greg warren
DESCRIPTION
Treatment and Recovery in AmericaNational Rx Drug Abuse Summit 4-10-12TRANSCRIPT

Treatment and Recovery in America
April 10-12, 2012 Walt Disney World Swan Resort

Accepted Learning Objectives: 1. Define when and how medication-assisted treatment methodologies for successful recovery of opioid addiction should be used. 2. Explain how to improve access and quality of care through strategic planning and community-wide coordination with local and state agencies. 3. Describe behavioral health issues faced by individuals within the corrections system and devise strategies to adequately address these clinical needs after incarceration.

Disclosure Statement
• All presenters for this session, Dr. Elinore McCance-Katz and Gregory C. Warren, have disclosed no relevant, real or apparent personal or professional financial relationships.

Baltimore Substance Abuse Systems, Inc.
Nuts and Bolts of Medication
Assisted Treatment and System
Coordination

Baltimore Substance Abuse Systems, Inc.
BSAS is a quasi-public agency incorporated in 1990.
In 1995, BSAS became responsible for the management of the publicly-funded substance abuse treatment and prevention service system.
The Chair of the 27-member Board is the Commissioner of Health.

Baltimore City’s Challenge • Heroin addiction remains high
– Treatment capacity falls short of demand despite expansion in treatment system
– Estimated 30,000 individuals with opioid dependence
– ~4,000 methadone treatment slots – Over 8,000 treatment admissions for opioids in FY
2008
• Consequences from heroin addiction are severe – Crime – Family and community disruption – Medical complications
• 1 in 48 Baltimore City residents are living with HIV and/or AIDS
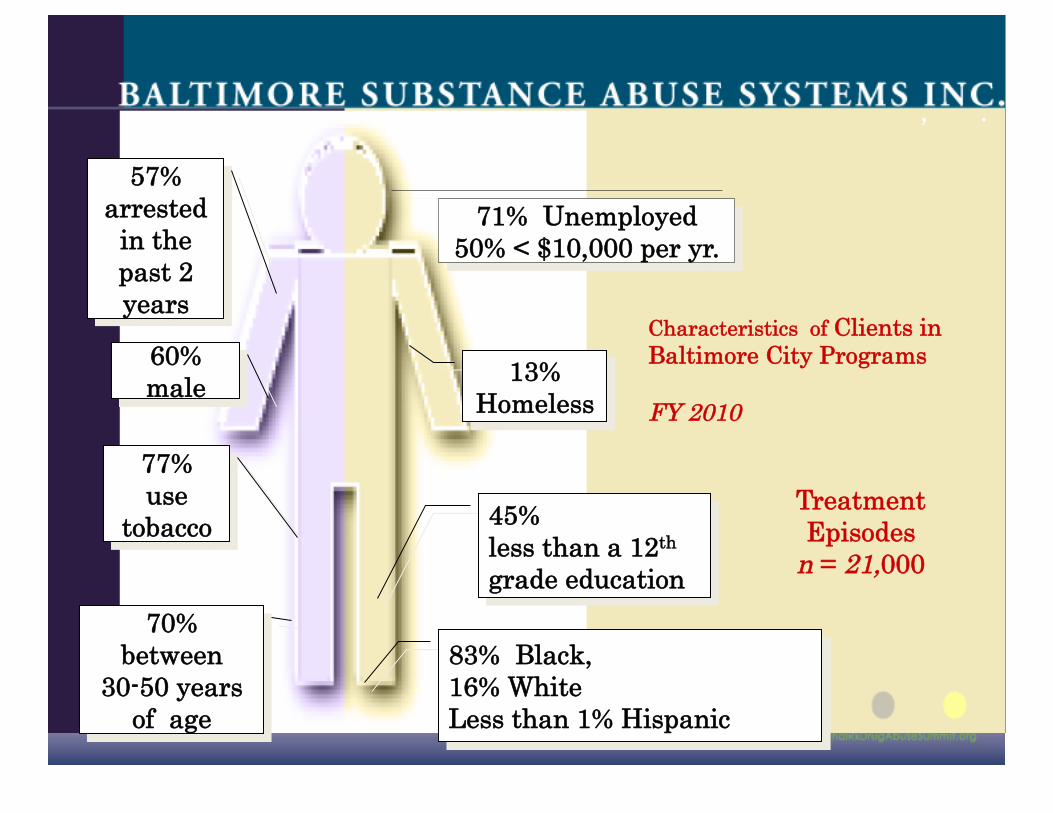
71% Unemployed 50% < $10,000 per yr.
83% Black, 16% White Less than 1% Hispanic
Characteristics of Clients in Baltimore City Programs
FY 2010
70% between
30-50 years of age
13% Homeless
45% less than a 12th grade education
77% use
tobacco
57% arrested
in the past 2 years
60% male
Treatment Episodes
n = 21,000
, .

Neighborhood Factors
• 78% felt drugs was a major problem • 31% felt neighborhood was safe to live • 26% felt neighborhood was a good
place to find a job • 59% felt living in the neighborhood
made it hard to stay out of jail

BSAS Vision and Mission VISION
We envision Baltimore as a city with healthy people, thriving families and safe communities.
HOW WE WILL ACHIEVE THIS We do this by planning, advocating for and helping to create coordinated networks of community-based and recovery focused services that build on the strengths and resilience of individuals, families, and communities.
Mission Baltimore Substance Abuse Systems seeks to ensure that
Baltimore residents receive high quality and comprehensive services proved to prevent and reduce substance abuse.

Concerns for the Future • Do our citizens have access to care?
• Do our citizens receive quality care?
• Individualized, continuous, coordinated care is better than disjointed, acute care which ignores the importance of the family and community
• Cultural and clinical diversity of services are better than “cookie cutter treatment”

Key Philosophical Understandings
• Pain and suffering are powerful motivators for change
• We need to be where people have their motivational moments
• Medication assisted treatment provides the time for counseling to work

Networks of formal and informal services developed and mobilized to sustain long-term recovery for individuals and families impacted by substance abuse.
“ The act of asking what the patient wants instead of what will be done to the patient.”
Recovery Oriented Systems of Care (ROSC)

Buprenorphine: 14 Methadone: 13

What is different about buprenorphine?

Buprenorphine Formulations
Buprenex (for pain only)
Subutex (for opioid addiction only)
Suboxone (for opioid addiction only, with naloxone)

How long do people need to stay on buprenorphine?
• Individualized • Studies demonstrate that staying on
medication in combination with counseling results in much better outcomes than detox
• 50% relapse rate within a year among patients who came off

Outcomes for Treatment As Usual • Of 3,753 admissions to Level I treatment in
FY08, 51% retained for 90 days or more
• Of 11,013 treatment discharges in FY08, only Prince George’s county had smaller change in substance use
• Relapse rates high – In methadone studies, 50-80% relapse within one
year after detoxification – 91% of patients receiving buprenorphine for 4
months had relapsed to prescription opioids within 2 months of taper*

19
Business Case for BBI in 2006 • Baltimore needs more effective treatment
for opioid dependence
• Review of literature and studies by UMBC – Medical costs are increased for patients
with drug abuse – Opioid addicts on methadone consume far
fewer Medicaid resources than addicts who go untreated
– Buprenorphine is economically viable alternative in city with limited methadone treatment capacity

Dept of Public Safety and Correctional Services
• Maryland manages the Detention Center – 4,000 inmates
• Men have a LOS of 28 days • Women have a LOS of 60 days
• Division of Correction – 22,000 inmate population
• 12,000 released annually • 9,000 are Baltimore City residents
– Over 70% have a diagnosis of Substance Abuse

OTP Interventions
• Maintain arrested OTP clients during Pre-Trial Status and reconnect them to their OTP at release
• Detox heroin-addicted inmates with non-opioids or on methadone
• Pregnancy protocol
• Buprenorphine conversion

Criminal History of Prison-based OTP Patients 1
Mean Age first crime 13.8
Age first arrest 16.5
Age first incarceration 20.6
Lifetime incarcerations 9.1
Past 30 days crime 25.5
Past 30 days crime-profit 24.8
Criminal Income ($/past 30 days)
8,057
1 Kinlock, Schwartz Gordon (2005)

Treating Prisoners with Heroin Addiction Histories
Most detainees with histories of heroin addiction do not receive drug abuse treatment while incarcerated
Such inmates typically become re-addicted within one month of release
Re-addiction is accompanied by the following: Increased criminal activity Unemployment High risk of HIV infection Greater risk of overdose death Incarceration

Offenders have more serious Substance Use & Other Disorders
• Offenders Have Higher Rates of Psycho-Social Dysfunctional Than the General Population – Substance Use Disorders – Mental Health and Somatic Health Disorders – Educational Deficiencies
• CJ Populations: 4 Times Greater SA Disorders NSDUH 2007

BBI Results
3,209 patients treated
2,094 (65%) obtained or had medical assistance
796 (38%) transferred to
continuing care
1,645 (79%) PAC
449 (21%) Health Choice
• Currently, 357 patients receiving full BBI services in treatment program
• Approximately 6% drop-out from continuing care

bSAS and B-MAT: Results • After controlling for baseline group differences, the B-MAT group
had less:
– Inpatient hospital admissions
– Inpatient days in hospital
– Outpatient hospital visits
– Emergency room visits
– Physician visits
• However, the only statistically significant differences compared to M-MAT and Abstinence-based treatment was for physician visits
• The M-MAT group has more health problems while the B-MAT and Abstinence groups have similar profiles
26

Factors to Improve Networkness? Integration or Boundaryless Processes of SA & CJ
Agencies Most Typical Activities: • Share Information with
agencies • Develop Client Eligibility
Across Agencies • Written Program
Programs • Joint Staffing of Program • Modified Program to Meet
Correctional and SA Agencies
• Written MOU between agency
Average Number of Activities Integrated: Drug Court=6.1 Probation/Parole=4.5 Prison=3.2 Jails=3.7
Interagency integration is associated with more use of EBPs, more holistic services, and improved outcomes
Fletcher, et al, in press ; Taxman & Perdoni, 2007

Project ACCESS
• Accountability • Communication • Collaboration • Efficiency • Security of Information • Service focus

BSAS ACCESS
Supports BSAS, Vision, Mission and Goals EHRc Information Sharing supports continuity of care.
EHRc Information Sharing furthers the goals of a ROSC approach.
EHRc Information Sharing frees up funding and staff so that it can be applied to improved Quality of Care.
• EHRc Information Sharing expands, consolidates and improves the quality of Public Health Data Repository.
• EHRc Information Sharing provides better quality and more complete data for evaluation and outcome reporting.

BSAS ACCESS Health Information Strategic
Planning New ways to collect, share and use data to serve
client. Interoperable systems and smooth information flow. “Wherever you go, there you are” • Better Quality data – reliable, consistent, complete. • New partnerships and collaborations in evaluating and
applying meaningful data. • Confidentiality and Consent

What providers tell us they want from their Information Systems
(From focus group discussions, interviews and in depth needs analyses) A fully functional, modern and meaningful use certified
EHR Consolidation of Information Systems and elimination of
redundant applications Access to additional client data and interoperability with
other client data systems
• Pricing discounts and additional leverage associated with forming an EHR (HIT) consortium
• Business practice and clinical practice management Information Systems improvements
• HIT advisement – How to get CMS incentive payments and how to avoid penalties

Draft - ACCESS Advisory Board • Behavioral Health Treatment Providers (2) • Consumers (2) • BSAS CEO • BSAS CIO • DPSCS CIO • Baltimore City CIO • DHMH CIO • BSAS Epidemiologist • University of Maryland Law Clinic • Health Care Access Maryland

Treatment Outcomes for the Criminal Justice Population
Drug Treatment Court N = 1,353
Other Criminal Justice N = 2,745
Criminal Justice Populations
Completion: 1,068 Incarceration: 21 Terminated: 264
Completion: 1,687 Incarceration: 71 Terminated: 987
Treatment Outcomes Drug Court Non-Drug Court Drug use during treatment 13% 38% Substance use at discharge 10% 25% 90 day retention in outpatient treatment (Level I) 63% 57% Completion of outpatient treatment (Level I) 52% 34% Continuity of care from ICF (Level III.7) to another LOC 73% 35% % change in employment from admission to discharge 183% 52%

Treatment Outcomes for the Criminal Justice Population
Drug Treatment Court N = 1,353
Other Criminal Justice N = 2,745
Criminal Justice Populations
Completion: 1,068 Incarceration: 21 Terminated: 264
Completion: 1,687 Incarceration: 71 Terminated: 987
Treatment Outcomes Drug Court Non-Drug Court Drug use during treatment 13% 38% Substance use at discharge 10% 25% 90 day retention in outpatient treatment (Level I) 63% 57% Completion of outpatient treatment (Level I) 52% 34% Continuity of care from ICF (Level III.7) to another LOC 73% 35% % change in employment from admission to discharge 183% 52%

Access: The Patient-Centered, Clinical Case Management Approach
A Recovery Oriented System of Care Not Constrained by Walls
Offender NEEDS
• Custody • Somatic Care • Substance Abuse Treatment • Mental Health Treatment • Case Management
Patient
NEEDS
• Substance Abuse treatment • Mental Health treatment • Somatic Care • Housing • Entitlement Benefits • Family Support Services • Faith-Based Services
DPDS DOC DPP Health Dept./Community Services

Shared Critical Understanding
• Correctional Services is an expectation of the public
• DPSCS is a part of Maryland’s public health system
• Our success is measured long after our offenders/patients leave

DPSCS and BSAS have a Shared Challenge
Information must follow the offender/patient and not reside and remain at the institution for it to do the greatest
good.
The Patient-Centered Approach

The Benefits of a DPSCS/BSAS Partnership
• BSAS will champion critical value added linkages which will improve offender’s health outcomes
• DPSCS/BSAS health information exchange becomes a higher priority to CRISP
• Direct benefit to 9,000 returning Baltimore City offenders annually

BSAS ACCESS
The Value Proposition Full-featured, meaningful use certified EHR for providers and partners. Consolidation of multiple provider applications on a single operating platform. (Replace UP and eliminate SMART data entry.) Information sharing between community resources and DPSCS. Steep discounts for high quality solution to providers and partners.
• More efficient and cost effective clinical and practice management for providers and partners • BSAS consultation and assistance in securing Medicaid incentive payments. • Information sharing between BSAS provider network, mental health, primary care providers, and other community resources. • Primary source, comprehensive public health data repository. • Comprehensive statistical evaluation and outcome reporting

BSAS- ACCESS
Design & Implementation
• Secure, segregated installations on a common operating platform • Custom module selection and configuration. • Economies of scale and cost reductions • Data sharing and information exchange • Aggregate public health data

Client Referral / Client Walk-in
Intake Administration Scheduling and Releases
AND
DATA FROM OTHER CONSORTIUM MEMBERS
Consent
Clinical Case Management / Documentation
Methadone (Other Meds) Management /
Dispensing EPrescription
Billing /Accounts Receivable/Financial
Management
Standard Practice Management Reporting
Compliance Reporting City, State, Federal
BSAS ACCESS Patient Management Work Flow

BSAS ACCESS BHCA
Entitlement
Benefits
BSAS Residential
BSAS Outpatien
t Programs
Health Providers thru CRISP
Health Departme
nt
FQHC GE
Centricity
BSAS Health Information Exchange
DPSCS OCMS BSAS
Methadone
Programs
DHMH SMART