fulwood hall hospital newapproachcomprehensive … · ourjudgementsabouteachofthemainservices...
TRANSCRIPT

This report describes our judgement of the quality of care at this location. It is based on a combination of what wefound when we inspected and a review of all information available to CQC including information given to us frompatients, the public and other organisations
Ratings
Overall rating for this location Good –––
Are services safe? Good –––
Are services effective? Good –––
Are services caring? Good –––
Are services responsive? Good –––
Are services well-led? Good –––
FFulwoodulwood HallHall HospitHospitalalQuality Report
Midgery LaneFulwoodPreston, PR2 9SZTel: 01772 704111Website: http://www.fulwoodhallhospital.co.uk
Date of inspection visit: 1 to 2 November 2016Date of publication: 01/06/2017
1 Fulwood Hall Hospital Quality Report 01/06/2017
Letter from the Chief Inspector of Hospitals
Fulwood Hall Hospital is operated by Ramsay Health Care UK Operations Ltd. The hospital has 29 beds, four of which aredouble rooms; the others are single en-suite. Facilities include three main operating theatres with laminar flow, anendoscopy/ minor operations unit and outpatient and diagnostic facilities.
The hospital provides surgery, medical care, services for children and young people age 16 and over, and outpatientsand diagnostic imaging. We inspected surgery and outpatient and diagnostic imaging.
We inspected this service using our comprehensive inspection methodology. We carried out the announced part of theinspection on 1 to 2 November 2016, along with an unannounced visit to the hospital on 14 November 2016.
To get to the heart of patients’ experiences of care and treatment, we ask the same five questions of all services: are theysafe, effective, caring, responsive to people's needs, and well-led? Where we have a legal duty to do so we rate services’performance against each key question as outstanding, good, requires improvement or inadequate.
Throughout the inspection, we took account of what people told us and how the provider understood and compliedwith the Mental Capacity Act (2005).
The main service provided by this hospital was surgery. Where our findings on staffing, for example, managementarrangements, also apply to other services, we do not repeat the information but cross-refer to the surgical core service.
The hospital provided care for medical conditions, children aged 16 and over and care for patients at the end of theirlife. The numbers of patients treated in the last 12 months was considered insufficient to provide separate core servicereports. Where information applied to these patients it was incorporated into either the surgery or outpatients report asappropriate.
Services we rate
We rated this hospital as good in safe, effective, caring, responsive and in the well-led domain.
• There was a good incident reporting culture, staff were aware of how to report incidents and were proactive withactions following an incident. Causes were investigated and changes implemented, where appropriate.
• All departments in the hospital were visibly clean and tidy with hand sanitisers at the entrance to each area. Therewere infection prevention policies in place that were followed and all staff adhered to the ‘arms bare below theelbow’ policy during the inspection.
• Staffing levels were planned and reviewed using Ramsay Health Care UK’s national electronic rostering managementsystem. The inpatient ward and theatres were fully staffed using Ramsay employees, either substantive or bank.
• The hospital had a comprehensive training package in place for all Fulwood Hall hospital staff. New employeesundertook a hospital induction package and mandatory training had high levels of attendance. Staff told us theywere well supported to continue their education with a scholarship fund.
• The staff we spoke to during the inspection were passionate about their job and caring. Staff worked especially hardto make the patient experience as pleasant as possible. Staff recognised and responded to the holistic needs of theirpatients from the first referral before admission to checks on their wellbeing after they were discharged from thehospital
• The hospital had a robust system for awareness, training and monitoring safeguarding adults at risk of abuse orneglect, and safeguarding children and young persons. Policies were based on national guidelines, and covered acomprehensive range of issues.
• The hospital had four on-site safeguarding leads, including a registered children’s nurse (who was also the regionalsafeguarding lead). They delivered training to level three for adult and children’s safeguarding. In addition, monthlysafeguarding sessions were delivered with a variety of topics and reflective discussion of cases.
Summary of findings
2 Fulwood Hall Hospital Quality Report 01/06/2017

• A range of care pathways were in place, based on national guidance from the National Institute of Health and CareExcellence (NICE) and the Royal College of Surgeons (RCS). Local and national audits measured outcomes includingNational Joint Registry and performance related outcome measures (PROMs) for elective surgery.
• The hospital exceeded its indicators for consultant led referral to treatment waiting times for NHS patients. Thereferral to treatment and the admitted for treatment waiting times were consistently above the standard.
• The staff responded to a patients individual needs using a communications slip included in healthcare records priorto admission. Requirements such as air mattresses, moving and handling equipment or diabetic menu required, perprepared in advance.
• Patient feedback was received from a variety of sources and was positive about the care and treatment received. Wereceived a large number of feedback cards and comments included “Fulwood Hall is amazing, all staff andconsultants take time to listen and your care and treatment is to the highest of standards. The hospital is clean andhygienic at all times.” One patient told us they were prepared to travel 100 miles to be treated at Fulwood Hallhospital.
• All areas were visibly clean and tidy. Sanitisers and hand washing facilities were available in all consultation rooms.The radiology department had cleaning schedules, which included cleaning equipment after each patient. Infectioncontrol audits demonstrated excellent compliance.
• Equipment in the diagnostic imaging department was safe and appropriate for use following Ionising RadiationMedical Exposure Regulations 2000 [IR(ME)R] and IRR99 regulations. Personal protective equipment was regularlychecked and safe. All equipment was maintained and regular audits were performed to ensure patient and staffsafety.
• Mandatory training rates for permanent staff within the departments were on target for full completion with datesscheduled for staff to complete outstanding training within the rolling twelve month period
• Care and treatment was provided to patients who used the outpatient, physiotherapy and diagnostic imagingdepartments in a kind and compassionate way. This was reflected in the patient satisfaction survey. One nursing staffmember told us they started work early to be able to accommodate the needs of one patient who required an earlierappointment slot due to the needs of the patient’s business.
• Patient clinical pathways were standardised. Pathway documents were used for each procedure, which included aspecific outpatient procedure care pathway. These took into account guidance and established practice, andincluded appropriate pre and post procedure checks and follow-up information.
• The hospital was proactive in developing practice and improving patient experience, with a number of initiatives inplace. During 2016, the hospital had engaged with external participants and the National Institute for Health and CareExcellence (NICE) in reviewing the quality standards for falls and the clinical guidance on urinary incontinence inwomen.
• The hospital carried out a quarterly consent audit. Although there were recurring deficiencies identified, such as alack of clear recording of the patient’s and clinician’s details, the results between July 2015 and June 2016 showedintermittent improvements in compliance with the policy. However, following concerted efforts by staff the audit inSeptember 2016 demonstrated a significant improvement at 97% compliance with the policy.
However:
• There were no new risks entered on the register since October 2015. Although there was evidence that themanagement team were aware of their risks and had robust arrangements in place to manage and reduce the risks,these risks were not recorded on any risk register. A number of risks including dementia awareness, falls, andoutpatient capacity should have been included. Risk assessments for basic health and safety requirements were inplace in all areas but managers had a lack of understanding how to rate a risk appropriately using the likelihood andseverity.
• There was a reliance on bank staff to fill unmet need for shifts.
Summary of findings
3 Fulwood Hall Hospital Quality Report 01/06/2017

• We observed incomplete records of weekly water outlet flushing checks, to reduce risk from legionella bacteria, somemonths’ records were missing from the file. Staff told us these checks had been done. Managers informed us thatpaper records for the missing months had been mislaid and that checks were now in place for the future. However,Legionella sampling had been carried out twice in March and October 2016. We viewed this documentation whichconfirmed there was no legionella present in the water system.
• At the time of the inspection, there was an approximate two-week wait for reporting of plain film X-rays in thediagnostic imaging department during to staffing issues.
• The hospital recognised that increasing demands for its services was not being matched by the physical capacity ofits facilities. There were issues with privacy and dignity in the diagnostic imaging waiting area, physiotherapy andpre-operative assessment clinic rooms. Staff had made efforts to adapt the area and their process to provide privacyand confidentiality. Managers had developed business plans to increase the size of the hospital which were to bereviewed by the board imminently.
Ellen Armistead
Deputy Chief Inspector of Hospitals (North)
Summary of findings
4 Fulwood Hall Hospital Quality Report 01/06/2017

Our judgements about each of the main services
Service Rating Summary of each main service
Surgery
Good –––
Staff were trained in the safeguarding of vulnerableadults and children. A safeguarding culture wasengrained in the departments and staff weresupported to identify and report safeguardingconcerns. Patient records were held securely.There was a higher than average use of bank staff tocover gaps in shifts for nursing and healthcareassistants.A range of care pathways, policies and procedureswere in place, based on guidance from the NationalInstitute of Health and Care Excellence (NICE) and theRoyal College of Surgeons (RCS).The hospital accommodated pre-admission visits forpatients living with a learning disability. This visitaimed to reduce patient anxiety, introducing thenursing team and identifying any specific individualrequirements, such as equipment or dietary needs.The hospital engaged with the local community tosupport service improvement. Groups such as theAlzheimers society, Galloways Society for the Blind andthe Preston Muslim society all assisted development ofthe service.
Outpatientsanddiagnosticimaging
Good –––
Mandatory training rates for permanent staff withinthe departments were on target for full completionwithin the rolling twelve-month period.The diagnostic imaging department was involved inmultidisciplinary meetings with outpatientconsultants to review imaging and reports.Care and treatment was provided to patients whoused the outpatient, physiotherapy and diagnosticimaging departments in a kind and compassionateway. This was reflected in the patient satisfactionsurvey.As a response to a number of complaints in thediagnostic imaging department in 2015, the hospitalhad implemented an improvement plan. This includedrecruitment of a new departmental manager. Therewas a clear improvement in the feedback thedepartment had recently received.The hospital took part in the Ramsay Health Care UKcustomer service excellence awards scheme. Two staff
Summary of findings
5 Fulwood Hall Hospital Quality Report 01/06/2017

in the physiotherapy department had received awardsand a staff member in the outpatient department hadtwo nominations. One staff member told us the awardscheme meant that staff ‘feel appreciated’.
Summary of findings
6 Fulwood Hall Hospital Quality Report 01/06/2017
Contents
PageSummary of this inspectionBackground to Fulwood Hall Hospital 9
Our inspection team 9
Why we carried out this inspection 9
How we carried out this inspection 9
Information about Fulwood Hall Hospital 10
The five questions we ask about services and what we found 12
Detailed findings from this inspectionOverview of ratings 18
Outstanding practice 55
Areas for improvement 55
Summary of findings
7 Fulwood Hall Hospital Quality Report 01/06/2017
Fulwood Hall Hospital
Services we looked atSurgery; Outpatients and diagnostic imaging.
FulwoodHallHospital
Good –––
8 Fulwood Hall Hospital Quality Report 01/06/2017

Background to Fulwood Hall Hospital
Fulwood Hall Hospital is operated by Ramsay Health CareUK Operations Ltd. The hospital opened as a purposebuilt facility in 1986. It is a private hospital in Preston,Lancashire. The hospital primarily serves thecommunities of the Preston area. It also accepts patientreferrals from outside this area. Fulwood Hall Hospital isone of three Ramsay Health Care UK Operations Ltdhospitals in the Lancashire County.
The hospital’s Registered Manager had been in post forfive months at the time of inspection, having transferredfrom a neighbouring Ramsey Healthcare hospital. Themanager was registered with the CQC in 29 June 2016.The hospital had a Controlled Drugs Accountable Officerwho had been registered for one year.
The hospital had one inpatient ward and was registeredto provide the following regulated activities: Treatment ofdisease, disorder or injury, surgical procedures,diagnostic and screening procedures and familyplanning.
There were no special reviews or investigations of thehospital ongoing by the CQC at any time during the 12months before this inspection. The hospital hadpreviously been inspected in September 2013, whichfound that the hospital was meeting all standards ofquality and safety it was inspected against.
Our inspection team
The team that inspected the service comprised a CQClead inspector, three further CQC inspectors, andspecialist advisors with expertise in governance, surgeryand diagnostic imaging. The inspection team wasoverseen by Nicola Kemp, Inspection Manager.
Why we carried out this inspection
We inspected this service as part of our nationalprogramme of inspections of independent healthcareusing our comprehensive inspection methodology.
How we carried out this inspection
This report describes our judgement of the quality of careat this location. We based it on a combination of what wefound when we inspected and from all informationavailable to us, including information given to us frompeople who use the service, the public and otherorganisations.
To get to the heart of patients’ experiences of care andtreatment, we ask the same five questions of all
services:are they safe, effective, caring, responsive topeople's needs and well-led? Where we have a legal dutyto do so we rate services’ performance against each keyquestion as outstanding, good, requires improvement orinadequate. Throughout the inspection, we took accountof what people told us and how the provider understoodand complied with the Mental Capacity Act 2005.
Summaryofthisinspection
Summary of this inspection
9 Fulwood Hall Hospital Quality Report 01/06/2017

Information about Fulwood Hall Hospital
Fulwood Hall Hospital provided a range of surgicalprocedures and outpatient services for patients aged 16and over including orthopaedic surgery, neurosurgery,general surgery, ear, nose and throat (ENT),gastroenterology, gynaecology, neurology,ophthalmology, vascular surgery, colorectal surgery,urology, physiotherapy and pain management.
In support, the hospital offers a range of diagnosticimaging including plain X-rays, dental X-rays, fluoroscopy(a technique that uses X-rays to obtain real-time movingimages) and arthrograms (imaging of a joint), generalultrasound scanning and ultrasound guided injections,urodynamic testing (assessing function of the bladderand urethra), and barium swallow investigations.
The diagnostic imaging department consisted of an X-rayroom and an ultrasound room. A mobile X-ray machinewas available for obtaining images of patients on theward in emergencies and an X-ray image intensifier wasavailable in theatre.
Although the hospital offers computerised tomography(CT) scanning and magnetic resonance imaging (MRI)scanning, these were carried out using a mobile scanningfacility operated by another provider within RamsayHealth Care UK, which was not part of this inspection.
The outpatient, diagnostic imaging and physiotherapydepartments are located next to each other. There areseven outpatient consultation and treatment rooms usedby the department, with a further two consultant andtreatment rooms contracted for use by anotherhealthcare provider.
The physiotherapy department offers a range of therapiesincluding musculoskeletal and lower back pain therapies,pulmonary rehabilitation, extracorporeal lithotripsy fortendons and heel pain, acupuncture, gynaecologicaltherapy, pelvic floor and urinary therapy, and handtherapy.
There were eight private consulting rooms supported byan outpatient treatment room, a pre-operativeassessment unit, as well as imaging facilities and a physioand sports therapy department.
Four theatre suites provided a variety of surgicalprocedures, including orthopaedic, gynaecological,general surgical, colorectal and varicose vein surgery. Oneof the theatres was Joint Advisory Group onGastrointestinal Endoscopy (JAG) accredited forendoscopy and other procedures, including gastroscopy,colonoscopy and sigmoidoscopy. Spinal injections arealso administered in this theatre.
A resident doctor was available on site 24 hours a day,seven days a week
Patient accommodation consisted of a day care facilityproviding 12 day case pods and, for inpatients, there were29 private or double, en-suite bedrooms.
Free car parking and disabled access was also available.Visitor’s hours were between the hours of 2pm and 4pmand from 6pm until 8pm with extended visiting hours forprivate patients.
During the inspection, we visited the ward area, surgicalday case and operating theatres, outpatients,physiotherapy and radiology. We spoke with 51 staffincluding; registered nurses, health care assistants,reception staff, medical staff, operating departmentpractitioners and senior managers. We spoke with sixpatients and one relative. We also received 45 ‘tell usabout your care’ comment cards which patients hadcompleted during and after our inspection. During ourinspection, we reviewed 38 sets of patient records.
Activity (July 2015 to June 2016)
• In the reporting period July 2015 to June 2016, therewere 8,540 inpatient and day case episodes of carerecorded at the hospital; of these 87% wereNHS-funded and 13% funded by other means.
• During the same reporting period, 77% of allNHS-funded patients and 71% of all other fundedpatients stayed overnight at the hospital.
• There were 30,927 outpatient total attendances in thereporting period; of these 80% were NHS-funded and20% were funded by other means.
Ninety-four doctors worked at the hospital underpractising privileges and there was one resident MedicalOfficer (RMO) on site at all times. Fulwood Hall Hospitalemployed 45.2 registered nurses, 18.6 operating theatre
Summaryofthisinspection
Summary of this inspection
10 Fulwood Hall Hospital Quality Report 01/06/2017

and care assistants and a further 61.8 staff, as well ashaving its own bank staff. The accountable officer forcontrolled drugs (CDs) was employed in addition to theRegistered Manager.
Track record on safety for the period July 2015 toJune 2016:
• No Never Events had been reported by the hospitalover the twelve months prior to our inspection.However, there were two incidents that involved theimplantation of the wrong intraocular lens andclassified as severe harm.
• There were a total of 89 clinical incidents: 80 no harm,four low harm, two moderate harm, two severe harmand one death
• There were three serious injuries• No incidences of hospital acquired Methicillin-resistant
Staphylococcus aureus (MRSA), Methicillin-sensitivestaphylococcus aureus (MSSA), Clostridium difficile(c.diff) or E-Coli.
• There was one incident of hospital acquired VenousThromboembolism (VTE) in the reporting period.
• The hospital reported 44 complaints against theservice, none of which were escalated to theParliamentary and Health Service Ombudsman.
Services accredited by a national body:
• Joint Advisory Group on GI endoscopy (JAG)accreditation
Services provided at the hospital under service levelagreement include:
• CT scanning (for under 18 year olds and wide bore forpatients who have claustrophobia)
• Microbiology• Nerve conduction studies• Pathology and histopathology• Pharmacy services• Registered Medical Officer
Summaryofthisinspection
Summary of this inspection
11 Fulwood Hall Hospital Quality Report 01/06/2017
The five questions we ask about services and what we found
We always ask the following five questions of services.
Are services safe?We rated safe as good because:
• There were low numbers of clinical and non-clinical incidentsthroughout the hospital and no never events. Staff understoodtheir duty to report incidents. Incidents were well investigated;the duty of candour was implemented, where necessary andlearning was shared. Staff had access to the electronic systemto record incidents and could give us examples of what wouldbe reported.
• The departments were clean, suitable for the services providedand equipment was regularly maintained and in date.Medicines were managed and stored safely, hygiene auditswere completed and the diagnostic imaging department hadimplemented policies and procedures to meet radiationexposure and protection regulations.
• Staff were trained in the safeguarding of vulnerable adults andchildren. A safeguarding culture was engrained in thedepartments and staff were supported to identify and reportsafeguarding concerns. Patient records were held securely.
• Mandatory training rates for permanent staff within thedepartments were on target for full completion with datesscheduled for staff to complete outstanding training within therolling twelve month period.
• Sufficient nursing, healthcare assistant and allied healthcareprofessional staff were rostered for the services provided in thedepartments.
• Staff had relevant skills to respond to patients who becameunwell within the departments and knew how to getemergency assistance.
However,
• The hospital reported high use of bank staff in the outpatientdepartment.
• Figures showed that mandatory training levels for bank staff inthe theatre and ward were low.
• The records of water flushing checks for the surgical unit wereincomplete.
Good –––
Are services effective?We rated effective as good because:
Good –––
Summaryofthisinspection
Summary of this inspection
12 Fulwood Hall Hospital Quality Report 01/06/2017

• A range of care pathways were in place, based on nationalguidance from the National Institute of Health and CareExcellence (NICE) and the Royal College of Surgeons (RCS). Stafffollowed policies and procedures, which were based on thisnational guidance.
• Hospital policies followed in the outpatient, physiotherapy anddiagnostic imaging departments was evidence-based and inline with relevant national and professional guidance.
• The hospital had a well embedded audit programme. This waspredominantly routine practice checklists such as recordkeeping, medicines management and infection, prevention andcontrol. . The audit results were consistently positive. On theoccasions where audit results dropped slightly, improvementswere made the following month. We were told there was nomedical involvement in clinical audits.
• Patients were assessed prior to admission for their preferredapproach for pain relief. Patients reported that their pain waswell managed during their course of treatment.
• A nutrition and hydration week was held at the hospital inMarch 2016 and a nutrition and hydration goals plan had beenimplemented, which was developed by Ramsay Health CareUK.
• Staff had the knowledge and skills to deliver care and treatmenteffectively and were supported by the managers in theircontinuing professional development. Students on the wardreported positive experiences of their placement, with goodsupport from supervising staff.
• There was a limited, but effective, multidisciplinary approachbetween the departments with a good working relationshipbetween the staff and consultants.
• The hospital had established thorough processes forappointing and supervising the Registered Medical Officer andfor approving consultants to carry out clinical practice atFulwood Hall Hospital.
• The hospital ensured continuous medical cover using theservices of a company that provided a Resident Medical Officer(RMO). Although the hospital did not offer a full seven-dayoutpatient service, the departments scheduled additionalclinics when needed to meet demand.
• Staff were aware of the processes in place for obtaininginformed consent, including the need to consider mentalcapacity assessment if necessary.
Summaryofthisinspection
Summary of this inspection
13 Fulwood Hall Hospital Quality Report 01/06/2017

• Despite reminders to staff, there were recurring deficienciesidentified by the consent audit. These included the clearrecording of the patient’s and the clinician’s details. However,the audit in September 2016 demonstrated a significantimprovement at 97% compliance with the policy.
However,
• The hospital did not routinely collect, or analyse, clinicalpatient outcome data specifically relating to outcomes foroutpatient care and treatments.
Are services caring?We rated caring as good, because:
• Staff spoke to patients and their carers with kindness, in waysthat respected their dignity. Nurses told us they felt they hadtime to be able to speak with patients and felt able to give100% of their time in caring for them.
• Care and treatment was provided to patients who used thehospital in a kind and compassionate way. This was reflected inthe patient satisfaction survey. Between January and June2016, the NHS Friends and Family test scores were an averageof 99%, which was positive.
• Staff supported patients living with dementia or learningdisabilities to visit the department prior to treatment to reduceanxiety. The hospital recognised the important role for carers ofpatients living with dementia or learning disabilities. Carerswere able to stay with their relatives and were given free mealsin the restaurant.
• Patients were involved in their care. There were given adequateinformation to understand the treatment being provided and tounderstand the role of the clinician looking after them.
• Staff provided emotional support to patients who received badnews. Appointments were scheduled for the end of the clinicday to enable the patient to take a longer appointment and inorder to ask questions and reflect.
Good –––
Are services responsive?We rated responsive as good, because:
• The hospital worked with local stakeholders, including theclinical commissioning groups and primary care providers tounderstand the needs of the local population and to plan itsservices accordingly.
• The hospital exceeded its targets for consultant led referral totreatment waiting times for NHS patients. Between July 2015
Good –––
Summaryofthisinspection
Summary of this inspection
14 Fulwood Hall Hospital Quality Report 01/06/2017
and June 2016, above 90% of patients were admitted fortreatment within 18 weeks of referral for treatment. No patientswaited longer than six weeks for a CT scan and only four waitedlonger than six weeks for an MRI scan.
• The hospital recognised that increasing demands for itsservices was not being matched by the physical capacity of itsfacilities. It had developed business plans to increase the size ofthe hospital which were to be reviewed by the boardimminently. In the interim, daily slot utilisation and weeklycapacity meetings were held.
• Staff met the individual needs of patients. Translation serviceswere available for people whose first language was not Englishand staff accommodated the needs of patients to pray or toattend appointments around their work commitments.
• The hospital developed an assistance dogs policy and workedwith the Alzheimer’s Society and Galloways Society for the Blindto ensure its services were accessible for patients living withdementia or with a disability.
• The number of patients who had their appointments cancelledbetween July 2015 and June 2016 was equivalent to 1% of thetotal number of patients seen. Of these, 98% received analternative appointment within 28 days.
• A communications slip was placed in patients’ notes prior toadmission that highlighted an individual’s additional needs.The ward diary noted requirements such as air mattresses,moving and handling equipment or diabetic menu required, asappropriate.
However,
• There was an approximate two week wait for reporting of plainfilm X-rays in the diagnostic imaging department at the time ofthe inspection due to staff holidays.
• There was a risk that patient privacy and dignity could becompromised in the diagnostic imaging waiting area and thatconfidential discussions with patients could be overheard inthe physiotherapy department.
• Increasing demand on the services provided, in conjunctionwith the physical capacity of the hospital, meant there was littleroom for appointments or clinics to overrun without affectingthe remaining slots.
• Limited information was collected, or available, relating to theclinics running late, cancellations or patients who did notattend appointments. This meant there was a risk that possibletrends, which may affect demand on the departments’ services,may not be identified.
Summaryofthisinspection
Summary of this inspection
15 Fulwood Hall Hospital Quality Report 01/06/2017
• The room available for pre-assessment appointments wassmall and was used by up to four members of staff as well astwo patients at a time. We felt that this facility did not offer thebest environment to protect patients’ dignity andconfidentiality.
Are services well-led?We rated well-led as good, because:
• There was a strong leadership team in place in the hospital.Senior leaders were visible and the majority of staff feltsupported by them, although staff were not as aware of thecorporate leaders.
• The Ramsay Health Care UK strategy was embedded in thehospital; staff were aware of the strategy and the values.
• There was a governance structure in place, which wassupported by appropriate policies and procedures. Acomprehensive audit programme was in place.
• The hospital had a clinical governance lead and regular clinicalgovernance meetings were held. The Medical AdvisoryCommittee met quarterly. This meeting included review ofincidents, governance reports and accreditation of medicalstaff.
• Staff consistently reported positive experiences of working inthe hospital. Staff said their leaders were visible, accessible andprovided them with support.
• Although the recent staff survey had highlighted some areasthat needed improvement, managers had created an actionplan and began work to improve staff engagement.
• NHS Friends and Family test scores were consistently very high,although the average response rates were low. However, thehospital’s patient satisfaction survey also indicated high levelsof satisfaction with the services offered.
• The hospital engaged with patients and various differentpatient groups in developing their services. This included theAlzheimer’s society, the Preston Muslim society and the localHealthwatch organisation.
• High numbers of staff worked to the best interests of patientsand colleagues and understood how their role contributed topatient care. Staff were supported to develop and could applyto the Ramsay Scholarship Fund to attend training courses.
However,
• The hospital level risk register did not appear to be a livedocument with no new risks added to the register since
Good –––
Summaryofthisinspection
Summary of this inspection
16 Fulwood Hall Hospital Quality Report 01/06/2017

October 2015. A number of risks that we would have expectedto see on the risk register over the last twelve months were noton the risk register, including dementia awareness, falls andhigh bank staffing levels in surgery.
• Although there was a strong emphasis on risk assessments ofequipment and procedures within the individual departments,there were no separate risk registers held in the specificdepartments that identified risks to the operation of theservices, control gaps or mitigation actions put in place for theindividual services. The hospital risk register did not includerisks related to the individual departments.
Summaryofthisinspection
Summary of this inspection
17 Fulwood Hall Hospital Quality Report 01/06/2017
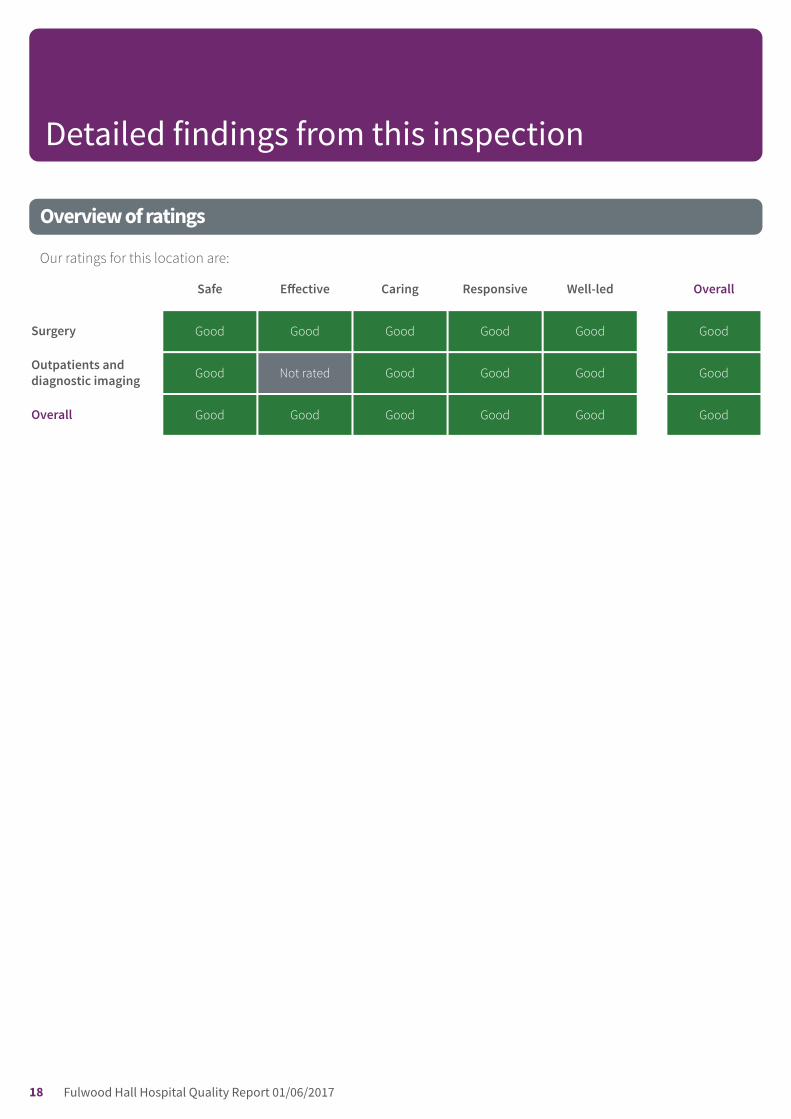
Overview of ratings
Our ratings for this location are:
Safe Effective Caring Responsive Well-led Overall
Surgery Good Good Good Good Good Good
Outpatients anddiagnostic imaging Good Not rated Good Good Good Good
Overall Good Good Good Good Good Good
Detailed findings from this inspection
18 Fulwood Hall Hospital Quality Report 01/06/2017

Safe Good –––
Effective Good –––
Caring Good –––
Responsive Good –––
Well-led Good –––
Are surgery services safe?
Good –––
The main service provided by this hospital was surgery.Where our findings on surgery – for example, managementarrangements – also apply to other services, we do notrepeat the information but cross-refer to the surgerysection.
We rated safe as good.
Incidents
• Incidents were reported by staff using an electronicreporting system. Staff we spoke with understood theirresponsibility to report incidents and could giveexamples of when they had done this. One example wasgiven regarding a patient whose level of care hadescalated and the nurse had needed to call for aparamedic ambulance for the patient’s transfer tohospital. This incident had also involved seniormanagement in the decision making and learning wasshared from this with staff on the ward.
• The hospital reported a total of 94 incidents from July2015 to June 2016. Of which 89 were clinical and fivenon-clinical incidents. Eighty four clinical incidents werereported as causing no or low harm. The theatre andinpatient areas had recorded 43 clinical incidents.Overall, the rate of clinical incidents was lower than therate for other independent acute hospitals.
• Departmental and senior managers reviewed andinvestigated incidents, put in place corrective actions, ifnecessary, and escalated any risks to the corporateteam. Root cause analyses were completed of anyserious incidents that occurred.
• Five root cause analysis reports were inspected and wefound investigation reports varied in quality. Whilst allinvestigations had clearly used root cause analysistechniques, the root cause itself was not identified. Forexample, a root cause was stated as ‘Failure to followprocedure’ without the question ‘why’ being repeatedlyasked until a root cause was identified. We discussedthis with the management team and quality lead whoagreed that further improvements could be made. Theteam had recently attended root cause analysis trainingand had found this really useful as a prompt to continueimproving the quality of the investigations.
• Evidence was seen of actions being taken in response tothemes in incidents. For example, a rise in the numberof patient falls incidents prompted a review by the‘Clinical Practice Review Group’. Staff were able to talkabout the actions currently being implemented toreduce patient falls. The clinical governance committeeminutes had many examples of actions taken in eachset reviewed.
• We saw there was a positive culture of learning fromincidents. An incident had occurred during 2015 where apatient with dementia had been missing from the wardfor a short period of time. This had resulted in a new‘Missing Patient Procedure’ and action plan beingidentified for the hospital, which was shared with otherRamsay sites. Other actions arising from this incidentincluded a review of security on ward exit doors, as wellas development of a dementia training package for staff.
• Lessons from incidents and complaints were shared in anumber of ways. Incidents were discussed in localmanagement and heads of department meetings andregionally in the northern matrons’ committeemeetings. Staff also had access to lessons learntbriefings from incidents and complaints.
Surgery
Surgery
Good –––
19 Fulwood Hall Hospital Quality Report 01/06/2017

• There were no reports of ‘never events’ from July 2015to June 2016. Never events are serious patient safetyincidents that should not happen if healthcare providersfollow national guidance on how to prevent them. Eachnever event type has the potential to cause seriouspatient harm or death but neither need have happenedfor an incident to be a never event.
• However, two incidents that involved the implantationof the wrong strength intraocular lens had occurred andhad been classified as severe harm. The hospitalmanagement team sought advice from the corporategovernance team and were advised not to report eitherof these incidents as Never Events. The patients in bothcases required further surgery to address these errors.Appropriate action had been taken by staff to reflectand learn following the errors.
• The duty of candour is a regulatory duty that relates toopenness and transparency and requires providers ofhealth and social care services to notify patients (orother relevant persons) of certain ‘notifiable safetyincidents’ and provide reasonable support to thatperson. We saw examples of duty of candour whichwere appropriate and timely.
• Senior staff were aware of the duty of candourrequirements. Operational staff were less aware of thelegislative requirements of the duty of candour;however, staff we spoke with were aware of theprinciples of the duty of being open and honest. TheWard Manager had delivered duty of candour grouptraining to all clinical staff.
• Mortality and morbidity were discussed in seniormanagement team meetings and medical advisorycommittee meetings. Minutes reviewed showed thisitem on the agenda. However, there had been no deathsreported under this provider’s care.
Clinical Quality Dashboard or equivalent
• The hospital submitted data to the NHS safetythermometer for NHS funded patients who had receivedcare and treatment. The NHS safety thermometer toolmeasures a snapshot of harms once a month, indicatingrisks such as the incidence of falls, pressure ulcers,blood clots, catheter and urinary infections.
• There was one case of hospital acquired VenousThromboembolism (VTE) or Pulmonary Embolism (PE)between July 2015 and June 2016. The hospitalcompleted patient screening for risk of venousthromboembolism and the percentage of patients
screened was above 95% for the reporting period (July2015 to June 2016). There were no falls with harm,pressure ulcers or catheter and urinary infectionsreported by the hospital in the same period.
• A safety thermometer was displayed in the theatre staffroom, which indicated a reduction in compliance furtherto incidences of surgical site infection. These findingshad been fully investigated through Root Cause Analysis(RCA), with no correlation between cases identified.Responsive measures had been implemented followingthis as a further precaution.
Cleanliness, infection control and hygiene
• Ward areas we inspected appeared to be visibly cleanand were in an orderly state, free from clutter.Housekeeping staff completed daily cleaning tasks andwe observed that checklists were completed, signedand up to date for these tasks. Staff told us they wouldclean pre-admission rooms and day case ‘pods’ readyfor the next day as a priority, covering the ward and inpatient area as ongoing and where required during theday
• The hospital had a standard infection controlprecautions policy in place, which covered areasincluding: hand hygiene; use of personal protectionequipment; safe use and disposal of sharps; andmaintaining a clean environment. The policy took intoaccount The Health and Social Care Act 2008: Code ofPractice for the Prevention and Control of Infections andRelated Guidance from the Department of Health, andNational Institute for Health and Care Excellence (NICE2012) guidance on Infection: Prevention and control ofhealthcare-associated infections in primary andcommunity care.
• An infection prevention and control environmental auditwas carried out each quarter. The results indicatedvaried compliance between August 2015 and May 2016(the lowest average compliance rate was 85% with thehighest compliance 98%). Where compliance was lower,action plans were put in place to address the issues. Theaction plans were reviewed at the next audit.
• Infection prevention and control in the hospital wassupported by the Ramsay Health Care UK northwesthospitals’ infection prevention and control plan.Infection prevention and control meetings were heldonce a quarter, which were supported by qualityregional meetings. The meetings included standingitems for review of infection incidents; the outcome of
Surgery
Surgery
Good –––
20 Fulwood Hall Hospital Quality Report 01/06/2017

any relevant audits that had been carried out; issuesarising from the environment; general buildings facilitiesinfection control issues; and, review of any relevantupdated guidelines and policies.
• There were no incidences of hospital acquiredMethicillin-resistant Staphylococcus aureus (MRSA),Methicillin-sensitive Staphylococcus aureus (MSSA),Clostridium difficile (C.diff) or Escherichia coli ( E. coli) atthe hospital for the reporting period (July 2015 to June2016). Patients were screened as part of theirpre-operative assessment.
• There had been fourteen surgical site infections (SSIs) intotal between April 2015 and March 2016 at the hospital.The rate of infections for primary hip arthroplasty,primary knee arthroplasty, upper gastro-intestinal andcolorectal, urological and vascular procedures wasabove the rate of other independent acute hospitals.The rate of infections during other orthopaedic andtrauma procedures was similar to the rate of otherindependent acute hospitals.
• We reviewed meeting minutes of the monthly clinicalgovernance committee and saw that incidence andmonitoring of surgical site infections was discussed andactions recorded. These included actions such asensuring that regular recording of patients’temperatures were documented during surgery. Wereviewed audit records which confirmed the identifiedactions had been implemented and progress reviewed.
• The hospital had a hand hygiene policy in place. Thepolicy was supported by a quarterly observational handhygiene audit. The policy took into account the HandDecontamination Guidelines from Infection ControlNurses Association and Clean Hands Saves Lives fromthe National Patient Safety Agency.
• Between 1 July 2015 and 30 June 2016 the averagehandwashing audit scores from July 2015 to June 2016were above 98%. The audit results indicated that thehospital complied with the National Institute for Healthand Care Excellence (NICE) Quality Standard 61.Although staff initials were used to identify those whocarried out the audit and those who were observed,there was no indication in the audit results of whichareas or departments the audits covered. This meantthere was a risk that poor trends in one particular areamay not be easily identified.
• We observed staff following the ‘arms bare below theelbow’ protocol and wearing personal protectiveequipment, such as gloves and aprons, when deliveringcare. Gowning procedures were followed in theatreareas.
• Pre-operative MRSA screening swabs were completedfor patients prior to their surgery.
• There were enough sinks and hand gels available forhandwashing. A hand hygiene policy and regularquarterly audits of handwashing practice on the wardwere in place. Aprons and gloves were availablethroughout the ward and day case area.
• We observed incomplete monthly records of weeklywater outlet flushing checks, which were only signed ashaving been checked in January 2016, February 2016and October 2016. Weekly flushing of water outlets isrecommended to reduce the risk of legionella bacteria.We noted that meeting minutes of the February 2016Clinical Governance committee had recommended tocarry out more frequent legionella monitoring checks.Staff told us that these checks had been done, oftenmore frequently than once a week, however thisrecording had been missed. Managers informed us thatpaper records for the missing months had been mislaidand that checks were now in place for the future.However, Legionella sampling had been carried outtwice in March and October 2016. We viewed thisdocumentation which confirmed there was nolegionella present in the water system.
• The hospital had a Service Level Agreement (SLA) withthe local NHS trust for decontamination of reusablemedical devices. This meant that the hospital hadsystems in place to meet nationally agreed standardsfor continuous improvement in the use anddecontamination of reusable medical devices. Reusablemedical devices include surgical instruments, such asforceps, as well as instruments for internalexaminations, such as endoscopes. Through this, thehospital demonstrated its approach to reducing risksfrom surgery and improving outcomes in patient safety,clinical effectiveness and patient experience.
• There were arrangements in place for the handling,storage and disposal of clinical waste including sharps.During our inspection, we saw that all sharps bins weresigned and dated, but these were not consistentlypartially closed when not in use.
Environment and equipment
Surgery
Surgery
Good –––
21 Fulwood Hall Hospital Quality Report 01/06/2017

• The operating theatre suite was clean, bright and in agood state of repair. Theatre equipment was checkedand in good working order. The anaesthetic machinewas checked daily and recorded in a log book, followinglocal policy and procedures. We observed complete andcurrent records were maintained for equipment checks.
• Theatre corridors were clean and free from congestionwith equipment, with large and well utilised storageareas available.
• In the operating theatre pack room, where surgical setswere stored, staff reported there were occasionalproblems with small holes or rips in external packaging.We did not see any evidence of this issue having beenreported as a risk. However, there was no evidence ofany theatre cases having been cancelled as a result ofdesterilised packs.
• A fridge was available in theatres for storing anemergency standby supply of blood for transfusion. Twounits of blood group O was available at all times,meeting statutory guidance.
• Some equipment checked in theatres did not displayservice stickers. The theatre manager advised thatservicing for some theatre equipment was provided byexternal contract arrangements. The theatre managerprovided evidence of all service details from anequipment inventory, which confirmed that allequipment servicing records were complete.
• Security tagged emergency resuscitation trolleys werechecked in theatres. These were complete with allrequired equipment and drugs for resuscitation,including a set of equipment for difficult intubationprocedures. All records of daily checks for these wereobserved as complete and in date.
• A security tagged resuscitation trolley was available onthe ward and equipment was checked daily, as well aswith a whole trolley check weekly. We saw that out oftwo months record checks for this, there were only twodays not signed as checked.
• A log book of all equipment, such as drug fridges andsyringe drivers, was kept on the ward. The log bookprovided maintenance and servicing records and wesaw all these records were checked and up to date.
• A hoist was available for patient use on the ward andthis was labelled, with up to date service history details.Staff completed manual handling training as part oftheir mandatory training, including training forappropriate use of hoists.
• The hospital did not perform bariatric surgery but hadequipment suitable to treat overweight patients such asload bearing trolleys and wheelchairs.
• Pressure redistribution mattresses could be ordered forpatients at risk of developing pressure damage. Staff wespoke with knew how to access these.
• Patients were seen for pre-operative assessmentappointments in a separate clinic. This room had twopatient bays, divided by a curtain. The treatment roomwas small, used by up to four members of staff and upto two patients at a time, and was a challenging workingenvironment. There were wall cupboards, a sink withhandwashing gel, personal protective equipment,oxygen cylinder, a nurse’s desk and a small foldawaytable. We observed patients attending theirappointments during our inspection and wereconcerned that this facility did not provide patients withthe best environment to protect their confidentiality anddignity. This had been noted and reflected in businesscase for the hospitals proposed development.
• The health and safety audit in late 2015 indicated overallcompliance of 95%. There was full (100%) complianceon workplace administration safety, plant andequipment, medical equipment, control of substanceshazardous to health (COSHH), electrical safety, officeareas, manual handling, and first aid, fire safety andevacuation, waste disposal, ventilation,decontamination, mechanical, building fabric andsystems, and the management of contractors. Actionswere identified to address areas that had not achievedfull compliance: occupational health (83%), generalworkplace safety (97%), medical gases (85%), and waterservices (92%).
• Patient led assessments of the care environment(PLACE) audits were completed between February andJune 2016 and scored similar to or better than theEngland average, including cleanliness, which scored100%.
Medicines
• The hospital had a medicines management policy,which provided guidance for prescribing andadministration of antibiotics and other medications. Aprescribing audit demonstrated 100% compliance forthe use and reason for prescribing, in line with the local
Surgery
Surgery
Good –––
22 Fulwood Hall Hospital Quality Report 01/06/2017

formulary. The medicines management policy alsooutlined directions for the storage, management andprescription of medical gases. We saw this was followedduring inspection.
• Medicines for ward and day case use were stored in alocked room in locked cupboards, including stock andtake home medications for patients. We checked fivedrugs at random in the stock cupboard and these werein date and matched stock records. Controlled drugswere kept in a separate locked cupboard, with randomchecks of three controlled drugs confirming all were indate and stock levels were correct.
• In theatre anaesthetic and recovery rooms, medicationswere locked in cupboards as directed by local policy. Adedicated pharmacy standard fridge was available formedicines’ storage and daily recording of fridgetemperatures were complete and up to date. Weobserved that log books for recording controlled drugswere signed as checked, with records complete and upto date. A log book for staff to ‘read and sign’ for localupdates, Ramsay Healthcare updates and alerts fromthe Medicines and Healthcare products RegulatoryAgency (MHRA) was in place, with this signed and datedby staff.
• A service level agreement (SLA) was in place with thepharmacy service of a local acute hospital trust. Amedicines reconciliation service was provided byrotational pharmacy staff to the ward, in a service levelagreement (SLA) from the local NHS trust. This coveredpharmaceutical care for patients at Fulwood HallHospital during their inpatient stay, in five half daysessions 9am-12 midday, Monday to Friday. The servicedid not provide any input to pre-operative assessmentclinic, although we were advised that this was underreview as part of the ongoing SLA. A pharmacytechnician was also on site one morning each week toundertake a weekly medicines stock-take, whichincluded medicine expiry date checks.
• On a daily basis, the pharmacist would review allpatients’ medications and double check any changes.There were occasions when patients were admittedafter 1.30pm and their medication review took place thefollowing morning. The pharmacist would refer to thepatients’ medication history and GP referral as a sourcefor any changes that may be required for patientmedications .These would be discussed with theResident Medical Officer (RMO), with any changesdocumented in the patient prescription.
• Pre- labelled medications for standard medicines suchas analgesia, laxatives and prophylaxis were supplied bythe trust. A secure medicines stock cupboard for routinemedications on the ward was re-stocked each week,from supplies at the trust. Email orders for medicinescould be requested by secure email from the hospital totrust pharmacy services. There were no concerns withconsultants requesting stocks items that were offstandard formulary for medicines.
• The pharmacist gave us an example of an issueregarding a patient commencing anticoagulantmedication during their inpatient stay. The patient hadnot been counselled prior to discharge and the patientwas later contacted at home. This issue was escalatedand the ward manager worked with the pharmacist toimplement a checklist to improve safety of patientsreceiving anticoagulants in the future. Development ofthis process had started at the time of our inspection.
Records
• The hospital had a medical records management policyin place, which took into account the requirements ofthe Data Protection Act (1998) and the Access to HealthRecords Act (1990). This set out responsibilities for allstaff members in the creation, handling, storage anddestruction of records. It also detailed standards forconfidentiality and set out rights to access records. Thepolicy was supported by a Caldicott guardian policy,based on the seven Caldicott principles and a clinicalrecord keeping policy, which set out the minimum datasets to be included within patient records. Informationsecurity incidents were recorded on the hospital’sincident reporting system.
• The hospital used paper based patient records. Therewas a robust process in place for the storage andmovement of all patient records within the department.Records needed were transferred to wards anddepartments from medical records each day and weresecurely stored in the nurses’ office and ward areas.During the inspection, we observed that a storagetrolley for case notes in the day case area was unlockedand unattended; however, we noted that staff wereusing the records intermittently at the time. We raisedthis to the ward manager, who noted this and ensuredstaff were instructed to maintain security of case notes
Surgery
Surgery
Good –––
23 Fulwood Hall Hospital Quality Report 01/06/2017

in storage trolleys on the ward at all times. On theunannounced inspection we saw case notes weresecurely kept in storage trolleys in ward and day caseareas showing an improvement.
• Except in the situation where treatment was transferredbetween the hospital and another regional RamsayHealth Care UK site, the hospital did not permit recordsto be taken off-site and all staff, including consultants,were aware of this policy.
• Patient records folders in each patient room includedrisk assessment information, patient information onMRSA, philosophy of care, policies and protocols andchaperone information.
• Nine sets of records were reviewed for patientsundergoing ophthalmic (eye) surgery. The patient’sconsent was clearly recorded in each case, with clearindication of which eye the procedure was to be carriedout. Patient name, date of birth, address and otherdemographic information was correctly recorded and allclinical entries were dated and signed by medical staff.
• We also reviewed an additional 12 sets of patient’spaper records. All were concise and legible with date,time and signatures completed.
• A hospital wide medical records audit programme wasin place which carried out checks quarterly. Between 1July 2015 and 30 June 2016, this showed a compliancerate of between 85% and 94%. The audits highlightedareas of shortfalls and identified the responsible personand date for completion. There was some indication inthe audit findings that similar shortfalls were still beingrepeated; this meant that actions to improve were notconsistently embedded.
• As the audits did not indicate which department or staffspeciality were involved it was not possible for us toidentify if any of the audit shortfalls related to staffwithin the outpatient, diagnostic imaging, orphysiotherapy departments.
Safeguarding
• The hospital had a number of safeguarding policies inplace, which were based on guidelines fromprofessional bodies and the Department of Health,
• The hospital had four on-site safeguarding leads. Theseincluded the registered children’s nurse (who was alsothe regional safeguarding lead), the regional adultsafeguarding lead, the outpatient department manager,and the physiotherapy manager. The hospital also had asafeguarding link nurse.
• Nursing staff completed safeguarding training to leveltwo, with the Resident Medical Officer (RMO) anddepartment leads completing level three safeguardingfor children and young people. Safeguarding vulnerableadults and safeguarding children training was includedin core mandatory training and completed by all staff..
• Non-clinical staff who had contact with children andyoung people were offered training to level two. Thismeant that staff were able to recognise and report, orobtain additional advice, if they identified a potentialsafeguarding concern.
• Although the hospital did not treat children under 16years of age, staff recognised the need to maintainsafeguarding children training as children oftenaccompanied adult patients. The registered children’snurse was notified by heads of department when it wasknown that a 16 or 17 year old patient was due to comeinto the hospital.
• Safeguarding policies covered a range of safeguardingissues including domestic abuse and female genitalmutilation (FGM). Staff were aware to be vigilant forindications of potential FGM or child sexual exploitation.Any concerns of this nature were discussed with theregistered children’s nurse who decided on any actionsto be taken.
• Clinical, non-clinical and administration staff were allaware of the types of issues that would need to bereported as a safeguarding concern or alert. All staff weasked referred to the safeguarding flowcharts displayedthroughout the hospital and were aware of the processto follow to obtain advice from the leads or to raise asafeguarding concern via the hospital’s incidentreporting system.
• A safeguarding calendar for staff training was in placeand staff held safeguarding discussions every month,with reflective discussion of cases. Topics on thecalendar included child exploitation and PREVENT (oneof the four elements of the government’scounter-terrorism strategy). FGM was part of thesemandatory training sessions with a 90 minute sessiondelivered by the paediatric safeguarding nurse.
• Staff received training in the PREVENT Strategy. As aresult of this training, a member of staff at the hospitalhad identified a patient who had potentially beenradicalised. The hospital notified the authorities whointervened with the individual involved. Easy to followflowcharts for actions to be taken where staff hadconcerns about patients who may be radicalised where
Surgery
Surgery
Good –––
24 Fulwood Hall Hospital Quality Report 01/06/2017

displayed in the departmental offices. These includedcontact details for the relevant leads in the hospital andin the police and had been used successfully by staff onat least one occasion. The hospital had threedesignated PREVENT leads
• The August 2016 monthly clinical services update fromthe provider identified a revised policy for safeguardingadults at risk of abuse and neglect. This also included asafeguarding topic of the month and lessons learned.
Mandatory training
• The hospital had a mandatory training policy. This wassupported by a mandatory training matrix thatidentified which courses staff needed to complete fortheir roles and the frequency that each course neededto be repeated. The policy set out employee’sresponsibility to ensure mandatory training wascompleted each year.
• Training was delivered through face to face training ande-learning packages for: data protection; emergencymanagement: fire and personal safety; equality, humanrights, and workplace diversity; health and safety;prevention of infection; information security; manualhandling; non-clinical basic life support; clinical basiclife support; and child protection. Nursing staff alsocompleted intermediate life support skills training (ILS)and other clinical skills training, such as for intravenousdrug administration and taking bloods.
• The hospital had an electronic system for recording andmonitoring mandatory training. The system highlightedany training due in red. The system was observed whilston site and training due was highlighted.
• Hospital figures indicated 98% of contracted staff on theward had completed their mandatory training, however,only 32% of bank staff in theatre, and 41% of bank staffin the ward were compliant with this. The hospital weretaking actions to improve the uptake of training withbank staff, including messages in wage slips andnewsletters. Efforts are ongoing by the HR Coordinatorsand the Heads of Department to improve further.
• Staff were provided with PREVENT training at theirmandatory training which gave them information andawareness about radicalisation.
Assessing and responding to patient risk
• The hospital admitted patients for surgery that wereconsidered low risk. A corporate admission criteriapolicy was followed using the local organisation’s
Pre-op Timelines Criteria (2016) document. Thisdocument provided a list of medical conditions thatwould exclude patients, for example trauma patients,bowel screening and patients with pacemakers. Someconditions were referred to matron for acceptance, forexample haemophilia. The document also stated thatchildren aged under 18 years would not be admitted forcosmetic or labial surgery. Patients were not rejected onthe basis of their Body Mass Index alone.
• Inpatient records reviewed included risk assessmentssuch national early warning scores (NEWS) and venousthromboembolism (VTE). NEWS had been adopted byRamsay healthcare and adapted to meet needs ofservices. NEWS were also noted as part of staffhandover.
• A sepsis pathway had been reviewed further to nationalguidance and nursing staff had completed local wardbased training sessions as an update for thisinformation.
• In surgical theatres, the World Health Organisation(WHO) Five Steps to Safer Surgery procedures werefollowed, as detailed in guidance from the NationalInstitute of Health and Care Excellence (NICE). Twosurgical patients were observed used this checklistduring our inspection, with two WHO checklistsobserved.
• Records of patients undergoing cataract eye surgeryincluded WHO checklists for cataract surgery, inaddition to an inpatient assessment form specifically forpatients undergoing this procedure.
• A designated member of theatre staff, generally anOperating Department Practitioner or anaestheticnurse, acted as a list safety officer in the anaestheticroom. This measure had been put in place in responseto an historic never event, with regard to WHO checklistprocess.
• Theatre policies were available in the theatre office anda copy of the major haemorrhage policy was besideeach phone in the theatre department.
• Although the hospital did not treat patients under theage of 16, all staff were trained in paediatric basic lifesupport. The registered children’s nurse was trained toEuropean paediatric advanced life support (EPALS) andthe Resident Medical Officer (RMO) was trained toadvanced life support level.
• The Registered Medical Officer (RMO) and one theatrenurse had completed training in Advanced Life Support(ALS) and Advanced Paediatric Life Support (APLS) skills,
Surgery
Surgery
Good –––
25 Fulwood Hall Hospital Quality Report 01/06/2017

with two theatre staff waiting to undertake this course.All qualified nursing staff completed Intermediated LifeSupport (ILS) skills training, with healthcare assistantscompleting Basic Life Support (BLS) training. No theatrestaff were trained in transporting critically ill patients fortransfer, if this was necessary the hospital called thelocal ambulance emergency service.
• There was 24 hour cover on site at the hospital from theRMO. The RMO carried a mobile intercom and could bereached throughout the hospital. Where a patient’scondition was changing or deteriorating, the RMO wouldinitially review the patient. If the RMO had furtherconcerns, they would raise contact with the individualconsultant to discuss further. The RMO advised therewas no difficulty in consultants’ responses, all wereusually available on contact or replied within a shorttime after contact. There were good communications inplace with nursing staff who would initially raiseconcerns to the RMO.
• In cases where patients required emergency transfer tothe local NHS hospital, there were goodcommunications for this with the on call medical orsurgical services. A patient transfer case was describedwhere there had been complications following surgery.The RMO had liaised with the on call registrar toco-ordinate the patient’s admission via the accident andemergency department.
• The hospital had implemented a falls assessmentprogramme as part of the admission process, to identifyand reduce incidents of falls in patients who may be atrisk.
Nursing and support staffing
• Staffing levels were planned and reviewed using theproviders electronic rostering management system,which embedded indicators for safety and effectiveness.The system enabled heads of departments to managerotas, shift allocations, annual leave and sicknessabsences, skill mix and staff requirements includingsenior cover.
• Staff told us that staffing was reviewed on each shiftaccording to admissions and patient acuity. Shift timeswere altered to meet the needs of the service and staffworked flexibly; this was confirmed in review of shiftrotas during inspection.
• Nursing handovers were held prior to each shift on theward, incorporating a recorded handover and a written
handover sheet. Patient details, including theircondition and mobility, medications, allergies,treatment plans and investigations required werediscussed during the handover.
• A pre-operative assessment clinic was held on Mondaysto Fridays, staffed by a lead sister, three staff nurses andtwo healthcare assistants. All surgical patients wereadmitted for planned procedures and patient acuity wasdetermined during pre-operative assessmentappointment.
• We saw good practice in the use of association forperi-operative practice (AFPP) guidelines. Staff wereallocated to theatre lists based on their skills andcompetencies. The role of surgical first assistant was notin place at the hospital, however four nurses were dueto be seconded to undertake this training fromSeptember 2016.
• Staff sickness rates between 1 July 2015 and 31 June2016 varied with an expected peak during the wintermonths. Average sickness rates for this period were 6%for registered ward nursing staff, 7% for ward health careassistant staff, 10% for theatre registered nursing staff,and 10% for theatre registered operating departmentpractitioner’s.
• Staff turnover rates between 1 July 2015 and 31 June2016 were low at 3% for registered nursing staff and 1%for health care assistant staff. In the theatre area for thesame period, there was a turnover of 13% of nursingstaff.
• The theatres and inpatient ward used bank staff whenadditional staff were required. The hospital did not useagency staff.
• At the time of our inspection, there was a vacancy for anew position of theatre deputy manager. There werethree vacant posts for operating departmentpractitioners (ODPs) or registered nurses (RNs) to workin scrub, anaesthetics and recovery areas in theatres.Data provided by the hospital showed the vacancy ratefor theatre health care assistants was above the averagecompared to other similar independent hospitals.However, permanent and bank staff worked flexibly inorder to ensure shifts were fully staffed as required.
Medical staffing
• The hospital had one resident medical officer (RMO), adoctor who resides at the hospital and is on call 24hours per day seven days per week, who was employedby a third party employer. A pre-employment training
Surgery
Surgery
Good –––
26 Fulwood Hall Hospital Quality Report 01/06/2017
file was provided to the hospital before each RMOarrived, for review and sign-off by matron. The RMO inpost at Fulwood Hall Hospital had worked at thehospital for 18 months and his file was complete and upto date.
• The RMO usually worked on a ward floor for a maximumof eight to nine hours per 24 hour shift on duty and notreceive more than five night calls in a seven day period.There was an escalation process in place to obtainstandby relief for a 24 hour rest break, if there was asignificant increase in the workload. Whenever possiblea doctor who was experienced with the hospital wasutilised for 24 hour relief cover.
• The RMO had daily contact with their employer formonitoring of their hours of duty and the number oftimes they had responded to calls during the night. Theemployer’s medical support team provided ongoingsupport staff to provide continuity of cover for when theRMO had completed their hours of duty
• The RMO had full access to consultant surgeon andanaesthetist contact details. All consultants withpractising privileges at the hospital provided 24-houron-call cover for patients post-operatively and werewithin a 30-minute drive time to the hospital. Where asurgeon was not available for a period of time a buddyarrangement was in place with another surgeon withinthe same specialty or sub-specialty. Where a surgeonwas on holiday or unavailable they also ensured thatappropriate cover was provided by their surgicalcolleagues.
• Radiologists provided on-call cover in case of need forurgent diagnostic services.
Emergency awareness and training
• The hospital had a business continuity managementpolicy, which included response and contingency plansfor unexpected events. Fire and bomb threat procedureswere displayed on office noticeboards in all threedepartments.
• Staff completed fire safety training as part of mandatorytraining and were aware of major incident responseplans.
• There was a hospital-wide resuscitation team in placefor responding to medical emergencies. This was led bythe RMO with a team of nursing and support staff, whowere all trained in advanced life support skills for adultsand children.
• Generators were available if there was a power failure.These were maintained by the hospital’s facilities team.
Are surgery services effective?
Good –––
We rated effective as good.
Evidence-based care and treatment
• The hospital’s policies and protocols were standardisedby Ramsay Health Care UK. They incorporated up todate recommendations and guidelines from theNational Institute for Health and Care Excellence (NICE)and other professional bodies including the relevantRoyal Colleges. Guidelines from the Association ofAnaesthetists of Great Britain and Ireland (AAGBI 2012)were utilised in theatres for checking anaestheticequipment.
• We saw evidence that updated clinical guidance wasreviewed by Ramsay Health Care UK and fed into thehospital’s clinical governance and medical advisorycommittees. A process was in place to determinewhether or not the guidance was applicable to theservices the hospital provided.
• We saw evidence of current guidelines of treatmentbeing implemented following a medical advisorycommittee (MAC) meeting. Decisions to changeprocesses were communicated to all staff, includingappropriate visiting consultants via letter and email andcascaded through staff meetings. Clinicalcommissioning groups were also updated.
• Clinical policies and procedures which reflectednational guidance were in place for staff to access onthe hospital intranet. Care pathways for treatment at thehospital were based on national guidance, includingfrom the National Institute of Health and CareExcellence (NICE) and Royal College of Surgeons (RCS).
• The hospital had a well embedded audit programme.This was largely routine practice checklists such asrecord keeping, medicines management and infection,prevention and control with no processes for reviewingclinical outcomes. The audit results were consistentlypositive. On the occasions where audit results droppedslightly, improvements were made the following month.
• We saw examples of additional clinical auditsundertaken as part of the commissioning for quality and
Surgery
Surgery
Good –––
27 Fulwood Hall Hospital Quality Report 01/06/2017

innovation (CQUIN). The hospital had a goodrelationship with its commissioners and used the CQUINprogramme to drive improvements and seek qualityopportunities. One of these had been to work with NICEto look at how the hospital could become moreinvolved.
• National Safety Standards for Invasive Procedures(NatSIPPS) were being introduced in theatres. NatSIPPShad been developed by NHS England as an additionalapproach to promote patient safety in surgical care.NatSSIPPS provide a framework for the development ofLocal Safety Standards for Invasive Procedures(LocSIPPS) by local clinicians and their patients. Thiswould allow the hospital to build on existingstandardised patient safety approaches, such as theWHO checklist.
Pain relief
• During pre-operative assessment, patients were askedabout their preferred post-operative treatment for painmanagement and this was reflected in care plans.
• The provider had a post-operative pain managementpolicy that was followed in the hospital. The policyincluded a pain score tool from one to ten was used forassessment of patients’ pain levels. The assessmentalso took into account current analgesia levels,non-verbal indicators and levels of discomfort.
• Patients were offered pain relief on the ward on aregular basis and told us their pain was well managedfollowing surgery and they had no complaints regardingthis.
• Record folders in patient rooms included National EarlyWarning Score charts for pain, which staff completed.We observed that pain management was also discussedin handover.
• Surgical patients were routinely contacted by telephone48 hours after discharge and asked whether or not theirpain was at an acceptable level, with advice given by aqualified nurse.
Nutrition and hydration
• Ramsay Health Care UK Operations Ltd. had a nutritionand hydration summary and goals document. This wasformulated by a nutrition and hydration link nurseproviding guidance, leaflets and education forcompletion of fluid balance charts. Patients wereassessed both pre-operatively and as inpatients using
the NICE recommended Malnutrition UniversalScreening Tool (MUST). A nutrition and hydration weekhad been held at the hospital between 14 and 20 March2016 to focus development in this area.
• Patients’ nutritional needs were assessed duringpre-operative assessments. Patients were offered quickaccess to appointments, with low waiting times tominimize the length of time they were nil by mouth.
• Training was provided by the Ward Manager on fluidbalance completion, with regular dates displayed instaff areas.
• The catering department provided meals to inpatientsand staff members and one patient told us that the chefwould speak to patients regarding their needs.Managers told us that the chef made daily calls topatients and could provide a range of meals for patientswith allergies or food preferences.
• Theatre fasting times were discussed during ward teammeetings in March 2016 and noted in the minutes. Theplan was to reduce fasting times for patients. Advice wasfor patients to eat as soon as possible following surgeryand if this was not achieved, it should be fullydocumented in records.
• Patients were asked about their tolerance of diet andfluids in a routine call, 48 hours post discharge. If therewere any negative answers to these questions, patientswere contacted for further assessment and advice by aqualified nurse.
• A nutrition and hydration audit undertaken in May 2016showed compliance at 98% which was a positiveoutcome.
• There were a large number of patient informationleaflets available for patients with specific dietaryrequirements. These included dietary advice for glutenfree diets, diabetes and carbohydrates, healthy eatingwith kidney problems and eating to protect your heart.
Patient outcomes
• Between July 2015 and June 2016, there were tenpatient readmissions to surgery within 28 days. This wasbetter than other independent acute hospitals of asimilar type.
• There were five unplanned returns to theatre between 1July 2015 and 30 June 2016. Three of these werepost-surgical infections which occurred between Julyand September 2015. A root cause analysis (RCA) hadbeen completed and there was found to be nocorrelation between these cases, all had occurred in
Surgery
Surgery
Good –––
28 Fulwood Hall Hospital Quality Report 01/06/2017

different theatres involving different staff and surgeons.Theatre air filters were checked and one was changed asa precautionary measure and decontamination issueswere reported from theatres to the localdecontamination hub following this finding. The othertwo returns to theatre were following a fall and forwrong lens surgery
• There were 20 unplanned transfers of patients to otherhospitals during the reporting period. This was not highcompared to other independent hospitals of a similartype at 1.5% of the number of patients treated. TheResident Medical Officer explained the decision makingprocess and gave us appropriate examples of patienttransfers. The nearest acute NHS hospital with anaccident and emergency department wasapproximately two miles from Fulwood Hall Hospital.
• Between July 2015 and June 2016, the hospitalparticipated in national and local audit programmes tomeasure treatment and care outcomes for a number ofconditions. Data was submitted to national auditprogrammes for the National Joint Registry (NJR) andthe global rating scale (GRS) annual report card forendoscopy.
• The National Joint Registry (NJR) collects informationon all hip, knee, ankle, elbow and shoulder replacementoperations, to monitor the performance of jointreplacement implants and the effectiveness of differenttypes of surgery. NJR data shows that between 1November 2015 and 31 October 2016, the hospitalcarried out 308 hip, 434 knee, and 13 shoulder jointreplacements with an average patient consent rate of99.6%.
• Elective surgery performance reported outcomesmeasures (PROMs) for hip, knee and groin surgery werereported and these outcomes were monitored at thehospital’s clinical governance committee.
• PROMs data for primary knee replacement showed, outof 220 records, 80.9% were reported as improved, with8.2% as worsened. PROMs data for primary hipreplacement showed out of 192 records, 87.5% werereported as improved and 7.3% reported as worsened.
• CQUIN audits of patient outcomes for hip and knee jointreplacements were similar to other hospitals in theNorth West region.
• The hospital offered cosmetic procedures such as breastsurgery, tummy tuck and rhinoplasty. These patientsaccounted for 2.8% of the total number of surgicalpatients treated. There were 239 cosmetic surgerypatients treated between July 2015 and June 2016.
• The Private Healthcare Information Network (PHIN)collects data from hospitals to produce information vitalsafety and quality indicators such as mortality rates,readmission rates and patient feedback. The firstperformance measures for hospitals are expected to beavailable from April 2017. Ramsay Health Care UK wasworking with PHIN to enable data to be provided.
Competent staff
• The hospital also had an induction policy, which wassupported by an induction booklet and checklist. Thepolicy set out the responsibilities of all relevant staffmembers, including the new employee. Staff confirmedinduction was completed on recruitment.
• Nursing staff supported student nurses during theirstudent placement on the ward. Student nurses wespoke with told us they had good support from staff asmentors on the ward and spoke positively about theirexperiences. One student said that all staffcommunicated and worked well with each other andthat it was like a family environment. Following a reallyenjoyable experience of being on the ward, one studentwas applying to join the bank staff for the hospital.
• Health Care Assistants were supervised by nursing staffto triage pre-operative assessment surveyquestionnaires, completed by patients prior to theiradmission.
• Fulwood Hall hospital had a continuing professionaldevelopment (CPD) policy in place. The policy set outstaff responsibilities to maintain an up to date CPD file.Funding existed for formal learning activities within boththe corporate and local training budgets and throughthe Ramsay Health Care UK Scholarship Fund. Staffcould request training through the Ramsay Health CareUK Academy prospectus.
• Consultants applying for practicing privileges,authorisation from the hospital to provide patient careand treatment, were interviewed by the HospitalManager and the Matron, and had to supply copies oftheir training certificates. Comprehensive additionalchecks were also made in accordance with RamsayHealthcare policies for granting practising privileges.These were reviewed every five years.
Surgery
Surgery
Good –––
29 Fulwood Hall Hospital Quality Report 01/06/2017

• There were procedures in place for reviewing the RMO’ssuitability to practice, with the Matron reviewing theirappropriate training and experience, prior to this beingapproved by the MAC committee. After appointment,the RMO would complete a period of supervisedinduction, supported by the Matron, completing relatedchecklists. The RMO completed annual appraisals andreviewed development objectives with the ClinicalMedical Lead, maintaining up to date evidence formedical revalidation. A quarterly assessment of this wasgiven to the hospital for feedback. Competency wasassured with the RMO undergoing mandatory training.This included advance life support (ALS), Europeanpaediatric life support (EPLS), NHS better bloodtransfusion, infection prevention and control, the MentalCapacity Act and Deprivation of Liberty Safeguards,equality and diversity, safeguarding children (levelthree), safeguarding vulnerable adults effectiveteamwork; data protection, manual handling and firesafety.
• The hospital also had a policy in place for responding toconcerns about a doctor’s practice. It set out the actionsto be taken when concerns were raised about anyGeneral Medical Council registered doctor in thehospital. It also detailed the level of support that wouldbe provided to the doctor, including retraining shouldconcerns be founded. The policy enabled information tobe discussed and shared between the doctor’sresponsible officer and the GMC liaison officer. Thepolicy did not set out any details about informing otherlocal healthcare providers about the concerns. However,this would be considered on a case by case basis.
• In operating theatres, one of the scrub nurses hadbecome a practice development practitioner, with linksto the local university. Theatre nursing and operatingdepartment practice (ODP) students were supportedwhilst on student placement at Fulwood Hall Hospital.Staff in theatres were positive about the opportunitiesfor continuing professional development that wereavailable through Ramsay Health Care UK OperationsLtd.
• Bank staff were regularly used to provide nursingsupport in theatres and we observed that an inductionprocess was completed and recorded for these staff.
Multidisciplinary working
• There was good communication between the hospitaland the local NHS trust. On occasions where patientsneeded to be transferred to local acute hospitals forurgent care, nursing staff would continue liaison for anyfurther follow up required.
• Pharmacy services were provided to Fulwood HallHospital in service level agreement with the local NHStrust. We observed that day to day communications andprocesses for this service were clear and efficient, withpatients receiving appropriate and timely medicationsfor their needs.
• Communications with other clinical services wereestablished, including for physiotherapy, whichprovided rehabilitation care as inpatient andoutpatients services.
• Staff at all levels reported there were good workingrelationships with consultants and the RMO, who wereeasily accessible when required.
• The hospital had a GP liaison officer available whowould communicate with doctors’ surgeries andproduced a GP newsletter to keep them updated onprogress, staffing and services at the hospital.
• There were communication systems in place for liaisonwith GPs, district nurses and social care services.
Seven-day services
• The RMO was based at the hospital 24 hours a day,seven days a week. The RMO had access to consultantcontact details in case of any further patient advicerequired. Consultants all were within a 30 minute drivetime of the hospital.
• The physiotherapy service provided a six day service forinpatients Monday to Saturday 8am to 5pm. Diagnosticimaging services were provided Monday to Saturday. Anon call facility was available for urgent diagnosticimaging services overnight and at weekends
Access to information
• Staff had access to the hospital’s policies andprocedures and to professional guidelines, on thehospital computer system. A hard copy of the policieswas also available in the hospital’s restaurant area
• Patient records were available in note trolleys in clinicalareas. Discharge letters were completed in a timely wayand we observed records of letters to GPs and patients.Patient notes were flagged to alert staff to individualpatient needs, such as diabetes, or equipment needs.
Surgery
Surgery
Good –––
30 Fulwood Hall Hospital Quality Report 01/06/2017
• Consultants with practicing privileges were notpermitted to remove records from the hospital, whichmeant that staff had good access to the informationrequired at the point of care.
Consent, Mental Capacity Act and Deprivation ofLiberty Safeguards
• The hospital had consent to treatment for competentadults and children/young people policy. The policyclearly set out that a person’s capacity to consent tocare and treatment was on a decision-specific basis.This meant that staff needed to consider a person’scapacity to understand the information being given,ability to retain the information to make a decision, touse or consider the information and to be able tocommunicate their decision. Interpreter services wereavailable if needed.
• Although the consent policy was robust and in line withrelevant guidance, the policy we reviewed had expiredin January 2016. This was escalated during theinspection. Staff were aware of the policy and how toreport any concerns about a patient’s mental capacityto consent.
• The hospital developed a flowchart for assessingconsent, which had since been shared with andimplemented by an NHS acute trust in the region.
• The hospital carried out a quarterly consent audit. Therehad been an improvement in compliance by staff in theconsent process from 77% in July 2015 to 88% in March2016, followed by a reduction to 84% in June 2016.However, recurring themes of non-compliance relatedto recording of full patient details on each page of theform; clear recording of the performing clinician’s name;and, evidence of the provision of information to thepatient. Action plans were in place to remind staff atteam meetings about following correct consentprocedures. The audit carried out in September 2016demonstrated a significant improvement at 97%compliance with the policy.
• During inspection we observed consent proceduresbeing followed appropriately. We also reviewed 21records where we saw consent records were completeand accurate.
• The Ramsay consent policy contained a specificstatement regarding patients for cosmetic surgery. Thisfollowed the General Medical Council and Royal Collegeof Surgeons guidance and included a two-stageConsent process with a cooling-off period of at least two
weeks between the stages to allow the patient to reflecton the decision. Where the two week cooling off periodwas not possible, reasons were recorded in the patient’smedical record. Information on the procedure was givento patients at a different time to the signing of theconsent form. All Cosmetic Surgeons and Fulwood Hallstaff are fully compliant with this policy.
• The hospital also had a Mental Capacity Act policy and aDeprivation of Liberty Safeguards (DoLS) policy in place.Consent and mental capacity were also taken intoaccount in the hospital’s safeguarding adults at risk ofabuse or neglect policy. Staff were aware of the policy.Staff we spoke with told us what the processes were toraise a DoLS application but had not done it.
• The hospital had a dementia screening tool. All patientsover the age of 65 who were referred to the outpatientdepartment were screened for dementia.
• Mental Capacity Act e-learning training was availableand a signature sheet was available for staff to sign oncompletion at the nurses’ station.
Are surgery services caring?
Good –––
We rated caring as good.
Compassionate care
• Nurses said they felt they had time to care and wereable to dedicate all of their time to patient care. Staffspoke of having honesty and openness whencommunicating with patients. One nurse said thatpatients want to know that if you say you are comingback in a minute, then you will be.
• The hospital submitted data to the NHS Friends andFamily Test and scored mainly better than the Englandaverage of NHS patients from January to June 2016.Overall Friends and Family Test scores for NHS fundedpatients were an average of 99% during this period. Thehospital recorded the data as outpatient, inpatient andday case. The monthly data was consistently highscoring with a range of 98-100%. The hospital met itsresponse rate threshold target of 40%; the averageresponse rate for inpatients during this period was 64%.All patient comments were recorded and any negativecomments were highlighted in order to promoteimprovement where possible.
Surgery
Surgery
Good –––
31 Fulwood Hall Hospital Quality Report 01/06/2017

• We observed staff talking to patients and their familiesin a courteous and helpful way, respecting their dignity.We heard one nurse responding to a patient during aphone call, when they needed to cancel their surgerydue to illness. The nurse was reassuring and providedthorough information when talking to the patient,transferring their call immediately in order to rearrangethe admission. The patient was informed that theconsultant would be advised of the cancellation and thereason for it. The nurse spoke calmly, in a caring andunderstanding way, taking time to ask if they hadeverything they needed and not to hesitate to contactfor any further advice.
• Staff told us they were more aware of the needs ofvulnerable patients, following specific training in thisarea. We saw written evidence of this in patient’s notes,where staff had considered the patients’ individualcircumstances, identifying relevant issues regardingindividual patient care needs.
• A patient told us the care they received was so goodthey were prepared to travel 100 miles to Fulwood HallHospital for further treatment. Another patient statedthey were put at ease, everything explained clearly andthey were made to feel special.
• Patient led assessments of the care environment(PLACE) audits were completed between February andJune 2016 and scored similar to or better than theEngland average, including food (92%), privacy, dignityand well-being (83%)
• The pre-admission treatment room was used forindividual clinic appointments for patients booked forsurgery. This room was used by up to four members ofstaff at a time and two patients, both as an office baseand for individual assessments. The room was crampedand there was only a curtain to separate the two patientcubicles. Staff working in the room would often turn onthe radio in order to limit patient conversations beingoverheard. Staff said they managed as best they could inthis environment and there had been no complaintsfrom patients. Where it was possible, patients were seenfor pre-assessment appointments in rooms on the mainward.
Understanding and involvement of patients and thoseclose to them
• Patient feedback was received from a variety of sourcesand was positive about the care and treatment received.We received a large number of feedback cards and
comments included “Fulwood Hall is amazing, all staffand consultants take time to listen and your care andtreatment is to the highest of standards. The hospital isclean and hygienic at all times.” and “Staff wereextremely caring. Answered all questions. Gaveattention when requested. Sympathetic butappropriately firm with aftercare (e.g. getting out of bedafter knee replacement surgery) Benefits explained.Beautiful clean facilities, spacious and safe. Day or nightattention perfect.”
• NHS Friends and Family test data showed high rates ofevaluation for service provision.
• Patients told us they had been provided withinformation about their operation and they knew whatto expect from their treatment. Patients felt involved inmaking decisions about their treatment and choiceswere explained.
• Nurses introduced themselves when speaking withpatients and relatives; patients reported they weretreated with respect and were involved in care planning.
• Senior staff told us the patient was always the focus ofcare and staff gave us examples of how they hadsupported individual’s needs. One example was apatient who presented for surgery and brought herassistance dog. At short notice the hospital foundsuitable accommodation and the staff left the hospitaland purchased a bed and food to enable the dog tostay.
• The hospital had arranged an afternoon tea formembers of a local GP practice as a PatientParticipation Group. This enabled patients to visit thehospital before their treatment and involve thecommunity.
Emotional support
• The hospital had a number of policies to address theemotional care needs of patients, including abereavement policy, a palliative care policy and achaperone policy. These policies reflected theorganisation’s intention to respect the uniqueness ofpatients and families’ needs, involving them inpatient-centred goal setting and care planning.
• One patient told us how they had been able to stayadditional days following surgery in order to feel moreconfident and prepared for discharge home.
Surgery
Surgery
Good –––
32 Fulwood Hall Hospital Quality Report 01/06/2017
• Staff were able to make notes of patients’ specificemotional needs to others caring for them using thecommunication slip added to the healthcare record.Patients were routinely contacted after discharge tooffer advice and check on pain levels.
• Patients were supported on discharge with informationon how to manage their specific conditions, nurses toldus they spent time ensuring patients understood.
Are surgery services responsive?
Good –––
We rated responsive as good.
Service planning and delivery to meet the needs oflocal people
• The hospital worked with other stakeholders to planand deliver its services to meet the needs of localpeople. The hospital’s Quality and ImprovementManager met regularly with the clinical commissioninggroup in contract and service development meetings.This enabled regular review of the hospital’s contract,the services offered and identification of local healthtrends.
• These meetings included discussion of progresstowards meeting the hospital’s agreed Commissioningfor Quality and Innovation (CQUIN) programme. Thehospital had achieved a number of CQUIN goals, forexample becoming a dementia friendly environment,but was also participation in the working towards fallsprevention across the Lancashire region goal.
• A GP liaison manager provided links between thehospital, the local primary care services and the clinicalcommissioning groups.
• The hospital recognised that increasing demands for itsservices was not being matched by the physical capacityof its facilities. It had developed business plans toincrease the size of the hospital which were to bereviewed by the board imminently. In the interim, dailyslot utilisation and weekly capacity meetings were held.
• The hospital had identified a pathway in pre-operativeassessment clinic that could be improved. If, duringtheir clinic appointment, it was identified that thepatient required an echocardiogram, they would have toreturn to their GP for a referral. Initial discussions were
proceeding with the local acute NHS trust andcommissioners to enable an urgent referral to be madethat would prevent delays and possible cancellation ofsurgery.
• A pre-operative assessment clinic was provided fivedays a week, offering patient assessment appointmentsprior to their surgery. Patients would be booked forsurgery from their consultant outpatient appointmentand referred for this assessment. Most patients waitedan average of four to six weeks for this, although somecould also be seen the week following their outpatientappointment when this was needed.
• Patients had access to patient information leafletsabout their condition. Some of this core information,including MRSA, sepsis and preventing wrong sitesurgery, was provided in patient folders in theirindividual rooms. Patients said they felt involved indecisions about their care and treatment.
Access and flow
• The hospital had a waiting list and management ofpatients accessing NHS treatment policy. This set outkey principles of how the hospital would managepatients waiting for treatment, with priority given tothose with urgent clinical need. The principlesincorporated the NHS 18-week referral to consultant-ledtreatment pathway (with diagnostic tests to be carriedout within six weeks). The policy detailed when the‘clock’ would stop and start, including for patients whodid not attend their appointments.
• The hospital demonstrated consistently high admittedfor treatment figures between July 2015 and June 2016.For eleven months, more than 97% of patients wereadmitted within 18 weeks of referral. In June 2016, theyrecorded the lowest figure of 94%, which is still abovean indicator of 92% for England.
• Patients we spoke with reported positive experiencewith choose and book system. They had experienced nodelays in the appointments system.
• Staff told us they liaised with GP’s, community staff andsocial services to ensure effective discharge to meetpatients’ needs and ensure a responsive, timely andsafe discharge.
• The hospital had cancelled 182 procedures for anon-clinical reason in the 12 months prior to ourinspection. Of these, 98% (179) patients were offered
Surgery
Surgery
Good –––
33 Fulwood Hall Hospital Quality Report 01/06/2017

another appointment within 28 days of the cancelledappointment. The number of cancelled procedures wasequivalent to only 1% of the total number of proceduresbetween July 2015 and June 2016.
Meeting people’s individual needs
• A simple communications slip was developed to identifypatients with additional needs. This was attached to thepatient record and meant that all staff were made awareof the patient’s needs as they progressed through thehospital and treatment pathway.
• We observed that details regarding any individualadditional needs were recorded in the ward diary inpreparation for patients who were due to be admitted inthe coming days. These included an order for a diabeticdiet for a patient, an air mattress for another patient anda hoist to aid moving and handling. Individual patientstickers were attached to each request to identify eachrequest.
• There were systems in place to flag up patients beingadmitted for cataract eye surgery who had additionalmedical conditions, such as diabetes. Administrativestaff would note any flags from referral details andwould print these details onto the booking form. Thiswould then be noted in the ward diary on the patient’sday of admission. We observed on one day of inspectionthat medical conditions for three patients had beenflagged in this way, in a theatre list of 36 patients.
• Mandatory training for staff included training onequality, human rights, and workplace diversity.
• Interpretation services were available through LanguageLine for people whose first language was not English.Staff told us the need for an interpreter was usuallyincluded on the referral form.
• The hospital supported Muslim staff, and patients, tofind a suitable place to pray.
• The hospitals patient-led assessments of the careenvironment (PLACE) score for the period February 2016to June 2016 for dementia was 71%. This was worsethan the national average (80%) for independenthospitals that have been assessed. However, for thesame period, the hospital scored 83% against a nationalaverage of 81% for patients living with a disability. Wesaw that a number of initiatives were in place forimproving care of patients with dementia.
• Appointments for pre-operative assessments wereoffered longer time slots to allow for identifying anypatients with particular medical issues. This would
include for example, patients who had issues withmedications, or diabetes that was not well controlled.Patients completed a questionnaire, which wasreviewed by health care assistants, who also completedinitial blood test and screening checks. All patients overage 50 completed electrocardiogram (ECG) screening aspart of pre-operative assessment.
• The patient’s age and medical history, together with thelevel of surgery being proposed determined the lengthof appointment time for pre-operative assessment.Patients with no medical history who were undergoingsmaller surgical procedures were offered shorterappointments.
• We observed patients undergoing a pre-operativeassessment appointment and saw that clearinformation was provided by nursing staff to patientsabout their planned surgery, including advice forpre-admission and anaesthetic fasting. Patientquestions were answered, including advice for onepatient on antibiotic treatment for an infection that thismay result in their surgery being postponed. The nurseadvised they would need to check this again with theconsultant and get back to the patient.
• Where indicated, nurses completed a falls assessmentquestionnaire and this was included in the patientrecord. Patients were given leaflets with informationabout the hospital and their surgery, as well as leafletsregarding deep vein thrombosis
• We saw that additional care systems which had beenestablished for patients living with dementia were beingfollowed by staff, including flags from pre-assessmentappointments and ward diary notes. Staff told us theywere more aware of the needs of patients in vulnerablecircumstances, following their safeguarding andPREVENT training.
• A dementia package had been introduced to provide forthe needs of patients who were living with dementia.This would be identified during the pre-operativeassessment appointment and further actions would bedetermined from this. For example, patients would beintroduced to a named nurse and offered pre-admissionvisits to familiarise themselves with the ward areas. Theprovider was planning to introduce the ‘forget-me-not’scheme to develop further support in meeting the needsof patients living with dementia.
• The hospital had engaged with a number of differentpatient groups, such as the Alzheimer’s’ society in orderto develop understanding of individual patient needs.
Surgery
Surgery
Good –––
34 Fulwood Hall Hospital Quality Report 01/06/2017

• Following work with the Alzheimer’s Society on ‘John’sCampaign’, the hospital introduced the ‘This is me’booklet for relatives and carers to provide details of thepatient’s personal preferences and needs. It had alsodeveloped a separate leaflet for carers ‘Workingtogether’ to understand how hospital staff could workwith, and support, them in the care of their relative.
• Nurses confirmed that an e-learning dementia packagehad been developed to support them in caring forpatients who were living with dementia. They said thisissue had been particularly highlighted when a patientwith dementia was on the ward, but their relatives hadnot always been available to stay with them. It wasidentified from this situation that wider supportmeasures were needed in order to respondappropriately to the individual needs of patients livingwith dementia.
• A resource box containing information for staff regardingpatients living with dementia or were blind wasavailable in the ward clerk’s office and this informationwas cascaded and documented in the ward meetingminutes.
• The hospital accommodated pre-admission visits forpatients living with a learning disability so they couldfamiliarise themselves with the environment prior totheir treatment. This visit aimed to reduce patientanxiety, introducing the nursing team and identifyingany specific individual requirements, such as equipmentor dietary needs.
• Further to an incident with a patient, the hospital hadimplemented and developed an assisted dogs policy tosupport the needs of people who were visuallyimpaired. This raised staff awareness of assistance dogsand set out the steps to be taken at various points in thepatient pathway to accommodate the needs of a patientwith an assistance dog.
• The Accessible Information Standard requires providersof NHS care to make information available to patientswho have information or communication needs relatingto a disability, impairment or sensory loss in a way thatthey can read, receive or understand. The hospitalcomplied with this standard. A communication slipaccompanied patient’s notes which indicated to staffany information or communication needs, and easyread leaflets were available for patients.
Learning from complaints and concerns
• The hospital had a management of patient complaintspolicy. The hospital aimed to acknowledge allcomplaints within three days and provide a fullresponse within 20 working days. In the period of July2015 to June 2016, the hospital received 44 complaints.The rate of complaints received was about the same asother independent hospitals we hold data for. Nocomplaints progressed to the Health ServiceOmbudsman or to ISCAS (Independent HealthcareSector Complaints Adjudication Service).
• The acknowledgement timescales for these complaintswere met. However, eight of the 44 complaints on thelog had extension letters sent. We could not determinethe length of delays from the log as the ‘Date final reply’column was actually the date a response was due by asopposed to the date the final response was sent.
• The Hospital Manager was responsible for responding tocomplaints; however, investigation of the complaint wasassigned to appropriate managers or staff. Details of allcomplaints were logged on the hospital’s incidentreporting system; the complaint incident report wasupdated at regular intervals throughout theinvestigation. There was also a process in place forpatients to escalate the complaint regionally andnationally.
• We reviewed a sample of six complaints. Of these, fourwere responded to later than the 20 working day target.In all four cases, a holding letter explaining the delaywas sent the day before the response was due. Thelongest delay in a response from this sample was threeweeks.
• Complaints were discussed by the clinical governancecommittee and learning shared with the qualitycommittee group, which was attended by the heads ofdepartments.
• Learning was also shared between the northern RamsayHealth Care UK sites through the northern matron’smeetings. Learning from systemic complaints wasshared with all Ramsay Health Care UK organisations ata corporate level. Learning was shared with staff in staffmeetings, through the ‘Lessons learnt’ briefing andthrough the hospital’s staff newsletter.
• Lessons learned from complaints were circulated tostaff in a clinical services monthly update newsletter.This also included update information regardingpolicies, pathways, clinical governance and training.
Surgery
Surgery
Good –––
35 Fulwood Hall Hospital Quality Report 01/06/2017

• Staff were given customer service training to assist themin dealing with complaints from patients. Staff told usthey attempted to resolve verbal patient concerns at thetime they were raised with staff. However, staff wereaware of the hospital’s complaint policy.
• We were given an example of staff resolving issues andlearning from experience. An inpatient who was blindexpressed his discomfort that he knew someone was inhis room but had not introduced themselves. Apologieswere made, the issue was raised and all staff were madeaware. Staff told us they now introduce themselveswhenever they enter a patients room.
Are surgery services well-led?
Good –––
We rated well-led as good.
Leadership / culture of service related to this coreservice
• The hospital was led by a general manager, who wassupported by a senior management team consisting ofthe matron, finance manager, operations manager andGP liaison.
• The management team understood the challenges onthe hospital to provide good quality care and were openand honest in sharing their concerns. The problem ofspace and capacity was an issue that was beingmanaged with daily slot utilisation and weekly capacitymeetings.
• Managers were encouraged to attend nationalconferences to provide updated knowledge to theservice. The Clinical Lead had attended a NICEconference and a national Health and Safety conferencein the 12 months prior to our inspection. The Matronattended a regional matron’s network as part of Ramsayhealthcare UK. This provided opportunity for sharingdevelopments and learning, with some positiveexamples of patient experience initiatives from here.
• The hospital had gathered feedback from the staffsurvey ‘My Voice’ conducted at the beginning of 2016.Although 75% of staff were satisfied with the seniormanagement team, only 39% of staff believing thecorporate team were visible and 35% believed the teamlistened to and acted on staff views and concerns.Engagement forums were formed with an action plan to
address the issues. As a result, a staff ball was planned,with free invitation offered for all staff to attend. TheChief Executive Officer was planning to attend this eventto meet and greet the Fulwood Hall Hospital team.
• Senior staff we spoke with during the inspectionreported they had good support from Ramsay HealthCare UK leaders also, there was good engagement fromstrategic leaders with staff at the local level. Staff told usthat senior leaders were visible and easily accessible.The hospital Matron was new to Fulwood Hall Hospitalbut not new to Ramsay Health Care UK and there wasgood communication in place. The hospital Matron hadan ‘open door ‘arrangement and was accessible forengagement with nursing staff and other staff on a dayto day basis.
• We observed there was a culture of openness andhonesty at Fulwood Hall Hospital, with a strong focus onpatient centred care. Staff at all levels had a positive andenthusiastic attitude towards the hospital, consistentlyreporting positive experiences of working at FulwoodHall Hospital. One member of staff said they ‘neverwanted to leave this hospital’ and that it was ‘lovelyworking here’; we did not hear any concerns expressedby any of the staff we spoke with during our visit. Staff intheatres and on the ward spoke positively aboutworking for the organisation, making particularreference to teamwork, flexibility and good workingconditions within Ramsay Health Care UK OperationsLtd.
• The hospital monitored performance against theWorkforce Race Equality Standard. This identified thatbetween April 2015 and March 2016, 1.5% of staff (fourindividuals) self-reported they were of black or minorityethnic (BME) backgrounds. None of these staff wereemployed in senior management positions (bands 8 or9 or visible senior management roles); however, thehospital reported that despite advertising internally andexternally applications were not received from peoplewith BME backgrounds.
• The hospital group monitored and reported oncompliance with the Equality Act (2010) in relation toemployed staff. Ramsay Health Care UK Operations Ltddeveloped objectives to address equality issues thathad arisen in the report.
• We received a number of comment cards from staff whoworked at Fulwood Hall Hospital. The commentsincluded “I feel that I was quickly accepted andintegrated into the team. All staff are extremely friendly”
Surgery
Surgery
Good –––
36 Fulwood Hall Hospital Quality Report 01/06/2017

and “As an employee… I have always been treated withdignity and respect.” “As an employee I feel a veryvalued member of the hospital. I work in a safe andhygienic place. I have also had two operations here andhad fantastic care from every department. Dignity wasalways there”
Vision and strategy for this this core service
• We were told about the ‘Ramsay Way’ and how thevalues were lived and breathed by all staff. Staff wereable to give examples of how these values contributedto their roles. Evidence of a recent interview wasprovided where the Ramsay values and knowledge ofthe company was part of the score criteria to supportvalued-based recruitment. Whilst the appraisals werenot directly linked to the values, ‘Understanding ofRamsay’ is a category and looks at the member of staff’sunderstanding and application of the company vision.
• One of the strategic work-streams was around growth ofthe business. However, the capacity of the hospital wasat its limit. We were told that a business case had beensubmitted to obtain funding to increase the physicalspace. The risk to meeting this objective was not on thehospital risk register. We discussed this with the seniormanagement team who acknowledged that this key riskand the actions they are taking would benefit frombeing recorded and managed via the risk register. TheSenior Management Team immediately added fourrelated risks to the register and demonstrated that theyhad been risk scored appropriately.
• The hospital had a regional business strategy for 2016/17 called ‘The Northern Blitz Spirit Strategy’. The viewwas for all Ramsay Health Care UK hospitals in theregion to work to improve the care provided. Peoplewere placed at the heart of the strategy, which focusedon effective engagement with patients, staff, consultantsand stakeholders in order to understand and respond tothe needs of the local health care economy. The strategyaimed to ensure robust and comprehensive governancearrangements were in place, including processes,people and planning, in order to provide effectiveservices to patients. Alongside this, a clinical strategywas developed in July 2016 to align with the five CQCdomains of safe, effective, caring, responsive and wellled.
• Both strategies were supported by the six ‘Ramsay WayValues’, and the ‘Six Cs of Nursing’ (care, compassion,competence, communication, courage and
commitment), and by a hospital business plan for 2016/17. The plan focussed on growth, cost control,governance, a ‘one big thing’, improvement of marketintelligence, operational detail, and ‘our people’. Amongthe key elements identified in the plan wasdevelopment of the physical hospital, to provideadditional clinic capacity within the outpatientdepartment and the continuing review anddevelopment of the diagnostic imaging department.
• Operational staff were aware of the Northern Blitz SpiritStrategy by name, however not all staff seemed surewhat the strategy meant. We saw that informationabout the strategy was included in the staff informationwe observed on site, including display on staff noticeboards and publication in the staff update newsletter.
• Operational staff were aware of the hospital’s ‘RamsayWay’ vision and values and were able tell us aboutthese. The hospital’s values were displayed at thereception desk and on the ward.
Governance, risk management and qualitymeasurement
• Staff were unaware of risk registers or how to get a riskon the risk register. Risk assessments for basic healthand safety requirements were in place in all areas andthere was an assumption that these were risk registers.
• During the inspection, the senior management teamwere initially unable to adequately demonstrate anunderstanding of how to rate a risk appropriately usinglikelihood and severity. A number of risks that we wouldhave expected to see on the risk register over the lasttwelve months were not on the risk register, includingdementia awareness, falls and high bank staffing levelsin surgery.
• However, we could see clear evidence that themanagement team were aware of these risks and hadrobust arrangements in place to manage and reduce therisks. Further, following discussion of this, the SeniorManagement Team immediately added four relatedrisks to the register and demonstrated they had beenrisk scored appropriately.
• The hospital level risk register did not appear to be a livedocument with no new risks added to the register sinceOctober 2015. The hospital had a risk register, which, inAugust 2016, identified 20 open risks, includingfinancial, environmental and clinical risks. The ‘risknames’ were all generic as opposed to being applicableto the hospital. The majority (15) of the open risks were
Surgery
Surgery
Good –––
37 Fulwood Hall Hospital Quality Report 01/06/2017

opened in January 2014. The risk register assessed theinherent, residual and acceptable risk ratings; alsoidentified the accountable executive, responsiblemanager and next review date for each risk.
• However, we saw that the risk descriptions on thehospital system were poor in terms of describing thestatus, cause and consequence of the risk. Additionally,the hospital level risk register did not indicate anycontrol measures already in place, or identify anymeasures needed to mitigate the risks identified. Therisk ratings were inappropriate and in a case, wereviewed with the senior management team actuallyaimed to increase the likelihood of the risk. It wasacknowledged by the senior management team that therisk register was not an accurate record of their key risksand how they were being managed. This was an areathe team were keen to address. During the inspection,the management team had begun work on a revised riskregister based on the existing risks and this revisedapproach demonstrated improvement.
• Following the inspection, actions were taken includingimproved training of senior staff by the generalmanager, a super user to ensure a consistent approach.In addition, the Risk Register was reviewed at allmeetings including Senior Management Team, Heads ofDepartment, Clinical Governance, Health & Safety andMedical Advisory Committee Meetings. At thesemeetings risks were reviewed, additional risks identified,risks were downgraded/upgraded/archived in line withcurrent circumstances. The risk register became a livesystem, which was constantly reviewed and amended.Furthermore, at a Ramsay corporate level, the riskregister was being reviewed by the Group Safety andWellbeing Manager and the policy was under review.
• The hospital had a committee structure, including aclinical governance committee and medical advisorycommittee. Evidence was seen in both committees ofsharing lessons learned from other hospitals in theRamsay group
• The clinical governance committee met bi-monthly.Standing agenda items discussed included review ofincidents, never events and complaints. Reports fromeach of the clinical groups in the hospital regarding newclinical, professional and other guidance and legislation,lessons learnt and any new hospital policies. Clinicalperformance and audit results and patient satisfactionresults.
• Meeting minutes of the clinical governance committeewere detailed, capturing discussions and informationshared at the meetings. However, actions were not giventimescales for completion and appeared to be regularlycarried over, with no assessment of the risk posed bythe actions not being undertaken in a timely way.Attendance at the committee was reasonable and themeeting was chaired by a Consultant Urologist. TheConsultant Chair was positive about the contribution ofclinicians in the clinical governance arrangements andenjoyed the positive impact he felt his unpaid role had.We were given examples of when the Chair had beenrequired to have discussions with his consultantcolleagues to address complaints or incidents. Apositive team culture was described amongst theclinical staff. The Chair of the clinical governancecommittee was also a member of the medical advisorycommittee (MAC), to highlight any clinical governanceissues. We could see this arrangement working via theminutes.
• Medical advisory committee (MAC) meetings were heldquarterly. Standing agenda items included review of thegeneral hospital update, review of the clinicalgovernance report and complaints. The MAC Chair’sreport, surgery cancellation rates, review of any newprocedures or standard operating procedures, andcredentialing of new consultants. As part of this,arrangements were in place by the MAC for checkingand confirming consultant’s indemnity insurance in linewith legislation, the consultant’s qualifications andregistrations. Actions arising from the various meetings,and the responsible person, were clearly recorded in theminutes of the meetings. Outstanding actions werereviewed at each meeting.
• We discussed practising privileges with the Chair of theclinical governance committee and were told that hecouldn’t remember a consultant having their privilegessuspended. The MAC Chair however, was able to give usan example of a suspension and explained in detail theprocess for monitoring the medical staff practisingprivileges and fitness to practice. Neither the MAC northe clinical governance committee discussed the riskregister. The Chair of the MAC had knowledge of thecurrent risks and progress of actions but acknowledgedthey were not on a formal register.
• Senior management meetings were held weekly. Theseincluded review of hospital activity, review of seniormanagement team monthly reports, clinical
Surgery
Surgery
Good –––
38 Fulwood Hall Hospital Quality Report 01/06/2017

performance, business developments, incidents andaudit results. Information from these meetings wasshared by department managers with staff in teammeetings.
• The hospital had a risk assessment policy in place,which was based on the Management of Health andSafety at Work Regulations 1999, in line with therequirements of a number of other regulations. Thepolicy detailed responsibilities for each member of staffand set out the actions to be taken to assess risk, torecord and to score risk assessments
• The departments had detailed risk assessments in placefor the environment, systems, use of equipment andsome clinical procedures. The assessments clearlyidentified the hazards related to each assessment, therisk score and mitigating actions or controls that were inplace. Where further risk factors or mitigating actionswere needed to reduce the risk an action owner andtarget completion date were identified. We reviewed arange of risk assessments across all three departments;they were all within date and appropriate.
• Staff were aware of their responsibilities in reportingrisks and we saw they were proactive in doing this.Managers communicated openly with staff, providingsupport for staff to report incidents within a “no blame”culture.
• There were a wide range of audits carried out in thehospital as part of the yearly audit programme for 2016/17, which included all departments. Although therewere some clinical speciality specific audits, it was notalways possible for us to disaggregate the data for thedepartments in general audits, such as hand hygieneand infection prevention and control.
• The hospital had a facility rules policy. Compliance withthe policy was mandatory for all consultants, staff andaccredited healthcare professionals. The rules assistedin the selection and granting of admitting rights and / orpractising privileges to a health care professional. Therules required an appropriate person to examine thecredentials of various categories of healthcareprofessionals; define and authorise a scope of clinicalpractice appropriate to the professional’s competence,performance and the needs of the facility in which theyworked; undertake ongoing assessment of thecompetence and performance of the professional; and,if necessary, re-define the authorised scope of clinicalpractice.
Public and staff engagement
• The hospital gathered feedback from patients in anumber of ways. The ‘We value your opinion’ leaflet(which also provided details of how to complain);through the hospital’s patient satisfaction survey results;and from the NHS Friends and Family test (which askspatients to rate how likely they would be to recommendthe service to their friends and family).
• Fulwood Hall Hospital held a patient participationgroup’s hospital tour on 5 May 2016. This provided thepublic with information about the hospital, including atour of the facilities and afternoon tea. These had beenwell attended and positively received, with plans forsimilar events to be held in the future.
• The hospital had engaged with a range of communitygroups, inviting them in to the hospital to supportservice improvement. This had included meetings withthe Alzheimer’s society in the development of itsdementia friendly policy and carer’s leaflet. It had alsoworked with Galloway’s Society for the Blind indeveloping its assistance dogs policy. Other communityengagement had involved Preston Muslim society andlocal Healthwatch organisations.
• The hospital took part in the Ramsay Health Care UKOperations Ltd customer service excellence awardsscheme. Two staff in the physiotherapy department hadreceived awards, and a staff member in the outpatientdepartment had two nominations. One staff membertold us the award scheme meant that staff ‘feelappreciated’.
• In January and February 2016, a staff survey ‘My Voice’had been undertaken. The results were analysed againstother Ramsay locations and published in a report. Themost positive, highest scoring answers for Fulwood Hallhospital included: working for the best interests of thepatient (98%), understanding what was expected oftheir role (96%), staff understanding their impact ondelivering patient care (95%), knowing how to deal withsafety issues (91%) and recommending the hospital tofriends and family (88%).
• The report provided the top five responses that requiredaction and the management team responded with thecreation of an action group. The responses for actionwere; I feel my pay is fair (30%), I am satisfied with mythe physical environment (57%), The corporateleadership team listen and act of views and concerns(35%), I receive recognition (54%) and I have the
Surgery
Surgery
Good –––
39 Fulwood Hall Hospital Quality Report 01/06/2017

resources to do my job (62%). We saw evidence inmeeting minutes of proposals from the engagementgroup, and an action plan with targets, progress ratingsand responsibilities assigned to individuals. Both thelocal management team and the corporate leadersresponded to the survey and improvements were inprogress.
• As a result of the staff engagement forums, Once amonth, the hospital delivered ‘month-end madness’ forstaff. This provided recognition for their work and took adifferent form each month; for example, the provision ofice-cream, a meal in the restaurant, or toffee apples orEaster eggs for staff. Senior staff told us that staff werereceptive to this, and there were good turnouts to otherevents organised by the hospital.
• The hospital had a staff development funding policy inplace, the ‘Ramsay Scholarship Fund’. This enabled staffto apply for financial support through the RamsayHealth Care UK Scholarship for courses costing morethan £500. Staff were permitted up to three days’ paidleave per year for study or examinations relating tocourses undertaken through the fund.
• The hospital had a disclosure of information(whistle-blower) policy. This set out the procedures to
follow with internal disclosures and with disclosures toregulatory bodies. Staff were aware of where to findhospital policies if needed on the intranet, and in thelibrary in the staff canteen.
Innovation, improvement and sustainability
• The hospital was proactive in developing practice andimproving patient experience, with a number ofinitiatives in place. During 2016, the hospital hadengaged with external participants and the NationalInstitute for Health and Care Excellence (NICE) inreviewing the quality standards for falls and the clinicalguidance on urinary incontinence in women.
• The hospital was introducing a clinical practice reviewgroup. The group, which was to consist ofmultidisciplinary staff across the hospital, would reviewprevious incidents and reports against current policiesand guidelines. This would enable identification ofareas that needed to change and would promotelearning and information sharing.
• The hospital had developed a new ‘Missing PatientProcedure’ after a patient with dementia was found tobe missing from the ward for a short period. Actionsfollowing this were shared with other RamsayHealthcare UK Operations Ltd sites, as well asdevelopment of a dementia training package for staff.
Surgery
Surgery
Good –––
40 Fulwood Hall Hospital Quality Report 01/06/2017

Safe Good –––
Effective Not sufficient evidence to rate –––
Caring Good –––
Responsive Good –––
Well-led Good –––
Are outpatients and diagnostic imagingservices safe?
Good –––
We rated safe as good.
Incidents
• The outpatient and diagnostic imaging department had46 clinical incidents and five non clinical incidentsbetween 1 July 2015 and 30 June 2016. This was similarto the rate of incidents for other independent healthproviders that we hold data for. There were no neverevents reported in the outpatient and diagnosticimaging department.
• All staff we spoke with were aware of the incidentreporting system and understood their responsibility toreport incidents.
• Due to the nature of outpatient consultations andlimited treatment, there were no specific safety goals setby the department. However, we were assured by theOutpatient Manager that safety of patients wasparamount for staff.
• There were no patient deaths related to care andtreatment received in the outpatient department. Assuch, the department was not involved in mortality ormorbidity reviews.
• We saw evidence that incidents were shared with theMedical Advisory Committee and the ClinicalGovernance meetings. Lessons learnt were shared withstaff in staff meetings, and through the lessons learntfive circle briefing.
Duty of candour
• Senior staff were aware of the duty of candourrequirements. Operational staff were less aware of thelegislative requirements of the duty of candour;however, staff we spoke with were aware of theprinciples of the duty of being open and honest.
• We saw evidence of the appropriate application of theduty of candour relating to an incident within thediagnostic imaging department. Because of a patientlabel error, a patient received a minimal but avoidableX-ray radiation exposure. The incident was appropriatelyreported to the regulatory organisations, investigatedand the root cause of the error identified. The referringconsultant spoke directly with the patient, apologisedand reassured them that any risk associated with theX-ray was minimal. The hospital subsequently wrote tothe patient providing an explanation of what happenedand an apology.
• Learning from this incident was shared with theconsultant and the nurse directly involved and resultedin the creation of an information leaflet for consultantsto reduce the likelihood of a similar incident occurring inthe future. It was also discussed at the diagnosticimaging team meeting.
Cleanliness, infection control and hygiene
• All departments were visibly tidy and clean with handgel sanitisers at the entrance of each area. Sanitisers,hand washing facilities and sterile wipes were availablein each consultation and treatment rooms. Personalprotection apron dispensers were available throughoutthe departments. We saw staff following the ‘arms barebelow the elbow’ requirement of the policy.
• A cleaning schedule and log was in place in thediagnostic imaging department. Staff cleaned clinical
Outpatientsanddiagnosticimaging
Outpatients and diagnosticimaging
Good –––
41 Fulwood Hall Hospital Quality Report 01/06/2017

equipment after each patient. Non-clinical areas werecleaned by the housekeeping team. Green stickers wereused to identify equipment that had been cleaned andwas ready for use.
• The hospital had a screening policy for patients whohad MRSA (methicillin-resistant staphylococcus aureus).All patients due to receive treatment in the outpatient’sdepartment were screened for MRSA. Patients wereswabbed and any MRSA positive screening results werenotified to the patient’s GP. Following treatment forMRSA, patients were rescreened before outpatienttreatment for their condition was started. This meanttreatment may be delayed if the patient remainedpositive for MRSA.
• Within the diagnostic imaging department, patientswith MRSA or other suspected communicable infectionswere allocated appointments at the end of the clinicfollowing which the area was cleaned. This reduced thelikelihood of transmission of infection.
• The outpatient department were compliant with theDepartment of Health’s technical memorandum ondecontamination of flexible scopes. The remainder ofequipment used was disposable. The diagnosticimaging department had a decontamination procedurein place for the use of ultrasound probes used intrans-vaginal scanning.
Environment and equipment
• The design, maintenance and use of the facilities andequipment within the department kept people whoused the hospital services safe. Risk assessments,including control of substances hazardous to health(COSHH) risk assessments, were in place for equipmentand chemicals in use within the departments. Wereviewed a number of these which were detailed, up todate and included mitigation and control factors whereappropriate.
• We checked a range of physical equipment in theoutpatient clinic treatments rooms. All portableelectrical appliances, except one weighing scale, hadbeen tested appropriately and labelled with the datewhen testing would be next required. The hospital’smaintenance team held a log of tested equipment. Wehighlighted the expired weighing scale to staff forchecking against the maintenance log. All disposable
equipment (such as dressings or swabs) we inspectedon the treatment trollies in each consultation room andthe storeroom were within the manufacturers’ expirydates.
• A resuscitation trolley was located in the outpatientdepartment. Daily checks were carried out for theautomatic defibrillator and suction machines. Thecontents of the trolley were checked once a week, afterwhich the trolley was secured with a new tamper tag.We checked the equipment in the trolley, which, exceptfor one suction tube, were within the manufacturers’expiry dates. Staff immediately replaced the dateexpired suction tube; we confirmed it had been done.
• In the diagnostic imaging department clear, illuminated,‘radiation in use’ warning signs were in place by doorsleading into any area where radiation equipment wasused. This reduced the likelihood of staff or members ofthe public entering the area while equipment was inuse.
• Detailed risk assessments were in place for each piece ofradiation equipment within the department. Theseincluded assessment of risks to staff and patients, stafftraining in the use of each piece of equipment, signageto ensure mitigation of risks (for example door to beclosed) and action plans for maintenance and repair.
• Processes were in place to ensure specialised personalprotective equipment (PPE) was available and used bystaff within the diagnostic imaging team. All staffmembers within the diagnostic imaging departmentwere issued with a personal radiation dose monitorbadge. Each badge was sent off every three months tobe checked centrally by the radiation protectionadvisors, and the individual staff member’s doseexposure was recorded. Staff were working within thesafe limits.
• Visual checks of personal protective equipment such aslead aprons were carried out regularly and results werelogged. The personal protective equipment had beenreplaced in April 2016; therefore, due to the risk ofunnecessary additional radiation exposure, X-ray checksto determine if there were any breaks in the protectivematerial were carried out only if there were visible signsof damage. Personal protective equipment checks wereincluded in the departments audit against the IonisingRadiation Medical Exposure Regulations 2000 [IR(ME)R]and IRR99 regulations. The audit results in May 2016indicated 93% compliance by the department, with oneof the areas of weakness relating to X-ray checks of
Outpatientsanddiagnosticimaging
Outpatients and diagnosticimaging
Good –––
42 Fulwood Hall Hospital Quality Report 01/06/2017

personal protective equipment. This was due toconcerns about radiation exposure to staff in carryingout these checks; as a result, the department put inplace a staff rota to carry out the checks in order toreduce the risk of radiation exposure.
• A contract was in place between Ramsay Health Care UKand a medical equipment and services provider for themaintenance of diagnostic imaging equipment. Thismeant equipment was repaired in a timely wayminimising any impact on the department.
Medicines
• The management of medicines in the outpatient anddiagnostic imaging departments kept people who usedthe services safe. The hospital had a medicinesmanagement policy; staff were aware of the policy andhow they could access it.
• Medicines in the outpatient department were stored in alocked cupboard. The room’s temperature was recordedand logged using a maximum/minimum thermometer.Medicines which needed to be stored at a lowertemperature so they were effective were stored in alocked fridge. Fridge temperatures were checked andlogged daily using a maximum/minimum thermometer;the temperatures recorded were consistently within theappropriate range of two to eight degrees Celsius. Wereviewed a sample of six different medications heldwhich were all within the manufacturers’ expiry datesand appropriately labelled if opened.
• Staff told us of one occasion when, due to a fault withthe air conditioning, the room temperature increased.Staff appropriately took advice from a pharmacist onwhether or not the medications held in the roomneeded to be removed; in this event no further actionwas needed.
• Medicines in the diagnostic imaging department werestored in a locked cupboard within the X-ray room.Medicines stored by the diagnostic imaging departmentincluded contrast media (an intravenous liquid used toenhance the internal images of the body) andanaphylaxis kit. We checked a range of medicines withinthe cupboard. All medications were within themanufacturers’ expiry dates.
• The department’s FP10 prescription pads were storedsecurely under lock and key. The department achievedfull compliance with this in the twice-yearly audit.
Records
• There were systems and processes in place in thedepartments to ensure the management of people’srecords were accurate, complete, legible, up-to-dateand stored securely. We reviewed thirteen sets of patientcare records within the outpatient department. All wereof good quality. Referrals, relevant history, patientconsent, plans of care, decisions and, whereappropriate, discharge summaries were all clearlyrecorded.
• The hospital reported only 1% of records were notavailable for clinic appointments. In this situation, therewas a process in place to print any electronic lettersheld and placed into a temporary record for theconsultant to use in clinic. Temporary records weresubsequently destroyed. There were no reported cliniccancellations within the department due to recordsbeing unavailable.
• The diagnostic imaging department held records withinthe picture archiving and communication system(PACS). Referring consultants also had access to thissystem which meant that copies of the images and thediagnostic imaging reports were directly available toconsultants. The department had a procedure in placefor requesting access to patient images held by otherhealthcare organisations through the PACS imageexchange portal system if needed.
• At the time of the inspection, the department was in theprocess of integrating a new digital PACS system.Although this improved response times for accessingand reviewing new images, staff were concerned aboutdelays caused in the retrieval and accessibility of olderimages that were stored on the old system. Staff told usthis was a known national problem with the PACSsystem supplier at its data centre, which meant therewere delays in the robotic retrieval of image data fromthe data tapes. This meant there was a risk that olderimages would not be available in a timely manner forreview by medical staff, if needed. This was a known riskthat was included in the department’s risk register.
• We reviewed four sets of patient records in thephysiotherapy department. The records were of goodquality, were legible, signed and dated. A clear patienthistory and care plan was recorded, which includedassessment of previous treatment and patient pain.
Safeguarding
• Safeguarding flowcharts were displayed throughout theoutpatient, diagnostic imaging, and physiotherapy
Outpatientsanddiagnosticimaging
Outpatients and diagnosticimaging
Good –––
43 Fulwood Hall Hospital Quality Report 01/06/2017

departments, including in staff offices and in clinicrooms. The flowcharts provided easy to follow guidancefor staff on the appropriate response to safeguarding orFGM concerns, including contact details for safeguardingleads that were able to provide advice.
• All staff in the outpatients and diagnostic imagingdepartments had completed safeguarding vulnerableadults and safeguarding children training which wasincluded in the mandatory training programme. Nursingstaff completed safeguarding training to level two, andthe Resident Medical Officer (RMO) and departmentleads completed level three safeguarding for childrenand young people. Non-clinical staff who had contactwith children and young people were offered training tolevel two.
Mandatory training
• Staff undertook mandatory training twelve months afterprevious completion. At the time of our inspection, 98%of all permanent hospital staff had either completedtheir training or were scheduled onto future trainingdates within the rolling twelve-month period. For staff inthe outpatient and diagnostic imaging department; 80%of outpatient staff, 66% of physiotherapy staff, and 57%of diagnostic imaging staff had completed mandatorytraining. Dates had been scheduled for the remainingstaff to complete their training within the rollingschedule. It was therefore expected that thedepartments would achieve full compliance.
• At the time of our inspection, the mandatory trainingcompletion rate for bank staff in the outpatient,physiotherapy and diagnostic imaging departments was87%.However, not all bank staff were used on a regularbasis. There was a process in place to schedulemandatory training when these bank staff were nextemployed; this also included updating staff on newpolicies and procedures.
Assessing and responding to patient risk
• The outpatient department had a resuscitation trolleyavailable for use in emergencies. Pocketcardiopulmonary resuscitation masks (used to safelydeliver rescue breaths during a cardiac arrest) wereavailable throughout the hospital.
• Although the hospital did not treat patients under theage of 16, all staff were trained in paediatric basic life
support. The registered children’s nurse was trained toEuropean paediatric advanced life support (EPALS) andthe Resident Medical Officer (RMO) was trained toadvanced life support level.
• Due to the nature of the work undertaken in theoutpatient department, staff were less likely toencounter deteriorating patients. However, theRegistered Medical Officer could be contacted by atwo-way radio to attend any deteriorating patient in thedepartments. A sepsis pack and flowchart had beenintroduced to the department to assist staff in theidentification of possible sepsis.
• The hospital had common policies and procedures inplace that set out details of diagnostic imaging staffresponsibilities shared with staff of the mobile MRI andCT scanning provider. These included the MRI safetypolicy, medical emergencies in scanner policy andmedical emergency/arrest on mobile scanner policy.
• The hospital had two radiation protection supervisors;the diagnostic imaging manager and the seniorradiographer. The supervisors were supported byRamsay Health Care UK radiation protection advisers.The advisers were available on call to provide advice.
• Two radiation protection adviser audits were carried outin 2016. The audit in February 2016 concluded that thedepartment was ‘partially compliant [with currentregulations] with a number of minor improvementsnecessary’. The audit made 12 recommendations to becompleted by April 2016; none of theserecommendations were repeated in the subsequentaudit in October 2016.
• The October 2016 audit indicated that the departmenthad improved and was ‘nearly fully compliant [withcurrent regulations] with only few minor improvementsnecessary’. The audit made five recommendations; all ofwhich the department was on course to complete by theend of 2016. These included ensuring non-RamsayHealth Care UK physiotherapists referring for imagingwere appropriately authorised to do so; the setting of adiagnostic reference level for mobile X-ray facet jointinjection procedures; a minor change in practice toreduce the dosage levels for barium swallowexaminations; a check of fluoroscopy dose rates everytwo months; and encouragement of staff uptake ofonline training in radiation protection.
Outpatientsanddiagnosticimaging
Outpatients and diagnosticimaging
Good –––
44 Fulwood Hall Hospital Quality Report 01/06/2017

• The Ionising Radiation Regulations 1999 (IRR99) requiresemployers to keep employee exposure to ionisingradiations as low as reasonably practicable and toensure that exposures must not exceed specified doselimits.
• The hospital held a copy of ‘local rules’ that were inplace to meet the IRR99 regulations. These weredisplayed on the wall of the X-ray room. The rules weresupported by the hospital’s incidents greater thanintended exposure of patients caused by proceduralerror policy. These set out the responsibility of staff toreport exposure incidents to the on-site radiationprotection supervisor, who in turn logged the incidenton the hospital’s incident reporting system. The incidentwas then reported directly to the group’s radiationprotection advisers for dose calculation and wherenecessary to the medical physics expert. The rules andpolicy also set out the dose thresholds for reportingradiation exposure incidents to the CQC and/or theHealth and Safety Executive.
• In line with the IR(ME)R regulations, and the hospital’spolicy, a training record was kept for all non-medicalreferrers’ scope of practice and entitlement to refer forimaging, which included referrals from the otherco-located healthcare provider.
• All permanent staff had signed to confirm they hadreceived up to date training and knowledge in line withthe regulations. Although some bank radiographer staffhad yet to sign, this was because the individualsinvolved had not since been on duty. The service leadtold us these bank staff would be asked to sign whenthey were next on duty.
• The hospital had an examination of females of childbearing age policy, which included a pathway flowchartfor staff to follow. Warning signs asking patients to tellstaff if they may be pregnant were clearly displayed ondoors into radiation controlled areas.
• A clinical radiology contrast agent and medicines fordiagnostic imaging policy was in place. This included atreatment pathway that was based on the Royal Collegeof Radiologists standards on the use of contrast agents.
• A pre and post checklist for radiological interventionswas used in the hospital. The pre intervention checkincluded confirmation by the patient of any knownallergies or use of anticoagulant medication, thepotential to be pregnant, or previous steroidalinjections. For imaging staff, the pre intervention check
included items such as checking ID, consent for theprocedure, relevant medical history and confirmation ofthe marked site and compliance with IR(ME)Rrequirements.
• The pre and post intervention checklist wassupplemented by the use of the World HealthOrganisation Surgical (WHO) Safety Checklist forRadiological Interventions. There was no information inthe hospital’s audit programme to indicate ifcompliance with the WHO checklist was audited.
• A two-way radio system was provided to staff of theother healthcare provider who operated the mobile CT/MRI unit. The radios were tested twice a day when theunit was on site. This aided communication betweenstaff in the mobile unit and staff in the hospitaldepartment in the event of a patient deteriorating.
• A process was in place within the diagnostic imagingdepartment for urgent review of images for unexpectedfindings or significant pathology. End of day reports,which highlighted any abnormal findings, wereproduced by staff in the mobile MRI/CT unit. Theseflagged potential issues that required urgent review andreporting by the on-duty radiologist. A check off systemwas used to record when these urgent requests hadbeen completed.
• The diagnostic imaging department provided a sevenday on-call mobile plain X-ray imaging service for urgentimages of patients on the inpatient ward. Theserequests were subject to clear referral and safety criteriadue to the risk of radiation exposure within the wardenvironment.
Nursing staffing
• Staffing levels were planned and reviewed using RamsayHealth Care UK’s national electronic rosteringmanagement system, which embedded indicators forsafety and effectiveness. This enabled heads ofdepartments to manage rotas, shift allocations, annualleave and sick absences, skill mix and staff requirementsincluding senior cover. The system provided indicatorsof safety and effectiveness and allowed heads ofdepartments to manage shift allocation, annual leaveand sickness absence.
• Staffing levels were reviewed on a daily basis to enableflexibility between the needs of patients and anyunforeseen issues that arose. As of 1 April 2016, theoutpatient department had 4.1 full-time equivalent
Outpatientsanddiagnosticimaging
Outpatients and diagnosticimaging
Good –––
45 Fulwood Hall Hospital Quality Report 01/06/2017

registered nursing staff and one full time equivalenthealth care assistant. No permanent nursing orhealthcare assistant staff left in the 24 months between1 July 2014 and 30 June 2016.
• There was no nursing staff sickness in the outpatientdepartment between 1 July 2015 and 30June 2016. Foreight of out twelve months in the same period there wasno sickness for healthcare assistants. In the remainingfour months, healthcare assistant sickness levels variedbetween 2.7% and 100%, however, this high variancelikely reflect the small number of health care assistantstaff in the department. There were no unfilled shiftsreported in the three months between April and June2016.
• Agency staff were not used in the outpatientdepartment. The use of bank nursing staff (as apercentage of all staff in the department) variedbetween 21% and 35% in each of the twelve monthsbetween 1 July 2015 and 30 June 2016. The use of bankhealthcare assistant staff varied between 35% and 91%for the same period.
• However, this usage of bank staff is likely to reflect theoverall small numbers of permanent staff within thedepartment and an increasing demand on the hospital’soutpatient services.
• New staff members in the outpatient department wereassigned a ‘buddy’ to provide support during theinduction phase and met regularly with their managerto review performance progress against the inductionprogramme.
Allied healthcare professionals staffing
• The diagnostic imaging department had threepermanent radiographers and four administration staff.The diagnostic imaging manager and some admin staffwere relatively new in post having been recruited withinthe last year as part of a department improvement plan.
• A bank of ten radiography staff were available to coverunfilled shifts, mainly in evenings and at the weekend.Bank staff were experienced within the department andhad received up-to-date training, risk assessments andwere within their documented scope of practice.
• The physiotherapy department had ten permanentphysiotherapy staff. A bank of eight staff includingqualified physiotherapists and physiotherapy assistantssupported the team. Staff worked flexibly to meet theneeds of the department.
Medical staffing
• In the period 1 July 2015 to 30 June 2016, the hospitalhad 94 doctors and dentists who were directlyemployed or were practicing under rules of privilege formore than six months. None had had practicingprivileges suspended in the twelve months prior toAugust 2016.
• Staff in the outpatient, physiotherapy and diagnosticimaging departments were able to request the RMO toattend any patient who became ill in the department.
Emergency awareness and training
• Staff had received emergency fire training, and told usthat the procedures for this were tested throughsimulation scenarios. Staff were aware of theirresponsibilities during a major incident. Contact detailsfor staff to be used in an emergency were also held inanother local Ramsay Health Care UK hospital. Thismeant that details were easily accessible in the eventthat staff at the hospital could not access the records.
Are outpatients and diagnostic imagingservices effective?
Not sufficient evidence to rate –––
We inspected but did not rate effective.
Evidence-based care and treatment
• Care and treatment was delivered in the department inline with legislation, standards and evidence basedguidance, including from professional bodies and theNational Institute for Health and Care Excellence (NICE).
• Patient clinical pathways were standardised. Pathwaydocuments were used for each procedure, whichincluded a specific outpatient procedure care pathway.These took into account guidance and establishedpractice and included appropriate pre and postprocedure checks and follow-up information.
• Diagnostic imaging procedures were carried out in linewith established practices from the Royal College ofRadiologists, the Ionising Radiation Medical ExposureRegulations [IR(ME)R] 2000 and the Ionising RadiationsRegulations 1999.
• Physiotherapy treatment was provided in line withestablished practice and guidance from the Chartered
Outpatientsanddiagnosticimaging
Outpatients and diagnosticimaging
Good –––
46 Fulwood Hall Hospital Quality Report 01/06/2017

Society of Physiotherapy. Physiotherapy care andtreatment was audited against the society’s QualityAssurance Standards audit tool, with the departmentachieving 95% compliance in the safe service audit and97% in learning and development. Physiotherapyequipment was risk assessed in line with the Provisionand Use of Work Equipment Regulations 1998.
• All physiotherapy staff were registered with the HealthCare Professionals Council (HCPC) and with theChartered Society of Physiotherapists.
Pain relief
• Pain relief medication was not held in the outpatientdepartment. Any pain relief medication would beprescribed to patients by consultants.
• The department had introduced a cross-site painmanagement clinic, mainly for musculoskeletal pain.The clinic, which ran every two weeks, was supported bythe physiotherapy department and the consultant wasable to refer directly into physiotherapy. Patients werescreened using the Keele STarT Back tool (a simpleprognostic questionnaire to identify modifiable risk forback pain disability) and those that requiredpsychological input were referred to a local NHS acutehospital trust. As part of this, the department alsointroduced a hospital anxiety and depression tool.
• The physiotherapy department offered acupuncturetherapy and shockwave therapy (mechanical pressurepulse treatment for tendon-related pain) for managingpain.
Patient outcomes
• Due to the nature of the services offered, patient clinicaloutcome data was not routinely collected by thehospital for the outpatient and diagnostic imagingdepartment. The physiotherapy department monitoredpatient progress using a number of tools, including theKeele STarT Back tool, the Oxford Hip Score, the StGeorge’s Respiratory Questionnaire, a visual analoguepain scale and patient pathway discharge assessmenttool.
• Although data from the discharge assessment tool wascollated, it was not available to us in a format thatenabled us to usefully analyse it. The remaining datafrom the other tools was used to understand individualpatient progress, but was not separately collated.
• The patient satisfaction survey showed that 100% ofthose who responded experienced improvement in theircondition.
Competent staff
• Staff had the skills, knowledge and experience to delivereffective care and treatment. All new staff, includingbank staff, were required to undertake an inductiontraining programme, in line with the hospital’s inductionpolicy. The induction programme varied in lengthdependant on the staff member’s role andcompetencies during which time the staff member metwith their line manager at regular intervals to reviewtheir performance. One staff member we spoke with hadbeen in post for six weeks and spoke positively aboutthe induction process which the staff member felt wassupportive. Another staff member told us newcolleagues were assigned to a buddy during theinduction phase.
• A competency framework was in place for existing staffand staff were expected to meet this. We viewed threenursing and three physiotherapy staff training files all ofwhich included competency records, training andaccreditation certificates.
• The hospital held records for all staff that hadappropriate training to administer radiation.Competency records were also kept. These includedcompetency to use each piece of equipment within thediagnostic imaging treatment rooms and the movementof equipment within the rooms. We reviewed theIR(ME)R procedures file within the diagnostic imagingdepartment. The documentation held was up to dateand included evidence that all staff had signed toconfirm they had received training and had undertakenappropriate reading of the relevant procedures.Similarly, staff signed to confirm they had read thediagnostic imaging clinical policies.
• Staff within the diagnostic imaging department wereregistered with the Healthcare Professionals Council(HCPC) and Chartered Society of Physiotherapists. Thephysiotherapy manager was encouraging all staff tobecome accredited with the Acupuncture Association ofChartered Physiotherapists. The manager also delivereda yearly acupuncture course, which was open to all staffacross the norther Ramsay Health Care UK hospitalsites.
• One staff member in the diagnostic imaging departmenttold us there was a ‘very positive engaged approach to
Outpatientsanddiagnosticimaging
Outpatients and diagnosticimaging
Good –––
47 Fulwood Hall Hospital Quality Report 01/06/2017

[continual personal development which] is activelyencouraged...’ and that professional radiology journalswere brought into the department for staff to read'. Staffwere also given regular opportunities to review previousdiagnostic imaging reports and apply these to theimages, which assisted their learning.
• Staff appraisals were carried out yearly betweenJanuary and December. By 1 November 2016, six out ofnine (66%) outpatient staff had received an appraisal;two staff had not yet had an appraisal and theremaining staff member was receiving separate reviewsfollowing a departmental transfer. By the same date, allphysiotherapy staff had received an appraisal.
• Staff we spoke with in all departments confirmed theyhad received appraisals this year. However, one staffmember told us their previous appraisal had beenapproximately two years earlier.
• Due to the small size of the departments, regular formalone-to-one meetings were not scheduled with staffunless there were performance management concerns.
Multidisciplinary working
• Physiotherapy staff were encouraged to attendappropriate outpatient consultant appointments.
• The physiotherapy team leader worked closely with theorthopaedic and spinal consultants in the relevantclinics and with one consultant on pain management.One physiotherapist was a specialist in gynaecologicalproblems, while another specialised in problems withhands. The team had a good working relationship withthe diagnostic imaging department.
• The diagnostic imaging department were involved inmultidisciplinary meetings with outpatient consultantsto review imaging and reports. As a result, imagingreports were able to be refined, re-issued or relevantaddendums added. The department also reviewed thehospital’s external reporting agency’s findings on the tenper cent double reporting sample of CT/MRI scan. Anyconcerns arising from this were fed directly to themedical advisory committee to consider if any changesin practice needed to be addressed.
Seven-day services
• The outpatient department offered a six day service,Monday to Friday between 8am and 9pm, and between8am and 2pm on a Saturday. The department did notoffer clinics on bank holidays.
• The physiotherapy department offered a six dayoutpatients service, Monday to Saturday between 8amand 5pm. Pilates classes were run each Tuesday andThursday. Physiotherapy staff provided treatment toinpatients on bank holidays but not to outpatients.
• Diagnostic imaging was carried out Monday to Saturday.An on-call facility was in place for urgent X-ray imagingrequests at night and the weekends.
Access to information
• Patient records were securely transported from themedical records office to the department each morningand afternoon. Although the hospital was aiming tointroduce an electronic patient record system for fullpatient records, this was not yet implemented.
• Diagnostic images and records were electronic, whichmeant they were accessible to clinical andphysiotherapy staff when needed. However, a knownissue with the diagnostic image data supplier meantthat older, historical images took longer to retrieve.Although this meant there was a risk that historicalimages may not be available for review in a timelymanner, there was no indication of any incidences whenthis had impacted overall patient care.
• Physiotherapy staff told us of one incident where apatient’s appointment was rescheduled as records werenot available. This had occurred because of a lateappointment booking where the patient’s treatmentwas transferred from another Ramsay Health Care UKhospital in the region.
• Discharge letters were sent to each patient’s GP within24 hours following completion of treatment.
Consent, Mental Capacity Act and Deprivation ofLiberty Safeguards
• There was a two-stage process to obtaining writtenconsent for outpatient procedure care pathways. Stageone was carried out by the consultant in the outpatientclinic and included discussion of the benefits and risksof treatment. This meant that patients were able tomake informed decisions about their treatment. Thesecond stage of consent was carried out on the day oftreatment and included confirmation that the risks oftreatment had been discussed with the patient. Patientswere given a copy of their signed consent.
• Verbal consent was obtained from patients undergoingphysiotherapy. However, if there was any concern about
Outpatientsanddiagnosticimaging
Outpatients and diagnosticimaging
Good –––
48 Fulwood Hall Hospital Quality Report 01/06/2017
a patient’s capacity to consent, staff rescheduled theappointment and requested assessment of the patient.Written consent was obtained from patients undergoingshockwave or acupuncture therapy.
• Flowcharts on mental capacity was displayed within thedepartment. Staff were aware of the policies andprocesses, but told us the majority of patients theytreated had capacity to consent to their care. Staff wereempowered to be able to stop a consultation ortreatment if they had any concerns about a patient’sability to consent to treatment. The patient would thenbe invited back to be assessed with family members inattendance. This was highlighted in an ophthalmicoutpatient appointment, where the nurse had concernsabout the patient’s capacity to consent to treatment.The nurse subsequently carried out a mental capacityassessment checklist with the patient and their carer.
• A separate consent form (consent form four) was usedfor patients who did not have capacity to consent totheir own treatment. This consent form includedassessment of the patient’s capacity to consent;assessment of the patient’s best interests and reasonswhy treatment could not be delayed until the patientrecovers capacity; and, involvement of the patient’scarer, relatives or attorney in the discussions.
Are outpatients and diagnostic imagingservices caring?
Good –––
We rated caring as good.
Compassionate care
• People who used the outpatient, physiotherapy anddiagnostic imaging departments were treated withkindness, dignity, respect and compassion when theyreceived treatment at the hospital. One patient in thephysiotherapy department told us ‘the staff are brilliant.They are caring, very good, explaineverything….absolutely wonderful’.
• The hospital recognised the important role that familyand carers played in the care and treatment of patientswho were living with dementia or learning disabilities.Relatives and carers were given a ‘Working Together’leaflet and they were able to stay overnight in thehospital if necessary. They were given an ‘I am a carer’
card to present at the restaurant for a meal. The hospitalalso used the Alzheimer’s Society’s ‘This is me’ guide,which assisted staff to understand the personalpreferences and needs of patients living with dementiain order to provide compassionate care.
• The outpatient department patient satisfaction survey,between January 2016 and September 2016, indicatedan average of 99% of respondents reported they weretreated with respect and dignity. Each outpatientconsultation room was private, which meant thatpatients’ privacy and dignity was maintained duringoutpatient appointments.
• The diagnostic imaging patient satisfaction surveyshowed that an average of 98% of respondents said thatthe team were friendly and reassuring during theexamination. Although there was a potential risk topatient privacy and dignity due to the layout of thediagnostic imaging changing area, this was not reflectedin the survey; 99% of respondents considered they hadprivacy whilst changing.
• The main reception area was at the entrance to thehospital and co-located with the main waiting patientwaiting area. Staff were sensitive in conversations withpatients, and were mainly involved with checkingpatients in for their procedures. We did not observe anyconfidential information being discussed at thereception desk.
• A chaperone service was available to patients, whichwas supported by the hospital’s chaperone policy. Signsto remind patients of the chaperone service were clearlydisplayed in all consultation and treatment rooms. Allnursing and healthcare assistant staff in the departmentwere used as chaperones; however, only registerednurses acted as chaperones for gynaecology clinics.Patient records were updated to indicate that achaperone was needed, or if there was a patientpreference to have a non-female chaperone.
• The nature of the treatments provided within theoutpatient, physiotherapy and diagnostic imagingdepartments meant that patients were, generally, notkept waiting within the department. However, whereclinics ran late, staff offered drinks to patients. Staff wereable to give food and drink for patients who werediabetic. A drinks vending machine was available in thereception waiting room and a snack vending machinewas located near to the department.
Outpatientsanddiagnosticimaging
Outpatients and diagnosticimaging
Good –––
49 Fulwood Hall Hospital Quality Report 01/06/2017

Understanding and involvement of patients and thoseclose to them
• Staff in the outpatient, physiotherapy and diagnosticimaging departments communicated with people abouttheir care and treatment in a way they couldunderstand.
• The patient satisfaction survey between January andSeptember 2016 showed an average of 97% ofrespondents said they were involved in decisions abouttheir care in the outpatient department and were givenenough time to discuss their health problems with adoctor.
• An average of 98% people indicated that doctors hadexplained the reasons for their treatment in a way theycould understand. Ninety-two per cent of people saidnurses had explained the treatment in a way they couldunderstand; and 100% indicated staff explained testresults in a way they could understand. Further, anaverage of 97% of respondents said they couldunderstand the answers given by nurses to theirquestions. This was supported by the patients we spokewith, who told us staff had explained appropriate andrelevant information and had provided contact numbersfor any questions the patient may have.
• The physiotherapy patient satisfaction survey indicatedthat an average of 94% of respondents were satisfiedwith the advice on self-care and exercises provided tothem during their treatment. However, 81% ofrespondents considered the written information theyhad been given was clear, easy to understand andhelped them to make decisions about their treatment.The department was, in conjunction with the outpatientdepartment, working to produce a combined patientinformation leaflets which include details such asphysiotherapy exercises to be undertaken. This hasbeen successfully trialled for an information leafletrelated to arthroscopy treatment.
• The patient satisfaction survey also showed that 100%of respondents were satisfied that physiotherapy staffhad taking into account any special needs such ashearing, sight and language. Ninety-four per cent ofrespondents felt they understood the role of thephysiotherapist treating them and 90% said they feltthey were listened to when asking questions.
• One physiotherapy patient told us they had attendedthe department for four separate appointments, duringwhich staff explained everything to the patient. The
patient said they were given contact numbers for thedepartment if they had any questions. The patient said‘staff were brilliant’ and that the care provided was‘absolutely wonderful’.
• In the diagnostic imaging department, an average of98% of respondents said that information given to themabout the examination was useful. However, an averageof 81% said they were told how to get results of theirexamination. Following a related complaint, thedepartment recognised there had been a risk ofcommunication breakdown with patients aboutwhether or not a follow-up appointment would beneeded to be given the results. The departmentintroduced a simple pro-forma slip to be given topatients after their examination. This providedinformation about whether or not a follow-upappointment was needed for results and prompted thepatient to make this with the bookings team.
• One nursing staff member told us they started workearly to be able to accommodate the needs of onepatient who required an earlier appointment slot due tothe needs of the patient’s business.
Emotional support
• Individual consultation rooms in the outpatientdepartment meant that privacy was maintained forpatients.
• The diagnostic imaging department informed staff inthe outpatient department if there would be bad newsfor a patient. As such, staff tried to scheduleappointments for patient receiving bad news towardsthe end of the clinic day. This enabled extra time for thepatient to ask questions or to reflect on their news. Theoutpatient department’s manager told us that despitethe physical limitations of the department, staff wouldtry to find an available room for a patient and theirrelatives if they wished after their consultation.
• There were sufficient numbers of nursing andhealthcare assistant staff on duty to be able to provideadditional emotional support to patients, if needed,without affecting delivery of the service.
• The outpatient department were able to offer tours ofthe relevant areas of the hospital to patients living withlearning disabilities prior to their treatment. This helpedto reduce any anxiety the patient may have.
Outpatientsanddiagnosticimaging
Outpatients and diagnosticimaging
Good –––
50 Fulwood Hall Hospital Quality Report 01/06/2017
Are outpatients and diagnostic imagingservices responsive?
Good –––
We rated responsive as good.
Service planning and delivery to meet the needs oflocal people
• The hospital was, except for staff offices, a single storeybuilding. The main entrance was by the car park. Thereception area was bright, clean and tidy. The open planwaiting area for patients was in the reception area.Toilet facilities, which included disabled access, werelocated off the main reception area and a range ofpatient information leaflets were available. There wasno separate waiting area for outpatients, who remainedin reception until called.
• Late clinics provided flexibility for patients andadditional clinics were scheduled where possible tomeet demand. Saturday morning clinics were offered inthe outpatient department and physiotherapydepartment added two additional evening classes and aSaturday morning clinic to help reduce waiting times.The physiotherapy department also supportedorthopaedic inpatients.
• There was clear signage throughout the hospital toguide patients to the appropriate department.
• Public transport to the hospital was adequate and freecar parking was available on-site. However, at peaktimes there were not enough parking spaces, whichmeant that patients and visitors parked on the road. Carparking facilities were being considered as part of thehospital development plans, including furtherencouragement for staff to park away from the site.
Access and flow
• There were 30,927 outpatient, physiotherapy anddiagnostic imaging attendances to the hospital betweenJuly 2015 and June 2016 of which 80% were NHSfunded. The remaining patients were self-paying orinsured.
• NHS referrals into the departments were from GPs,consultants and through the NHS choose and bookappointment system.
• Between July 2015 and June 2016, an average of 99.5%of NHS non-admitted patients started outpatienttreatment within 18weeks of referral against the targetof 95%. In the same period, 99% of patients who had notyet completed their treatment had commencedtreatment within 18 weeks of referral. This was betterthan the hospital’s target of 92%.
• Between July 2015 and June 2016, no NHS patientswaited longer than the six-week target for a CT scan. ForMRI scans one patient (out of 80, 1.3%) in July 2015 andthree patients (out of 121; 2.5%) in March 2016 waitedlonger than six weeks. For non-obstetric ultrasoundscans, one patient (out of 131; 0.8%) in July 2015 andone patient (out of 60; 1.7%) in January 2016 waitedlonger than six weeks.
• All available consultation and treatment rooms werefully utilised and with increased demand, physicalcapacity within the department was an issue recognisedby hospital management. Future development plans forthe hospital included increasing the physical capacity ofthe department.
• The physical limitations of the department meant therewas limited ability to absorb delays in clinics that wererunning late. The outpatient manager discussed anylate running clinics with the relevant consultant and aprocess was in place to take these forward to the seniormanagement team if necessary. Waiting patients wereinformed by staff if clinics were running late, and whenappropriate, additional refreshments were provided.The hospital did not keep a record of cliniccancellations; however, consultant staff were expectedto provide six weeks’ notice of any periods of leave andclinic cancellations. The outpatient manager told usthat, in the event of a cancellation, a new appointmentwas made with the patient before they left thedepartment.
• The outpatient and diagnostic imaging department’srostered staff to take account of overrunning clinics ortheatre lists. Physiotherapy staff managed their ownclinics, which meant that clinics generally ran to time.Although the physiotherapy department aimed for afour week wait for treatment for new NHS patients at thetime of our visit, staff were booking new patients forJanuary 2017 (an approximate nine week wait). Thephysiotherapy department had recently implemented
Outpatientsanddiagnosticimaging
Outpatients and diagnosticimaging
Good –––
51 Fulwood Hall Hospital Quality Report 01/06/2017

two additional evening classes and an extra Saturdaymorning clinic to address the waiting time delay;however, it was too early to identify the impact on thewaiting list.
• The hospital did not collect data relating to clinic delays.However, the physiotherapy department told us aprocess was in place for the discharge of patients, at thephysiotherapist’s discretion, following two consecutivemissed appointments.
• The diagnostic imaging department reported plain X-rayfilms internally. At the time of our visit, there was anapproximate two week delay in reporting of theseimages because of the half-term holidays. Thediagnostic imaging manager expected this to beresolved once staff returned from leave.
Meeting people’s individual needs
• Entrances to the hospital were accessible towheelchairs, with automatically opening doors. Alldepartments were located on the ground floor of thehospital. Accessible toilets for patients living with adisability were located behind the reception area andwithin the departments. Refreshments, including water,tea, and coffee were available from a vending machinein the waiting area at a small cost to NHS patients; otherfunded patients were given a token for refreshments.
• In the diagnostic imaging department a small changingand waiting area was situated next to the X-ray room.The changing area consisted of two small cubicles,separated by only a curtain, with a chair and a smalllockable cupboard in each for patient property. Patientswho had changed then needed to walk past others inthe waiting area in order to access the X-ray room. Thismeant there was a risk that patient privacy and dignitycould be compromised.
• Staff were aware this was an issue and told us it hadbeen raised for inclusion in the future developmentplans in the hospital. In the meantime, staff told us theykept patients in their own clothes as far as possible toreduce the number of instances where patients neededto change. Staff also told us they would not ask twopatients to use the changing area at the same time andthey would escort patients from the changing area tothe X-ray room to help ensure patient dignity wasmaintained.
• The physiotherapy department included one individualtreatment room and an open plan area with threetreatment bays separated by privacy curtains and asmall rehabilitation area including gym equipment.
• The physiotherapy department had a small waitingarea, which included a toilet for patients. However, asthere was no separate door between the waiting areaand the treatment area, there was a risk that patientswaiting for treatment could overhear conversationswithin the treatment area particularly at busy timeswhen noise levels in the department increased. Staffwere also aware this was an issue and again it had beenraised for inclusion in the future development plans forthe physiotherapy department.
• Translation services were available for patients whosefirst language was not English. Staff were also able toaccess British Sign Language interpreters if needed.
• Patient information leaflets were readily available in thewaiting area and in all the departments. Although themajority of leaflets displayed in the departments were inEnglish, staff were able to download leaflets in otherlanguages if needed. Easy read leaflets were availablefor patients who were living with learning disabilities.
• The patient leaflets clearly explained the patient’scondition and treatment and were provided duringconsultations. This meant patients were able toconsider their options at home before making anydecisions to proceed.
• A signature guide was used to assist patients with poorvision when signing documents including consentforms.
• The hospital reported they did not see large numbers ofpatients with learning disabilities or people living withdementia. However, staff also received training onpeople living with dementia and had attended a talkfrom the Alzheimer’s Society as part of the hospital’sequality and diversity Commissioning for Quality andInnovation (CQUIN) programme. Information aboutdementia was shared in hospital newsletters. One of thephysiotherapists had been trained as a dementiafriendly champion. Reception staff alerted thedepartments when a patient, known to have dementia,arrived.
Learning from complaints and concerns
• The hospital recognised there had been an increase inthe number of complaints about the diagnostic imagingdepartment because of staffing and responsiveness
Outpatientsanddiagnosticimaging
Outpatients and diagnosticimaging
Good –––
52 Fulwood Hall Hospital Quality Report 01/06/2017
issues that the department had experienced in the lattermonths of 2015. However, the Matron supported thediagnostic imaging team throughout theimplementation of the department’s improvement plan.The number of complaints received about thedepartment reduced following the recruitment of thenew departmental manager
• In line with the hospital’s complaints policy, the hospitalacknowledged complaints relating to the departmentwithin two working days enclosing a copy of thecomplaints procedure information leaflet. We reviewedtwo complaint files within the diagnostic imagingdepartment. Both demonstrated robust complaintinvestigation and included appropriate responseswithin the complaint policy’s 20 working day timescale.One of the complaints resulted in the introduction of afollow-up slip to advise patients on whether or not theyrequired a follow-up appointment.
• The diagnostic imaging department had, as a result of apatient complaint, introduced a communication slipwhich ensured that patients were aware if they neededto be seen again in a follow-up clinic to obtain results.
• Staff in the physiotherapy department told us that, as aresult of a patient complaint, they had redesigned thearthroscopy patient leaflet. This meant that informationfrom both the outpatient and the physiotherapydepartment was included in the leaflet and preventedthe patient receiving conflicting information. Thedepartment was aiming to roll this out for otherconditions and procedures.
Are outpatients and diagnostic imagingservices well-led?
Good –––
We rated well-led as good.
Leadership and culture of service
• The hospital manager was supported by the matron andthe physiotherapy, outpatient and diagnostic imagingdepartmental managers. Although the physiotherapyand outpatient managers had been in post for sometime, the diagnostic imaging manager had beenrecruited earlier in 2016.
• Staff in all departments spoke positively about thesenior management team, the Matron, and their line
managers. Staff said that the senior management teamwere visible within the hospital but there was lessvisibility or recognition or corporate staff. However, thiswas not unanimous; two staff members expressedreservations about the leadership styles of twomanagers.
• One staff member told us ‘since matron has been onboard we have been a lot more supported’. The samestaff member said that senior management were ‘veryapproachable’ with an ‘open door policy’. This wasreflected by a member of reception staff who told us thehospital manager was ‘approachable’. Another staffmember who had worked on the bank before becomingpermanent, spoke very positively about the departmentmanager, and told us they felt ‘more valued andinvolved in the department than ever before’. Othercomments made by staff included: ‘second family forme’, ‘feel supported’, ‘lovely place to work’, and ‘I loveinteracting with patients’. However, staff also reflectedconcerns about the physical capacity of the hospital inlight of increasing demand for the hospital’s services.
• The Matron held monthly one-to-one meetings with thedepartmental managers and attended departmentalteam meetings bi-monthly.
Vision and strategy for this this core service
• The diagnostic imaging department faced a number ofperformance and governance issues in 2015, which hadbeen recognised by the hospital. A development andimprovement action plan was implemented in January2016. The action plan, driven by the matron and the newdiagnostic imaging manager, covered areas such acompliance with IR(ME)R and radiation protectionregulations, medicines management, cleanliness andinfection prevention and control, training, medicalemergency response, reporting and documentation,and patient communication. The majority of actionshad been completed by 30 July 2016. The twooutstanding actions related to collation of bank stafftraining records and the replacement of chairs in theX-ray room and waiting area.
• Although there was no separate strategy for theoutpatient department, staff were aware of ‘TheNorthern Blitz’ strategy and the visual representation ofthe plan was displayed in the departmental offices.
Governance, risk management and qualitymeasurement
Outpatientsanddiagnosticimaging
Outpatients and diagnosticimaging
Good –––
53 Fulwood Hall Hospital Quality Report 01/06/2017
• Although there was a governance framework in thehospital, which supported the delivery of good qualitycare in the department, the hospital’s risk register didnot include any open outpatient, physiotherapy ordiagnostic imaging departmental specific risks on theregister, nor did it indicate any mitigation or controlfactors for risks that had been included.
• Further there were no separate risk registers held in theindividual departments. When asked about this, staffreferred us to the schedule of risk assessments.Although the list of risk assessments wascomprehensive for the physiotherapy and diagnosticimaging departments, we could not be assured thatrisks affecting the day to day running of each of thedepartments, or the services they offered, had beenidentified; for example capacity and staffing issues.
• As part of the wider corporate organisation, the hospitalhad a clear governance and committee structure inplace including clinical governance, medical advisory,health and safety, head of department, bloodtransfusion and infection prevention and controlcommittees. The governance structure was supportedby detailed policies and procedures.
• Staff were clear about their roles, how they fitted withinthe hospital structure, and who held the relevant lines ofreporting responsibility.
• Team meetings were held in each of the departments,which shared learning and updates to policies andprocedures.
• The diagnostic imaging manager recognised that auditshad not always been completed in the department in2015 due to performance issues within the department.However, since starting in post, the manager hadre-implemented the audit programme. The results ofaudits were discussed at the various committees..
Public and staff engagement
• NHS Friends and Family test scores between July 2015and June 2016 demonstrated an average of 98% of atotal of 1858 NHS funded respondents were likely orextremely likely to recommend the hospital’s outpatientdepartment. One patient commented in the survey ‘Ihave used Fulwood Hall on a number of occasions inthe past and have always been extremely satisfied withits courtesies and treatments that I have received. This iswhy I have chosen the hospital for this treatment andwhy I have already recommended family and friends touse Fulwood Hall’.
• However, the Friends and Family test response rates forthe outpatient department were very low at an averageof 4.3% for the same period and did not meet thehospital’s target of 10% response rate.
• The hospital took part in the Ramsay Health Care UKcustomer service excellence awards scheme. Two staffin the physiotherapy department had received awardsand a staff member in the outpatient department hadtwo nominations. One staff member told us the awardscheme meant that staff ‘feel appreciated’.
Innovation, improvement and sustainability
• The hospital had drawn up development plans toincrease physical capacity throughout the hospital. Theplans included increasing the capacity in the outpatientand diagnostic imaging departments, improvement ofequipment and facilities and consideration of re-sitingthe physiotherapy department.
• The physiotherapy manager was considering thedevelopment of outreach clinics in local gyms andleisure centres. It was also hoped to move towards fullelectronic patient records for the physiotherapydepartment.
Outpatientsanddiagnosticimaging
Outpatients and diagnosticimaging
Good –––
54 Fulwood Hall Hospital Quality Report 01/06/2017
Outstanding practice
• The hospital had a robust system for awareness,training and monitoring safeguarding adults at risk ofabuse or neglect, and safeguarding children andyoung persons. Policies and procedures werecomprehensive. There were four safeguarding leadsand training was delivered to all staff. Additionalsafeguarding sessions were delivered monthly. Staffgave us examples of when safeguarding issues hadbeen identified and led to changes within the hospital.
• All staff worked hard to ensure that patients weretreated with kindness, dignity and respect. This wasreflected in both monthly Friends and Family audits
and in the comments and reflections of patients at thetime of the inspection. Many examples were given ofpatient experiences and changes to process andprocedures as a response to feedback.
• The hospital had excellent referral to treatment timesfor both outpatient and diagnostic services andsurgical treatments. Between July 2015 and June 2016,an average of 99.5% of non-admitted patients startedoutpatient treatment within 18 weeks of referralagainst the target of 95%. In the same period, 99% ofpatients who had not yet completed their treatmenthad commenced treatment within 18 weeks of referral.This exceeded the hospital’s target of 92%.
Areas for improvement
Action the provider SHOULD take to improve
• The provider should ensure that all housekeepingrecords of weekly water outlet checks are accurate, upto date and maintained.
• The provider should consider the most appropriateenvironment is available for conducting pre- operativeassessment appointments, in order to protect patientdignity and confidentiality.
• Staff should ensure records trolleys are kept lockedwhen not in use.
• The hospital should consider how it can ensurecompletion of mandatory training by bank staff intheatre and the ward in a timely manner.
• The hospital should consider how it can measureclinical effectiveness of patient care and treatment inthe outpatients department.
• The hospital should consider how it can preventrecurring deficiencies in the consent process identifiedwithin the consent audit.
• The hospital should consider how it can ensure thetimely reporting of plain film X-rays during highperiods of leave, such as school holidays.
• The hospital should consider how it could track andanalyse data relating to the late running of clinics,clinic cancellations and patients who did not attendappointments within the departments.
• The hospital should consider how it can address thelow percentage of staff recruited from a black andminority ethnic background.
• The hospital should consider how it can improve theidentification of risks to the operation of thedepartments and services offered and the logging ofthese on departmental and hospital risk registers.
• The provider should ensure that risks to patients areidentified, assessed and monitored consistently, andthat action plans are updated and contain enoughdetail to enable staff to reduce those risks effectively.
Outstandingpracticeandareasforimprovement
Outstanding practice and areasfor improvement
55 Fulwood Hall Hospital Quality Report 01/06/2017