headaches, headaches and more headaches. diagnostic ... nov 1630 stocks…dural venous sinus...
TRANSCRIPT
Headaches, headaches and more headaches! Diagnostic dilemmas; looking beyond
PDPH
Dr Gary Stocks
Queen Charlotte’s & Chelsea Hospital Imperial College Healthcare NHS Trust
OAA 3 day course Nov 2012
Case report
• Primip 20 yr old
• One migraine in past
• Requesting epidural
Case report
• Dural Puncture
Case report
• Primip 20 yr old
• One migraine in past
• Requesting epidural
• Dural Puncture
• Epidural resited
• SVD
Day 2 postpartum
• Headache occurs
– Postural
– Occipital
– Neck pain
• Diagnosis: PDPH
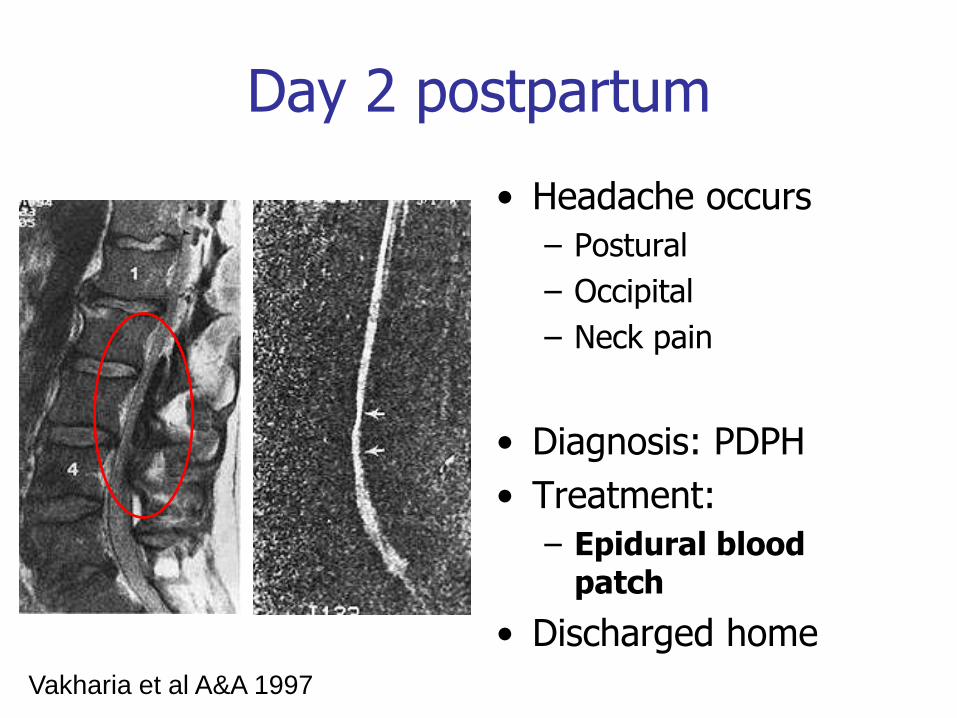
Day 2 postpartum
• Headache occurs
– Postural
– Occipital
– Neck pain
• Diagnosis: PDPH
• Treatment:
– Epidural blood patch
• Discharged home
Vakharia et al A&A 1997
Day 3 postpartum
Headache returns!
Now what?
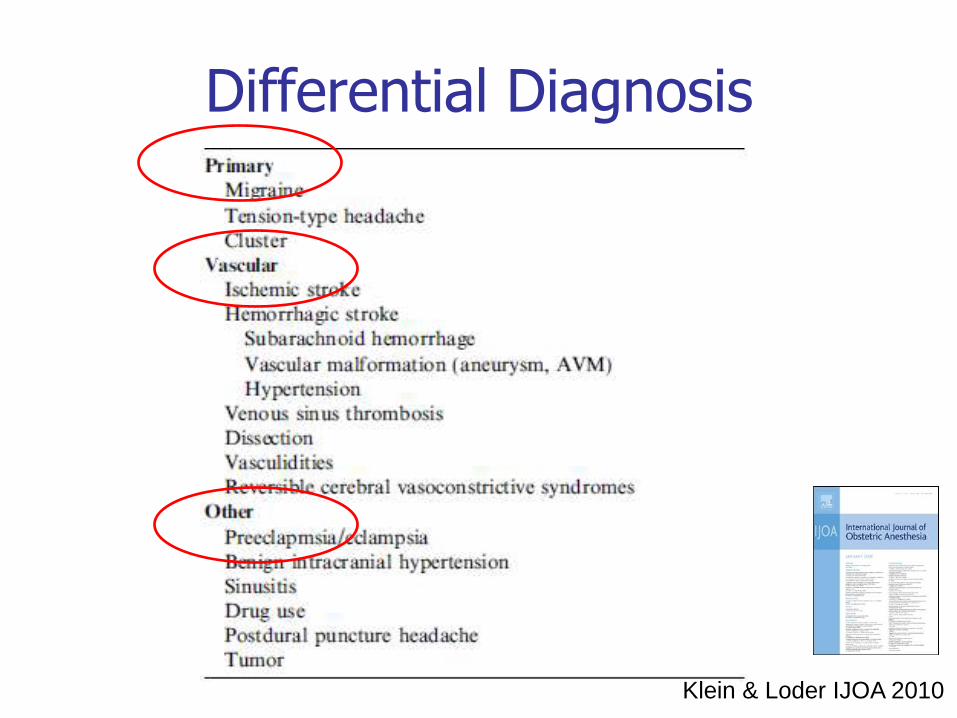
Differential Diagnosis
Klein & Loder IJOA 2010
Incidence
• Goldszmidt, Can J Anaesth 2005
– 985 women 39% headache
– Tension/migraine 20x > PDPH
– 4% debilitating
– Risk factors
• Dural puncture
• Previous headache history
• Multiparity
• maternal age
Primary headache
Tension Migraine
Cluster headache
Migraine
• Precipitated post natally – Falling oestrogen levels
– Sleep disturbance
– Emotional stress
Migraine
• Precipitated post natally – Falling oestrogen levels
– Sleep disturbance
– Emotional stress
• Symptoms – International Classification for Headache Disorders
– Severe, throbbing
– Often unilateral
– Nausea, vomiting, photophobia
Migraine
• Precipitated post natally – Falling oestrogen levels
– Sleep disturbance
– Emotional stress
• Symptoms – International Classification for Headache Disorders
– Severe, throbbing
– Often unilateral
– Nausea, vomiting, photophobia
• Relieved by – Rest
– Sumatripan
– Ergotamine
Primary Headaches
Key points to remember
Migraine flares up after delivery
Migraine is associated with secondary causes
New primary headache is a concern
Low threshold for further evaluation
Back to the case report
• Headache returns
• Failed EBP
• Not Primary headache
• ?
Pre-eclampsia
• BP
• Proteinuria
• Visual disturbances
• reflexes
• urate
• liver enzymes/coagulopathy
Postpartum:
• Readmitted to hospital
• 2nd epidural blood patch: 20ml
• Successfully resolved all symptoms
• Discharged home
Returns again!
• Persistent occipital headache
• Intermittent / throbbing
• Non-postural
• Increasing sedation/confusion
Postpartum

Red flag headache features
• New neurology
• Change in character
• New headache-unilateral
• Vomiting
• Change in mental status
• Unrelieved by analgesics

Red flag headache features
• New neurology
• Change in character
• New headache-unilateral
• Vomiting
• Change in mental status
• Unrelieved by analgesics
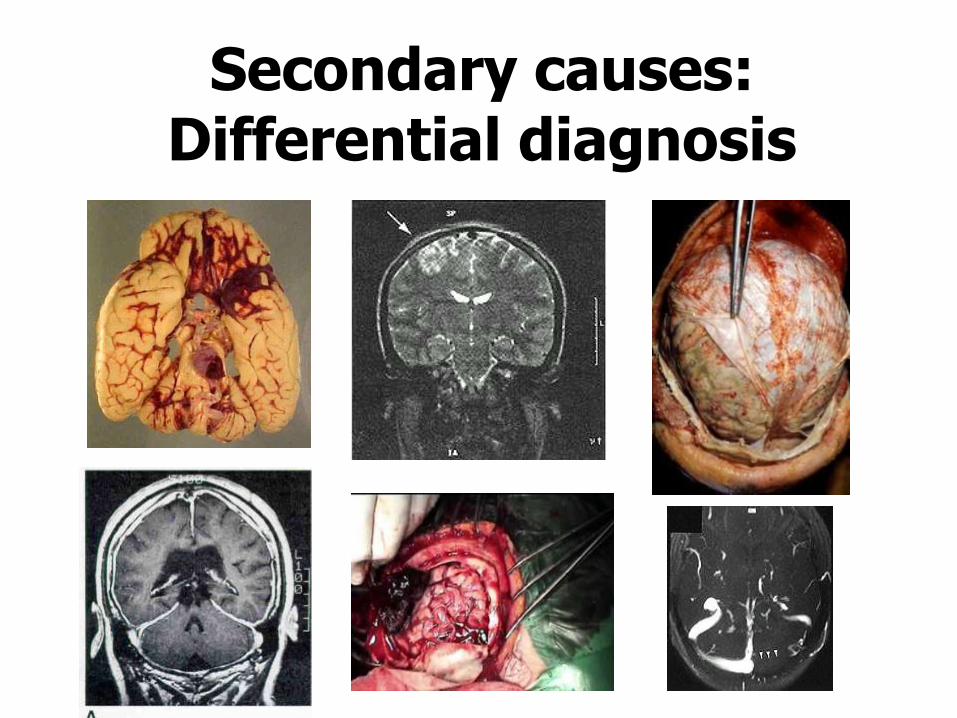
Secondary causes: Differential diagnosis
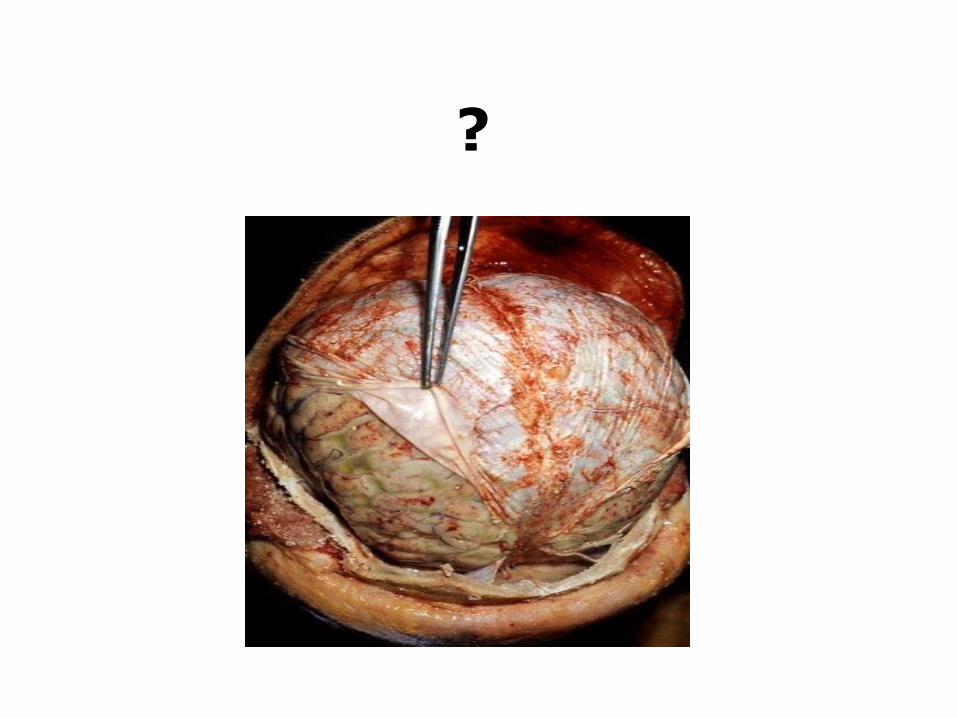
?
Meningitis: 1:10000 - 1:50000
• Fever
• Nausea & vomiting
• Neck stiffness
• WCC
• CSF glucose
• LP > microorganisms
Meningitis: prevention
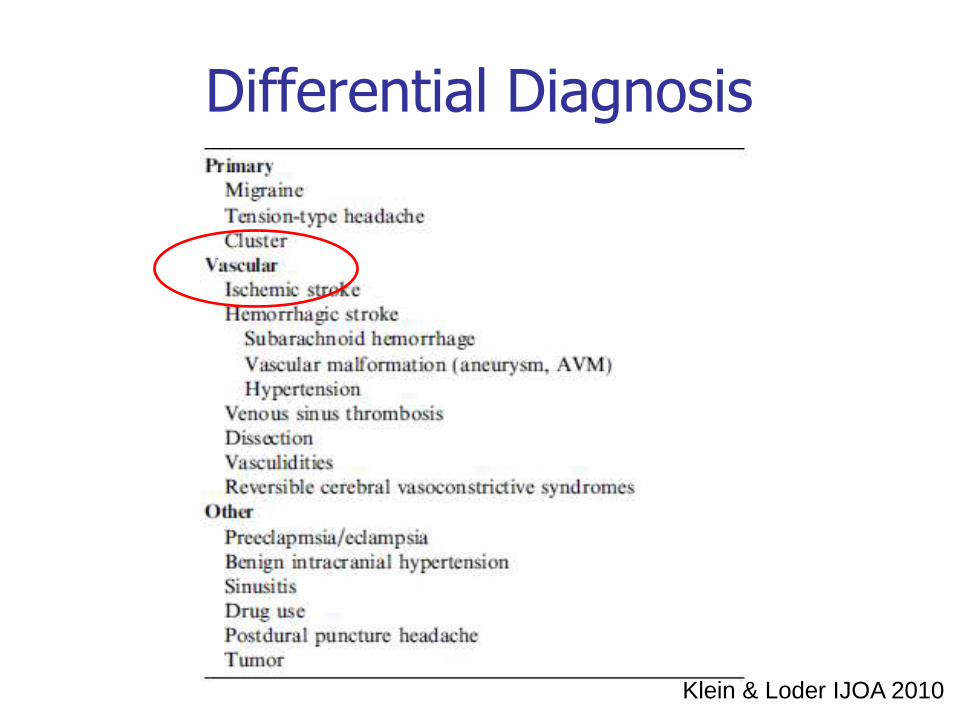
Differential Diagnosis
Klein & Loder IJOA 2010
Postpartum stroke
• Incidence
– 4.3-210/100 000
– 3rd trimester/postpartum
• Aetiology
– Hypercoaguability
– ↑ oestrogen→vasodilation
and vessel rupture
Classification of stroke
1. Ischaemic emboli
2. Venous sinus thrombosis
3. Pre-eclampsia/eclampsia
Only 10% stroke patients get headache
Ischaemic
Haemorrhagic
Thrombotic
?
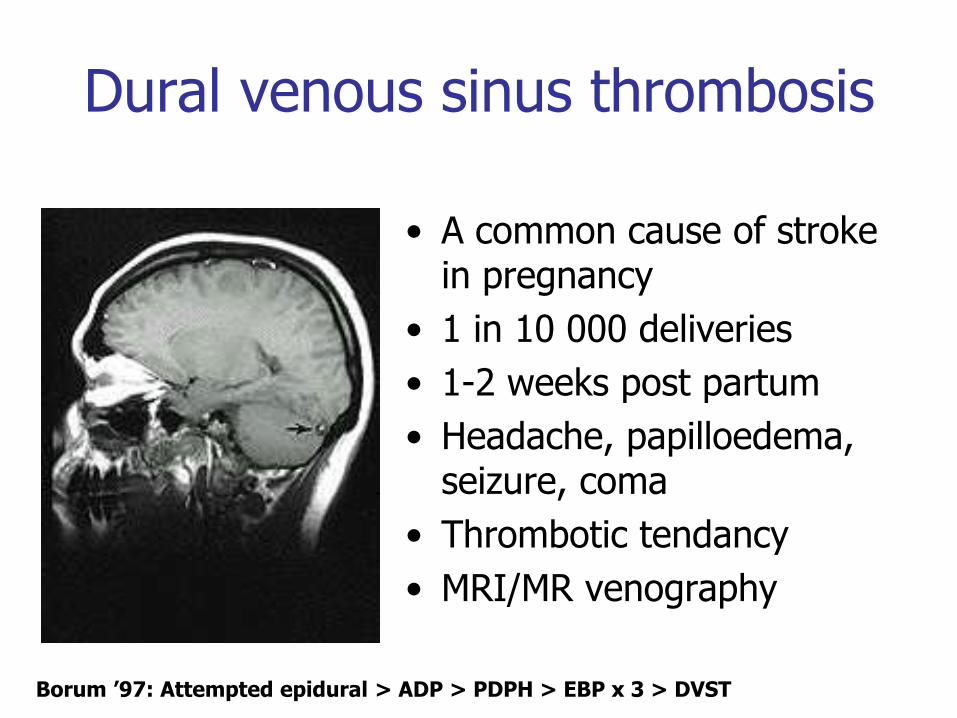
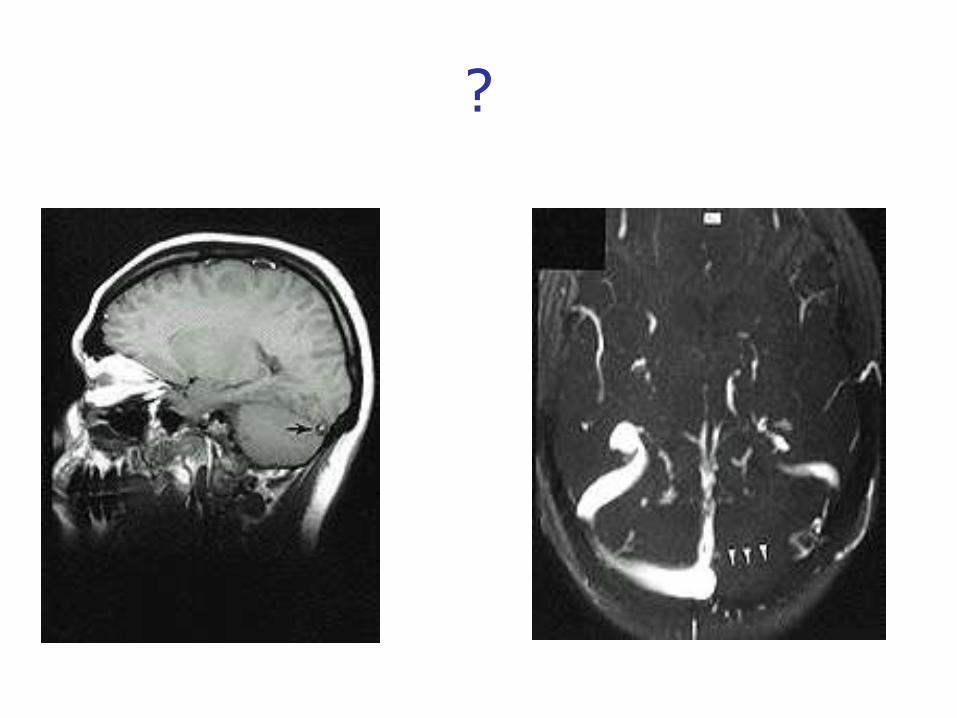
Dural venous sinus thrombosis
• A common cause of stroke in pregnancy
• 1 in 10 000 deliveries
• 1-2 weeks post partum
• Headache, papilloedema, seizure, coma
• Thrombotic tendancy
• MRI/MR venography
Borum ’97: Attempted epidural > ADP > PDPH > EBP x 3 > DVST
?
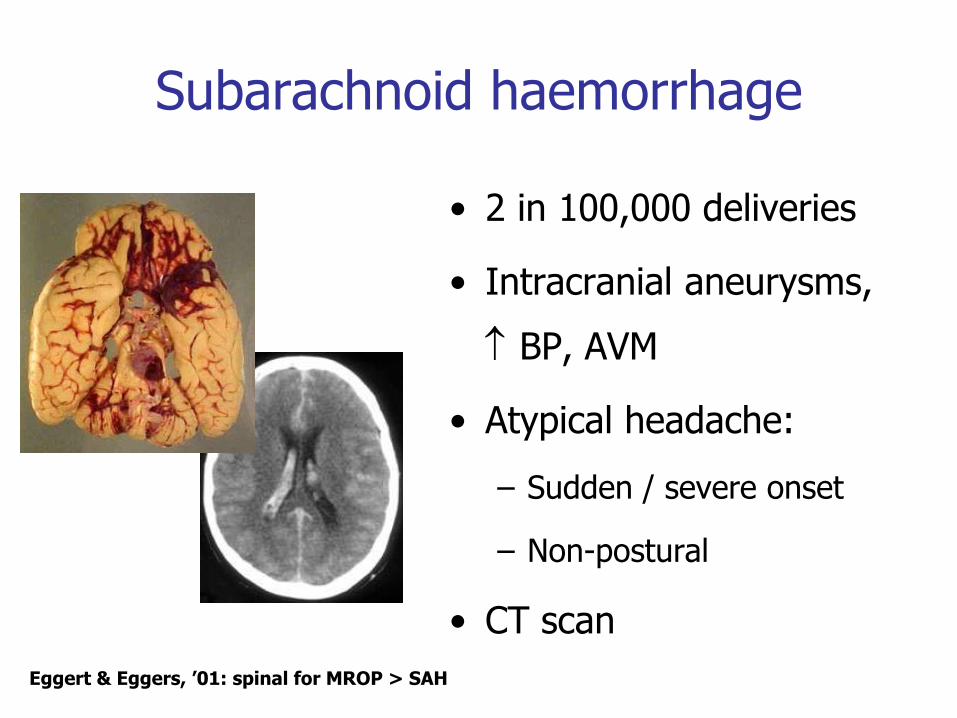
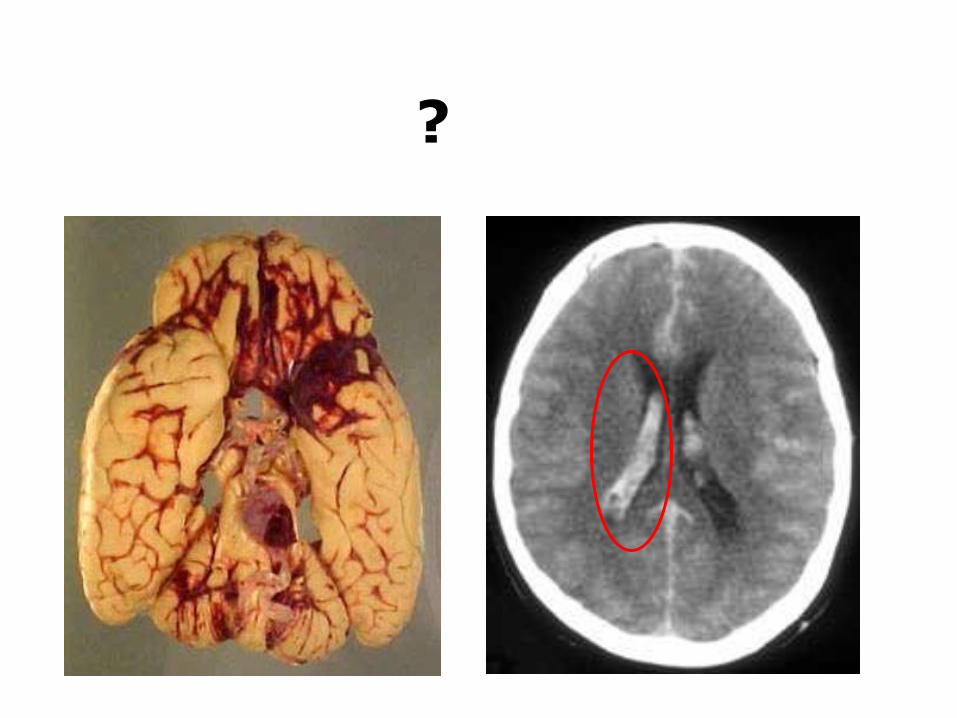
Subarachnoid haemorrhage
• 2 in 100,000 deliveries
• Intracranial aneurysms,
BP, AVM
• Atypical headache:
– Sudden / severe onset
– Non-postural
• CT scan
Eggert & Eggers, ’01: spinal for MROP > SAH
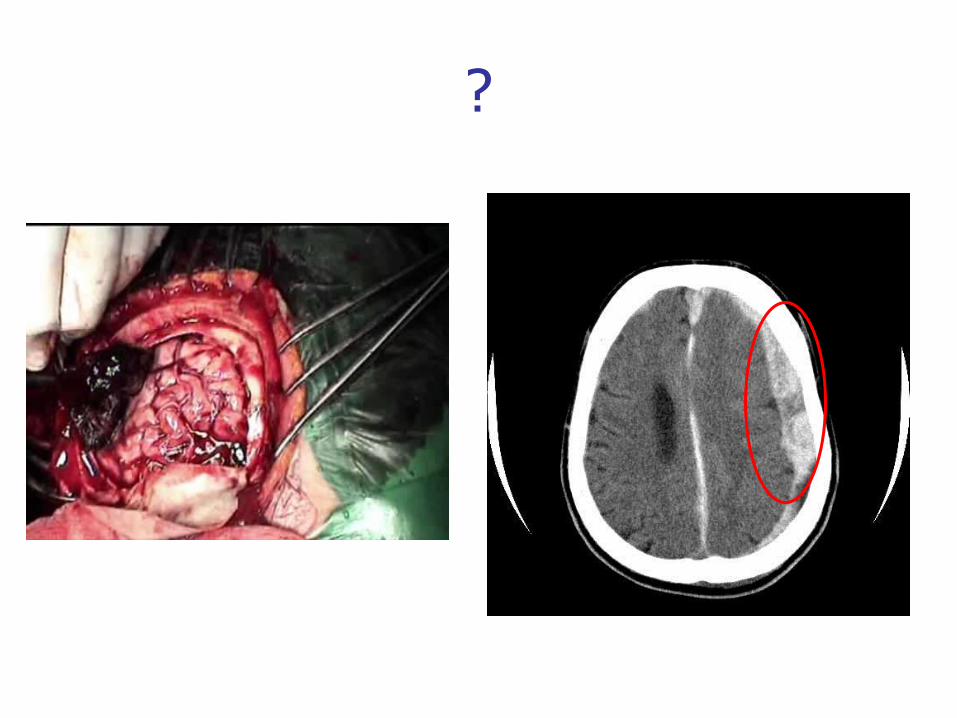
?
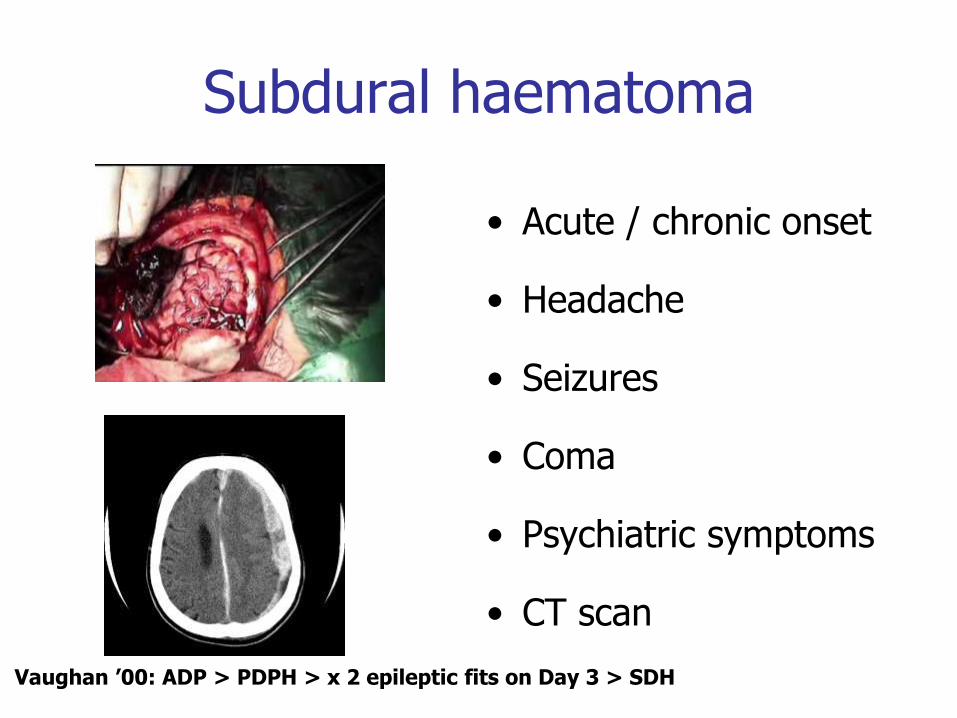
Subdural haematoma
• Acute / chronic onset
• Headache
• Seizures
• Coma
• Psychiatric symptoms
• CT scan
Vaughan ’00: ADP > PDPH > x 2 epileptic fits on Day 3 > SDH
Reversible cerebral vasoconstriction syndrome (RCVS)
• Described in 2007
• Severe headache ± neurology
• Cerebral artery constriction
• Resolves 1-3 months
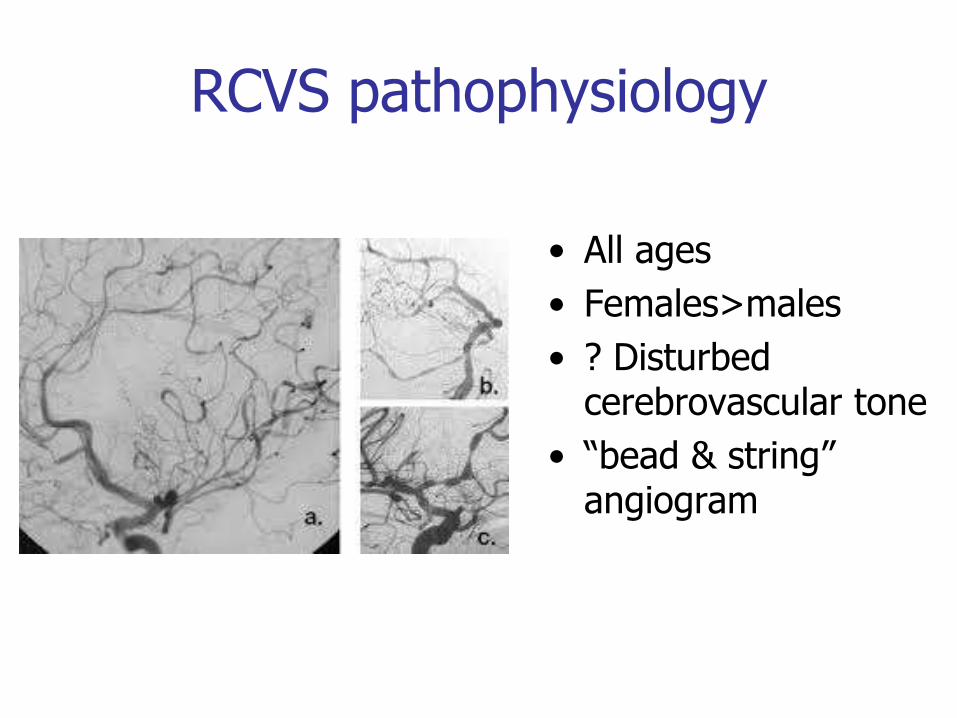
RCVS pathophysiology
• All ages
• Females>males
• ? Disturbed cerebrovascular tone
• “bead & string” angiogram
RCVS aetiology
• Idiopathic but 25-60% are exposed to vasoactive substances or postpartum
• In postpartum 50-70% have had vasoconstrictors for PPH
RCVS Thunderclap headache
• Sudden onset
• Like SAH
• Major complications
– Ischaemic or haemorrhagic stroke
• Diagnosis
– CT –tive SAH
– Normal LP
– Cerebral angiogram
Case report: Headache back!
• Persistent occipital headache
• Intermittent / throbbing
• Non-postural
• Increasing sedation/confusion
Postpartum
Neurology opinion
• Migraine
• Analgesics / fluids
Postpartum: Day 5 (night)
• 4 Grand Mal seizures
Portrait of a Man After a Grand Mal Seizure
Postpartum: Day 5 (night)
• 4 Grand Mal seizures
• Treatment
– Diazepam & phenytoin
• On examination
– No focal neurology
– No papilloedema
– No hypertension
– Normal bloods
• CT/MRI
Portrait of a Man After a Grand Mal Seizure
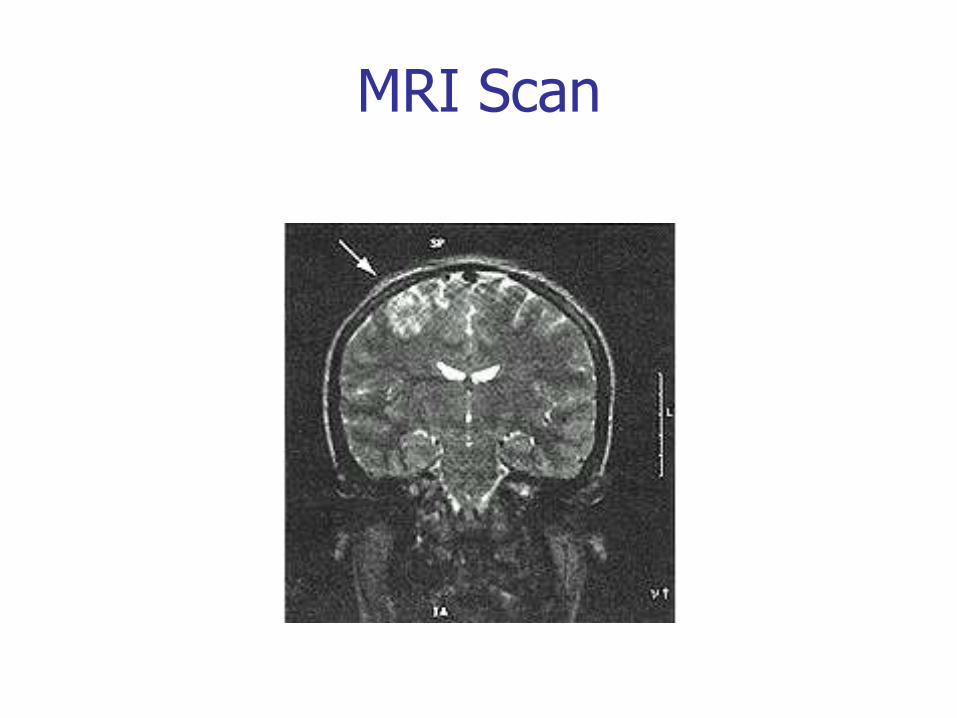
MRI Scan
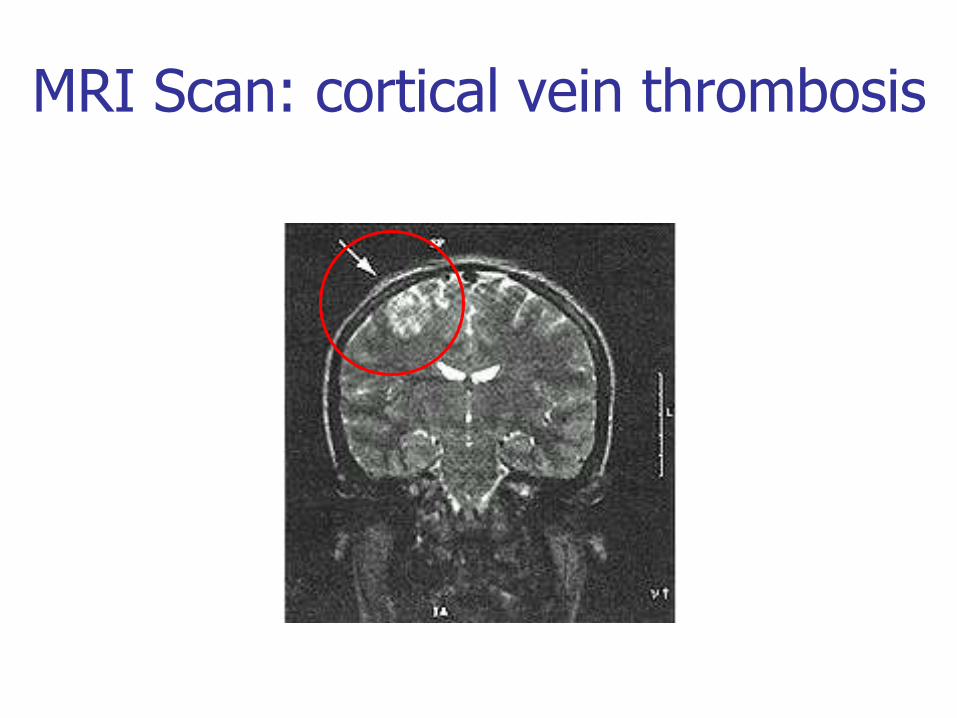
MRI Scan: cortical vein thrombosis
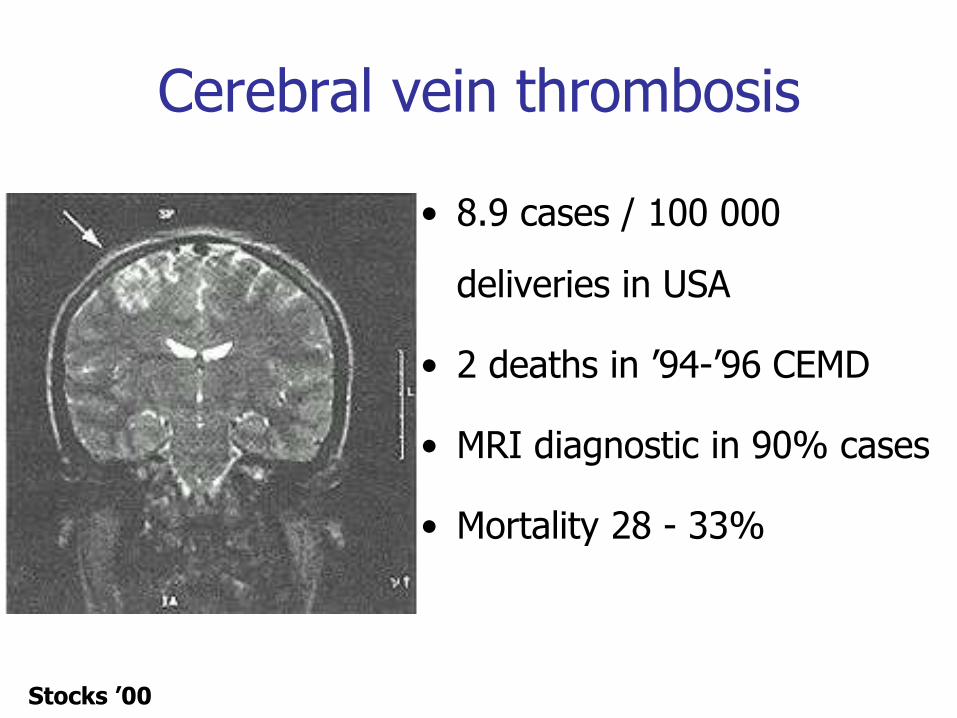
Cerebral vein thrombosis
• 8.9 cases / 100 000
deliveries in USA
• 2 deaths in ’94-’96 CEMD
• MRI diagnostic in 90% cases
• Mortality 28 - 33%
Stocks ’00
Cerebral Vein Thrombosis
• Headache/papilloedema
• Seizures/hemiplegia
• Coma
• Thrombotic tendency
– Pregnancy
– Protein C, S
• MRI
Further Management
• Transferred to neurology unit
• Lumbar puncture:- xanthochromia
• Coagulant screen:- normal
• NOT anticoagulated
• Full recovery
• Avoid oral contraceptives
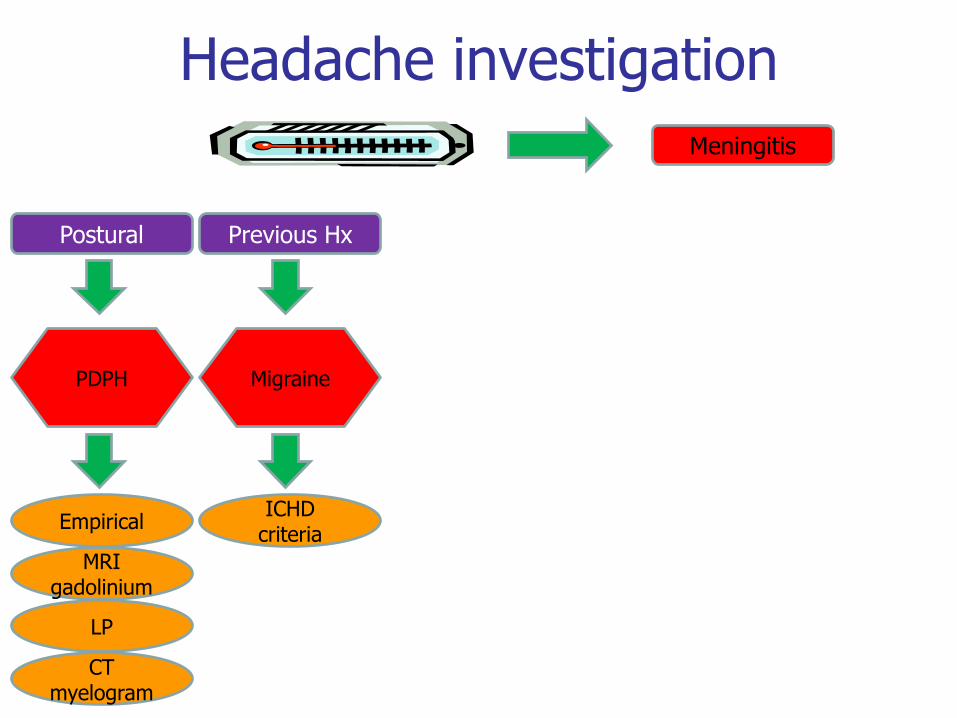
Headache investigation
Headache investigation
Meningitis
Headache investigation
Postural
Meningitis
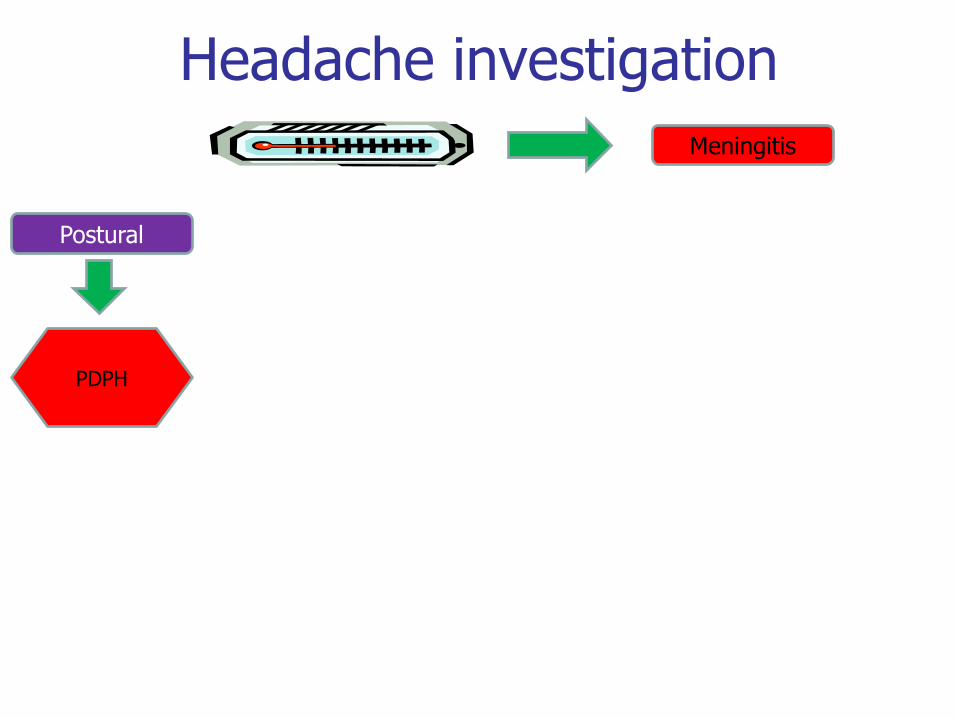
Headache investigation
Postural
PDPH
Meningitis
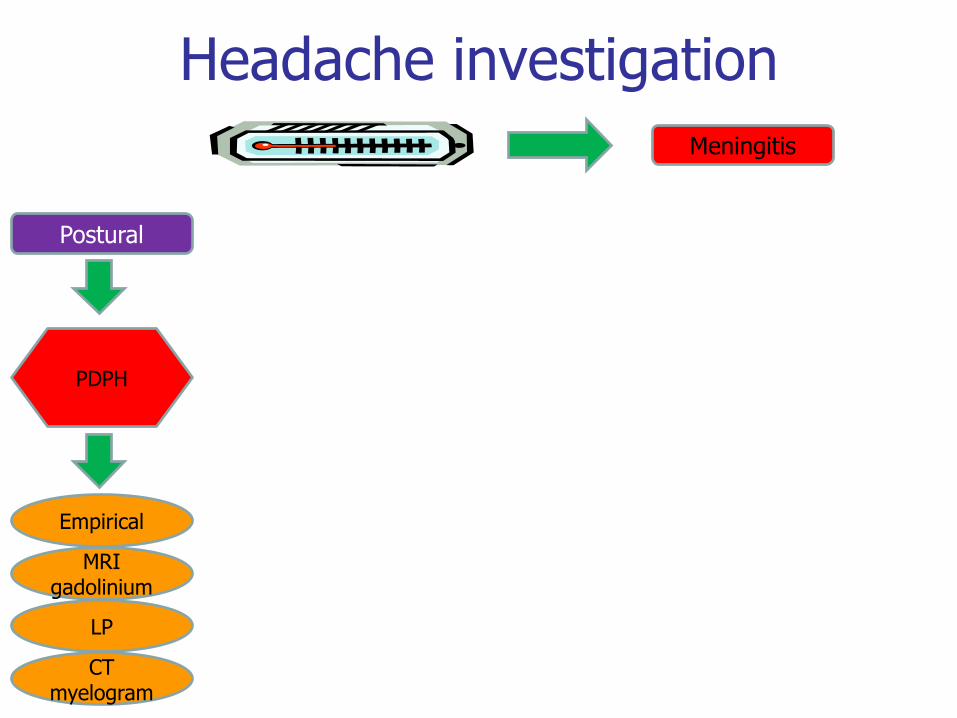
Headache investigation
Postural
PDPH
Empirical
MRI gadolinium
LP
CT myelogram
Meningitis
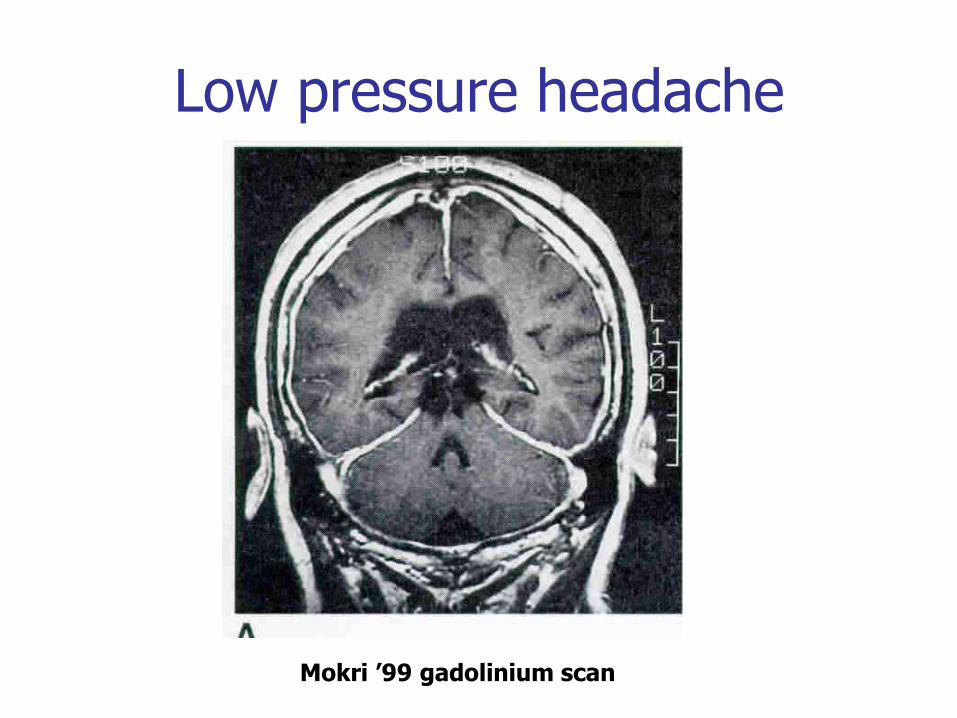
Low pressure headache
Mokri ’99 gadolinium scan
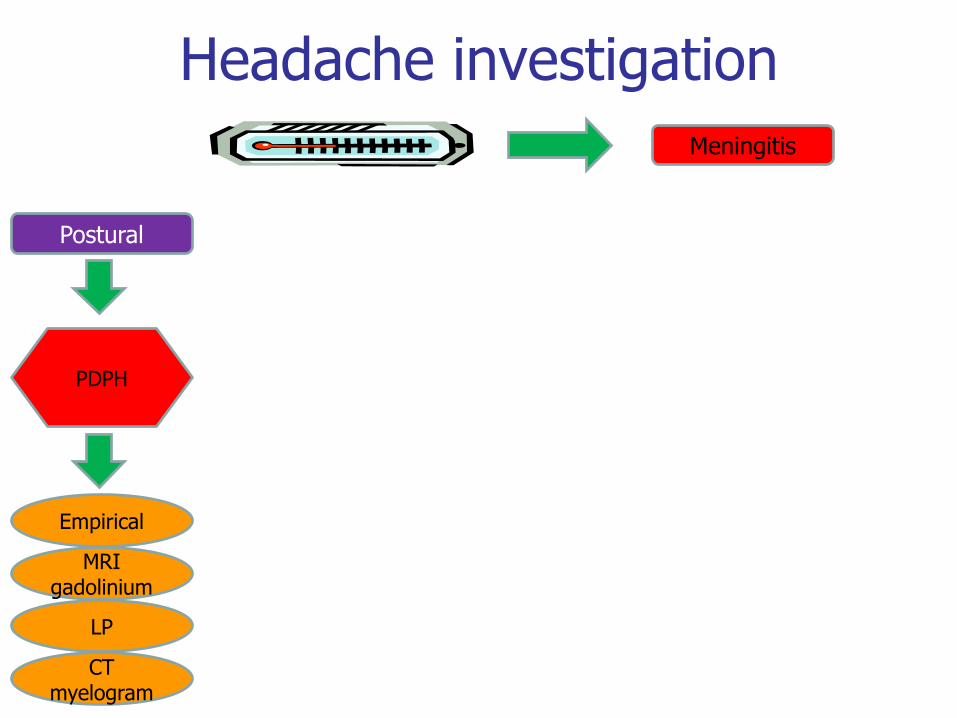
Headache investigation
Postural
PDPH
Empirical
MRI gadolinium
LP
CT myelogram
Meningitis
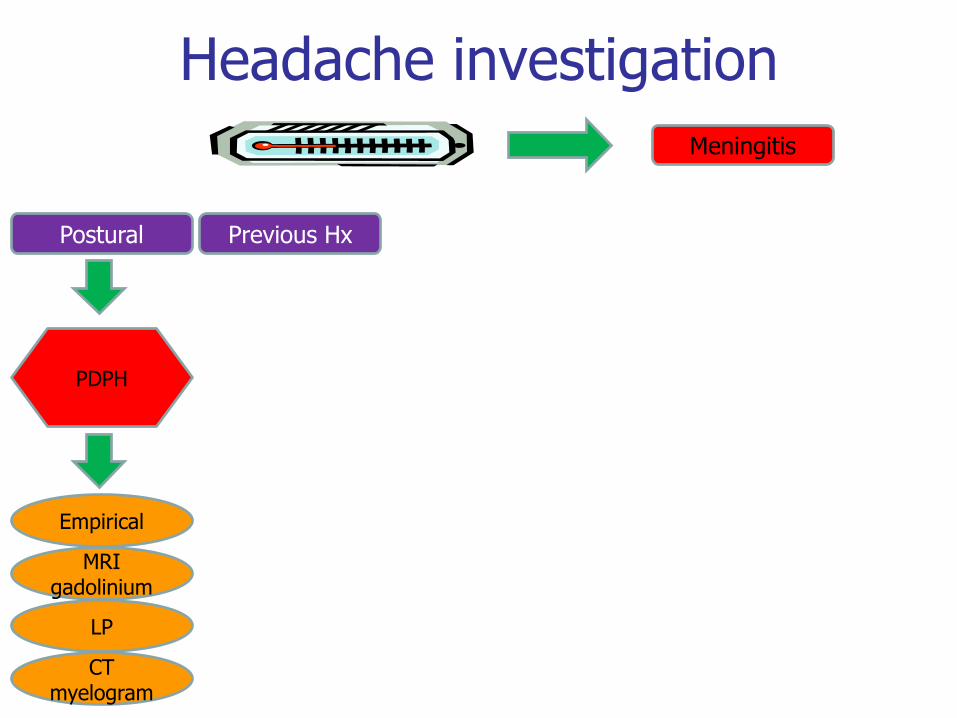
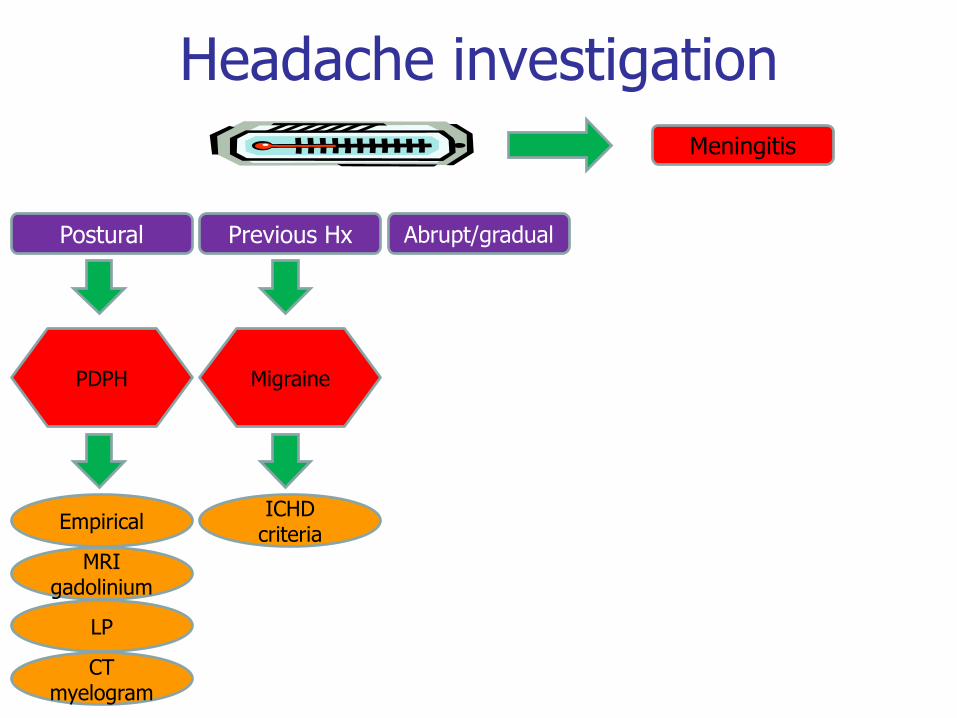
Headache investigation
Postural Previous Hx
PDPH
Empirical
MRI gadolinium
LP
CT myelogram
Meningitis
Headache investigation
Postural Previous Hx
PDPH
Empirical
MRI gadolinium
LP
CT myelogram
Migraine
ICHD criteria
Meningitis
Headache investigation
Postural Previous Hx Abrupt/gradual
PDPH
Empirical
MRI gadolinium
LP
CT myelogram
Migraine
ICHD criteria
Meningitis

Headache investigation
Postural Previous Hx Abrupt/gradual
PDPH
Empirical
MRI gadolinium
LP
CT myelogram
Migraine
ICHD criteria
CVT SAH RCVS
Meningitis
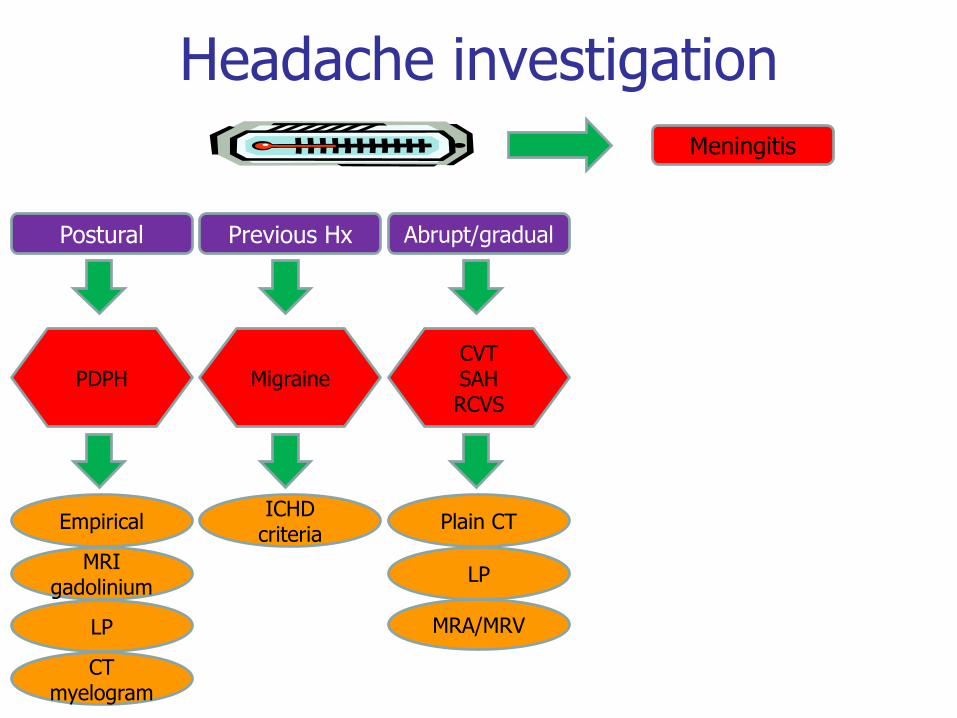
Headache investigation
Postural Previous Hx Abrupt/gradual
PDPH
Empirical
MRI gadolinium
LP
CT myelogram
Migraine
ICHD criteria
CVT SAH RCVS
MRA/MRV
LP
Plain CT
Meningitis
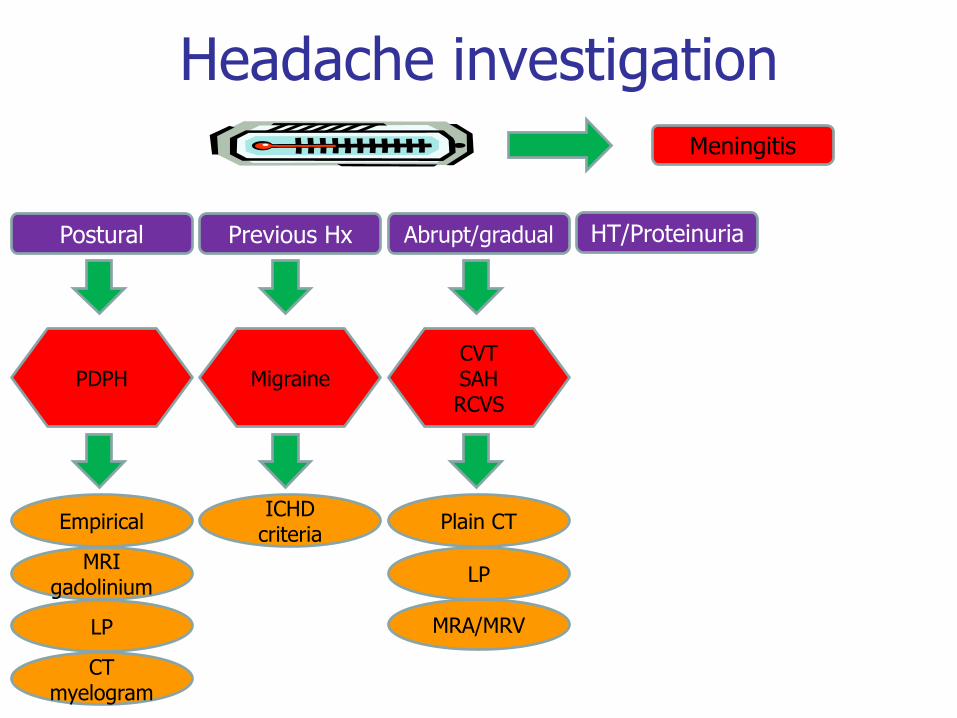
Headache investigation
Postural Previous Hx HT/Proteinuria Abrupt/gradual
PDPH
Empirical
MRI gadolinium
LP
CT myelogram
Migraine
ICHD criteria
CVT SAH RCVS
MRA/MRV
LP
Plain CT
Meningitis
Headache investigation
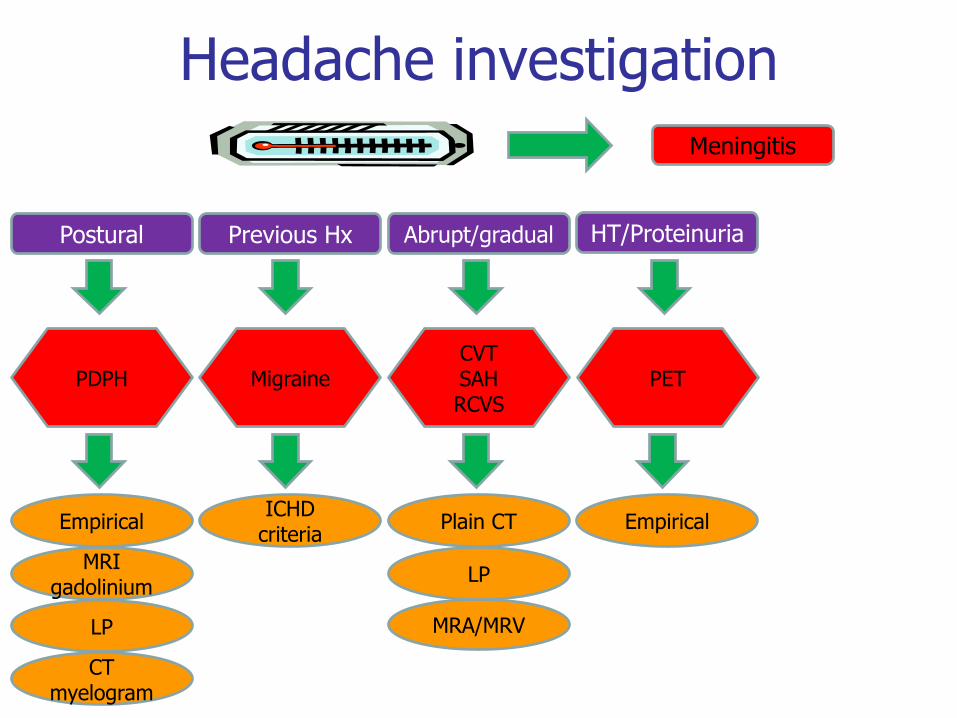
Postural Previous Hx HT/Proteinuria Abrupt/gradual
PDPH
Empirical
MRI gadolinium
LP
CT myelogram
Migraine
ICHD criteria
CVT SAH RCVS
PET
MRA/MRV
Empirical
LP
Plain CT
Meningitis
Headache investigation
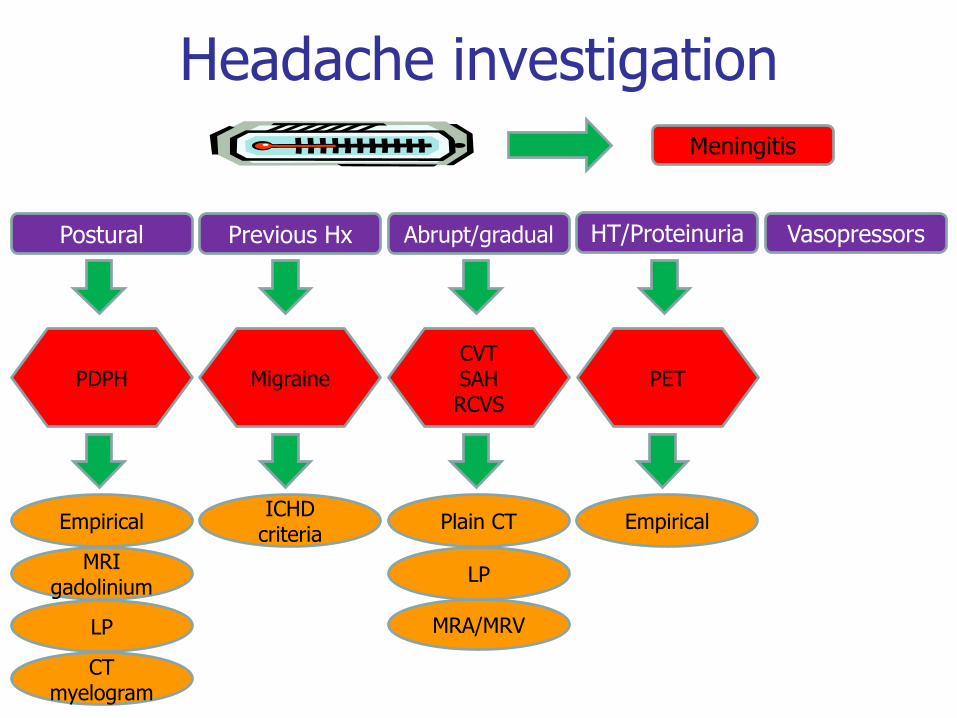
Postural Previous Hx Vasopressors HT/Proteinuria Abrupt/gradual
PDPH
Empirical
MRI gadolinium
LP
CT myelogram
Migraine
ICHD criteria
CVT SAH RCVS
PET
MRA/MRV
Empirical
LP
Plain CT
Meningitis
Headache investigation
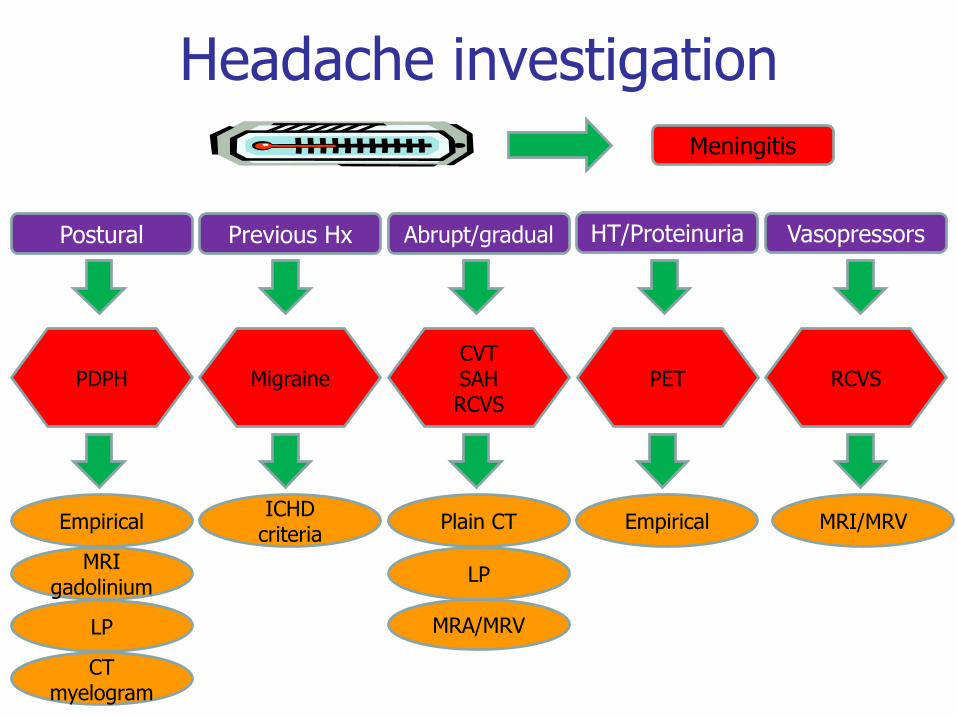
Postural Previous Hx Vasopressors HT/Proteinuria Abrupt/gradual
PDPH
Empirical
MRI gadolinium
LP
CT myelogram
Migraine
ICHD criteria
CVT SAH RCVS
PET RCVS
MRA/MRV
MRI/MRV Empirical
LP
Plain CT
Meningitis