healthy outcomes paediatric program for scarborough (hopps ... · healthy outcomes paediatric...
TRANSCRIPT
Healthy Outcomes Paediatric Program for Scarborough | Phone: 647-461-7030 | Fax: 416-284-3168 | [email protected] Central Booking Office: Galaxy 12 Child & Teen Clinic, Scarborough and Rouge Hospital – Centenary Site,
2867 Ellesmere Road, Scarborough, ON, M1E 4B9
www.rougevalley.ca/hopps | www.tsh.to/hopps
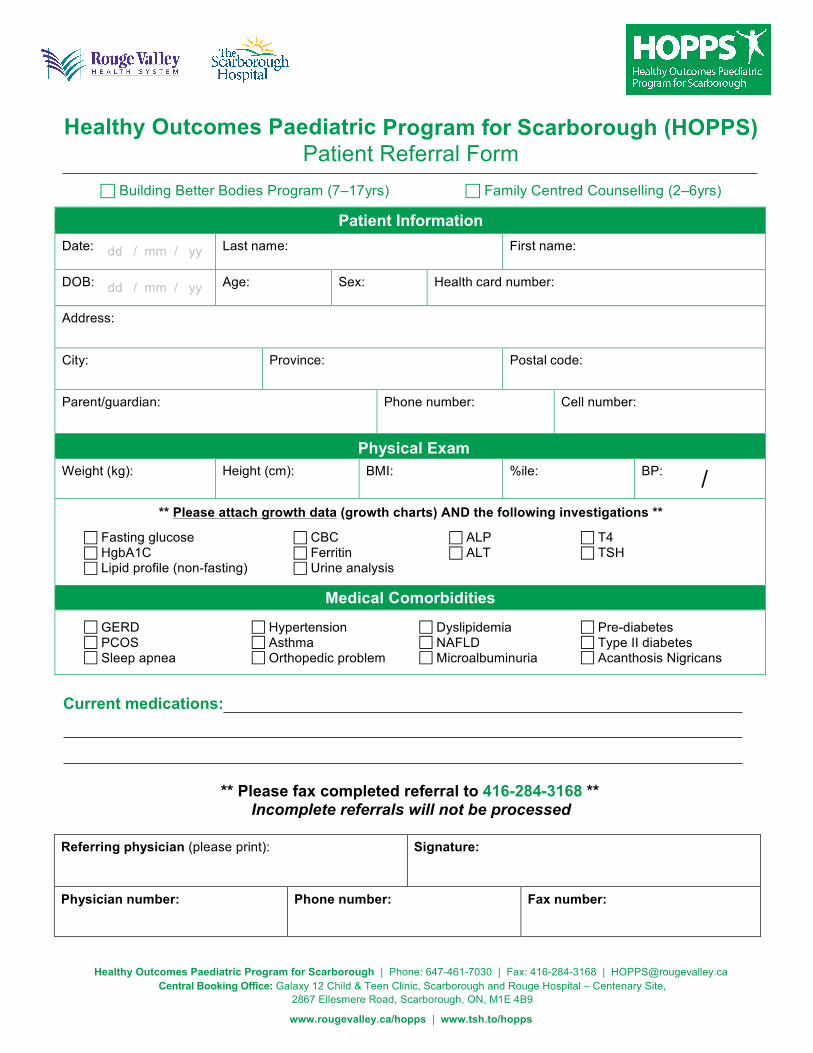
Healthy Outcomes Paediatric Program for Scarborough (HOPPS) Patient Referral Form
Building Better Bodies Program (7–17yrs) Family Centred Counselling (2–6yrs)
Patient Information Date: Last name: First name:
DOB: Age: Sex: Health card number:
Address:
City: Province: Postal code:
Parent/guardian: Phone number: Cell number:
Physical Exam Weight (kg): Height (cm): BMI: %ile: BP:
** Please attach growth data (growth charts) AND the following investigations **
Fasting glucose CBC ALP T4 HgbA1C Ferritin ALT TSH Lipid profile (non-fasting) Urine analysis
Medical Comorbidities
GERD Hypertension Dyslipidemia Pre-diabetes PCOS Asthma NAFLD Type II diabetes Sleep apnea Orthopedic problem Microalbuminuria Acanthosis Nigricans
Current medications:
** Please fax completed referral to 416-284-3168 ** Incomplete referrals will not be processed
Referring physician (please print): Signature:
Physician number: Phone number: Fax number:
dd / mm / yy
dd / mm / yy
/