hepatitis and renal disease
TRANSCRIPT
Renal Disease and Viral Hepatitis
Richard McCrory
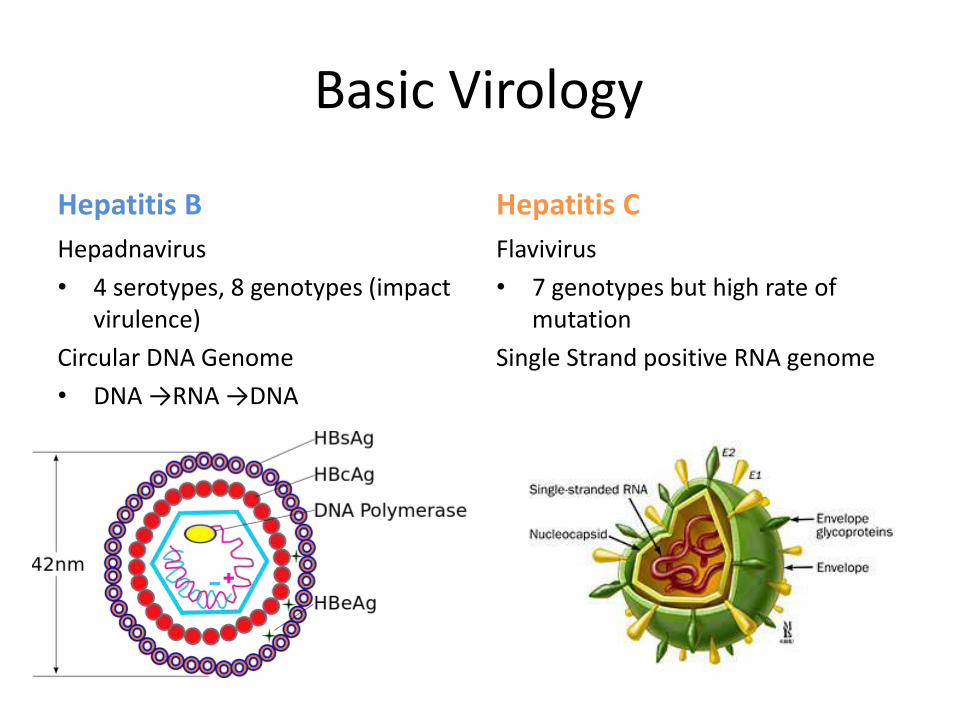
Basic Virology
Hepatitis B
Hepadnavirus
• 4 serotypes, 8 genotypes (impact virulence)
Circular DNA Genome
• DNA →RNA →DNA
Hepatitis C
Flavivirus
• 7 genotypes but high rate of mutation
Single Strand positive RNA genome
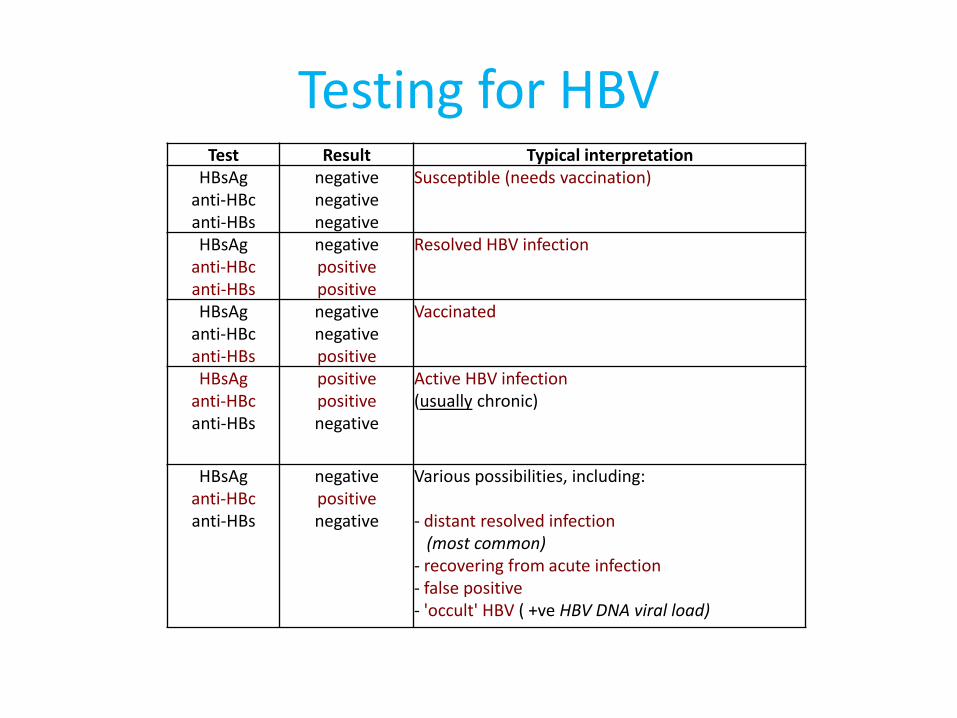
Testing for HBVTest Result Typical interpretation
HBsAganti-HBcanti-HBs
negativenegativenegative
Susceptible (needs vaccination)
HBsAganti-HBcanti-HBs
negativepositivepositive
Resolved HBV infection
HBsAganti-HBcanti-HBs
negativenegativepositive
Vaccinated
HBsAganti-HBcanti-HBs
positivepositivenegative
Active HBV infection(usually chronic)
HBsAganti-HBcanti-HBs
negativepositivenegative
Various possibilities, including:
- distant resolved infection (most common)
- recovering from acute infection- false positive- 'occult' HBV ( +ve HBV DNA viral load)
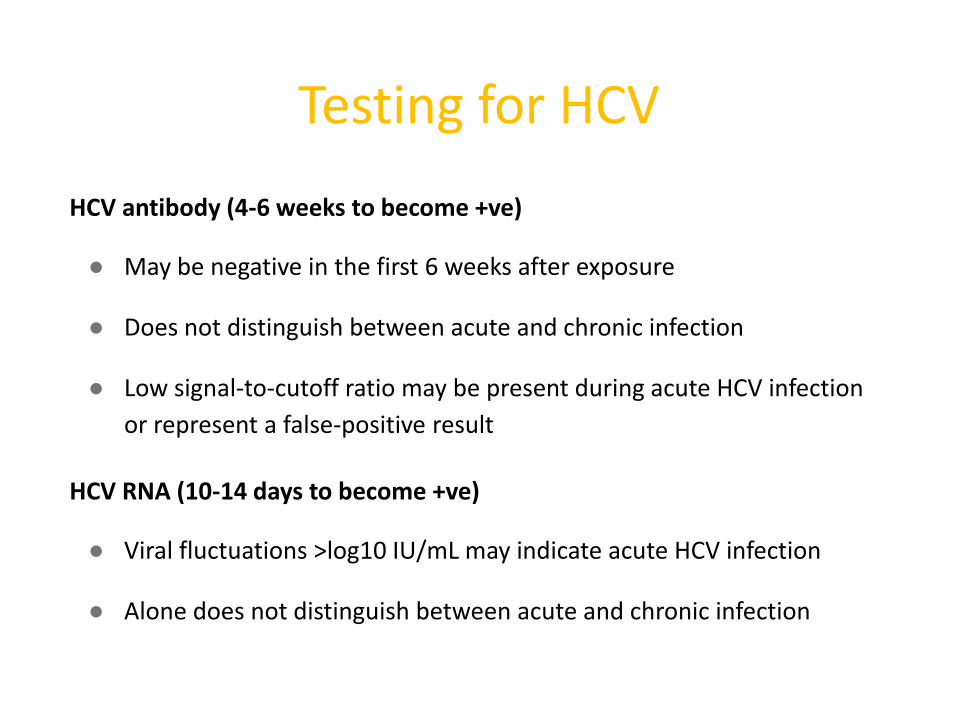
Testing for HCV
HCV antibody (4-6 weeks to become +ve)
● May be negative in the first 6 weeks after exposure
● Does not distinguish between acute and chronic infection
● Low signal-to-cutoff ratio may be present during acute HCV infection
or represent a false-positive result
HCV RNA (10-14 days to become +ve)
● Viral fluctuations >log10 IU/mL may indicate acute HCV infection
● Alone does not distinguish between acute and chronic infection
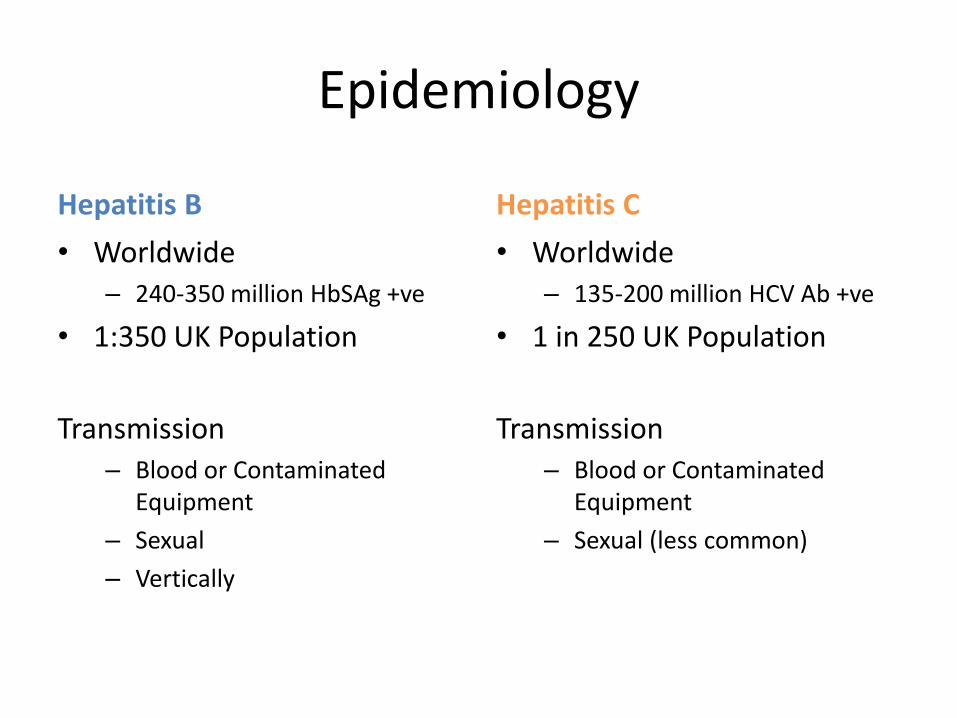
Epidemiology
Hepatitis B
• Worldwide– 240-350 million HbSAg +ve
• 1:350 UK Population
Transmission– Blood or Contaminated
Equipment
– Sexual
– Vertically
Hepatitis C
• Worldwide– 135-200 million HCV Ab +ve
• 1 in 250 UK Population
Transmission– Blood or Contaminated
Equipment
– Sexual (less common)
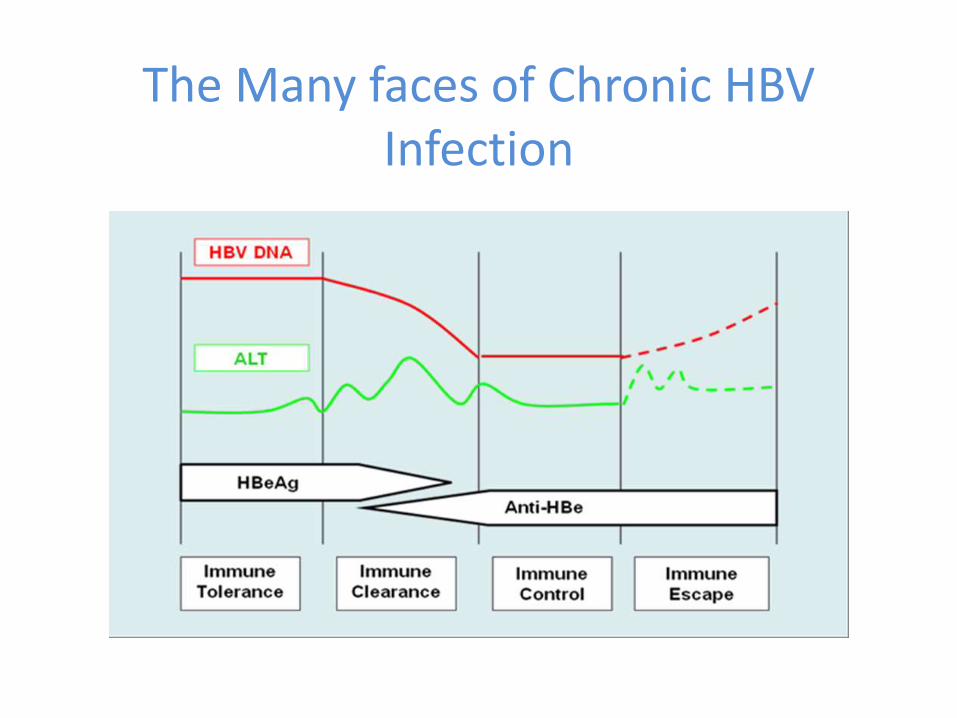
The Many faces of Chronic HBV Infection
Associations of Viral Hepatitis with CKD / ESRD in Taiwan
HBV
HBV +ve prevalence >15% 1985
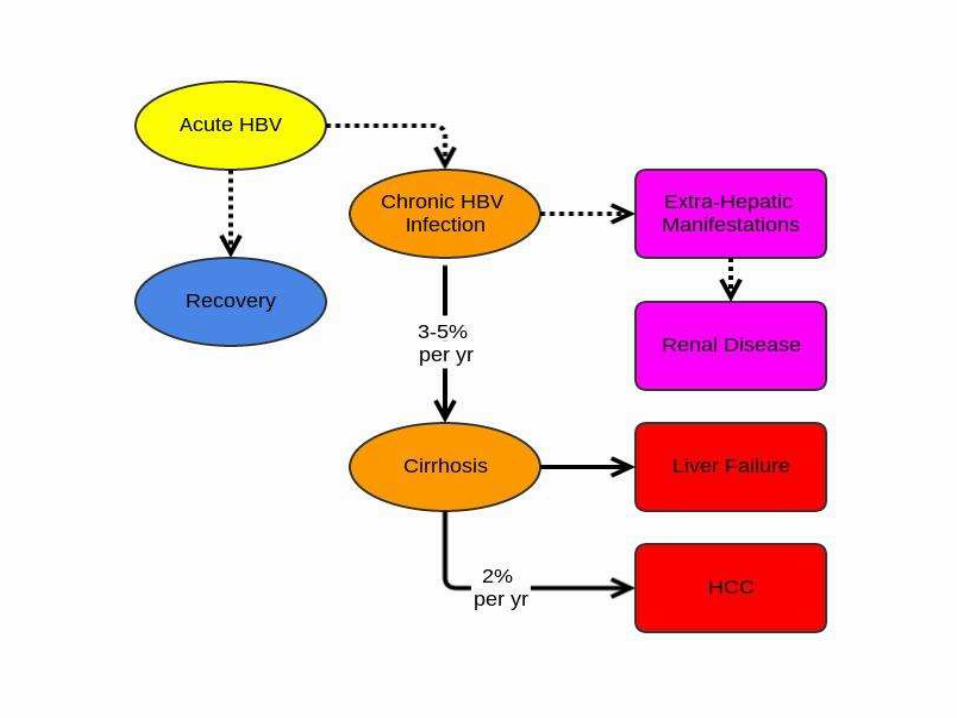
Incidence of ESRD in untreated chronic HBV cohort 2% (HR 3.85)
HCV
High HCV Prevalence
• Incidence of ESRD in chronic HCV patients 2.14 fold higher than age matched cohort
• Patients aged 50-59 had highest incidence
BUTTaiwan has high prevalence of Type 2 DiabetesAssociations between T2DM and both Hepatitis Viruses
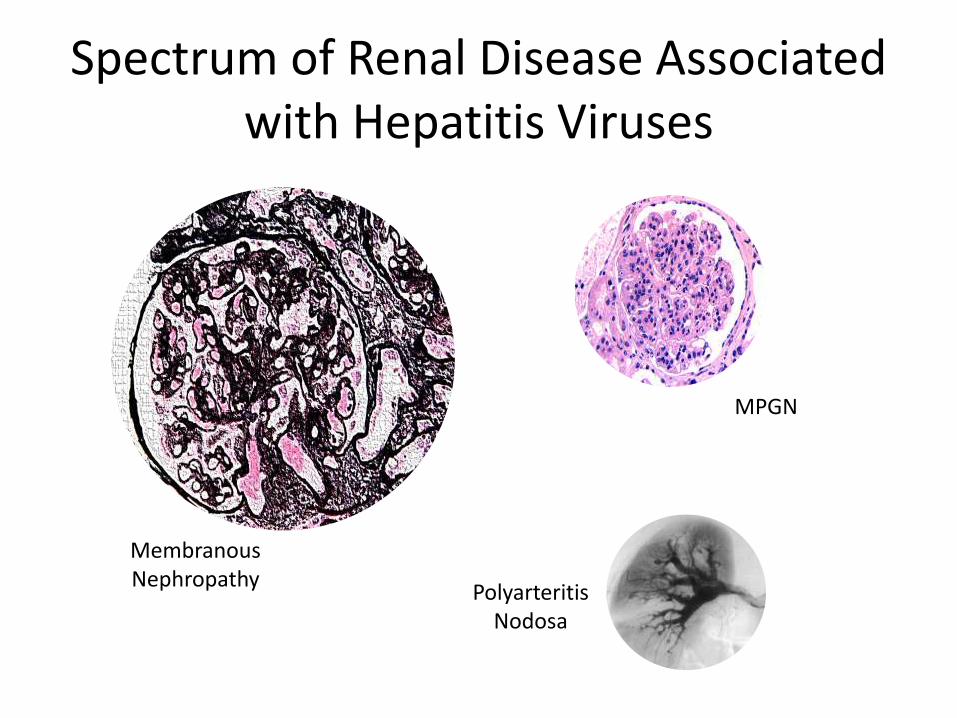
Spectrum of Renal Disease Associated with Hepatitis Viruses
Membranous Nephropathy
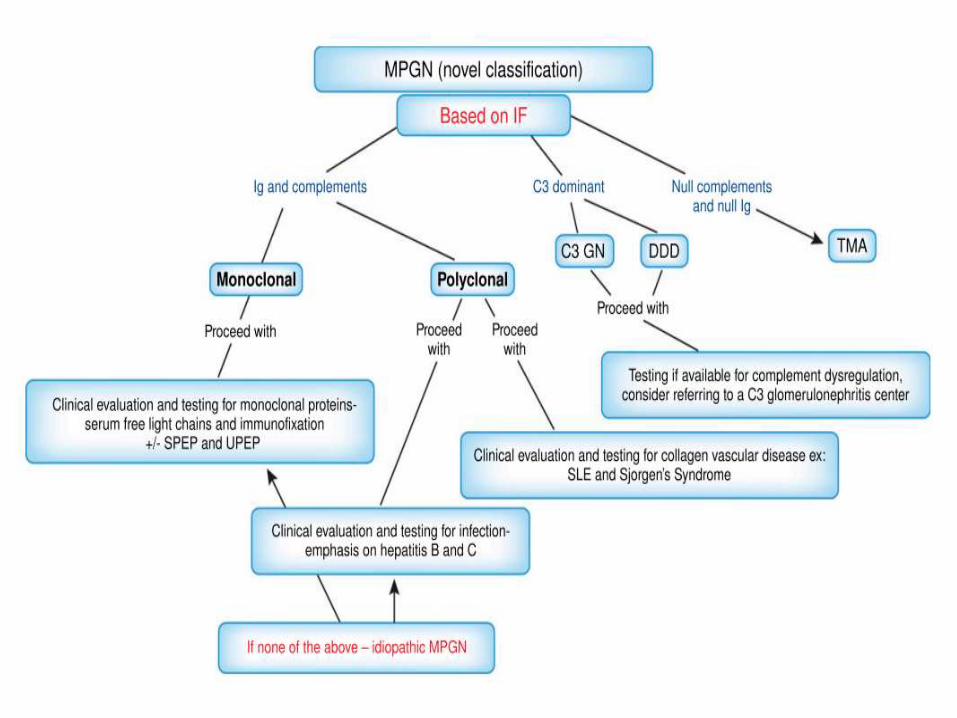
MPGN
PolyarteritisNodosa
Sample Questions
A 41-year-old woman with a recent diagnosis of hepatitis C infection was
found to have a serum creatinine of 167 umol/L. Urine dipstick was
positive for 3+ protein and + blood
Other results are as follows:
24hr Urinary protein - 2.7 g/24 h
C4 - <0.14 g/L C3 - 0.23 g/L
Rheumatoid factor – Positive
ANCA / ANA / Anti-GBM - Negative
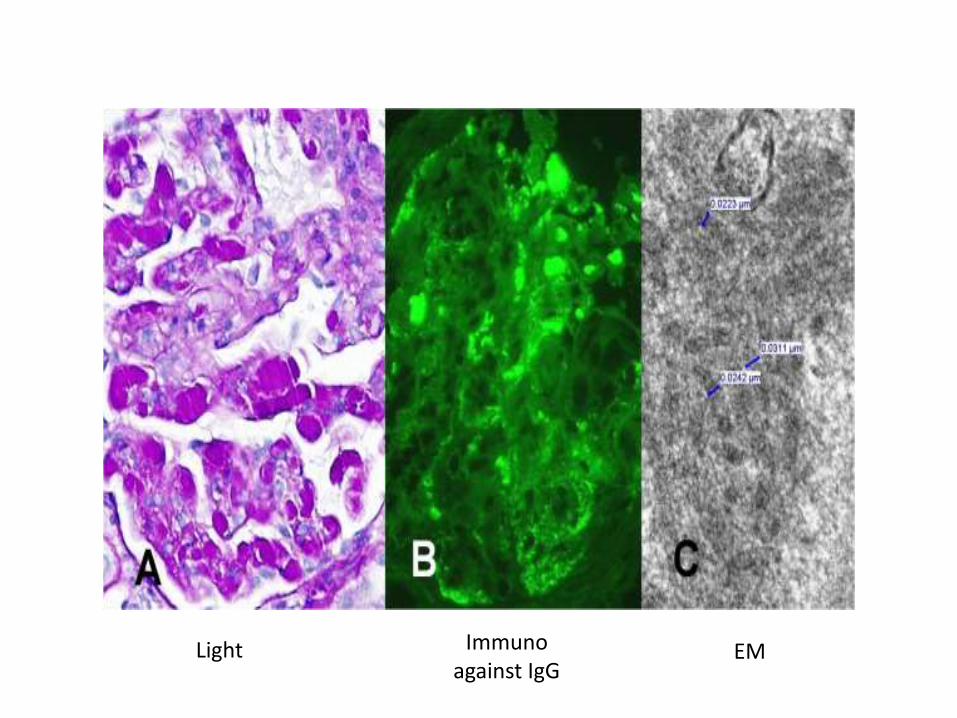
Light Immunoagainst IgG
EM
What is the most likely diagnosis?
A. IgA Nephropathy
B. Cryoglobulinemic Glomerulonephritis
C. Membranous Nephropathy
D. Thrombotic Microangiopathy
E. Crescentic Glomerulonephritis
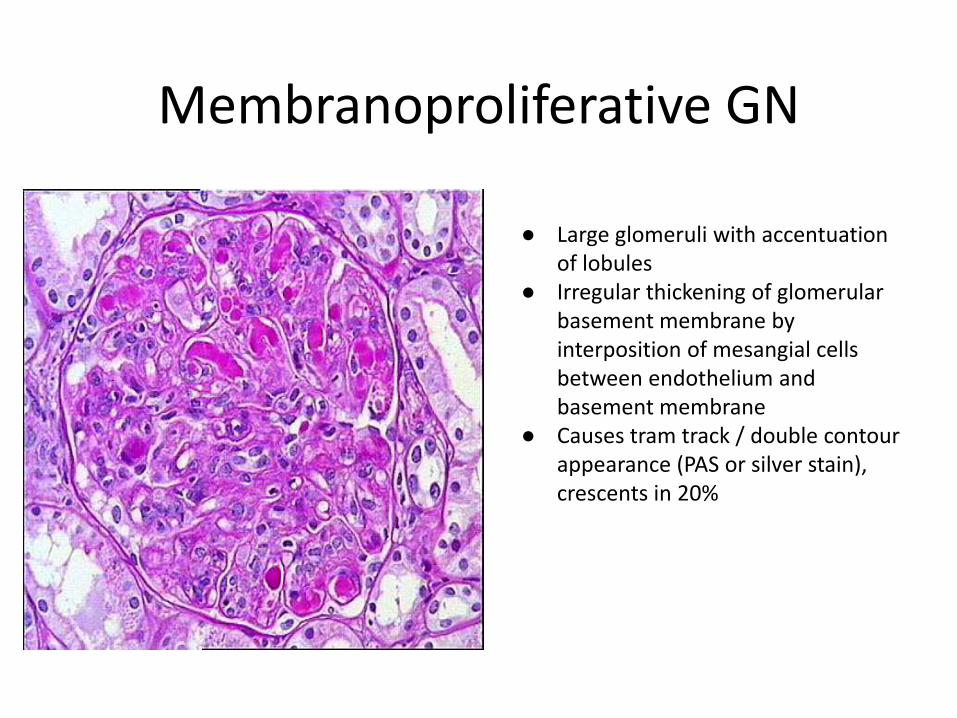
Membranoproliferative GN
● Large glomeruli with accentuation of lobules
● Irregular thickening of glomerular basement membrane by interposition of mesangial cells between endothelium and basement membrane
● Causes tram track / double contour appearance (PAS or silver stain), crescents in 20%
Cryoglobulins in HCV
Type II cryoglobulins● IgM directed against Fc of IgG● Rheumatoid Factor behaviour
40-90% of patients with Chronic HCV have evidence of cryoglobulins● <10% of these will manifest with vasculitis
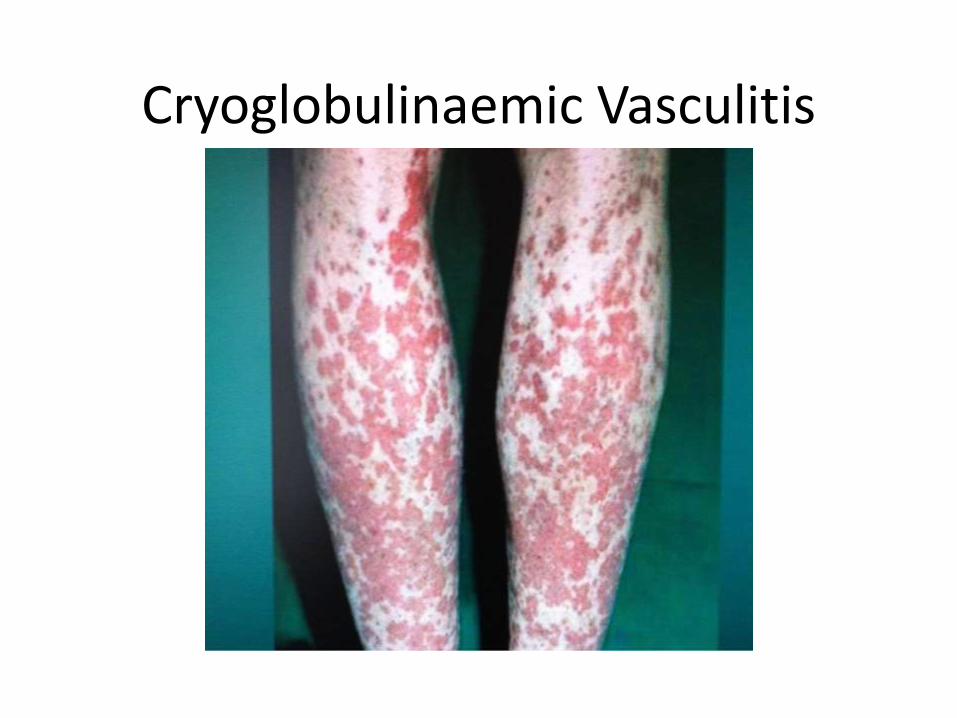
Cryoglobulinaemic Vasculitis
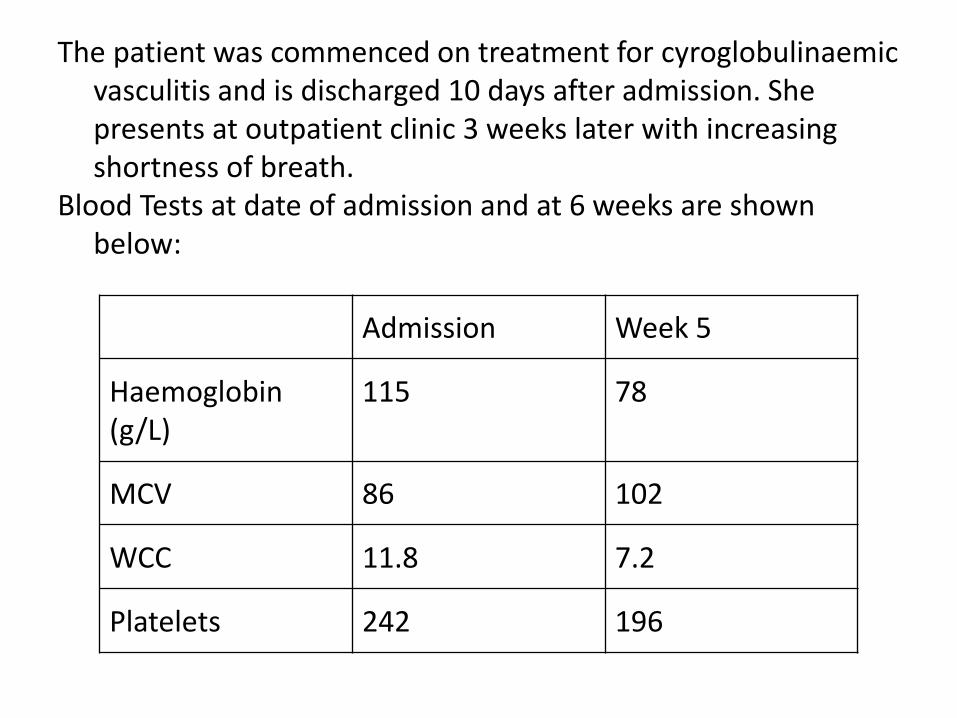
The patient was commenced on treatment for cyroglobulinaemicvasculitis and is discharged 10 days after admission. She presents at outpatient clinic 3 weeks later with increasing shortness of breath.
Blood Tests at date of admission and at 6 weeks are shown below:
Admission Week 5
Haemoglobin(g/L)
115 78
MCV 86 102
WCC 11.8 7.2
Platelets 242 196
What agent started at treatment is most likely to explain the patient’s shortness of breath?
A. CyclophosphamideB. Interferon-AlphaC. RibavirinD. Losartan
HCV Related Glomerular Disease
● Membranoproliferative GN● IgA Nephropathy● Post-infectious GN● Thrombotic Microangiopathy● FSGS● Fibrillary GN
Treatment of HCV-related renal disease
Patients with nephrotic-range proteinuria and/or progressive renal failure:
● Immunosuppressive plus antiviral treatmento Rituximab: 375 mg/m2 weekly for 4 wko Cyclophosphamide: 2 mg/kg per d for 2 to 4 monthso Methylprednisolone pulses: 0.5 to 1 g/d for three consecutive
days● RBV daily: initial dose according to GFR● Some newer agents do not require dose adjustment for GFR● Plasma exchange in case of high cryoglobulin levels
o 3 l of plasma three times per week for 2 or 3 wk
Antivirals for Hepatitis C
Virologic cure = Sustained Virological Response● Absence of detectable HCV RNA >12 weeks after
completion of therapy
Response depends heavily on Genotype● Genotype 1 - 40% response at 48 weeks● Genotype 2/3 - 80% response rate within 12 weeks
HBV Associated Membranous (HBV-MN)
Children● Strong (>80%) Male Preponderance● Commonly presents with nephrotic
syndrome or microscopic haematuria
● Often don’t have overt liver disease
● Remission correlates with viral clearance
Adults● Less favourable prognosis● Proteinuria + Hypertension
In high titre HBsAg Patients● Nephrotic Syndrome + Abnormal
LFTs = >50% RRT at 3yrs
HBeAg / Anti-HBe immune complexes likely culprit for sub-epithelial deposit substrate
HBV DNA can be detected in glomerular & interstitial tissues
Treatment of HBV-MN
Don’t forget measures utilised for other proteinuricdisease!
Immunosuppression monotherapy● Causes more harm than good● Increases viral replication, accelerates
progressionAntivirals
● Suppresses viral load, facilitates clearance of antigen
Interferon● Helps accelerate seroconversion
Antivirals in Hepatitis B
• Aim of therapy – to promote seroconversion• No new drugs in Phase 3 trials presently
• Nucleoside Analogues– Lamivudine
• Cheaper• Mutation Resistance increases with treatment duration
– Entecavir• More Expensive• <1% resistance rate at three years treatment
• Interferon– Finite duration of treatment– No mutation resistance– Side effects can be difficult to manage
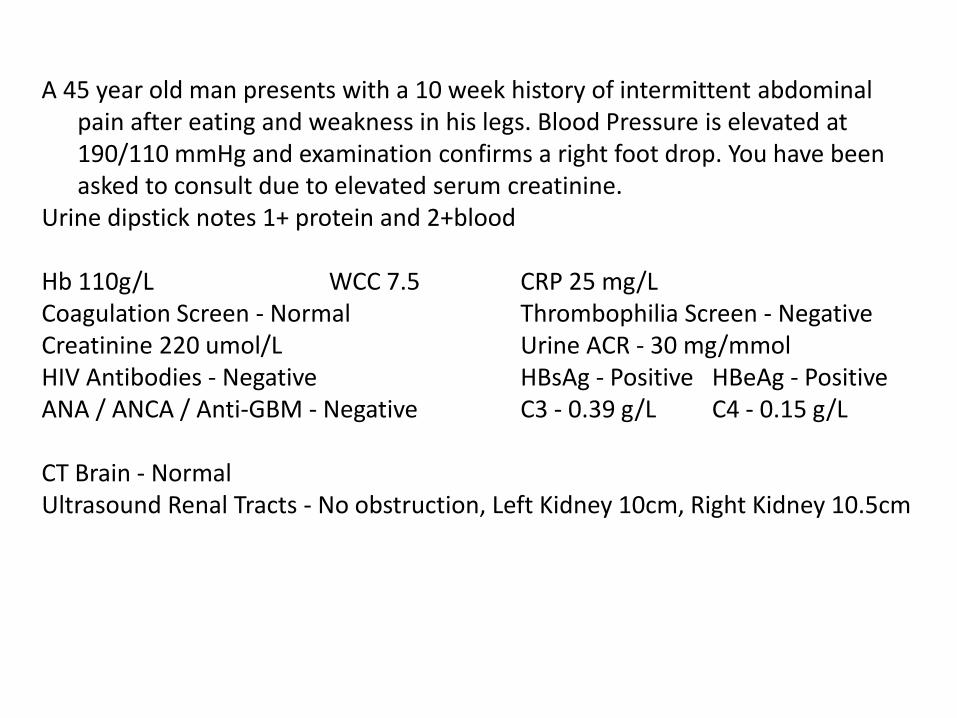
A 45 year old man presents with a 10 week history of intermittent abdominal pain after eating and weakness in his legs. Blood Pressure is elevated at 190/110 mmHg and examination confirms a right foot drop. You have been asked to consult due to elevated serum creatinine.
Urine dipstick notes 1+ protein and 2+blood
Hb 110g/L WCC 7.5 CRP 25 mg/LCoagulation Screen - Normal Thrombophilia Screen - NegativeCreatinine 220 umol/L Urine ACR - 30 mg/mmolHIV Antibodies - Negative HBsAg - Positive HBeAg - PositiveANA / ANCA / Anti-GBM - Negative C3 - 0.39 g/L C4 - 0.15 g/L
CT Brain - NormalUltrasound Renal Tracts - No obstruction, Left Kidney 10cm, Right Kidney 10.5cm
Which of the following would be the best investigationto perform next?
A. Renal BiopsyB. Mesenteric AngiographyC. CT Abdomen with ContrastD. Sural Nerve BiopsyE. Gastroscopy
“Testing is Cheap,Treatment is not”
Viral Hepatitis & Dialysis
DOPPS (2004)● HCV prevalence ranged from 3-23% HD units
over 3 continents● HBV from 0-5%
● Prevalences in Developing World– 18-80%
Vaccinating CKD Patients against HBV
Why not?
– Reduced efficacy of the vaccine
– The low rate of hepatitis B infection
CDC Position (2012)
“The cost of vaccinating patients is mitigated by the reduced need for monthly surveillance of antigen and antibody status”
Use of HBV Vaccines as treatment for HBV?
“Third generation” vaccines show increased immunogenic response in CKD patients
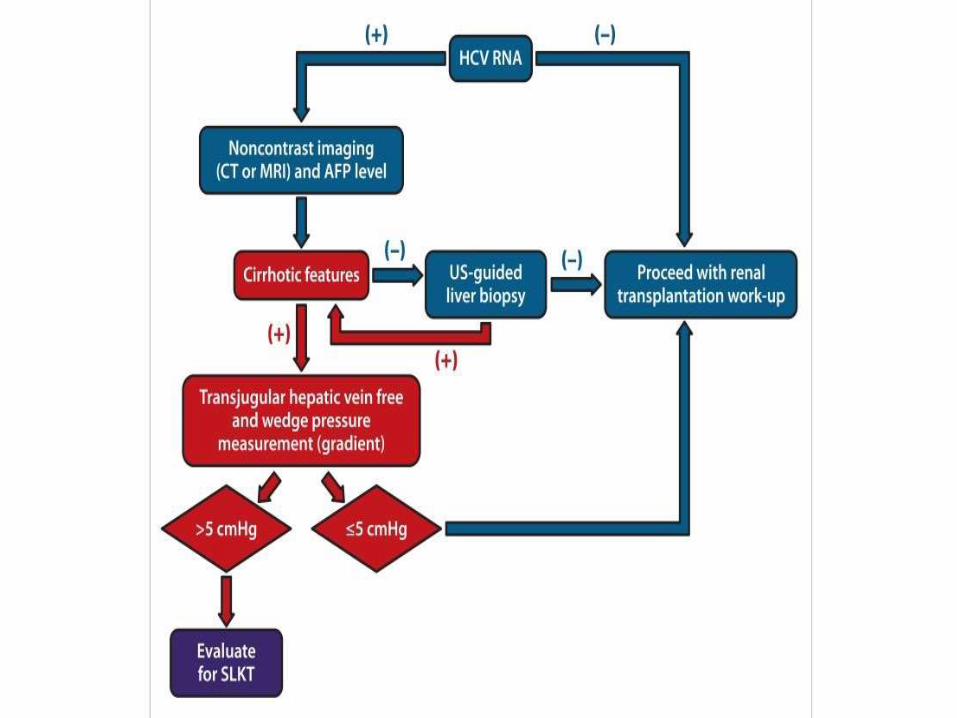
Chronic HBV and Pre-RT evaluation
Involve a Hepatologist!HBeAg status and HBV DNA copy load can help
determine risk of reactivation post-TxHBsAg +ve patients routinely need liver biopsy
Are they a candidate for combined liver-kidney transplant?
Hepatitis B & Renal Transplantation
The HBsAg Positive Donor Kidney● Should not be transplanted into HBV-naive
recipients except in urgent scenario● Risk of de novo infection reduced if donor
anti-HBc positive
General Rules for Recipients with HBV
HBsAg +ve Recipients● Lifelong anti-viral therapy
Anti-HBc +ve(or -ve) / anti-HBs +ve Recipients● No prophylaxis immediately needed, may
need vaccine booster if titre <10IU/ml, need antiviral until anti-HBs >10IU/ml
● HBV DNA monitoring (NICE guidance)
Hepatitis C & Renal Transplantation
The HCV +ve donor kidneyGood experience of transplanting into HCV+ve
recipientsTransplantation confers survival advantage over
staying on waiting listBUT Higher rates of Graft Loss, Rejection
Episodes, NODAT, CMV Disease
Potential KT Recipients with HCV
Sustained virological response preferable to be achieved pre-transplant
Immunosuppression encourages HCV reactivation even if SVR initially achieved
Recommendations on Treatment of Hepatitis C (2014)● Suggest IFN-free regime pre-Tx Regimens of anti-HCV
therapy post transplant similar to non-transplanted patients (without IFN)
● Newer agents not yet extensively investigated
“New Drugs; New Interactions”
Don’t Forget...
● HCC Screening (USS & AFP) (HBV/HCV)● Monitoring blood glucose for development of
NODAT (HCV)
Take Home Points
Testing & Prevention is CheapBurden of Disease & Treatment is Costly
Hepatitis B● Preventing Transmission & Vaccination Works
Hepatitis Co “On the Cusp of Change” with new antivirals