gunnar Ågren 2005 the swedish public health policy gunnar Ågren
TRANSCRIPT
Gunnar Ågren 2005
The Swedish Public Health Policy
Gunnar Ågren
Historical background to the Swedish Public Health policy
A good system for vital statistics since 1750
From 1800 construction of community health services
A long tradition of popular struggle against the negative health effects of alcohol
The concern for the health of mothers and children was an important part of the welfare policy in the 1930’s and further on
Universal health insurance. Regional councils responsible for health services
A strong political commitment to healthGunnar Ågren 2005
A background to present public health work
Health has been an important part of social welfare
On the other hand no comprehensive public health policy
The medical perspective on public health has been very dominating especially after World War II
No strong emphasis on prevention with exception for injury prevention and occupational health
Primary care not very well developed
Gunnar Ågren 2005
Factors promoting a new public health policy
Increasing costs for health care – a disproportionate amount to highly specialized hospital care. Need for more preventive in health services
HIV/AIDS illustrated the need for a comprehensive preventive strategy
Increasing concern about inequity in health
A strategy group on public health in the government administration was formed in 1987
National Institute of Public Health founded 1992
Gunnar Ågren 2004
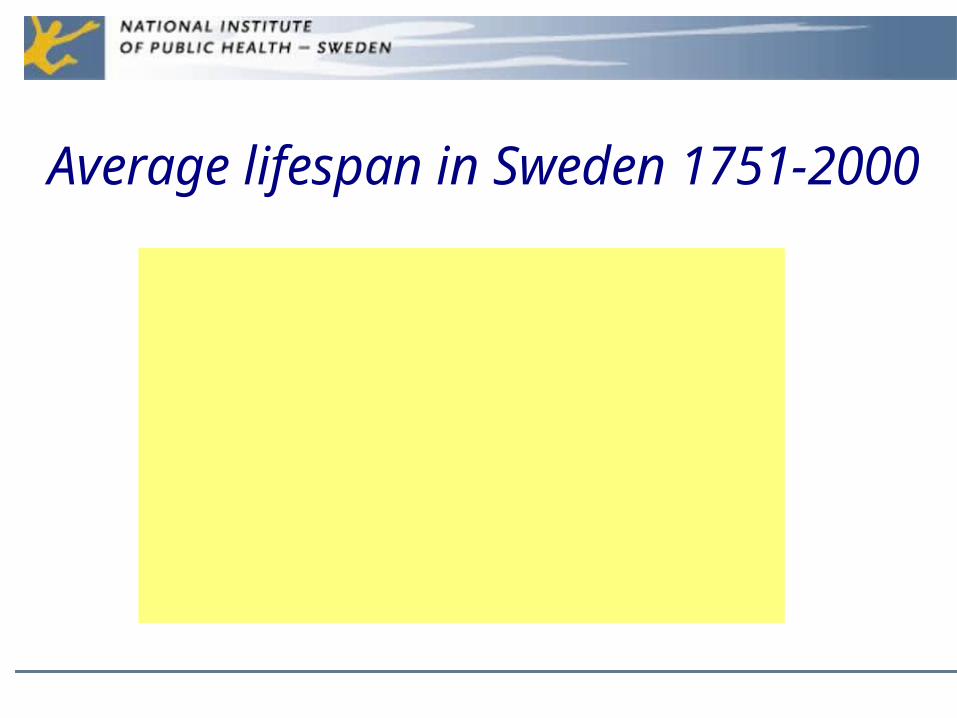
Average lifespan in Sweden 1751-2000
0
20
40
60
80
100
Females
Males
VaccinationAlcohol Sanitation
Rationing of alcohol
Ended 1955
National Public Health CommitteeIn 1997 a national public health committee was formed
All main political parties were represented, a number of experts
Many important NGO’s were represented
Main task: to propose public health goals and strategies
The committee worked for three years, a number of interim reports was delivered
The task of the committee – to propose national public health goals which should guide all sectors of the society
The goals were approved by the parliament in a revised version 2003.
Gunnar Ågren 2005
Gunnar Ågren 2005 7
Swedish public health policy- main target
areas 1. Participation and influence in the society
2. Economic and social security
3. Secure and favorable conditions during childhood and adolescence
4. Healthier working life
5. Healthy and safe environments and products
6. Health and medical care that more actively promotes good health
7. Effective protection against communicable diseases
8. Safe sexuality and good reproductive health
9. Increased physical activity
10. Good eating habits and safe food
11. Reduced use of tobacco and alcohol, a society free from illicit drugs and doping and a reduction in the harmful effects of excessive gambling.
To express the goals in relation to health determinants was an important decision
There is an obvious relation between the goals and political actions in order to achieve them
The main area of public health work becomes placed outside the health and medical sector
If the goals are broadly accepted they will guide actions in many sectors of the society
Gunnar Ågren 2005
Some problems
In some instances it may be hard to show that the fulfilment of a goal leads to improved health.
Economists, administrators and others may have difficulties in accepting population health as a desirable political goal
Conclusion – you have to provide good scientific evidence in order to promote public health policy
Gunnar Ågren 2005
A new role for NIPH
• Monitor the public health policy• Centre of excellence in the field of methods in
public health policy• Supervision of legislation concerning alcohol,
tobacco and illicit drugs• Support to regions and municipalities• Specific programmes concerning HIV and
gambling depency
How has the public health policy been implemented?
The main objectives have been approved by the parliament which gives them a strong political support
Indicators for all main objectives have been decided by the National Institute of Public Health after negotiations with other governmental agencies
18 agencies at national level are instructed by the government to participate in the public health policy
8 regions have been instructed to integrate public health into regional development plans
More than 50% of the 290 Swedish municipalities have adopted public health programs
Gunnar Ågren 2005
A public health policy report will be delivered to the government 2005
• The report will be based on the 38 main indicators and further indicators in specific areas
• There will be a report on how the policy have been implemented and what actions have been taken
• The report will evaluate the policy and discuss prioritizations and revisions
Gunnar Ågren 2005
1. 1. Participation and influence in the society
• Lack of participation and Lack of participation and influence harmful for Public influence harmful for Public HealthHealth
• Solid scientific evidence for the Solid scientific evidence for the causal relation between high causal relation between high demands-low control and demands-low control and diseasedisease
• Support for local participation, Support for local participation, culture, ethnic integration part culture, ethnic integration part of the public health policyof the public health policy
2. Economic and social security• Loss of security causes economic
stress• Lack of employment and lack of
access to social services bad for health
• The poverty trap: Poverty > disease > lower incomes and higher expenditures > increased poverty
• Social welfare and equality is good for Public Health
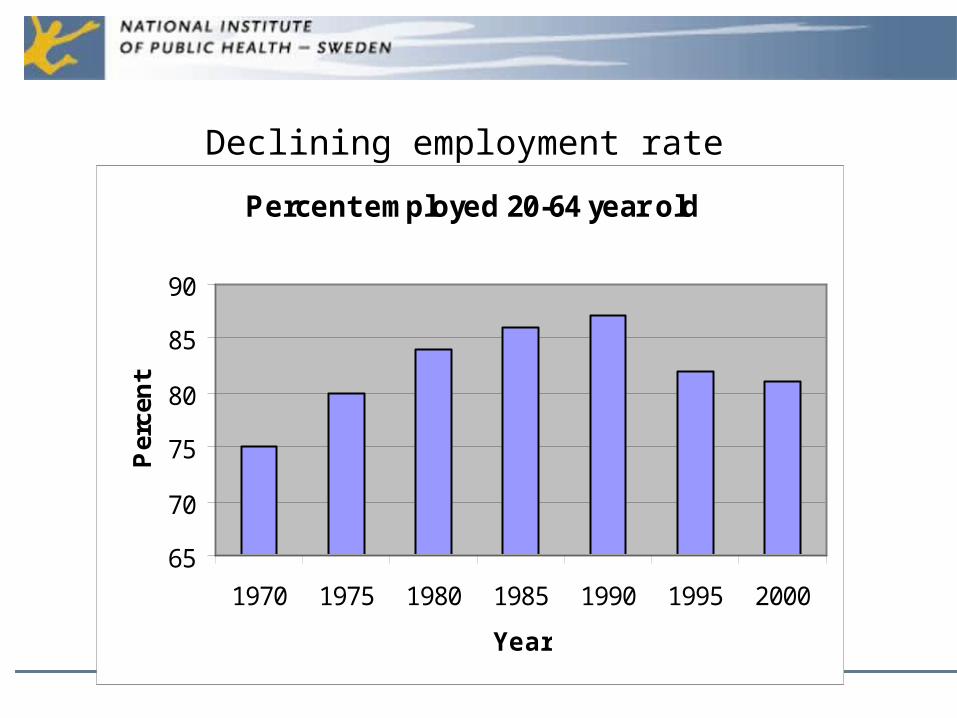
Percent employed 20-64 year old
65
70
75
80
85
90
1970 1975 1980 1985 1990 1995 2000
Year
Per
cen
t Declining employment rate
3. Secure and favorable conditions during childhood and adolescence
• Childhood conditions important for health later in life
• Support and education to parents, good child care, health schools
• Comprehensive maternity care has been very important for the low infant mortality in Sweden
• Declining mental health among young people a major problem
4. Healthier working life
• Taking good care of the workforce an important factor for social and economic developement
• Stress at work-places and lack of influence important problems
• Worse working conditions for females
• Large increase in work related health problems
5. Healthy and safe environments and products
• Integrate environmental policy with public health work
• Noise and air pollution the most important problems from a health perspective in Sweden
• Global warming, air pollution – especially indoor, access to fresh water
• Injury protection is very effective also in economic terms
• Cooperation against the great global health risks
6. Health and medical care that more actively promotes good health
• A well developed and accessible primary care important for prevention
• Maternity and child care of particular importance
• Integration of medical and social services
• Health promotion and disease prevention important for the entire health sector.
Main problems from a public health perspective
• Reduced accessability due to high fees• Increasing costs for drugs• Difficult to control total costs in a market
system with a lot of providers• Difficult to introduce prevention• Lack of cooperation with other sectors in
society especially in rehabilitation
7. Effective protection against communicable diseases
• HIV/AIDS, Malaria och TBC important threats to the entire population and work-force i many countries
• Most new cases of HIV are infected outside Sweden
• International cooperation is in the self-interest of all countries
8. Safe sexuality and good reproductive health
• Unsafe sex the second most important health risk in developing countries
• Sexually transmitted disease increasing
• Trafficing an important health risk
9.Increased physical activity
• Sedentary life-style and lack of healthful physical activity a major health risk
• Main determinant of Cardiavascular disease, diabetes, osteoporosis, cancer
• Promotion of physical activity in schools and workplaces an important public health measure
10.Good eating habits and safe food
• Today approximately 1 billion people suffer from malnutrition
• Approximately the same number are overweight which is a major cause of premature mortality
• A unequal distribution of food is a major problem in all parts of the world
• To much fat and sugar and to little fruit and vegetables the main problem
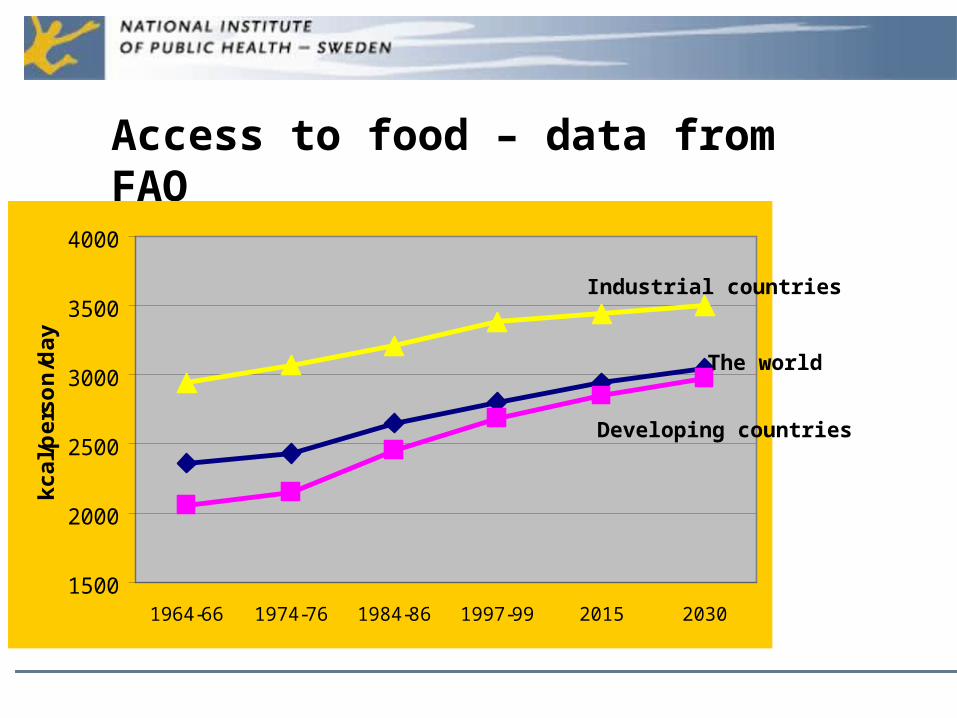
Access to food – data from FAO
1500
2000
2500
3000
3500
4000
1964-66 1974-76 1984-86 1997-99 2015 2030
kc
al/
pe
rso
n/d
ay
Industrial countries
The world
Developing countries
11. Reduced use of tobacco and alcohol, a society free from illicit drugs and doping and a reduction in the harmful effects of excessive gambling
• Tobacco the first and alcohol the third determinant of global burden of disease
• The average taxation on alcohol beverages has decreased internationally
• The Swedish alcohol consumption of alcohol has increased
• Tobacco-related mortality increasing internationally but decreasing in Sweden
• Distribution of illicit drugs an organised market connected with international crime. Sweden has a restrictive policy on illicit drugs
Källa: Undersökningen av levnadsförhållanden, SCB
1980 1985 1990 1995 20000
10
20
30
40
Andel dagligrökare
Män
Kvinnor
Percentage of daily smokers, 16-84 years, 1980-2002
Males
Females
June 1st 2005 – smoking will be prohibited in restaurants
Gunnar Ågren 2005 28
The main tasks of the Swedish National Institute of Public Health
National centre of competence in the field of public healthFollow-up of the effects of the national public health policySupervision of the legislation concerning alcohol, tobacco and narcotics Advisory functions to the governmentCooperation with research funding agencies and support to coordination of public health researchStrategic support to politicians and professionals at regional and local levels, who have the main responsibility for public health workation and support to professionals at regional and local levels
Which are the main Swedish public health problems?
1. The increase in work-related health problems and absence from work
2. The increase in mental health problems, especially among young people
3. The increase in obesity and sedentary life-style
4. The increasing alcohol consumption
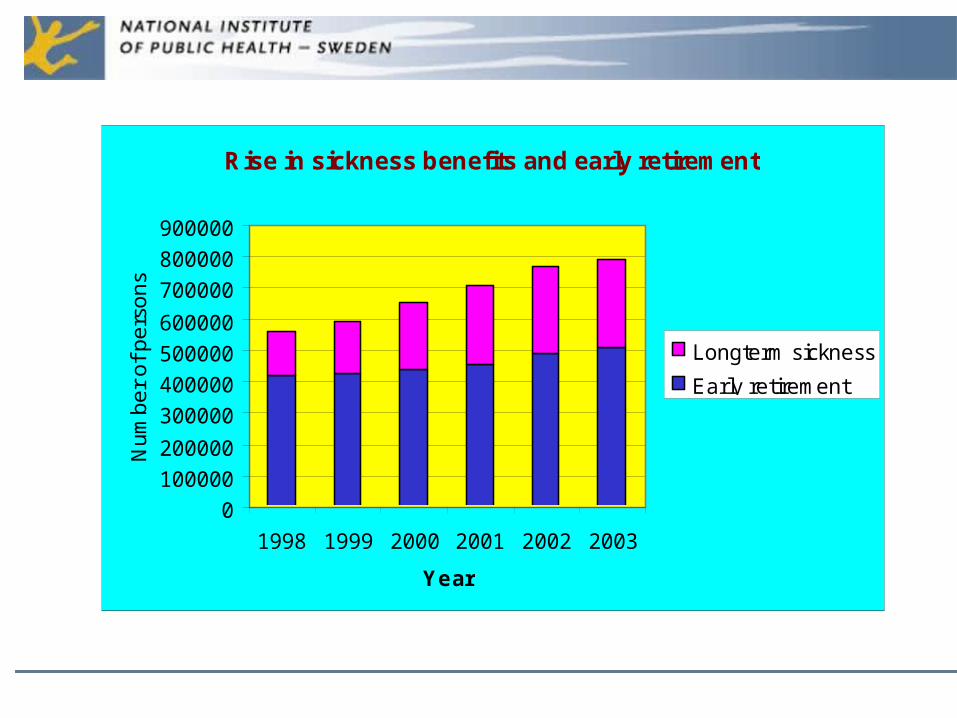
Rise in sickness benefits and early retirement
0
100000
200000
300000
400000
500000
600000
700000
800000
900000
1998 1999 2000 2001 2002 2003
Year
Nu
mb
er
of
pe
rso
ns
Longterm sickness
Early retirement
Possible actions
• Better working environment• Stricter rules for certification of sick leave• Better occupational health services• Lower benefits during sick-leave• Create jobs for people with decreased
working capacity
The Swedish alcohol consumptionLitres 100% alcohol/inhabitant
1990 1993 1995 1996 1998 2000 2001 20025
6
7
8
9
10
Sweden entered EU
Possible actions
• Restriction on sales and drinking in restaurants
• Education• Harder rules against drinking and driving• Information
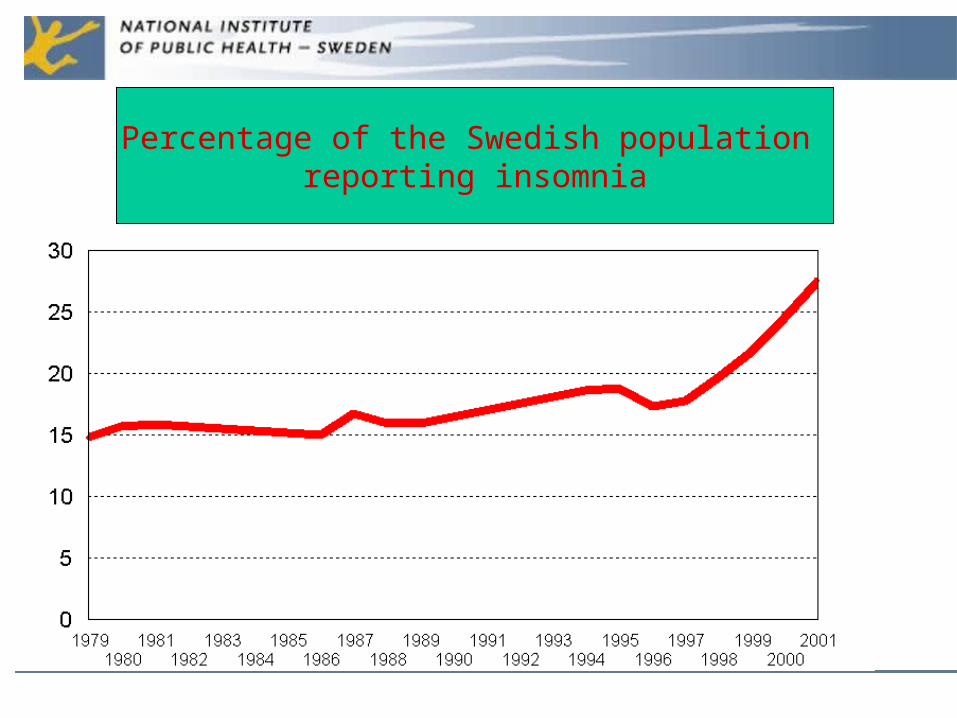
Percentage of the Swedish population reporting insomnia
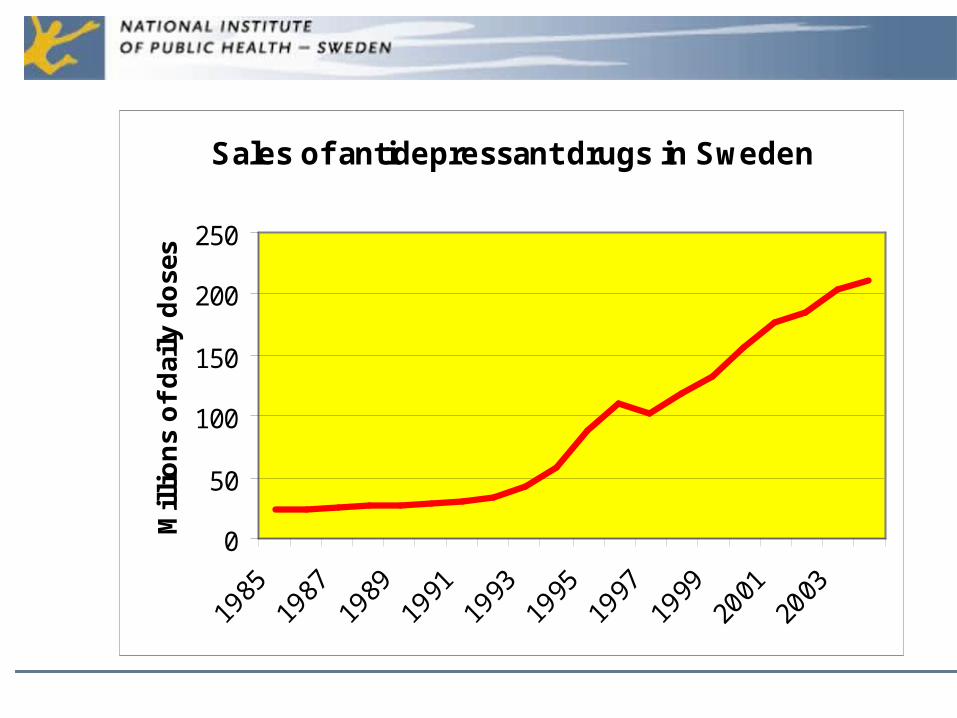
Sales of antidepressant drugs in Sweden
0
50
100
150
200
250
Mil
lio
ns
of
dai
ly d
ose
s
Possible actions
• Support to parents of small children• Better maternity and child care• Health promoting schools• Increase work opportunities for young people• Decrease negative stress in work places and
schools
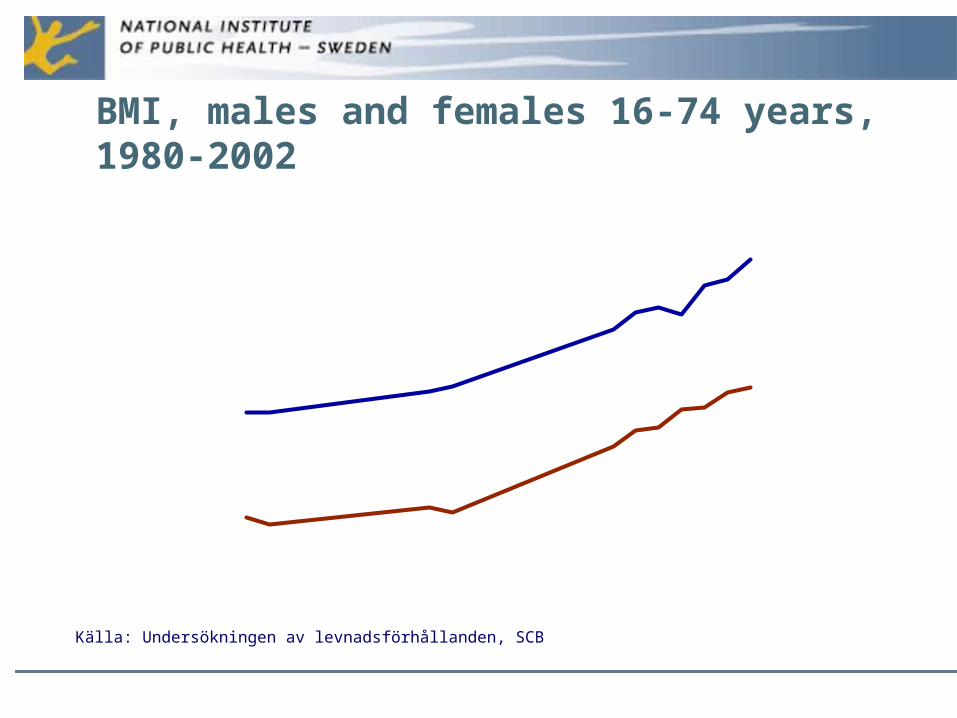
Källa: Undersökningen av levnadsförhållanden, SCB
BMI, males and females 16-74 years,1980-2002
1980 1989 1998 200123
23,5
24
24,5
25
25,5
26
Medel-BMI
Män
Kvinnor
Possible actions
• Decrease the intake of fat and sugar. Increase fruit and vegetables.- Pricing?
• Increase physical activity at least 30 minutes a day (60 minutes for young people)
• Prescriptions of physical activity and better food habits by doctors
• Physical activity in schools and work places.• Restrictions on food advertisments in TV to
children
Final conclusions
• The Swedish public health is still good in an international scale
• However, considerable health gaps• Mental health and self-reported health decreasing,
especially among young people• A number of threats against the health• A national public health policy is important to fight
those threats• International co-operation important in the field of
public health