global acute myocardial infarction perspectives
TRANSCRIPT

Global Acute MyocardialInfarction PerspectivesBeyond Door-to-Balloon Interventions
Sameer Mehta, MD, MBAa,b,e,*,Jennifer C. Kostela, MS, MDc,d, Estefania Oliveros, MDe,Camilo Pena, MDe, Rebecca Rowen, BSd, Kevin Treto, BSf,Ana Isabel Flores, MDe, Salomon Cohen, MDg,Tracy Zhang, BSe
KEYWORDS
� STEMI � PPCI � Acute myocardial infarction � Global AMI care
KEY POINTS
� Currently, the three main constraints in ST elevation myocardial infarction (STEMI) intervention inNorth America are delayed patient presentation, excessive rates of self-transportation, and legis-lative barriers.
� Enhanced patient education and legislative solutions will propel the United States to be foremostamong nations in providing STEMI care.
� Globally, acute myocardial infarction (AMI) care must undergo four phases of development, guidedby population-based programs of AMI management.
� Adherence to North American and European guidelines globally remains an unrealistic goal givenunparalleled cultural, demographic, and fiscal dynamics.
� Globally, a pharmacoinvasive approach to STEMI care must be based upon socioeconomic imped-ance.
Dramatic progress has beenmade,most notably inthe United States, in door-to-balloon (D2B) inter-ventions.1,2 As a result, D2B times that weredismally low are now improving in the UnitedStates. Specifically, D2B times ranged from 4%to 10% a decade ago and now exceed 90%.3
This increasehas resulted in unprecedented reduc-tions in mortality from acute myocardial infarction(AMI).4,5 Several centers nowachieve high volumes
Disclosure: Sameer Mehta is Chief Medical Officer, Asiaauthors report no conflict of interest regarding the conta Miller School of Medicine, University of Miami, 1400 NoMedical Center, 3663 South Miami Avenue, Miami, FL 3Queens, 56-45 Main Street, Flushing, NY 11355, USA; d RNorth Brunswick, NJ 08902, USA; e Lumen Foundation, 5School of Medicine, 786 Seneca Meadows Road, Winter Sugia, Instituto Mexicano del Seguro Social, Avenida Clubquilucan Edo de Mexico, 52779, Mexico* Corresponding author. 185 Shore Drive South, Miami,E-mail address: [email protected]
Intervent Cardiol Clin 1 (2012) 479–484http://dx.doi.org/10.1016/j.iccl.2012.06.0012211-7458/12/$ – see front matter � 2012 Elsevier Inc. All
of D2B interventions, with mortalities ranging from2% to 3%. Parallel to this decrease in mortality isan evenmore powerful reduction inmorbidity asso-ciated with AMI.6–8
EUROPE AND CANADA
Most of the progress that the United Statesachieved was initially learned from the experience
Pacific, for the Medicines Company. The rest of theent herein.rthwest 12th Avenue, Miami, FL 33136, USA; b Mercy3133, USA; c Internal Medicine, New York Hospitaloss University School of Medicine, 630 US Highway 1,5 Pinta Road, Miami, FL 33133, USA; f Ross Universityprings, FL 32708, USA; g Departamento de Neurocir-de Golf#3 Torre A Dep. 1501, Lomas Country, Huix-
FL 33133.
rights reserved. interventional.th
eclinics.com
Mehta et al480
of primary percutaneous coronary intervention(PPCI) in Europe and Canada.9,10 In particular,uniform success across the continent of Europewas highly inspiring. Although most early PPCIwas performed in the United States, the truepopulation-based benefits were noticed in Europe,initially in the Czech Republic, Denmark, and theNetherlands.9,11–13 This work was notable forshowing that patients who were transferred forPPCI did better than those treatedwith thrombolytictherapy, despite the added transfer times.14–16
However, Europe comprises several countries thatare relatively small and have very sophisticatedambulance services, and patient awarenessremains significantly higher in Europe than in theUnited States.17 Therefore, Europe succeeded increating superb AMI care. Further progress inEurope clearly will be slow because of the near-total penetration of excellent ST elevation myo-cardial infarction (STEMI) care in the continent.Nonetheless, outstanding public educational cam-paigns, such as STENT for LIFE,9 are adding newdimensions of care across the spectrum of preho-spital presentation, STEMI care, and post–myocar-dial infarction management. The STENT for LIFEprogram has made numerous additional contribu-tions, such as improving the overall care of patientspresenting with an AMI. Very few patients nowmisscare altogether, and those that receive thrombolytictherapy are obtaining the treatment earlier. Europehas also advanced innovative prehospital manage-ment of patients with AMI treated with thrombolytictherapy and with PPCI.Despite themassive sizeof the country, theprog-
ress in Canada was similar to that in Europe.However, this occurred in a nation where almost90% of the population is populated in large urbanareas close to the United States border. In Canada,several excellent population-basedPPCIprogramshave been created, particularly in Ontario.10,18
AMAZING STEMI PROGRESS IN THE UNITEDSTATES
The progress in the United States was expected tooccur through the creation of a national STEMIpolicy, akin to trauma care. In this model, patientswould be preferentially transported to an STEMIcenter in a manner similar to trauma patients. Itwasalsoanticipated that, similar toa level 1nationaltrauma program, patients with AMI would obtainclinical triage and transfer to a center performing24/7 PCI. However, none of these innovationsoccurred, being hindered by legislative challenges.Nevertheless, some amazing and unprecedentedprogress was made through collaborative actionsof American Heart Association (AHA) and America
College of Cardiology (ACC). Leadership withinthese organizations conceptualized an STEMIsystem-of-care approach.19 Its genius was notonly this remarkable joint educational endeavorbut also the urgent incorporation of an STEMIsystemsof caremandateasaClass I recommenda-tion in the current AHA/ACCguidelines.20With suchan STEMI system-of-care methodology, everyhospital in this vast nation is mandated topronounce itself as either aPCI or a non-PCI facility.Transfer protocols have been formed to createunambiguous pathways of transfer from a non-PCI to a PCI facility. This monstrously difficult taskhas been achieved almost single-handedly byAHA’s Mission Lifeline.21
Clear navigational pathways of patient carehave facilitated the STEMI process that appearedchaotic and simply impossible to achieve.Phenomenal advancements in the ambulance
services have occurred, including remarkablepenetration of information technology into ambu-lances,22 development of innovative guidelinesfor prehospital alert23 and triage, and establish-ment of a somewhat controversial but colossalmandate permitting STEMI interventions to be per-formed without surgical stand-by.24
It is a tribute to the United States’ collaboratingorganizations and the brilliance of some individualcardiologists (Dr Timothy Henry, Dr Ivan Rokos, DrChristopher Granger, Dr James Jollis, Dr HenryTing, Dr Cindy Grines, Dr Alice Jacobs, Dr ElizabethBradley, Dr Harlan Krumholz, and Dr BrahmajeeNallamothu) that have enabled this unprecedentedbreakthrough.
CHALLENGES IN U.S. STEMI INITIATIVES
Deficiencies, however, still exist in the manage-ment of AMI in the United States, particularly inSTEMI interventions. These limitations currentlyexist in three large areas: delayed patient presen-tation, excessive rates of self-transportation, andlegislative barriers. With regard to legislativeissues, two disruptive practices prevail. With thefirst one, patients with STEMI being transportedby ambulance are not always taken to an STEMIinstitution first. An equally distributed second setof circumstances legislatively impairs the prompttransfer of patients with STEMI from a non-PCI toa PCI institution.25–27 These three challenges arereviewed in detail.In addition to these three mega-challenges,
several smaller deficiencies are also seen,including some philosophic disagreements. AreD2B times excellent scientific parameters ora fuzzy metric prone to manipulation? Are physi-cians not better off measuring true ischemic
Global AMI Perspectives 481
times? Physicians performing STEMI interventionsdo not seem to have adequate volumes. SpecificSTEMI interventional training is lacking altogetherand thrombus management for STEMI lesions isclearly inadequate. Controversies exist as towhether bare metal or drug-eluting stents aresuperior. Thrombectomy devices, at best, arecrude. Mostly, achieving D2B times on weekendsand off-hours remains challenging.28 Finally,several patients are uninsured, placing deepburden on hospitals and attending physicians.
Returning to the three major constraints inpresent STEMI care, the authors discern lack ofpatient education as the most critical flaw. Makinga difference in this crucial deficit will not be easy.Lack of patient education often results froma myriad of causes that include cultural andeducational dissimilarities. Educating patientsabout the need and availability of STEMI interven-tions is a formidable task. Patients must beeducated to promptly recognize the symptoms ofa heart attack without referring their clinical stateto a primary physician and, even worse, rela-tives.29 Women in particular demonstrate atypicalsymptoms, the recognition of which must bea major component of patient education.28 Simi-larly, elderly patients manifest presentations thatare more difficult to recognize because they livealone. Early recognition of heart attack will requirea multifaceted approach and the earnest efforts ofa broad segment of stakeholders, includingpatients, family physicians, internists, cardiolo-gists, hospital administrators, insurers, medicalsocieties, community organizations, and otherphilanthropic organizations. Ultimately, patientsmust educate themselves and learn to recognizetheir presenting clinical symptoms that may repre-sent a heart attack. The role of media can never beoveremphasized.
For the United States to continue its unprece-dented success in combating heart attacks,patient education must remain paramount.
Legislation represents the next major impasse.D2B times in STEMI interventions are still the lowhanging fruit in AMI care. Without education andprudent legislation, further progress in AMI carecan only be limited. Legislation must be enactedin two specific areas. First, a patient who is identi-fied as having a heart attack must be safely andurgently transported to a PCI center and bypassthe nearest facility.22,30–33 The secondary partic-ular anomaly pertains to appropriate transfer ofa patient with STEMI from a non-PCI to a PCI insti-tution. Disturbingly, these non-PCI institutions areconflicted by financial reasons and they oftendelay transportation that is urgently needed forthese patients. Disparate management is also
encountered at these non-PCI institutions basedon the patient’s insurance status and the abilityto pay.
The authors firmly believe that enhanced patienteducation and legislative solutions will propel theUnited States to be foremost among nations inproviding STEMI care.
GLOBAL STEMI CARE
Unfortunately, approximately 7.5 million patientsstill continue to die from an imminently treatableentity that costs more than $400 billion in healthcare resources.34 As tremendous as the gains ofAMI care are in the Western World, so are thedesolate conditions prevailing in developing coun-tries in caring for patients with heart attacks.Trained interventional cardiologists are easilyable to perform STEMI interventions in developedand in developing countries. It is not the STEMIprocedure but the STEMI process that is lackingin most countries. Although an STEMI interventionprocedure is not terribly complicated, it does entailimmediate availability and moderate skills. A muchlarger problem pertains to the process and thegross unavailability of adequate resourcesrequired for caring for a patient with STEMI. Ambu-lance services are often qualitatively and quantita-tively lacking, and financial constraints preventSTEMI interventions from being performed inseveral developing countries. These countriesstruggle to provide basic cardiac catheterizationservices even in major metropolitan areas. Devel-oping sophisticated 24/7 STEMI teams is clearlynot possible, nor does there seem to be a realisticchance of its happening for decades. Poorer coun-tries have very meager financial resources, makingallocation of funds and services for the care ofpatients with heart attack extremely difficult.Based on these deep financial constraints, it isunrealistic to expect STEMI interventions tobecome a dominant form of AMI management inthese developing countries.
Based on the authors’ extensive global work,they confidently predict a phased global progressin AMI care. With this proposed methodology,developing countries will go through the scenariodepicted in Table 1. Basic thrombolytic therapymust be universally available as a first stage.Further development of infrastructure and ambu-lance services can lead to a mid-stage pharma-coinvasive management. Only after decades ofdeep financial resource allocation and govern-mental commitment can one expect progress tothe final phase of population-based, pragmaticD2B management for patients with STEMI. Theauthors believe that most countries will progress
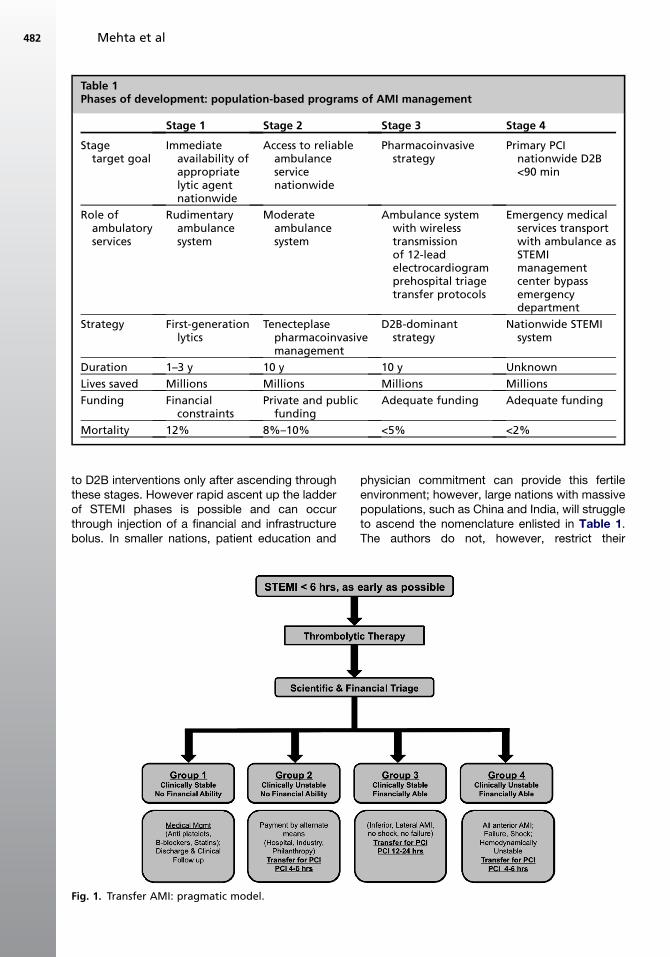
Table 1Phases of development: population-based programs of AMI management
Stage 1 Stage 2 Stage 3 Stage 4
Stagetarget goal
Immediateavailability ofappropriatelytic agentnationwide
Access to reliableambulanceservicenationwide
Pharmacoinvasivestrategy
Primary PCInationwide D2B<90 min
Role ofambulatoryservices
Rudimentaryambulancesystem
Moderateambulancesystem
Ambulance systemwith wirelesstransmissionof 12-leadelectrocardiogramprehospital triagetransfer protocols
Emergency medicalservices transportwith ambulance asSTEMImanagementcenter bypassemergencydepartment
Strategy First-generationlytics
Tenecteplasepharmacoinvasivemanagement
D2B-dominantstrategy
Nationwide STEMIsystem
Duration 1–3 y 10 y 10 y Unknown
Lives saved Millions Millions Millions Millions
Funding Financialconstraints
Private and publicfunding
Adequate funding Adequate funding
Mortality 12% 8%–10% <5% <2%
Mehta et al482
to D2B interventions only after ascending throughthese stages. However rapid ascent up the ladderof STEMI phases is possible and can occurthrough injection of a financial and infrastructurebolus. In smaller nations, patient education and
Fig. 1. Transfer AMI: pragmatic model.
physician commitment can provide this fertileenvironment; however, large nations with massivepopulations, such as China and India, will struggleto ascend the nomenclature enlisted in Table 1.The authors do not, however, restrict their
Global AMI Perspectives 483
predictions to having a single stage of develop-ment at a single time. For example, the possibilitydefinitely exists that in particular countries, severalstages of care be delivered simultaneously. Withthis methodology, several metropolitan cities willprovide D2B interventions, and rural areas willdeliver basic thrombolytic therapy. Good medicalmanagement remains an integral part of theproposed management strategies.
Regarding pharmacoinvasive management, itseems transparent to the authors that sciencecannot remain the sole guidance for care ofpatients with AMI. Specially, the authors allude topharmacoinvasive management and United Statesand European guidelines that mandate PCIstrategy universally for patientswho receive throm-bolytic therapy (Fig. 1).14–16,33
SUMMARY
The authors sincerely believe that scientific recom-mendations must be balanced with fiscalprudence. With earnest conviction, they proposea strategy that balances medicine and financialrealities. This financial balance will be needed todeliver appropriate care to the millions of peoplein developing countries who are vulnerable toa heart attack.
REFERENCES
1. Herrin J, Miller LE, Turkmani DF, et al. National
performance on door-in to door-out time among
patients transferred for primary percutaneous coro-
nary intervention. Arch Intern Med 2011;171(21):
1879–86.
2. Nallamothu BK, Bates ER, Wang Y, et al. Driving
times and distances to hospitals with percutaneous
coronary intervention in the United States: implica-
tions for prehospital triage of patients with ST-
elevation myocardial infarction. Circulation 2006;
113(9):1189–95.
3. Krumholz HM, Herrin J, Miller LE, et al. Improve-
ments in door-to-balloon time in the United States,
2005 to 2010. Circulation 2011;124(9):1038–45.
4. Nallamothu B, Bates ER. Percutaneous coronary
intervention versus fibrinolytic therapy in acute
myocardial infarction: is timing (almost) everything?
Am J Cardiol 2003;92:824–6.
5. Keeley EC, Boura JA, Grines CL. Primary angio-
plasty versus intravenous thrombolytic therapy for
acute myocardial infarction: a quantitative review of
23 randomised trials. Lancet 2003;361(9351):13–20.
6. Stenestrand U, Lindback J, Wallentin L. Long-term
outcome of primary percutaneous coronary inter-
vention vs prehospital and in-hospital thrombolysis
for patients with ST-elevation myocardial infarction.
JAMA 2006;296(14):1749–56.
7. Shavelle DM, Rasouli ML, Frederick P, et al.
Outcome in patients transferred for percutaneous
coronary intervention (a national registry of myocar-
dial infarction 2/3/4 analysis). Am J Cardiol 2005;
96(9):1227–32.
8. Brodie BR, Stuckey TD, Hansen C, et al. Benefit of
coronary reperfusion before intervention on outcomes
after primary angioplasty for acute myocardial infarc-
tion. Am J Cardiol 2000;85(1):13–8.
9. Widimsky P, Wijns W, Fajadet J, et al. Reperfusion
therapy for ST elevation acute myocardial infarction
in Europe: description of the current situation in 30
countries. Eur Heart J 2010;31(8):943–57.
10. LeMayM.CodeSTEMI: implementation of a city-wide
program for rapid assessment and management of
myocardial infarction. CMAJ 2009;181(8):E136–7.
11. Andersen H, Nielsen TT, Rasmussen K, et al. DANA-
MI-2. A comparison of coronary angioplasty with
fibrinolytic therapy in acute myocardial infarction.
N Engl J Med 2003;349(8):733–42.
12. Widimsky P, Budesinsky T, Vorac D, et al. Long
distance transport for primary angioplasty vs imme-
diate thrombolysis in acute myocardial infarction.
Final results of the randomized national multicentre
trial–PRAGUE-2. Eur Heart J 2003;24(1):94–104.
13. Widimsky P, Groch L, Zelizko M, et al. Multicentre
randomized trial comparing transport to primary
angioplasty vs immediate thrombolysis vs combined
strategy for patients with acute myocardial infarction
presenting toacommunity hospitalwithoutacatheter-
ization laboratory. The PRAGUE study. Eur Heart J
2000;21(10):823–31.
14. Larson DM, Duval S, Sharkey SW, et al. Safety and
efficacy of a pharmaco-invasive reperfusion strategy
in rural ST-elevation myocardial infarction patients
with expected delays due to long-distance transfers.
Eur Heart J 2012;33(10):1232–40.
15. D’Souza SP, Mamas MA, Fraser DG, et al. Routine
early coronary angioplasty versus ischaemia-
guided angioplasty after thrombolysis in acute ST-
elevation myocardial infarction: a meta-analysis.
Eur Heart J 2011;32(8):972–82.
16. BohmerE,HoffmannP,AbdelnoorM,etal.Efficacyand
safety of immediate angioplasty versus ischemia-
guided management after thrombolysis in acute
myocardial infarction in areas with very long transfer
distances results of the NORDISTEMI (NORwegian
study on DIstrict treatment of ST-elevation myocardial
infarction). J Am Coll Cardiol 2010;55(2):102–10.
17. Lee RS, Kaushal R, Bholat T, et al. Patient differ-
ences by mode of hospital arrival for ST-elevation
myocardial infarction treated with primary PCI. Avail-
able at: http://www.tctmd.com/txshow.aspx?tid5
2640&id5110728&trid52. Accessed March 26,
2012.
Mehta et al484
18. So DY, Ha AC, Turek MA, et al. Comparison of
mortality patterns in patients with ST-elevation
myocardial infarction arriving by emergency
medical services versus self-transport (from the
prospective Ottawa Hospital STEMI Registry). Am
J Cardiol 2006;97(4):458–61.
19. Jacobs AK, Antman EM, Ellrodt G, et al. Recommen-
dation to develop strategies to increase the
number of ST-segment-elevation myocardial infarc-
tion patients with timely access to primary per-
cutaneous coronary intervention. Circulation 2006;
113(17):2152–63.
20. Wright RS, Anderson JL, Adams CD, et al. 2011
ACCF/AHA focused update incorporated into the
ACC/AHA 2007 Guidelines for the Management of
Patients with Unstable Angina/Non-ST-Elevation
Myocardial Infarction: a report of the American
College of Cardiology Foundation/American Heart
Association Task Force on Practice Guidelines
developed in collaboration with the American
Academy of Family Physicians, Society for Cardio-
vascular Angiography and Interventions, and the
Society of Thoracic Surgeons. J Am Coll Cardiol
2011;57(19):e215–367.
21. American Heart Association. Mission: Lifeline. Avail-
able at: http://missionlifelinecommunity.americanheart.
org/home. Accessed March 1, 2012.
22. Sanchez-Ross M, Oghlakian G, Maher J, et al. The
STAT-MI (ST-Segment Analysis Using Wireless Tech-
nology in Acute Myocardial Infarction) trial improves
outcomes. JACC Cardiovasc Interv 2011;4(2):
222–7.
23. Diercks DB, Kontos MC, Chen AY, et al. Utilization
and impact of pre-hospital electrocardiograms for
patients with acute ST-segment elevation myocardial
infarction: data from the NCDR (National Cardiovas-
cular Data Registry) ACTION (Acute Coronary Treat-
ment and Intervention Outcomes Network) Registry.
J Am Coll Cardiol 2009;53(2):161–6.
24. Dehmer GJ, Kutcher MA, Dey SK, et al. Frequency
of percutaneous coronary interventions at facilities
without on-site cardiac surgical backup—a report
from the American College of Cardiology-National
Cardiovascular Data Registry (ACC-NCDR). J Am
Coll Cardiol 2007;99(3):329–32.
25. Harjai K, Orshaw P, Boura J, et al. Reperfusion delay
in patients with ST-elevation myocardial infarction
presenting to hospitals without angioplasty
capability: should ‘door-to-ambulance’ time be the
new quality parameter for non-PCI hospitals? 2012.
Available at: http://www.tctmd.com/txshow.aspx?
tid52640&id5110743&trid52. Accessed March
26, 2012.
26. Wang TY, Nallamothu BK, Krumholz HM, et al. Asso-
ciation of door-in to door-out time with reperfusion
delays and outcomes among patients transferred
for primary percutaneous coronary intervention.
JAMA 2011;305(24):2540–7.
27. Miedema MD, Newell MC, Duval S, et al. Causes of
delay and associated mortality in patients trans-
ferred with ST-segment-elevation myocardial infarc-
tion. Circulation 2011;124(15):1636–44.
28. Concannon TW, Nelson J, Goetz J, et al.
A percutaneous coronary intervention lab in every
hospital? Circ Cardiovasc Qual Outcomes 2012;
5(1):14–20.
29. Hand MM. “Act in Time to Heart Attack Signs” action
plan: a patient-based critical pathway. Crit Pathw
Cardiol 2002;1(1):61–5.
30. Ting HH, Rihal CS, Gersh BJ, et al. Regional
systems of care to optimize timeliness of reperfusion
therapy for ST-elevation myocardial infarction: the
Mayo Clinic STEMI Protocol. Circulation 2007;
116(7):729–36.
31. Ting HH, Krumholz HM, Bradley EH, et al. Imple-
mentation and integration of prehospital ECGs into
systems of care for acute coronary syndrome:
a scientific statement from the American Heart Asso-
ciation Interdisciplinary Council on Quality of Care
and Outcomes Research, Emergency Cardiovas-
cular Care Committee, Council on Cardiovascular
Nursing, and Council on Clinical Cardiology. Circula-
tion 2008;118(10):1066–79.
32. Concannon TW, Kent DM, Normand SL, et al.
Comparative effectiveness of ST-segment-elevation
myocardial infarction regionalization strategies. Circ
Cardiovasc Qual Outcomes 2010;3(5):506–13.
33. Rokos IC, French WJ, Mattu A, et al. Appropriate
cardiac cath lab activation: optimizing electrocardio-
gram interpretation and clinical decision-making for
acute ST-elevation myocardial infarction. Am Heart J
2010;160(6):995–1003.e1–8.
34. Bradley E, Roumanis S, Radford M, et al. Achieving
door-to-balloon times that meet quality guidelines:
how do successful hospitals do it? J Am Coll Cardiol
2005;46(7):1236–41.