horticultural therapy: the healing garden and gardening in ... · pdf filepediatric...
TRANSCRIPT
PEDIATRIC REHABILITATION, 2004, VOL. 7, NO. 4, 245–260
Horticultural therapy: the ‘healing garden’and gardening in rehabilitation measuresat Danderyd Hospital RehabilitationClinic, Sweden
INGRID SODERBACK, MARIANNE SODERSTROMand ELISABETH SCHALANDER
Accepted for publication: 15 January 2004
Keywords Garden, gardening, healing, neurological diseases,occupational therapy
Summary
Objectives: Objectives were to review the literature onhorticultural therapy and describe the Danderyd HospitalHorticultural Therapy Garden and its associated horticulturaltherapy programme.Design: The literature review is based on the search words
‘gardening’, ‘healing garden’ and ‘horticultural therapy’. Thedescription is based on the second author’s personal knowl-edge and popular-scientific articles initiated by her. Thematerial has been integrated with acknowledged occupationaltherapy literature.Setting: The setting was the Danderyd Hospital
Rehabilitation Clinic, Sweden, Horticultural Therapy Garden.Participants: Forty-six patients with brain damage partici-
pated in group horticultural therapy.Results: Horticulture therapy included the following forms:
imagining nature, viewing nature, visiting a hospital healinggarden and, most important, actual gardening. It was expectedto influence healing, alleviate stress, increase well-being andpromote participation in social life and re-employment for
people with mental or physical illness. The HorticulturalTherapy Garden was described regarding the design of theoutdoor environment, adaptations of garden tools, cultivationmethods and plant material. This therapy programme formediating mental healing, recreation, social interaction,sensory stimulation, cognitive re-organization and trainingof sensory motor function is outlined and pre-vocational skillsand the teaching of ergonomical body positions are assessed.Conclusion: This study gives a broad historic survey and
a systematic description of horticultural therapy with empha-sis on its use in rehabilitation following brain damage.Horticulture therapy mediates emotional, cognitive and/orsensory motor functional improvement, increased social parti-cipation, health, well-being and life satisfaction. However, theeffectiveness, especially of the interacting and acting forms,needs investigation.
Introduction
The value of horticulture therapy is witnessed by thefact that, for their very survival, humans have soughtaspects of nature such as open views, closeness to waterand a place of refuge over the past 40 000 years at least.Horticultural therapy includes interventions mediatedby nature-oriented views and spaces such as gardensand everything associated with them, the plantsand material related to them, garden tools and gardenoccupations performed among disabled people [1–3]for healing and for restoring or improving health andwell-being or for rehabilitation or simply for generalbenefit.
The benefits of using horticulture therapy are that(a) patients may be able to continue the occupationsat home using adaptations learned during therapy ses-sions at a hospital; and (b) such therapeutic sessions are
Pediatric Rehabilitation ISSN 1363–8491 print/ISSN 1464–5270 online # 2004 Taylor & Francis Ltdhttp://www.tandf.co.uk/journals
DOI: 10.1080/13638490410001711416
Authors: Ingrid Soderback (author for correspondence;e-mail: [email protected]), Dr Med Sci,Occupational Therapist/Licensed, University Lecturer,Responsible Scientific Leader, Department of Public Healthand Caring Science, Uppsala University, Sweden; MarianneSoderstrom, Head occupational therapist, Project Leader,Rehabilitation Clinic, Danderyd Hospital, 182 88 Danderyd,Sweden (died February 2004); Elisabeth Schalander,Occupational Therapist/Licensed, Specialist in Horticulturetherapy, Rehabilitation Clinic, Danderyd Hospital andAcademeia Garden: Inspiration and Design, Akersberga,Sweden.
Dev
Neu
rore
habi
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Ank
ara
Uni
v. o
n 10
/30/
12Fo
r pe
rson
al u
se o
nly.
easy to vary and adapt to individual’s ability to performthe activities.A hospital healing garden or therapeutic garden is
a nature-oriented space, indoors or outdoors, with atherapeutic or rehabilitative potential [4]. It is a placeof sanctuary where the basic urge for contact withnature can be met [5]. A healing garden seeks to providemaximum influence on health. It should be designedwith a plentiful variety of plant materials that flowerin different seasons, attract birds and butterflies, withleaves or grass that move with a light breeze, pools thatreflect the sky and provide a home for fish. Sculpturesand other designs should be unambiguously positive.The design should facilitate visibility (the garden shouldinvite one to visit it), security and physical comfort. Thegarden should be open to all and give a sense offamiliarity. It should be calm and quiet so that its voices(water-splash, birdsong) can be heard [6]. Optimallydesigned, the gardens facilitate non-discrimination ofthe participants’ age, genus, class, previous occupation,cultural heritage or ethnicity. In addition, at its best,the gardening facilitates social interaction in termsof previous experience of gardens and gardening or ofdisablement. This may provide a common subject fordiscussion and may help participants to find newfriends.A further justification for healing gardens is that the
quality of a hospital’s physical environment affectspatients’ medical outcomes and care quality [7]. In theUSA, for example, paediatric and long-stay hospitalsare expected to have access to grounds, parks andplaygrounds and adjacent countryside [6, 8].A healing hospital garden involves patients, friends,
relatives and staff participating in, for example,planning plant-beds, sowing, tending and watering theplants, harvesting, communicating, etc.The literature shows that therapeutic gardening has
been used for (a) changing mood positively [e.g., 6, 9],(b) influencing health and well-being by viewing photo-graphs, slides, videos of outdoor nature and gardenscenes [e.g., 10, 11] and (c) reaching solace or relief byenvisaging natural scenes of grass, trees, water, sky,rocks, flowers, and so on [7, 12, 13].The general objective of this study was to examine
the rarely-documented descriptions of how gardeningmediates health, well-being and function among peoplesuffering from neurological [14–17] or musculoskeletaldiseases.More specific aims were (a) to briefly review historic
aspects of horticultural therapy and its use amongdisabled people for care or rehabilitation and (b) todescribe hospital therapeutic (healing) garden design
and to summarize experience of its use and of gardening
among patients with neurological and/or musculoskele-
tal diseases from 1983 to the present, with emphasis
on horticultural therapy at Danderyd Hospital
Rehabilitation Clinic.
Method
For the review part of this study, literature searches
were performed in the Allied and Complimentary
Medicine (AMED) [18] database, the Cumulative
Index to Nursing & Allied Health Literature�
(CINHAL) [19] database, in MEDLINE [20] and
among Internet information from the American
Horticulture Therapy Association [21] and the ‘Lucas’
library of the Swedish Agricultural University, Alnarp
[22]. The search words ‘gardening’, ‘healing garden’ and
‘horticulture therapy’ were used. The CINAHL search
resulted in 87 hits for ‘gardening’. These hits were
restarted by the search words ‘gardening or horticul-
ture’, resulting in 21 hits. A primary selection suiting
the present study subject from the two searches gave 39
articles. The MEDLINE search added one relevant hit,
while the AMED search gave 324 hits for ‘gardening’.
The searches were then restricted to publications after
1990, giving an additional 20 Hits. Only five more pub-
lications were found, most information overlapping
with the CINAHL database. The search in the
American Horticulture Therapy Association gave 52
hits, of which 15 were judged to suit the present subject.
Four hits were added from the ‘Lucas’ search. The arti-
cles finally used are marked in the reference list with an
*. The references from selected literature judged as most
important were further scrutinized, forming a selection
of the most cited literature and authors.
The description of the Danderyd Hospital Rehabili-
tation Clinic horticultural therapy measures is based
mainly on the second author’s (MS) clinical experience
as initiator of horticultural therapy in rehabilitation in
Sweden. Her oral information was supplemented
by popular-scientific publications in Swedish [23–28],
originating from her instructs, plus candidate’s theses
[e.g., 29] and master’s theses [e.g., 30] published between
1989–2000. A short version of the present report was
presented during the Brain Injury Conference in
Stockholm, Sweden, in May 2003 and an abstract was
published [31].
Retrospective data from the medical records of the
Danderyd Hospital Rehabilitation Clinic were used to
describe the horticultural therapy gardening groups.
I. Soderback et al.
246
Dev
Neu
rore
habi
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Ank
ara
Uni
v. o
n 10
/30/
12Fo
r pe
rson
al u
se o
nly.

Results
literature review
The origins of the healing garden and gardening
The use of the natural environment has variedthrough the centuries and reflected each culture’s beliefsand values. Nature, the green landscape, sunlight andfresh air were from the latter 17th century until themiddle of the 20th century an essential component ofthe healing process in various hospital settings, such assanatorium parks [6, 32, 33].
Mental-hospital aspects of the healinggarden and gardening
Starting with the idea that visiting nature and gardensfor sitting, working and talking about the worldbeneficially influences people’s health, gardening wasa prescribed intervention in mental hospitals from theearly 20th century [24, 33]. The notion originated fromthe Moral Treatment Movement [34]. Patients withmental illness were scheduled to perform occupationssuch as sewing, weaving and woodwork. Being occupiedwas supposed to promote patients’ establishment ofconcepts of time, work and cultural value. Moreover,such occupation was expected to control inactivity andanxiety [34]. The American psychiatrist and neurobiol-ogist Adolf Mayer stated that ‘man learns to organizetime and he does it in terms of doing things’ [34, 35].Performance of these occupations resulted in mentalhospitals becoming self-sufficient communities.As the concept of humanism permeated to German
psychiatric care in the 1920s, this idea of supplyingpatients with occupation spread over the industrialworld. On the premises of mental hospitals, largeparks and vegetable and flower gardens were createdand maintained by the patients, gardening beingperformed by the patients with a disturbed sense oftime and reality. The patients did necessary daily gardenwork such as digging, sowing, weeding, harvesting, etc.There existed the empirical experience that gardenwork helped patients to feel the rhythm of each dayand understand how the garden and gardening shiftedduring the seasons. This idea was adopted in Swedishmental hospitals during the 1940s [32].The notion that the mentally-ill could become organ-
ized by doing gardening was more or less abandonedbetween 1960–1980. A closeness to nature was lostand participation in the natural cycle and absolutehuman dependence on nature was obscured. Further,as psychopharmacology entered mental hospitals,
therapeutic effects on patients were achieved withoutoutdoor activities. Patient labour was no longer con-sidered necessary or desirable. Food was prepared inlarge central kitchens, so that patients no longer parti-cipated in the handling of natural raw ingredients fromthe garden. Finally, the institutional mental hospitalsettings were dismantled. The beautiful hospital parksand gardens became mostly a memory, although someparks still exist to provide recreation [32].
However, the idea that environmental design affectsmedical outcomes has been regaining popularity, sincethe 1960s [7, 36].
Rehabilitative aspects of the healinggarden and gardening
In the 1950s, after the two World Wars, the returnhome of mentally and physically wounded soldiersincreased the demand for rehabilitation. A more activeform of medical rehabilitation started to evolve.Rehabilitative centres began to use elements of natureas therapy in physical, occupational and speech pro-grammes [32]. The therapeutic value of gardening andits place in a rehabilitation plan were described in 1957[37, ibid. 38].
In England in the mid-1960s, hospital gardens werecreated for teaching purposes and were used by organi-zations for advisory services, and for demonstratingthe adaptation of gardening tools [39] and how agood garden design should be accessible to peoplewith disabilities [40]. Interestingly, these services cannowadays be incorporated in an interactive multimedialearning environment, e.g. using the ‘Greenhat DesignGuidelines’ which seek to mediate social interaction andemployment-related skills [41].
The hospital gardens in Oxford and Northwood,Middlesex, were designed for research into the feasibil-ity of using gardening for rehabilitation for ambulant,but crutch-dependent, patients or wheelchair users [40].
The therapeutic garden at Mary Marlborough Lodge,England was used by 5–12 year-old disabled childrenwho were wheelchair users or born with congenitalupper-limb malformations. The garden was initiallyintended for relaxation therapy, but soon became avery suitable hobby area for these children and usedfor training in the use of their prostheses [42].
In the 1970s, in England, the view that gardeningmediates rehabilitative intervention was expandedfor use among patients with rheumatoid arthritis forexample or following hand surgery. Particularly forpatients with hemiplegia, garden tools were adaptedfor use with one hand [17]. Gardening was expanded
Horticultural therapy
247
Dev
Neu
rore
habi
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Ank
ara
Uni
v. o
n 10
/30/
12Fo
r pe
rson
al u
se o
nly.

to indoor activities and a choice of suitable plants wasdescribed [43]. During the 1971 Chelsea Flower Show,the garden accessible for handicapped people was aprominent theme [32]. In 1973, in the USA, horticulturewas an accepted part of rehabilitation through theNational Council for Therapy and Rehabilitation [38].Studies during the 1970s seem mainly to describe the
garden design to facilitate patients’ increasing participa-tion in gardening and maintenance of interest inthe activity. However, gardening was now not only apracticable occupation, but also related to therapy. Thetherapeutic use of gardening was expanded to embracean activity in which patients could engage [44] and aform of relaxation therapy. Kaplan [ibid. 38, 45], in1972, made a scientific psychological analysis of thebenefits of participating in gardening. The experienceof plants growing gave the participant satisfaction andmaintained interest in gardening. The analysis wasbased on the statement that ‘humans need a comfort-able and stimulating environment to visit’ [38, 45].Moreover, gardening was adopted in nursing homesfor geriatric patients with decrepitude. In 1979, oneof the first more regular scientific evaluations ofhorticultural therapy was conducted. This was adirect-observation (n¼ 29 experimental group), experi-mental evaluation study of non-engagement or engage-ment in indoor gardening among 32 physically impairedresidents of a nursing home, with a mean age of 81years. The study outcomes were engagement accountedfor in terms of performing daily living activities or usingrecreational material or getting around or interactingwith other residents. Those residents who participatedin weekly gardening sessions were engaged more than90% of the observed time, while non-participating resi-dents were engaged less than 40% of the observedtime. It might be concluded that doing gardeningoverflowed into social and occupational engagementin daily activities among older residents [44].In the 1980s, the value of gardening as therapy was
expanded to include programmes for re-employmentamong people with disabilities. Relf [ibid. 38, 46, 47]emphasized ‘the potential benefits in self-concept, socialinteraction, work habits, academic-skill development,and physical abilities among handicapped individuals’who participated in a horticultural pre- or vocationaltraining programme. In the same spirit, the purposesof gardening were discussed for use in occupationaltherapy. Here, gardening was advocated as a toolfor observing and assessing the patients’ employmentabilities. The people were asked to do garden tasksthat required physical activity such as climbing steps,slopes, walking or otherwise transporting themselves
on various surfaces, bending, lifting and carrying andhandling garden material. The therapeutic approach tousing gardening was also suggested for functionalmotor improvement of limbs. Finally, gardeningwas a rehabilitation-supported activity for patientswith disabilities seeking new recreational hobbies afterdischarge or a way of enabling them to achieve greaterself sufficiency [48]. The first Swedish healing gardenwas created at Danderyd Hospital RehabilitationClinic.
The term horticultural therapy became common inthe health sciences during the 1980s and all forms ofactivity connected with nature, e.g. viewing photoswith natural scenes [12] or visiting (healing) gardens,were included in the therapy sessions. The philosophywas based on the evolutionary belief that human sur-vival and ability to thrive and gain fulfilment dependupon one’s relationship with nature. This—the biophiliaframework—created by the biologist E. O. Wilson [49]mentions ‘the innately emotional affiliation of humanbeings to other living organisms’ [ibid. 50]. Severalscientists have adopted the biophilia theory for demon-strating human [51] interaction with the environment.
As one example, physiological reactions to thecreative and less creative environment were studied for6months among elderly people in a service home. Theexperimental group studied gardening during the winterand practiced it during summer. Coping and signs ofself-esteem improved significantly among the experi-mental group [10, 11].
Another example was people suffering fromAlzheimer’s disease who had access to a healing gardendesigned according to the Environment-Behaviourcriteria, that is to give a sense of nature, weatherand plants, reducing fear and promoting security. Theresidents enjoyed being outdoors and a relaxing effect onhealth and wellbeing was observed in terms of decreasedanxiety and aggression [9]. The outcome of horticultureas a recreation appeared to have beneficial effects onwellbeing [12, 52].
The use of horticultural therapy for children withvarious impairments was extensively described in the1980s. The therapy was used in a transitional employ-ment programme for adolescents with developmentaldisabilities [1] or for children with exceptional [53],cerebral-palsy [54] or behavioural disorders [55]. Atherapeutic gardening programme for children hospital-ized with behavioural disorder emphasized both adiscussion group and an active performing group.Obese children did gardening (cultivating, planting,maintenance and harvesting) for 30–45minutes perday during a summer with the aim of increasing their
I. Soderback et al.
248
Dev
Neu
rore
habi
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Ank
ara
Uni
v. o
n 10
/30/
12Fo
r pe
rson
al u
se o
nly.

physical activity [56]. The pre-school children’s involve-
ment in plant-stimulated discovery activities [57, 58]
was considered. Williams and Mattson [59] showed,
during a 5-month study, that children participating in
a professionally supervised gardening programme
increased their self-esteem and horticultural knowledge
and that the garden looked better than that tended by
unsupervised participants.
In the 1990s, the trend was [60, 61] to bring nature
back into urban environments. Landscape architects
promoted the building of parks and public gardens,
lined streets with trees and created indoor environments
using plants, flowers and water effects [62]. Aesthetic
hospital environments were promoted [63]. The
purposes were to facilitate life in a healthy and recrea-
tional environment, helping people to recover from
unhealthy stress [64]. Thus, the research focused on
the interaction between the natural environment and
human health [5, 36]. The meaning that green
areas and urban parks connected to institutions and
playgrounds has for children and adults was observed.
People with access to this kind of facility spent more
time outdoors, increased their concentration and slept
better than these without this possibility [65, 66].
Theoretical explanations of why people in a nature
environment experience relief of stress release and
healing were further developed, enriched, debated and
tested during the 1990s. Relf [67] states that the positive
emotional effect of participation in nature or a nature-
related environment was explained by several underpin-
ning theories, as follows:
(a) Kaplan’s [68] ‘evolutionary theory’ states that:
‘visual patterns of the natural environment are
easiest to interpret because a human uses his
involuntary attention’. This form of attention is
preferable and may release negative stress. This
assumption is explained by the brain’s pre-
programmed preparedness to sort out different
stimuli in a natural environment, where man
was originally meant to live. The opposite is
directed attention, which occurs when humans
are bombarded by information from the urban,
artificial, environment which has to be sorted
out. This attention requires much energy leading
to overloading and negative stress, i.e. easy dis-
traction, difficulties in planning and implementing
and to feelings of impatience and irritability [33].
Kaplans’ theory shows that natural environments
have a positive influence on the participants’
ability to concentrate.
(b) Ulrich et al.’s [13] ‘psycho-evolutionary theory’states that: ‘humans have long adapted positivelyto nature for survival and therefore react withpositive emotional physiological responses when
in natural or nature-related environments whichinfluence intellect, meaning and behaviour’(present author’s translation). This theory has
been proved acceptable through several studies[12, 13, 52, 69, 70].
(c) According to Relf’s [67] ‘cultural learning theory’,
‘a human adapts to the natural environment wherehe or she developed, and which led to a preferencefor familiar trees and flowers’. This statement con-tributed to the formulation of the theory of ‘the
living environment’ [65]. This theory prompted thesuggestion that environments should be created tofacilitate memories of competence and experience
among people with dementia. Noteworthy is thestudy by Ottosson [16]. He himself suffered frombrain damage which caused aphasia (inability to
read and write), spatial dysgnosia (difficulties inorientation in the near environment) and lack ofcontrol over life. Using an introspective self-studymethod he investigated the importance of visiting
nature, which influenced all his senses, gave himfeelings of well-being and helped him to overcomehis life-crisis.
Originating with Smith [71], the idea of usinghorticultural therapy as a stress management pro-
gramme for emotional relief was transferred to rehabili-tation programmes in Sweden for people suffering fromburnout [72].
The restorative value of participation in nature was
examined with the keywords; (a) being away—from an
urban stressful environment to spend time in natural
surroundings, (b) extent—the environment absorbs
humans mentally and physically and, therefore, the
environment visited should include some new things
to explore and discover, (c) fascinating—the environ-
ment should include stimuli that fascinate the visitor
and encourage attention and concentration, and
(d) compatibility—the environment meets the
individual’s goal [33, 67, 73].
Research also emphasized the design of a healing
garden [74–76] and the concept of horticulture therapy
was scientifically evaluated according to theory. It has
been recommended that the physical design of a healing
garden should be according to the ‘theory of supportive
health care design’ [69]. This theory stresses the environ-
mental characteristics that support or facilitate coping
and restoration following illness and hospitalization.
Horticultural therapy
249
Dev
Neu
rore
habi
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Ank
ara
Uni
v. o
n 10
/30/
12Fo
r pe
rson
al u
se o
nly.
A supportive health care physical environment should
facilitate privacy, promote social support and natural
distractions, give opportunities for physical movement
and provide involvement with nature. Patients’ out-
come in terms of health and wellbeing has been proved
to be positively influenced if they can see or have access
to natural surroundings (trees, flowers and water) or
regularly spend time in healing hospital therapeutic
gardens [65, 69]. Further research results show a very
high likelihood of reduced stress and anxiety, improve-
ment of patient satisfaction, a high likelihood of
sleep improvement and a moderate likelihood of pain
reduction and infection occurrence [6, 7, 11, 70]. The
emotional healing effect of horticultural therapy was
further investigated by Barnes [64]. Even a low degree
of ‘passive’ participation in the nature environment may
influence emotional restoration [64].
Moreover, horticultural therapy is world-wide [77]
in varying health care and hospital settings, for
example acute care [4] and hospice care [78], and is
being extensively studied among adults with visual dis-
abilities [79], elderly people with diagnosed dementia
[80, 81] and people with autism [82] or sensory
deficits [83].
From 2000 until the present (2004), the same trends
in horticultural therapy continue. How hospital healing
(therapeutic) gardens should be designed has been
further investigated [7, 70]. Whether or not participants
are disabled (e.g. frail elderly people [84] or AIDS suf-
ferers [85]), their perception of experience [86] and
meaning [51, 87, 88] in terms of health benefits [89,
90], wellbeing [91], reduced stress [92, 93] or improved
quality of life [94] are described. Studies of horticultural
therapy for people with neurological diseases are still
rare [14–16]. However, Sarno and Chambers [15] have
outlined a horticultural therapy programme for individ-
uals with aphasia.
In Sweden, in day nursery homes and primary
schools, children with physical disabilities (walking
with sticks, wheelchair users, the visually impaired)
or mental retardation are integrated with ‘normal’
children. This raises issues of legitimate claims upon
accessible playgrounds and school yards [95]. An out-
door pathway in a wood passing through a whale, a
pergola and a dinosaur bridge have been laid out
in connection with Bracke Ostergard, a children’s
hospital in Goteborg, Sweden. Here the children
can drive their PermobileTM (electric wheelchairs)
themselves because a light-beam sensor under the
wheelchair corresponds to a reflector at the edge of
the pathway [96].
the healing hospital garden and the use of
horticultural therapy at danderyd hospital
rehabilitation clinic
Background
Organized by the occupational therapy department ofthe Rehabilitation Clinic, Danderyd Hospital, the firstSwedish Horticulture Therapeutic Garden (DHHTG)was opened in 1986. The DHHTG was designedfor patients with physical disabilities, mainly followingcognitive and/or musculoskeletal impairments. Thisgarden and its associated activities constituted a supple-mentary activity among others of daily life and handi-craft which mediated the patients’ rehabilitation.
Purposes of the DHHTG
The purposes of the DHHTG concept were(a) therapeutic; as a meeting point for relaxation, reliefand rehabilitation and (b) for training team membersin horticultural therapy.
Several requirements for use of the garden were:
. accessible for visiting and gardening apart fromdisability,
. adaptation of garden tools for use among patients,
. visitors offered a non-demanding, calm and silentnatural environment,
. gardening as a leisure activity preserved orencouraged as a new leisure interest with the inten-tion of being continued after discharge,
. gardening mediating occupational therapy, and
. as a centre for education in concept of healingtherapeutic garden [25, 28, 97] for, among others,patients and rehabilitation teams in Sweden.
Design of the DHHTG
Landscape architect Gustav Alm designed theDHHTG as a result of close team work with therelevant staff of the Danderyd Hospital RehabilitationClinic. The DHHTG has been improved over the yearsin step with increased experience of horticulturaltherapy. The DHHTG is situated in a north–southorientation between two blocks of Danderyd Hospital.It measures 20� 30metres (figure 1).
The garden has extensive access to sunlight and issheltered from severe winds. The ground is accessiblefor wheelchair users and for people using walking aids,according to the principles that (a) all differences inlevels are avoided or clearly marked and with guide-rails, (b) the walkways are paved with concrete slabs
I. Soderback et al.
250
Dev
Neu
rore
habi
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Ank
ara
Uni
v. o
n 10
/30/
12Fo
r pe
rson
al u
se o
nly.
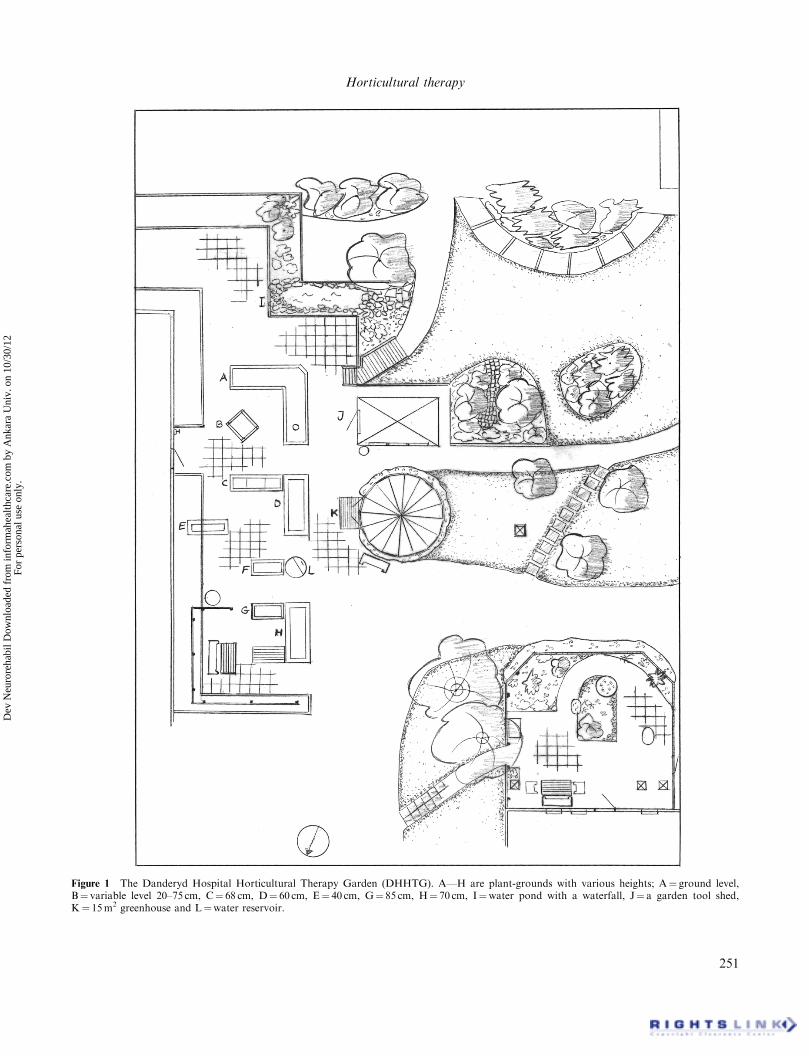
Figure 1 The Danderyd Hospital Horticultural Therapy Garden (DHHTG). A—H are plant-grounds with various heights; A¼ ground level,B¼ variable level 20–75 cm, C¼ 68 cm, D¼ 60 cm, E¼ 40 cm, G¼ 85 cm, H¼ 70 cm, I¼water pond with a waterfall, J¼ a garden tool shed,K¼ 15m2 greenhouse and L¼water reservoir.
Horticultural therapy
251
Dev
Neu
rore
habi
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Ank
ara
Uni
v. o
n 10
/30/
12Fo
r pe
rson
al u
se o
nly.

and are slightly inclined to avoid slippery surfaces,(c) there is enough space between the plant beds toallow two wheelchairs to meet easily.In one corner of the garden is a long, 108-square-foot
tool-shed with a sedum covered roof and two compostbins. The tool-sheds are well stocked with gardeningtools and other material. The placing of each tool ismarked with symbols, for easy finding and replacement,and at a height reachable by all users. The hooks forhanging the tools on are designed for ease of handling.Another part of the garden is screened off by a
robust, 2metre-high, 6metre long trellis, serving as anaid to standing. A 160-square-foot round greenhouseallows cultivation experiments protected from theNordic climate. A pond and a waterfall heighten thenatural impression. Nearby garden furniture invitesone to relax, calm down and be sociable. A bouletrack encourages activity.The bedding areas and flowerbeds have five different
working heights allowing various working positions(e.g. standing up, bending or sitting). The highest bed-ding areas are tables, which a wheelchair user can drivebeneath and round. A wooden bench for sitting andresting and for putting material down on surroundsthe larger bedding areas. There is an electric point onthe shed wall. Watering is performed from a tap on theshed or from a covered water tank with a tap [28].
Design of gardening tools for the DHHTG
Ergonomically [98], the DHHTG seeks (a) to use themost ergonomical garden tools for the various elements:digging, cultivating, sowing, planting, watering, raking,loosening or breaking up weeds, trimming or cutting,cutting faded or fresh flowers and vegetables, mowinggrass, moving garden material, tools and oneself about,covering new plants [25] and (b) the most appropriateergonomical body positions.Most DHHTG garden tools (the plant/beds out, try or
tables, mini-garden-house-boxes; watering cans, varioustypes of spade, rake, pitchfork, pruning shears, wheel-barrow, carts or baskets and/or aprons with big pocketsfor tools and material and for protection gloves) wereavailable on the market. However, the selections werebased on principles of occupational-therapy ergonomics[98] and adapted for use among patients with neuromus-culoskeletal and movement-related impairments.The ergonomics included the principles that [24, 28]:
(a) all tools were as light as possible (figure 2a),(b) tools with separate handles are used to facilitate
the adaptation of exchangeable handles. This
allows adaptation to the individual patient’s needfor purposeful training (figure 2b),
(c) the tool allows optimal biomechanical body posi-tions (e.g. suitable handle lengths for sitting orstanding working positions) (figure 2c),
(d) the design permits the lowest possible workload(e.g. less muscle strength is required when bothhands and one foot are used for making holes inhard earth and with a curved rake handle) (figure2d),
(e) the tools useable with a two-hand-grip by peoplewith a weak or paretic arm and hand (figure 2e),
(f) the angle between the tool head, e.g. spade andhandle allows optimal work functions—a neutralbody position in the forearm when gripping (figure2f), and
(g) wooden tool-handles designed to suit various gripfunctions and functional use and in neutral handpositions (figure 2g).
Cultivating in the DHHTG
Different methods and materials are used forcultivating, where possible at different heights andreachable from some distance. Examples are (a) theuse of raised cultivation beds, (b) movable mini-hot-houses and hot-beds, (c) square-foot cultivation inframes or (d) cultivation directly in a sack at groundlevel near the trellis, (e) in a box, (f) in pots arrangedin a rotation system or (g) in a hanging pipe orbasket [28].
Seeds for the DHHTG
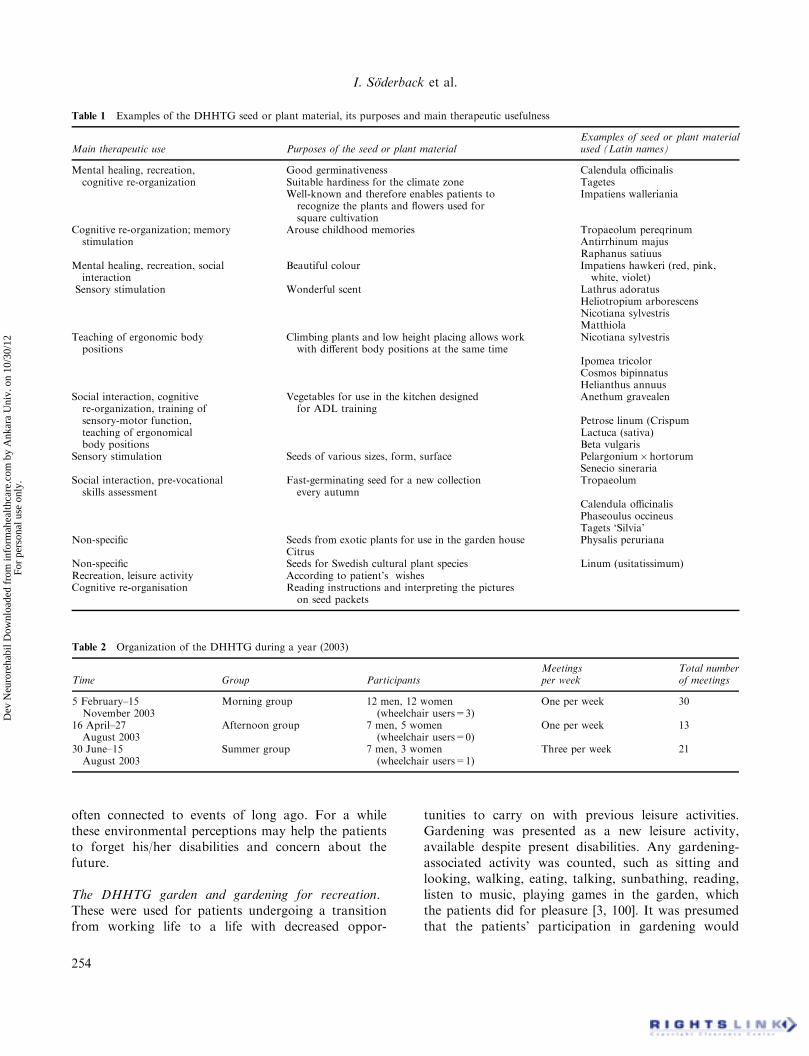
Seeds and plants were chosen to reflect the varioustherapeutic approaches described in table 1.
Participants in and organization of DHHTG gardening
Participants. The patients, aged 18–65 years, takingpart in the Danderyd hospital horticultural therapyrehabilitation suffered from pain- or movement-relatedimpairments (hemiparesis or paraplegia) and/or cogni-tive (speaking, reading spatial orientation, memorydysfunction, attention, concentration and logicalreasoning difficulties) and/or were depressed. Disabil-ities ranged from major to minor insufficiency. Thus,some patients were wheelchair users, but others had amajor memory disability with no movement-relateddisability. Patients’ families and friends and staff werealso welcome to participate.
I. Soderback et al.
252
Dev
Neu
rore
habi
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Ank
ara
Uni
v. o
n 10
/30/
12Fo
r pe
rson
al u
se o
nly.

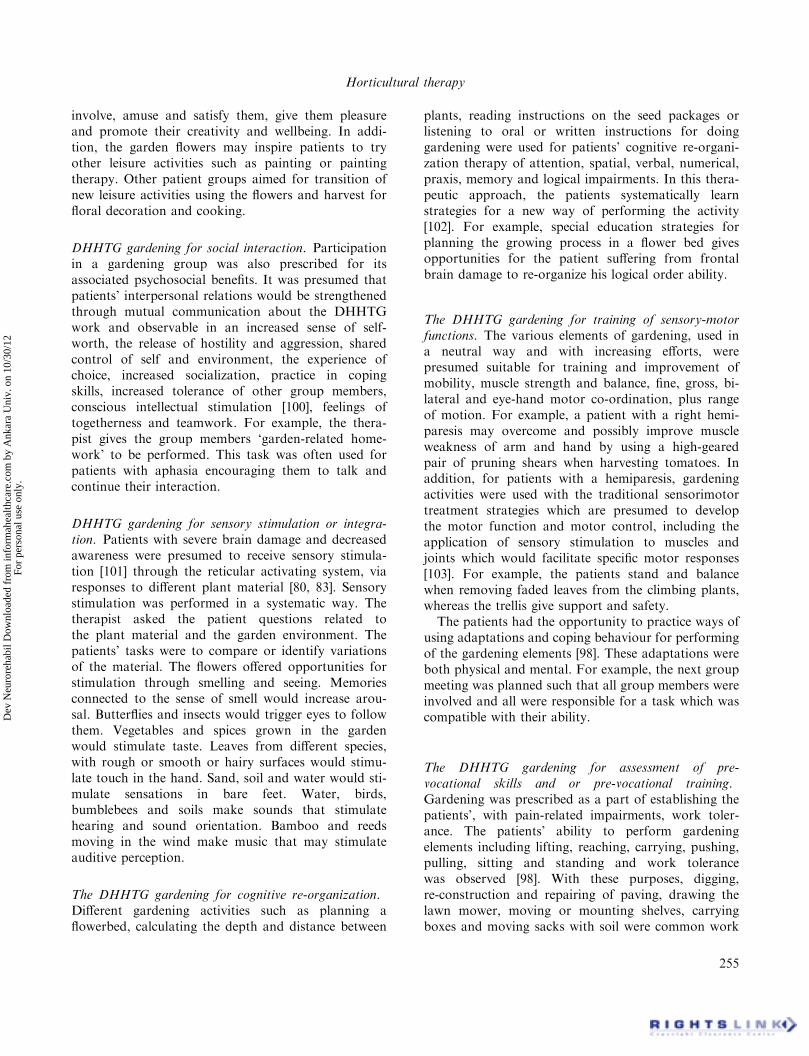
Organization. The patients gardened as one of severalself-chosen activities during the sessions. These wereorganized in groups whose composition changed atintervals during the term. The organization andparticipants are shown in table 2. From February tomid-November 2003, 72 patients (23men) sufferingfrom brain damage (e.g. stroke, haemorrhage, braintrauma), aged 18–65 years, participated in one ofthree gardening groups. Each patient participated as agroup member, but was prescribed individual garden-ing work: his or her ‘therapeutic tonic’. Thisindividual work was intended to be done at othertimes than the group meetings.
All the gardening tasks were performed in a neutral
way. They were graded from easiest to most difficult.
For example, the patient was asked to plan a flowerbed
with only one plant species. The degree of difficulty of
this activity increased when the same flowerbed was to
be planned for year-round flowering with spring tulips,
early summer herbs, summer flowers and finally autumn
flowers for drying.
Therapeutic use of the DHHTG. As indicated above,the DHHTG gardening concept was used as a tonic.The therapeutic purposes were individualised to oneor a combination of (a) mental healing, (b) recreation,(c) social interaction, (d) sensory stimulation, (e)cognitive re-organization, (f) sensorymotor function,(g) assessment of pre-vocational skills and (h) teachingof ergonomical body positions.
The DHHTG as a place for mental healing. It was pre-sumed that time regularly spent in the DHHTG maypositively influence visitors’ minds and may cure oralleviate physical illness [99], especially among thosewith severe brain damage. The DHHTG was afavourable place frequently visited for resting, medita-tion and relaxing relief; or for meeting family andfriends in a non-hospital environment. There are manyfragrances in a garden regardless of season, affordingtopics for conversation and prompting memories.Grass and dew, flowers and berries, these things are
Figure 2 a. Lightweight garden tools are required, e.g. from the left: Lightweight (3.8 kg) wheelbarrow in cloth, with raised handles for optimalergonomic standing or walking position; Medium-weight (about 9 kg) ‘easy wheelbarrow’ can be pushed or pulled with one hand (in hemiparesis);Standard weight (about 12 kg) wheelbarrow shown for comparison. b. Garden tools with detachable handles allow individual adaptation. c. Suitabletool lengths facilitate optimal biomechanical body positions such as standing and sitting. Marks for easy lengthening or shortening of telescopichandle. d. Garden tools should facilitate as low a work load as possible. For example digging is facilitated when both hands and one foot. e. Gardentools adapted for use with a two-hand-grip. Slings can be added to afford a useful grip for weak arm and hand muscles. f. Garden tools for work in aneutral body position are recommended, for example gripping the handle of this cultivator. g. The handles of these garden tools are enlarged withsoft plastic, decreasing the grip muscle strength required.
Horticultural therapy
253
Dev
Neu
rore
habi
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Ank
ara
Uni
v. o
n 10
/30/
12Fo
r pe
rson
al u
se o
nly.
often connected to events of long ago. For a whilethese environmental perceptions may help the patientsto forget his/her disabilities and concern about thefuture.
The DHHTG garden and gardening for recreation.These were used for patients undergoing a transitionfrom working life to a life with decreased oppor-
tunities to carry on with previous leisure activities.Gardening was presented as a new leisure activity,available despite present disabilities. Any gardening-associated activity was counted, such as sitting andlooking, walking, eating, talking, sunbathing, reading,listen to music, playing games in the garden, whichthe patients did for pleasure [3, 100]. It was presumedthat the patients’ participation in gardening would
Table 2 Organization of the DHHTG during a year (2003)
Time Group ParticipantsMeetingsper week
Total numberof meetings
5 February–15November 2003
Morning group 12 men, 12 women(wheelchair users=3)
One per week 30
16 April–27August 2003
Afternoon group 7 men, 5 women(wheelchair users=0)
One per week 13
30 June–15August 2003
Summer group 7 men, 3 women(wheelchair users=1)
Three per week 21
Table 1 Examples of the DHHTG seed or plant material, its purposes and main therapeutic usefulness
Main therapeutic use Purposes of the seed or plant materialExamples of seed or plant materialused (Latin names)
Mental healing, recreation,cognitive re-organization
Good germinativeness Calendula officinalisSuitable hardiness for the climate zone TagetesWell-known and therefore enables patients torecognize the plants and flowers used forsquare cultivation
Impatiens walleriania
Cognitive re-organization; memorystimulation
Arouse childhood memories Tropaeolum pereqrinumAntirrhinum majusRaphanus satiuus
Mental healing, recreation, socialinteraction
Beautiful colour Impatiens hawkeri (red, pink,white, violet)
Sensory stimulation Wonderful scent Lathrus adoratusHeliotropium arborescensNicotiana sylvestrisMatthiola
Teaching of ergonomic bodypositions
Climbing plants and low height placing allows workwith different body positions at the same time
Nicotiana sylvestris
Ipomea tricolorCosmos bipinnatusHelianthus annuus
Social interaction, cognitivere-organization, training ofsensory-motor function,teaching of ergonomicalbody positions
Vegetables for use in the kitchen designedfor ADL training
Anethum gravealen
Petrose linum (CrispumLactuca (sativa)Beta vulgaris
Sensory stimulation Seeds of various sizes, form, surface Pelargonium�hortorumSenecio sineraria
Social interaction, pre-vocationalskills assessment
Fast-germinating seed for a new collectionevery autumn
Tropaeolum
Calendula officinalisPhaseoulus occineusTagets ‘Silvia’
Non-specific Seeds from exotic plants for use in the garden house Physalis perurianaCitrus
Non-specific Seeds for Swedish cultural plant species Linum (usitatissimum)Recreation, leisure activity According to patient’s wishesCognitive re-organisation Reading instructions and interpreting the pictures
on seed packets
I. Soderback et al.
254
Dev
Neu
rore
habi
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Ank
ara
Uni
v. o
n 10
/30/
12Fo
r pe
rson
al u
se o
nly.
involve, amuse and satisfy them, give them pleasureand promote their creativity and wellbeing. In addi-tion, the garden flowers may inspire patients to tryother leisure activities such as painting or paintingtherapy. Other patient groups aimed for transition ofnew leisure activities using the flowers and harvest forfloral decoration and cooking.
DHHTG gardening for social interaction. Participationin a gardening group was also prescribed for itsassociated psychosocial benefits. It was presumed thatpatients’ interpersonal relations would be strengthenedthrough mutual communication about the DHHTGwork and observable in an increased sense of self-worth, the release of hostility and aggression, sharedcontrol of self and environment, the experience ofchoice, increased socialization, practice in copingskills, increased tolerance of other group members,conscious intellectual stimulation [100], feelings oftogetherness and teamwork. For example, the thera-pist gives the group members ‘garden-related home-work’ to be performed. This task was often used forpatients with aphasia encouraging them to talk andcontinue their interaction.
DHHTG gardening for sensory stimulation or integra-tion. Patients with severe brain damage and decreasedawareness were presumed to receive sensory stimula-tion [101] through the reticular activating system, viaresponses to different plant material [80, 83]. Sensorystimulation was performed in a systematic way. Thetherapist asked the patient questions related tothe plant material and the garden environment. Thepatients’ tasks were to compare or identify variationsof the material. The flowers offered opportunities forstimulation through smelling and seeing. Memoriesconnected to the sense of smell would increase arou-sal. Butterflies and insects would trigger eyes to followthem. Vegetables and spices grown in the gardenwould stimulate taste. Leaves from different species,with rough or smooth or hairy surfaces would stimu-late touch in the hand. Sand, soil and water would sti-mulate sensations in bare feet. Water, birds,bumblebees and soils make sounds that stimulatehearing and sound orientation. Bamboo and reedsmoving in the wind make music that may stimulateauditive perception.
The DHHTG gardening for cognitive re-organization.Different gardening activities such as planning aflowerbed, calculating the depth and distance between
plants, reading instructions on the seed packages orlistening to oral or written instructions for doinggardening were used for patients’ cognitive re-organi-zation therapy of attention, spatial, verbal, numerical,praxis, memory and logical impairments. In this thera-peutic approach, the patients systematically learnstrategies for a new way of performing the activity[102]. For example, special education strategies forplanning the growing process in a flower bed givesopportunities for the patient suffering from frontalbrain damage to re-organize his logical order ability.
The DHHTG gardening for training of sensory-motorfunctions. The various elements of gardening, used ina neutral way and with increasing efforts, werepresumed suitable for training and improvement ofmobility, muscle strength and balance, fine, gross, bi-lateral and eye-hand motor co-ordination, plus rangeof motion. For example, a patient with a right hemi-paresis may overcome and possibly improve muscleweakness of arm and hand by using a high-gearedpair of pruning shears when harvesting tomatoes. Inaddition, for patients with a hemiparesis, gardeningactivities were used with the traditional sensorimotortreatment strategies which are presumed to developthe motor function and motor control, including theapplication of sensory stimulation to muscles andjoints which would facilitate specific motor responses[103]. For example, the patients stand and balancewhen removing faded leaves from the climbing plants,whereas the trellis give support and safety.
The patients had the opportunity to practice ways ofusing adaptations and coping behaviour for performingof the gardening elements [98]. These adaptations wereboth physical and mental. For example, the next groupmeeting was planned such that all group members wereinvolved and all were responsible for a task which wascompatible with their ability.
The DHHTG gardening for assessment of pre-vocational skills and or pre-vocational training.Gardening was prescribed as a part of establishing thepatients’, with pain-related impairments, work toler-ance. The patients’ ability to perform gardeningelements including lifting, reaching, carrying, pushing,pulling, sitting and standing and work tolerancewas observed [98]. With these purposes, digging,re-construction and repairing of paving, drawing thelawn mower, moving or mounting shelves, carryingboxes and moving sacks with soil were common work
Horticultural therapy
255
Dev
Neu
rore
habi
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Ank
ara
Uni
v. o
n 10
/30/
12Fo
r pe
rson
al u
se o
nly.

tasks. The observed results were presumed to contri-bute to defining the individual patient’s capability[104] to perform employed work.
DHHTG gardening for teaching ergonomic bodypositions. The various gardening occupations were usedfor work-tolerance training. However, the emphasishere was on the most appropriate ergonomic bodyposition and use of garden tools following anthropo-metric principles. For example, during gardening, thejoints were in neutral positions; the gardener directlyfacing the job without twisting his or her body, back,neck or hips. The knees were preferably bent (whenpossible) when picking up items from the ground [98].Kneeling was avoided with the use of raised plant-beds and a garden stool. Further, the gardeners weretaught to work in the most comfortable way [24].It was presumed that this ergonomic approach wouldprevent injuries to muscles and bones and mightafford pain relief. Teaching ergonomic body positionswas used for 45 minutes once a week individually orto groups. The patients with Rheumatoid Arthritisand Chronic Obstructive Lung Disease were giveninformation about suitable tools and working methodsbut did not do gardening.
Educational use of the DHHTG
During a 3-day seminar, rehabilitation team staffwere taught about gardening and the design of a gardenfor horticultural therapy. The members of these teamswere interested in starting their own horticulturaltherapeutic gardening programmes. The results ofthis training contributed to the introduction of �300horticultural-therapeutic gardens throughout Swedentoday. The concept of DHHTG horticultural therapyhas spread and is now in use in nursing homes, rehabili-tation clinics and acute care among people with infirmi-ties, mental retardation, mental illness, neurologicaldiseases such as dementia, multiple sclerosis, strokeand brain damage and musceloskeletal diseases suchas rheumatoid arthritis [24]. DHHTG has been furtheradapted by agricultural training establishments inSweden. The ALNARP campus of the SwedishUniversity of Agricultural Sciences offers a half-termuniversity course ‘Tradgard och park som rehabiliter-ing’ (Gardens and Parks as Rehabilitation) (http://www.movium.slu.se) and the ULTUNA campus inUppsala a quarter-term course in ‘Skoltradgardskurs’(Gardens in the Swedish School System).
Discussion
Restrictions in the literature search and the literatureavailable in the databases used made it difficult to detect
past and present trends in horticultural therapy.
However, the results of this historic review indicatedfour different intervention approaches: (a) ‘Virtual’
elements from nature in the form of pictures, reading
or discussion [10], (b) viewing nature through films orwindows [12, 13], (c) interacting, i.e. visiting a hospital
healing garden and receiving impressions and experi-
ence [44, 80, 94], and (d) action through doing garden-ing jobs [87, 94]. The latter approach was strongly
suggested [4, 87, 92, 105–107], but its use was sparsely
demonstrated, which justifies this description of garden-ing in DHHTG related mainly to patients suffering
from brain damage. The literature suggests or describes
horticultural therapy as a mediator intended to affectpatients’ (a) emotional functions such as stress [75, 84,
93], increasing wellbeing [87,91] or influencing healing
[4], (b) sensory-motor functions and activities [48, 80,83], (c) cognitive functions and activities [14] and
(d) promoting participation in social life, such as
prevocational training [14] or the avoidance of socialisolation [10] or the promotion of human habits [108].
The descriptions concerned people with mental [94, 106,
107, 109] or physical illness requiring vocational train-ing [1, 14, 46].
However, there were very few descriptions of howhorticulture therapy has been used for people with
brain damage. Consequently, the present study may
contribute with its description of how horticulturaltherapies are being organized at Danderyd Rehabili-
tation Clinic. The patients with brain damage interacted
in the garden, mediating healing and social interactions.They interacted by doing gardening jobs, mediating in
reaction the training of sensory stimulation, cognitive
re-organization, sensory-motor functions and pre-vocational skills. The presentation is based on personal
communication and popular-science articles [23, 24,
26–28] in Swedish, combined with acknowledgedoccupational therapy literature. However, it would
have been desirable to use direct observation or medical
records for analysis. Therefore, even if full identificationof this horticultural-therapeutic approach and its effec-
tiveness is still incomplete, it may be helpful to plan and
conduct such direct studies.
Many of the articles reviewed include recommenda-
tions for planning horticultural therapy [110], the
designing of a hospital healing garden [6, 75] in theform of herb [111] or hospice [78] gardens, suggestions
for suitable plant material [112], methods and tools
I. Soderback et al.
256
Dev
Neu
rore
habi
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Ank
ara
Uni
v. o
n 10
/30/
12Fo
r pe
rson
al u
se o
nly.

adapted for people with various disabilities [113]and, finally, exploration of the importance of speciallandscapes (adventure playgrounds, children’s farms,ecological parks or landscaped school grounds) tofacilitate children’s learning [114].Another value of the DHHTG was its use for training
in horticultural therapy for rehabilitation team mem-bers. This has resulted in the establishment of newhospital gardens in Sweden. A similar process hasbeen going on over the past 16 years in the UK,where the project strongly promotes its healthbenefits [115].The articles used in this study for reviewing the
literature of horticultural therapy represent severaldifferent disciplines: anthropology, environmentalpsychology, horticulture, landscape architecture, medi-cine [67] and occupational therapy. This in turn mayhave influenced the selection of articles and restrictedthe review. However, the findings presented above arecomparable to those of an integrative literature reviewby Jones and Haight [108] published in 2002. Theseauthors reviewed 24 articles on the use of the naturalenvironment in the form of plants or plant material astherapeutic interventions, either virtually or actually,among resident patients with altered mental healthstatus or learning disabilities: older adults with alteredlevels of impairment.Although horticulture therapy was strongly advo-
cated, its effects were less established, except for theenvisaging and viewing aspects. It was suggestedthat the envisaging and viewing form of horticulturaltherapy, based on the hypothesis of a beneficial rela-tionship between humans and the natural environmentpositively affects mood and provides mental restora-tion. This tallies with Relf ’s [67] review (see above)that ‘views of nature have positive, psychologicalresponses, physiological impacts (lower blood pressure,reduced muscle tension), and a reduced need formedical treatment occurs’.The interacting form of horticulture was evaluated
[115] among 22 patients on a geriatric ward who hadaccess to an indoor conservatory garden connectedwith an outdoor garden. The patients behaviour wasobserved regarding their movements on the ward1 month before the gardens were installed and 1 and 6months thereafter. The results demonstrated positivereactions and increased the number of visits to theoutdoor garden following installation of the indoorconservatory.Elderly people’s (n¼ 24) action was assessed during a
3-month structured gardening intervention, showing asignificant improvement (p<0.000) in wellbeing [87].
A study with an hermeneutic phenomenologicalresearch approach [94] was conducted among peoplewith chronic mental illness (n¼ 10) who were membersof a club. The aims were to explore the participants’experiences of gardening.
When horticulture was used in this group-basedsetting immediate and positive effects were observed interms of quality of life, well being and self-concept.
Summary
This article (a) gives a broad historic overview ofhow horticultural therapy has been used; (b) describesthe design and organization of Danderyd HospitalHorticultural Therapeutic Garden and (c) for patients’with brain injuries, outlines how gardening as a tonicoffers a supplement to their rehabilitation, in terms ofmental healing, recreation, social interaction, sensorystimulation, cognitive reorganization, training ofsensorimotor function, pre-vocational assessment andthe teaching of ergonomics. However, the effectivenessof these intervention approaches remains to be proved.
Acknowledgements
Our deep thanks for financial support are due to the Rehabilitation
Clinic, Danderyd Hospital and to Stiftelsen Oskar Hirsch Minne (The
Oskar Hirsch Memorial Foundation).
References
1. Airbart, D. L., Williams, T. and Westrick, P.: Horticulturaltraining for adolescents special education students. Journal ofTherapeutic Horticulture, 2: 17–22, 1987.*
2. Hagedorn, R.: Occupational Therapy. Perspectives and process(London: Churchill Livingstone), 1995.
3. Hagedorn, R.: Environment and opportunity: the potential ofhorticulture for enriching the life of disabled people. ClinicalRehabilitation, 2: 249–251, 1988.*
4. Marcus, C. C. and Barnes, M.: Acute care hospitals: casestudies and design guidelines. In: C. D. Marcus and M. Barnes(editors) Healing gardens: Therapeutic Benefits and DesignRecommendations (New York: John Wiley), pp. 157–234, 1999.
5. Zeisel, J.: Introduction. In: A. Dilani (editor) Design & Health.The therapeutic benefits of design (Stockholm: Svensk Byggtjanst),p. 7, 2001.
6. Cooper Marcus, C.: Gardens and health. In: A. Dilani (editor)Design & Health. The therapeutic benefits of design (Stockholm:Svensk byggtjanst), pp. 61–71, 2001.
7. Ulrich, R. S.: Effects of healthcare environmental design on med-ical outcomes (DCHP). In: A. Dilani (editor) Design & Health. Thetherapeutic benefits of design (Stockholm: Svensk byggtjanst), pp.49–59, 2001.
8. The Center for Health Design: Strategies for success: TheEnhanced Standards of the Joint Commission on Accreditation ofHealthcare Organisations (The Center for Health Design), 1998.
9. Zeisel, J.: Health Outcomes. Improvements from Alzheimer’s CareDesign. Design & Health. The therapeutic benefits of design(Stockholm: Svensk Byggtjanst), 2001.
Horticultural therapy
257
Dev
Neu
rore
habi
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Ank
ara
Uni
v. o
n 10
/30/
12Fo
r pe
rson
al u
se o
nly.
10. Arnetz, B., Theorell, T., Levi, L. et al.: An experimentalstudy of social isolation of elderly people: psycho-endocrine andmetabolic effects. Psychosomatic Medicine, 45: 395–406, 1983.*
11. Theorell, T.: Physiological reactions to creative and less creativeenvironments. In: A. Dilani (editor) Design & Health. Thetherapeutic benefits of design (Stockholm: Svensk Byggtjanst),pp. 11–16, 2001.*
12. Ulrich, R. S.: Views through a window may influence recoveryfrom surgery. Science, 224: 420–421, 1984.*
13. Ulrich, R. S., Simons, R., Losito, B. et al.: Stress recoveryduring exposure to natural and urban environment. Journal ofExperimental Psychology, 11: 201–230, 1991.*
14. DeHart Bennett, M. E. and Relf, D.: Horticultural occupa-tions for persons with intellectual disabilities. AustrianOccupational Therapy Journal, 27: 143–146, 1990.*
15. Sarno, T. M. and Chambers, N.: A horticultural therapyprogramme for individuals with acquired aphasia. Activities inAdaptation and Aging, 22: 81–91, 1997.*
16. Ottosson, J.: Naturens betydelse i en livskris (The importance ofnature when being a crisis of life) (In Swedish) (Lund: Movium.Alnarp), 1998.
17. White, A. S. and Lake, C.: Gardening for the disabled. NursingTimes, 24: 678–680, 1973.*
18. Allied and Complementary Medicine (AMED) 1985-to-present. Available online at: http://www.ovid.com/site/catalog/DataBase/12.jsp?top¼2&mid¼3&bottom¼7&subsection¼ 10
19. Cumulative Index toNursing &AlliedHealth Literature�
CINAHL Information Systems. CINAHL�, 1982-to-present.Available online at: http://www.ovid.com/site/catalog/DataBase/40.jsp?top¼2&mid¼3&bottom¼7&subsection¼10
20. US National Library of Medicine. MEDLINE�—SpecificSubjects Internal/General Medicine, 1966–to-present. Availableonline at: http://www.ovid.com/site/catalog/DataBase/900.jsp?top¼2&mid¼3&bottom¼7&subsection¼10
21. American Horticultural Therapy Association, 2001.Available online at: http://www.hort.vt/human/JTHort.html.
22. Sveriges Lantbruksuniversitet: database: Lucas: The Libraryof Alnarp, 2003. Available online at: http://www.bib.slu.se
23. Dahlba« ck, B., Normell, L. and So« derstro« m, M.: Beskrivningav traningstradgarden for rorelsehindrade vid Medicinska rehabili-teringskliniken, Danderyds sjukhus och uppfoljning av tre arsverksamhet (Description of the training garden for people withmovement disabilities in the Medical rehabilitation clinic,Danderyd hospital and a three year follow-up) (In Swedish)(Stockholm: Rehabilitation clinic, Danderyd hospital), 1989.
24. Sandberg, K., Ahlgren, G., Einarsson, L. et al.:Mojligheternas tradgard, en tradgard for alla. (The possibilitygarden, a garden for all people) (In Swedish). In: K. Sandberg(editor) (Stockholm: Hjalpmedelsinstitutet och Sveriges utbild-ningsradio AB), pp. 124–126, 2000.
25. Landin Lorentzen, L.: Utrustning for rorelsehindrades tradgard-sarbete. Forstudie och utvardering (Equipment for gardeningamong people with movement-related disabilities. Pre-studyand evaluation) (In Swedish) (Huddinge, Stockholm: LandinLorentzen Design AB), 1998.
26. Jansson, E.: Traningstradgard—for rikare liv (Training garden—for enriching life) (In Swedish). Arbetsterapuen (Official magazinefor Swedish Occupational Therapists), pp. 4–9, 1987.
27. Fagerstro« m, C.: Arbeta i tradgarden ren terapi: Danderyds sju-khus later patienterna trana koncentration och finmotorik (Workin the garden is therapy. Patients at Dandryd hospital is trainingconcentration and fine mobility) (In Swedish). Landstingsvarlden,(Magazine for people employed in the Stockholm CountyCouncil), 1994.
28. So« derstro« m, M., Dahlba« ck, B. and Jansson, E.: Traning itradgard for framtida liv. Om horticulture therapy—for informationand inspiration (A lease on life—thanks to garden training)(In Swedish) (Stockholm: Rehabilitation clinic, Danderydhospital), 1994.
29. Ahlstro« m, C.: Upplevelser och erfarenheter av tradgardsaktivit-eter i arbetsterapi: fyra personer med stroke (Experiences of horti-culture in occupational therapy: four people suffering fromstroke) (In Swedish) (Stockholm: The university high school forhealth sciences, the Dept. of Occupational therapy, KarolinskaInstitute), 1996.
30. Mannervik, G. and Lyberg, M.: Tradgardsaktiviteter—sedda urkonkret, symbolisk och sjalvbelonande dimension samt den materi-ella omgivinings krav (Activities in garden—a concrete, symbolicand self-rewarding perspective and the requirement of the physicalsurrounding environment) (In Swedish) (Stockholm: The univer-sity high school for health sciences, the Dept. of Occupationaltherapy, Karolinska Institute), 1994.
31. So« derstro« m, M.: Horticulture therapy in rehabilitation. BarinInjury, 17: 1–4, 2003.
32. So« derstro« m, M.: Redan de gamla grekerna (Already the oldGreeks) (In Swedish). In: K. Sandberg (editor) Mojligheternastradgard, en tradgard for alla (The possibility garden, a gardenfor all people) (In Swedish) (Stockholm: Hjalpmedelsinstitutetoch Sveriges utbildningsradio AB (The Swedish Institute forHandicapped and The Swedish Broadcasting AB)), 2000.
33. Jernberg, A.: Natur och tradgard inom vard och omsorg (Natureand garden within care and caring (In Swedish) (Falun: Dalaransforskningsrad och Institutionen for landskapplannering, SverigesLantbruksuniveritet (The Swedish University of AgriculturalScience), 2001.
34. Baum, C. and Christiansen, C.: The occupational therapycontext. Philosophy—principles, practice. In: C. Christiansen(editor) Occupational therapy. Enabling function and well-being(Thorofare, NJ: SLACK Inc), p. 118, 1997.
35. Meyer, A.: The philosophy of occupational therapy. Archivesof Occupational Therapy, 1: 1–10, 1922.
36. Corcoran, M. and Gitlin, L.: The role of the physical environ-ment in occupational performance. In: C. Cristensen and C. Baum(editors) Occupational therapy. Overcoming human deficits(Thorofare, NJ: SLACK), pp. 1–10, 1997.
37. Menninger, C. F. and Pratt, J. R.: The therapy of gardening.Popular Gardening, 8: 54, 1957.*
38. Riordan, R. J.: Gardening as a rehabilitation adjunct. Journal ofRehabilitation, 49: 39–41, 1983.*
39. Chaplin, M.: Garden tools. Nursing Times, 11: 1069–1071,1974.*
40. Chaplin, M.: Gardening in rehabilitation. Physiotherapy,59: 80–83, 1973.*
41. Brown, D. J., Powell, H. M., Battersby, S. et al.: Designguidelines for interactive multimedia learning environment topromote social inclusions, Disability and Rehabilitation 24: 587–597, 2002.*
42. White, A. S.: Gardening for the disabled child. Medical BiologyIllustrations, 17: 270–272, 1967.
43. Chaplin, M.: Indoor gardening for handicapped people, Vol. 12(London: BT Batsford (original)), 1979.*
44. Powell, L., Felce, D., Jenkins, J. et al.: Increasing engagementin a home for the elderly by providing an indoor gardeningactivity. Behaviour Research & Therapy, 17: 127–135, 1979.*
45. Kaplan, R.: Some psychological benefits of gardening.Environment and Behaviour, 5: 145–162, 1972.*
46. Relf, P. D.: The use of horticulture in vocational rehabilitation.Journal of Rehabilitation, 47: 53–56, 1981.*
47. Relf, P. D.: Not your usual tools. National Council for therapyand rehabilitation through horticulture newsletter, 110: 1–4, 1983.*
48. McBey,M.A.: Janforum. The therapeutic aspects of gardens andgardening: an aspect of total patient care. Journal of AdvancedNursing, 10: 591–595, 1985.*
49. Wilson, E. O.: Biophilia: the human bond with other species(Cambridge: Harvard University Press), 1984.
50. Frumkin, H.: Human health and the natural environment.American Journal of Preventive Medicine, 20: 241–242, 2001.*
I. Soderback et al.
258
Dev
Neu
rore
habi
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Ank
ara
Uni
v. o
n 10
/30/
12Fo
r pe
rson
al u
se o
nly.
51. Manuel, P. M.: Occupied with ponds: exploring the meaning,bewaring the loss for kids and communities of nature’s smallspaces. Journal of Occupational Science, 10: 31–39, 2003.*
52. Ulrich, R. S.: Natural versus urban scenes. Some psychologicaleffects. Environment and Behavior, 13: 553–556, 1981.*
53. Doutt, K. M., Airhart, D. L. and Willis, T. W.: Horticulturaltherapy. Activities for exceptional children. Journal of TherapeuticHorticulture, 4: 10–14, 1989.*
54. Ackley, D. and Cole, L.: The effect of horticultural therapyprogramme on children with cerebral palsy. Journal ofRehabilitation, 53: 70–73, 1987.*
55. McGinnis, M.: Gardening as therapy for children with behav-ioral disorders. Journal of Child and Adolescent Psychiatric andMental Health Nursing, 2: 87–91, 1989.*
56. Kien, C. L. A. R. C.: Physical activity in middle school-agedchildren participating in a school-based recreation program.Archives of Pediatric Adolescent Medicine, 157: 811–815, 2003.*
57. Bunn, D. E.: Group cohesiveness is enhanced as children engagein plant stimulated discovery activities. Journal of TherapeuticHorticulture, 1: 37–43, 1986.*
58. Eberbach, C.: Gardens from a child’s view—an interpretationof children’s art-work. Journal of Therapeutic Horticulture, 2:9–16, 1987.*
59. Williams, P. N. and Mattson, R. H.: Horticultural activitiesand demographic factors influence children’s self-esteem. Journalof Therapeutic Horticulture, 3: 39–54, 1988.*
60. Smith, D. J.: Horticultural therapy: the garden benefits everyone.Journal of Psychosocial Nursing and Mental Health Services,36: 36–37, 1998.*
61. Gardam, M. A., Arthurs, B. P. and Miller, M. A.: An eye forhorticulture. Lancet, 21: 876, 1998.*
62. Scarfone, S. C.: Design of outdoor environments for wellnessin the role of landscape architecture. Journal of TherapeuticHorticulture, 8: 68–71, 1996.*
63. Biley, F. C.: Hospitals: healing environments? ComplementaryTherapy in Nursing and Midwifery, 2: 110–115, 1996.*
64. Barnes, M.: Designing for emotional restoration: understandingenvironmental cues. Journal of Therapeutic Horticulture, 8:11–14, 1996.*
65. Grahn, P.: Om parkers betydelse: parkers mojligheter att under-latta och berika foreningsverksamhet och arbete pa daghem, skolor,servicehus och sjukhus (About parks importance) (In Swedish)(Lund: Alnarp: Sveriges Lantbruksuniversitet. (Swedish agricul-ture university)), 1991.
66. Ku« ller, R. and Ku« ller, M.: Stadens gronska, aldres utevistelseoch halsa (The green foliage, elder people’s outdoor visit andhealth) (In Swedish) (Stockholm: Statens rad for byggnadsforskn-ing), 1994.
67. Relf, D.: Human issues in horticulture. Horticulture Technology,2: 1–11, 1992.*
68. Kaplan, R. and Kaplan, S.: Experience of nature—A psycholo-gical perspective (Cambridge: Cambridge University), 1989.
69. Ulrich, R. S.: Effects of health facility interior design on well-ness: theory and scientific research. Journal of Health Care Design,3: 97–109, 1992.*
70. Ulrich, R. S.: Evidence-based environmental design for improvingmedical outcomes. Healing by design: Building for health care in the21st Century (Montreal: McGill University Health Care), 2000.
71. Smith, R.: Understanding and overcoming burnout. Journal ofTherapeutic Horticulture, 1: 15–24, 1986.*
72. Johansson, A.: Tillbaka till naturen (Back to nature) (InSwedish). Dagens Nyheter (The Daily News) (Stockholm), pp.20–22, 2003.
73. Kaplan, S.: The restorative environment: nature and humanexperience. In: D. Relf (editor) The role of horticulture inhumanwell-being and social development: A national symposium(Portland, OR: Timber Press), pp. 134–142, 1992.
74. Alison, P. C., Barnes, M., Burnett, J. et al.: The anatomy ofa healing garden. Journal of Health Design, 10: 101–112, 1998.*
75. Salamy, V. M.: Stress management through garden design.Journal of Therapeutic Horticulture, 8: 32–35, 1996.*
76. Ottosson, J. and Grahn, P.: Utemiljons betydelse for aldre medstort vardbehov: fallstudien ‘Med ogon kansliga ror gront’ (Theimportance of the outdoor environment for old people whohas a major caring need) (In Swedish) (Lund: SverigesLantbruksuniversitet), 1998.
77. Zhou, W. and Relf, D.: Horticulture for special populations inChina. Journal of Therapeutic Horticulture, 6: 10–15, 1991.*
78. Wood, A.: Hospice gardens. European Journal of Palliative Care,6: 19–21, 1999.*
79. Martin-Yates, T.: A comparison of the effects of horticulturaltherapy and pet therapy on self-esteem and wellbeing of adultswith visual disabilities. Journal of Therapeutic Horticulture, 5:47–58, 1990.*
80. Bryant, W.: Creative group work with confused elderly people:a development of sensory integration therapy. British Journal ofOccupational Therapy, 54: 187–192, 1991.*
81. Darbyshire, P.: Nursing narratives: flowering potential to help apatient with severe dementia rediscover his old gardening skills.Nursing Times, 88: 48, 1992.*
82. Schleien, S. J., Rynders, J., Musonen, T. et al.: Teachinghorticulture skills to adults with autism: a replicated case study.Journal of Therapeutic Horticulture, 6: 21–37, 1991.*
83. Shirtliffe, D.: Sensory growth. Nursing Times, 92: 42–43, 1996.*84. Smith, D. J. and McCallion, P.: Alleviating stress for family
caregivers of frail elders using horticulture therapy. Activities inAdaptation and Aging, 22: 93–105, 1997.*
85. Hoffman, C. L.: Psychological restoration among AIDS care-givers: Maintaining self-care (Ann Arbor, MI: University ofMichigan), 1991.*
86. Fry, P. L.: Healthy gardening: how to get the most from yourgardening experience. Vibrant Life, 16: 16–19, 2000.*
87. Heliker, D., Chadwick, A. and O’Connell, T.: The meaningof gardening and the effects on perceived well being of a gardeningproject on diverse populations of elders. Activities in Adaptationand Aging, 24: 35–56, 2000.*
88. Unruh, A. M., Smith, N. and Scammel, C.: The occupation ofgardening in life-threatening illness: a qualitative pilot project.Canadian Journal of Occupational Therapy, 67: 70–77, 2000.*
89. Mountford, M.: Health benefits of horticultural therapy: howthe joys of gardening can engender other positive and peacefuleffects on our lives. Positive Health, 65: 24–26, 2001.*
90. Starbuck, J.: The natural way. Why I recommend gardening forhealth. Bottom Line Health, 14: 10, 2000.*
91. Spurgeon, T.: Therapeutic horticulture—growing for optimumwellbeing. Positive Health, 71: 19–22, 2001.*
92. Lochrie, C.: The grace of gardening: in addition to its mentalbenefits, gardening helps counteract the physical harms of stress.Vibrant Life, 19: 16–18, 2003.*
93. Wadso« , K. and Lo« fdahl, M.: Vad betyder grona miljoerfor personer med stressrelaterade besvar? (What means greenenvironments for people with stress-related illness?). SvenskRehabilitering (Magazine for Swedish Rehabilitation), 3: 24–27,2003.
94. Perrins-Margalis, N. M., Rugletic, J., Schepis, N. M. et al.:The immediate effects of a group-based horticulture experienceon the quality of life of persons with chronic mental illness.Occupational Therapy in Mental Health, 16: 15–32, 2000.*
95. Winnberg-Lindqvist, P.: Traningslek i tradgard (Play andtraining in the garden) (In Swedish). In: K. Sandberg (editor)Mojligheternas tradgard, en tradgard for alla (The possibilitygarden, a garden for all people) (In Swedish) (Stockholm:Hjalpmedelsinstitutet och Sveriges utbildningsradio AB),pp. 140–145, 2000.
96. Sandberg, K.: Pers paradis (Per’s paradise) (In Swedish). In:K. Sandberg (editor) Mojligheternas tradgard, en tradgard foralla (The possibility garden, a garden for all people) (In
Horticultural therapy
259
Dev
Neu
rore
habi
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Ank
ara
Uni
v. o
n 10
/30/
12Fo
r pe
rson
al u
se o
nly.

Swedish) (Stockholm: Hjalpmedelsinstitutet och Sveriges utbild-ningsradio AB), pp. 146–148, 2000.
97. So« derstro« m, M.: Tradgarden ett ovningsfalt (Garden as a placefor practice) (In Swedish). In: K. Sandberg (editor)Mojligheternastradgard, en tradgard for alla (The possibility garden, a garden forall people) (In Swedish) (Stockholm: Hjalpmedelsinstitutet ochSveriges utbildningsradio AB), pp. 134–139, 2000.
98. Stein, F., So« derback, I. and Cuttler, S.: Applying theErgonomic Model to Everyday Occupation. home and work envir-onment, 2004 in press.
99. National Library of Medicine (PubMed): MeSH terms isNLM’s controlled vocabulary used for indexing articles inPubMed. Available online at: http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?db¼PubMed, 2002.
100. Glantz, C. H. and Rishman, N.: Leisure activities. In:C. Christiansen (editor) Occupational therapy. Enabling functionand well-being (Thorofare, NJ: SLACK Inc), p. 253, 1997.
101. Gutman, S. A.: Traumatic brain injury. In: L. W. Pedretti andM. B. Early (editors) Occupational therapy. Practice skill forphysical dysfunction (London: Mosby), p. 685, 1997.
102. So« derback, I.: Intellectual function training and intellectualhousework training in patients with acquired brain damage. Astudy of occupational therapy methods. Thesis. Department ofRehabilitation Medicine, Danderyd Hospital; The Departmentof Social Care and Rehabilitation, Stockholm College of Healthand Caring Sciences; Department of Physical Medicine andRehabilitation, Karolinska Institute. Stockholm: KarolinskaInstitute, 1988.
103. Gentile, P. A. and Iyer, M. B.: Traditional sensorimotorapproaches to treatment: an overview. In: C. Baum andC. Christiansen (editors) Occupational therapy. Overcominghuman deficits (Thorofare, NJ: SLACK Inc), p. 253, 1997.
104. So« derback, I., Schult, M.-L. and Jacobs, K.: A criterion-referenced multidimensional job-related model predictingcapability to perform occupations among persons with chronic
pain. Work. A journal of Prevention, Assessment andRehabilitation, 15: 25–39, 2000.
105. Chiu, L.: Facility profile. Planting hope horticulture therapyand training program. Rehabititation Management: TheInterdisciplinary Journal of Rehabilitation, 12: 92–94, 1999.
106. Davies, J.: Towards a happier life: therapeutic horticulture asa means of mental health rehabilitation. Rehabilitation Network,57: 9–11, 2000.*
107. Galvin, K., Sharples, A., Hume, S. et al.: Users’ perspectivesof work rehabilitation with horticultural therapy. British Journalof Therapeutic Rehabilitation, 7: 262–265, 2000.*
108. Jones, M. M. and Haight, B. K.: Environmental transforma-tions: an integrative review. Journal of Gerontological Nursing,28: 23–27, 2002.*
109. Myers, M. S.: Empowerment and community building througha gardening project. Psychiatric Rehabilitation Journal, 22:181–183, 1998.*
110. Goodban, A. and Goodban, D.: Horticultural therapy: agrowing concern, part 2. British Journal of OccupationalTherapy, 53: 468–470, 1990.*
111. Burrough, R.: The Barber-Surgeons’ herb garden. EuropeanJournal of Herbal Medicine, 4: 51–52, 1999.*
112. Bate, M.: Making a physic garden—II. Simile, 3: 10–13, 1993.*113. Pitt-Nairn, E. J., Relf, P. D. and McDaniel, A. R.: Analysis
of factors which can affect the preferences of older individualsfor hand pruners. Physical and Occupational Therapy inGeriatrics, 10: 77–90, 1992.*
114. Moore, R. C.: Compact nature: the role of playing and learninggardens on children’s lives. Journal of Therapeutic Horticulture,8: 72–82, 1996.*
115. Pachanal, N. A., McWha, J. L. and Arathoon, M.: Holistichealth care. Passive therapeutic gardens: a study on an inpatientgeriatric ward. Journal of Gerontology Nursing, 29: 4–10, 2003.*
116. Twigg, S.: Enriching lives through horticulture. A life in the day,6: 18–23, 2002.*
I. Soderback et al.
260
Dev
Neu
rore
habi
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Ank
ara
Uni
v. o
n 10
/30/
12Fo
r pe
rson
al u
se o
nly.