance with evaluation results. The committee reviews program, faculty, intern and resident evaluation processes, as well as ensures program modification by specialty and program director as needed in accordance with evaluation results. When necessary the committee approves affiliations within the scope of AOA policies and procedures. The Committee is responsible for the development, implementation and oversight of the internal review process and monitors duty hours and moonlighting compliance.
i. MEMBERSHIP: The Medical Education/Governance Committee is comprised of the Regional DME (chair), individual institution DMEs, individual program directors (or their designee), Chief Executive Officers (CEOs) of each primary PBCGME facility at which residencies are based, ADMEs, Regional Medical Education Coordinator, Alumni Representative, and Chief Administrative Resident. Other members may be appointed, from time to time, by the Regional DME. The Regional Medical Education Coordinator serves as committee secretary. All members are strongly encouraged to attend the education committee meetings when logistically possible, or send a representative when they are unable to attend.
1. CEOs and major affiliate representatives will report on updates to their facilities, as well as any issues that may affect or involve GME.
2. Chief Administrative Resident will report on updates pertaining to the Council and issues involving Housestaff, as well as updates on Emergency Preparations/Disaster Response, Community Service, Resident Activities and CISM).
3. Program Directors will present minutes of quarterly C&A Committees, and monthly updates and issues pertaining to their programs.
4. DMEs will present Faculty Reports, Updates on Strategic Plan, Resident Performance and Best Practices.
ii. The Medical Education/Governance Committee will meet monthly (at least ten times per year) and is responsible for maintaining improving program quality. Meetings of this committee are held at the sponsoring OPTI, and minutes are reported to the Medical Executive Committees of the sponsoring hospital and base hospitals of all residency programs.
iii. There is an Executive Committee of Medical Education/Governance Committee, comprised of the Regional DME, DMEs and CEOs. This Executive Committee is authorized
Core Manual July 2014 page 48
to conduct urgent or emergent business, as deemed necessary by the Regional DME, between regularly scheduled meetings of the Medical Education/Governance Committee.
iv. Through the individual DMEs, the Regional DME prepares and presents an annual report on the “state of AOA educational programs in the institution” to the Medical Staff and Governing Boards of each participating facility, with a copy to the OPTI. Copies of annual reports shall be available for on-site reviews. The annual report will review the activities of the Medical Education Committee and programs with attention to: 1. The supervision, responsibilities, and evaluation of interns, residents, and fellows; 2. Compliance with the duty hour standards in base institution and at affiliated
institutions; 3. The base institution’s internal review activities; 4. The safety and quality of patient care provided by the trainees; 5. Progress on the Core Competencies.
d. RESIDENT COUNCIL: Resident Council is a peer organization supported by the PBCGME Graduate
Medical Education Committee. The Resident Council serves as a liaison between the Housestaff
and program administration. The council is made up of appointed representatives (Chief
Residents) from each accredited graduate medical education program. The council is chaired by
the Chief Dermatology Fellow, or his/her designee, who shall represent the Council, and all
residents, at the PBCGME Medical Education Committee. It is the responsibility of the Chair to
bring pertinent housestaff issues and concerns to the attention of the Medical Education
Committee, as well as to disseminate appropriate and relevant information from that
Committee to the Housestaff.
The Housestaff Council’s purpose: i. Represents the voice of interns/residents and fellows in decisions the PBCGME
makes for graduate medical education. Provides a forum for discussion among
the Housestaff in graduate medical education at PBCGME hospitals about the
educational, professional and work environment issues that relate to their
graduate training at the PBCGME,
ii. Advocates on behalf and in the interest of house staff by seeking issues, relaying
resident concerns, and developing solutions to those concerns. Encourages the
active participation by Housestaff and fellows in the promotion of excellence in
the development, assessment and implementation of their training programs,
iii. Educates by providing a point of communication between Housestaff, faculty,
and PBCGME leadership. Encourages those in training at the PBCGME to discuss
and exchange ideas relevant to professional issues and trends affecting graduate
medical education at the PBCGME,
iv. Organizes and plans social activities for residents,
v. Serves the housestaff overall by the development and implementation of plans
to improve resident and fellow education, service, and life. Offers pertinent
recommendations to the Graduate Medical Education Committee (GMEC),
program directors, faculty and administrators at PBCGME on issues including, but
not limited to work environment, accreditation, and program concerns and
successes as they affect the needs and interests of the Housestaff and fellows at
PBCGME facilities, and
vi. Acts as fact-finding body, at the request of RDME, DME(s) and/or Program
Director(s) to investigate issues pertaining to student or housestaff behavior or
performance.
Core Manual July 2014 page 49
IX. LEGAL STATUS OF HOUSESTAFF; HOUSESTAFF EVALUATION PROCESS; AOA standards require an effective evaluation of all components of PBCGME programs. This evaluation must relate to the educational objectives of the program and shall include the housestaff’s clinical experiences, intellectual abilities and skills, and attitudes and interpersonal relationships. At the completion of each rotation, housestaff will be evaluated on the Core Competencies, by the appropriate professional staff. These evaluations shall be signed by the assigned trainer, reviewed by the Program Director, and maintained on file in the Medical Education Office. The Program Director and Curriculum and Advancement Committee shall review the performance of every resident on a quarterly basis to insure that educational objectives are being met. All evaluations, logs, and summaries are to be submitted no later than three (3) working days after the end of each rotation. Failure to complete these documentation requirements on time may result in disciplinary actions including suspension from rotation, and paychecks being delayed. PBCGME forms will be utilized by the various services to evaluate performance while on each rotation, as well as a form for departmental evaluation of housestaff along with forms for housestaff’s evaluation of the PBCGME rotation. The 360-degree evaluation is beneficial to the Hospital in determining housestaff attitude and performance while on each particular service and also in determining the strengths and or weaknesses of our training programs. It is incumbent upon all housestaff to provide their medical students, underclassman and nurses that they have interacted with during the rotation, with a copy of the 360-degree evaluation form to be returned directly to the Office of Medical Education. To enhance self-learning and improvement, housestaff should complete a 360-degree evaluation on themselves. Faculty must warn Housestaff that their performance is below expectation and that they are in jeopardy of failing the rotation half-way through the rotation, unless the attitude, performance or behavior that warrants failure occurs solely following the half-way point. The Housestaff are also encouraged to routinely request feedback from their faculty at least at the half-way point of a rotation. 1. GENERAL INFORMATION Housestaff are employees of PBCGME facilities and, as such, subject to the terms of the Employee Handbook, as well as this document. Housestaff are responsible to the Board of Trustees, the Chief Executive Officer, and the Regional Director of Medical Education, Director of Medical Education and Program Director. 2. TERMINATION WITHOUT THE RIGHT TO APPEAL: The Institution may terminate the Resident immediately for cause and without the right to counseling or appeal, for any of the following non-academic reasons:
i. Intern/Resident/Fellow’s death or permanent disability. The term “disability” means a physical or
mental impairment that causes Physician to be unable to perform the essential functions of
Physician’s job as set forth in this Agreement for 6 consecutive months, with reasonable
accommodation, after consideration of any job protection benefits afforded by applicable state
or federal law.
ii. Intern/Resident/Fellow’s license or registration with the Florida Board of Osteopathic Medicine
as an unlicensed physician is suspended, subject to probation, revoked, or canceled.
iii. Intern/Resident/Fellow’s professional liability coverage is cancelled by the Institution’s insurer or
Intern/Resident/Fellow becomes uninsurable for any reasonable amount under the terms and
conditions of the professional liability insurance provided.
iv. Upon a determination by the Institution that Intern/Resident/Fellow’s has a measurable quantity
in blood or urine of non-prescribed controlled substances or that Intern/Resident/Fellow’s is
Core Manual July 2014 page 50
working while impaired by alcohol or prescribed narcotics while on the Practice’s property or
during working hours.
v. Upon the imposition of any restriction or limitation by any governmental or professional
authority having jurisdiction over Intern/Resident/Fellow’s to such an extent that
Intern/Resident/Fellow’s cannot engage in the full practice of medicine as an intern, resident or
fellow, as required hereunder;
vi. Upon the determination of the Institution in good faith that Intern/Resident/Fellow’s is not
providing adequate patient care to a degree expected for the Intern/Resident/Fellow’s training
level; or that the health, safety, or welfare of patients is jeopardized by continuing
Intern/Resident/Fellow’s employment;
vii. Insubordination and/or refusal to perform assigned duties.
viii. Violation of AOA Work Hour Rule.
ix. Absence from assigned rotation or scheduled call without prior written approval from the
department of Medical Education.
x. Violation of the regulations regarding confidential information.
xi. Abuse, neglect or inconsiderate treatment of patients, personnel or visitors (e.g., threatening or
intimidating patients, visitors, coworkers or others. Fighting, use of obscenities, etc ...)
xii. Possession of Institution equipment (including library texts) or personal belongings of the
patients or fellow workers without the consent of the owner.
xiii. Unauthorized use or unauthorized possession of illegal or intoxicating substances or substances
which can alter states of consciousness.
xiv. Willful destruction, misuse or defacing of Institution property, equipment or supplies.
xv. Gambling while on duty.
xvi. Soliciting or accepting tips from attendings or patients.
xvii. Violation of the regulations regarding confidential information.
xviii. Lack of commitment to learning
xix. Prejudice
xx. Arrogance
xxi. Lack of accountability
xxii. Failure to submit to drug screening, when requested by DME and/or CEO.
xxiii. Deliberately restricting output and/or gross neglect of duty.
xxiv. Behavior generally considered immoral, unethical or improper in a hospital setting.
xxv. Sexual harassment.
xxvi. Dishonesty.
xxvii. Possession of potentially dangerous weapons.
xxviii. Professional incompetence.
xxix. Substantial breach of the terms of this Agreement or the Training Manual.
xxx. Serious neglect of duty or violation of Institution rules, regulations or policies.
xxxi. Conviction of a crime thought by the Program Director or Director of Medical Education to
render the Intern/Resident/Fellow unfit professionally to practice medicine. Conviction of any
felony.
xxxii. Conduct seriously and clearly prejudicial to the best interest of the Institution.
xxxiii. Falsification of Institution records including falsification of medical records and falsification of
any information supplied to the Institution by the Intern/Resident/Fellow as part of the entrance
requirements of the Program, or knowingly giving false information or assisting others in doing
so.
xxxiv. Intern/Resident/Fellow’s actions or inactions are cause for termination consistent with
Institution’s policies as applied to all employees.
Core Manual July 2014 page 51
xxxv. Intern/Resident/Fellow’s is in material breach of the Intern/Resident/Fellow Agreement.
xxxvi. Any conduct that Institution determines in good faith to be unethical, unprofessional, unlawful,
or fraudulent, is detrimental to patient care, or impairs the reputation or operations of the
Institution, or any behavior that is deemed unprofessional or conduct unbecoming a physician
and/or house officer.
If the Director of Medical Education determines that the Intern/Resident/Fellow has materially breached any of these forms of gross negligence or misconduct, areas, he or she shall be authorized to terminate the Intern/Resident/Fellow Agreement or take such disciplinary action, including fines, as may be appropriate, and dismiss the Intern/Resident/Fellow for cause without the right to appeal or the progressive counseling procedures described herein.
3. ACADEMIC DEFICIENCIES The Hospital and Department have clearly defined procedures for academic and disciplinary action. Academic dismissals result from failure to attain a proper level of scholarship or competence in the seven domains of competency required of osteopathic physicians.
The Program Director will use multiple tools in assessing academic performance, and identifying academic deficiencies. These tools include Resident Evaluations, 360-Degree Evaluations, and In-service Examinations.
The purpose of this policy is to assure that house staff receives procedural due process in matters of academic discipline and promotion. This procedure is to be followed in certain instances in which an Intern/Resident/Fellow is disciplined or not offered promotion to the next OGME level for academic reasons. The Program Director is primarily responsible for decisions on academic discipline and non-promotion of the Intern/Resident/Fellow. The Medical Education Committee assures the Intern/Resident/Fellow of due process in these procedures. . Immediate dismissal without hearing will be allowed where patient or staff safety is judged by the Program Director to be at imminent risk, or for causes listed under Section 4, below.
4. GENERAL APPEAL ISSUES
i. The following sanctions are available in the academic discipline of Intern/Resident/Fellows: 1. Informal resolution, which may or may not be documented in the
Intern/Resident/Fellow’s file. 2. Oral reprimand, a notice of which must be placed in the
Intern/Resident/Fellow’s file. 3. Written reprimand, a copy of which must be placed in the
Intern/Resident/Fellow’s file. 4. Probation, with the length of time specified along with any other sanctions as
specified. 5. Suspension, with the length of time specified. This may be with or without
pay. 6. Non-renewal of contract. 7. Dismissal.
ii. Combination of sanctions may be used. Suspensions and/or terminations may begin
immediately if the Regional DME, DME or Program Director believes that immediate
action is needed to protect the quality of patient care or stable operations of the
hospital. (Sanctions number 4 through 7 may be appealed by the
Intern/Resident/Fellow. However, immediate dismissal without hearing will be
allowed where patient or staff safety is judged by the Program Director to be at
imminent risk, or for causes listed under Termination Without the Right to Appeal
Section, below.) Sanctions that are appealed do not go into effect until the appeal
Core Manual July 2014 page 52
process is completed except for those immediate suspensions/terminations as noted
above.
Intern/Resident/Fellows may respond in writing to sanctions number 2 through 7, which will be entered into the Intern/Resident/Fellow’s file.
iii. The Program Director shall not consider anonymous reports, but need not reveal the
identity of any person reporting information about possibly sanctionable events.
1. The Program Director shall review all reports alleging rule violations or
deficiencies in clinical performance, meet promptly with the
Intern/Resident/Fellow to discuss any reports which the Program Director
believes to have substance, and place a written account of the meeting,
including pertinent discussion, problems identified, and plans for
remediation in the Intern/Resident/Fellow’s file.
5. APPEALS i. An Intern/Resident/Fellow who has received one of the appealable sanctions and
who wishes to appeal it must file an appeal within thirty (30) days of receiving the sanction. Each appeal must be in writing and must specify the sanction being appealed, the reasons for appeal, any new information the Intern/Resident/Fellow wishes to be considered, and any alternate sanctions the Intern/Resident/Fellow might accept. The appeal must be filed with the RDME or DME. Failure to file within thirty (30) days forever bars an appeal by the Intern/Resident/Fellow.
ii. On receipt of an appeal, the DME shall send copies of the appeal to the involved
Program Director and shall name an ad hoc subcommittee to hear the appeal. The
DME shall notify the Intern/Resident/Fellow/Resident/Fellow of receipt of the
appeal and of the membership of the subcommittee. The DME shall request the
record of the meeting at which the sanction was given and other supporting data
from the Program Director. The subcommittee shall consist of the DME and three
other members of the GMEC, a least two of whom are from departments other than
the Intern/Resident/Fellow’s. For an Intern, these two members must be from
departments through which the Intern has not rotated or not directly involved in the
alleged offenses. The DME shall appoint a secretary for the subcommittee.
iii. Within ten (10) days of its formation, the subcommittee shall meet to hear the
appeal. Housestaff are not allowed legal counsel at hearings concerning academic
issues. The Intern/Resident/Fellow may designate another Intern/Resident/Fellow
or a member of the medical staff as his/her representative before the
subcommittee. The hearing proceedings will be closed, and treated as confidential
peer review. The hearing will consist of a presentation by the involved Program
Director and a presentation by the Intern/Resident/Fellow or his/her representative.
The Intern/Resident/Fellow and/or his/her representative may introduce further
written evidence with the permission of a majority of the subcommittee. The
subcommittee has the right to question both presenting parties.
iv. The subcommittee meets in executive session to decide it recommendation. A
majority of the members of the subcommittee must support a recommendation in
order for it to be enacted. The subcommittee is limited to making the following
recommendations:
1. Upholding the sanction
2. Imposing a sanction of lesser severity
3. Imposing no sanction
Core Manual July 2014 page 53
v. The subcommittee’s report will be presented to the GMEC at its next regular
meeting. The report will be in writing and give the subcommittee’s recommendation
and the reasons for it. The GMEC will vote on whether to accept the report. If the
report is not accepted, the DME will within ten (10) days, convene a special meeting
of the GMEC for a de novo appeal hearing, which will be conducted in the same
manner as in C. The Program Director whose decision is being appealed may not
participate in the GMEC’s deliberations or votes. If the report is accepted, in will be
referred to the CEO of the hospital for final action.
vi. The involved Program Director and the Intern/Resident/Fellow shall be informed in
writing of any reports filed or actions taken in the appeal process. The Program
Director will file a copy of all reports and notifications of action in the
Intern/Resident/Fellow’s personnel file.
6. MISCELLANEOUS
xi. A decision not to certify an Intern/Resident/Fellow as eligible for a specialty
certification exam is not a sanction covered by this procedure.
xii. A copy of this procedure has been given to each Intern/Resident/Fellow at the start
of postgraduate training at Palm Beach Consortium for Graduate Medical
Education by incorporation into the Training Manual.
xiii. Notice of sanction, appeal, or committee action may be given by personal service
or by first class mail. Time is of the essence in all proceedings. In cases of
disciplinary infractions that are judged irremediable, the B. hospital and
department will provide the resident with adequate notice, in writing, of specific
ground(s) and the nature of the evidence on which the disciplinary action is based.
The resident will be given an opportunity for a hearing in which the disciplinary
authority will provide a fair opportunity for the resident’s position, explanations
and evidence. Finally, no disciplinary action will be taken on grounds which are not
supported by substantial evidence. The department and/or medical education
committee will act as the disciplinary authority. Housestaff will not be allowed
counsel at hearings concerning disciplinary issues. Pending procedures on such
disciplinary action, the hospital in its sole discretion may suspend the resident,
when it is believed that such suspension is in the best interests of the hospital or
patient care
xiv. Immediate dismissal without hearing will be allowed where patient or staff safety
is judged by the Program Director to be at imminent risk, or for causes listed
under the Termination Without the Right to Appeal Section. If the program’s
Director of Medical Education determines that the Intern/Resident/Fellow has
materially breached any of these forms of gross negligence or misconduct, he or
she shall be authorized to terminate the training agreement or take such
disciplinary action, including fines, as may be appropriate, and dismiss the
Intern/Resident/Fellow for cause without the right to appeal or the progressive
counseling procedures described above. Further, If the Intern/Resident/Fellow by
action or inaction commits or allows to occur any action or course of action,
which the base training institution reasonably believes involved moral turpitude
or is contrary to the interests or patient care or the general welfare of the
institution, the institution may terminate the Intern/Resident/Fellow without
prior notice and without the right to appeal or progressive counseling
procedures.
Core Manual July 2014 page 54
APPENDIX I: CRITERIA FOR FACULTY APPOINTMENT FOR THE ASSUMPTION
OF TEACHING RESPONSIBILITIES University faculty appointments are made by the Osteopathic Post-Doctoral Training Institution (Consortium for Excellence in Medical Education/Nova Southeastern University College of Osteopathic Medicine) and core medical schools based upon the recommendation of the Regional Director of Medical Education. Teaching responsibilities within the programs of the Palm Beach Consortium for Graduate Medical Education are designated by the Regional Director of Medical Education based upon the recommendation and review of the DME/Program Directors and Medical Education Committee. Teaching responsibilities may be revoked at any time, with or without cause, by the Regional Director of Medical Education or DME/Program Directors based upon professional competence, teaching ability, conduct, continued needs of the program or changes in curriculum. Criteria for Appointment of Teaching Responsibilities: The following criteria must be met in order for appointment of teaching responsibilities at the Palm Beach Consortium for Graduate Medical Education (PBCGME):
1. Either personally provide a lecture (at least once per month) to House Staff and/or participate in Morning
Report or other Educational Conference (at least once per month); or accept housestaff on rotation service on a monthly basis, or in longitudinal continuity of care on a weekly basis.
2. For those physicians accepting housestaff on clinical rotation, either inpatient or outpatient, residents
must be provided with goals, objectives and expectations prior to the start of the rotation, verbal assessment of performance mid-way during the rotation, and completion (with return to Medical Education office) of resident evaluations within ten (10) days following completion of rotation.
3. For those physicians assuming teaching responsibilities to include accepting housestaff on their
Consortium rotation service: i. One of the hospitals of the Palm Beach Consortium for Graduate Medical Education must be a
primary hospital of practice in order to provide a sufficient patient base (volume of case activity) at PBCGME to ensure rotation is a rewarding educational experience. For services not available at a PBCGME Hospital, this requirement shall be automatically waived.
ii. Teaching Physician must meet all criteria for staff membership. iii. Application for teaching faculty responsibilities may be made any time after six months of
medical staff membership at a PBCGME facility. The physician must be in good standing on the medical staff, and not have any outstanding peer review or utilization management issues.
iv. Teaching Physician must available to respond to the housestaff and program administration in a timely and professional manner;
v. Teaching Physician must demonstrate willingness and availability to provide instruction at the bedside settings, and to allow the intern/resident an active role in patient care under supervision.
4. For those physicians assuming teaching responsibilities to include accepting housestaff into their
ambulatory clinical setting: i. Demonstrate willingness and availability to provide instruction in the ambulatory setting, and to
allow the intern/resident an active role in patient care under supervision. 5. For those providing monthly lecture, or participating in morning report or other educational conference:
i. May not have more than three (3) unexcused absences per year. If unable to attend due to foreseen circumstance (such as vacation), must find substitute presenter (or swap days with another lecturer). If unable to attend due to unforeseen circumstance (e.g., patient emergency), must contact the Chief Resident, or Office of Medical Education, to alert for the need of a back-up lecture.
Core Manual July 2014 page 55
6. Satisfy all of the AOA standards which include qualification, by training and experience to perform the role assigned, proficiency in their area of practice and training and experience to perform this role.
7. Have a genuine interest and ability in teaching. 8. Abide by the policies of the Department of Medical Education, including the Training Manuals and the
Code of Conduct.
9. Have access to the internet and regularly (on at least a weekly basis) check an email account, the address of which is provided to (and updated with) the Medical Education Department.
10. Be Board Certified (or Eligible, if within one year following completion of their training) in their medical
specialty by AOA or ABMS. 11. Teaching Physicians must participate in periodic faculty development activities. These activities must be
recorded on a curriculum vita or other Consortium/OPTI records for review at program/OPTI on-site reviews. If unable to attend, they shall review a video-tape of the presentation, or review salient features of the program with the training program director.
12. Core faculty must demonstrate a minimum of 15 hours of faculty development over the course of 5 years.
Core faculty members are either defined by the specialty college or are those faculty members who play a significant role in curricular development, delivery, assessment of residents and of the program.
13. Teaching Physicians must be competent in recognizing early fatigue and sleep deprivation and to alter schedules and counsel residents as necessary, while maintaining continuity of patient care.
14. Upon request of the Director of Medical Education or Program Directors, faculty members with teaching responsibilities must demonstrate a willingness to participate in the interview process for internship and residency candidates, who are interested in postdoctoral training programs relevant to the respective faculty member’s medical field and provide feedback or recommendations to the Director of Medical Education or Program Directors, regarding candidate’s qualifications.
15. Upon the recommendation of the Director of Medical Education or Program Directors, certain criteria
may be waived at the discretion of the Medical Education Committee. Circumstances for waiving of criteria may include:
i. Immediate appointment to faculty status and teaching responsibility to ensure compliance with internship or residency program requirements;
ii. A prevailing shortage of specific specialty physicians on teaching faculty, which may necessitate recruitment of adjunct faculty not on staff at a PBCGME Consortium.
iii. A candidate for teaching faculty appointment is joining an active practice whose associates are currently active teaching faculty members at PBCGME; and where such candidate will have immediate access to sufficient patient volume with which to meet above criteria.
iv. A graduate of a residency training program at PBCGME who has just entered into private practice.
16. All teaching physicians are expected to act in accordance with the terms of the PBCGME Code of Conduct
and to conduct themselves in a respectful and ethical manner commensurate with the principles and practices of the highest standards of medical care in their relationships with patients, house staff, medical students, physicians, Consortium employees and with the Consortium and community as a whole.
17. Based upon the fixed number of House Staff at PBCGME annually (e.g., in accordance with the number of
funded positions under the Medicare cap limit and the number of accredited positions per program), the daily responsibilities of such House Staff in response to faculty and their patients, and the limited number of lectures available in a given month, there may be a limit placed on the number of faculty that may be approved at any one time. Accordingly, meeting the above criteria does not ensure or entitle any right to appointment or reappointment to faculty status and/or teaching responsibilities. Further, appointment
Core Manual July 2014 page 56
to faculty status and/or teaching responsibilities does not ensure or entitle any right to the faculty member being scheduled for lectures, or being assigned medical students, or housestaff to their service.
APPENDIX II: Resident Work Hours Policy
Trainee Duty Hours Policy
Situations in which trainees work an excessive numbers of hours can lead to errors in judgment and clinical decision-making, and negatively impact the physical and mental well-being of trainees. These errors can impact on patient safety, as well as the safety of the physician trainees through increased motor vehicle accidents, stress, depression and illness.
PBCGME, its base institutions, DMEs, and program directors make every attempt to avoid scheduling excessive work hours leading to sleep deprivation, fatigue or inability to conduct personal activities.
Residents are not assigned to work physically on duty in excess of 80 hours per week, averaged over a 4-
week period, inclusive of in-house night call and any allowed moonlighting. No exceptions to this policy
are permitted.
Residents may not work in excess of 24 consecutive hours.
a. Allowances for already initiated clinical care, transfer of care, educational debriefing and
formal didactic activities may occur, but shall not exceed 4 additional hours and must be
reported by the resident/fellow in writing with rationale to the DME/program director and
reviewed by the MEC for monitoring individual residents and program. These allowances are not
permitted for OGME-1 trainees.
b. Residents may not assume responsibility for a new patient or any new clinical activity after
working 24 hours.
Residents must have 48-hour periods off on alternate weeks, or at least one 24-hour period off each week and have no call responsibility during that time. At-home call is not assigned on these free days.
Upon conclusion of a 20-24 hour duty shift, trainees must have a minimum of 12 hours off before being required to be on duty or on call again.
a. Upon completing a duty period of at least 12 but less than 20 hours, a minimum period of 10 hours off must be provided.
All off-duty time must be totally free from clinical or assigned classroom educational activity.
Rotations in which a resident is assigned to Emergency Department duty must ensure that residents work no longer than 12 hour shifts with no more than 30 additional minutes allowed for transfer of care and shall be required to report in writing to the DME/program director for review by the MEC, only any time exceeding the 30 additional minutes, for monitoring individual trainees and program.
In cases where a resident is engaged in patient responsibility which cannot be interrupted at the duty hour limits, additional coverage will be assigned as soon as possible by the attending staff to relieve the trainee involved. Patient care responsibility is not precluded by the duty hours policy.
The resident will not be assigned to in-hospital call more often than every third night averaged over any consecutive four-week period. Home call is not subject to this policy, however it must satisfy the requirement for time off. Any time spent returning to the hospital must be included in the 80 hour maximum limit.
At the residents request, the training institution will provide comfortable sleep facilities or provide another mechanism for a resident to return home (e.g. cab fare) to trainees who are too fatigued at shift conclusion to safely drive.
Core Manual July 2014 page 57
APPENDIX III: Resident Supervision Policy
Trainee Supervision Policy 1. GENERAL
Housestaff are employees of their PBCGME base-facility, and are under the supervision of the Chief Executive
Officers, Regional Director of Medical Education, Directors of Medical Education, Program Directors and
Associate Program Directors. With respect to participation in direct patient care activities, the Housestaff are
responsible to the attending physician. With respect to overall professional training and academic affairs, the
Housestaff are responsible to the Regional Director of Medical Education, or his/her designee. In all other
respects, the Housestaff are responsible to the Chief Executive Officer of the Hospital or his/her designee, for
the faithful and satisfactory performance of duties as a member of the hospital organization. The Medical
Education Committee is concerned only with the education of the resident, the quality of his or her work, and
his/her demeanor and professionalism. Like other employees and medical staff, and Housestaff must obey
the rules which have been established. Cooperative effort between all groups is the most productive of
harmonious relationships.
OGME training is designed to offer structured and supervised exposure to balance learning with service appropriate to trainee levels of documented expertise. Housestaff are, within broad limits, responsible for the patients on their service. In the clinical learning environment, each patient must have an identifiable, appropriately‐credentialed and privileged attending physician who is ultimately responsible for that patient’s care. Legally, the attending physician is responsible for everything pertaining to the patient; including any orders housestaff may write. Therefore, housestaff should not add to or change any physician's order without first consulting the attending physician. In an emergency, housestaff may act immediately to save a life/limb or prevent permanent disability and then immediately consult with the attending physician. Housestaff are required to call the attending physician when adding to or changing orders. As the individual resident progresses through the training process and develops competencies, attending physician will grant liberties based upon the residents competencies and abilities. The privilege of progressive responsibility in patient care delegated to each intern/resident must be assigned by the program director and attendings functioning as supervising physicians. Supervision is provided on a graduated basis as the trainee progresses through the training program, based on evaluation of individual knowledge and skill as well as institutional policy, program and specialty college requirements.
a. The supervising physician is responsible for determining the activities the trainee will be allowed to perform within the context of the assigned levels of responsibility, and for being available to the trainee.
b. Trainees are responsible for seeking consultation when it is clinically indicated, based on the trainee’s level of training and institutional policy.
PBCGME programs demonstrate that the appropriate level of supervision is in place for all interns/residents who care for patients. Supervision may be exercised through a variety of methods. Some activities require the physical presence of the supervising attending. Interns/residents and attendings should inform patients of their role in the patient’s care. Attending physician supervision assignments are of sufficient duration to assess the knowledge and skills of each intern/resident and delegate to him/her the appropriate level of patient care authority and responsibility.

Core Manual July 2014 page 58
The program director will evaluate each intern’s/resident’s abilities based on specific criteria. When available, evaluation should be guided by specific national standards‐based criteria. The intern/resident is responsible for knowing the limits of his/her scope of authority, and the circumstances under which he/she is permitted to act with conditional independence. In particular, OGME‐1 interns/residents should be supervised either directly or indirectly with direct supervision immediately available. Trainees participate in supervision of other trainees at lower levels of OGME in their respective specialties. Senior residents or fellows should serve in a supervisory role of junior interns/residents in recognition of their progress toward independence, based on the needs of each patient and the skills of the individual resident or fellow.
PBCGME programs have set guidelines for circumstances and events in which interns/residents must communicate with appropriate supervising attendings, such as the transfer of a patient to an intensive care unit, or end‐of‐life decisions. Prior to all admissions, housestaff must consult with the attending of record. As individual members of the housestaff become more proficient, attendings may grant them greater liberties.
The attending physician (and consultants, if appropriate) must be called for any significant change of status, or transfer of patients.
Tip: Attendings (and more senior residents) should never be called and simply asked what to do. Always have a plan to present.
All patients admitted by a resident through the emergency room must be seen by the emergency medicine physician, and a direct conversation must be held between the emergency medicine attending physician and the resident’s supervising attending physician, in order that the attending physician be directly aware of and accept the admission. That conversation should include the elements of patient condition, admitting diagnosis and treatment plan, which will then be relayed by either of the attending physicians to the resident doing the admission.
2. LEVELS OF SUPERVISION
In the development and description of systems to oversee intern/resident supervision and graded
authority and responsibility, each program uses the following classification of supervision.
a. Direct Supervision —The supervising physician is physically present with the intern/resident and
patient
b. Indirect Supervision:
i. Direct supervision immediately available – The supervising physician is physically within
the confines of the site of patient care, and immediately available to provide Direct Supervision
Example: The intern/resident is seeing patients in a clinic setting, and the supervising physician in his/her office is immediately available to see the patient together with the intern/resident as needed. The supervising physician is in another area of the hospital, but is immediately available to see the patient together with the intern/resident in the labor and delivery department as needed.
ii. Direct supervision available – The supervising physician is not physically present within
the confines of the site of patient care, is immediately available via phone, and is available to
provide Direct Supervision.
Core Manual July 2014 page 59
Example: An intern/resident is on call for the internal medicine service and needs advice from
the supervising physician in order to manage a patient’s care. This can be done either by
telephone or electronically. After communication with the intern/resident, if the attending
determines additional assistance is needed, the attending physician is available and able to go to
the hospital and see the patient together with the resident.
vii. Oversight-The supervising physician is available to provide review of
procedures/encounters with feedback provided after care is delivered.
Example: A resident is seeing a patient in either the nursing home or at home, and the
supervising physician can then review the patient chart, discuss.
3. SUPERVISION OF PROCEDURES.
a. Direct Supervision
Interns/residents will need to demonstrate SUCCESSFUL COMPLETION of program-specific set number procedures completed under the direct supervision of an attending physician credentialed to perform that procedure at the facility in which the procedure is being done prior to being authorized to perform such procedures under indirect supervision. Procedure logs must be signed by the attending physicians who are credentialed to perform that specific procedure at the facility within which the Housestaff are rotating, and who has observed him or her perform the procedure competently. Note: competence includes the ability to appropriately explain the procedure, discuss risks, and obtain consent along with the preparation, mechanics of the procedure, and follow-up. When the required number of signatures (may vary from program to program) are received for a given procedure, the log is to be returned to the Program Director for review. The program director may give approval of indirect privileges, or require that additional procedures be done under direct supervision. Once an intern/resident is approved for indirect supervision of a procedure, the Medical Education Office will notify the Nursing Department. Completion of procedure logs is essential in order to verify competency to outside organizations, following graduation.
b. Indirect Supervision
Any procedure that requires a formal, documented patient consent (e.g., chest tubes, central
lines, lumbar punctures) must be done with direct supervision immediately available, where the
supervising physician is physically within the confines of the site of patient care, and immediately
available to provide Direct Supervision
i. In an EMERGENCY situation, where a patient risks death if the procedure is not done
immediately, the intern/resident may act to do what is necessary to save a life, even if
the supervising physician is not immediately available.
c. Other procedures (e.g., insertion of intravenous lines, venipuncture for blood work, vaccines)
may be done with direct supervision available, where the supervising physician is not physically
present within the confines of the site of patient care, but immediately available via phone, and
is available to provide Direct Supervision.
4. Resident/Patient Caps
The Palm Beach Consortium for Graduate Medical Education is committed to a culture of and
commitment to quality patient care, patient safety and appropriate education. Accordingly, on inpatient
services, OGME-1 residents should each be responsible for no more than 6 patients, and upper level
residents should each be responsible for no more than 12 patients.
Core Manual July 2014 page 60
APPENDIX IV: Code of Conduct
PURPOSE To ensure quality Medical Education by promoting a safe, cooperative, professional health care environment and to prevent or eliminate, to the extent possible, conduct that:
Disrupts the operation of the program or hospital; Affects the ability of others to do their job; Creates a “hostile work environment” for medical students or members of the teaching or house staffs; Interferes with an individual’s ability to practice or learn competently; and/or Adversely affects or impacts the community’s confidence in the hospital’s ability to provide quality medical education.
PROFESSIONALISM The Hospital’s educational mission is promoted by professionalism in faculty/house staff/ student/staff relationships. Professionalism is fostered by an atmosphere of mutual trust and respect. Actions of teaching staff or house staff members that harm this atmosphere undermine professionalism and hinder fulfillment of the Hospital’s educational mission. Students and house staff members should, at all times, address attending physicians by using their last name, only (e.g., Dr. Smith). Students/house staff members and members of the teaching staff should limit their interactions, including social interactions, to that of a professional nature, only. Trust and respect are also diminished when those in positions of authority abuse or appear to abuse their power. Those who abuse their power in such a context violate their duty to the hospital and teaching program. SEXUAL HARASSMENT includes unwelcome sexual advances, requests for sexual favors, and other verbal or physical conduct of a sexual nature. Policy: PBCGME does not tolerate sexual harassment by and to house staff members and responds to every complaint, providing proper remediation when harassment is determined.* Definition: Unwelcome sexual advances-requests for sexual favors and other verbal or physical conduct of a sexual nature-constitute sexual harassment when: 1. Submission to such conduct is made either explicitly or implicitly a term or condition of an individual's employment or education or training or 2. Submission to or rejection of such conduct by an individual is used as the basis for employment or academic decisions affecting such individuals or 3. Such conduct has the effect of unreasonably interfering with an individual's work or academic performance or creating an intimidating, hostile, or offensive working or learning environment. Complaint Procedures: Individuals who believe that they have been sexually harassed should notify either their Program Director, or the Regional Director of Medical Education, or the Director of Medical Education. Because of the sensitive and discriminatory nature of the charges of sexual harassment, complaint procedures will include the following principles: 1. Efforts will be made to restrict information regarding complaints to the complainant, the accused party, and those persons directly involved in processing the matter. 2. The Regional Director of Medical Education will advise and consult with either or both parties to the complaint. 3. If necessary, a formal investigation of the complaint will be conducted by the Regional Director of Medical Education or his designee. 4. Investigations will be conducted as promptly as possible, and results will be reported to both parties involved. 5. If a complaint is found to be valid, action will be taken through appropriate channels of program administration, hospital administration and medical staff to rectify the situation and to reasonably ensure that such incidents do not occur in the future. Appeal will be open to either the complainant or the accused party. 6. The Human Resources Office will serve as a resource with regard to interpretation of sexual harassment guidelines. *Equal Employment Opportunity Commission "Guidelines on Discrimination Because of Sex" (29CFR 1604.011) define sexual harassment and consider it a violation of Title VII of the Civil Rights Act of 1964.

Core Manual July 2014 page 61
CONSENSUAL RELATIONSHIP Members of the teaching staff exercise power over house staff, students, and staff whether in providing praise or criticism, evaluations, recommendations for their further studies or future employment, or conferring other benefits. All amorous or sexual relationships between members of the teaching staff and house staff members, students, or personnel staff are unacceptable when the teaching staff member has any professional responsibilities for the other. Such situations greatly increase the possibility that teaching staff members will abuse power and this abuse may lead to sexual exploitation. Voluntary consent by the other in such a relationship is suspect, given the fundamental asymmetric nature of the relationship. Moreover, house staff, students, and staff may be affected by such unprofessional behavior because it places the teaching staff member in a position to favor or advance one person's interest at the expense of others and implicitly makes obtaining benefits contingent on amorous or sexual favors. Therefore, the hospital will view such relationships as a violation of this policy if teaching staff members engage in amorous or sexual relations with house staff members, students, or staff for whom they have professional responsibility even when both parties have consented or appear to have consented to the relationship. Should a teaching staff member find him/herself in a supervisory relationship with someone he/she has already had a relationship with, he/she should notify the Director of Medical Education or Program Director immediately and ask for reassignment. Any concerned person may initiate complaints about alleged violations of this policy. Such complaints should be brought to the attention of the Regional Director of Medical Education or designee. House staff members exercise power over other house staff, students, and staff whether in providing praise or criticism, evaluations, recommendations for their further studies or future employment, or conferring other benefits. All amorous or sexual relationships among house staff members, between house staff and students, or house staff and personnel staff are unacceptable when the house staff member has any professional responsibilities for the other. Such situations greatly increase the possibility that house staff members will abuse power and this abuse may lead to sexual exploitation. Voluntary consent by the other in such a relationship is suspect, given the fundamental asymmetric nature of the relationship. Moreover, other house staff, students, and staff may be affected by such unprofessional behavior because it places the house staff member in a position to favor or advance one person's interest at the expense of others and implicitly makes obtaining benefits contingent on amorous or sexual favors. Therefore, the hospital will view such relationships as a violation of this policy if house staff members engage in amorous or sexual relations with other house staff members, students, or staff for whom they have professional responsibility even when both parties have consented or appear to have consented to the relationship. Should a house staff member find him/herself in a supervisory relationship with someone he/she has already had a relationship with, he/she should notify his/her supervisor immediately and ask for reassignment. Any concerned person may initiate complaints about alleged violations of this policy. Such complaints should be brought to the attention of the Regional Director of Medical Education or designee. Sanctions appropriate to the offense will be applied by the Regional Director of Medical Education or designee. Possible sanctions may include, but are not limited to, removal of teaching privileges, reprimand, consideration in promotion decisions, termination of employment, and immediate dismissal. House staff members disciplined or terminated on grounds of violation of this policy shall have such rights as are provided in the Resident Manual. ZERO TOLERANCE POLICY FOR UNPROFESSIONAL OR ABUSIVE BEHAVIOR Background: Numerous studies have demonstrated that medical students and house staff often believe they are abused in the setting of medical education. Because the relationship between faculty and students or house staff is hierarchical, it remains the ethical responsibility of the faculty to assure that those students and house staff are professionally mentored and respectfully treated. A renewed interest in teaching professionalism to medical students and house staff has been demonstrated by a variety of organizations such as the AOA, ACGME, AAMC, and AMA.

Core Manual July 2014 page 62
PBCGME believes that all patients, ancillary support personnel, co-workers and students are entitled to equitable, respectful, and professional interaction. Also that professionalism is best learned through a mentoring process between the faculty and students. Policy: 1) The program directors will address any perceived breaches of professional behavior with medical staff members, house staff, or their supervisors. 2) Continued violations of this policy shall be reported to the Director of Medical Education or designee. 3) Criticism of performance will be discussed in private with the student or intern/resident/fellow. 4) Discussions about patient care with consulting medical staff among house staff or students will be carried out in a civil tone and volume. Shouting, cursing, name-calling or personal attacks have no place in such discussions. When physically present in the hospitals, professional conversation and interactions are critical to patient care and to the functions of the hospitals. IMPAIRED PRACTITIONER Policy: It is the policy of this hospital and teaching program to properly investigate and act upon concerns that a member of the teaching or house staff is suffering from impairment. The hospital will conduct its investigation and act in accordance with pertinent state and federal law, including, but not limited to, the Americans With Disabilities Act. Procedure: If the DME/PD/Regional Director of Medical Education has a reasonable suspicion that a member of the Teaching or House Staff is impaired, physically, mentally or due to drugs or alcohol, he/she shall takes steps to preserve the educational process and facilitate the safety of the impaired staff member. Upon suspicion of drug or alcohol abuse, the DME, in consultation with the hospital’s Chief Executive Officer (or his/her designee) may order drug testing of the practitioner. Refusal to submit to testing will be grounds for immediate dismissal from the teaching program. If the impairment of a member of the teaching places the educational process is in jeopardy, the DME shall remove that practitioner from teaching staff. If the member of the teaching staff is also a member of the medical staff, the DME may refer, in writing, to the Physician Support Committee for investigation and report to be submitted to the Executive Committee. If the impairment of a member of the housestaff places the teaching program or patient safety in jeopardy, the DME shall suspend all patient care activities of that practitioner, and refer the practitioner to the Physician Support Committee for investigation with a report to be submitted to the Medical Education Committee.
Core Manual July 2014 page 63
APPENDIX V: Substance Abuse Policy PBCGME is committed to the philosophy that an effective physician is a good teacher. On each clinical service, residents participate actively in the clinical instruction of third year and fourth year medical students. Residents also teach other physicians and professional staff through interactions and formal presentations.
SCOPE: All Company-affiliated facilities including, but not limited to, hospitals, ambulatory surgery centers, home health agencies, physician practices, service centers, outpatient imaging centers, and all Corporate Departments, Groups, Divisions and Markets. This policy covers all employees and students as well as those applying for employee positions.
PURPOSE: To prohibit inappropriate drug or alcohol use by our employees and students in the workplace in order to prevent a threat to the quality of care we provide to patients, the safety of our workplace and a healthy work environment. To articulate our intent that all conduct be consistent with all relevant federal, state and local laws and regulations relating to drug or alcohol use by employees (this includes employees and Facilities outside the U.S. and the laws of the country where the Facility is located) and students. To the extent that this policy conflicts with such laws and regulations, such laws and regulations will govern.
POLICY: 1. Assistance
a. The Company recognizes that alcohol abuse, substance abuse, and addiction arise out of treatable illnesses. The Company also realizes that early intervention and support improve the success of rehabilitation. To support employees, the Company: i. Encourages employees to seek help if they are concerned that they or their family members may have
a drug and/or alcohol problem. ii. Encourages employees to utilize the services of qualified professionals in the community to assess the
seriousness of suspected drug or alcohol problems and identify appropriate sources of help. iii. Offers all employees and their family assistance with drug or alcohol problems through the Employee
Assistance Program (EAP). iv. Allows eligible staff the use of vacation time while seeking treatment for drug or alcohol problems.
b. Treatment for alcoholism and/or drug use disorders may be covered by a personal benefit plan. However, the ultimate financial responsibility for treatment belongs to the individual.
2. Shared Responsibility a. A safe and productive workplace free of inappropriate alcohol or drug use is achieved through cooperation
and shared responsibility. b. It is the responsibility of each employee and student to:
i. Adhere to this policy. ii. Notify his or her supervisor at the Facility of any arrest or conviction involving drugs or alcohol prior to
his or her next scheduled shift or clinical duty. iii. Cooperate fully with any investigation related to alleged violations of this policy. iv. Investigate, report, and/or intervene in the event of reasonable suspicion of violations of this policy. v. Safeguard Controlled Substances from unauthorized access.
3. Prohibited Behavior
a. The following activities are strictly prohibited and may lead to discipline, up to and including immediate discharge: i. The sale, manufacture, distribution, purchase, use, or possession of alcohol, alcoholic beverages,
illegal substances, non-prescribed controlled substances, or drug paraphernalia by an employee or student on Facility premises or during his or her working hours.
ii. Reporting to work, or being at work, while under the influence of or while impaired by alcohol,
Core Manual July 2014 page 64
alcoholic beverages, illegal substances, prescribed or non-prescribed controlled substances. For the purpose of the Policy, an employee or student is presumed to be under the influence of alcohol if a blood test or other scientifically acceptable testing procedure shows a blood alcohol level of .04 or more.
iii. Reporting to work, or being at work, with the smell of alcohol on one’s breath or person, or a measurable quantity of non-prescribed Controlled Substances in one’s blood or urine.
iv. A conviction for sale or possession with intent to distribute any drugs, including prescription drugs. v. Theft or diversion of facility medications. vi. Refusal for any reason to submit or consent to a drug/alcohol screen requested by any management
personnel at the Facility. vii. Participation in any act that would create or allow false documentation of security and/or safety
practices. viii. Tampering with or otherwise altering drug testing samples or security equipment or systems.
b. Notwithstanding the foregoing, during facility-sponsored activities, the facility CEO, Administrator, Practice Manager or individual with senior level responsibility for the facility, at his/her discretion, may approve the responsible and limited serving of alcoholic beverages.
c. Prescription medications are not prohibited under this policy when taken as prescribed under the direction and monitoring of a physician.
4. Duty to Report, Detection and Reasonable Suspicion
a. An employee or student must notify his or her supervisor whenever he or she is taking a prescribed or over-the-counter drug that the employee or student has been advised will, or based upon the drug profile is likely to, impair job performance (e.g., drowsiness or diminished ability to focus)
b. An employee or student must notify his or her supervisor if the employee or student has reasonable concerns that another employee or student has violated this policy.
5. Searches If a supervisor has a reasonable suspicion that an employee or student has violated this policy, the supervisor may require the employee or student to submit to a search or inspection. By entering Facility property, each employee or student consents to such searches and inspections. Searches can be conducted of pockets, clothing, lockers, wallets, purses, briefcases, lunchboxes, backpacks, duffel bags, desks, work stations, equipment, and other areas. See also the Company’s general policy regarding searches in the Theft and Violence in the Workplace Policy, SS.001.
6. Drug and Alcohol Testing a. To ensure the accuracy and fairness of our testing program, all collection and testing will be conducted
pursuant to guidelines established by the Medical Review Officers and, if applicable, in accordance with Substance Abuse and Mental Health Services Administration (SAMHSA) guidelines; a confirmatory test; the opportunity for a split sample; review by an MRO, including the opportunity for employees or students who test positive to provide a legitimate medical explanation, such as a physician's prescription, for the positive result; and a documented chain of custody.
b. All drug-testing information will be maintained in separate confidential records. c. Employees and students will be required to participate, at a minimum, in testing as follows:
1) post offer, pre-employment; 2) prior to an acquisition which includes the employment of the seller’s employees, Corporate
Human Resources will compare the seller’s drug testing policy to this policy in the required due diligence process and will make a recommendation to the Division President expected to operate the newly acquired business based on that comparison.
3) upon reasonable suspicion; 4) after a reportable accident; and 5) after an on-the-job injury to any person (e.g., another employee, student, a patient, the person to
be tested) when it is possible that the acts or omissions of the employee or student to be tested may have caused or been partially responsible for the injury.
d. Substances tested for at hire must at a minimum include amphetamines, barbiturates, benzodiazepines, opiates, marijuana, codeine, and cocaine. Reasonable suspicion and reportable accident testing should
Core Manual July 2014 page 65
include amphetamines, barbiturates, benzodiazepines, carisoprodol, opiates, fentanyl analogues, methadone, meperidine, marijuana, and cocaine.
e. Testing for the presence of alcohol will be conducted by analysis of breath, saliva, blood or other accepted testing methodology.
f. Testing for the presence of the metabolites of drugs will be conducted by the analysis of urine, blood, saliva, or other accepted testing methodology.
g. The MRO will review all non-negative reports. Any non-negative drug test result due to a physician-approved medication will be reported as a negative result. If it appears that the person tested is impaired by the use of medications for which the employee or student has a valid prescription, the report should note that fact. Medications that could affect an applicant’s ability to perform his or her job may result in restrictions or recommendation for accommodation with respect to those tasks.
7. Violations of Policy
Employees or students will be subject to discipline, including possible termination, if they violate this policy in any way.
8. Pre-Employment Tests With respect to a person who has been offered employment, if the person refuses to take the pre-employment drug tests described above, or tests positive for any non-prescribed Controlled Substances or Illegal Substances, the offer of employment will be withdrawn.
DEFINITIONS: Controlled Substances: any drug or chemical substance whose possession and use are regulated under the Controlled Substances Act. Illegal Substances: any drug the possession or sale of which violates federal law (in the U.S.) or the country, state or local law of the jurisdiction in which the Facility is located. Impairment: Practitioner impairment occurs when a substance-related disorder interferes with his or her ability to engage in professional activities competently and safely. Medical Review Officer (MRO): A licensed physician not employed by HCA or an HCA affiliate who oversees the medical aspects of this policy. The MRO could be affiliated with the reference lab contracted with by the Facility. The MRO should have appropriate medical training to interpret and evaluate an individual’s positive test results, medical history and any other relevant medical information. HCA Affiliate: any entity (partnership, corporation, joint venture, LLC, etc.) that HCA ultimately owns or controls 50% or more of, including its 50% owned joint ventures. Facility: a facility owned by an HCA Affiliate, including, but not limited to, hospitals, ASCs, urgent care and imaging centers, billing offices, revenue service centers, and corporate, division, and market offices. Reportable Accident: Any employee or student involved in an on-the-job accident which involves injury requiring medical treatment or evaluation to the employee, student, or another person, property damage, or lost time from the job will be required to be tested for drugs and alcohol. An exception may be made provided it is immediately apparent to management that the employee or student is not at fault.
PROCEDURES: 1. General
a. Upon notification that any person has a reasonable suspicion that an employee or student of a Facility is violating, or has violated, this policy, the leadership of the Facility shall conduct an investigation. If, after an initial investigation, there appears to be some credibility to the suspicion, the Facility shall take whatever action necessary to protect patients, students, and employees, including, if the circumstances indicate that it is appropriate, immediately removing the employee or student from his or her work area and escorting him/her to a designated testing location, and conducting a search of the work area. The employee or student will be asked to sign a consent form prior to testing.
b. Any employee or student who is tested based upon a reasonable suspicion of a violation of this policy shall be immediately suspended pending results.
c. Any employee or student whose blood alcohol content exceeds the maximum set forth in this policy, or tests positive for non-prescribed Controlled Substances or illegal substances, will be immediately suspended. The Facility shall then seek legal review by the employment section of the Legal Department.
Core Manual July 2014 page 66
d. During a suspension for violation of this policy, the employee or student shall not be allowed access to the Facility with the exception for medical treatment.
e. The Facility will provide employees and students who test positive with contact information for substance
abuse resources. 2. Voluntary Self-Reporting
An employee or student who voluntarily self-reports substance abuse may, in the Facility’s sole discretion, be offered an opportunity to participate in a rehabilitation program. In such cases, the Facility may require, as a condition of continued employment, that the employee or student abide by the terms set forth by the Facility.
3. Organizational Reporting
In the event of a violation of this policy, the Facility will, if required by law, or if not required then if the Facility deems it appropriate, notify: (a) governmental agencies with jurisdiction over drug and alcohol issues (e.g., police, FDA, DEA); (b) if applicable, any professional licensing boards; and (c) appropriate Company executives (e.g., Division, HR, Legal, PR, Risk Management, HCI).
4. Confidentiality
All information received by the Facility through compliance with this policy is confidential. Access to this information is limited to those who have a legitimate need to know within the Company or those outside the Company in law enforcement.
5. Communication and Training
Communicating this policy is critical to the Company’s success. To ensure all employees or students are aware of their role in supporting this policy, each Facility shall prepare a plan for ensuring: a. The policy will be reviewed in orientation sessions for all employees and students. b. The policy will be reviewed annually by all employees and students. c. Leadership/designee will discuss the policy and organizational procedure during orientation of staff
managers. 6. Financial Reporting
a. Charges for employee drug screens, physician physicals, and fit for duty physicals should be reported under Account Title: Post Employment Drug Screens/Physicals #294.
b. Charges for potential employee drug screens, physician physicals, and fit for duty physicals should be reported under Account Title: Pre-employment Backgrounds/Drug Screens/Physicals #866.
7. Policy Monitoring
Monitoring of policy compliance will occur through Compliance Process Reviews by the Corporate Ethics and Compliance Department and Quality Review System Surveys by the Clinical Services Group.
REFERENCES: Records Management Policy, EC.014 Theft and Violence in the Workplace Policy, SS.001 Pre-Employment Health and Drug Screen Process Flow Charts
Core Manual July 2014 page 67
APPENDIX VII: ENDIX VI: Institutional Core Competency Plan
The institutions of the Palm Beach Consortium for Graduate Medical Education (PBCGME) consortium, including West Palm Hospital, Palms West Hospital, St. Lucie Medical Center, and University Hospital and Medical Center, are committed to providing educational, financial, and human resources necessary to support OGME and its development. This commitment indicates the dedication to quality in training by the institutions faculty as well as willingness to substantially comply with AOA training requirements to include all elements of a competency based experience and program, faculty and trainee outcome assessment. To this end, the faculty has developed this Institutional Core Competency Plan, which describes specific methodologies to teach and evaluate all trainees in the required competencies. It is expected traditional interns as well as all residents receive an adequate exposure to core competencies as an education goal. I. Core Competency Training Requirements The base institutions of PBCGME, seek to ensure that each graduate medical education program defines, teaches and evaluates, in accordance with AOA and specialty college requirements, the specific knowledge, skills, attitudes and experience required for trainees to learn and demonstrate the following basic core competencies:
a. Medical knowledge, c. Patient care, d. Interpersonal and communication skills, e. Professionalism, f. Practice-based learning and improvement, and g. Systems-based practice.
The competencies are integrated into all internship and residency programs through this Institutional Core Competency Plan, which has been drafted by the Regional DME and approved and supported by the Medical Education Committee. The Medical Education Committee will provide routine monitoring of the plan and, with the assistance of the DMEs and support staff, the internship and residency program directors will retain responsibility for implementation of the plan. This plan describes the methodology used for exposure and presentation to osteopathic trainees, as well as the processes utilized for assessment and evaluation of trainee proficiency. The plan will be updated annually with expansion of methods of teaching and evaluation. Program Director Annual Reports for each trainee will measure proficiency in each competency. The core competency requirements bear the same significance in the training of residents as specific clinical knowledge and skills and are necessary for successful program completion and ability to qualify for certification board examination. II. TEACHING TOOLS A. Medical knowledge Lectures are given twice daily, as part of our core didactic series. In addition, attendings are encouraged to give regular “spontaneous” lectures as part of their clinical rounds, as are residents. In addition, attendings give regular reading assignments to housestaff. Residents are required to develop skills as medical educators by giving presentations before peers and faculty, as well as participate in the instruction of medical students. Residents are routinely instructed in medical procedures. Housestaff sit for COMLEX Part III and In-Service Examinations. Our program provides for supervised observation of the clinical decision-making abilities of residents. We require attendance at seminars or CME, Grand Rounds, Lectures. Residents are required to participate in a directed readings program and journal club. Periodic assessment is made of resident critical thinking and problem-solving abilities.
Core Manual July 2014 page 68
Residents are required to participate in research activities that critically evaluate current medical information and scientific evidence; develop as a medical educator by having residents give presentations before peers, faculty, and participate in the instruction of medical students; routinely assess the skill and outcomes of residents in their performance of medical procedures; and develop programmatic education in Life Long Learning. Lectures, workshops and behavioral psycho-social multi-cultural issues are provided in medical specialties as appropriate. B. Patient Care Clinical rounds, including bedside teaching, are utilized on a daily basis. Residents are supervised in the performance of medical interviewing techniques to assess the resident’s skill and ability. Residents are provided instruction on the development and implementation of effective patient management plans. Residents are taught the proper methods for requesting and sequencing diagnostic tests and consultative services. Residents are instilled with the need to provide a caring attitude that is mindful of cultural sensitivities, patient apprehensions, and accuracy of information. Residents are provided instructional programs for the performance of medical procedures where appropriate. A credentialing program has been developed for residents to validate their competency in the performance of medical procedures where appropriate. Residents are instructed in the performance of a medical procedure, any potential complications and known risks to the patient (informed consent). Residents are taught to counsel patients and their families on health promotion and lifestyle activities related to good health maintenance; refer patients to non-for-profit and community service organizations that support health promotion and behavioral modification programs; and work with professionals from varied disciplines as a team to provide effective medical care to patients that address their diverse healthcare needs. C. Interpersonal and Communication Skills Development and refinement of interpersonal and communication skills pertaining to patients, colleagues and other staff members is integrated into all rotations, with Faculty members providing constant observations, guidance, recommendations and assessment. Residents are required to demonstrate patient interviewing techniques, including the ability to assess the health of non-English-speaking and deaf patients. Residents are taught to involve patients and families in decision-making, illustrate the use of appropriate verbal and non-verbal skills when communicating with patients, families and faculty, and to demonstrate an understanding of cultural and religious issues and sensitivities in the doctor-patient relationship. Residents are taught to communicate medical problems and patient options at appropriate levels of understanding; maintain comprehensive, timely, and legible medical records. Residents are also taught respectful interactions with health practitioners, patients, and families of patients; to elicit medical information in effective ways; and to demonstrate an understanding of resources available to physicians to assist with appropriate assessment of communication-impaired patients; as well as to work effectively with others as a member or leader of a healthcare team. D. Professionalism Residents are taught to present an honest representation of a patient’s medical status and the implications of informed consent to medical treatment plans; to maintain a patient’s confidentiality and demonstrate proper fulfillment of the physician’s role in the doctor-patient relationship; commitment to an appropriate and non-exploitive relationship with patients; to inform patients accurately of the risks associated with medical research projects, the potential consequences of treatment plans, and the realities of medical errors in medicine; to treat the terminally ill with compassion in the management of pain, palliative care, and preparation for death.; to participate in course/program (compliance and end of life).Workshops, lectures, bedside and clinic/office teaching, and to serve as a role model in behavior.

Core Manual July 2014 page 69
Residents are taught to understand conflicts of interest inherent in medicine and the appropriate responses to societal, community, and healthcare industry pressures; to use limited medical resources effectively and avoid the utilization of unnecessary tests and procedures; to recognize the inherent vulnerability and trust accorded by patients to physicians and uphold the highest moral principles that avoid exploitation for sexual, financial, or other private gain; to pursue life-long learning goals in clinical medicine, humanism, ethics, and gain insight into the understanding of patient concerns and the proper relationship with the medical industry; and to utilize workshops, lectures, bedside and clinic/office teaching. Residents are taught to become knowledgeable and responsive to the special needs and cultural origins of patients; to be an advocate for continuous quality of care for all patients; to prevent the discrimination of patients based on defined characteristics; and to understand the legal obligations of physicians in the care of patients. E. Practice-based Learning and Improvement Residents are taught to use reliable and current information in diagnosis and treatment; to understand how to use the medical library and electronically mediated resources to discover pertinent medical information; and to demonstrate the ability to extract and apply evidence from scientific studies to patient care. Feedback is provided, by faculty, on resident presentations. Residents attend Journal Clubs. Residents are taught to understand and participate in quality assurance activities at the hospital and at ambulatory sites; to apply the principles of evidence-based medicine in the diagnosis and treatment of patients; and to measure the effectiveness of resident practice patterns against results obtained with other population groups in terms of effectiveness and outcomes. Residents participate in research activities as required by the respective specialty colleges; demonstrate computer literacy, information retrieval skills, and an understanding of computer technology applied to patient care and hospital systems; and apply study designs and statistical methods to the appraisal of clinical studies. F. Systems-based practice Residents attend instruction in matters of health policy and structure, and are encouraged to understand business applications in a medical practice. Residents are expected to show operational knowledge of health care organizations, state and federal programs, and understand the role of the resident as member of the health care team in the hospital, ambulatory clinic, and community. Residents are taught to understand local medical resources available to patients for treatment and referral; participate in advocacy activities that enhance the quality of care provided to patients; and practice clinical decision-making in the context of cost, allocation of resources, and outcomes. Residents are encouraged to attend guest lectures/seminars with policy makers as well as to attend hospital utilization review, quality and other administrative and multi-disciplinary meetings. G. Osteopathic Philosophy Principles and Manipulative Treamtent Residents are expected to demonstrate and apply knowledge of accepted standards in OPP/OMT appropriate to their specialty. The educational goal is to train a skilled and competent osteopathic practitioner who remains dedicated to life-long learning and to practice habits in osteopathic philosophy and manipulative medicine. This competency is not evaluated separately but its teaching and evaluation in the training program occurs through the other competencies into which this competency has been fully integrated.
III. ASSESSMENT TOOLS A. CURRENT 1. Monthly Service Rotation Evaluation
Core Manual July 2014 page 70
(Medical knowledge, Patient care, Interpersonal and communication skills, Professionalism, Practice-based learning and improvement) An assessment tool used to provide a global rating of performance. The forms record categories of behaviors, not specific actions, based on rating scales. Attending physicians complete these evaluations at the end of every month. Completed forms are reviewed by the Director of Medical Education, Associate DME, Program Directors, Curriculum and Advancement Committees, and Medical Education Committee, on a quarterly basis. Evaluations are to be completed by the faculty member who directly supervised the resident and faculty members are to use their secure New Innovations login credentials. New Innovations website is new-innov.com and institution name is “HCAEFL”.
Use(s) Evaluates: • Global performance Familiarity Advantage(s) Quick and simple to complete Highly subjective • Rater biases Disadvantage(s) o Leniency o Halo effect Require direct observation of ratee • Second hand opinions reduce utility Rater training required
2. Procedure/Case Logs (Osteopathic philosophy and osteopathic manipulative medicine, Medical knowledge, Patient care) An assessment tool used to quantify patient encounters over a period of time. Interns and residents are required to maintain procedure and case logs, which are reviewed by the Director of Medical Education, Associate DME, Program Directors, Curriculum and Advancement Committees, and Medical Education Committee, on a quarterly basis.
Use(s) Evaluates: • Document training experience o Scope o Volume o Variety Advantage(s) Can direct training • Fill exposure gaps • Increase procedural opportunities Number of cases does not assure competence • Need to track patient outcomes Assurance of data accuracy • Quality assurance Disadvantage(s) Time consuming activity • Data entry
3. Portfolios (Osteopathic philosophy and osteopathic manipulative medicine, Medical knowledge, Patient care, Interpersonal and communication skills, Professionalism, Practice-based learning and improvement) An assessment tool used to document learning experiences. Usually a compilation of forms completed on New Innovations and/or submitted directly to the Medical Education office (i.e., case logs, procedural logs, research
Core Manual July 2014 page 71
activity, committee involvement, lectures and conferences attended, etc.). The Administrative DME and support staff maintain portfolios on each intern and resident. The entire portfolio is then reviewed by the Director of Medical Education, Associate DME, Program Directors, Curriculum and Advancement Committees, and Medical Education Committee, on a quarterly basis.
Use(s) Evaluates: • A record of learning accomplishments Advantage(s) Useful for self-reflection on learning Provide a global view of experiences Disadvantage(s) Time consuming to create Difficult to assign a score
4. Written Examination/Annual Specialty College In-Service Examination (Osteopathic philosophy and osteopathic manipulative medicine, Medical knowledge, Patient care, Interpersonal and communication skills, Professionalism) An assessment tool used to assess not only the examinee’s knowledge base, but also the ability to apply it to clinical situations. The most common written examination format uses multiple-choice questions. Currently utilized are the annual specialty college in-service examinations and Part III NBOME (all interns).
Use(s) Evaluates: • Knowledge base • Level of understanding Advantage(s) Familiarity Can cover many content areas quickly Can be graded quickly Can monitor progress over time • Use of anchor (repeated) questions Disadvantage(s) Require statistical analysis Passing scores should be predetermined Sampling error can occur • Use test blueprint
5. Objective Structured Clinical Examination (OSCE) (Implementation Date: 1/05) (Osteopathic philosophy and osteopathic manipulative medicine, Interpersonal and communication skills) An assessment tool that consists of multiple stations. The stations include various elements of clinical encounters. The stations include standardized patients (actors trained to portray illness in a standardized manner), actual patients, and/or components of clinical encounters (i.e., electrocardiograms for interpretation, radiographs for interpretation, etc.). Interns and Residents will attend quarterly Competency-Based learning sessions on OMM and Behavioral Medicine at West Palm Hospital. Annual OSCEs will be conducted on each second-year resident, by NSUCOM.
Use(s) Evaluates: • Communication skills • Interpersonal skills • Professionalism • Psychomotor abilities Advantage(s) Multiple assessments • Improves validity • Improves reliability
Core Manual July 2014 page 72
Useful feedback information • What the resident does well • What needs improvement Disadvantage(s) Expensive • 12 – 18 stations recommended • Selection/Creation of stations • Training of standardized patients (SPs) • Payment of SPs Difficult to design • Scoring criteria • Passing thresholds
6. 360-Degree Evaluation
(Osteopathic philosophy and osteopathic manipulative medicine, Medical knowledge, Patient care, Interpersonal and communication skills, Professionalism, Practice-based learning and improvement, and Systems-based practice) An assessment tool used to rate the performance of a resident. All individuals that have contact with the resident should complete the evaluation on New Innovations if they have the appropriate access or may submit a hardcopy to the office of Medical Education. The information obtained may reveal trends (i.e. patterns of behavior) with certain groups (i.e., nursing staff, adolescent patients, geriatric patients, midlevel practitioners, etc.) that may be useful when providing feedback to the resident.
Use(s) Evaluates: • Communication skills • Interpersonal skills • Professionalism • Teamwork ability Advantage(s) Multiple raters • Improves validity • Improves reliability Fosters self-reflection • Self-rating is a component Disadvantage(s) Peer pressure during process • Hesitation to be honest Difficult to design • Standard set of items for all raters • Group-specific subset of items Requires several raters • Not less than 20 attending physicians • Not less than 20 patients • At least two or more from other groups
B. FUTURE 1. Chart Stimulated Oral Recall Examination (Medical knowledge, Patient care, Interpersonal and communication skills) An assessment tool used to assess clinical problem-solving ability. Provides the ability to investigate the examinee’s rationale for requesting information (i.e., historical or physical examination data), interpretation of information provided, and management of selected cases, not evident by simply reviewing the chart.
Use(s) Evaluates: • Problem-solving ability Advantage(s) o Ability to use information o Ability to select the next step
Core Manual July 2014 page 73
Selected cases can be covered quickly Can ask a series of related questions Disadvantage(s) Examiners must be trained Scoring can be debated Cases selection can be difficult High anxiety level for some examinees
2. Checklist (Osteopathic philosophy and osteopathic manipulative medicine, Medical knowledge, Patient care, Interpersonal and communication skills, Professionalism, Practice-based learning and improvement, and Systems-based practice) An assessment tool used to evaluate specific behaviors or tasks that are components of a more complex activity. The checklist records whether the action was performed or not. If performed, the checklist can be designed to identify if the action was performed accurately, partially correct, or unsatisfactorily/wrong.
Use(s) Evaluates: • Actions that are objective o Specific o Measurable Examples: • Interviewing • Medical procedures Advantage(s) Useful information for feedback • What was not done • What was done o Correctly o Acceptably o Incorrectly Disadvantage(s) Difficult to design • What are the required actions • Requires expert opinion/consensus Evaluator variability • Raters need to be trained Only useful for fundamental skill assessment
IV. REMEDIATION PLAN Those who fail to meet performance expectations of the Institutional Core Competency Plan will be evaluated by the Regional DME, DMEs and/or Program Directors, who will make specific, individualized recommendation to the pertinent Curriculum and Advancement Committees and Medical Education Committee, for corrective action. V. ANNUAL SUMMARY The DMEs will compile annual written evaluation summaries of overall programmatic effectiveness, which will be reviewed by the Regional Director of Medical Education.