heart.journal, pregnancy in with homograft aortic...
TRANSCRIPT
British Heart.Journal, 1970, 32, 416-49.
Successful pregnancy in a patient with ahomograft aortic valve
W. A. LittlerFrom Liverpool Regional Cardiac Centre, Sefton General Hospital, Liverpool I5
A case is described of a 27-year-old woman whose aortic valve was replaced by a homograft.Eighteen months after the operation she gave birth to a normal healthy girl.
Experience in the management of pregnancyafter successful prosthetic or homograftvalve replacement is not great, and the poten-tial hazards are numerous. This report con-cerns the management and progress of such acase, after successful homograft replacementof the aortic valve, performed because ofsevere aortic regurgitation.
Case reportThis 27-year-old woman gave a past history ofrheumatic fever at the age of 13 and again at I6.Aortic regurgitation was diagnosed when she wasI9, but at that time she was symptomless, andno treatment was advised. At the age of 23 shebegan to complain of increasing effort dyspnoea,and of spontaneous nocturnal dyspnoea, and wasstarted on treatment with lanatoside C and fruse-mide. The symptoms did not improve, but shenever had true effort pain or syncope, and therewas never any evidence of fluid retention.
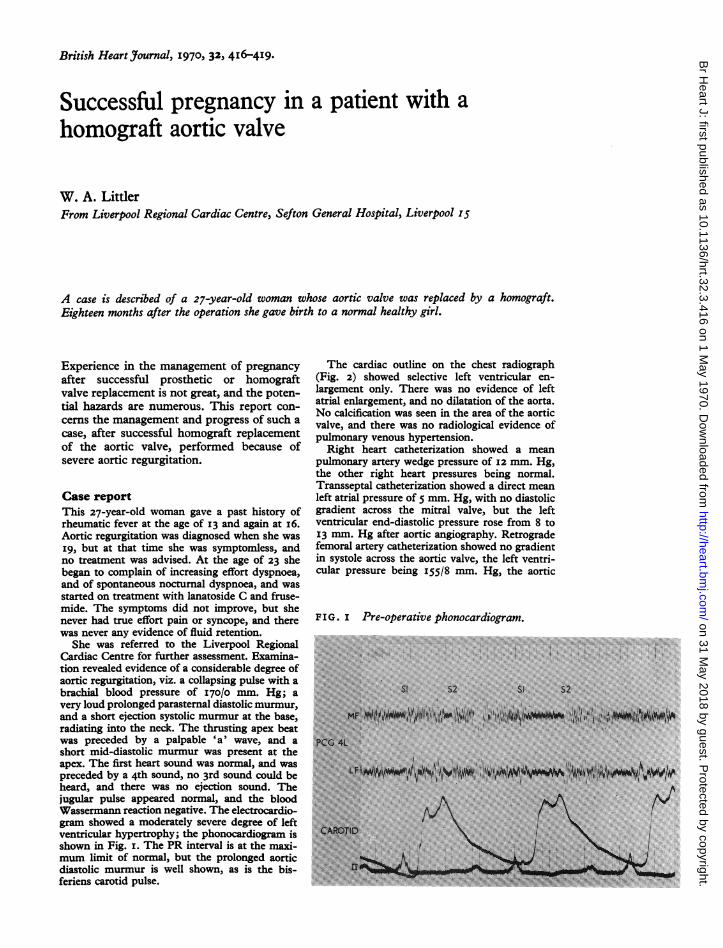
She was referred to the Liverpool RegionalCardiac Centre for further assessment. Examina-tion revealed evidence of a considerable degree ofaortic regurgitation, viz. a collapsing pulse with abrachial blood pressure of I70/0 mm. Hg; avery loud prolonged parasternal diastolic murmur,and a short ejection systolic murmur at the base,radiating into the neck. The thrusting apex beatwas preceded by a palpable 'a' wave, and ashort mid-diastolic murmur was present at theapex. The first heart sound was normal, and waspreceded by a 4th sound, no 3rd sound could beheard, and there was no ejection sound. Thejugular pulse appeared normal, and the bloodWassermann reaction negative. The electrocardio-gram showed a moderately severe degree of leftventricular hypertrophy; the phonocardiogram isshown in Fig. I. The PR interval is at the maxi-mum limit of normal, but the prolonged aorticdiastolic murmur is well shown, as is the bis-feriens carotid pulse.
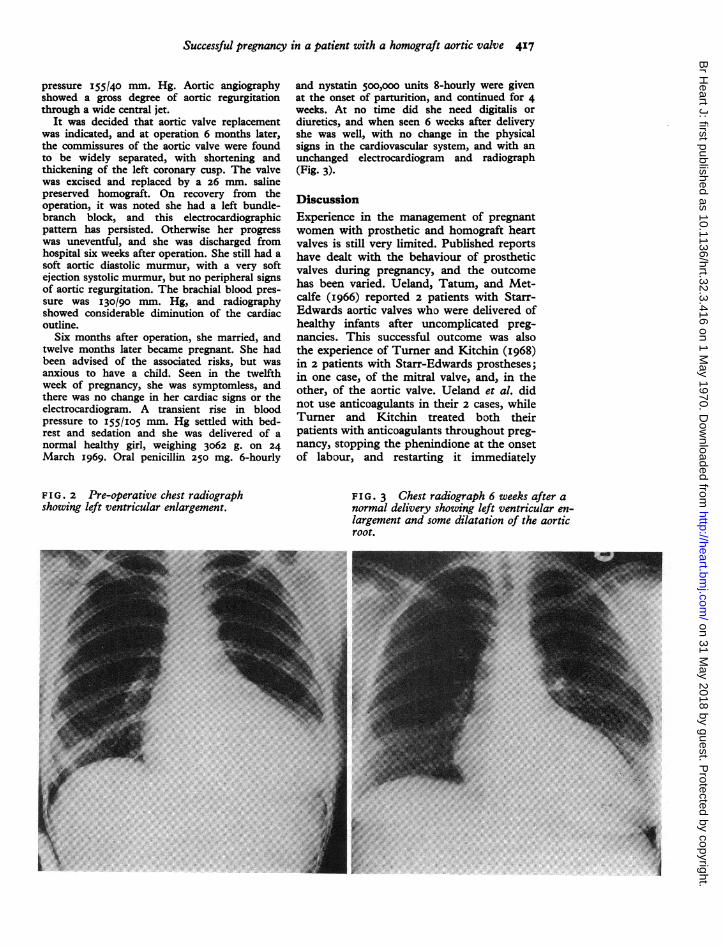
The cardiac outline on the chest radiograph(Fig. 2) showed selective left ventricular en-largement only. There was no evidence of leftatrial enlargement, and no dilatation of the aorta.No calcification was seen in the area of the aorticvalve, and there was no radiological evidence ofpulmonary venous hypertension.
Right heart catheterization showed a meanpulmonary artery wedge pressure of I2 mm. Hg,the other right heart pressures being normal.Transseptal catheterization showed a direct meanleft atrial pressure of 5 mm. Hg, with no diastolicgradient across the mitral valve, but the leftventricular end-diastolic pressure rose from 8 to13 mm. Hg after aortic angiography. Retrogradefemoral artery catheterization showed no gradientin systole across the aortic valve, the left ventri-cular pressure being I55/8 mm. Hg, the aortic
FIG . I Pre-operative phonocardiogram..:' ',........
on 31 May 2018 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.32.3.416 on 1 May 1970. D
ownloaded from
Successful pregnancy in a patient with a homograft aortic valve 417
pressure 155140 mm. Hg. Aortic angiographyshowed a gross degree of aortic regurgitationthrough a wide central jet.
It was decided that aortic valve replacementwas indicated, and at operation 6 months later,the commissures of the aortic valve were foundto be widely separated, with shortening andthickening of the left coronary cusp. The valvewas excised and replaced by a 26 mm. salinepreserved homograft. On recovery from theoperation, it was noted she had a left bundle-branch block, and this electrocardiographicpattern has persisted. Otherwise her progresswas uneventful, and she was discharged fromhospital six weeks after operation. She still had asoft aortic diastolic murmur, with a very softejection systolic murmur, but no peripheral signsof aortic regurgitation. The brachial blood pres-sure was 130/90 mm. Hg, and radiographyshowed considerable diminution of the cardiacoutline.
Six months after operation, she married, andtwelve months later became pregnant. She hadbeen advised of the associated risks, but wasanxious to have a child. Seen in the twelfthweek of pregnancy, she was symptomless, andthere was no change in her cardiac signs or theelectrocardiogram. A transient rise in bloodpressure to I55/I05 mm. Hg settled with bed-rest and sedation and she was delivered of anormal healthy girl, weighing 3062 g. on 24March I969. Oral penicillin 250 mg. 6-hourly
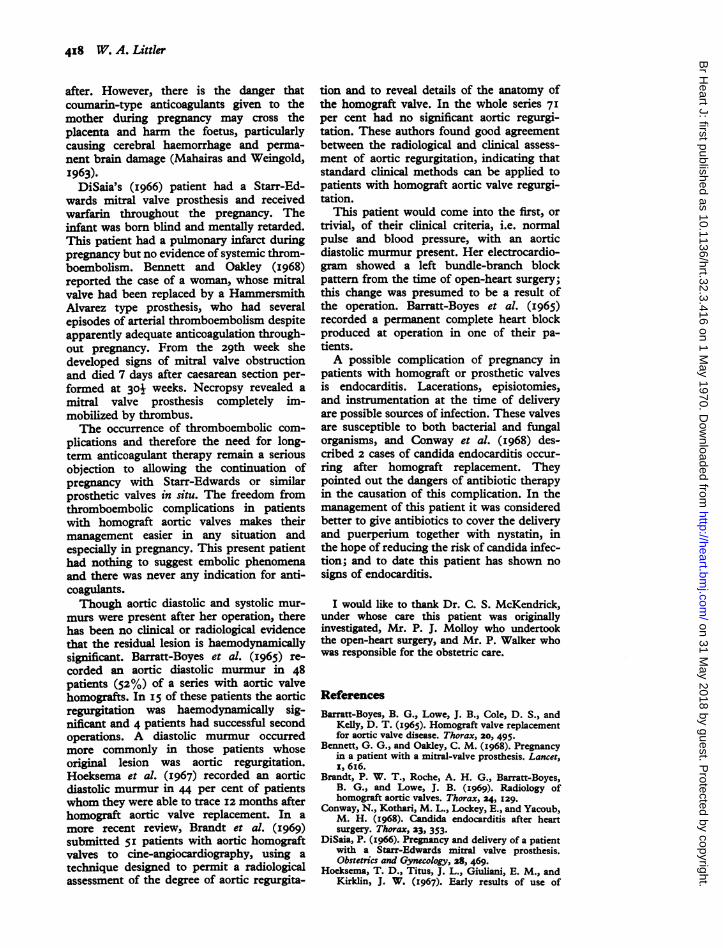
and nystatin 5oo,ooo units 8-hourly were givenat the onset of parturition, and continued for 4weeks. At no time did she need digitalis ordiuretics, and when seen 6 weeks after deliveryshe was well, with no change in the physicalsigns in the cardiovascular system, and with anunchanged electrocardiogram and radiograph(Fig. 3).
DiscussionExperience in the management of pregnantwomen with prosthetic and homograft heartvalves is still very limited. Published reportshave dealt with the behaviour of prostheticvalves during pregnancy, and the outcomehas been varied. Ueland, Tatum, and Met-calfe (I966) reported 2 patients with Starr-Edwards aortic valves who were delivered ofhealthy infants after uncomplicated preg-nancies. This successful outcome was alsothe experience of Turner and Kitchin (I968)in 2 patients with Starr-Edwards prostheses;in one case, of the mitral valve, and, in theother, of the aortic valve. Ueland et al. didnot use anticoagulants in their 2 cases, whileTurner and Kitchin treated both theirpatients with anticoagulants throughout preg-nancy, stopping the phenindione at the onsetof labour, and restarting it immediately
FIG. 2 Pre-operative chest radiograph FIG. 3 Chest radiograph 6 weeks after ashowing left ventricular enlargement. normal delivery showing left ventricular en-
largement and some dilatation of the aorticroot.
on 31 May 2018 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.32.3.416 on 1 May 1970. D
ownloaded from
418 W. A. Littler
after. However, there is the danger thatcoumarin-type anticoagulants given to themother during pregnancy may cross theplacenta and harm the foetus, particularlycausing cerebral haemorrhage and perma-nent brain damage (Mahairas and Weingold,I963).
DiSaia's (I966) patient had a Starr-Ed-wards mitral valve prosthesis and receivedwarfarin throughout the pregnancy. Theinfant was born blind and mentally retarded.This patient had a pulmonary infarct duringpregnancy but no evidence of systemic throm-boembolism. Bennett and Oakley (I968)reported the case of a woman, whose mitralvalve had been replaced by a HammersmithAlvarez type prosthesis, who had severalepisodes of arterial thromboembolism despiteapparently adequate anticoagulation through-out pregnancy. From the 29th week shedeveloped signs of mitral valve obstructionand died 7 days after caesarean section per-formed at 301 weeks. Necropsy revealed amitral valve prosthesis completely im-mobilized by thrombus.The occurrence of thromboembolic com-
plications and therefore the need for long-term anticoagulant therapy remain a seriousobjection to allowing the continuation ofpregnancy with Starr-Edwards or similarprosthetic valves in situ. The freedom fromthromboembolic complications in patientswith homograft aortic valves makes theirmanagement easier in any situation andespecially in pregnancy. This present patienthad nothing to suggest embolic phenomenaand there was never any indication for anti-coagulants.Though aortic diastolic and systolic mur-
murs were present after her operation, therehas been no clinical or radiological evidencethat the residual lesion is haemodynamicallysignificant. Barratt-Boyes et al. (I965) re-corded an aortic diastolic murmur in 48patients (52%) of a series with aortic valvehomografts. In I5 of these patients the aorticregurgitation was haemodynamically sig-nificant and 4 patients had successful secondoperations. A diastolic murmur occurredmore commonly in those patients whoseoriginal lesion was aortic regurgitation.Hoeksema et al. (I967) recorded an aorticdiastolic murmur in 44 per cent of patientswhom they were able to trace I2 months afterhomograft aortic valve replacement. In amore recent review, Brandt et al. (I969)submitted 5I patients with aortic homograftvalves to cine-angiocardiography, using atechnique designed to permit a radiologicalassessment of the degree of aortic regurgita-
tion and to reveal details of the anatomy ofthe homograft valve. In the whole series 7Iper cent had no significant aortic regurgi-tation. These authors found good agreementbetween the radiological and clinical assess-ment of aortic regurgitation, indicating thatstandard clinical methods can be applied topatients with homograft aortic valve regurgi-tation.
This patient would come into the first, ortrivial, of their clinical criteria, i.e. normalpulse and blood pressure, with an aorticdiastolic murmur present. Her electrocardio-gram showed a left bundle-branch blockpattern from the time of open-heart surgery;this change was presumed to be a result ofthe operation. Barratt-Boyes et al. (I965)recorded a permanent complete heart blockproduced at operation in one of their pa-tients.A possible complication of pregnancy in
patients with homograft or prosthetic valvesis endocarditis. Lacerations, episiotomies,and instrumentation at the time of deliveryare possible sources of infection. These valvesare susceptible to both bacterial and fungalorganisms, and Conway et al. (I968) des-cribed 2 cases of candida endocarditis occur-ring after homograft replacement. Theypointed out the dangers of antibiotic therapyin the causation of this complication. In themanagement of this patient it was consideredbetter to give antibiotics to cover the deliveryand puerperium together with nystatin, inthe hope of reducing the risk of candida infec-tion; and to date this patient has shown nosigns of endocarditis.
I would like to thank Dr. C. S. McKendrick,under whose care this patient was originallyinvestigated, Mr. P. J. Molloy who undertookthe open-heart surgery, and Mr. P. Walker whowas responsible for the obstetric care.
ReferencesBarratt-Boyes, B. G., Lowe, J. B., Cole, D. S., and
Kelly, D. T. (1965). Homograft valve replacementfor aortic valve disease. Thorax, 20, 495.
Bennett, G. G., and Oakley, C. M. (I968). Pregnancyin a patient with a mitral-valve prosthesis. Lancet,I, 6I6.
Brandt, P. W. T., Roche, A. H. G., Barratt-Boyes,B. G., and Lowe, J. B. (i969). Radiology ofhomograft aortic valves. Thorax, 24, 129.
Conway, N., Kothari, M. L., Lockey, E., and Yacoub,M. H. (I968). Candida endocarditis after heartsurgery. Thorax, 23, 353.
DiSaia, P. (I966). Pregnancy and delivery of a patientwith a Starr-Edwards mitral valve prosthesis.Obstetrics and Gynecology, 28, 469.
Hoeksema, T. D., Titus, J. L., Giuliani, E. M., andKirklin, J. W. (1967). Early results of use of
on 31 May 2018 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.32.3.416 on 1 May 1970. D
ownloaded from
Successful pregnancy in a patient with a homograft aortic valve 419
homografts for replacement of the aortic valve inman. Circulation, 35 Suppl. I, p. 9.
Mahairas, G. H., and Weingold, A. B. (I963). Fetalhazard with anticoagulant therapy. AmericanJ3ournal of Obstetrics and Gynecology, 8s, 234.
Turner, R. W. D., and Kitchin, A. H. (1968). Preg-nancy after mitral-valve prosthesis. Lancet, I, 862.
Ueland, K., Tatum, H. J., and Metcalfe, J. (I966).Pregnancy and prosthetic heart valves. Obstetricsand Gynecology, 27, 257.
10
on 31 May 2018 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.32.3.416 on 1 May 1970. D
ownloaded from