heart failure in childhood
TRANSCRIPT
HEART FAILURE IN CHILDHOOD
by Siti Sarah Nasution
1211356
CONTENTSPhysiology Definition
EpidemiologyEtiology
PathophysiologyClinical Features
InvestigationsManagement
Differential Diagnosis
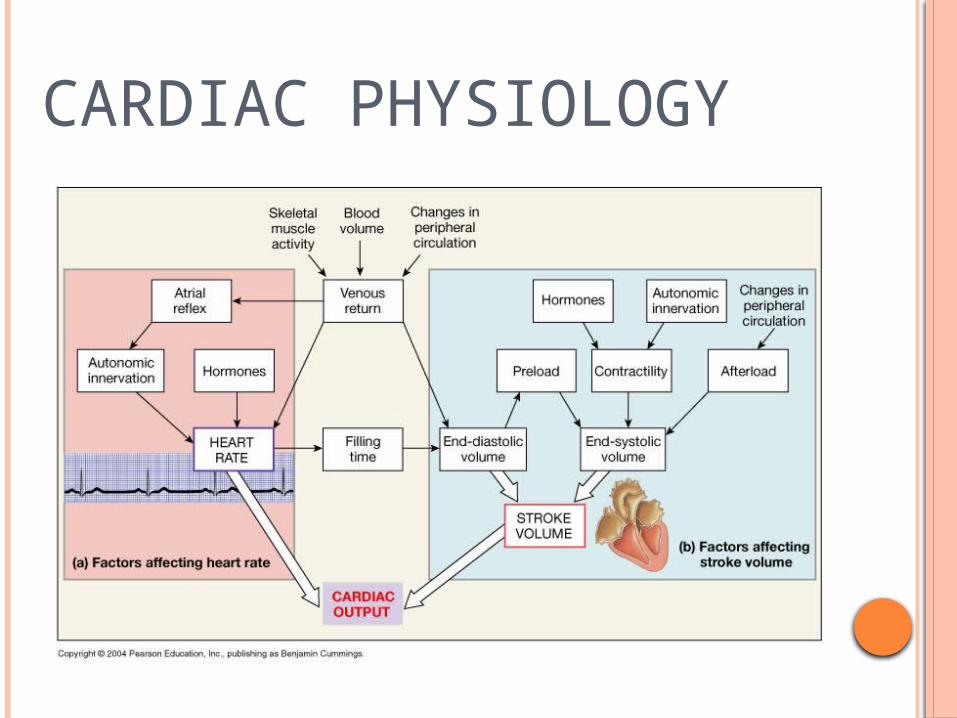
CARDIAC PHYSIOLOGY
CARDIAC PHYSIOLOGY
DEFINITIONHeart Failure occurs when the heart is unable to deliver adequate cardiac output to meet the metabolic needs of the body.
Nelson Textbook of Pediatrics, 19th Edition.
EPIDEMIOLOGY
CongenitalVSD
ASD
Aortic Stenosis
PDA
Coarctation of the Aorta
Cardiac Muscle RelatedRheumatic Heart DiseaseEndocarditisMyocarditis
OthersArrythmiaThyrotoxicosisAnemia Toxic drugs
Most common case of Heart Failure in Malaysia:(from Malaysian Pediatrics Association)
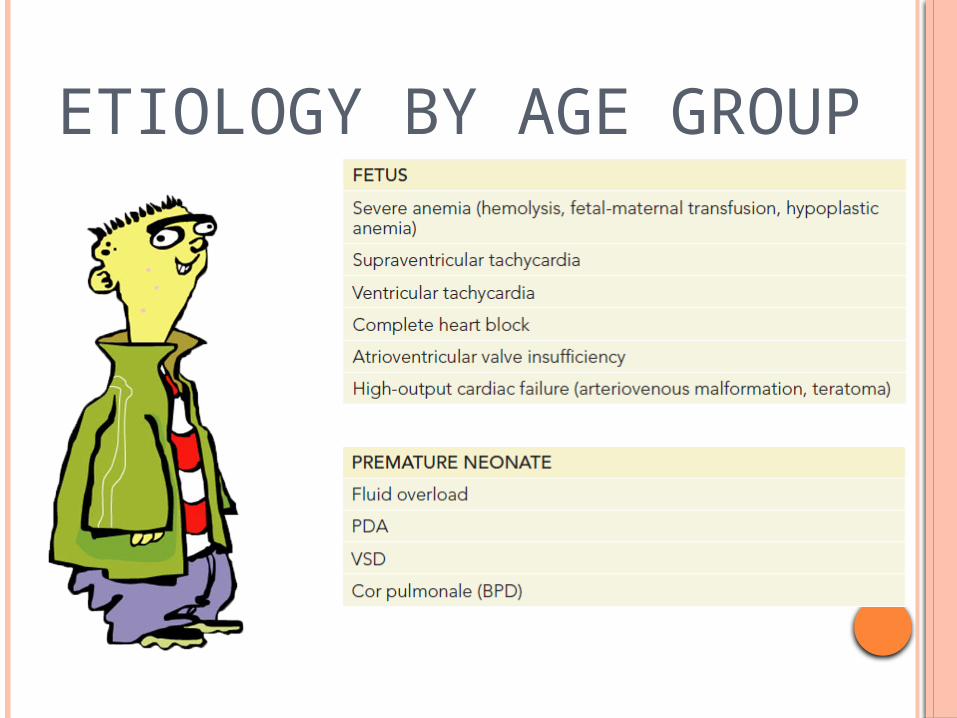
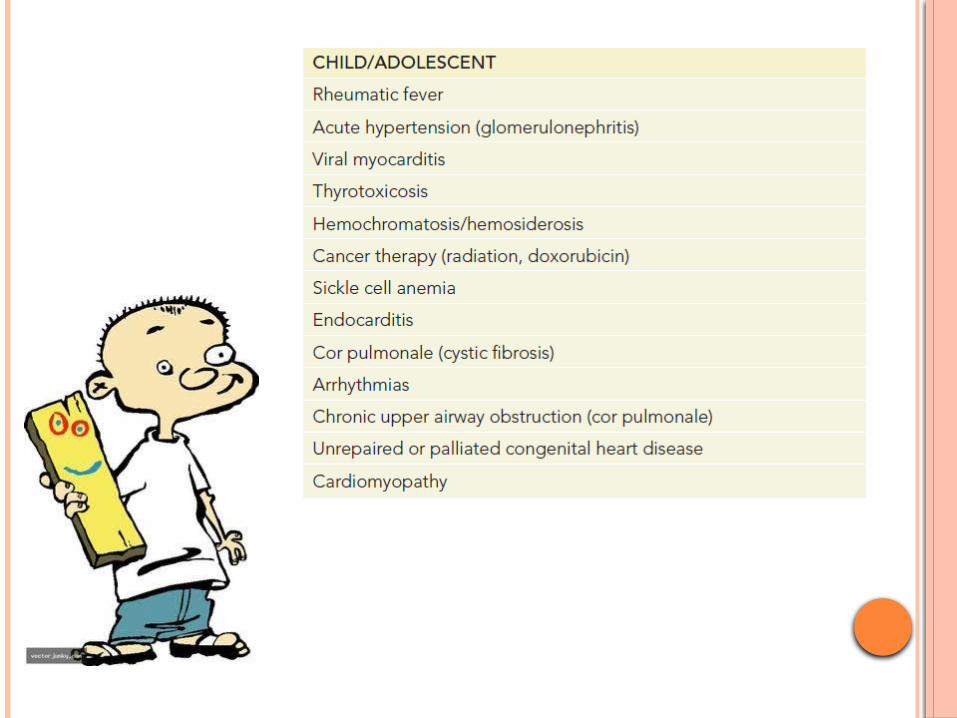
ETIOLOGY BY AGE GROUP


PATHOPHYSIOLOGY
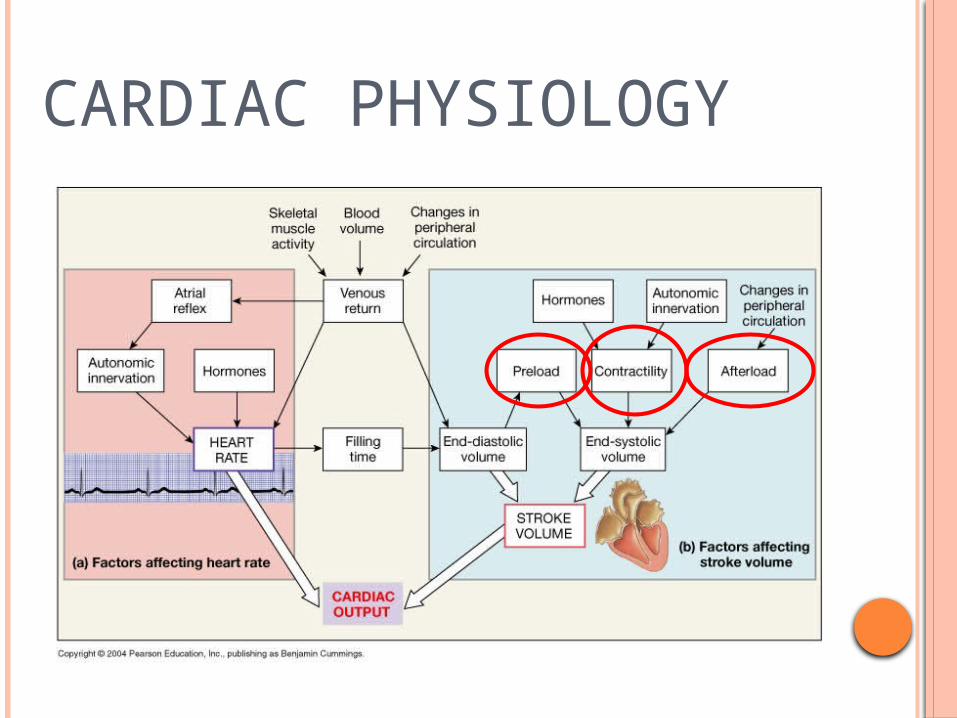
FACTORS AFFECTING CARDIAC PERFORMANCE:
Preload AfterloadContractility Heart Rate

AFTERLOAD VS PREALOAD PATHOLOGY
AfterloadObstruction
High Lt ventricle systolic pressure
Increase contractility sue to pressure overload.
Prolongation cause diminish cardiac contractility
HF
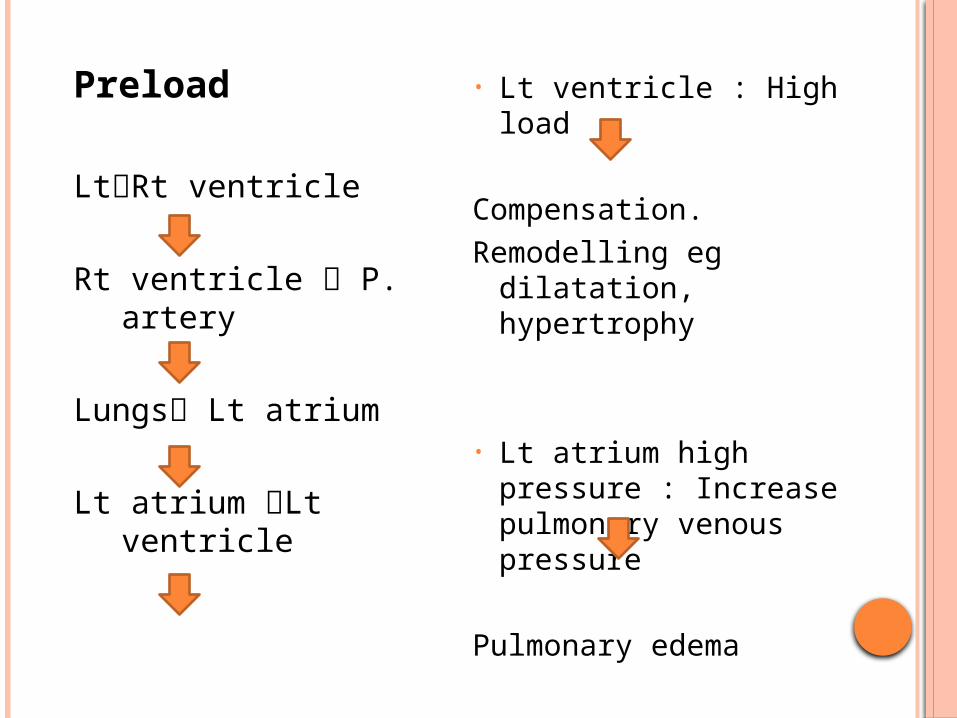
Preload
LtRt ventricle
Rt ventricle P. artery
Lungs Lt atrium
Lt atrium Lt ventricle
• Lt ventricle : High load
Compensation.Remodelling eg dilatation,
hypertrophy
• Lt atrium high pressure : Increase pulmonary venous pressure
Pulmonary edema

ABNORMAL LOADING CONDITIONS
Preload (Volume overload)
VSD PDA Valvular Insufficiency
*Most common cause in children.
Afterload(Pressure overload)
• Aortic Stenosis• Pulmonary
Stenosis• Coarctation of
the Aorta
Contractility :
Normal : Frank-Starling Law – is the ability of the heart to
change force of contraction dependent on the change of preload.
HF: Myocardium abnormalities either congenital or acquired.
(Intrinsic contractility compromised). Eg: myocarditis,
cardiomyopathy, muscular dystrophy.
Heart Rate :
Eg: Tachyarrythmias shortens the diastolic time interval for
ventricular filling. Also affect the time for coronary perfusion.
LEFT, RIGHT AND BIVENTRICULAR HEART FAILURE
1. Left-sided heart failure.
Reduce left ventricular output. High pressure in left atrial, pulmonary vein. Pulmonary congestion.
2. Right-sided heart failure.
Reduce right ventricular output, for any given right atrium pressure. Eg. Chronic lung disease.
3. Biventricular heart failure.
Secondary to the progression of the disease. Eg. Dilated cardiomyopathy, ischemic heart disease.
Heart fails to keep pace with the hemodynamic demands.
Decrease myocardial performance. Myocardium metabolic demand unmet.
Compensatory mechanism take place.
Initially compensated, at the end become decompensated.
Functional and structural disturbance of the heart
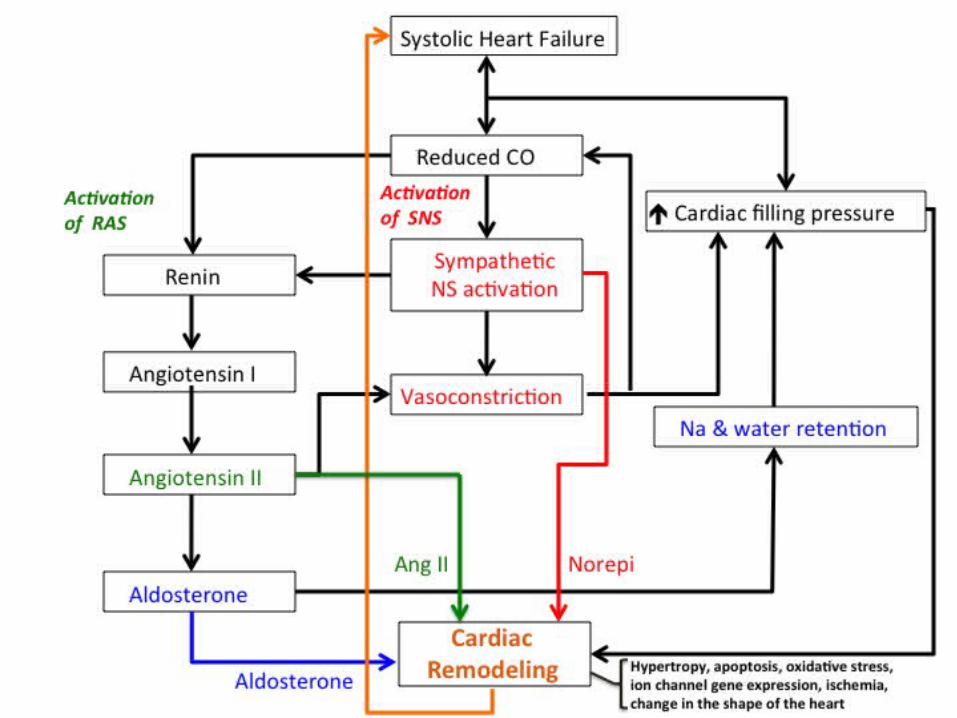
COMPENSATORY MECHANISM
1. Frank-Starling Mechanism
2. Neurohormonal System Activation - RAAS - Symphatoadrenal Axis
3. Myocardium Structural Changes - Hypertrophy, apoptosis etc.
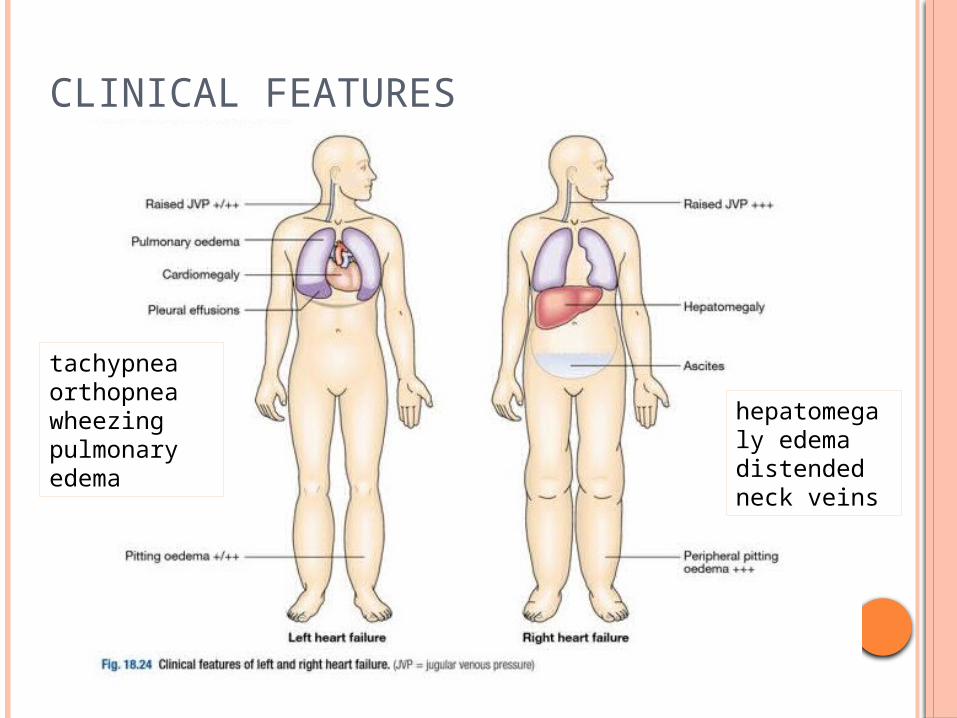
CLINICAL FEATURES
tachypnea orthopnea wheezingpulmonary edema
hepatomegaly edema distendedneck veins

Sign and Symptoms in Infancy
Symptoms Feeding difficulty : poor suck, prolonged time to feed,
sweating during feeding Recurrent chest infections Failure to thrive
Sign Resting tachypnoea, subcostal recession Tachycardia, poor peripheral pulses, poor peripheral perfusion Hyperactive praecordium, praecordial bulge Hepatomegaly Wheezing

In children, the sign and symptoms may be similar with adults.
• Fatigue• Effort intolerance• Anorexia• Abdominal pain• Dyspnea• Orthopnea• Cough• Edema (dependent part of body)• Cardiomegaly• JVP raised
Common sign of heart failure in adults eg.
Increase jugular venous pressure, Leg edema, Basal crackles
Are NOT usually found in chlidren.
INVESTIGATION
Chest X-ray -cardiomegaly-pulmonary edema
ECG-chamber hypertrophy-assess the cause of HF (Not diagnosis)-evaluate rhythm disorder- QRS morphologic n ST-T wave abnormalities
= myocardial inflammatory ds n pericardiatis
Echocardiography-assess ventricular function-parameter : Children – fractional shortening Adult – ejection fraction
Doppler Ultrasound-estimate CO-Assess cardiac function, wall motion abnormalities
MRA (Magnetic Resonance Angiography)
-Lt Rt ventricle: function, volume, mass.

Serum B-type Natriuretic Peptide (BNP)
-cardiac neurohormone released in response to increased ventricular wall tension
-Increase in: Adult : CHF Children : HF (systolic dysfunction) & volume
overload (Lt-Rt shunt)
Arterial Blood gases
-pH, PaO2, PaCO2 abnormalities checking.

Right sided Heart FailureCardiomegaly

TREATMENT
AimEnhancing cardiac contractilityReducing the preload & afterloadImproving oxygen delivery
General
O2 supplement, in a propped up position Strict bed rest rarely necessary Keep warm n gentle handling Fluid restriction (3/4 normal) only if not dehydrated or in
shock Correct the anemia, electrolyte imbalance, treat concomitant
chest infection
ANTI-FAILURE MEDICATION
Frusemide •loop diuretic, •use with potassium supplement or together with potassium sparing diuretics
Spironolactone •potassium sparing diuretic•modest diuretic effect

Captopril •ACE inhibitor•Afterload reducing agent
Digoxin Useful in:excessive tachycardia supraventricular tachyarrhythmias
IV Inotropic agents•Use for high force contraction• Acute HF•Cardiogenic shock•Post low output syndrome
SPECIFIC MANAGEMENT
Etiology establishment Specific treatment for targeted etiology Congenital - Surgical or transcatheter
treatment Heart block - Pacemaker Post infectious glomerulonephritis - Control
BP Acute rheumatic carditis - High dose aspirin
DIFFERENTIAL DIAGNOSIS Acute Renal Failure Acute Respiratory Distress Syndrome Cirrhosis Emphysema Nephrotic Syndrome Pneumonia Pulmonary Edema
REFERENCES
Nelson Textbook of Paediatrics, 19th edition. Nelson Essentials of Paediatrics, 7th edition. Paediatric Protocols for Malaysian Hospitals,
3rd edition. Davidson’s Principles and Practice of
Medicine, 21st edition.