glenoid-labral cyst entrapping the suprascapular nerve ......electroneurogram studies showed an...
TRANSCRIPT

Case Report
Glenoid-Labral Cyst Entrapping the Suprascapular Nerve: Dissolution After Arthroscopic Debridement of an
Extended SLAP Lesion
Martin H. Chochole, M.D., Wolfgang Senker, M.D., Christian Meznik, M.D., and Martin J. Breitenseher, M.D.
Summary: Glenoid labral cysts are commonly associated with labral tears, which can cause pain or instability. We present the case of a patient, referred for neurolog- ical complaints, who was actually suffering from supraspinatus nerve entrapment syndrome. Electroneurogram studies showed an isolated lesion of the branch to the infraspinatus muscle. Magnetic resonance imaging confirmed a glenoid labral cyst extending from the cranial glenoid to the scapular notch. After arthroscopic debridement of an extended SLAP-lesion that had caused joint fluid extrusion, the dissolution of the cyst was associated with complete neurological recovery. The patient is pain free and range of motion is normal. An attempt at an arthroscopic procedure seems warranted in cases like this, since cysts that accompany labral tears can dissolve after rigorous debridement of the torn labrum, much like meniscal cysts. Extended and hazardous open excisions can thus be avoided. Key Words: Shoulder--Glenoid-labral cyst--Supraspinatus nerve entrapment--SLAP le- sion--Arthroscopy.
S urgical treatment of glenoid-labral cysts has been reported mostly as an open procedure that is techni-
cally demanding. 1-3 Seldom are these cysts treated con- servativly or eventually combined with ultrasound or computed- tomography-gu ided puncture. There are some recent articles about arthroscopic treatment par- tially combined with puncture and/or open resection. 4
Glenoid-labral cysts are commonly associated with labrat tears that are identified in most cases as SLAP- lesions, and accompanied by distinct shoulder instabil- ity. It is hypothesized that cysts may arise f rom joint fluid extrusion in a mechanism analogous to that which
From the Orthopaedic Department, General Hospital, Amstetten, Austria.
Address correspondence and reprint requests to Martin Chochole, M.D., Department of Orthopaedic Surgery, General Hospital, Kran- kenhausstral3e 21, A-3300 Amstetten, Austria.
© 1997 by the Arthroscopy Association of North America 0749-8063/97/1306-166053.00/0
causes meniscal or popliteal cysts. 4 Cystic masses in the supraspinatus or the spinoglenoid notch as well as hypertrophy of the inferior transverse scapular liga- ment? '5 can cause chronic inferior suprascapular nerve entrapment, j'4'6'7 This entrapment is a rare condition. 7 Severe weakness and atrophy of the spinatus muscles is associated with vague pain around the scapula that later spreads to the upper arm, and is attributed to the sensory components that carry pain fibers from the glenohumeral and the acromioclavicular joint. 3'8 Mag- netic resonance imaging (MRI) is essential for visuali- sation of the nature and extent o f the soft tissue lesion, and electromyography is needed to establish an accu- rate neurological diagnosis.
CASE REPORT
In August 1996, a 46-year-old male construction worker presented for a shoulder consultation. He was
Arthroscopy: The Journal of Arthroscopic and Related Surgery, Vol 13, No 6 (December), 1997." pp 753-755 753
754 M. H. CHOCHOLE ET AL.
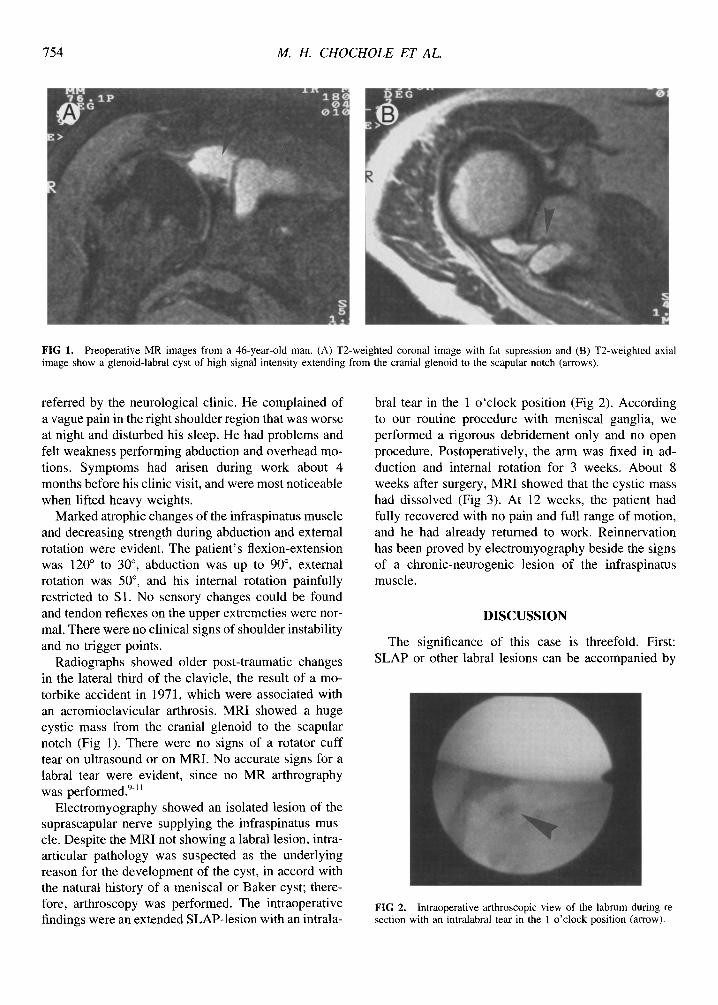
FIG 1. Preoperative MR images from a 46-year-old man. (A) T2-weighted coronal image with fat supression and (B) T2-weighted axial image show a glenoid-labral cyst of high signal intensity extending from the cranial glenoid to the scapular notch (arrows).
referred by the neurological clinic. He complained of a vague pain in the fight shoulder region that was worse at night and disturbed his sleep. He had problems and felt weakness performing abduction and overhead mo- tions. Symptoms had arisen during work about 4 months before his clinic visit, and were most noticeable when lifted heavy weights.
Marked atrophic changes of the infraspinatus muscle and decreasing strength during abduction and external rotation were evident. The patient's flexion-extension was 120 ° to 30 °, abduction was up to 90 °, external rotation was 50 ° , and his internal rotation painfully restricted to S 1. No sensory changes could be found and tendon reflexes on the upper extremeties were nor- mal. There were no clinical signs of shoulder instability and no trigger points.
Radiographs showed older post-traumatic changes in the lateral third of the clavicle, the result of a mo- torbike accident in 1971, which were associated with an acromioclavicular arthrosis. MRI showed a huge cystic mass from the cranial glenoid to the scapular notch (Fig 1). There were no signs of a rotator cuff tear on ultrasound or on MRI. No accurate signs for a labral tear were evident, since no MR arthrography was performed. 9-1~
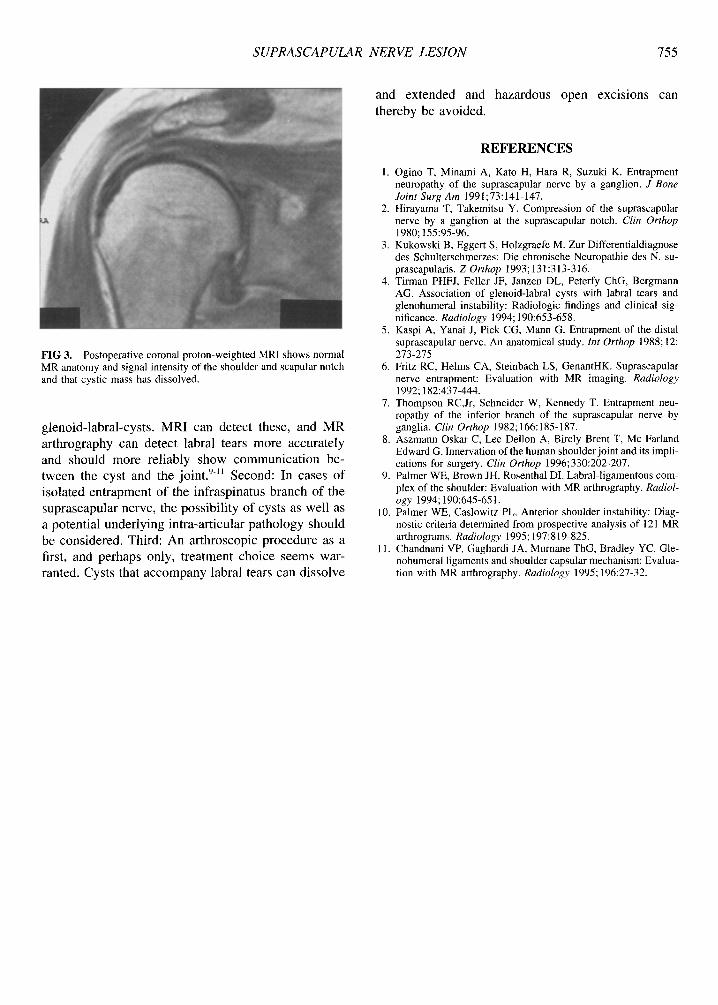
Electromyography showed an isolated lesion of the suprascapular nerve supplying the infraspinatus mus- cle. Despite the MRI not showing a labral lesion, intra- articular pathology was suspected as the underlying reason for the development of the cyst, in accord with the natural history of a meniscal or Baker cyst; there- fore, arthroscopy was performed. The intraoperative findings were an extended SLAP-lesion with an intrala-
bral tear in the 1 o 'clock position (Fig 2). According to our routine procedure with meniscal ganglia, we performed a rigorous debridement only and no open procedure. Postoperatively, the arm was fixed in ad- duction and internal rotation for 3 weeks. About 8 weeks after surgery, MRI showed that the cystic mass had dissolved (Fig 3). At 12 weeks, the patient had fully recovered with no pain and full range of motion, and he had already returned to work. Reinnervation has been proved by electromyography beside the signs of a chronic-neurogenic lesion of the infraspinatus muscle.
DISCUSSION
The significance of this case is threefold. First: SLAP or other labral lesions can be accompanied by
FIG 2. Intraoperative arthroscopic view of the labrum during re- section with an intralabral tear in the 1 o'clock position (arrow).
SUPRASCAPULAR N ERVE LESION 755
FIG 3. Postoperative coronal proton-weighted MRI shows normal MR anatomy and signal intensity of the shoulder and scapular notch and that cystic mass has dissolved.
g leno id- labra l -cys t s . M R I can detec t these, and M R
ar th rography can de tec t labral tears m o r e accura te ly
and should m o r e re l i ab ly s h o w c o m m u n i c a t i o n be-
tween the cys t and the jo in t . 9-~1 Second : In cases o f
i so la ted en t r apmen t o f the inf raspina tus b ranch o f the
suprascapula r nerve , the poss ib i l i ty o f cysts as we l l as
a po ten t ia l unde r ly ing in t ra-ar t icu lar p a t h o l o g y should
be cons idered . Third : An a r th roscop ic p rocedure as a
first, and perhaps only, t r ea tment c h o i c e seems war-
ranted. Cys ts that a c c o m p a n y labral tears can d i s so lve
and ex t ended and haza rdous open exc i s ions can
the reby be avo ided .
R E F E R E N C E S
1. Ogino T, Minami A, Kato H, Hara R, Suzuki K. Entrapment neuropathy of the suprascapular nerve by a ganglion. J Bone Joint Surg Am 1991;73:141-147.
2. Hirayama T, Takemitsu Y. Compression of the suprascapular nerve by a ganglion at the suprascapular notch. Clin Orthop 1980; 155:95-96.
3. Kukowski B, Eggert S, Holzgraefe M. Zur Differentialdiagnose des Schulterschmerzes: Die chronische Neuropathie des N. su- prascapularis. Z Orthop 1993; 131:313-316.
4. Tirman PHFJ, Feller JF, Janzen DL, Peterfy ChG, Bergmann AG. Association of glenoid-labral cysts with labral tears and glenohumeral instability: Radiologic findings and clinical sig- nificance. Radiology 1994; 190:653-658.
5. Kaspi A, Yanai J, Pick CG, Mann G. Entrapment of the distal suprascapular nerve. An anatomical study. Int Orthop 1988; 12: 273-275
6. Fritz RC, Helms CA, Steinbach LS, GenantHK. Suprascapular nerve entrapment: Evaluation with MR imaging. Radiology 1992; 182:437-444.
7. Thompson RC,Jr, Schneider W, Kennedy T. Entrapment neu- ropathy of the inferior branch of the suprascapular nerve by ganglia. Clin Orthop 1982; 166:185-187.
8. Aszmann Oskar C, Lee Dellon A, Birely Brent T, Mc Farland Edward G. Innervation of the human shoulder joint and its impli- cations for surgery. Clin Orthop 1996;330:202-207.
9. Palmer WE, Brown JH, Rosenthal DI. Labral-ligamentous com- plex of the shoulder: Evaluation with MR arthrography. Radiol- ogy 1994; 190:645-651.
10. Palmer WE, Caslowitz PL. Anterior shoulder instability: Diag- nostic criteria determined from prospective analysis of 121 MR arthrograms. Radiology 1995; 197:819-825.
11. Chandnani VP, Gagliardi JA, Murnane ThG, Bradley YC. Gle- nohumeral ligaments and shoulder capsular mechanism: Evalua- tion with MR arthrography. Radiology 1995; 196:27-32.