gender-specific clinicopathological features and survival in patients with renal cell carcinoma...
TRANSCRIPT
BJUIB J U I N T E R N A T I O N A L
© 2 0 11 T H E A U T H O R S
B J U I N T E R N A T I O N A L © 2 0 11 B J U I N T E R N A T I O N A L | doi:10.1111/j.1464-410X.2011.10667.x 1
What ’ s known on the subject? and What does the study add? There has been some controversy about the gender differences in survival in patients with RCC.
Korean women with RCC had a lower proportion of clear cell histology and a higher proportion of chromophobe histology. This histological difference might have driven the better survival rates in Korean women.
OBJECTIVE
• To assess whether there are gender-specifi c differences in the clinicopathological features and prognosis in a large cohort of Korean patients with renal cell carcinoma (RCC) compared with Western patients.
PATIENTS AND METHODS
• Medical records of 1616 patients clinically diagnosed with RCC who underwent partial or radical nephrectomy were analysed between January 1988 and July 2009. • In all, 1508 patients diagnosed with RCC based on pathology reports were included for evaluation. • The mean follow-up period was 73.1 months. • The gender-specifi c differences in the clinicopathological features and survival
rates were evaluated using the Kaplan – Meier method and Cox proportional hazards models.
RESULTS
• Of the 1508 patients, 439 (29.1%) were women. • Korean men had a higher proportion of clear cell histology (84.3% vs 72.0%, P < 0.001) and a lower percentage of chromophobe histology (5.2% vs 12.5%, P < 0.001) than Korean women. • There were no gender-specifi c differences in pathological T stage, positive lymph nodes or distant metastases, or Fuhrman ’ s nuclear grade ( P > 0.05). • For both cancer-specifi c and overall survival, Kaplan – Meier curves showed that
women had a better survival rate than men ( P = 0.039 and P = 0.015, respectively).
CONCLUSIONS
• Korean women with RCC had signifi cantly better survival rates than Korean men. • Additionally, Korean women with RCC had a lower proportion of clear cell histology and a higher proportion of chromophobe histology. • This histological difference might have driven the better survival rates in Korean women.
KEYWORDS
renal cell carcinoma , prognosis , gender , nephrectomy
Study Type – Therapy (case series) Level of Evidence 4
Gender-specifi c clinicopathological features and survival in patients with renal cell carcinoma (RCC) Sangchul Lee , Hwang Gyun Jeon * , Cheol Kwak , Hyeon Hoe Kim , Seok-Soo Byun † , Sang Eun Lee † and Eunsik Lee Department of Urology, Seoul National University Hospital, Seoul , * Department of Urology, CHA Bundang Medical Center, CHA University , and † Department of Urology, Seoul National University Bundang Hospital, Seongnam, Korea
INTRODUCTION
Globally, RCC occurs nearly twice as often in men than in women [ 1,2 ] . Korean men have also shown this higher incidence compared with Korean women [ 3 ] . The age-adjusted incidence rates of RCC in Korean men and women according to the Korean cancer registry system in 2007 were 7.1 and 2.8 per 100 000 person-years, respectively [ 3 ] .
Reproductive factors including parity, maternal age at fi rst birth, use of hormone replacement therapy, and use of oral contraceptives may be related to this gender-specifi c difference in incidence rates [ 4,5 ] .
It has been observed that women have better survival rates after radical and partial nephrectomy than men, although the reason
for this survival advantage is unclear [ 6 ] . Previous studies on gender-specifi c clinicopathological features and survival rates in RCC mostly involved patients from the USA or European countries. Little has been reported about the gender-specifi c features of Asian patients with RCC. Well-known prognostic factors for RCC include anatomical (e.g. TNM classifi cation and tumour size), histological (e.g. Fuhrman
Accepted for publication 27 July 2011

L E E E T A L .
© 2 0 11 T H E A U T H O R S
2 B J U I N T E R N A T I O N A L © 2 0 11 B J U I N T E R N A T I O N A L
grade and histological subtype), clinical (e.g. symptoms and performance status), and molecular features (e.g. p53 and carbonic anhydrase IX) [ 7 ] . Gender has also been reported as a prognostic factor in RCC [ 8 ] . Racial and ethnic differences in the incidence and survival of patients with RCC have been reported. Asian-Americans had a lower incidence rate and higher survival rate than all other races and ethnicities in the USA [ 2,9 ] . Both gender-specifi c and racial differences in incidence and survival of patients with RCC may be related to various factors, including genetic, clinicopathological, and environmental factors.
Our main objectives were to investigate gender-specifi c differences in the clinicopathological features and prognoses in Korean patients with RCC and to evaluate the racial and ethnic differences between Korean and Western populations.
PATIENTS AND METHODS
Data from 1616 consecutive patients clinically diagnosed with solitary RCC who underwent radical or partial nephrectomy at the Seoul National University Hospital in Korea between January 1988 and July 2009 were retrospectively analysed. This study was approved by the Institutional Review Board of Seoul National University Hospital.
Among the 1616 patients, 1508 patients (93.3%) were diagnosed with RCC based on pathology reports. The other 108 patients (6.7%) were diagnosed with benign diseases, including renal angiomyolipoma (55 patients), oncocytoma (26), cystic nephroma (eight), cysts (four), and other benign conditions (15). Women (58/497) had a higher percentage of benign pathology than men (51/1120). All patients diagnosed with benign renal tumours (108) were excluded from further study.
Of the remaining 1508 patients, only those who received regular follow-up care (i.e. physical examination, chest radiography, and abdominal CT) were included for further study.
The entire cohort of 1508 was divided according to gender. The clinical characteristics at the time of diagnosis including age, body mass index (BMI),
presenting symptoms, and Eastern Cooperative Oncology Group (ECOG) performance status, were evaluated.
The pathological data, including tumour size (the largest tumour diameter), histological subtype, sarcomatoid differentiation, tumour necrosis, the Fuhrman nuclear grade, and pathological stage, were reviewed by an expert uropathologist. All tumours were staged according to the seventh edition of the American Joint Committee on Cancer (AJCC) staging manual. The AJCC pathological stage group was used and supplemented by the AJCC clinical stage group when the pathological stage was not recorded. Any tumours diagnosed based on the previous edition were re-staged using the AJCC seventh edition rules [ 10 ] .
The clinicopathological variables were evaluated using chi-squared, Fisher ’ s exact tests, and the independent t -test. Cancer-specifi c survival (CSS) and overall survival (OS) were evaluated for men and women using the Kaplan – Meier method. CSS was defi ned as the time from initial diagnosis of RCC to death caused by RCC. The follow-up duration was calculated from the date of surgery to the date of death or the last follow-up visit. The Cox proportional hazard ratio (HR) was used to determine the signifi cant factors related to survival. All P values were two-sided, with P < 0.05 considered to indicate statistical signifi cance.
RESULTS
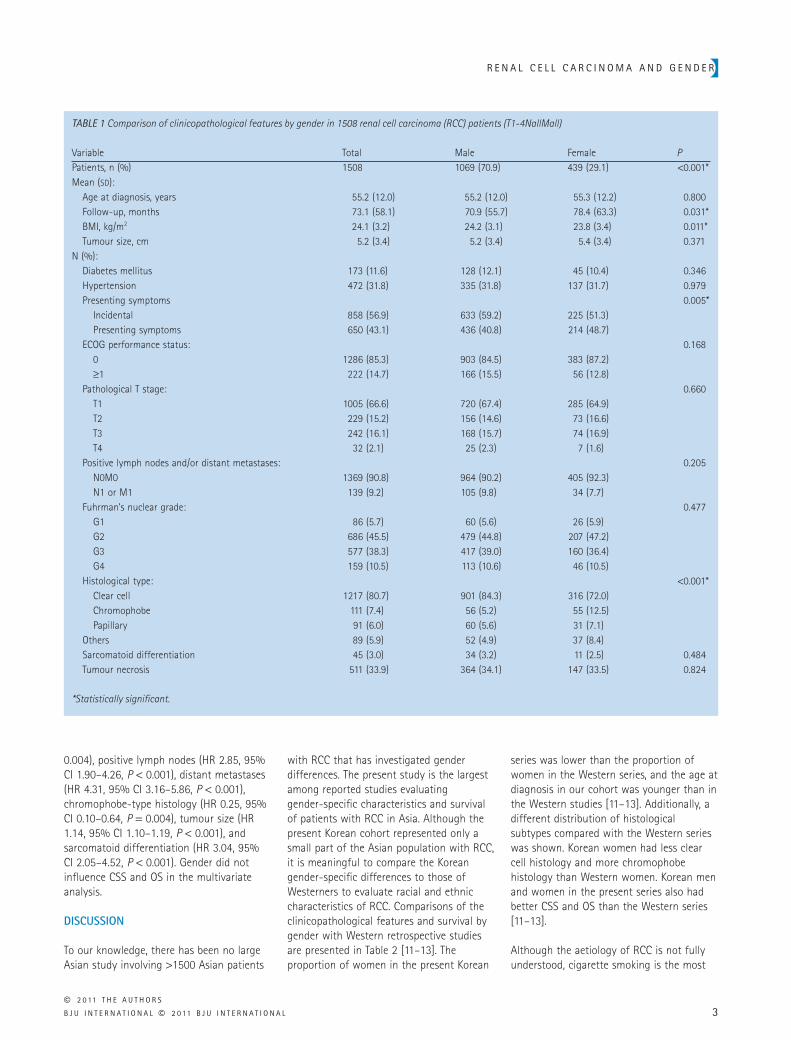
Comparisons of the clinicopathological features by gender among the 1508 patients with RCC are shown in Table 1 . More than 70% of the patients were men. There were no statistically signifi cant differences in age at diagnosis, ECOG performance status, diabetes mellitus, hypertension, tumour size, pathological T stage, positive lymph nodes or distant metastases, Fuhrman ’ s nuclear grade, sarcomatoid differentiation, and tumour necrosis between men and women. There were some clinical differences in BMI and the presence of presenting symptoms at the time of diagnosis. The mean BMI was 24.2 kg/m 2 for men and 23.8 kg/m 2 for women ( P = 0.011). The proportion of patients with presenting symptoms at diagnosis were 40.8% for men and 48.7%
for women ( P = 0.005). There were pathologically distinct differences in histological subtype distribution between men and women ( P < 0.001). In the subgroup analysis, men had a signifi cantly higher proportion of clear cell type RCC than women (84.3% vs 72.0%, P < 0.001). The proportion of chromophobe-type RCC in men was signifi cantly lower than in women (5.2% vs 12.5%, P < 0.001). However, there was no signifi cant gender-specifi c difference in the incidence of papillary type RCC by subgroup analysis ( P = 0.283).
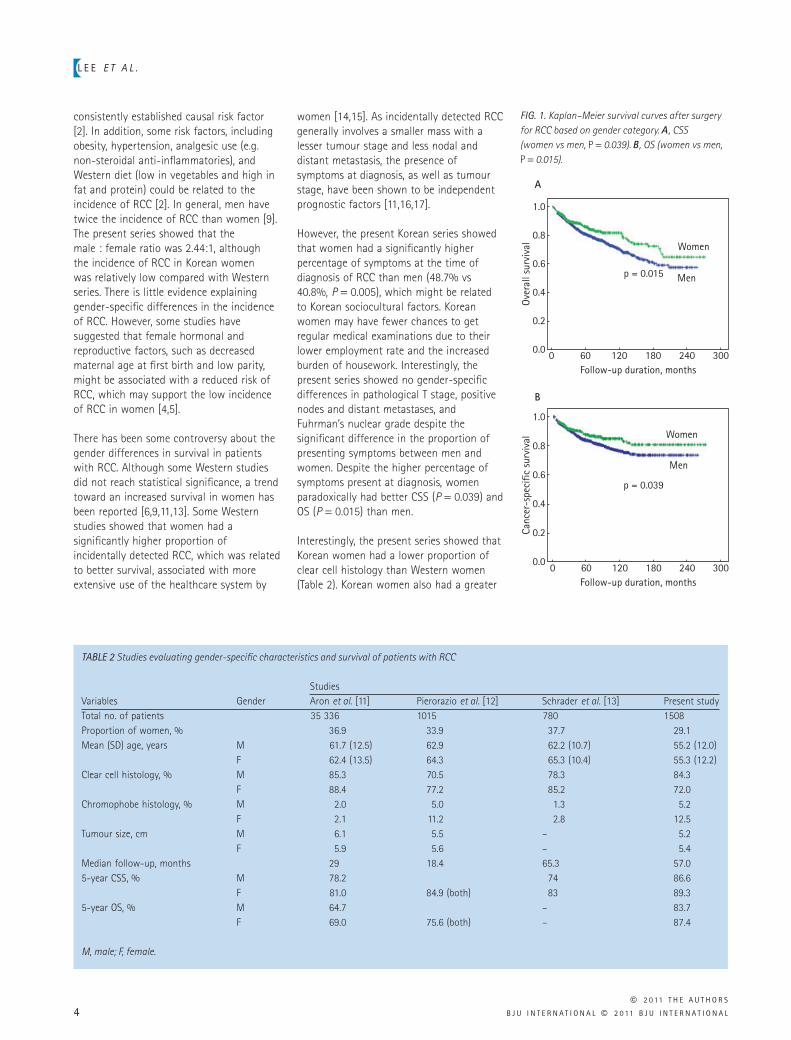
Figure 1 shows the Kaplan – Meier survival curve for CSS and OS between men and women. Women had signifi cantly better CSS ( P = 0.039) and OS ( P = 0.015) than men. The 5-year CSS was 83.7% for men and 87.4% for women. The 10-year CSS was 76.5% for men and 84.9% for women. The 5-year OS was 80.4% for men and 85.6% for women. The 10-year OS was 70.3% for men and 81.4% for women. Factors that signifi cantly infl uenced CSS in the univariate analysis were gender ( P = 0.039), age at diagnosis ( P < 0.001), presenting symptoms at diagnosis ( P < 0.001), ECOG performance status ( P < 0.001), BMI ( P < 0.001), T stage ( P < 0.001), lymph node or distant metastases ( P < 0.001), Fuhrman ’ s nuclear grade ( P < 0.001), chromophobe-type histology ( P = 0.001), tumour size ( P < 0.001), sarcomatoid differentiation ( P < 0.001), microvascular invasion ( P < 0.001), and tumour necrosis ( P < 0.001). Factors that signifi cantly infl uenced OS in the univariate analysis were the same as those affecting CSS. Independent factors affecting CSS in the multivariate analysis were age at diagnosis (HR 1.03, 95% CI 1.02 – 1.04, P < 0.001), presenting symptoms at diagnosis (HR 1.62, 95% CI 1.17 – 2.25, P = 0.004), BMI (HR 0.94, 95% CI 0.90 – 0.99, P = 0.020), positive lymph nodes (HR 2.94, 95% CI 1.92 – 4.49, P < 0.001), distant metastases (HR 4.97, 95% CI 3.55 – 6.97, P < 0.001), chromophobe-type histology (HR 0.21, 95% CI 0.07 – 0.61, P = 0.004), tumour size (HR 1.13, 95% CI 1.08 – 1.19, P < 0.001), microvascular invasion (HR 1.58, 95% CI 1.13 – 2.21, P = 0.007), and sarcomatoid differentiation (HR 2.87, 95% CI 1.88 – 4.40, P < 0.001). Independent factors having an infl uence on OS in the multivariate analysis were age at diagnosis (HR 1.05, 95% CI 1.04 – 1.06, P < 0.001), presenting symptoms at diagnosis (HR 1.38, 95% CI 1.06 – 1.80, P = 0.018), BMI (HR 0.94, 95% CI 0.90 – 0.98, P =
R E N A L C E L L C A R C I N O M A A N D G E N D E R
© 2 0 11 T H E A U T H O R S
B J U I N T E R N A T I O N A L © 2 0 11 B J U I N T E R N A T I O N A L 3
0.004), positive lymph nodes (HR 2.85, 95% CI 1.90 – 4.26, P < 0.001), distant metastases (HR 4.31, 95% CI 3.16 – 5.86, P < 0.001), chromophobe-type histology (HR 0.25, 95% CI 0.10 – 0.64, P = 0.004), tumour size (HR 1.14, 95% CI 1.10 – 1.19, P < 0.001), and sarcomatoid differentiation (HR 3.04, 95% CI 2.05 – 4.52, P < 0.001). Gender did not infl uence CSS and OS in the multivariate analysis.
DISCUSSION
To our knowledge, there has been no large Asian study involving > 1500 Asian patients
with RCC that has investigated gender differences. The present study is the largest among reported studies evaluating gender-specifi c characteristics and survival of patients with RCC in Asia. Although the present Korean cohort represented only a small part of the Asian population with RCC, it is meaningful to compare the Korean gender-specifi c differences to those of Westerners to evaluate racial and ethnic characteristics of RCC. Comparisons of the clinicopathological features and survival by gender with Western retrospective studies are presented in Table 2 [ 11 – 13 ] . The proportion of women in the present Korean
series was lower than the proportion of women in the Western series, and the age at diagnosis in our cohort was younger than in the Western studies [ 11 – 13 ] . Additionally, a different distribution of histological subtypes compared with the Western series was shown. Korean women had less clear cell histology and more chromophobe histology than Western women. Korean men and women in the present series also had better CSS and OS than the Western series [ 11 – 13 ] .
Although the aetiology of RCC is not fully understood, cigarette smoking is the most
TABLE 1 Comparison of clinicopathological features by gender in 1508 renal cell carcinoma (RCC) patients (T1-4NallMall)
Variable Total Male Female P Patients, n (%) 1508 1069 (70.9) 439 (29.1) < 0.001 * Mean ( SD ): Age at diagnosis, years 55.2 (12.0) 55.2 (12.0) 55.3 (12.2) 0.800 Follow-up, months 73.1 (58.1) 70.9 (55.7) 78.4 (63.3) 0.031 * BMI, kg/m 2 24.1 (3.2) 24.2 (3.1) 23.8 (3.4) 0.011 * Tumour size, cm 5.2 (3.4) 5.2 (3.4) 5.4 (3.4) 0.371N (%): Diabetes mellitus 173 (11.6) 128 (12.1) 45 (10.4) 0.346 Hypertension 472 (31.8) 335 (31.8) 137 (31.7) 0.979 Presenting symptoms 0.005 * Incidental 858 (56.9) 633 (59.2) 225 (51.3) Presenting symptoms 650 (43.1) 436 (40.8) 214 (48.7) ECOG performance status: 0.168 0 1286 (85.3) 903 (84.5) 383 (87.2) ≥ 1 222 (14.7) 166 (15.5) 56 (12.8) Pathological T stage: 0.660 T1 1005 (66.6) 720 (67.4) 285 (64.9) T2 229 (15.2) 156 (14.6) 73 (16.6) T3 242 (16.1) 168 (15.7) 74 (16.9) T4 32 (2.1) 25 (2.3) 7 (1.6) Positive lymph nodes and/or distant metastases: 0.205 N0M0 1369 (90.8) 964 (90.2) 405 (92.3) N1 or M1 139 (9.2) 105 (9.8) 34 (7.7) Fuhrman ’ s nuclear grade: 0.477 G1 86 (5.7) 60 (5.6) 26 (5.9) G2 686 (45.5) 479 (44.8) 207 (47.2) G3 577 (38.3) 417 (39.0) 160 (36.4) G4 159 (10.5) 113 (10.6) 46 (10.5) Histological type: < 0.001 * Clear cell 1217 (80.7) 901 (84.3) 316 (72.0) Chromophobe 111 (7.4) 56 (5.2) 55 (12.5) Papillary 91 (6.0) 60 (5.6) 31 (7.1) Others 89 (5.9) 52 (4.9) 37 (8.4) Sarcomatoid differentiation 45 (3.0) 34 (3.2) 11 (2.5) 0.484 Tumour necrosis 511 (33.9) 364 (34.1) 147 (33.5) 0.824
* Statistically signifi cant.
L E E E T A L .
© 2 0 11 T H E A U T H O R S
4 B J U I N T E R N A T I O N A L © 2 0 11 B J U I N T E R N A T I O N A L
consistently established causal risk factor [ 2 ] . In addition, some risk factors, including obesity, hypertension, analgesic use (e.g. non-steroidal anti-infl ammatories), and Western diet (low in vegetables and high in fat and protein) could be related to the incidence of RCC [ 2 ] . In general, men have twice the incidence of RCC than women [ 9 ] . The present series showed that the male : female ratio was 2.44:1, although the incidence of RCC in Korean women was relatively low compared with Western series. There is little evidence explaining gender-specifi c differences in the incidence of RCC. However, some studies have suggested that female hormonal and reproductive factors, such as decreased maternal age at fi rst birth and low parity, might be associated with a reduced risk of RCC, which may support the low incidence of RCC in women [ 4,5 ] .
There has been some controversy about the gender differences in survival in patients with RCC. Although some Western studies did not reach statistical signifi cance, a trend toward an increased survival in women has been reported [ 6,9,11,13 ] . Some Western studies showed that women had a signifi cantly higher proportion of incidentally detected RCC, which was related to better survival, associated with more extensive use of the healthcare system by
women [ 14,15 ] . As incidentally detected RCC generally involves a smaller mass with a lesser tumour stage and less nodal and distant metastasis, the presence of symptoms at diagnosis, as well as tumour stage, have been shown to be independent prognostic factors [ 11,16,17 ] .
However, the present Korean series showed that women had a signifi cantly higher percentage of symptoms at the time of diagnosis of RCC than men (48.7% vs 40.8%, P = 0.005), which might be related to Korean sociocultural factors. Korean women may have fewer chances to get regular medical examinations due to their lower employment rate and the increased burden of housework. Interestingly, the present series showed no gender-specifi c differences in pathological T stage, positive nodes and distant metastases, and Fuhrman ’ s nuclear grade despite the signifi cant difference in the proportion of presenting symptoms between men and women. Despite the higher percentage of symptoms present at diagnosis, women paradoxically had better CSS ( P = 0.039) and OS ( P = 0.015) than men.
Interestingly, the present series showed that Korean women had a lower proportion of clear cell histology than Western women ( Table 2 ). Korean women also had a greater
TABLE 2 Studies evaluating gender-specifi c characteristics and survival of patients with RCC
Variables GenderStudiesAron et al. [ 11 ] Pierorazio et al. [ 12 ] Schrader et al. [ 13 ] Present study
Total no. of patients 35 336 1015 780 1508Proportion of women, % 36.9 33.9 37.7 29.1Mean (SD) age, years M 61.7 (12.5) 62.9 62.2 (10.7) 55.2 (12.0)
F 62.4 (13.5) 64.3 65.3 (10.4) 55.3 (12.2)Clear cell histology, % M 85.3 70.5 78.3 84.3
F 88.4 77.2 85.2 72.0Chromophobe histology, % M 2.0 5.0 1.3 5.2
F 2.1 11.2 2.8 12.5Tumour size, cm M 6.1 5.5 – 5.2
F 5.9 5.6 – 5.4Median follow-up, months 29 18.4 65.3 57.05-year CSS, % M 78.2 74 86.6
F 81.0 84.9 (both) 83 89.35-year OS, % M 64.7 – 83.7
F 69.0 75.6 (both) – 87.4
M, male; F, female.
p = 0.015 Men
1.0
A
B
0.8
0.6
0.4
0.2
Ove
rall
surv
ival
0.00 60 120
Follow-up duration, months180 240 300
Women
p = 0.039
Men
1.0
0.8
0.6
0.4
0.2Canc
er-s
peci
fic s
urvi
val
0.00 60 120
Follow-up duration, months180 240 300
Women
FIG. 1. Kaplan – Meier survival curves after surgery for RCC based on gender category. A , CSS (women vs men, P = 0.039). B , OS (women vs men, P = 0.015).

R E N A L C E L L C A R C I N O M A A N D G E N D E R
© 2 0 11 T H E A U T H O R S
B J U I N T E R N A T I O N A L © 2 0 11 B J U I N T E R N A T I O N A L 5
proportion of chromophobe histology than Korean men (5.2% vs 12.5%, P < 0.001). In addition, the present series retained chromophobe histology as a good prognostic factor for RCC in the multivariate analysis (HR 0.25, 95% CI 0.10 – 0.64, P = 0.004). The sex differences in RCC histological subtype might affect gender-specifi c survival. Some studies reported that histological subtype had a signifi cant association with disease-specifi c survival at univariate analysis [ 18,19 ] . However, Western studies showed that the prognostic value of histological subtype disappeared at the multivariate analysis because prognosis might be more infl uenced by TNM stage and Fuhrman grade [ 18,19 ] . In addition, the presence of sarcomatoid differentiation and tumour necrosis have been considered potential histological prognostic factors in RCC [ 7,20,21 ] . The present series showed no signifi cant differences between men and women for the presence of sarcomatoid differentiation, tumour necrosis, TNM stage, and Fuhrman grade. In the present Korean series, the prognostic value of the histological subtype in gender-specifi c survival may be more important than in the Western series.
Few studies have examined the racial and ethnic differences in RCC. Asians and Pacifi c Islanders were reported to have a lower incidence of RCC and higher survival rates than all other races and ethnicities [ 9 ] . The clinicopathological characteristics of the Asian population with RCC may be related to the lower incidence and better survival rate in the Asian population. Genetics, lifestyle, diet, and environmental exposures may contribute to these racial and ethnic differences [ 9,22 ] .
In the present study, Kaplan – Meier curves showed that women had signifi cantly better CSS and OS compared with men. Meanwhile, multivariate analysis showed that gender was not a statistically signifi cant predictor of CSS and OS. The independent predictors showing signifi cant gender-specifi c differences in terms of clinical views were symptoms at the time of diagnosis of RCC and histological subtype. The aforementioned explanation may be applied to the potential association between RCC and gender. It can be cautiously assumed that other more powerful prognostic factors may hinder the effect of gender as a prognostic variable in multivariate analysis.
The limitations of the present study include its retrospective nature. Also, we could not assess the patients that did not undergo surgical management, who were clinically diagnosed with RCC. In addition, our analyses lacked specifi c data on patients ’ reproductive factors and socioeconomic factors associated with use of the healthcare system.
In conclusion, Korean women with RCC had signifi cantly better survival rates than Korean men, although gender was a statistically non-signifi cant predictor of CSS and OS in multivariate analysis. Additionally, Korean women with RCC had a lower proportion of clear cell histology and a higher proportion of chromophobe histology. This histological difference might have driven the better CSS and OS in Korean women.
ACKNOWLEDGEMENTS
Institutional Review Board (IRB) approval number: H-1006-093-322.
CONFLICT OF INTEREST
None declared.
REFERENCES
1 Curado MP , Edwards B , Shin HR et al . Cancer Incidence in Five Continents . Lyon : International Agency for Research on Cancer , 2009
2 Lipworth L , Tarone RE , McLaughlin JK . The epidemiology of renal cell carcinoma . J Urol 2006 ; 176 : 2353 – 8
3 Headquarters of Korean Central Cancer Registry . Cancer registry system in Korea . 2007 . Available at: http://ncc.re.kr . Accessed September 2011
4 Lee JE , Hankinson SE , Cho E . Reproductive factors and risk of renal cell cancer: the Nurses ’ Health Study . Am J Epidemiol 2009 ; 169 : 1243 – 50
5 Kabat GC , Silvera SA , Miller AB et al . A cohort study of reproductive and hormonal factors and renal cell cancer risk in women . Br J Cancer 2007 ; 96 : 845 – 9
6 Woldrich JM , Mallin K , Ritchey J et al . Sex differences in renal cell cancer presentation and survival: an analysis of
the National Cancer Database, 1993 – 2004 . J Urol 2008 ; 179 : 1709 – 13
7 Volpe A , Patard JJ . Prognostic factors in renal cell carcinoma . World J Urol 2010 ; 28 : 319 – 27
8 Kutikov A , Egleston BL , Wong YN et al . Evaluating overall survival and competing risks of death in patients with localized renal cell carcinoma using a comprehensive nomogram . J Clin Oncol 2010 ; 28 : 311 – 7
9 Stafford HS , Saltzstein SL , Shimasaki S et al . Racial/ethnic and gender disparities in renal cell carcinoma incidence and survival . J Urol 2008 ; 179 : 1704 – 8
10 Edge SB , Byrd DR , Compton CC et al . The american joint committee on cancer: the 7th edition of the AJCC cancer staging manual and the future of TNM . Ann Surg Oncol 2010 ; 17 : 1471 – 4
11 Aron M , Nguyen MM , Stein RJ et al . Impact of gender in renal cell carcinoma: an analysis of the SEER database . Eur Urol 2008 ; 54 : 133 – 40
12 Pierorazio PM , Murphy AM , Benson MC et al . Gender discrepancies in the diagnosis of renal cortical tumors . World J Urol 2007 ; 25 : 81 – 5
13 Schrader AJ , Sevinc S , Olbert PJ et al . Gender-specifi c characteristics and survival of renal cell carcinoma . Urologe A 2008 ; 47 : 1182 – 6
14 Tsui KH , Shvarts O , Smith RB et al . Renal cell carcinoma: prognostic signifi cance of incidentally detected tumors . J Urol 2000 ; 163 : 426 – 30
15 Beisland C , Medby PC , Beisland HO . Renal cell carcinoma: gender difference in incidental detection and cancer-specifi c survival . Scand J Urol Nephrol 2002 ; 36 : 414 – 8
16 Ficarra V , Prayer-Galetti T , Novella G et al . Incidental detection beyond pathological factors as prognostic predictor of renal cell carcinoma . Eur Urol 2003 ; 43 : 663 – 9
17 Lam JS , Shvarts O , Pantuck AJ . Changing concepts in the surgical management of renal cell carcinoma . Eur Urol 2004 ; 45 : 692 – 705
18 Gudbjartsson T , Hardarson S , Petursdottir V et al . Histological subtyping and nuclear grading of renal cell carcinoma and their implications for survival: a retrospective nation-wide study of 629 patients . Eur Urol 2005 ; 48 : 593 – 600
L E E E T A L .
© 2 0 11 T H E A U T H O R S
6 B J U I N T E R N A T I O N A L © 2 0 11 B J U I N T E R N A T I O N A L
19 Patard JJ , Leray E , Rioux-Leclercq N et al . Prognostic value of histologic subtypes in renal cell carcinoma: a multicenter experience . J Clin Oncol 2005 ; 23 : 2763 – 71
20 Lee SE , Byun SS , Oh JK et al . Signifi cance of macroscopic tumor necrosis as a prognostic indicator for renal cell carcinoma . J Urol 2006 ; 176 : 1332 – 7
21 Cheville JC , Lohse CM , Zincke H et al .
Sarcomatoid renal cell carcinoma: an examination of underlying histologic subtype and an analysis of associations with patient outcome . Am J Surg Pathol 2004 ; 28 : 435 – 41
22 Tarabeia J , Kaluski DN , Barchana M et al . Renal cell cancer in Israel: sex and ethnic differences in incidence and mortality, 1980 – 2004 . Cancer Epidemiol 2010 ; 34 : 226 – 31
Correspondence: Eunsik Lee, Department of Urology, Seoul National University Hospital, 28, Yongon-dong, Chongno-gu Seoul 110-744, Korea. e-mail: [email protected]
Abbreviations : CSS , cancer-specifi c survival ; OS , overall survival ; AJCC , American Joint Committee on Cancer ; BMI , body mass index ; ECOG , Eastern Cooperative Oncology Group ; HR , hazard ratio .