functional gastrointestinal disorders(fgids) in children ... · functional gastrointestinal...
TRANSCRIPT
Functional Gastrointestinal Disorders(FGIDs) in Children:
A Developing Country
Insight.
Eyad Altamimi, MD
Pediatric Gastroenterologist
Associate Professor of Pediatrics
Mu’tah University

Functional Gastrointestinal Disorders (FGIDs)
include a variable combination of age-
dependent, chronic or recurrent
gastrointestinal symptoms not otherwise
explained by structural or biochemical
abnormalities
Gastroenterology,2006

The term functional emphasizes that many
of the symptoms may accompany normal
development (eg, infant regurgitation) or
may be a response to otherwise normal
internal or external cues (eg, constipation
following painful stooling)
Gastroenterology,2006

Etiology & Pathophysiology
Despite the availability of isolated findings
and hypothesis the etiology of most of
FGIDs still need to be determined
J Pediatr Gastroenterol Nutr,2013
J Pediatr, 2015

The pathophysiology
of FGID is thought to
involve
abnormalities in the
relationship
between the enteric
and central nervous
systems
In Adult Gut:
- 100 million neurons located along the gut
which produce various neurotransmitters,
regulating mood and satiety N Engl J Med,1996
- 95% of the body`s total serotonin is
located in the gut ACS Chem Neurosci,2013

There is a high prevalence of psychiatric
disorders in FGID patients(anxiety and
depression)
Patients with internalizing psychiatric
disorders are found to have a higher
prevalence of pain predominant FGID

Diagnosis:

Physician’s lack of understanding
or appreciation of the illness
Absence of reliable biologic
markers and specific diagnostic
tests
Curr Pediatr Rep ,2013

Approach of FGID symptoms

Historical Background:
Apley`s Define RAP
Pediatric Working
Team met in Rome
ROME II Criteria
published
ROME III Criteria
published
ROME IV Criteria
published
1958
1997
1999
2006
2016

Rome criteria
The process involved group consensus
using:
- clinical experience
- extensive review of the literature
Goals:
- Diagnostic tool (accurate and definitive)
- Research tool ( facilitate and
advancement)

Rome criteria Symptom-based ( not organ related)
Symptom characteristics
Presence of associated symptoms
Impairment of daily activities
Age-specification:
- Patient– reporting
- Parents – reporting
Presence of alarming symptoms/signs



Cyclic Vomiting
Must include all of the following:
1. Two or more periods of intense
nausea and unremitting
vomiting or retching lasting hours
to days
2. Return to usual state of health
lasting weeks to months
Intense
Normal in between

Functional Constipation
Must include 2 or more of the following in a
child with a developmental age of at least 4
years with insufficient criteria for diagnosis of
IBS:
1. Two or fewer defecations in the toilet per
week
2. At least 1 episode of fecal incontinence per
week
3. History of retentive posturing or excessive
volitional stool retention
4. History of painful or hard bowel movements
5. Presence of a large fecal mass in the rectum
6. History of large diameter stools that may
obstruct the toilet
*Criteria fulfilled at least once per week for at
least 2 months before diagnosis
Infrequent, painful, large-
diameter with retentive
posturing

Treatment:

BIOPSYCHOSOCIAL MODEL
Takes into account the physical and psychosocial
components of the illness

The main goal
of the therapy
for children
with a FGID is to
re-establish a
normal daily
life for both the
patient and the
family

Most Important Part
Establishing connection with the patient
and family
Addressing the concerns
Tailor the work-up according to patient
condition
Explanation and reassurance
Medications to restore age appropriate
activities

Therapeutic Interventions:
Psychological and
cognitive behavioral
therapy
Diet manipulation
Hypnotherapy
Acupuncture
Bulking agents
Pro- and prebiotics,
Pharmacotherapy:
- Antispasmodics
- Tricyclic antidepressants
- Anti- diarrheals
- Stool softeners
- Antibiotics
- Melatonin
- Chloride channel
agonists

Reassurance and Placebo
Explaining the benign nature of the pain
Use familiar terms (e.g. IBS)
Compare to familiar symptom(e.g.
Headache)
Address any catastrophic thinking(patient
& family)
Discourage symptom re- enforcement
(missing school)
Explain the role of emotion
60% of patients improve with placebo
Curr Pediatr Rep , 2013

Addressing Mental Health Disorders
one-third of children presenting to general
practice for evaluation of abdominal pain,
anxiety and depressive problems persisted
during 1 year of follow-up Scand J Prim Health Care,2012
It may be reasonable to involve psychiatrist
early on

It was concluded that there was no evidence that
fiber supplements or lactose-free diets were effective
in the management of children with intermittent or
chronic abdominal pain

In childhood IBS, a
low FODMAP diet
decreases
abdominal pain
frequency.
Gut microbiome
biomarkers may be
associated with low
FODMAP diet
efficacy.
Aliment Pharmacol Ther ,2015

Tricyclic Antidepressants Used effectively in chronic pains
Analgesic effect is separate from the anti-
depressant effect
Used in small doses
Need weeks to feel the effect
Side effects with therapeutic implications:
- Increased sleepiness
- Delayed intestinal motility
ECG monitoring is recommended

Probiotics
The use of Lactobacillus rhamnosus GG
moderately increases treatment success in
children with pain-predominant FGID,
particularly among children with IBS
Aliment Pharmacol Ther, 2011

Probiotics
Despite evidence that changes in enteric
flora may play a role in childhood IBS there
is currently little agreement on when, for
how long, and which probiotic to use in
children with FGID

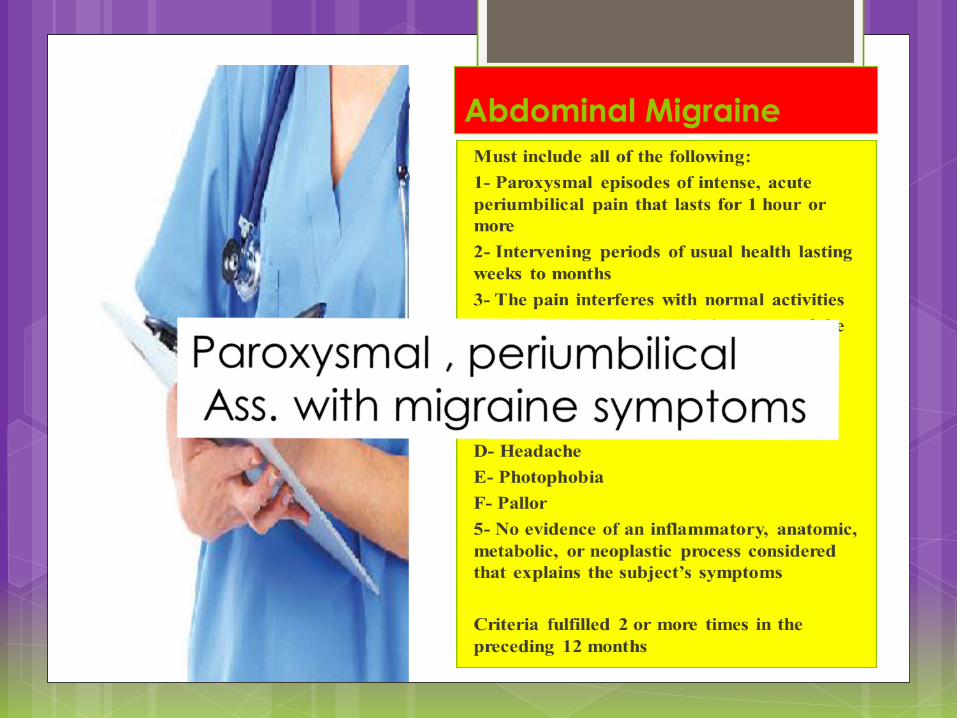
Cyproheptadine
Widely used in children with
dyspeptic symptoms, poor
appetite and as prophylaxis
of cyclic vomiting and
abdominal migraine
episodes
86% response rate in children
with Functional Abdominal
Pain
Minerva Pediatr, 2008

Montelukast
Used based on the
finding of duodenal
eosinophilia in children
with FD
Two studies showed a
significant clinical
benefit in children
receiving montelukast

Burden of FGIDs:
Recent Metanalysis:
A Worldwide pooled
prevalence for functional
abdominal pain disorders
13.5%(95% CI 11.8-15.3)
South America (16.8%)
Asia (16.5%)
Europe (10.5%)

Burden of Constipation:
The worldwide prevalence
varies between 0.7% and
29.6%
Pediatrician visit: 3% to 5%
Ped.GI consults: 25%
What about Jordan?

I will present briefly two studies :
- one clinic based (childhood
constipation)
- Community- based (FGIDs
prevalence)

At our clinic, 25.9% of clinic consults are due to chronic constipation
Males comprise 54.8% Most common age group were the Pre-schoolers 43.7%
Fecal incontinence affected 28.6 %

ARABIC TRANSLATION OF THE ROME III CRITERIA IS NOW AVAILABLE
Eyad M. Altamimi,MD & Mohammad Al Safadi,MD
Pediatric Department, Mu'tah University, Alkarak, Jordan
Introduction
Functional gastrointestinal disorders affect children of
all ethnic groups. Rome criteria are symptom-based
criteria allow a positive diagnosis of functional
gastrointestinal disorders (FGIDS).
The symptom based questionnaires are dependent
on the understanding of the questions and
expressions, which mandate these questionnaires
being addressed in the patient`s mother language.
As for Arabic speaking children there was no Arabic
version of these questionnaires. This was depriving
those children and their treating physicians from this
very important diagnostic tool. So, we decided to
translate the ROME III questionnaires into Arabic.
Methods
The Rome Foundation was contacted. Our interest in
translating the criteria was expressed. The foundation
permission was obtained. The process was
performed according to the translation guidelines
prepared by the foundation. The final validated Arabic
version get the foundation recognition and approval
on 12th of June,2012.
Conclusion We are so happy to denote that Arabic
translation of ROME III criteria is now
available for usage, through the Rome
Foundation website at:
http://www.romecriteria.org/translations/.
We believe this validated translation will
be of tremendous value in diagnosis of
(FGIDS) in Arabic speaking children.
Discussion
The major issues during the translation
process were the cultural sensitivity of
the topic and the availability of
simple terms describing the symptoms.
These problems were solved by using the
predetermined standardized
method of translation, the enthusiasm of
the working team and the help of the
foundation translation supervisor.
References
Appendix E: Rome III Diagnostic Questionnaire for
the Pediatric Functional GI Disorders
(http://www.romecriteria.org/questionnaires/)
Rome criteria translation Guidelines
(http://www.romecriteria.org/translations/guidelines.
cfm)

Prevalence Of Functional
Gastrointestinal Disorders In
Jordanian Children
The project is supported by a network grant from the European
Society for Pediatric Gastroenterology, Hepatology and Nutrition
(ESPGHAN), to study Prevalence Of Functional Gastrointestinal
Disorders In The European- Mediterranean Area

Methods: The prevalence of FGIDs has been
assessed using the Arabic version of the
questionnaires on pediatric GI symptoms
based on Rome III Criteria (QPGS-RIII)
The parent-report form has been used for
subjects aged between 4-10 years (Group
A), while the self-report form has been
used for subjects aged between 11-18
years (Group B)
Children and adolescents have been
enrolled in schools distributed throughout
the national territory

Results: A total of 815 children recruited. Males
comprise 46 % male. Median age was
14.9 years (range 10-18 years). A total of
322 subjects (39.5%) met criteria for a
FGID. Abdominal pain predominant FGIDs
were the most common affecting 18% of
the children followed by defecation
disorders. Functional constipation was
diagnosed in 15.3%.

Results:
A total of 773 subjects (49 % male, median
age 7.9 years, range 4-10 years)
completed our study
A total of 192 subjects (24.8%) met criteria
for a FGID. Defecation disorders were the
most common group of FGIDs
Functional constipation was diagnosed in
12.2 %. Abdominal pain predominant
FGIDs were seen in 7%. Abdominal
migraine and Irritable bowel syndrome
were the most common 3.6 and 3.2
respectively.

Table 1: Prevalence of FGIDs in Jordanian
children 4-10 yrs. of age
Disorder Prevalence Estimate [95%
C.I.) (x100)
Functional Dyspepsia 0.131 [0.003 to 0.728]
Irritable Bowel Syndrome 3.19 [2.033 to 4.748]
Abdominal Migraine 3.607 [2.274 to 5.41]
Cyclic Vomiting Syndrome 1.374 [0.63 to 2.592]
Functional Abdominal Pain Syndrome- Lower 0.135 [0.003 to 0.751]
Functional Abdominal Pain Syndrom Upper 0 [0 to 0.482]
Functional Abdominal Pain Lower 0.41 [0.085 to 1.195]
Functional Abdominal Pain Upper 0.531 [0.145 to 1.353]
Functional Constipation 12.242 [9.948 to 14.848]
Non retentive fecal incontinence 0.707 [0.23 to 1.643]
Rumination Syndrome 0.149 [0.004 to 0.828]
Aerophagia 5.037 [3.513 to 6.968]
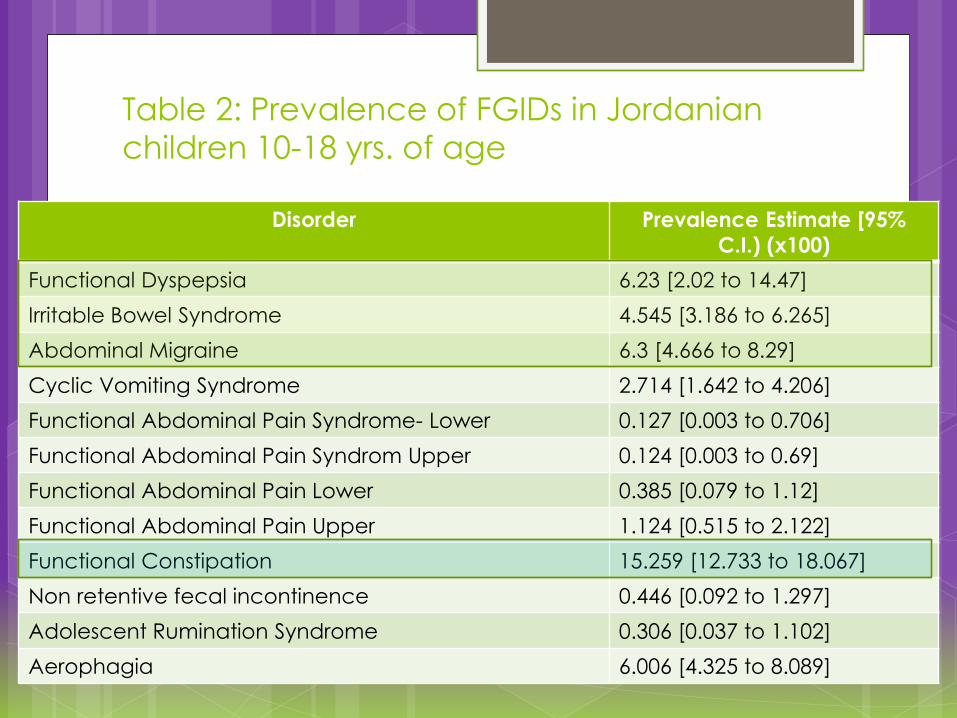
Table 2: Prevalence of FGIDs in Jordanian
children 10-18 yrs. of age
Disorder Prevalence Estimate [95%
C.I.) (x100)
Functional Dyspepsia 6.23 [2.02 to 14.47]
Irritable Bowel Syndrome 4.545 [3.186 to 6.265]
Abdominal Migraine 6.3 [4.666 to 8.29]
Cyclic Vomiting Syndrome 2.714 [1.642 to 4.206]
Functional Abdominal Pain Syndrome- Lower 0.127 [0.003 to 0.706]
Functional Abdominal Pain Syndrom Upper 0.124 [0.003 to 0.69]
Functional Abdominal Pain Lower 0.385 [0.079 to 1.12]
Functional Abdominal Pain Upper 1.124 [0.515 to 2.122]
Functional Constipation 15.259 [12.733 to 18.067]
Non retentive fecal incontinence 0.446 [0.092 to 1.297]
Adolescent Rumination Syndrome 0.306 [0.037 to 1.102]
Aerophagia 6.006 [4.325 to 8.089]

Conclusion:
Functional constipation is the most common
disorder in Jordanian children 4-10 yrs.
Abdominal pain-predominant Functional
gastrointestinal disorders are the most
common followed by functional
constipation in Jordanian children 10-18yrs.
