genetic considerations in hypertrophic cardiomyopathy
TRANSCRIPT
Progress in Cardiovascular Diseases 54 (2012) 456–460www.onlinepcd.com
Genetic Considerations in Hypertrophic CardiomyopathyCarolyn Y. Ho⁎
Cardiovascular Division, Brigham and Women's Hospital, Boston, MA
Abstract Hypertrophic cardiomyopathy (HCM) is characterized by unexplained left ventricular
Statement of ConflFunding sources: T
Health (K23 HL07890⁎ Address reprint
Division,BrighamandE-mail address: C
0033-0620/$ – see frodoi:10.1016/j.pcad.20
hypertrophy that develops in the absence of pressure overload or storage/infiltrative processes.Approximately 20 years ago, mutations in genes encoding sarcomere proteins were identified asthe cause of HCM. Although there are limitations to current clinical application, genetic testingcan identify the specific gene mutation responsible for causing HCM in patients and their family.This provides a definitive means to identify at-risk relatives, as well as new opportunities to studypathogenesis, and developing novel strategies for disease prevention and modification. (ProgCardiovasc Dis 2012;54:456-460)
© 2012 Elsevier Inc. All rights reserved.Keywords: Genetics; Hypertrophy; Cardiomyopathy
Hypertrophic cardiomyopathy (HCM) has been recog-nized to be a familial disease with autosomal-dominantinheritance for more than half a century.1 In the 1980s,linkage studies were performed in families, comparing thegenetic background of family members with HCM to thosewithout disease. These efforts led to the seminal discoverythat HCM is caused by mutations in genes encodingsarcomere proteins, including β-myosin heavy chain(MYH7), cardiac myosin binding protein C (MYBPC3),cardiac troponin T (TNNT2), cardiac troponin I (TNNI3),cardiac actin (ACTC), α-tropomyosin (TPM1), essentialmyosin light chain (MYL3), and regulatory myosin lightchain (MYL2).2 Sarcomere mutations can be found in∼50% of patients referred for clinical genetic testing;however, this yield is strongly influenced by familyhistory. Approximately 60% of adult and pediatric patientswith a family history of HCM will have a sarcomeremutation identified (positive genetic testing results). Incontrast, only ∼30% of patients without a family historywill have positive results, often due to sporadic or de novomutations that may be passed on to the next generation.2
ict of Interest: see page 459.he author is supported by the National Institutes of1 and 1P20HL101408).requests to Carolyn Y. Ho, MD, CardiovascularWomen'sHospital, 75 Francis St, Boston,[email protected].
nt matter © 2012 Elsevier Inc. All rights reserved.12.03.004
More than 1000 distinct mutations have been identified,most commonly involvingmyosin heavy chain andmyosinbinding protein C. Most mutations are unique to a singlefamily, rarely recurring in unrelated patients.
Symptoms, age of onset, pattern and extent of leftventricular hypertrophy (LVH), degree of obstruction, andrisk for sudden cardiac death can vary considerably, evenwithin the same family. Given the heterogeneity of bothgenotype and phenotype, identifying the exact mutationresponsible for disease usually does not substantiallyinfluence management or provide insight into prognosis,including the risk for sudden death. However, more severeconsequences (cardiovascular death, stroke, progressivesymptoms, systolic dysfunction) have been demonstratedin patients with HCM with sarcomere mutations thanpatients who do not have a sarcomere mutation identified.3
Gene dosage effects have also been described as patientswith more than 1 mutation (∼5% incidence) may havemore severe disease, particularly in rare situations wheremore than 2 mutations are present in a single individual, orif patients have homozygous mutations and do not expressany normal protein.4
Family evaluation
The goals of family screening are to identify relativeswith unrecognized HCM and to follow at-risk individuals
456

Abbreviations and Acronyms
HCM = hypertrophiccardiomyopathy
LVH = left ventricularhypertrophy
457C.Y. Ho / Progress in Cardiovascular Diseases 54 (2012) 456–460
for disease development,assessing risk for suddendeath as appropriate. Hy-pertrophic cardiomyopa-thy follows autosomal-dominant inheritance;therefore, each first-de-
gree relative of an affected patient has a 50% chance ofcarrying the mutation and potentially developing HCM.Because diagnosis and sudden cardiac death risk are bothlinked to the presence of LVH and because the penetranceof LVH is age dependent, clinical evaluation mustcontinue longitudinally. Screening is most frequent(annually) during adolescence and early adulthood (age,12-21 years) when LVH most commonly emerges. Earlychildhood screening is appropriate if there is a familyhistory of early-onset disease or other concerns. Duringadulthood, screening is recommended every ∼5 years orin response to clinical change because LVH can developlate in life.5,6 Genetic testing can provide importantinsights into family management by definitively identify-ing at-risk relatives—those that have inherited the family'spathogenic mutation.
Genetic testing
Although originally available only through specializedacademic research laboratories, the development of fasterand less expensive DNA sequencing methodology hasfostered the transition of genetic testing for HCM to theclinic (see www.genetests.org for further information).Commercially available testing was introduced in 2003.Genetic testing typically falls into 2 categories: diagnostic(comprehensive sequence analysis to identify a disease-causing mutation in a patient with HCM) and predictive(focused genetic testing to determine if the mutationpreviously identified in the family is present in a relative).Currently, all laboratories use a candidate-gene strategyfor diagnostic genetic testing, analyzing the sequence ofsarcomere genes as well as a small number of genesassociated with metabolic/storage and mitochondrialdisease that may mimic HCM by causing increased leftventricular wall thickness.7
Although genetic testing can provide valuable informa-tion, accurate interpretation is complex. Unlike more familiartypes of laboratory testing, genetic testing results areprobabilistic rather than binary or quantitative. This is a keyconsideration because the clinical use of genetic testing restalmost entirely on the predicted probability that the variant isdisease causing. However, it may be difficult to accuratelypredict if a DNA variant identified in a patient is truly diseasecausing (pathogenic), disease modifying, or merely a benignpolymorphism or a rare variant present in a small proportionof the general population. If the clinical significance of thevariant is unclear and not confidently predicted to be the cause
of HCM, genetic testing results are noninformative andcannot be used in a predictive manner to identify at-riskrelatives. Negative genetic testing results are also noninfor-mative. Failing to identify a mutation does not exclude thepossibility of genetic disease or obviate the need forlongitudinal clinical screening in at-risk relatives. Fur-thermore, results may evolve over time. As we gain moreexperience in sequencing reference populations in differentethnic backgrounds and in sequencing more patients andfamilies with HCM, new information may emerge. As aresult, a variant's classification as benign or pathogenicmay change substantially.
Guidelines for the management of HCM give a class Irecommendation for genetic testing in patients with anatypical clinical presentation of HCM or when anothergenetic condition is suspected to be the cause.6 Genetictesting is considered “reasonable” to facilitate theidentification of at-risk family members (class IIarecommendation). Fig 1 reviews practical considerationsto guide the use of genetic testing, focusing on familialdisease because the yield and impact of genetic testing aretypically highest in this setting.
Genetic testing should be considered a family test,rather than a test for an individual patient. Indeed, themanagement of the family member with HCM whoundergoes initial comprehensive genetic testing may notbe substantially changed by the results. The implications ofdownstream, predictive genetic testing in family membersmay be more dramatic because it allows definitiveidentification of relatives who are at risk for developingHCM from those who are not at risk. Thus, if a pathogenicsarcomere mutation is identified in the family proband,predictive genetic testing provides a cost-effective anddefinitive means of family screening. Longitudinal evalu-ation can be focused onmutation carriers because only theyare at risk for developing disease.
Other than serial clinical screening to assess for theemergence of clinically overt disease, optimal manage-ment of mutation carriers who have not yet developedLVH and a clinical diagnosis of HCM has not beenestablished. The natural history of this prehypertrophicstage is not well characterized but is likely variable,depending on the specific mutation, as well asenvironmental and genetic modifiers. Family historyand individual factors such as lifestyle and comorbid-ities are important considerations in determining follow-up. For example, earlier screening may be appropriateif there is a family history of childhood-onset disease orsudden death. More extensive evaluation may beconsidered if an apparently healthy, young mutationcarrier is a serious athlete. Formal exercise restrictionsfor preclinical mutation carriers are not advocated byUS consensus guidelines, although European Societyof Cardiology recommendations are more restrictivedue to the unknown impact of strenuous athletics inthis context.8

Fig 1. Considerations for genetic testing. Genetic testing may provide important information when trying to differentiate HCM from other genetic causes ofcardiac hypertrophy. In addition, genetic testing can be highly informative in assessing families with HCM. Genetic testing should be avoided in theabsence of diagnostic clinical features. Predictive testing should only be performed if there is a high degree of confidence that the family's mutation isdisease causing (pathogenic).
458 C.Y. Ho / Progress in Cardiovascular Diseases 54 (2012) 456–460
Future directions: characterizing early phenotypesand developing preventive treatment
Identifying the genetic basis of HCM allows uniqueopportunities to identify risk and prevent disease.Extraordinary advances have been made in characteriz-ing the genetics underlying HCM. For true preventivemedicine to be developed, more knowledge is needed todefine the precise steps that lead from mutation todisease, including steps that could be targeted tointerrupt phenotypic progression. With this knowledge,we will be able to achieve the ultimate goal: changingthe natural history of sarcomere mutations to prevent thedevelopment of HCM.
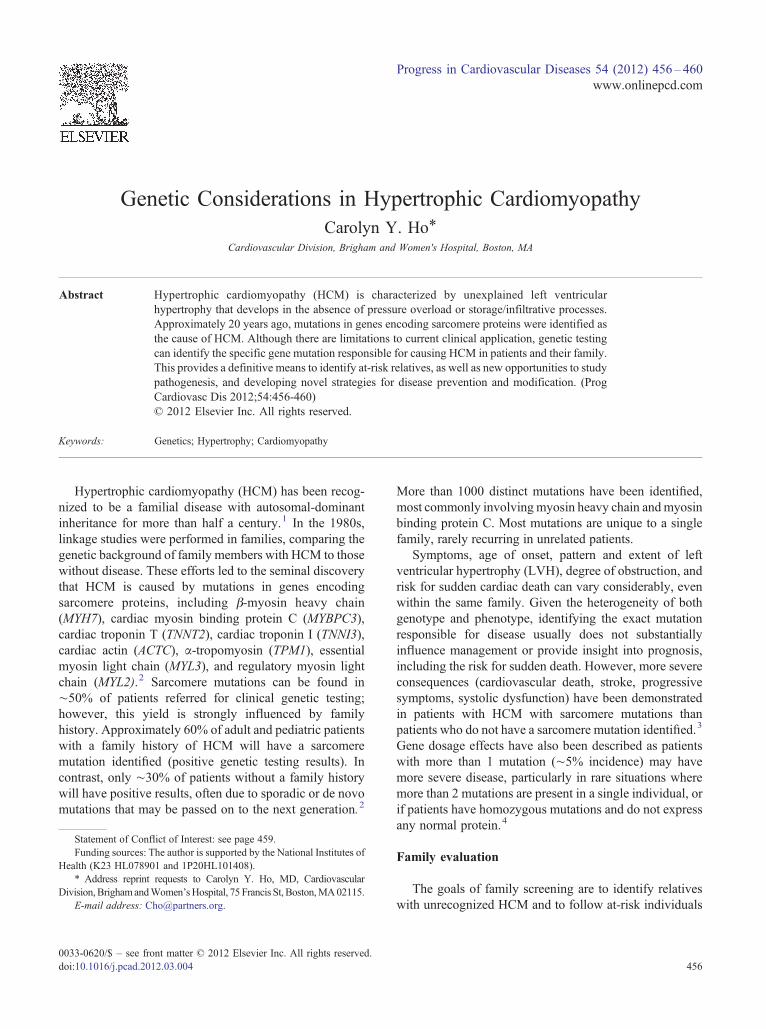
Rudimentary disease prevention based on genetictesting is currently available in the form of assistedreproduction using preimplantation genetic diagnosis(PGD). With PGD, in vitro fertilization is performed,and a single cell is removed from early-stage embryosfor genetic testing to determine if the family's pathogenicmutation is present or absent (Fig 2). Only embryoswithout evidence of the mutation are used to initiatepregnancy. The decision to pursue PGD is clearly ahighly personal one. It requires confidence that the DNAvariant identified in the family is the cause of HCM, andit mandates the use of in vitro fertilization. This optionmay be a particular consideration for families in whomdisease expression is consistently malignant.
Disease-modifying studies are in active developmentin animal models of HCM. For example, mouse modelsof HCM have demonstrated that abnormalities in
intracellular calcium handling may be one of the earliestmanifestations of sarcomere mutations.9,10 These abnor-malities are demonstrable at ∼4 weeks of age; far inadvance of diastolic abnormalities (age, ∼6 weeks) andmicroscopic LVH, fibrosis, and disarray (age, ∼20-25weeks). Early treatment with the L-type calcium channelblocker, diltiazem, appeared to attenuate the develop-ment of LVH and fibrosis if started early in life whilecardiac morphology was still normal.10 These studieshave several intriguing clinical implications. Theysuggest a mechanistic link between calcium imbalanceand disease development. Moreover, they provide someof the first evidence that mechanism-based pharmaco-logic therapy may influence the natural history of HCM.To test the feasibility of this strategy, a pilot humanrandomized control trial was initiated, comparingdiltiazem to placebo in sarcomere mutation carrierswho have not yet developed LVH (http://clinicaltrials.gov/ct2/show/NCT00319982).
More recently, early treatment with the angiotensin IIreceptor blocker, losartan, in prehypertrophic HCM micehas also shown promise in decreasing the developmentof fibrosis and LVH. This effect may be mediatedthrough its inhibition of transforming growth factor β–mediated pathways.11 In these studies, losartan was alsounable to reverse established hypertrophy, again empha-sizing the potential importance of early treatment andpreventive strategies.
Progress is being made in translating these basicdiscoveries to human disease. By studying sarcomeremutation carriers before clinical diagnosis with HCM,
Fig 2. Preimplantation genetic testing. Genetic testing is performed on embryos before implantation to attempt achieving a pregnancy that does not carry thefamily's pathogenic mutation.
459C.Y. Ho / Progress in Cardiovascular Diseases 54 (2012) 456–460
we can more precisely characterize the early consequencesof these mutations, improving our understanding ofhow HCM develops. Such studies have demonstratedthat diastolic abnormalities,12 impaired myocardialenergetics,13 increased collagen synthesis,14 and ECGabnormalities15 are present in sarcomere mutation carrierswhen left ventricular wall thickness is normal. Confirma-tory studies and longitudinal evaluation are needed toclarify how these early phenotypes relate to diseasedevelopment and to serious consequences of HCM, suchas heart failure and sudden death. Such collaborativebasic science and clinical investigation will help us usegenetic insights to truly transform medicine by identifyingat-risk individuals early in life, before clinical diagnosis;refining understanding of disease pathogenesis; and,ultimately, developing new treatment paradigms to slowor prevent disease development, rather than simplypalliating symptoms.
Statement of Conflict of Interest
All authors declare that there are no conflicts of interest.
References
1. Hollman A, Goodwin JF, Teare D, et al: A family with obstructivecardiomyopathy (asymmetrical hypertrophy). Br Heart J 1960;22:449-456.
2. Konno T, Chang S, Seidman JG, et al: Genetics of hypertrophiccardiomyopathy. Curr Opin Cardiol 2010.
3. Olivotto I, Girolami F, Ackerman MJ, et al: Myofilament proteingene mutation screening and outcome of patients with hypertrophiccardiomyopathy. Mayo Clin Proc 2008;83:630-638.
4. Girolami F, Ho CY, Semsarian C, et al: Clinical features and outcomeof hypertrophic cardiomyopathy associated with triple sarcomereprotein gene mutations. J Am Coll Cardiol 55:1444-53.
5. Maron BJ, McKenna WJ, Danielson GK, et al: American College ofCardiology/European Society of Cardiology clinical expert consensusdocument on hypertrophic cardiomyopathy. A report of the American

460 C.Y. Ho / Progress in Cardiovascular Diseases 54 (2012) 456–460
College of Cardiology Foundation Task Force on Clinical ExpertConsensus Documents and the European Society of CardiologyCommittee for Practice Guidelines. J Am Coll Cardiol 2003;42:1687-1713.
6. Gersh BJ, Maron BJ, Bonow RO, et al: 2011 ACCF/AHA guidelinefor the diagnosis and treatment of hypertrophic cardiomyopathy:executive summary: a report of the American College of CardiologyFoundation/American Heart Association Task Force on PracticeGuidelines. Circulation 2011.
7. Arad M, Maron BJ, Gorham JM, et al: Glycogen storage diseasespresenting as hypertrophic cardiomyopathy. N Engl J Med2005;352:362-372.
8. Pelliccia A, Zipes DP, Maron BJ: Bethesda Conference #36 and theEuropean Society of Cardiology Consensus Recommendationsrevisited a comparison of U.S. and European criteria for eligibilityand disqualification of competitive athletes with cardiovascularabnormalities. J Am Coll Cardiol 2008;52:1990-1996.
9. Fatkin D, McConnell BK, Mudd JO, et al: An abnormal Ca(2+)response in mutant sarcomere protein–mediated familial hypertro-phic cardiomyopathy. J Clin Invest 2000;106:1351-1359.
10. Semsarian C, Ahmad I, Giewat M, et al: The L-type calcium channelinhibitor diltiazem prevents cardiomyopathy in a mouse model.J Clin Invest 2002;109:1013-1020.
11. Teekakirikul P, Eminaga S, Toka O, et al: Cardiac fibrosis in mice withhypertrophic cardiomyopathy is mediated by non-myocyte prolifera-tion and requires TGF-beta. J Clin Invest 2010;120:3520-3529.
12. Ho CY, Sweitzer NK, McDonough B, et al: Assessment ofdiastolic function with Doppler tissue imaging to predictgenotype in preclinical hypertrophic cardiomyopathy. Circulation2002;105:2992-2997.
13. Crilley JG, Boehm EA, Blair E, et al: Hypertrophic cardiomyopathydue to sarcomeric gene mutations is characterized by impairedenergy metabolism irrespective of the degree of hypertrophy. J AmColl Cardiol 2003;41:1776-1782.
14. Ho CY, Lopez B, Coelho-Filho OR, et al: Myocardial fibrosis as anearly manifestation of hypertrophic cardiomyopathy. N Engl J Med2010;363:552-563.
15. Lakdawala NK, Thune JJ, Maron BJ, et al: Electrocardiographicfeatures of sarcomeremutation carrierswith andwithout clinically overthypertrophic cardiomyopathy. J Am cardiol 2011;108:1606-1613.