fisiopatologia tiroides
TRANSCRIPT
FISIOPATOLOGIA TIROIDEA
II Curso de Fisiopatología Clínica 2009
FRANCO EDGARD MIO PALACIOSMEDICO ENDOCRINOLOGO
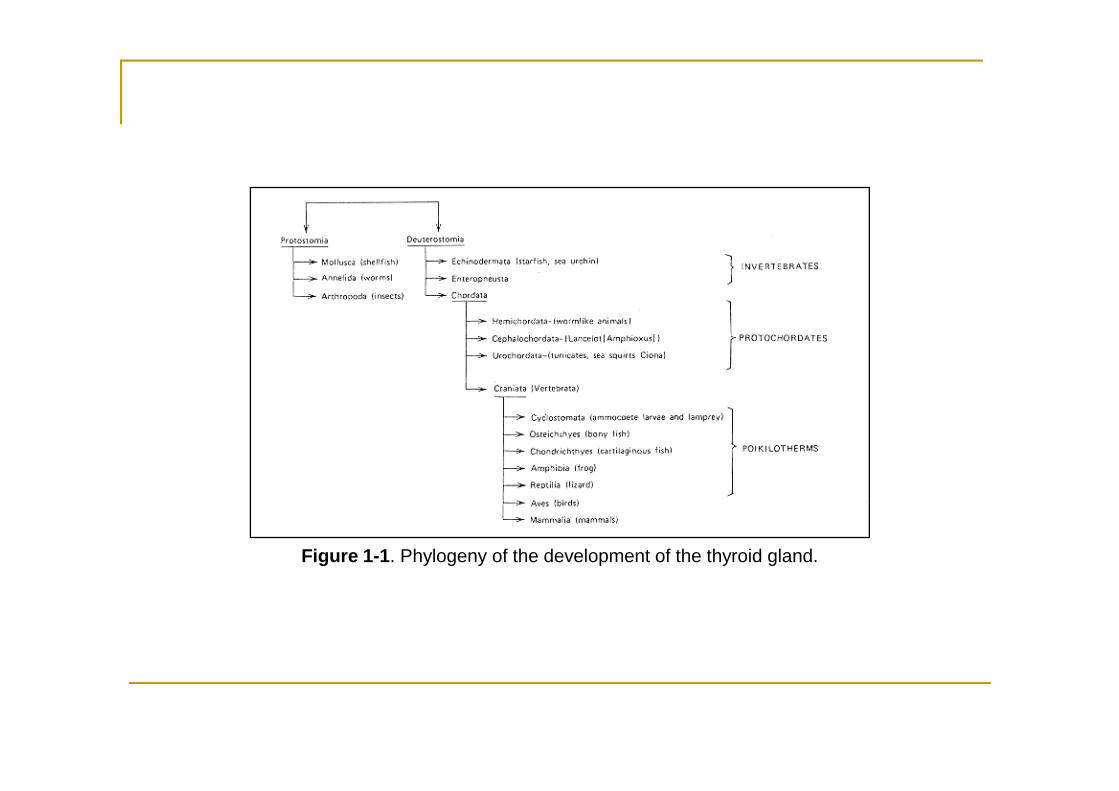
Figure 1-1. Phylogeny of the development of the thyroid gland.
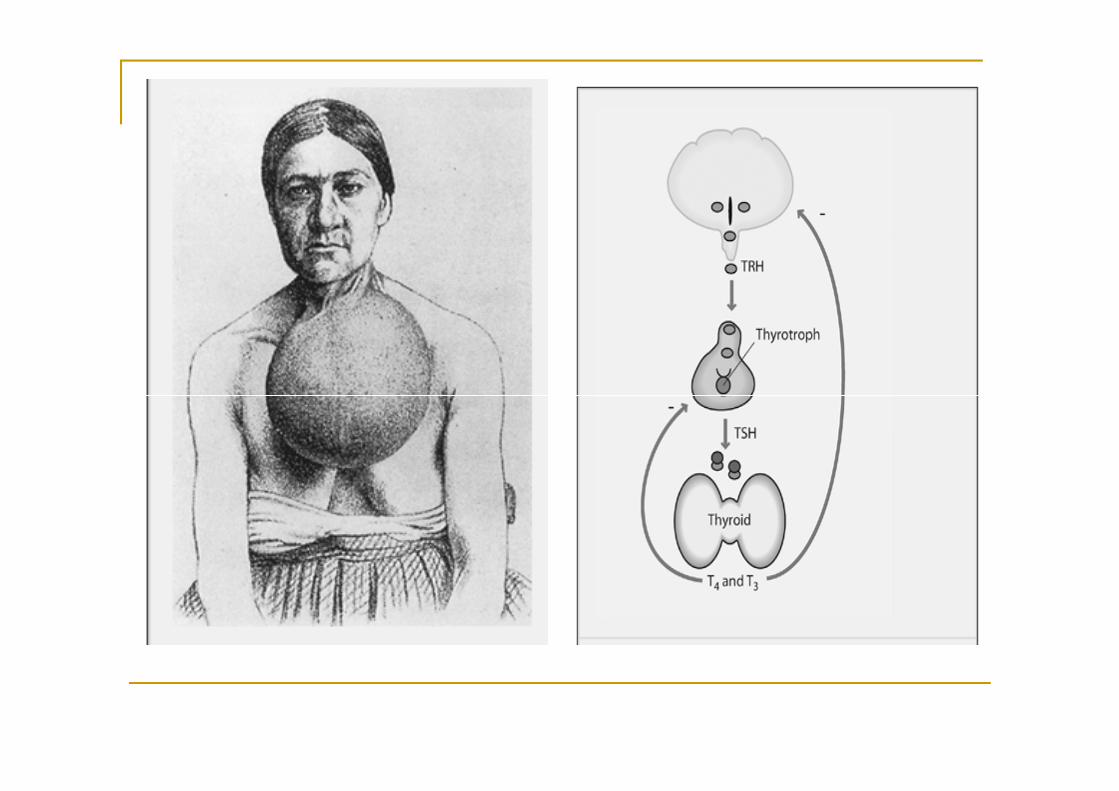
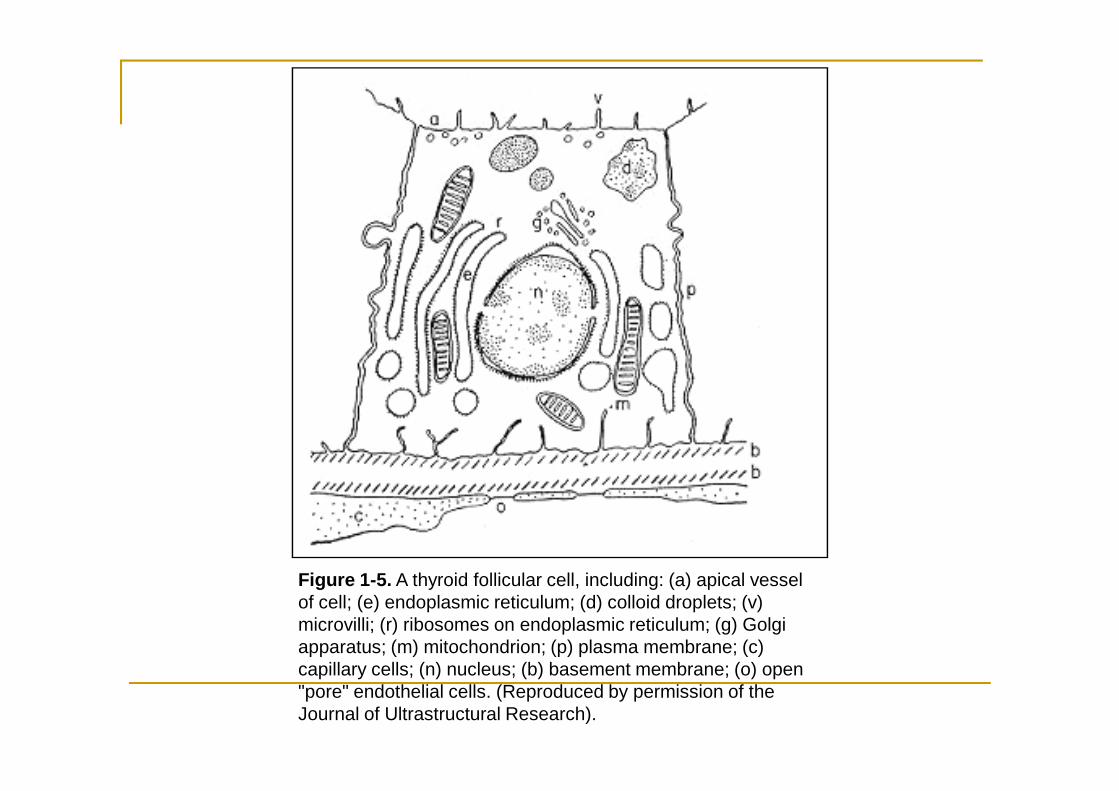
Figure 1-5. A thyroid follicular cell, including: (a) apical vessel of cell; (e) endoplasmic reticulum; (d) colloid droplets; (v) microvilli; (r) ribosomes on endoplasmic reticulum; (g) Golgi apparatus; (m) mitochondrion; (p) plasma membrane; (c) capillary cells; (n) nucleus; (b) basement membrane; (o) open "pore" endothelial cells. (Reproduced by permission of the Journal of Ultrastructural Research).
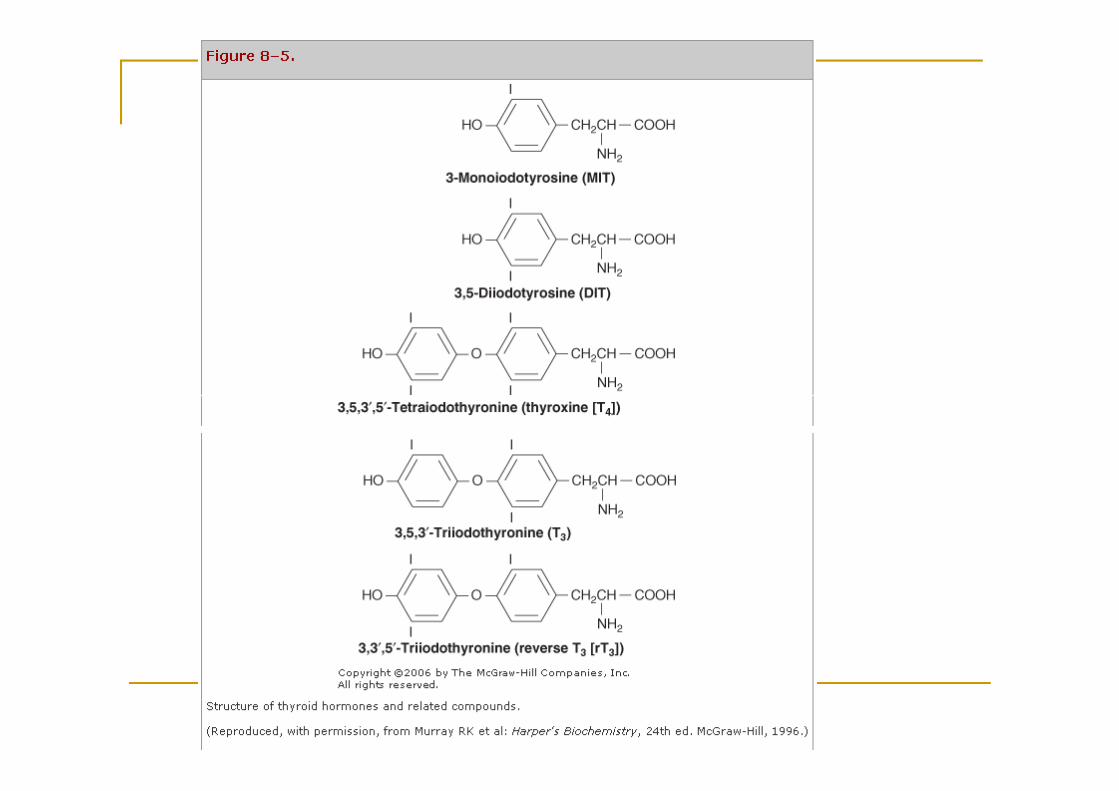
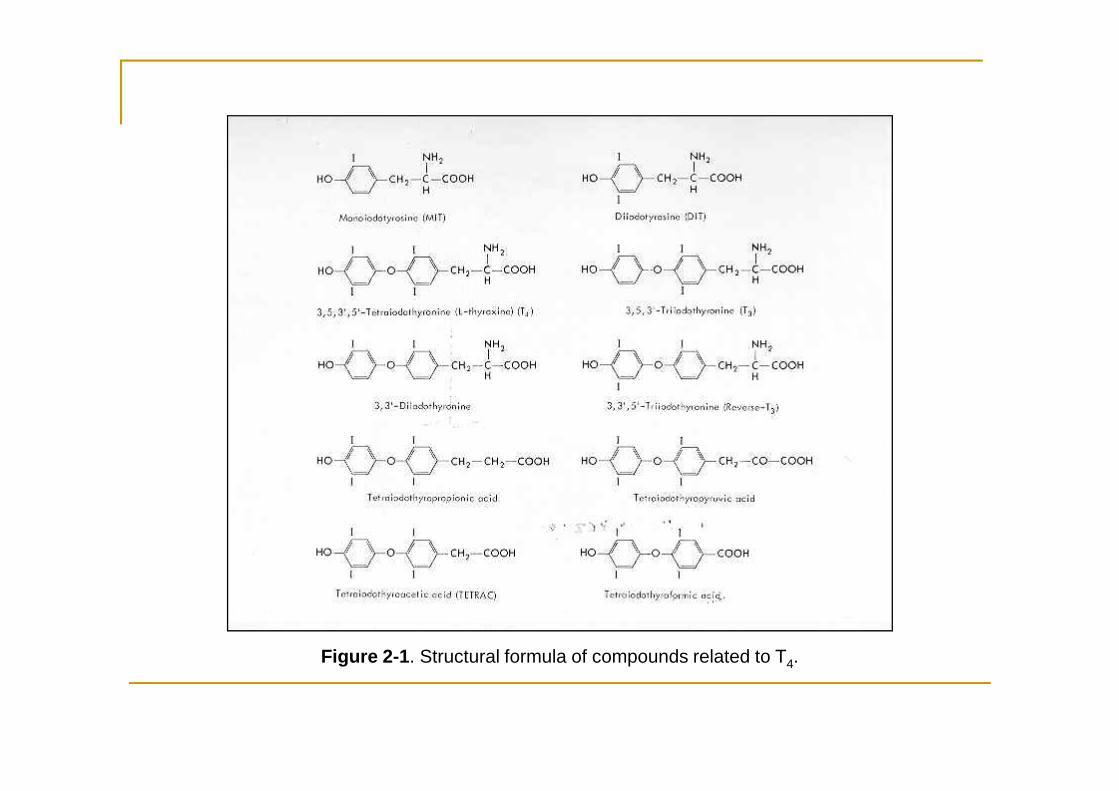
Figure 2-1. Structural formula of compounds related to T4.
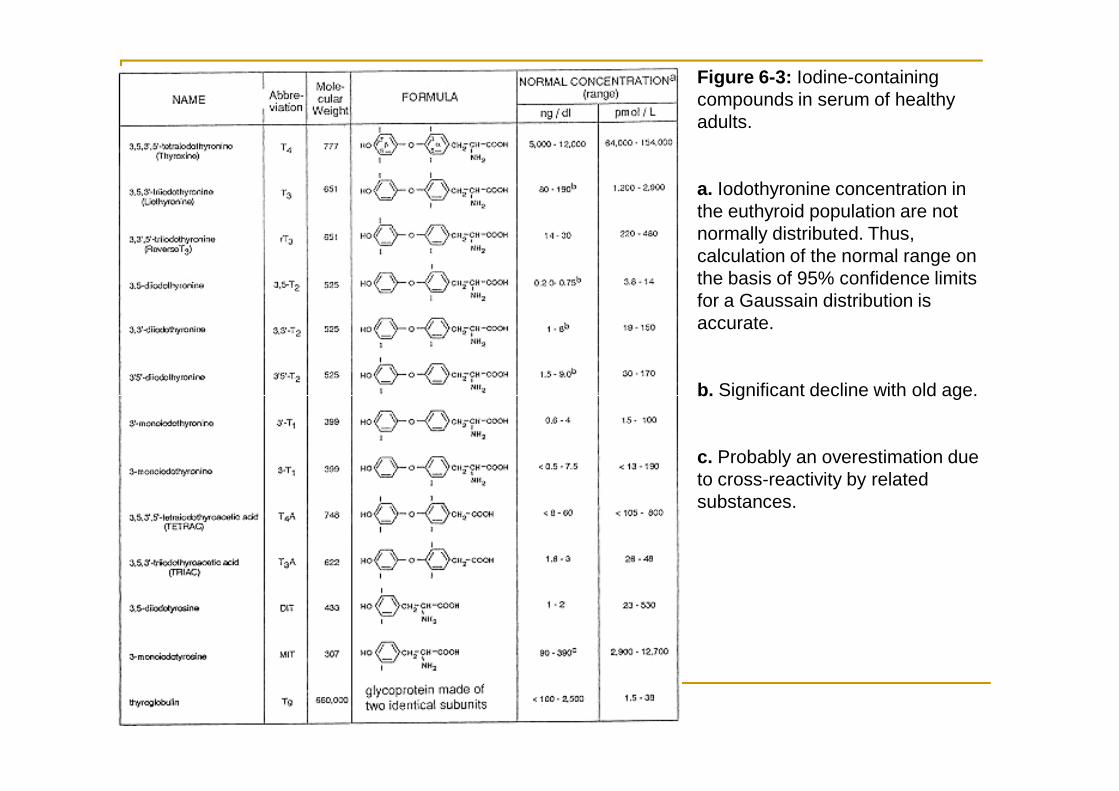
Figure 6-3: Iodine-containing compounds in serum of healthy adults.
a. Iodothyronine concentration in the euthyroid population are not normally distributed. Thus, calculation of the normal range on the basis of 95% confidence limits for a Gaussain distribution is accurate.
b. Significant decline with old age.b. Significant decline with old age.
c. Probably an overestimation due to cross-reactivity by related substances.
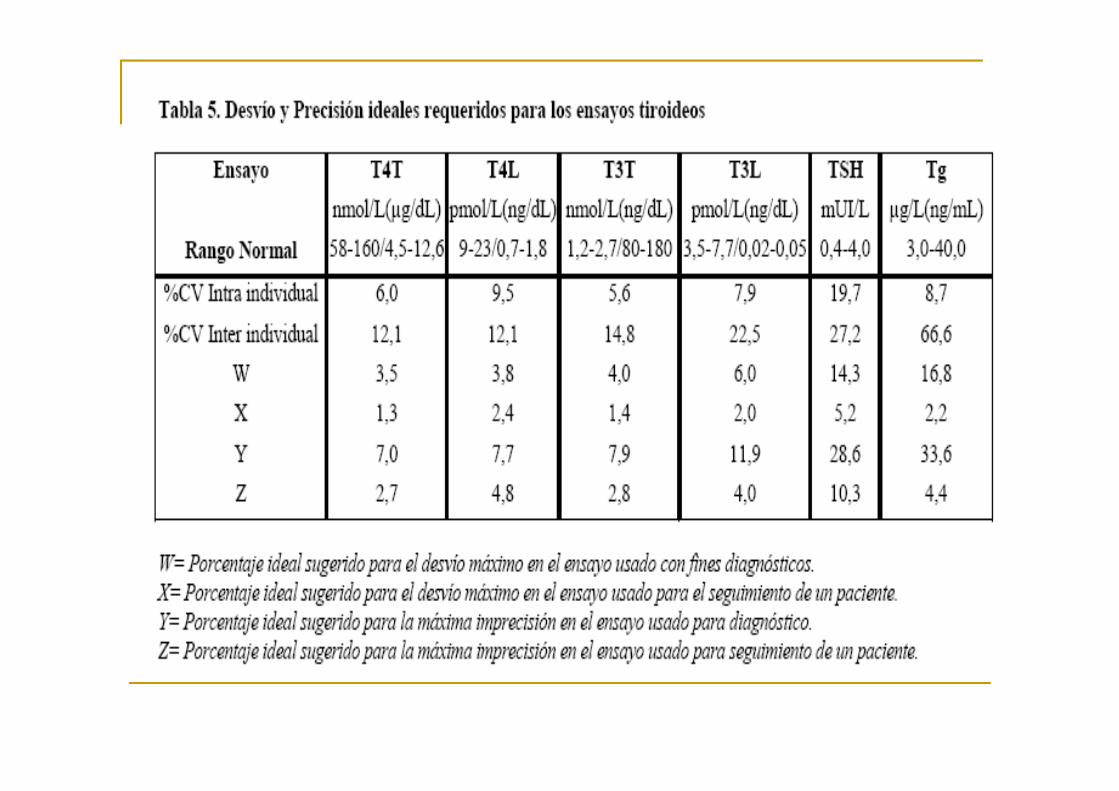
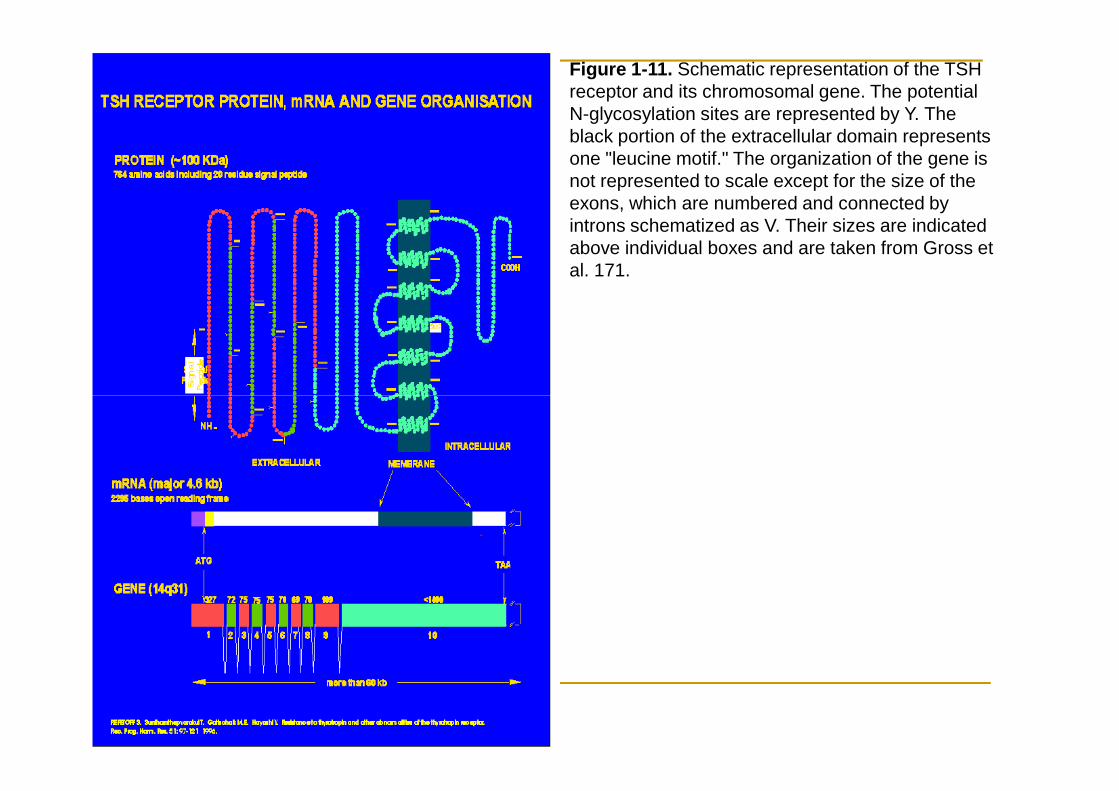
Figure 1-11. Schematic representation of the TSH receptor and its chromosomal gene. The potential N-glycosylation sites are represented by Y. The black portion of the extracellular domain represents one "leucine motif." The organization of the gene is not represented to scale except for the size of the exons, which are numbered and connected by introns schematized as V. Their sizes are indicated above individual boxes and are taken from Gross et al. 171.
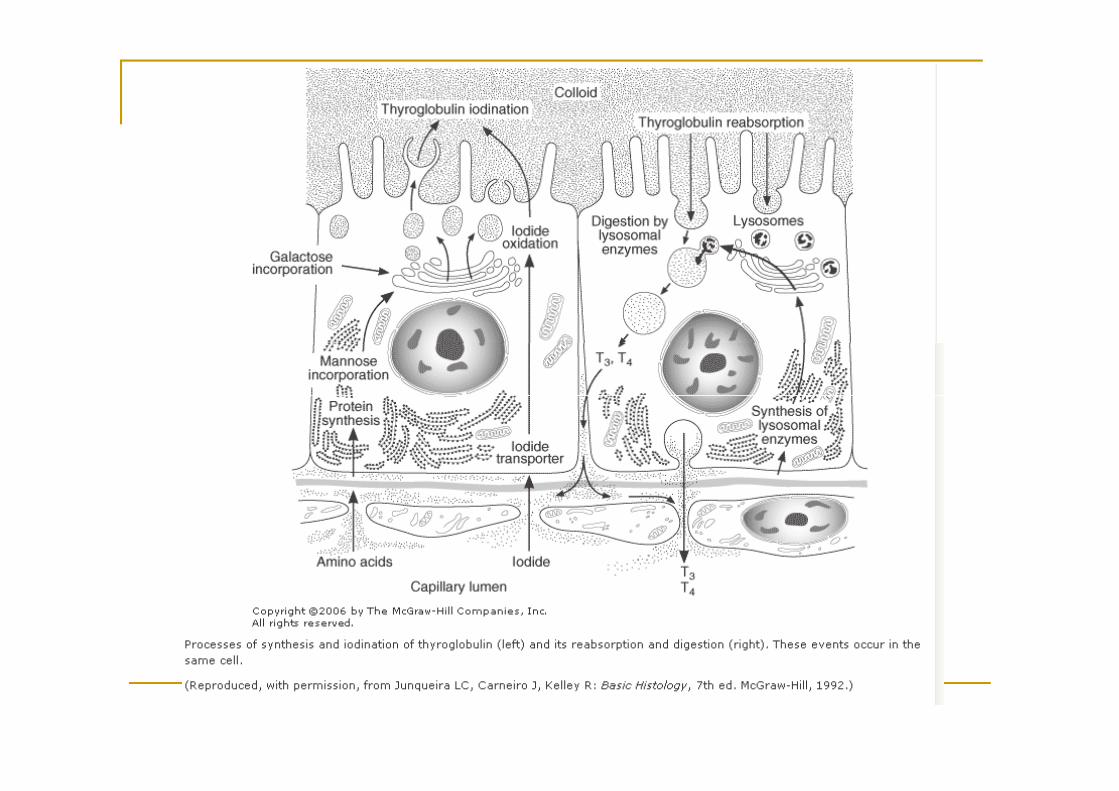
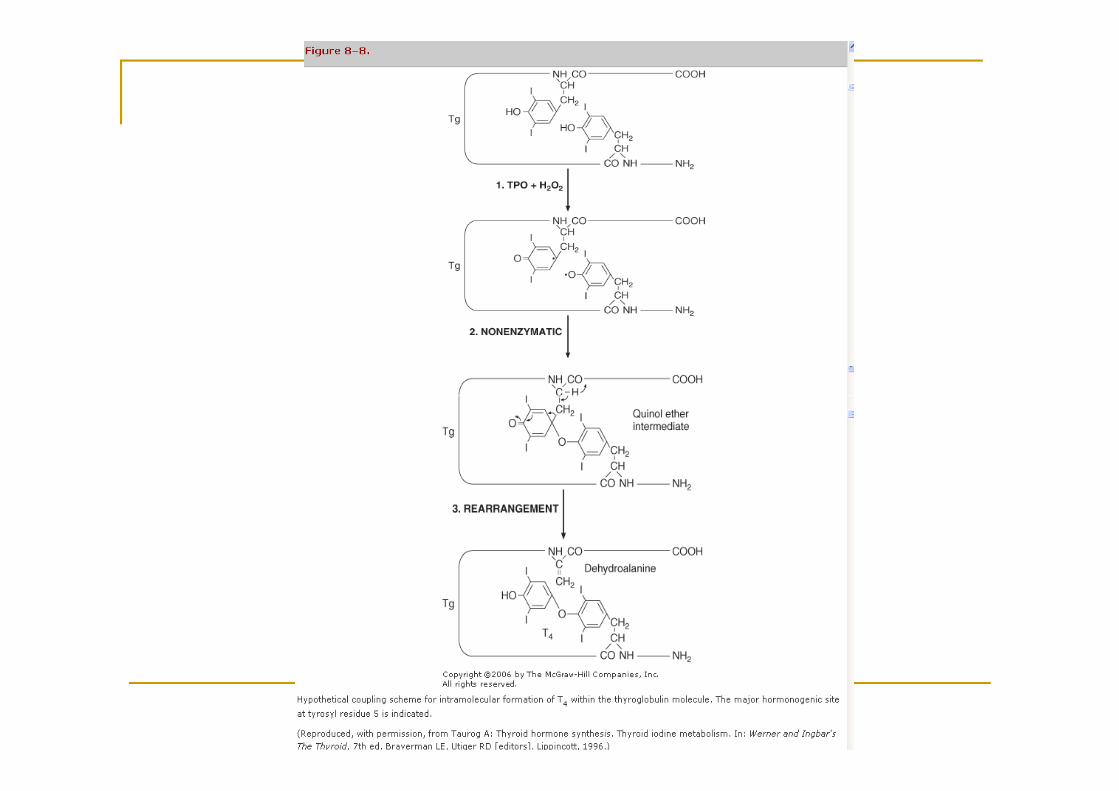
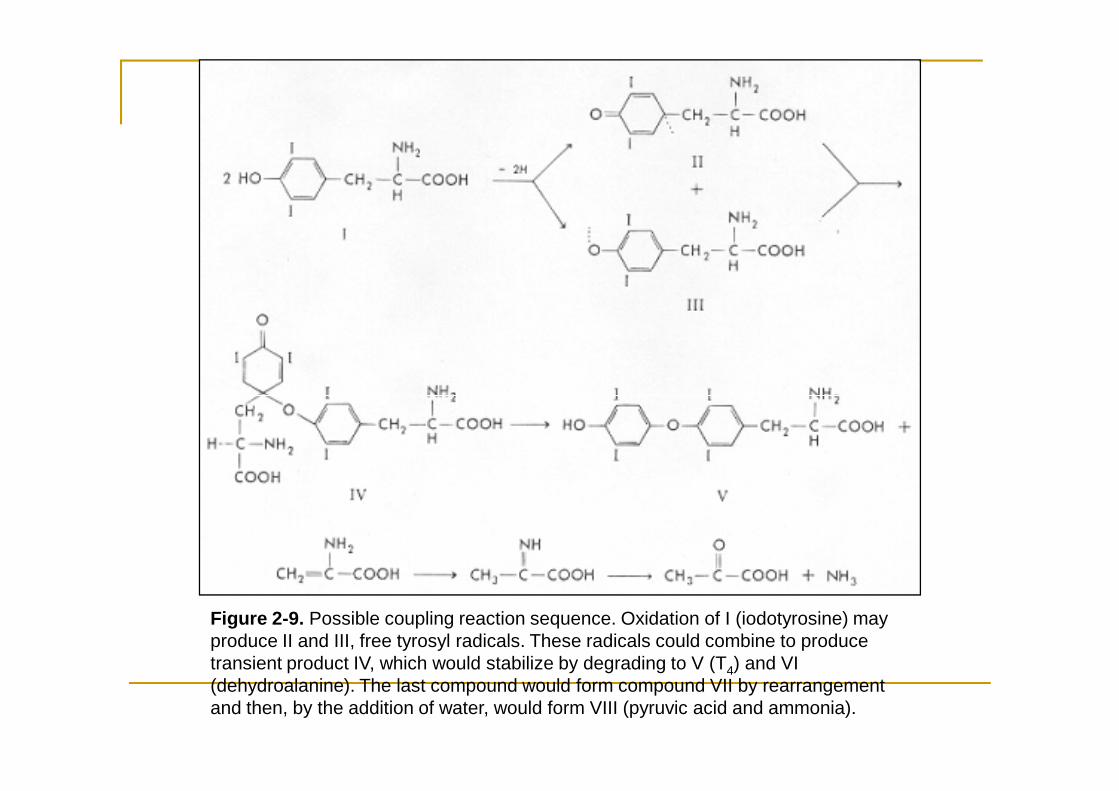
Figure 2-9. Possible coupling reaction sequence. Oxidation of I (iodotyrosine) may produce II and III, free tyrosyl radicals. These radicals could combine to produce transient product IV, which would stabilize by degrading to V (T4) and VI (dehydroalanine). The last compound would form compound VII by rearrangement and then, by the addition of water, would form VIII (pyruvic acid and ammonia).
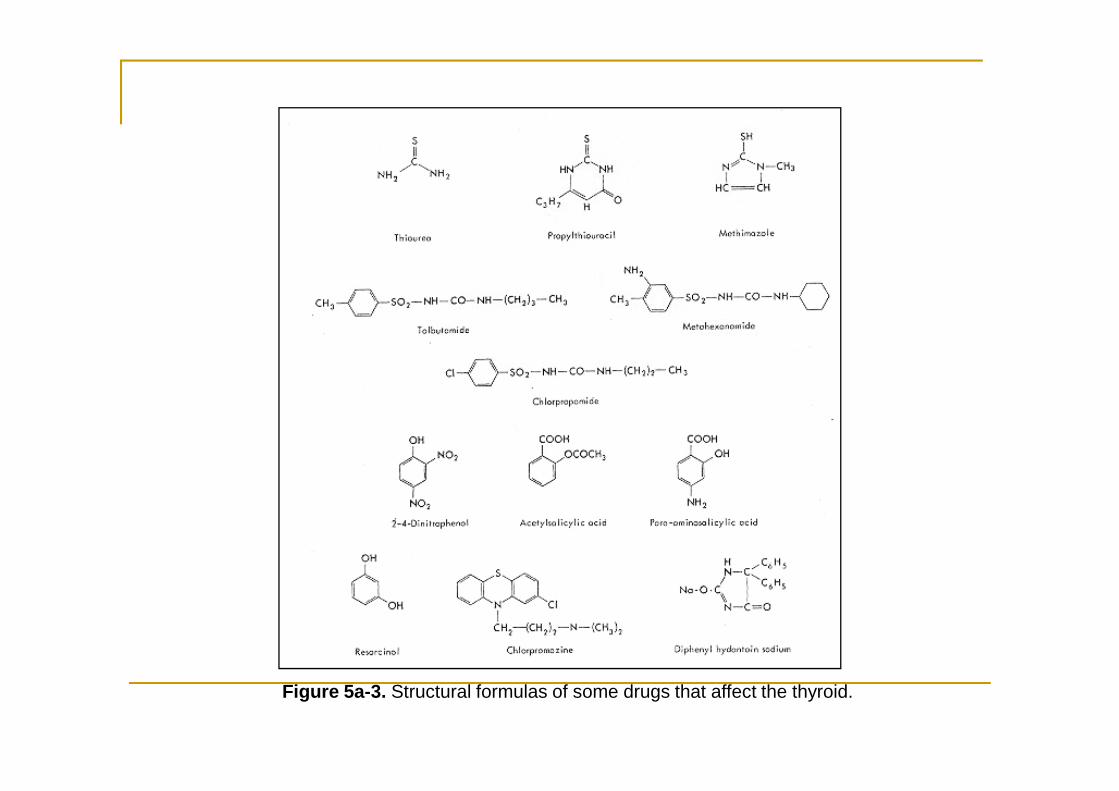
Figure 5a-3. Structural formulas of some drugs that affect the thyroid.
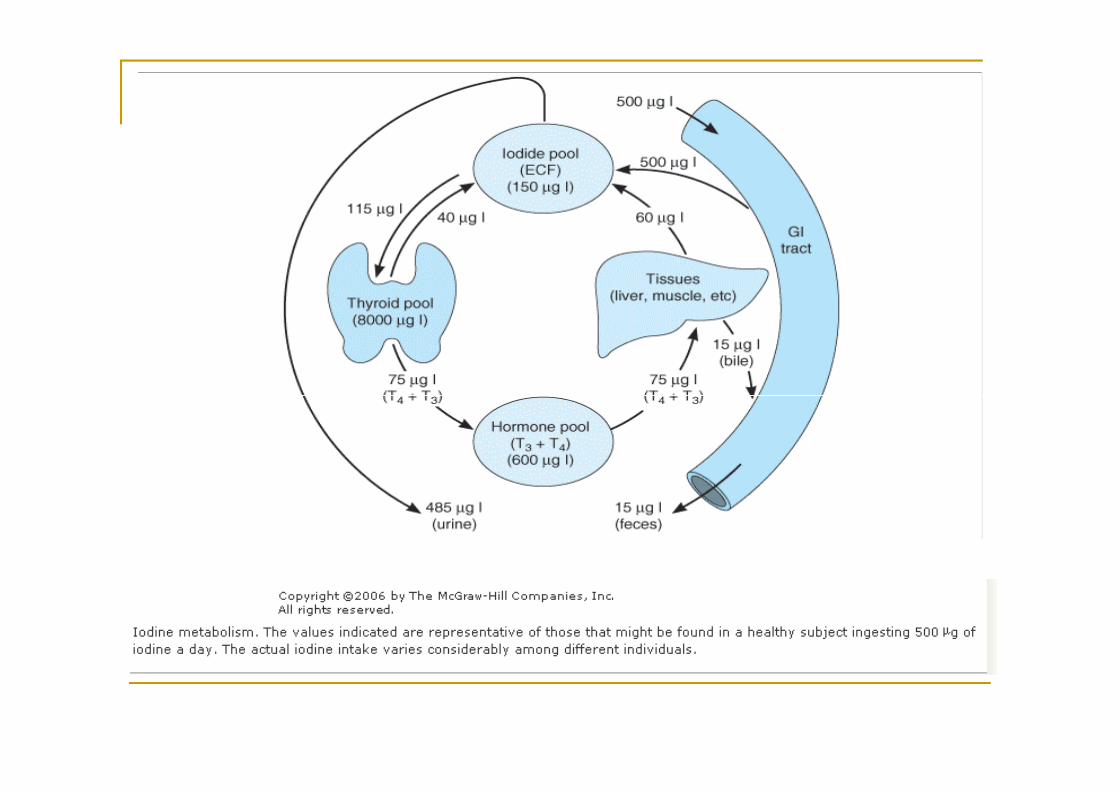
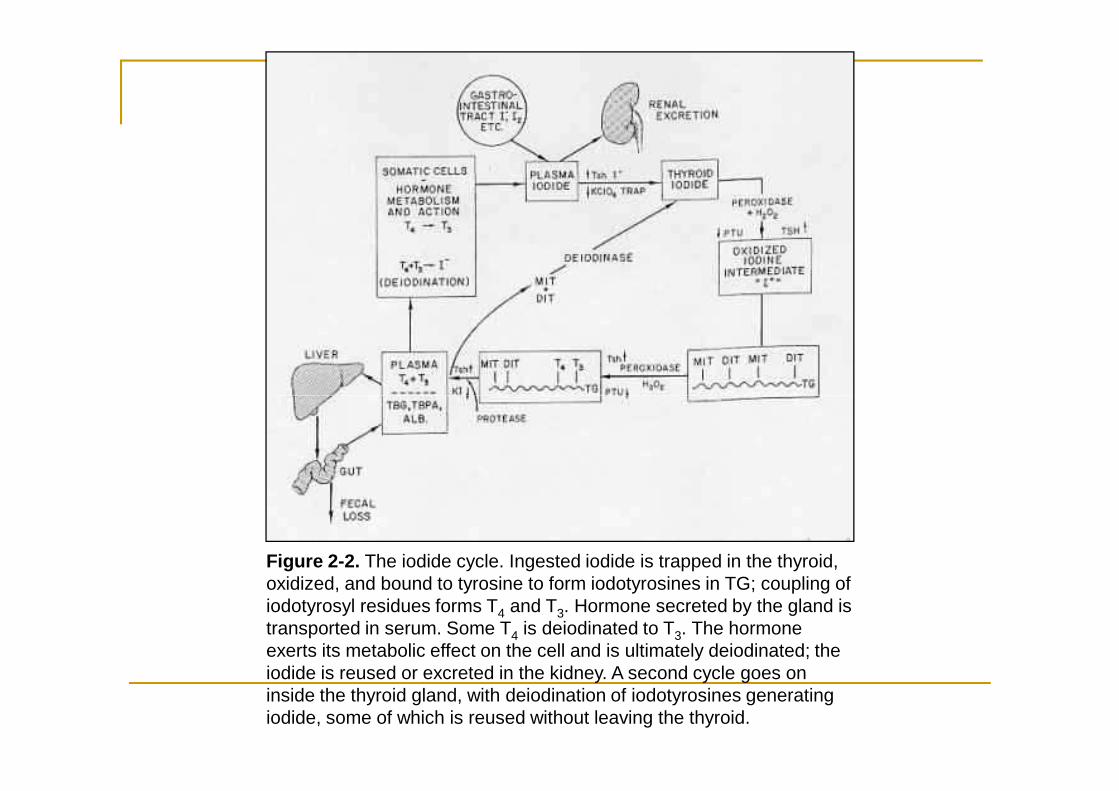
Figure 2-2. The iodide cycle. Ingested iodide is trapped in the thyroid, oxidized, and bound to tyrosine to form iodotyrosines in TG; coupling of iodotyrosyl residues forms T4 and T3. Hormone secreted by the gland is transported in serum. Some T4 is deiodinated to T3. The hormone exerts its metabolic effect on the cell and is ultimately deiodinated; the iodide is reused or excreted in the kidney. A second cycle goes on inside the thyroid gland, with deiodination of iodotyrosines generating iodide, some of which is reused without leaving the thyroid.
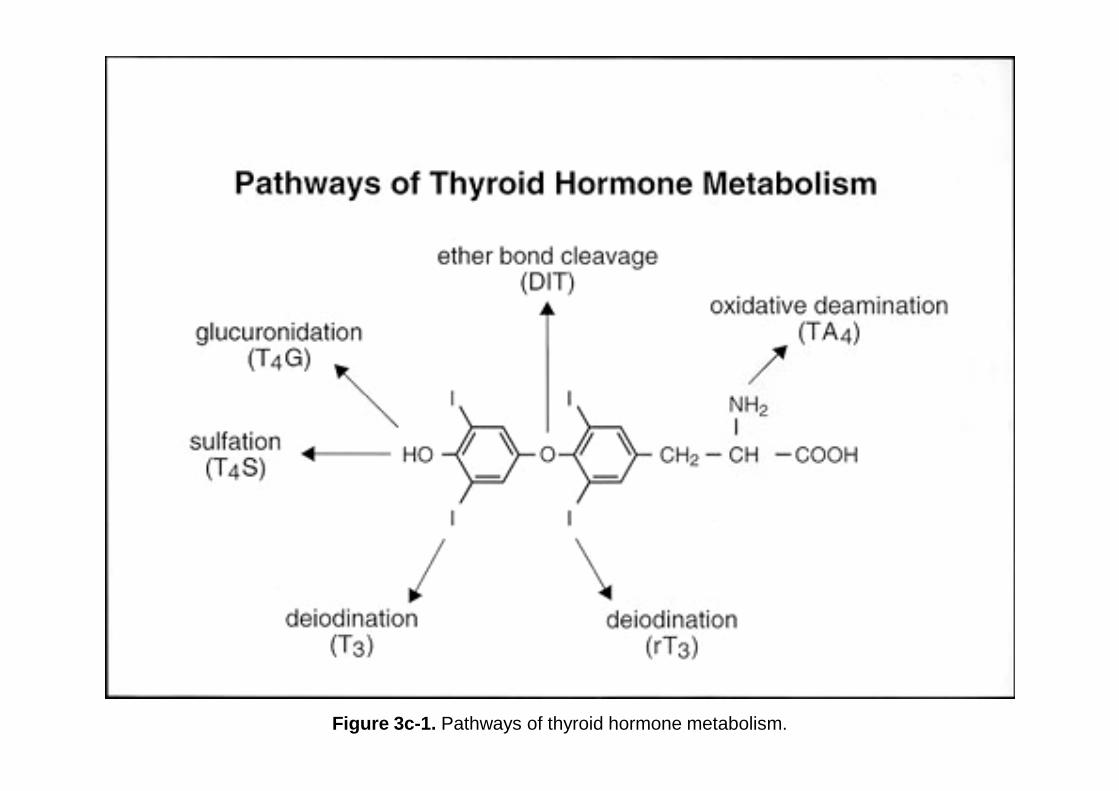
Figure 3c-1. Pathways of thyroid hormone metabolism.
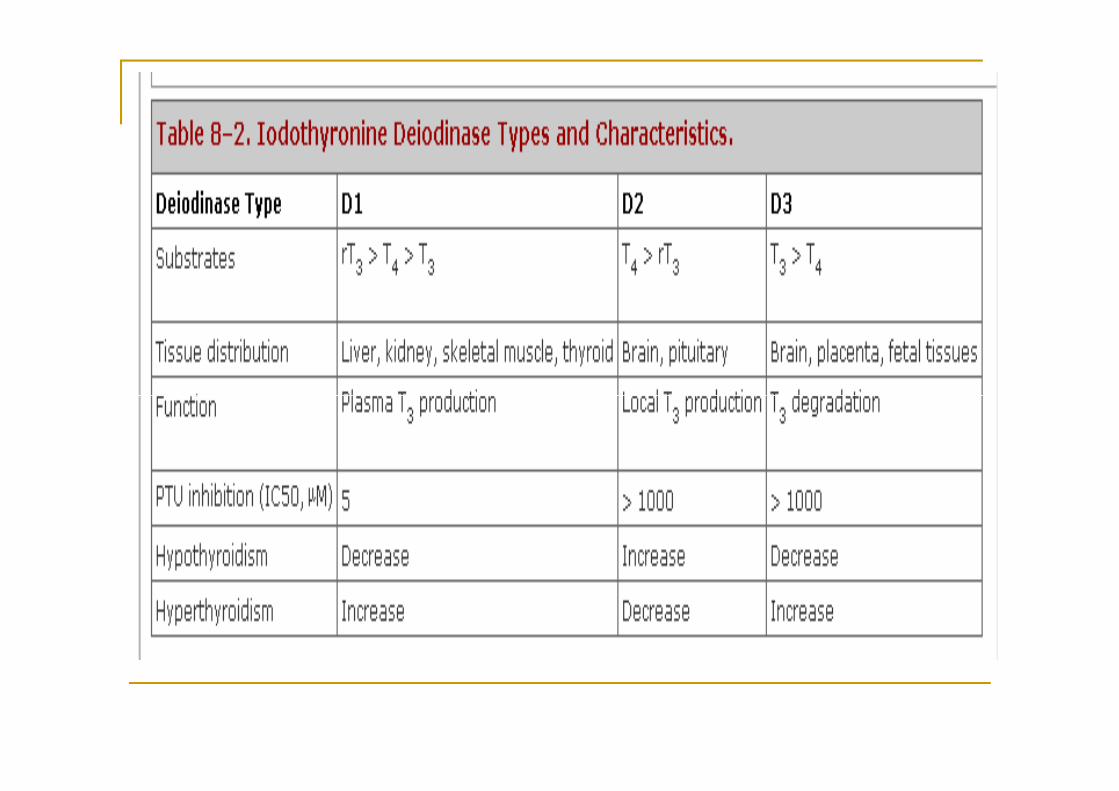
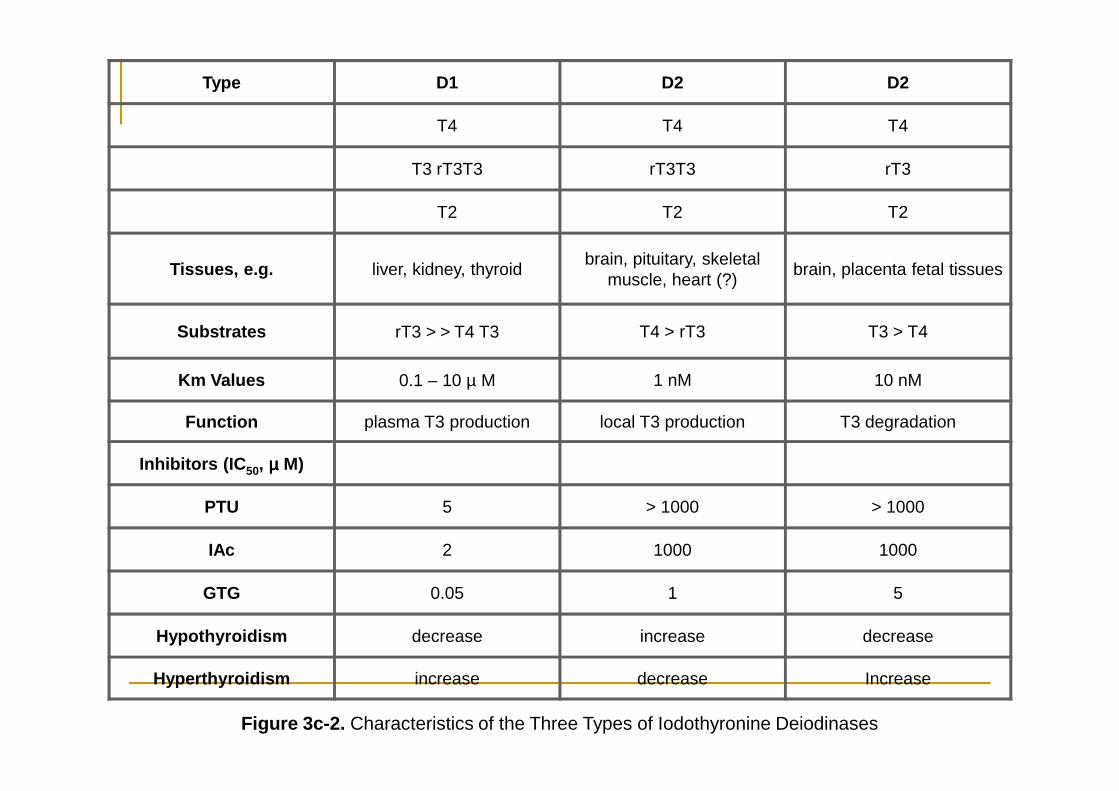
Type D1 D2 D2
T4 T4 T4
T3 rT3T3 rT3T3 rT3
T2 T2 T2
Tissues, e.g. liver, kidney, thyroidbrain, pituitary, skeletal
muscle, heart (?)brain, placenta fetal tissues
Substrates rT3 > > T4 T3 T4 > rT3 T3 > T4
Km Values 0.1 – 10 µ M 1 nM 10 nM
Function plasma T3 production local T3 production T3 degradation
Inhibitors (IC50, µµµµ M)
PTU 5 > 1000 > 1000
IAc 2 1000 1000
GTG 0.05 1 5
Hypothyroidism decrease increase decrease
Hyperthyroidism increase decrease Increase
Figure 3c-2. Characteristics of the Three Types of Iodothyronine Deiodinases
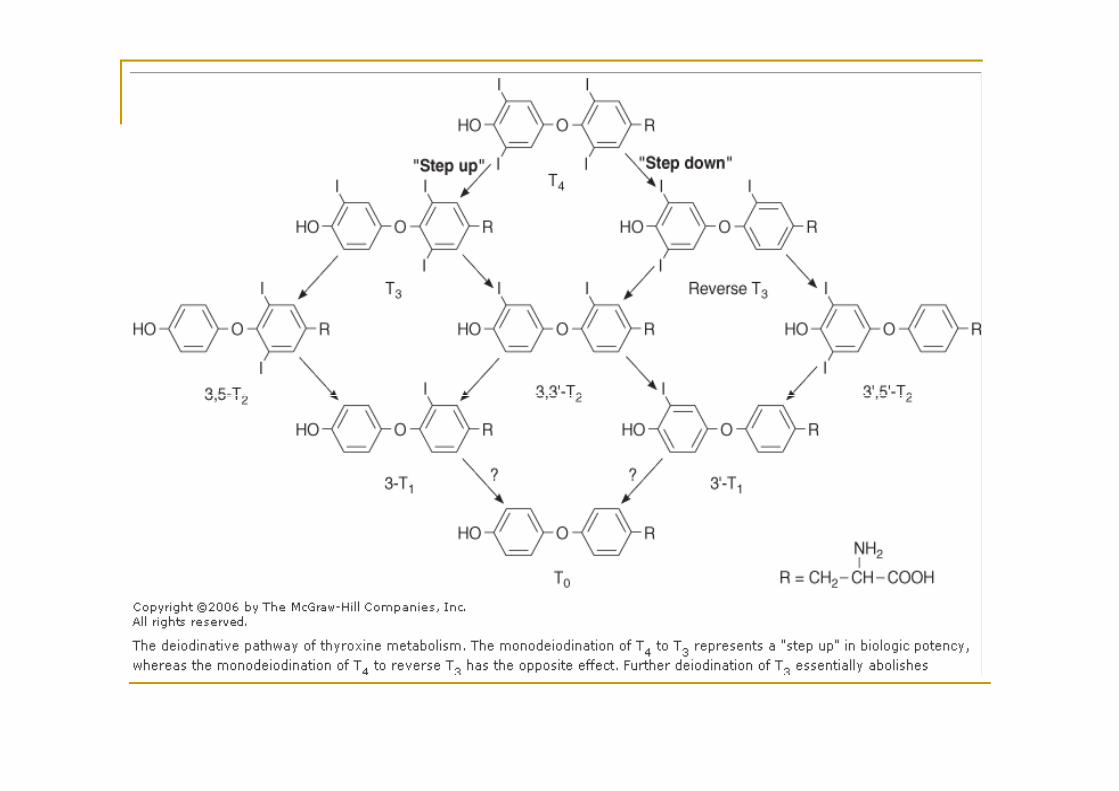
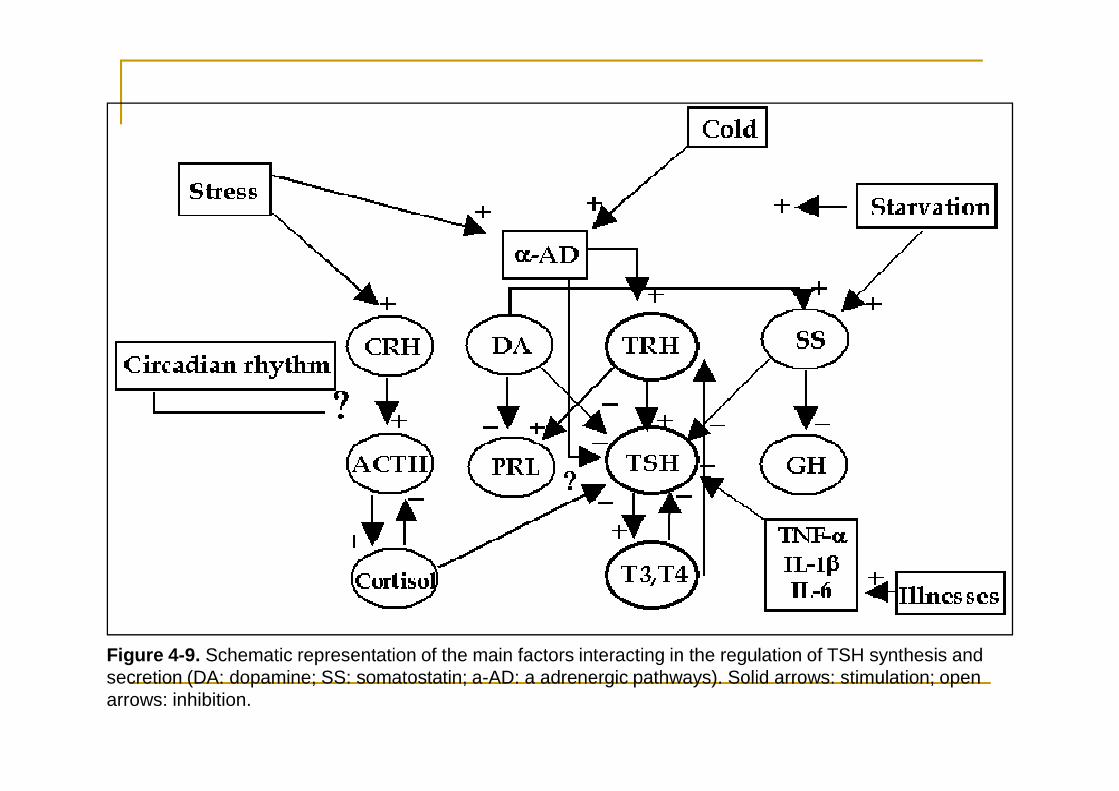
Figure 4-9. Schematic representation of the main factors interacting in the regulation of TSH synthesis and secretion (DA: dopamine; SS: somatostatin; a-AD: a adrenergic pathways). Solid arrows: stimulation; open arrows: inhibition.
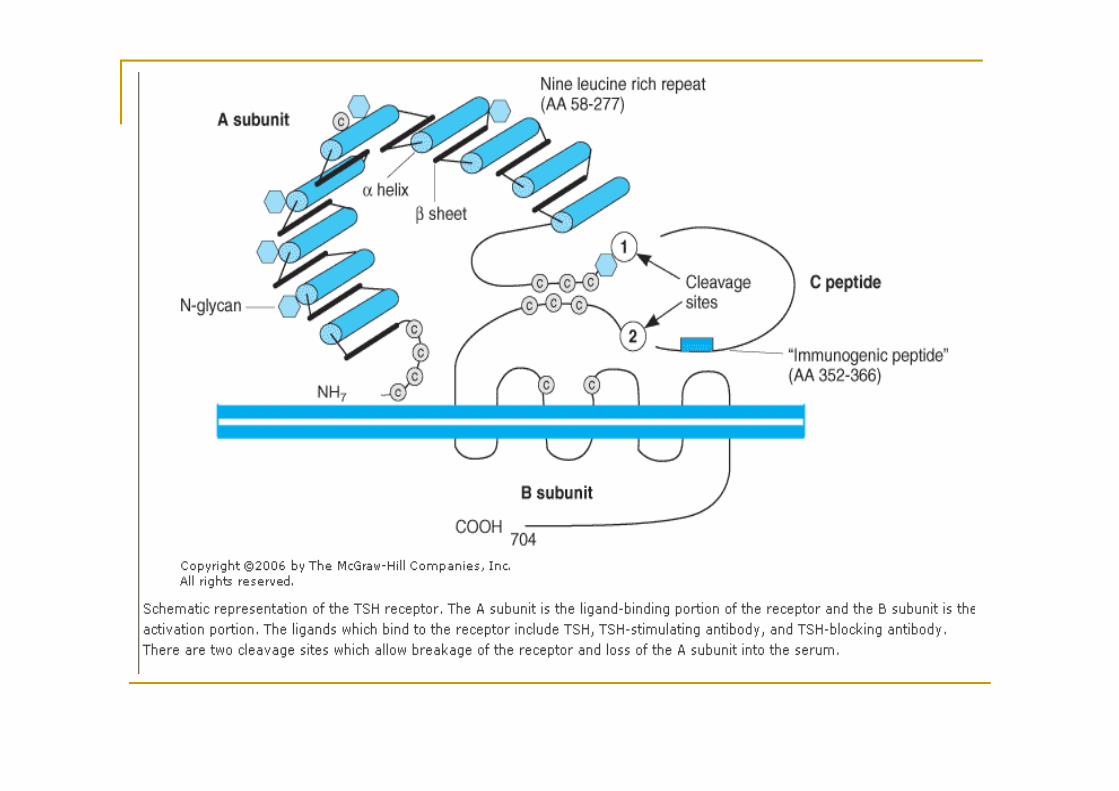
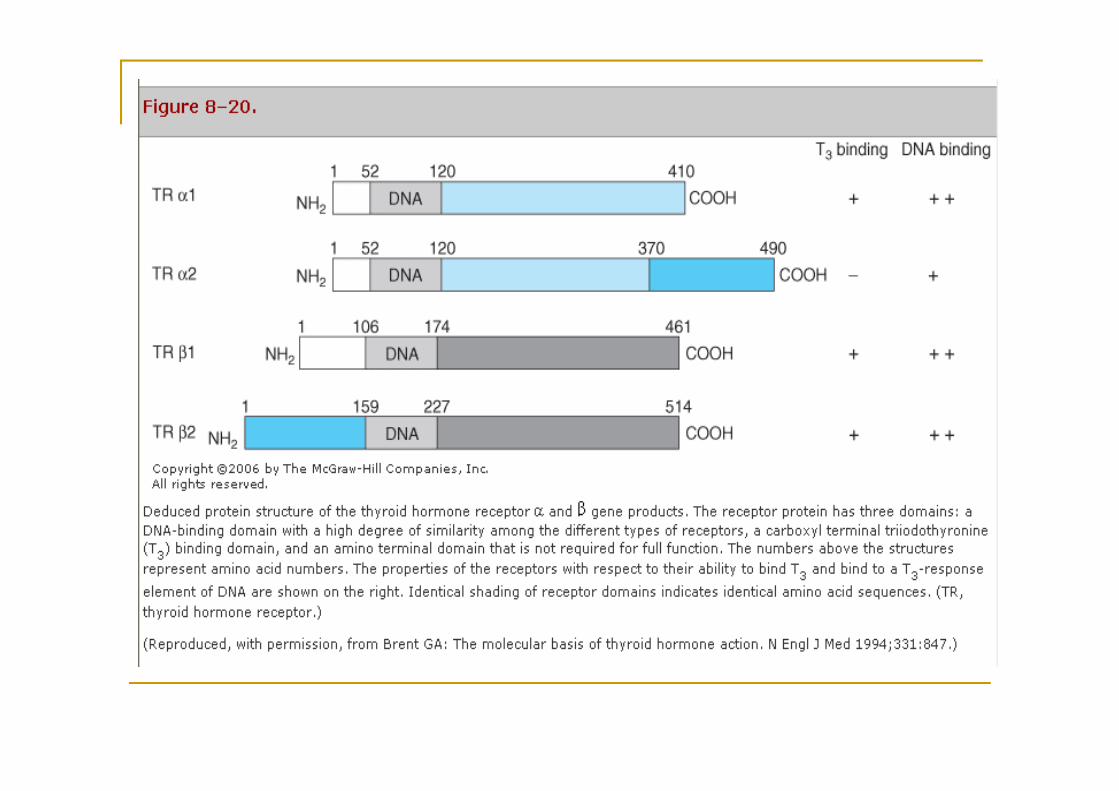
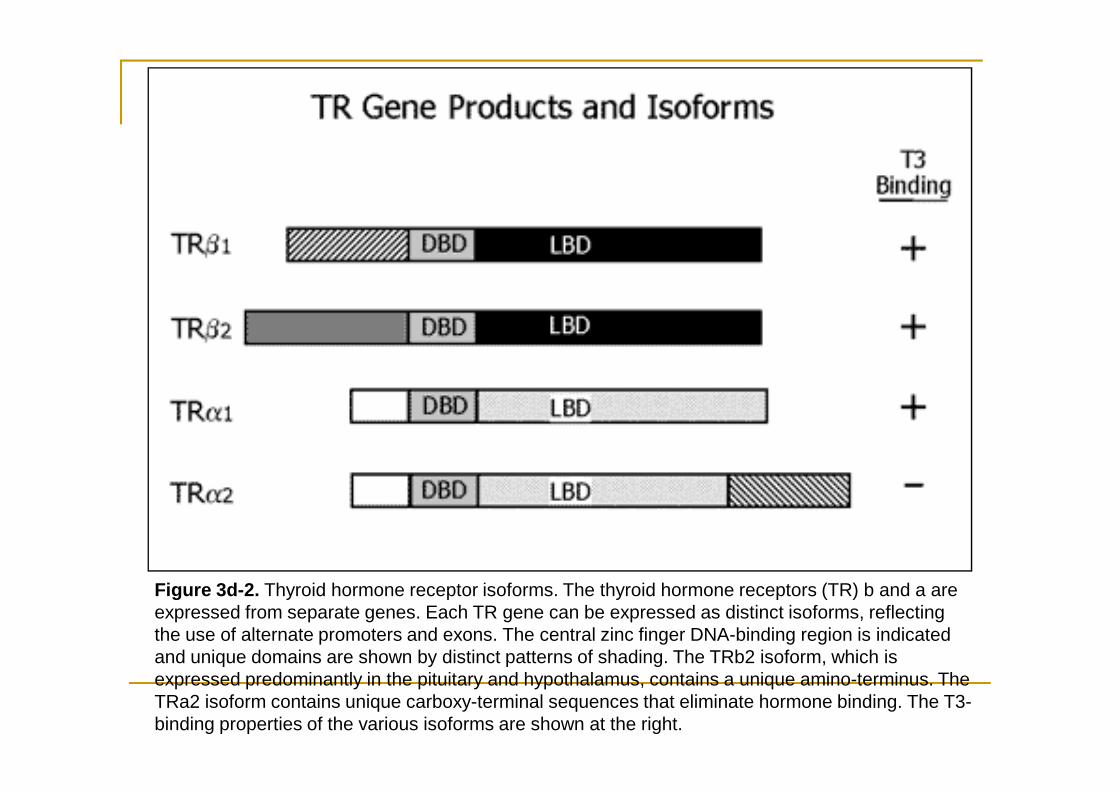
Figure 3d-2. Thyroid hormone receptor isoforms. The thyroid hormone receptors (TR) b and a are expressed from separate genes. Each TR gene can be expressed as distinct isoforms, reflecting the use of alternate promoters and exons. The central zinc finger DNA-binding region is indicated and unique domains are shown by distinct patterns of shading. The TRb2 isoform, which is expressed predominantly in the pituitary and hypothalamus, contains a unique amino-terminus. The TRa2 isoform contains unique carboxy-terminal sequences that eliminate hormone binding. The T3-binding properties of the various isoforms are shown at the right.
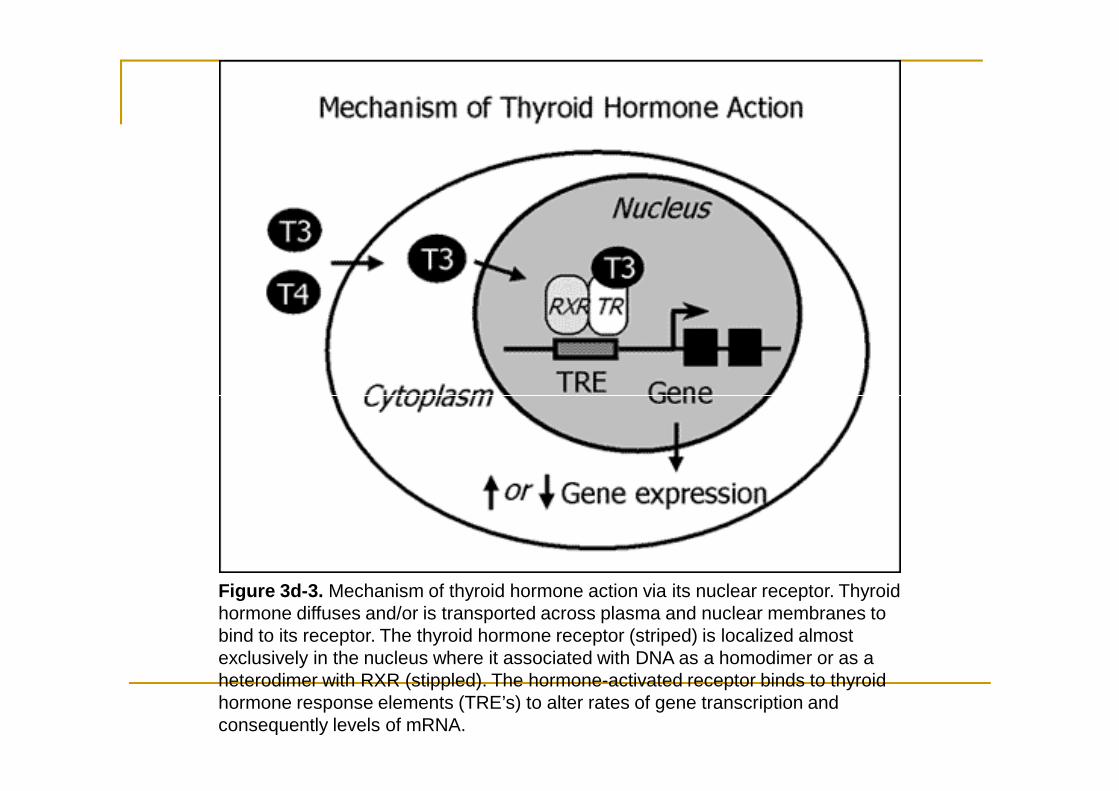
Figure 3d-3. Mechanism of thyroid hormone action via its nuclear receptor. Thyroid hormone diffuses and/or is transported across plasma and nuclear membranes to bind to its receptor. The thyroid hormone receptor (striped) is localized almost exclusively in the nucleus where it associated with DNA as a homodimer or as a heterodimer with RXR (stippled). The hormone-activated receptor binds to thyroid hormone response elements (TRE’s) to alter rates of gene transcription and consequently levels of mRNA.
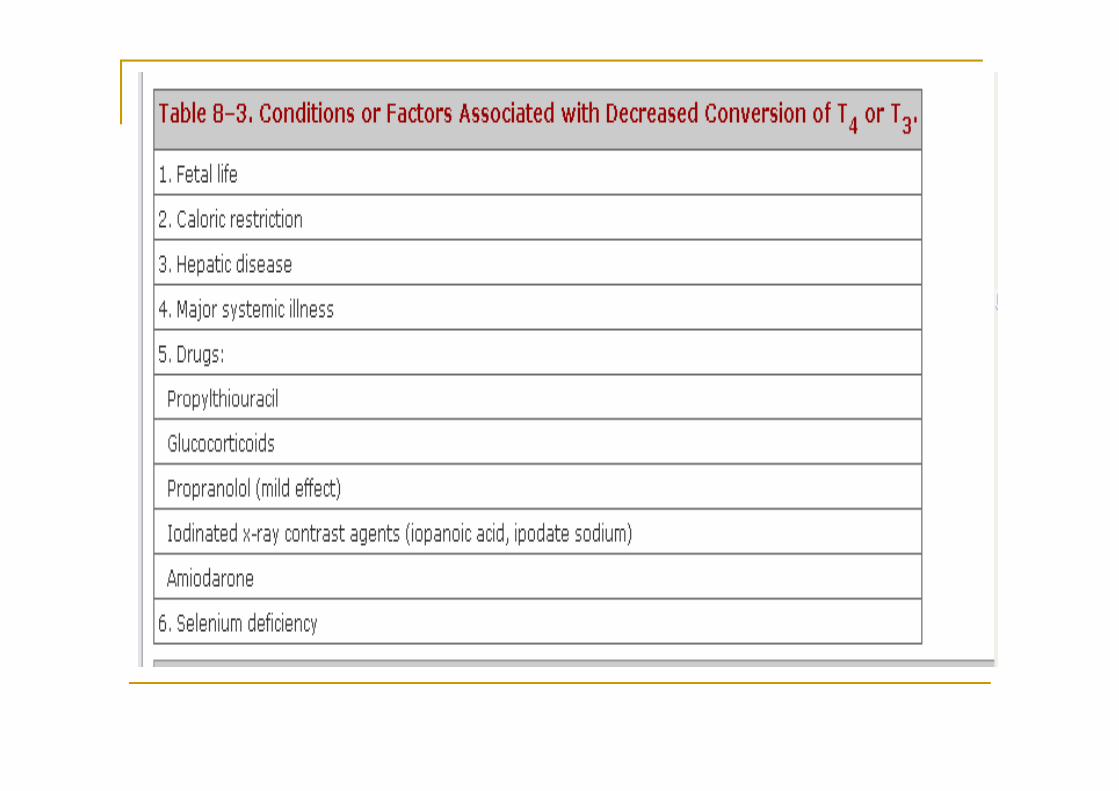
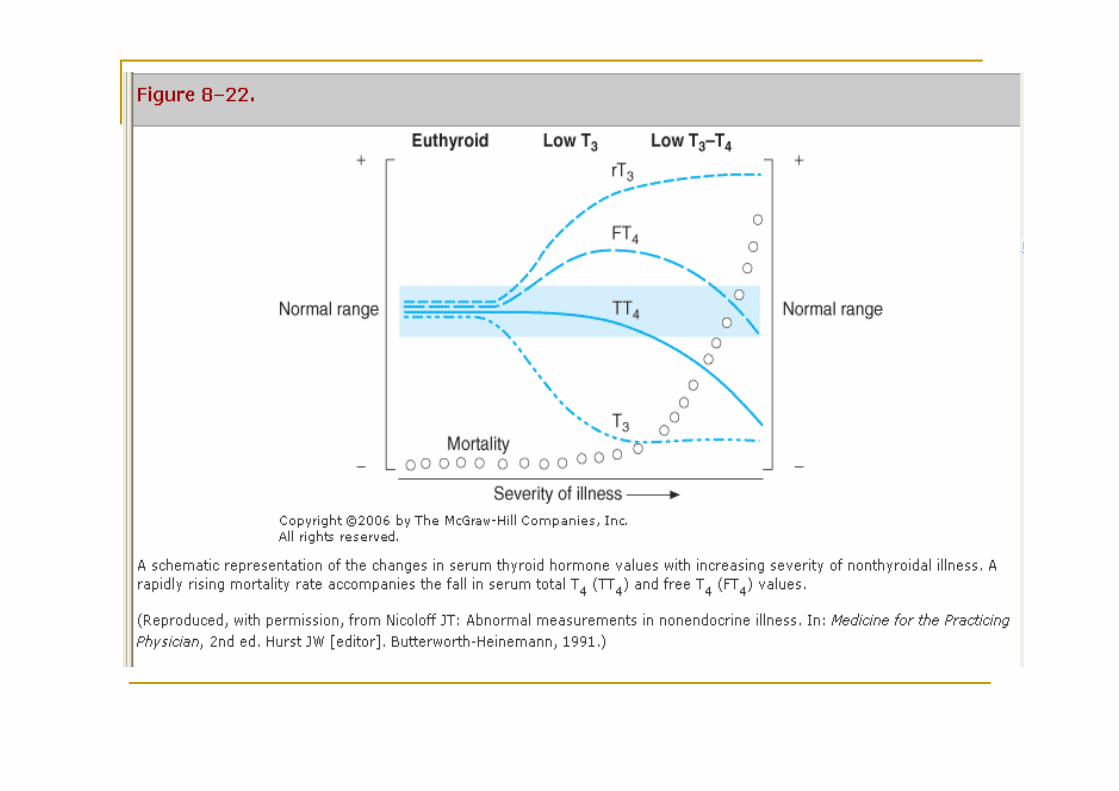
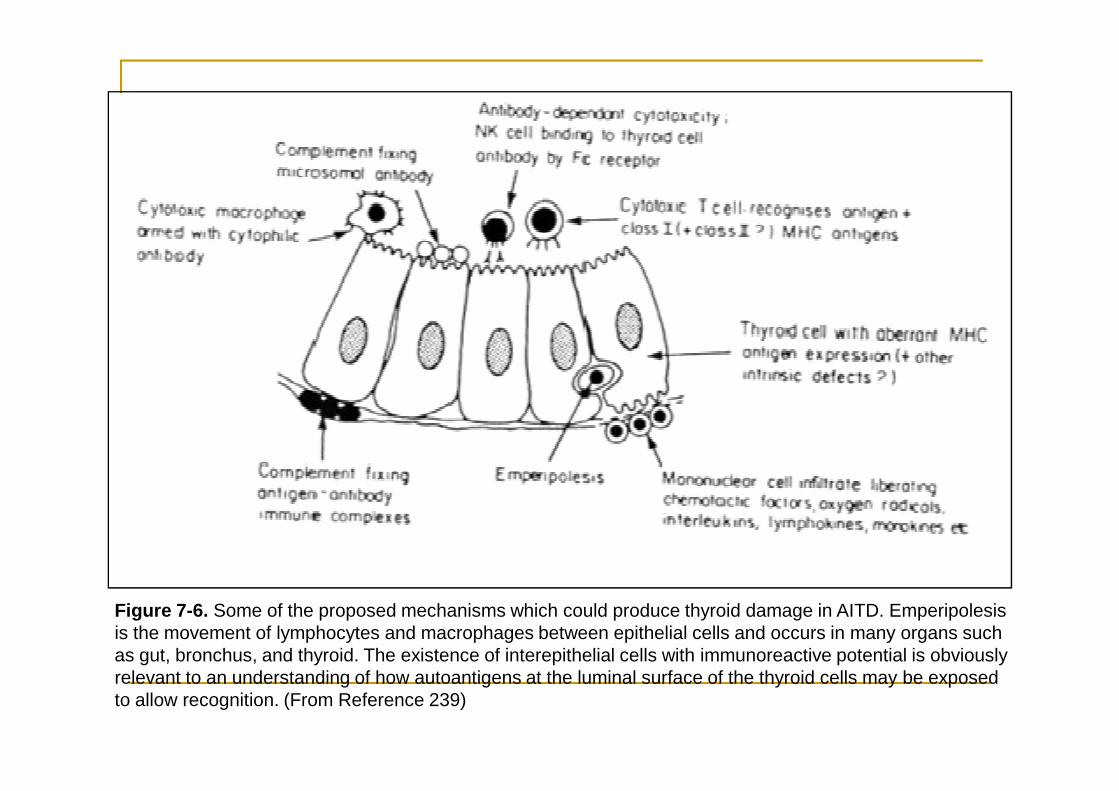
Figure 7-6. Some of the proposed mechanisms which could produce thyroid damage in AITD. Emperipolesis is the movement of lymphocytes and macrophages between epithelial cells and occurs in many organs such as gut, bronchus, and thyroid. The existence of interepithelial cells with immunoreactive potential is obviously relevant to an understanding of how autoantigens at the luminal surface of the thyroid cells may be exposed to allow recognition. (From Reference 239)
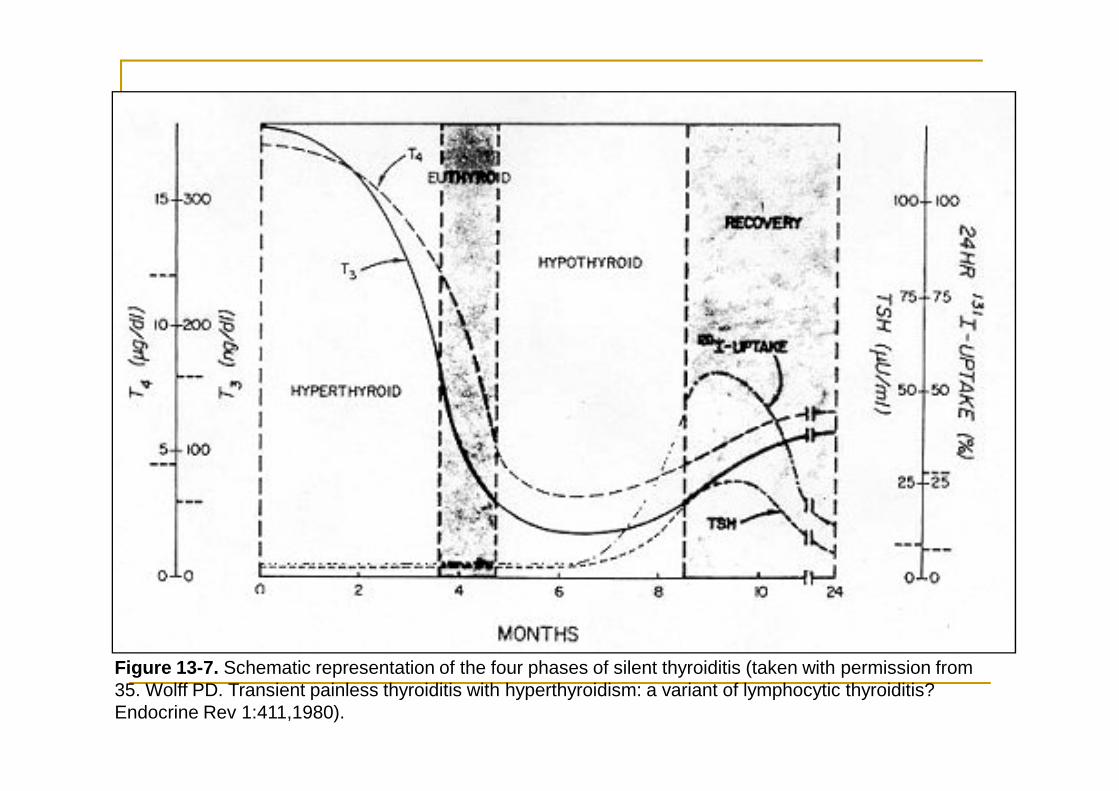
Figure 13-7. Schematic representation of the four phases of silent thyroiditis (taken with permission from 35. Wolff PD. Transient painless thyroiditis with hyperthyroidism: a variant of lymphocytic thyroiditis? Endocrine Rev 1:411,1980).
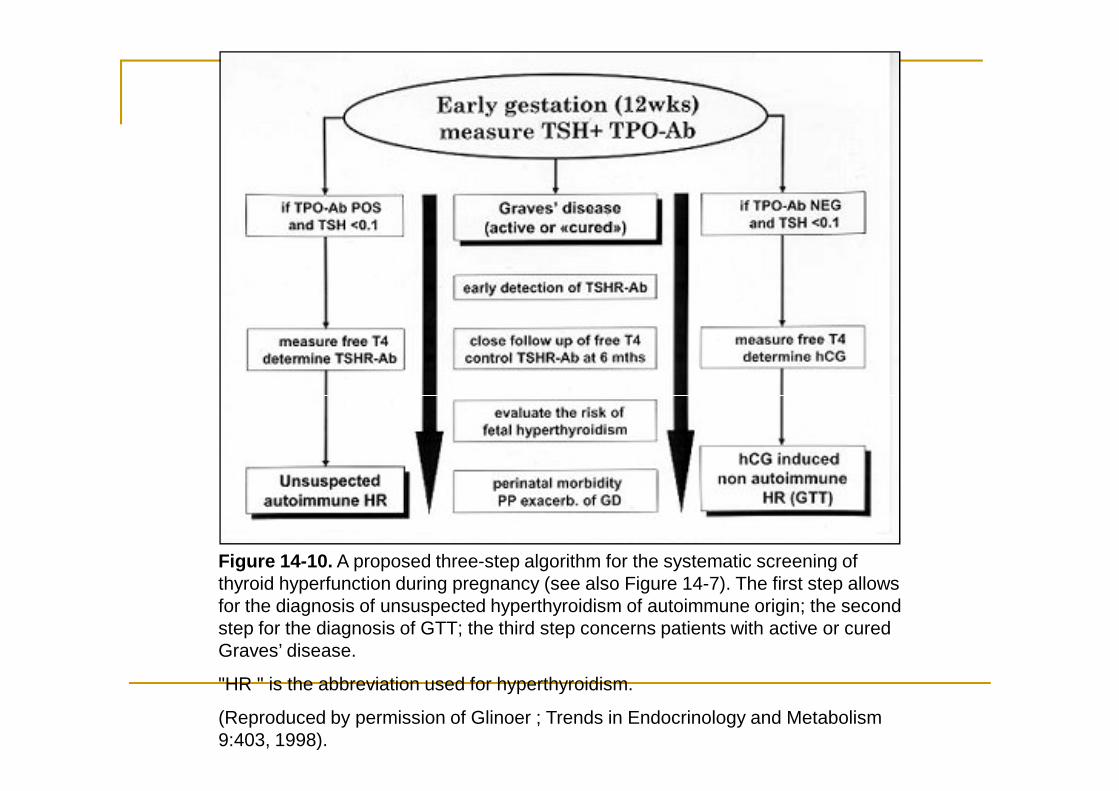
Figure 14-10. A proposed three-step algorithm for the systematic screening of thyroid hyperfunction during pregnancy (see also Figure 14-7). The first step allows for the diagnosis of unsuspected hyperthyroidism of autoimmune origin; the second step for the diagnosis of GTT; the third step concerns patients with active or cured Graves’ disease.
"HR " is the abbreviation used for hyperthyroidism.
(Reproduced by permission of Glinoer ; Trends in Endocrinology and Metabolism 9:403, 1998).
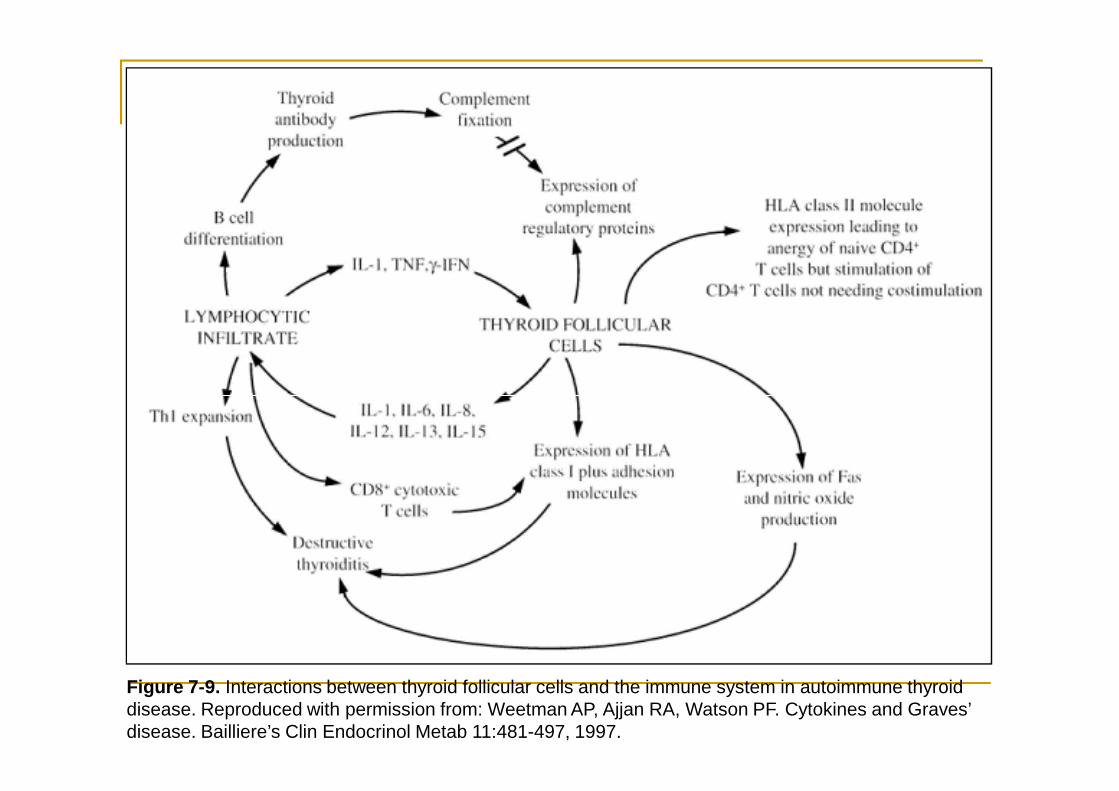
Figure 7-9. Interactions between thyroid follicular cells and the immune system in autoimmune thyroid disease. Reproduced with permission from: Weetman AP, Ajjan RA, Watson PF. Cytokines and Graves’ disease. Bailliere’s Clin Endocrinol Metab 11:481-497, 1997.
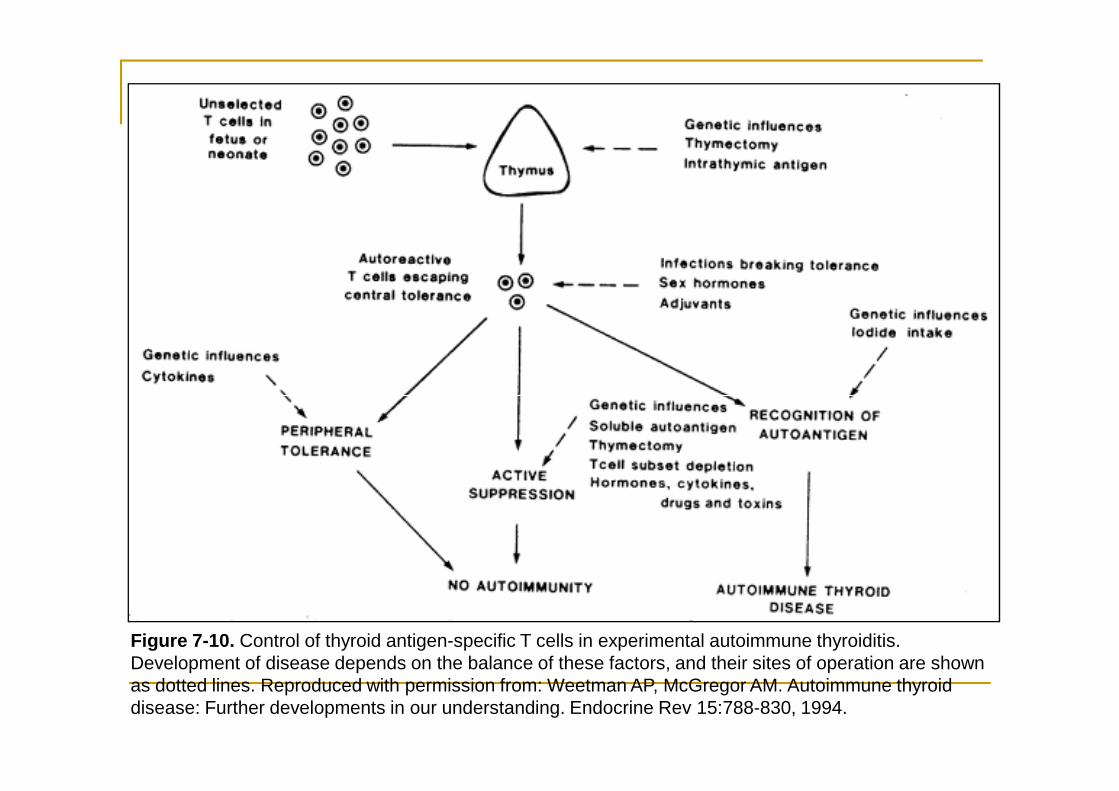
Figure 7-10. Control of thyroid antigen-specific T cells in experimental autoimmune thyroiditis. Development of disease depends on the balance of these factors, and their sites of operation are shown as dotted lines. Reproduced with permission from: Weetman AP, McGregor AM. Autoimmune thyroid disease: Further developments in our understanding. Endocrine Rev 15:788-830, 1994.
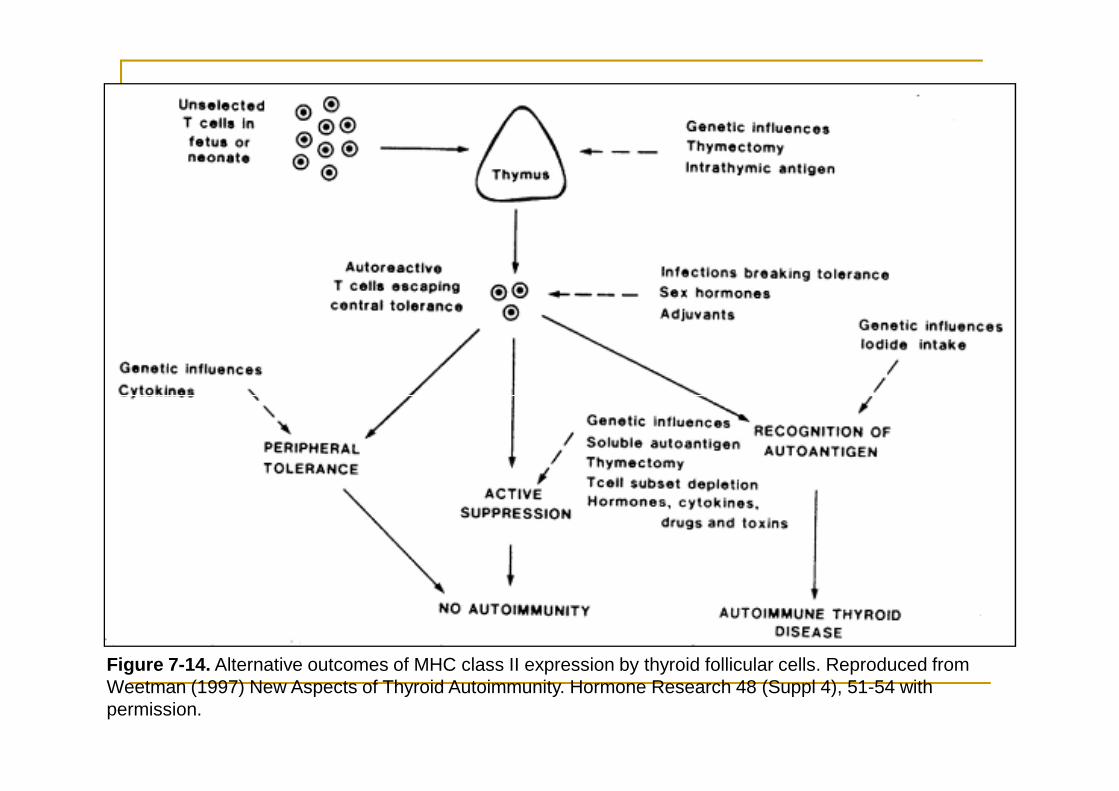
Figure 7-14. Alternative outcomes of MHC class II expression by thyroid follicular cells. Reproduced from Weetman (1997) New Aspects of Thyroid Autoimmunity. Hormone Research 48 (Suppl 4), 51-54 with permission.
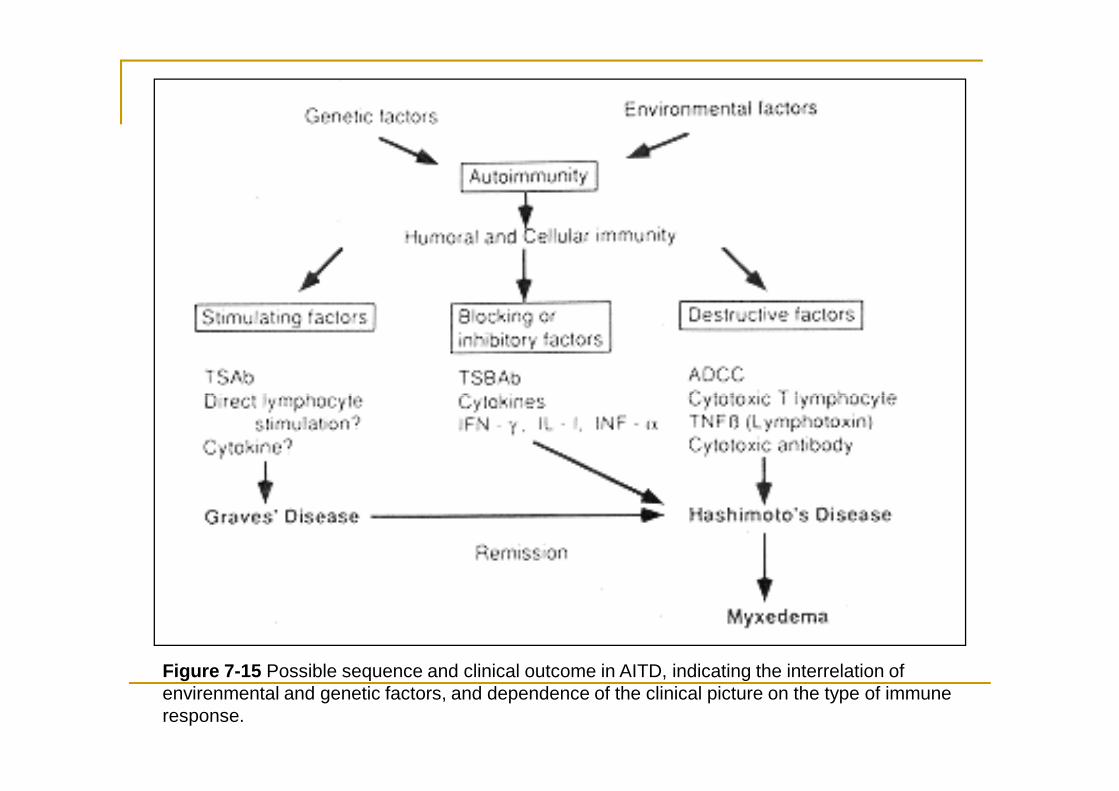
Figure 7-15 Possible sequence and clinical outcome in AITD, indicating the interrelation of envirenmental and genetic factors, and dependence of the clinical picture on the type of immune response.
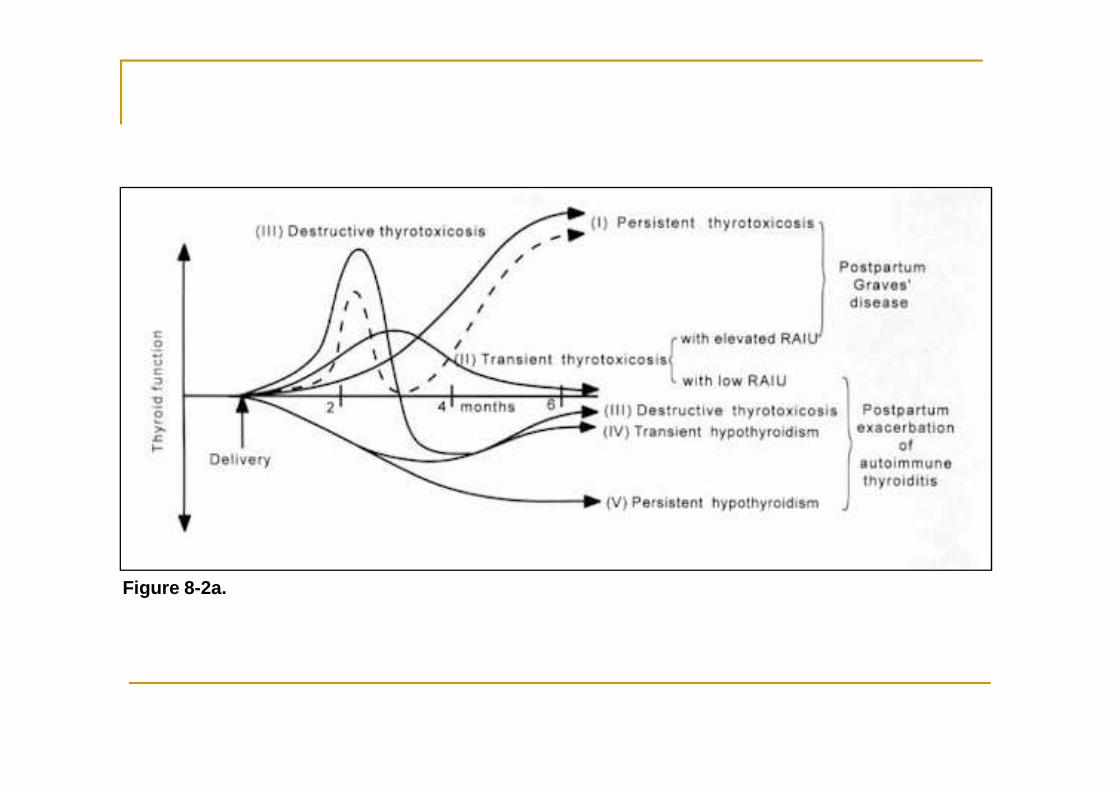
Figure 8-2a.
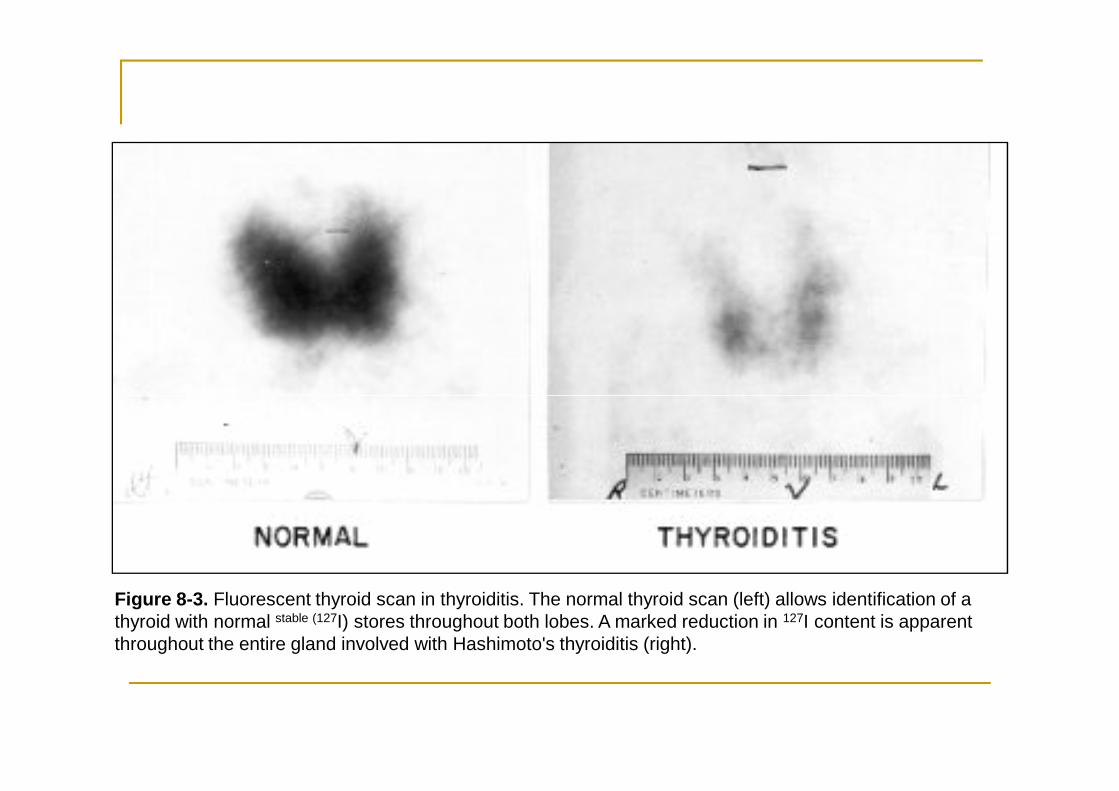
Figure 8-3. Fluorescent thyroid scan in thyroiditis. The normal thyroid scan (left) allows identification of a thyroid with normal stable (127I) stores throughout both lobes. A marked reduction in 127I content is apparent throughout the entire gland involved with Hashimoto's thyroiditis (right).
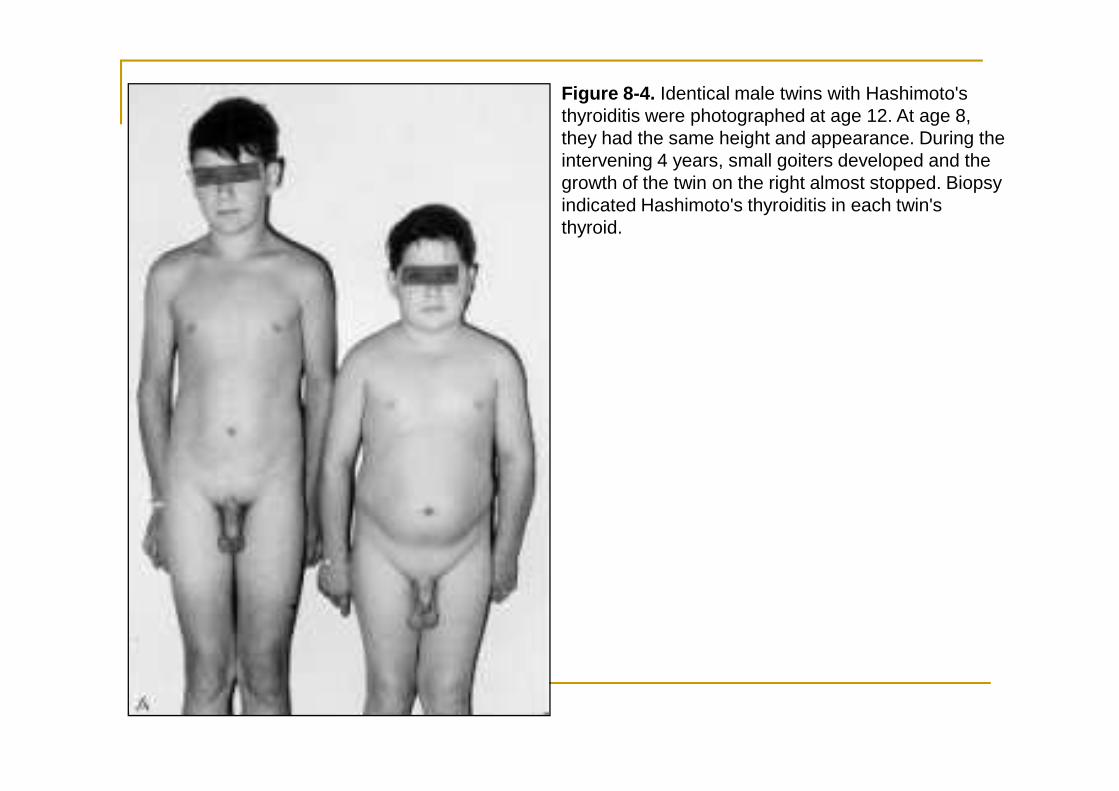
Figure 8-4. Identical male twins with Hashimoto's thyroiditis were photographed at age 12. At age 8, they had the same height and appearance. During the intervening 4 years, small goiters developed and the growth of the twin on the right almost stopped. Biopsy indicated Hashimoto's thyroiditis in each twin's thyroid.
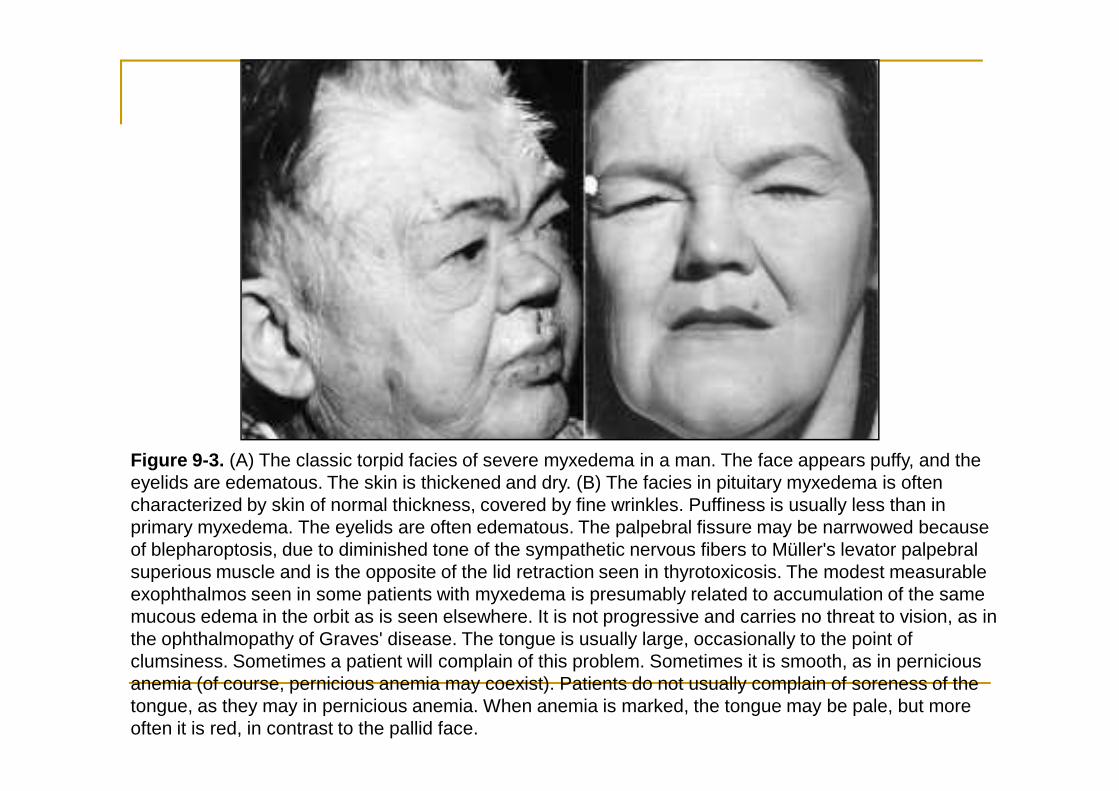
Figure 9-3. (A) The classic torpid facies of severe myxedema in a man. The face appears puffy, and the eyelids are edematous. The skin is thickened and dry. (B) The facies in pituitary myxedema is often characterized by skin of normal thickness, covered by fine wrinkles. Puffiness is usually less than in primary myxedema. The eyelids are often edematous. The palpebral fissure may be narrwowed because of blepharoptosis, due to diminished tone of the sympathetic nervous fibers to Müller's levator palpebral superious muscle and is the opposite of the lid retraction seen in thyrotoxicosis. The modest measurable exophthalmos seen in some patients with myxedema is presumably related to accumulation of the same mucous edema in the orbit as is seen elsewhere. It is not progressive and carries no threat to vision, as in the ophthalmopathy of Graves' disease. The tongue is usually large, occasionally to the point of clumsiness. Sometimes a patient will complain of this problem. Sometimes it is smooth, as in pernicious anemia (of course, pernicious anemia may coexist). Patients do not usually complain of soreness of the tongue, as they may in pernicious anemia. When anemia is marked, the tongue may be pale, but more often it is red, in contrast to the pallid face.
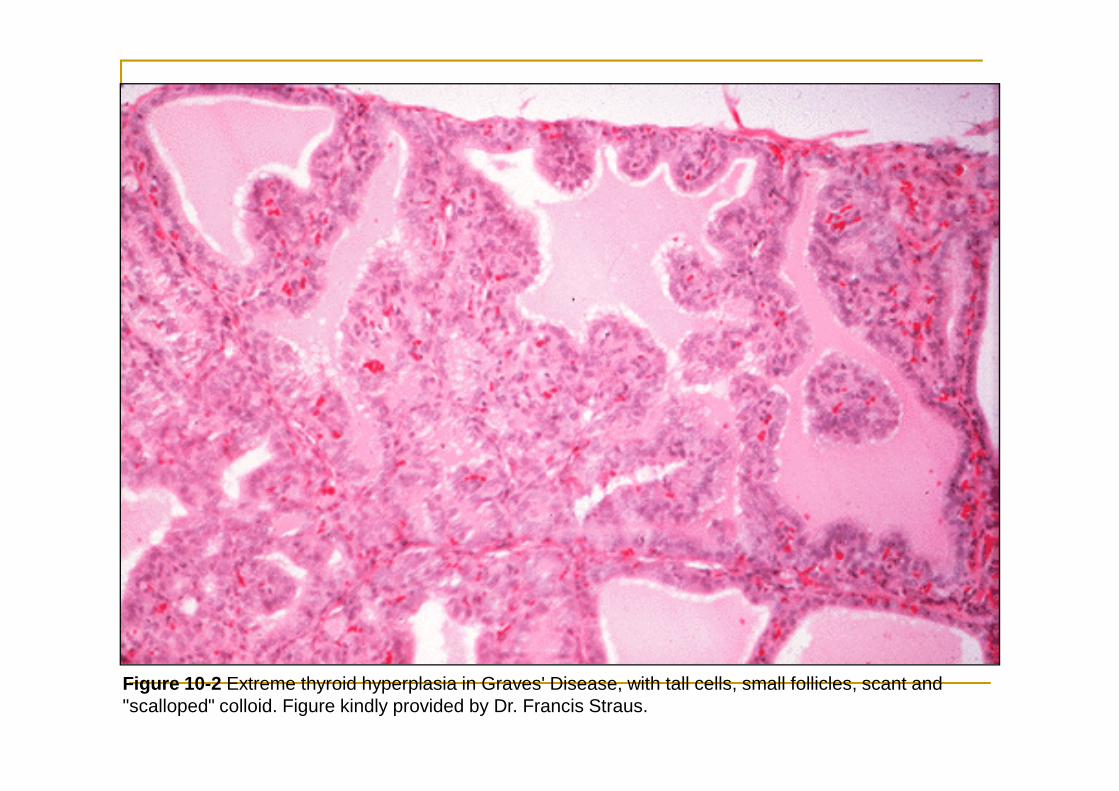
Figure 10-2 Extreme thyroid hyperplasia in Graves' Disease, with tall cells, small follicles, scant and "scalloped" colloid. Figure kindly provided by Dr. Francis Straus.
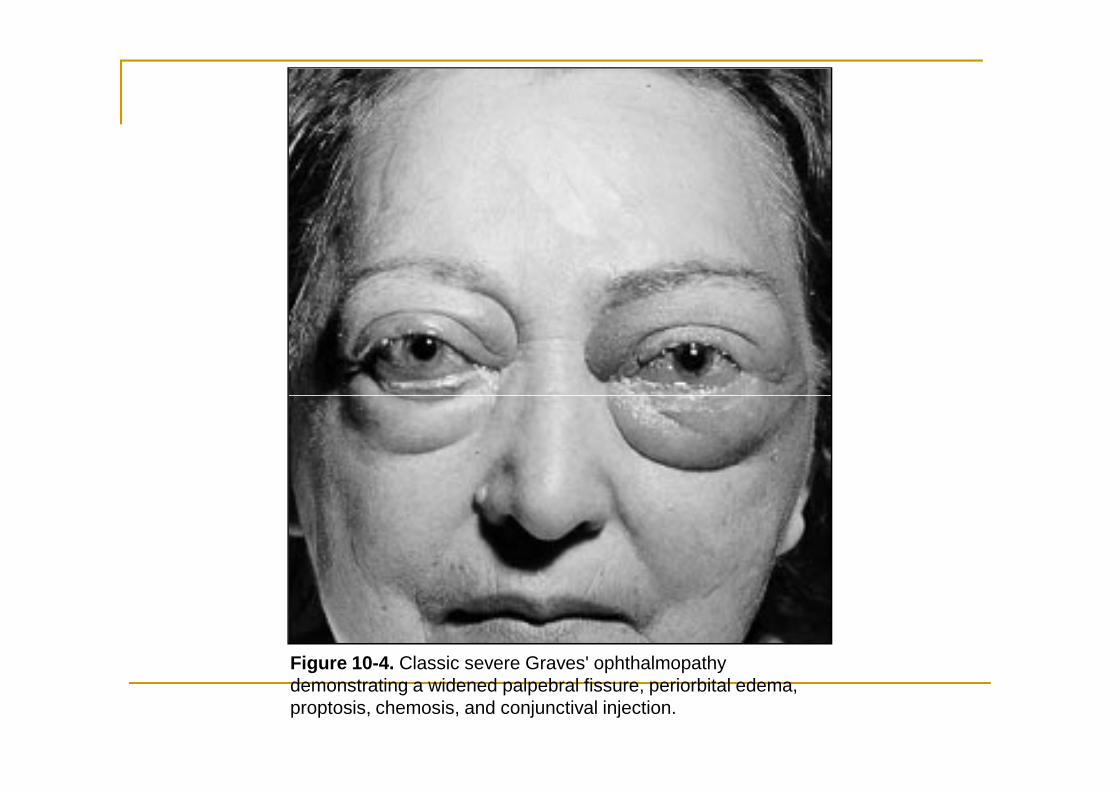
Figure 10-4. Classic severe Graves' ophthalmopathy demonstrating a widened palpebral fissure, periorbital edema, proptosis, chemosis, and conjunctival injection.
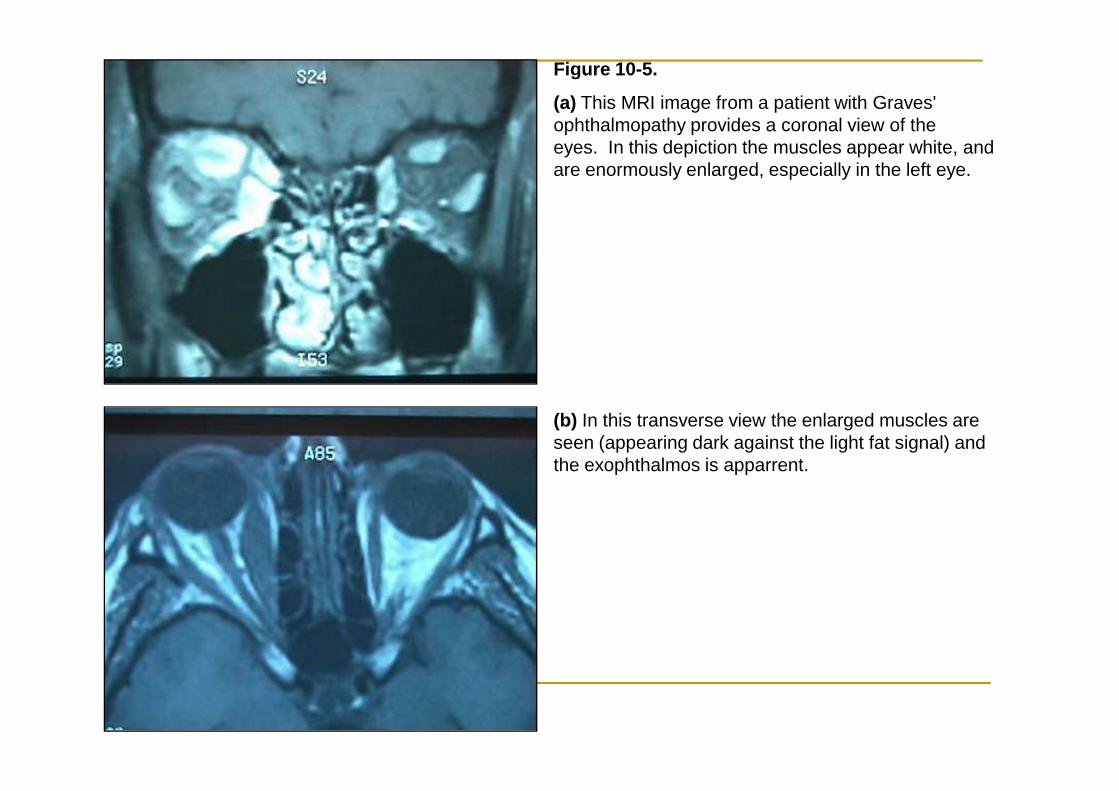
Figure 10-5.
(a) This MRI image from a patient with Graves' ophthalmopathy provides a coronal view of the eyes. In this depiction the muscles appear white, and are enormously enlarged, especially in the left eye.
(b) In this transverse view the enlarged muscles are seen (appearing dark against the light fat signal) and the exophthalmos is apparrent.
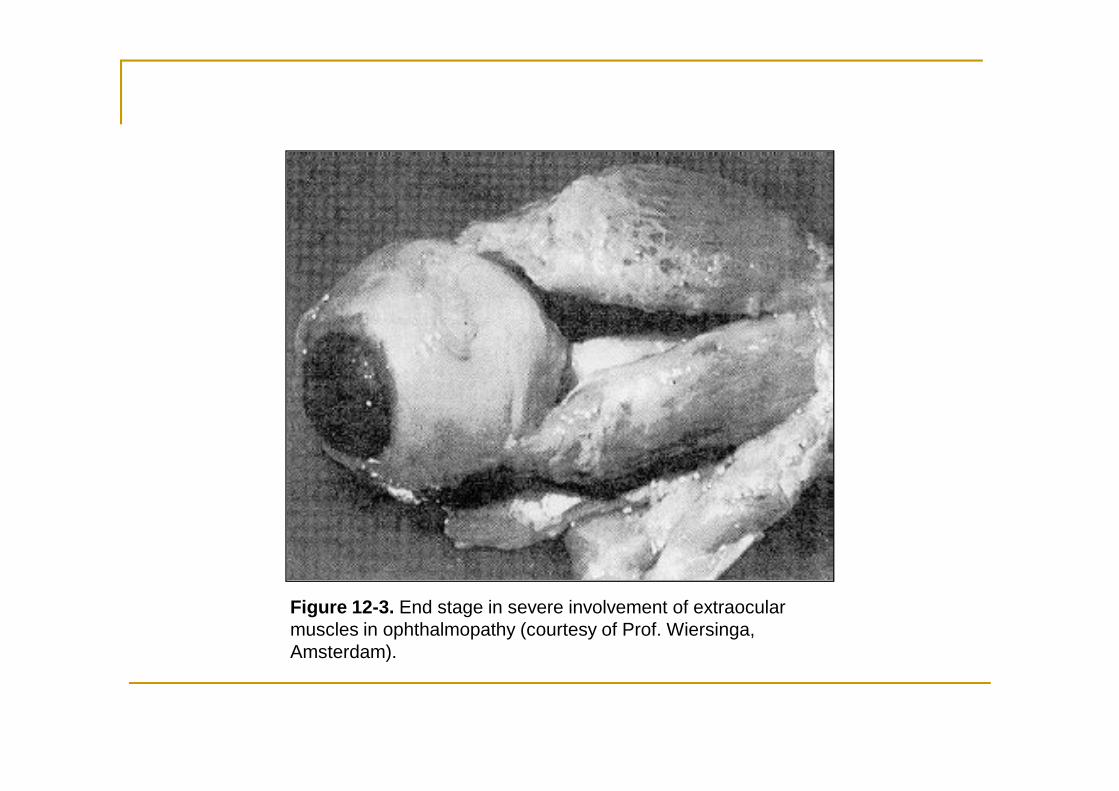
Figure 12-3. End stage in severe involvement of extraocular muscles in ophthalmopathy (courtesy of Prof. Wiersinga, Amsterdam).
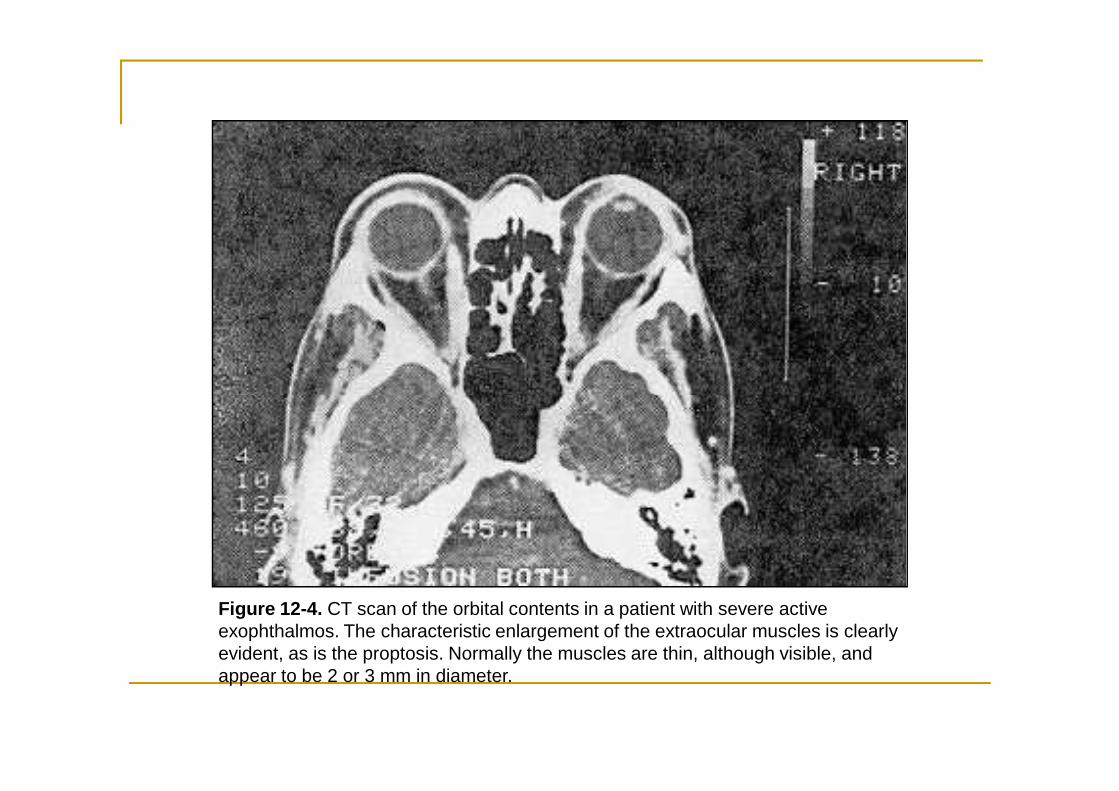
Figure 12-4. CT scan of the orbital contents in a patient with severe active exophthalmos. The characteristic enlargement of the extraocular muscles is clearly evident, as is the proptosis. Normally the muscles are thin, although visible, and appear to be 2 or 3 mm in diameter.
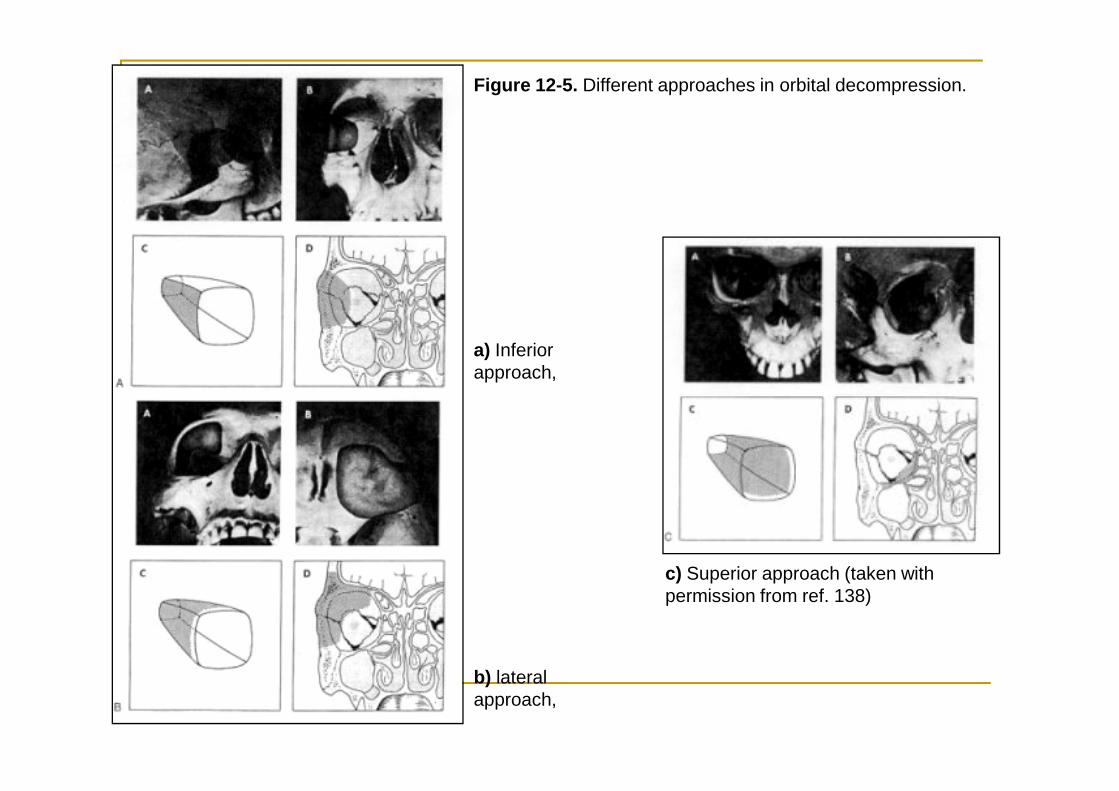
Figure 12-5. Different approaches in orbital decompression.
a) Inferior approach,
b) lateral approach,
c) Superior approach (taken with permission from ref. 138)
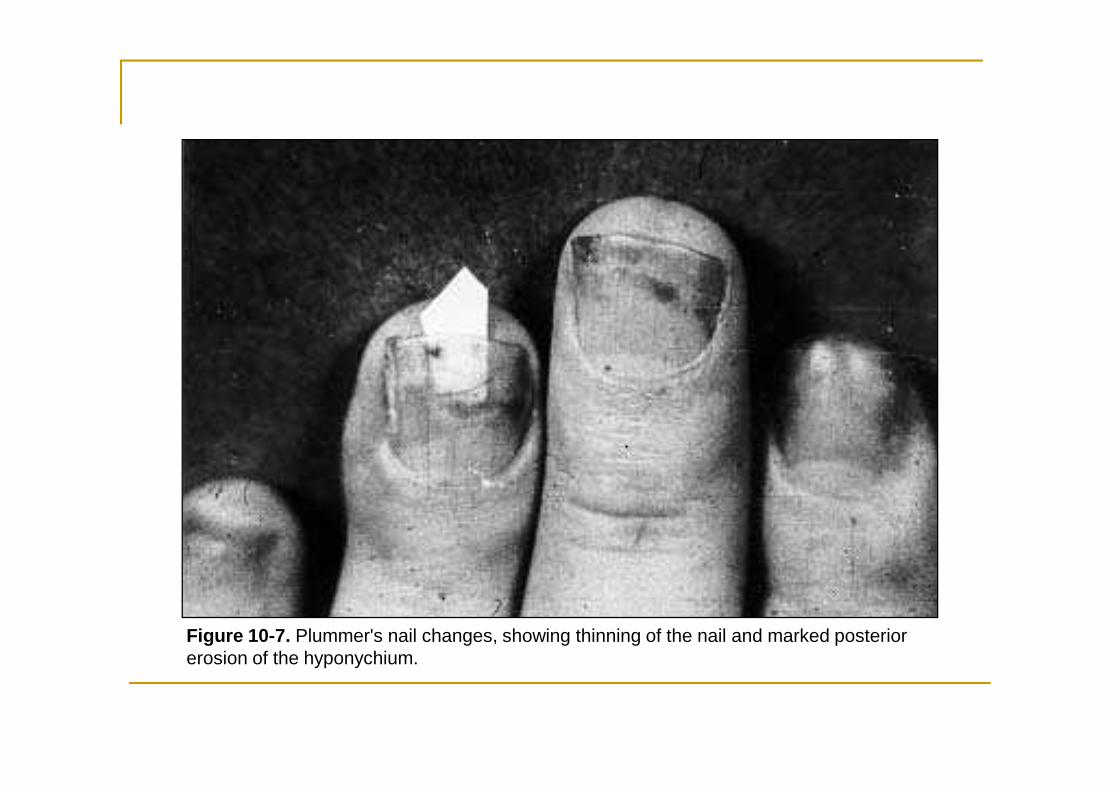
Figure 10-7. Plummer's nail changes, showing thinning of the nail and marked posterior erosion of the hyponychium.
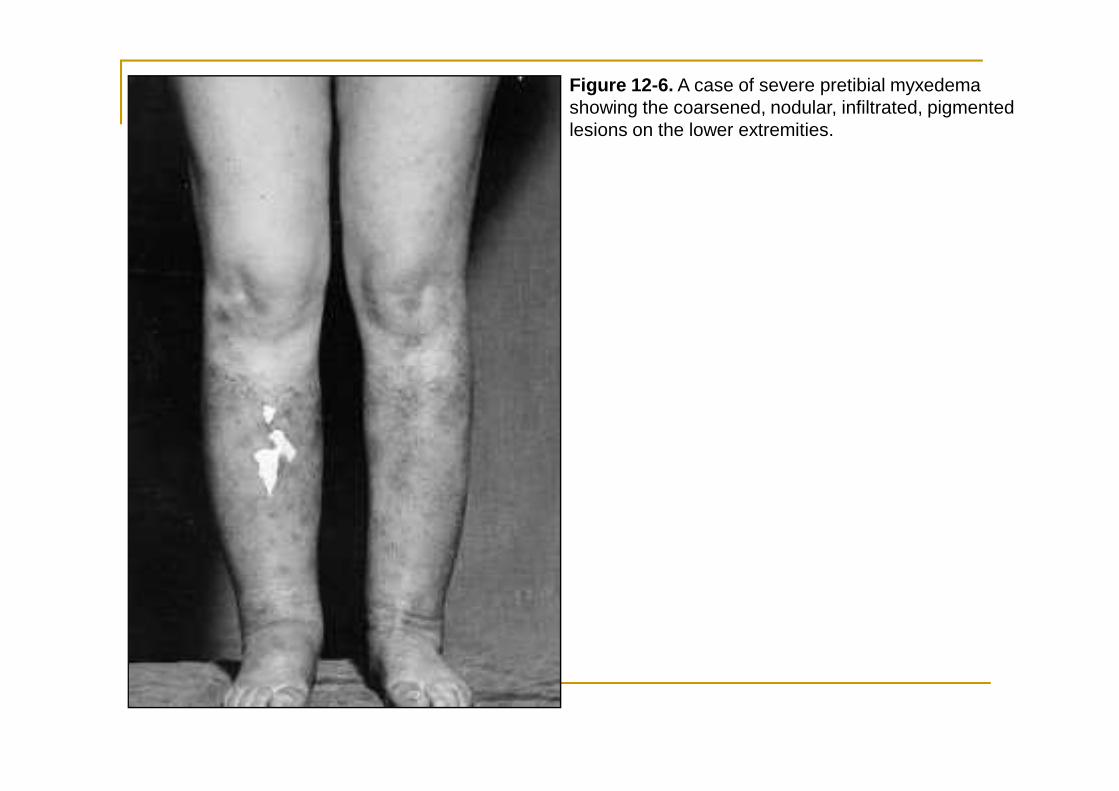
Figure 12-6. A case of severe pretibial myxedema showing the coarsened, nodular, infiltrated, pigmented lesions on the lower extremities.
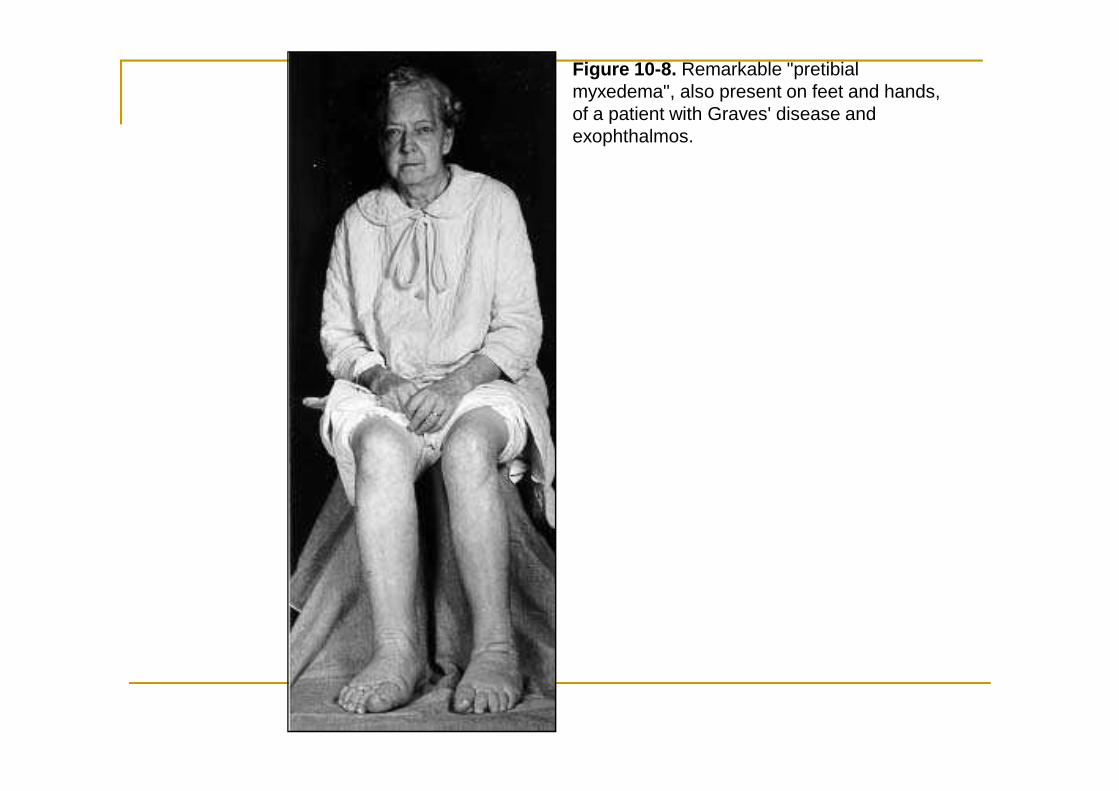
Figure 10-8. Remarkable "pretibial myxedema", also present on feet and hands, of a patient with Graves' disease and exophthalmos.
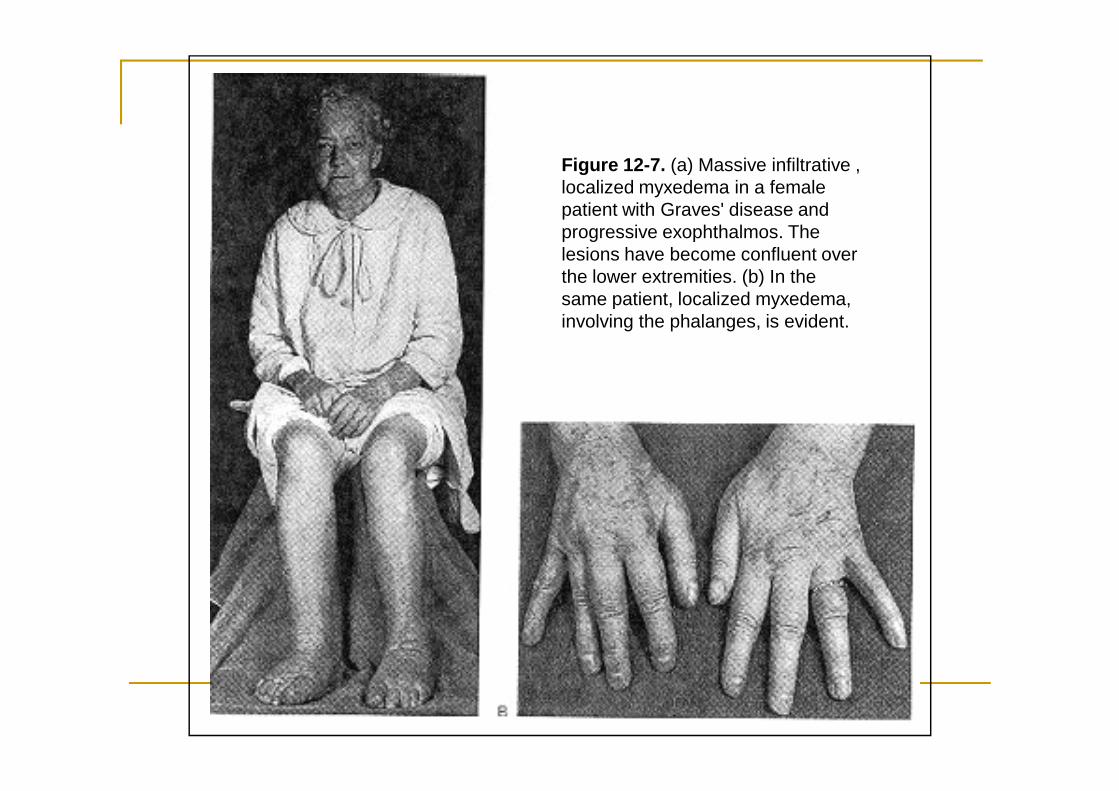
Figure 12-7. (a) Massive infiltrative , localized myxedema in a female patient with Graves' disease and progressive exophthalmos. The lesions have become confluent over the lower extremities. (b) In the same patient, localized myxedema, involving the phalanges, is evident.
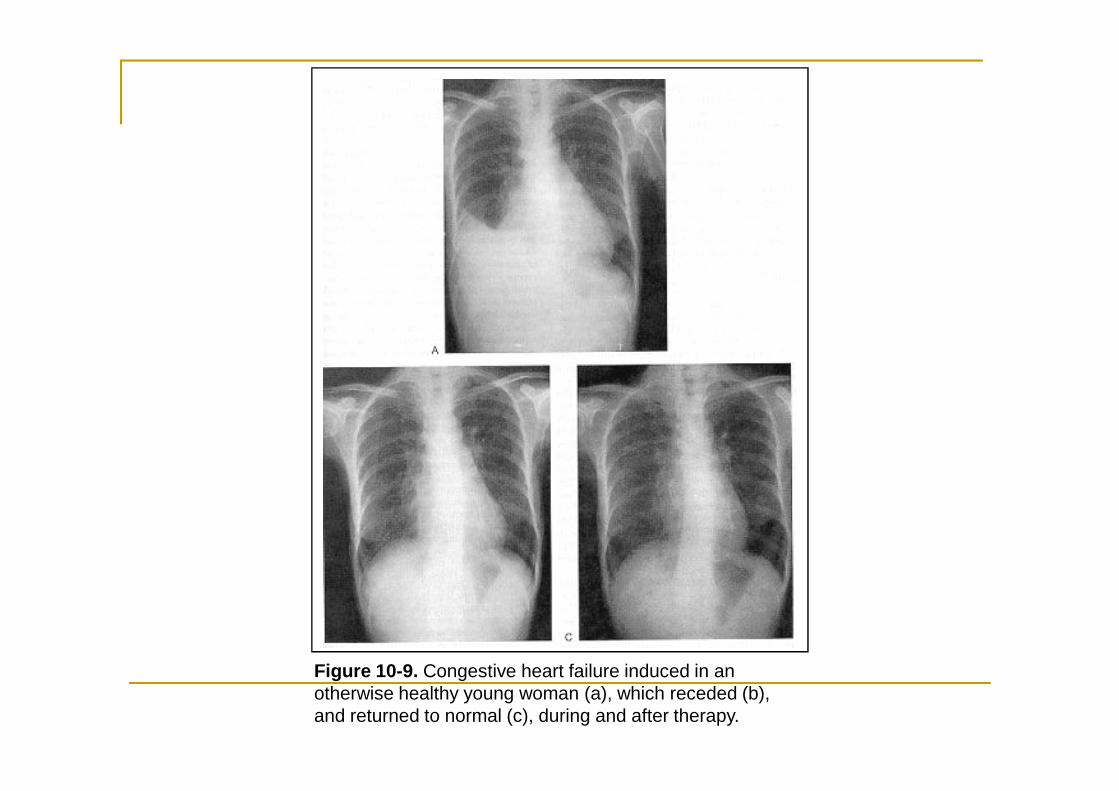
Figure 10-9. Congestive heart failure induced in an otherwise healthy young woman (a), which receded (b), and returned to normal (c), during and after therapy.
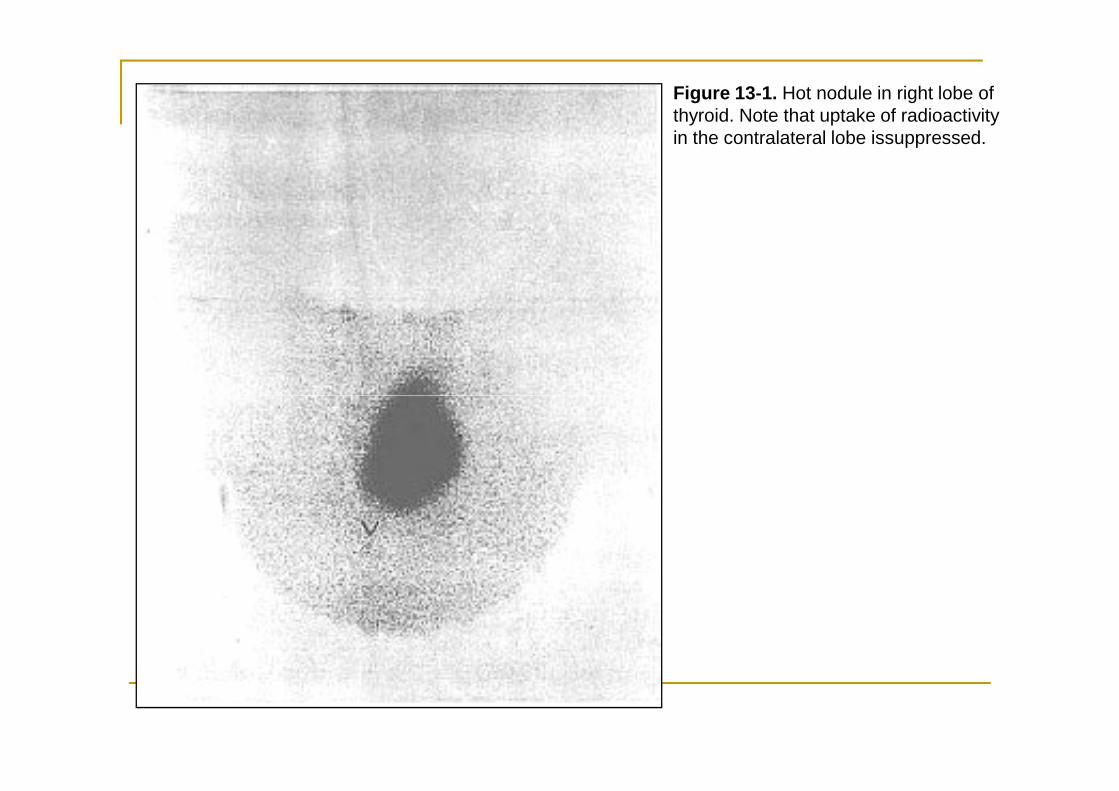
Figure 13-1. Hot nodule in right lobe of thyroid. Note that uptake of radioactivity in the contralateral lobe issuppressed.
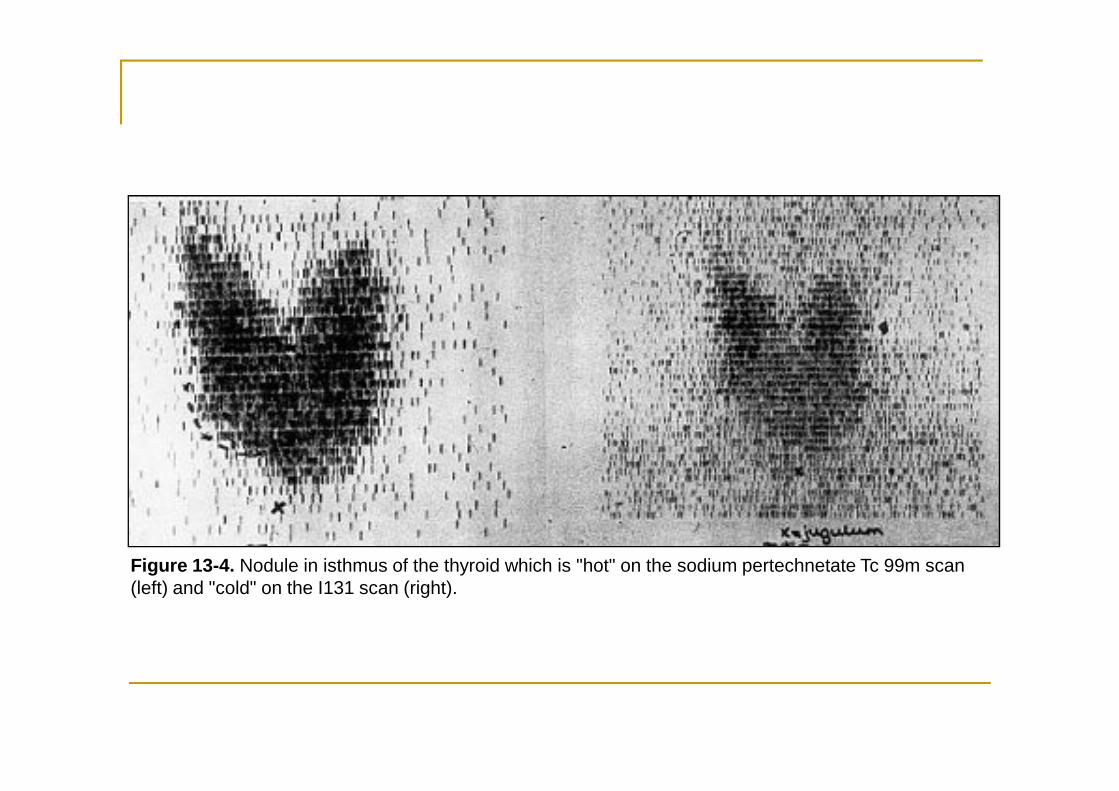
Figure 13-4. Nodule in isthmus of the thyroid which is "hot" on the sodium pertechnetate Tc 99m scan (left) and "cold" on the I131 scan (right).
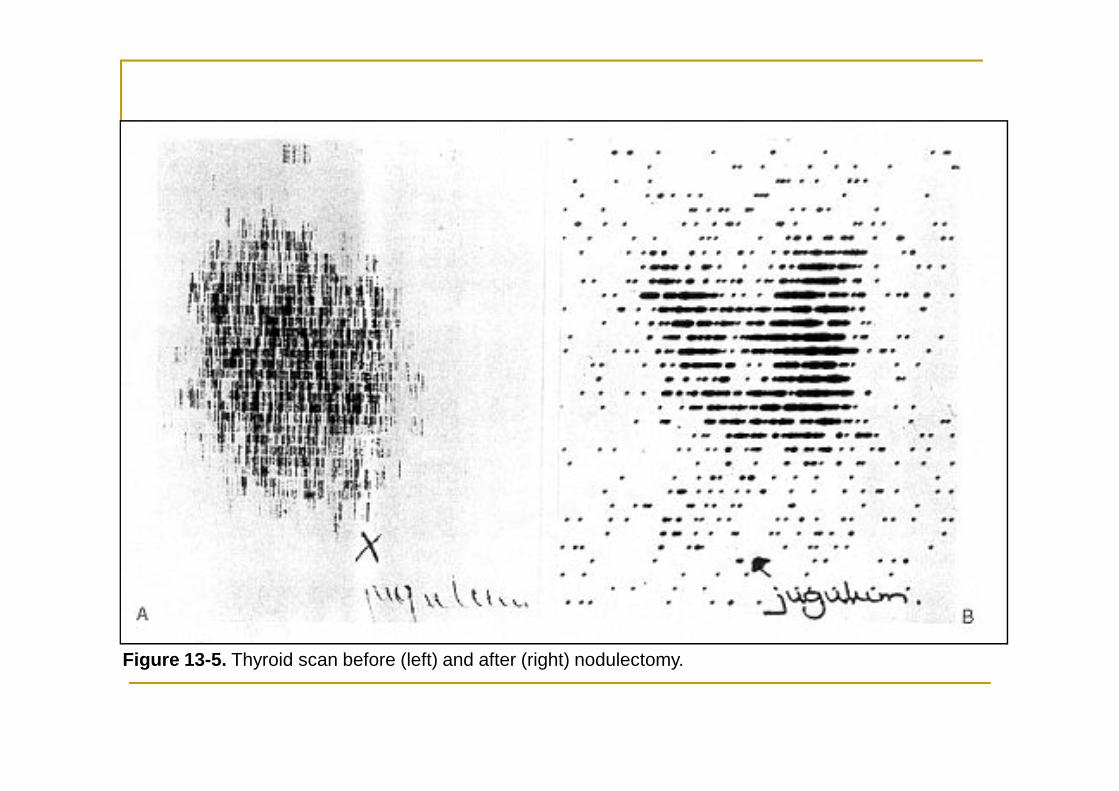
Figure 13-5. Thyroid scan before (left) and after (right) nodulectomy.
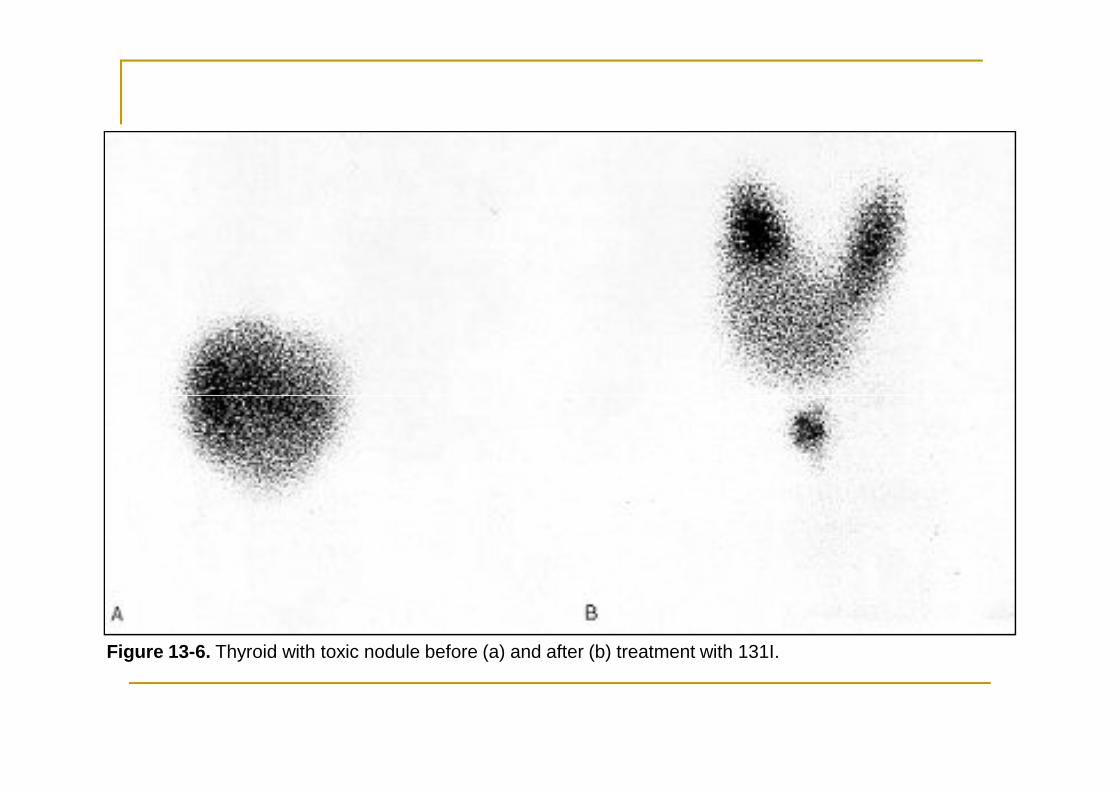
Figure 13-6. Thyroid with toxic nodule before (a) and after (b) treatment with 131I.
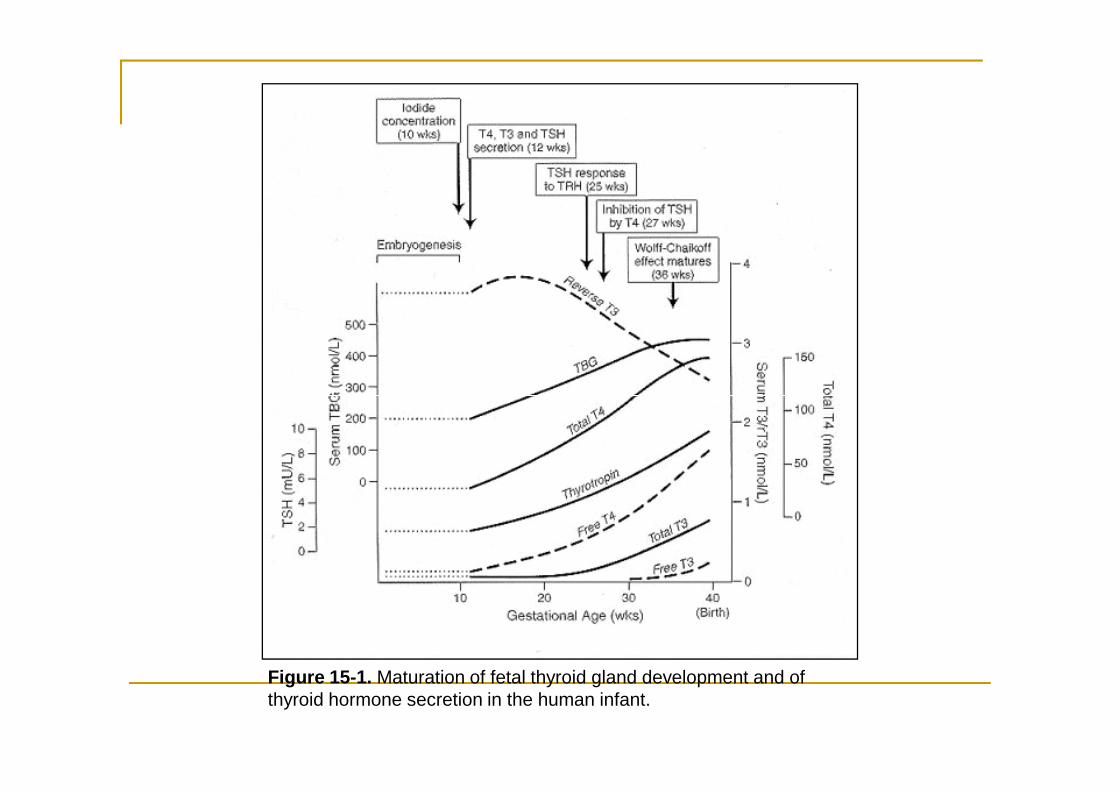
Figure 15-1. Maturation of fetal thyroid gland development and of thyroid hormone secretion in the human infant.
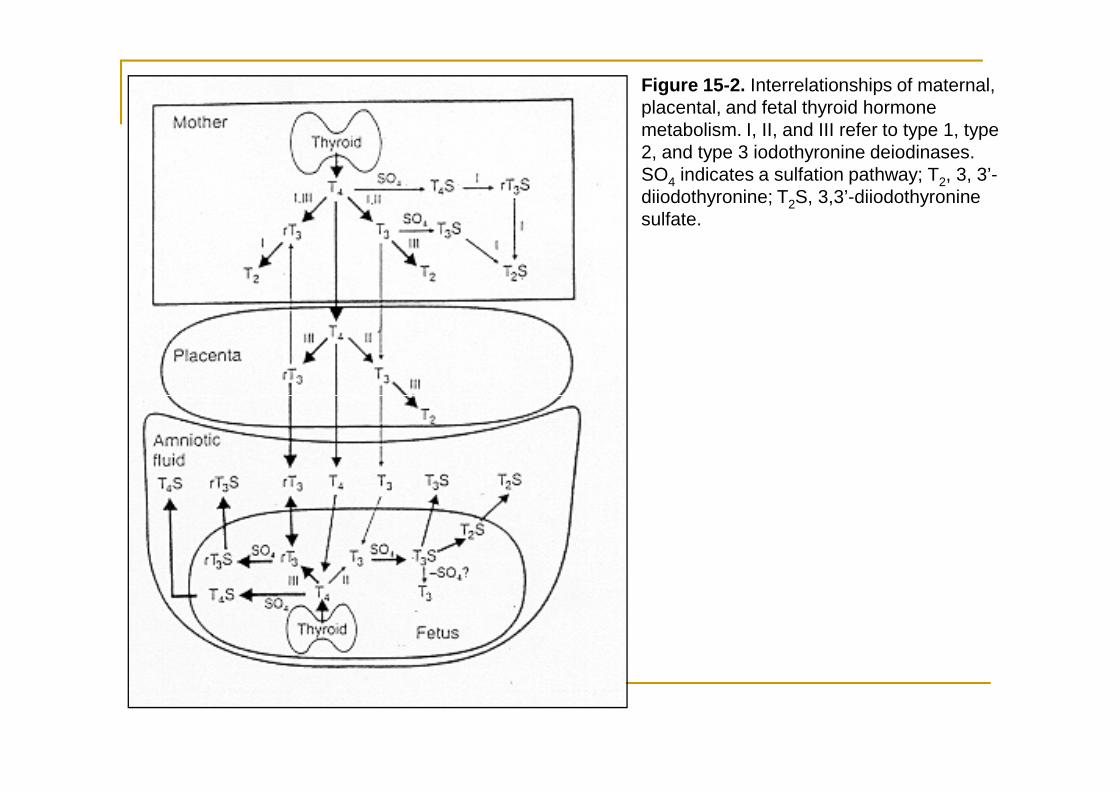
Figure 15-2. Interrelationships of maternal, placental, and fetal thyroid hormone metabolism. I, II, and III refer to type 1, type 2, and type 3 iodothyronine deiodinases. SO4 indicates a sulfation pathway; T2, 3, 3’-diiodothyronine; T2S, 3,3’-diiodothyronine sulfate.
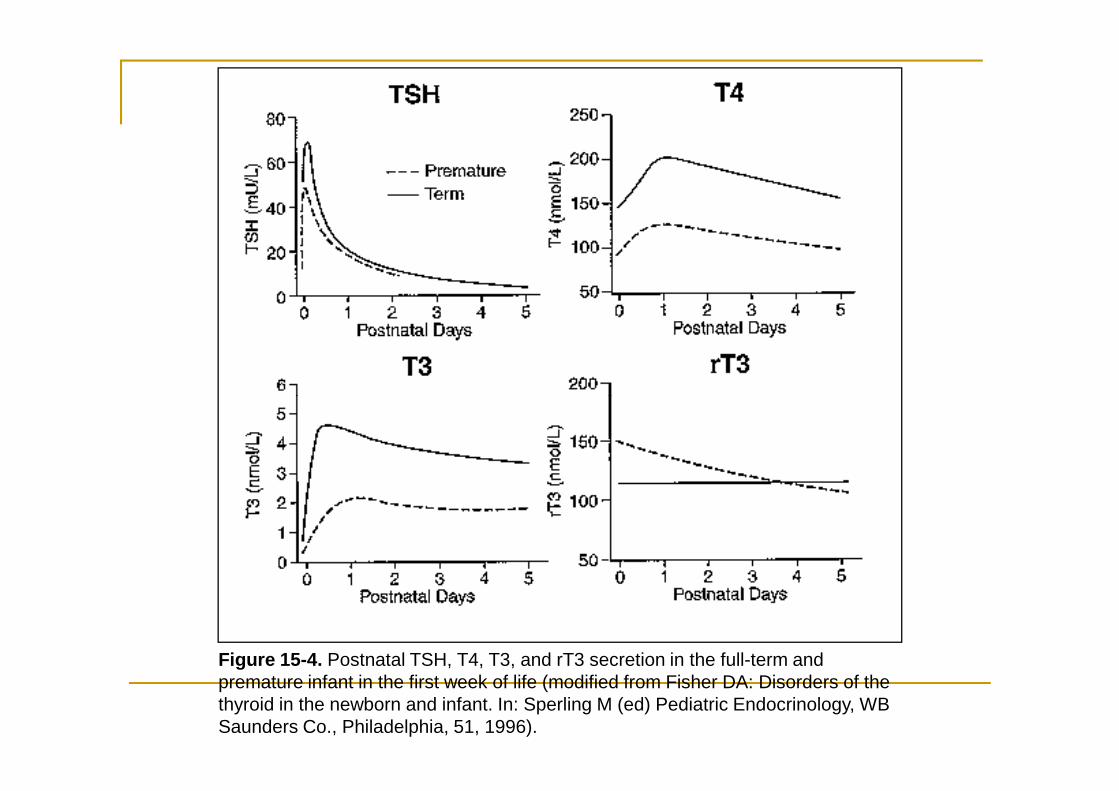
Figure 15-4. Postnatal TSH, T4, T3, and rT3 secretion in the full-term and premature infant in the first week of life (modified from Fisher DA: Disorders of the thyroid in the newborn and infant. In: Sperling M (ed) Pediatric Endocrinology, WB Saunders Co., Philadelphia, 51, 1996).
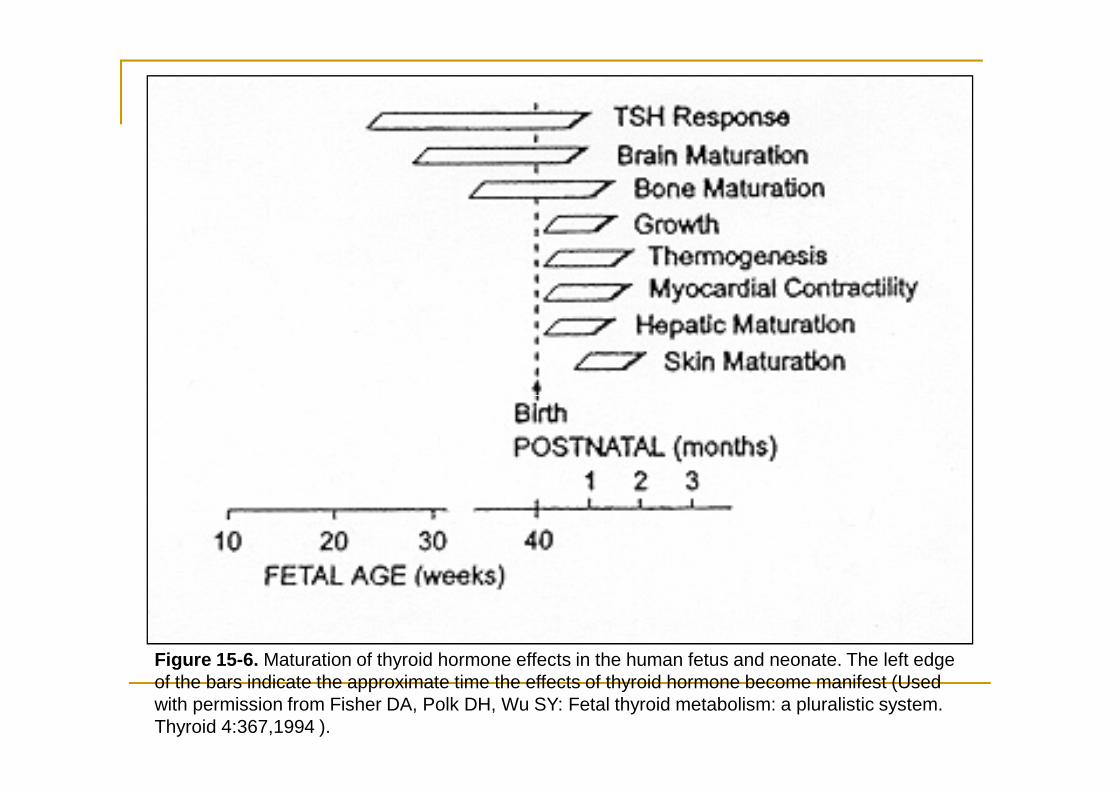
Figure 15-6. Maturation of thyroid hormone effects in the human fetus and neonate. The left edge of the bars indicate the approximate time the effects of thyroid hormone become manifest (Used with permission from Fisher DA, Polk DH, Wu SY: Fetal thyroid metabolism: a pluralistic system. Thyroid 4:367,1994 ).
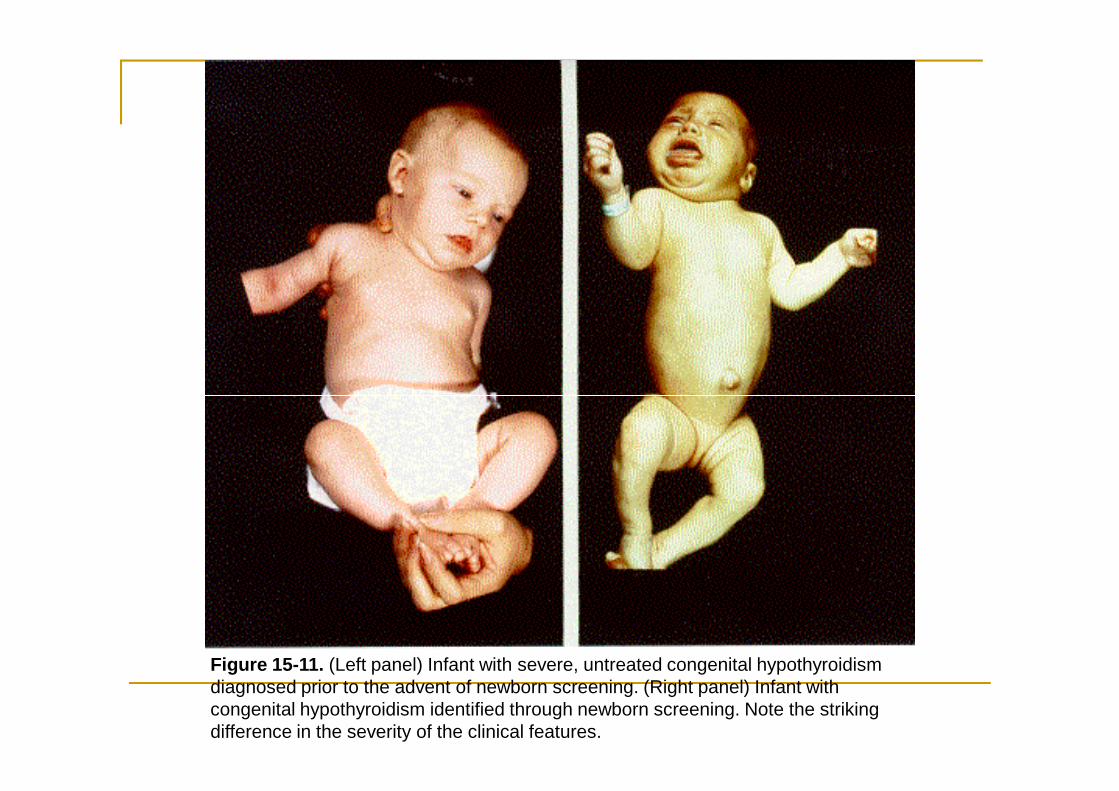
Figure 15-11. (Left panel) Infant with severe, untreated congenital hypothyroidism diagnosed prior to the advent of newborn screening. (Right panel) Infant with congenital hypothyroidism identified through newborn screening. Note the striking difference in the severity of the clinical features.
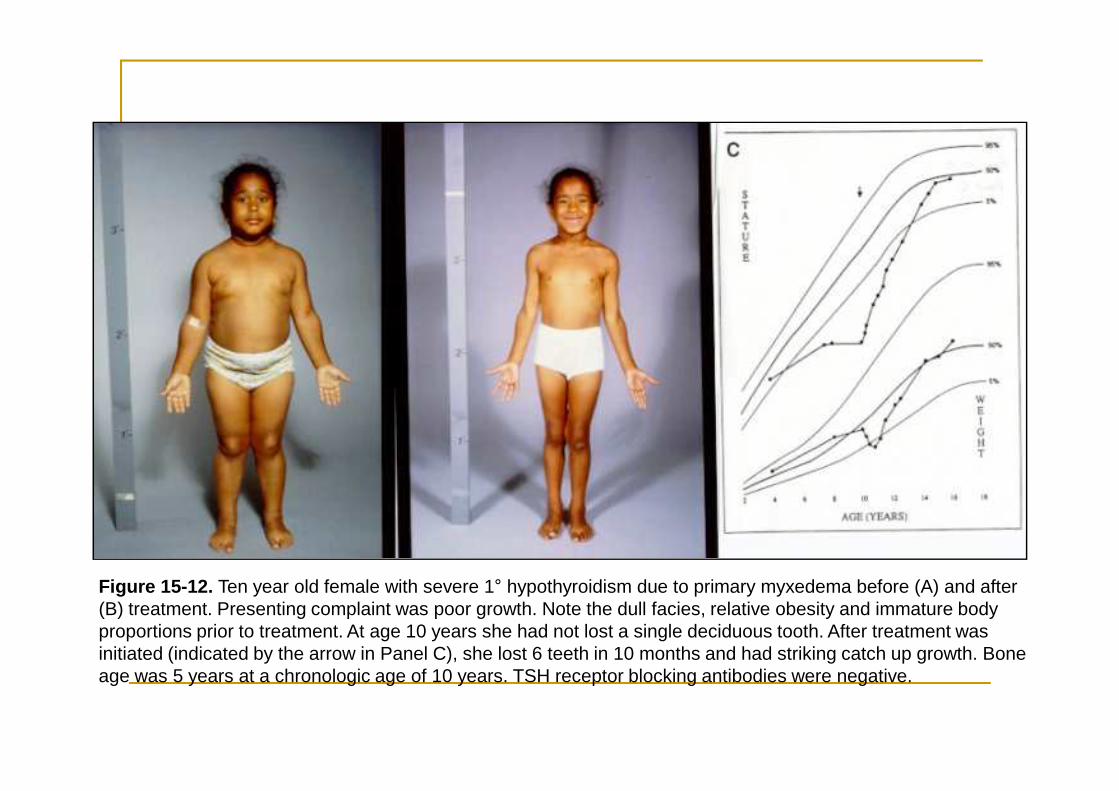
Figure 15-12. Ten year old female with severe 1° hypothyroidism due to primary myxedema before (A) and after (B) treatment. Presenting complaint was poor growth. Note the dull facies, relative obesity and immature body proportions prior to treatment. At age 10 years she had not lost a single deciduous tooth. After treatment was initiated (indicated by the arrow in Panel C), she lost 6 teeth in 10 months and had striking catch up growth. Bone age was 5 years at a chronologic age of 10 years. TSH receptor blocking antibodies were negative.
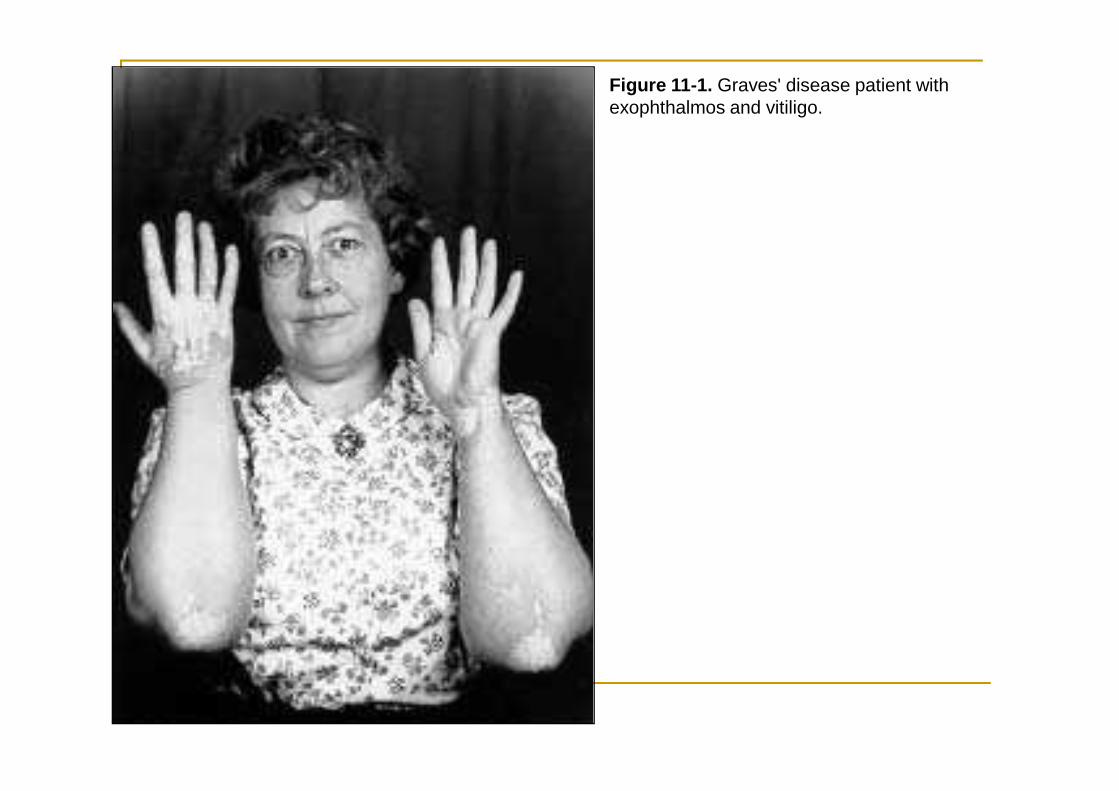
Figure 11-1. Graves' disease patient with exophthalmos and vitiligo.
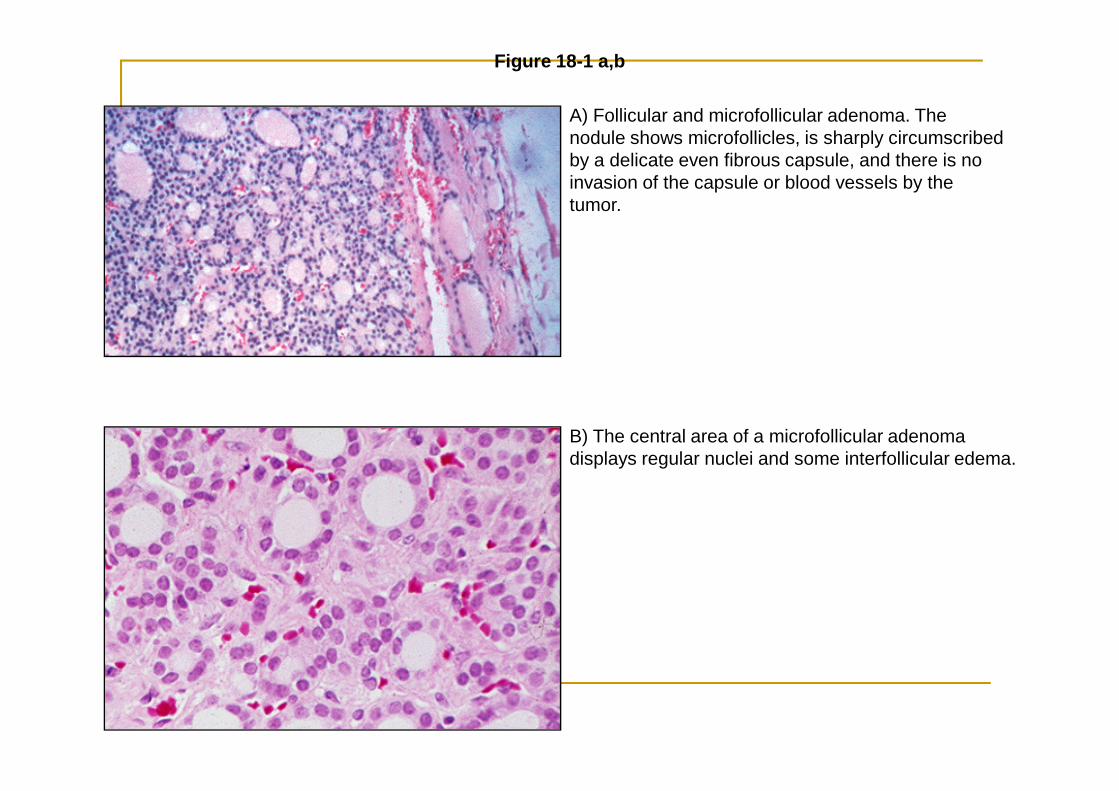
A) Follicular and microfollicular adenoma. The nodule shows microfollicles, is sharply circumscribed by a delicate even fibrous capsule, and there is no invasion of the capsule or blood vessels by the tumor.
Figure 18-1 a,b
B) The central area of a microfollicular adenoma displays regular nuclei and some interfollicular edema.
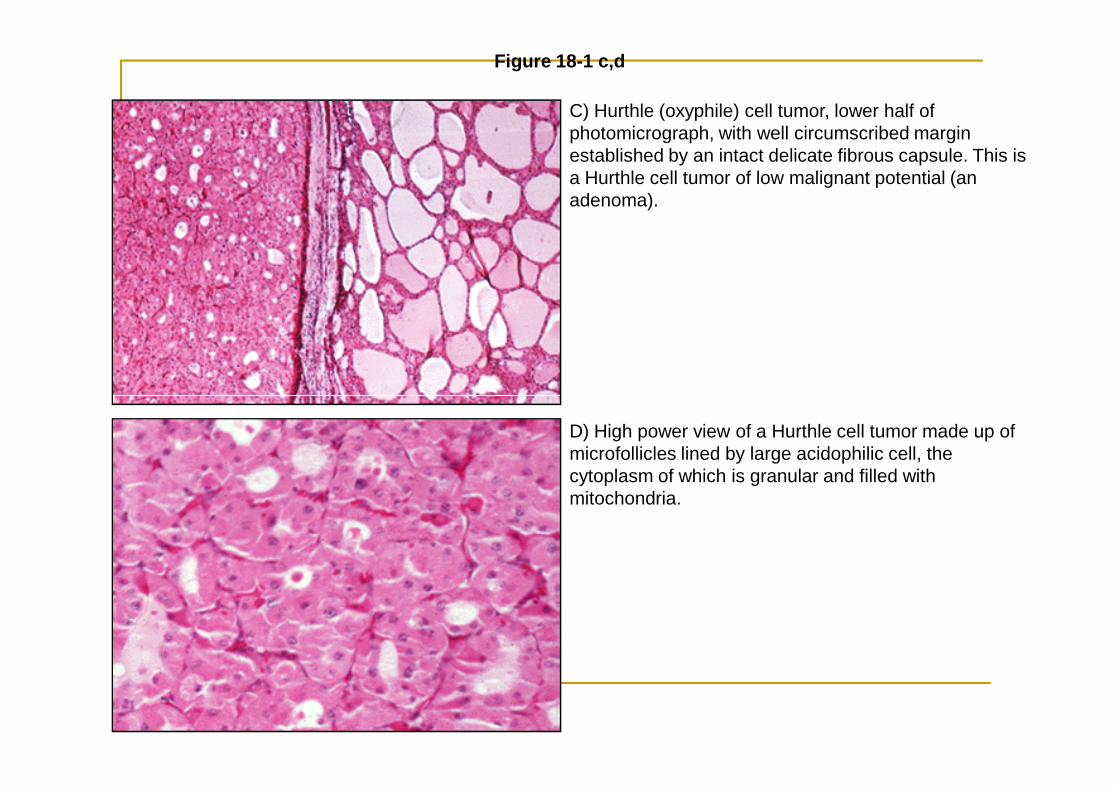
C) Hurthle (oxyphile) cell tumor, lower half of photomicrograph, with well circumscribed margin established by an intact delicate fibrous capsule. This is a Hurthle cell tumor of low malignant potential (an adenoma).
Figure 18-1 c,d
D) High power view of a Hurthle cell tumor made up of microfollicles lined by large acidophilic cell, the cytoplasm of which is granular and filled with mitochondria.
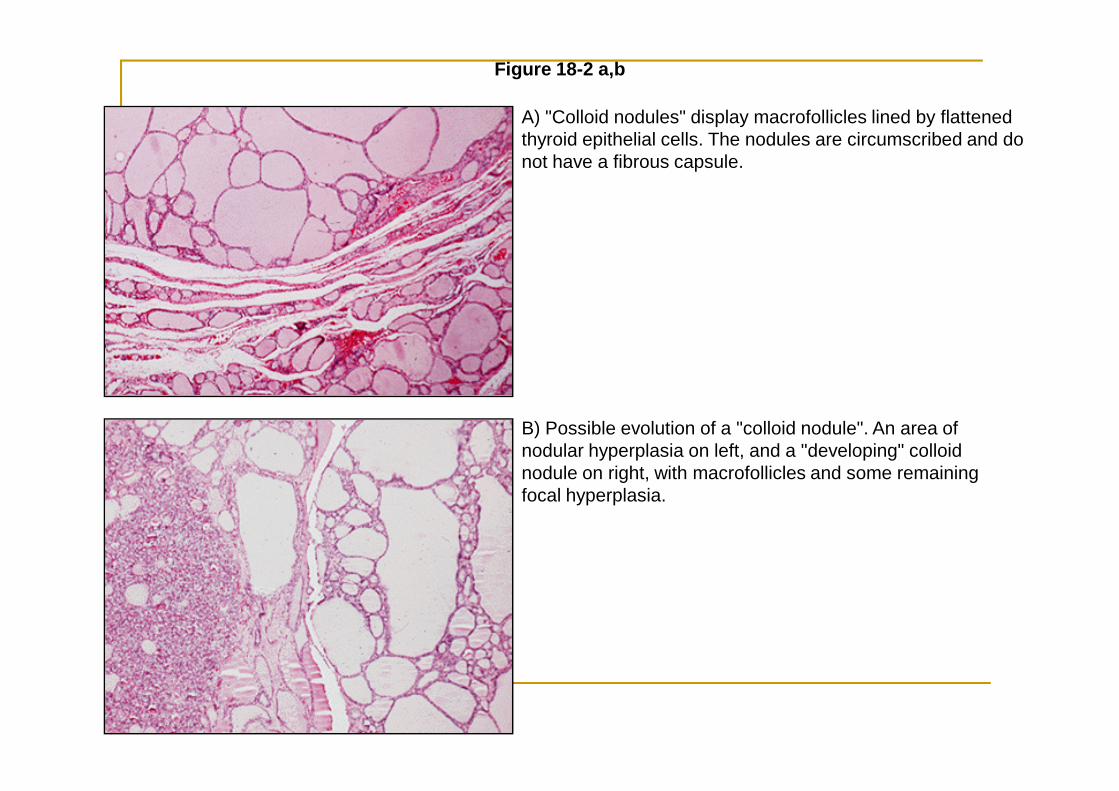
A) "Colloid nodules" display macrofollicles lined by flattened thyroid epithelial cells. The nodules are circumscribed and do not have a fibrous capsule.
Figure 18-2 a,b
B) Possible evolution of a "colloid nodule". An area of nodular hyperplasia on left, and a "developing" colloid nodule on right, with macrofollicles and some remaining focal hyperplasia.
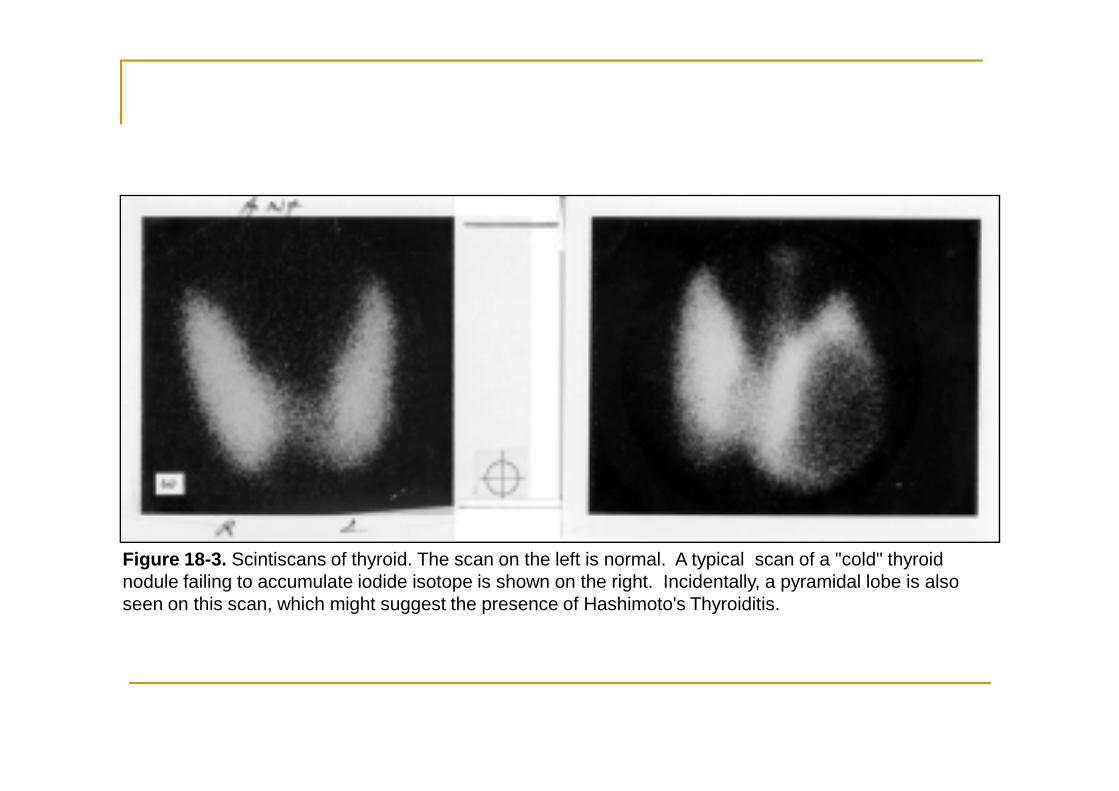
Figure 18-3. Scintiscans of thyroid. The scan on the left is normal. A typical scan of a "cold" thyroid nodule failing to accumulate iodide isotope is shown on the right. Incidentally, a pyramidal lobe is also seen on this scan, which might suggest the presence of Hashimoto's Thyroiditis.
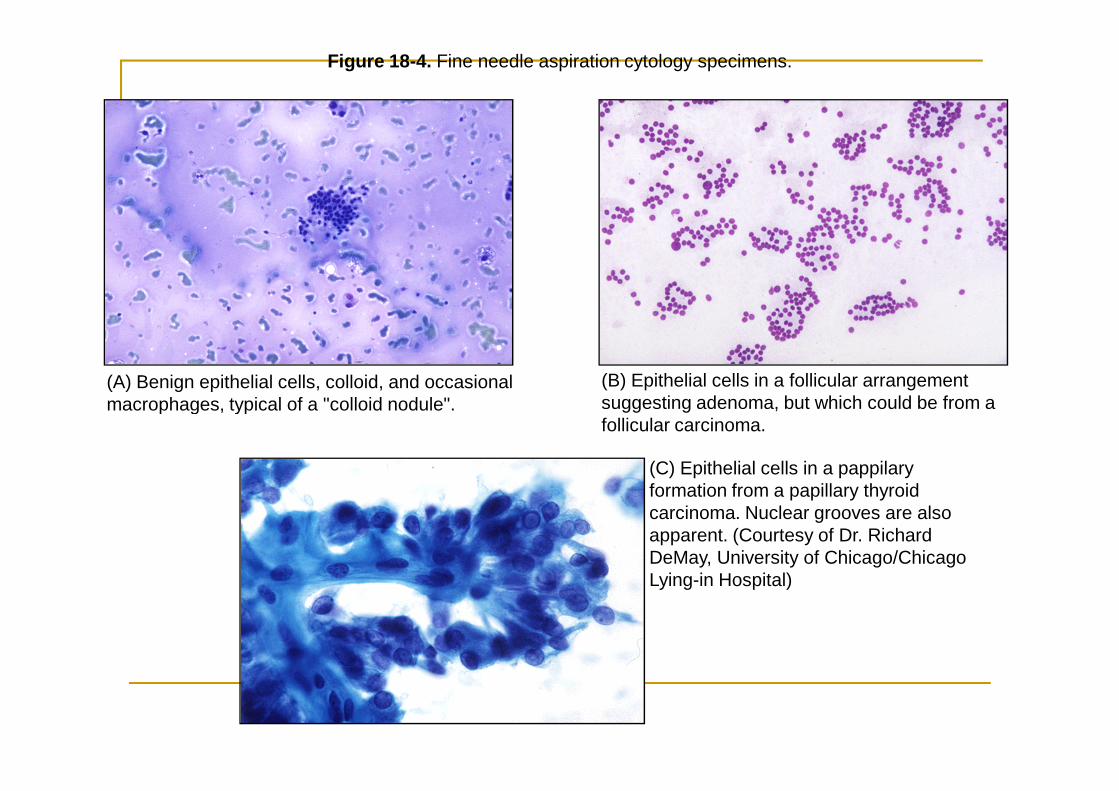
Figure 18-4. Fine needle aspiration cytology specimens.
(A) Benign epithelial cells, colloid, and occasional macrophages, typical of a "colloid nodule".
(B) Epithelial cells in a follicular arrangement suggesting adenoma, but which could be from a macrophages, typical of a "colloid nodule". suggesting adenoma, but which could be from a follicular carcinoma.
(C) Epithelial cells in a pappilary formation from a papillary thyroid carcinoma. Nuclear grooves are also apparent. (Courtesy of Dr. Richard DeMay, University of Chicago/Chicago Lying-in Hospital)
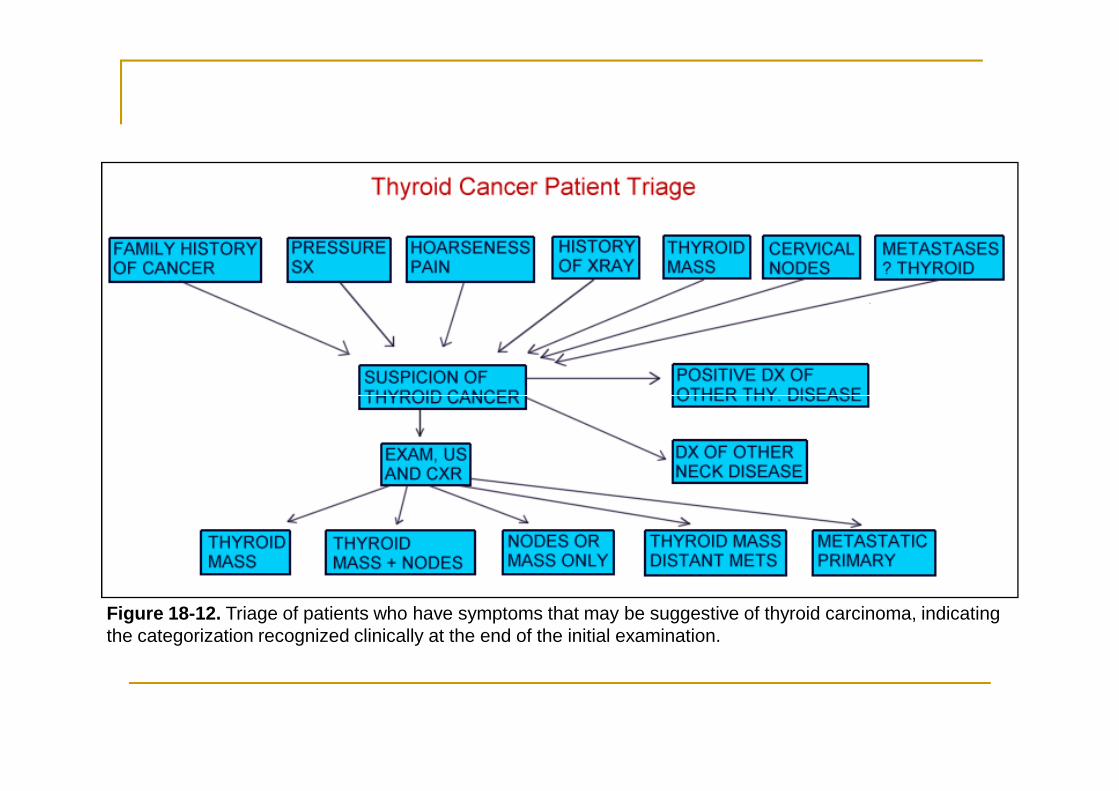
Figure 18-12. Triage of patients who have symptoms that may be suggestive of thyroid carcinoma, indicating the categorization recognized clinically at the end of the initial examination.
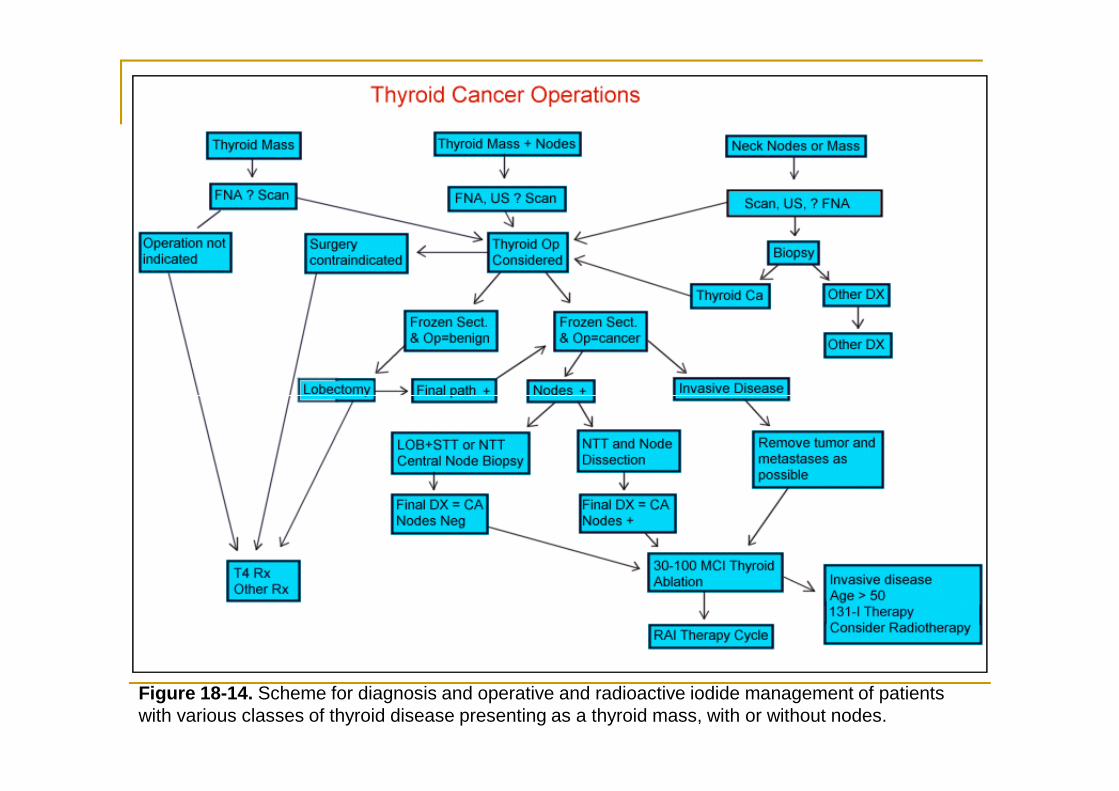
Figure 18-14. Scheme for diagnosis and operative and radioactive iodide management of patients with various classes of thyroid disease presenting as a thyroid mass, with or without nodes.
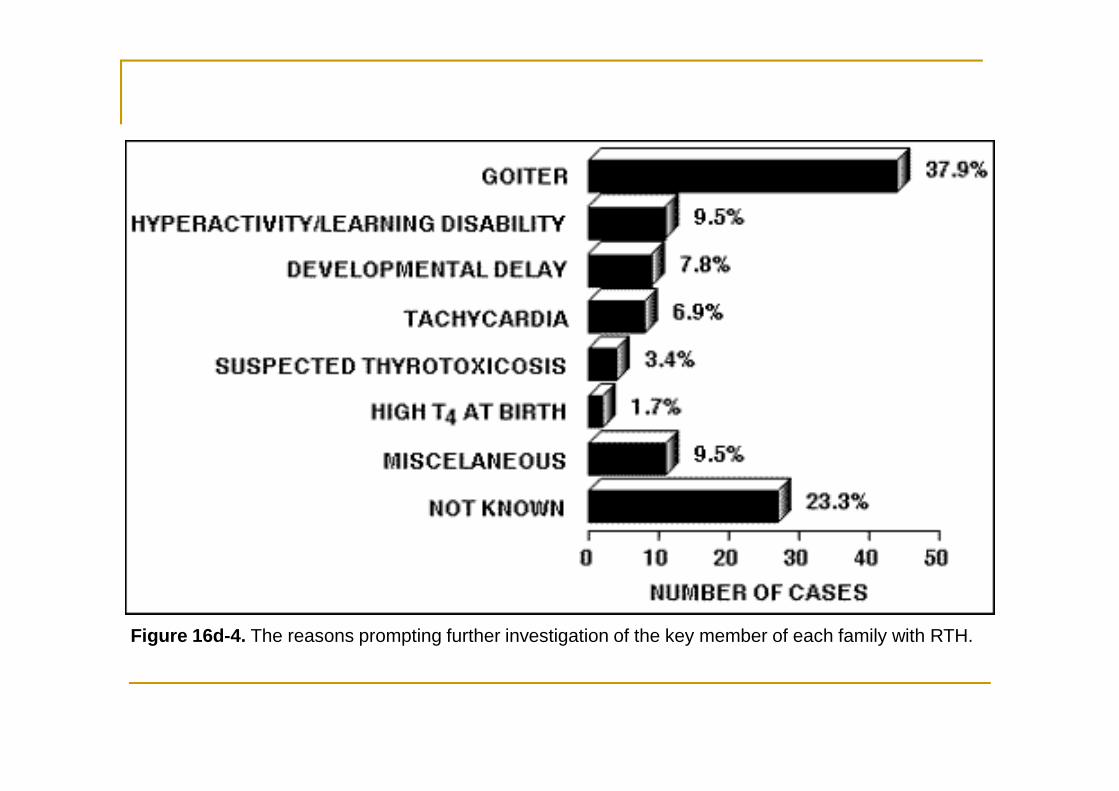
Figure 16d-4. The reasons prompting further investigation of the key member of each family with RTH.
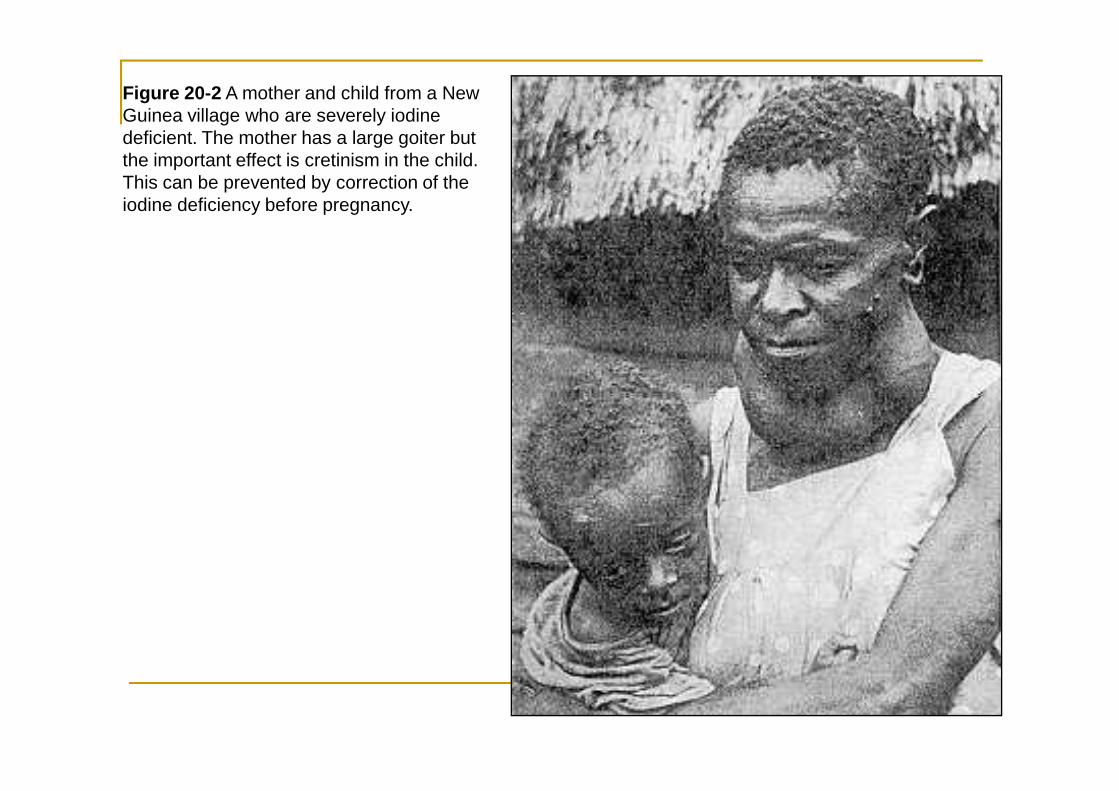
Figure 20-2 A mother and child from a New Guinea village who are severely iodine deficient. The mother has a large goiter but the important effect is cretinism in the child. This can be prevented by correction of the iodine deficiency before pregnancy.
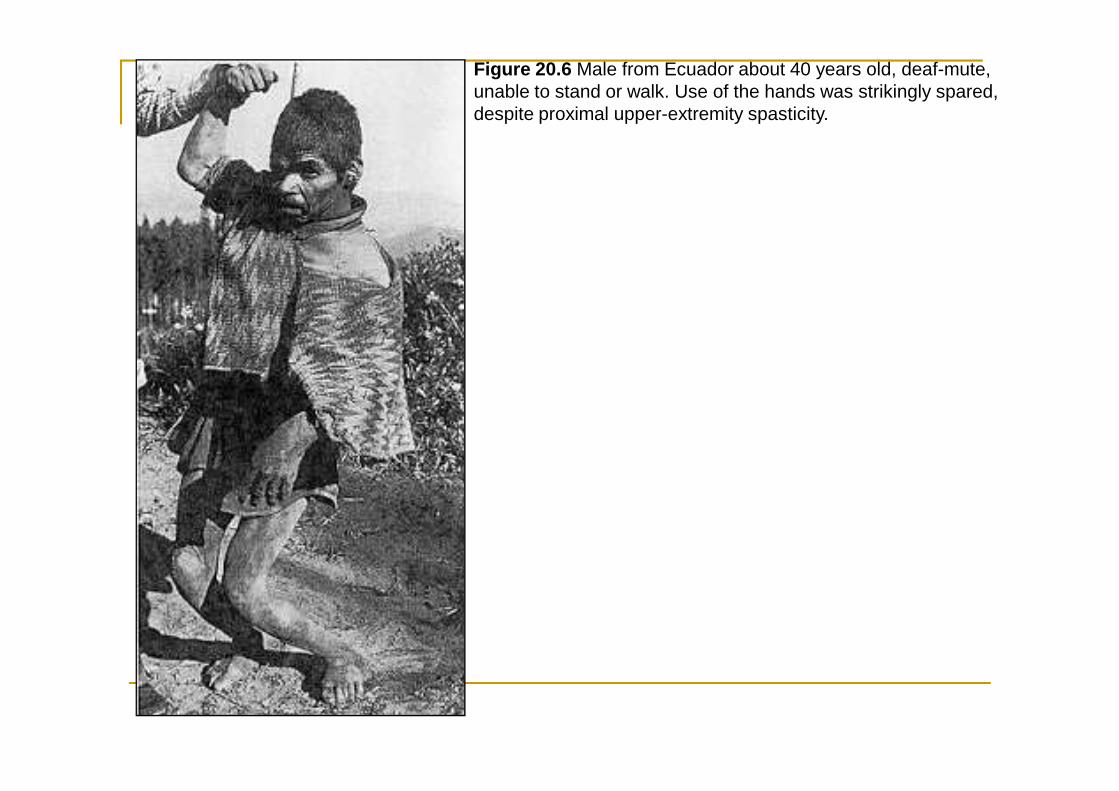
Figure 20.6 Male from Ecuador about 40 years old, deaf-mute, unable to stand or walk. Use of the hands was strikingly spared, despite proximal upper-extremity spasticity.
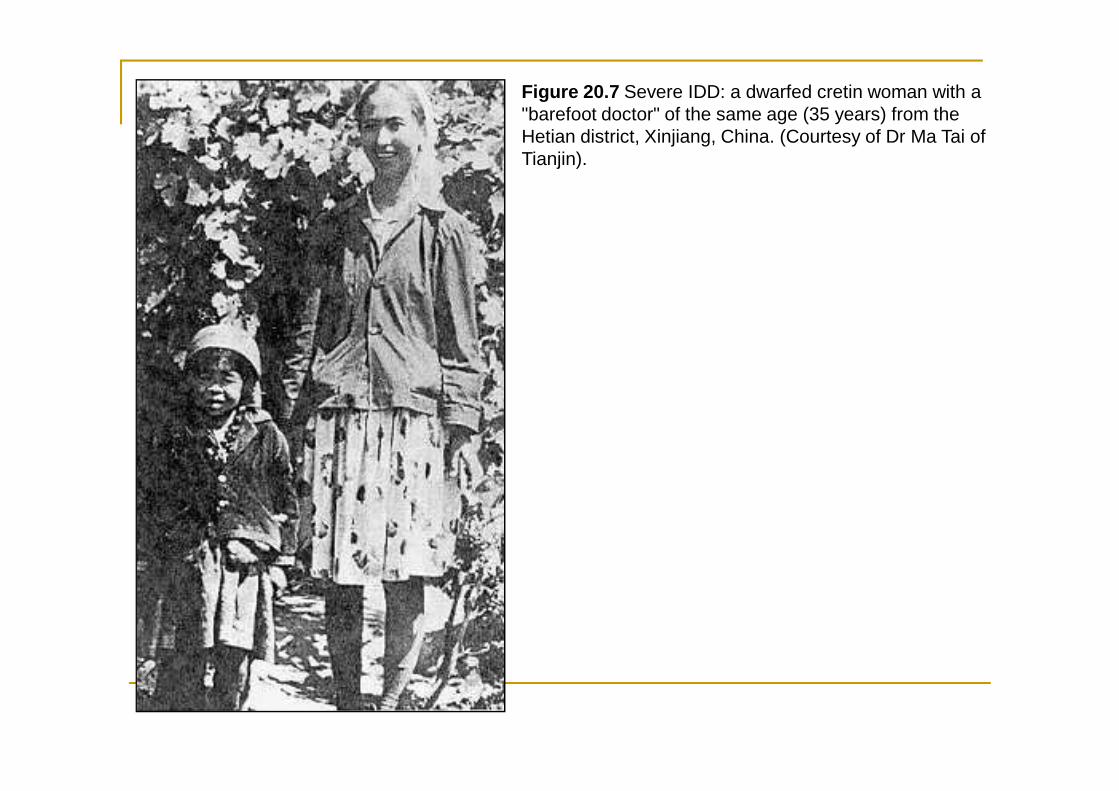
Figure 20.7 Severe IDD: a dwarfed cretin woman with a "barefoot doctor" of the same age (35 years) from the Hetian district, Xinjiang, China. (Courtesy of Dr Ma Tai of Tianjin).
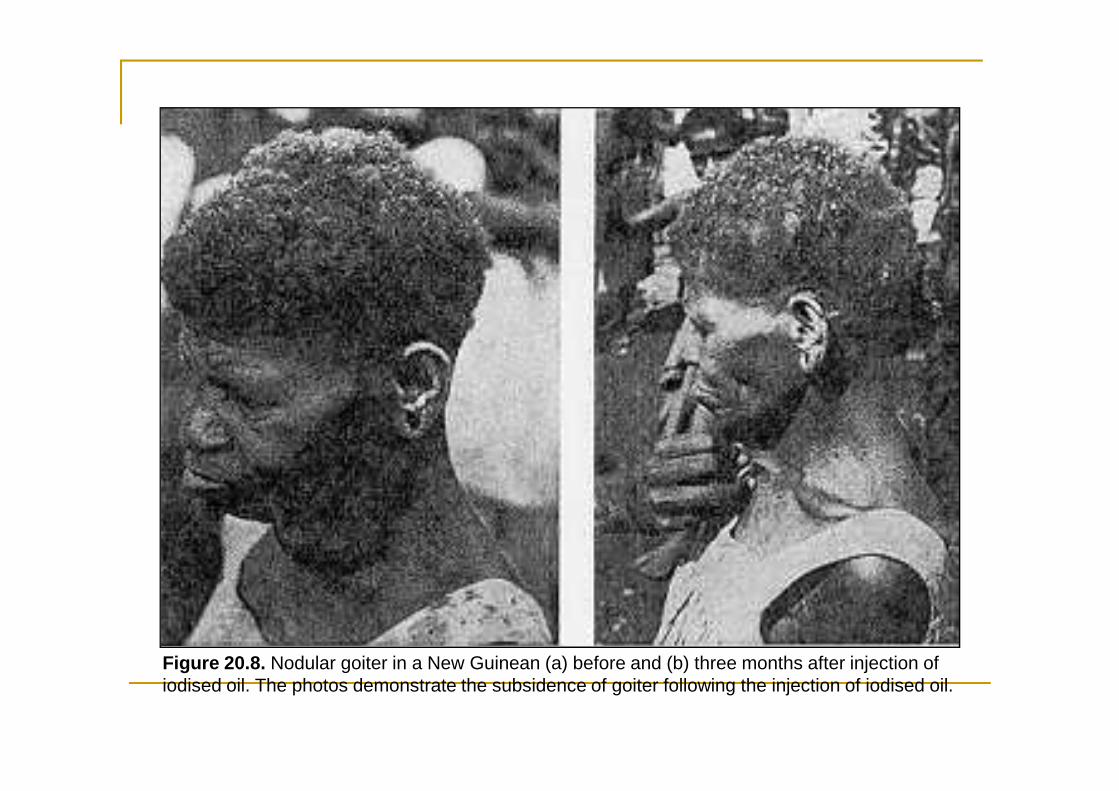
Figure 20.8. Nodular goiter in a New Guinean (a) before and (b) three months after injection of iodised oil. The photos demonstrate the subsidence of goiter following the injection of iodised oil.
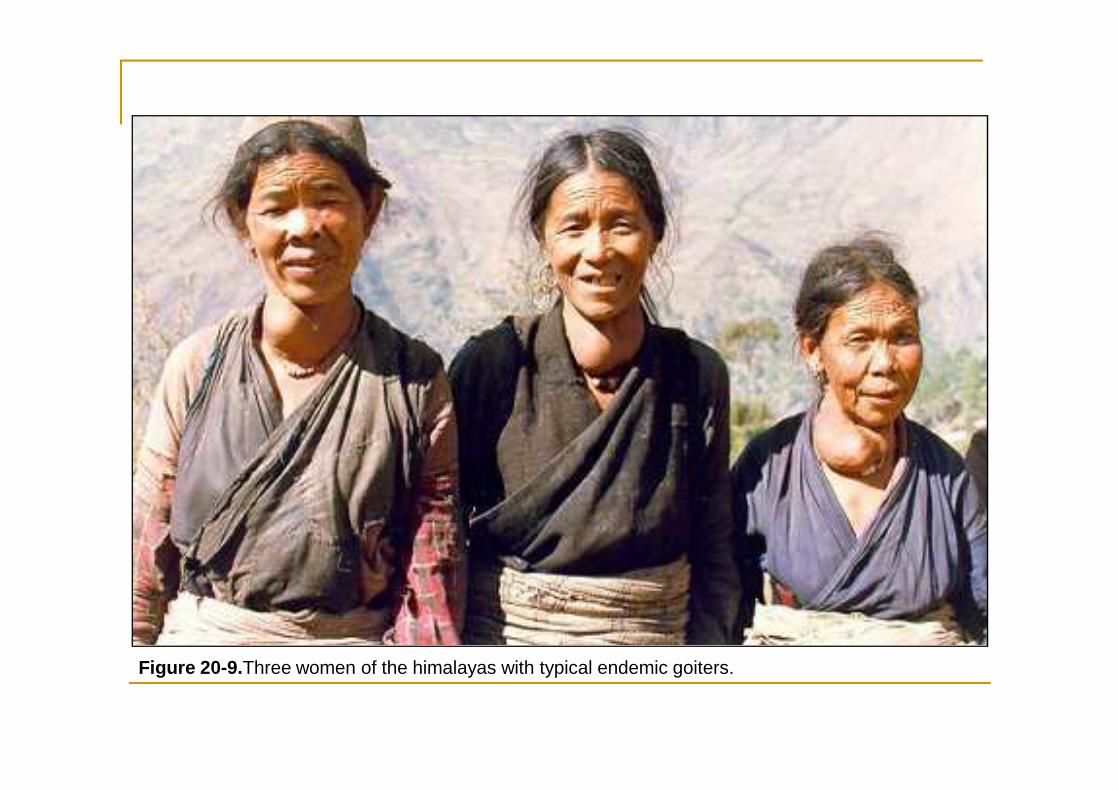
Figure 20-9.Three women of the himalayas with typical endemic goiters.
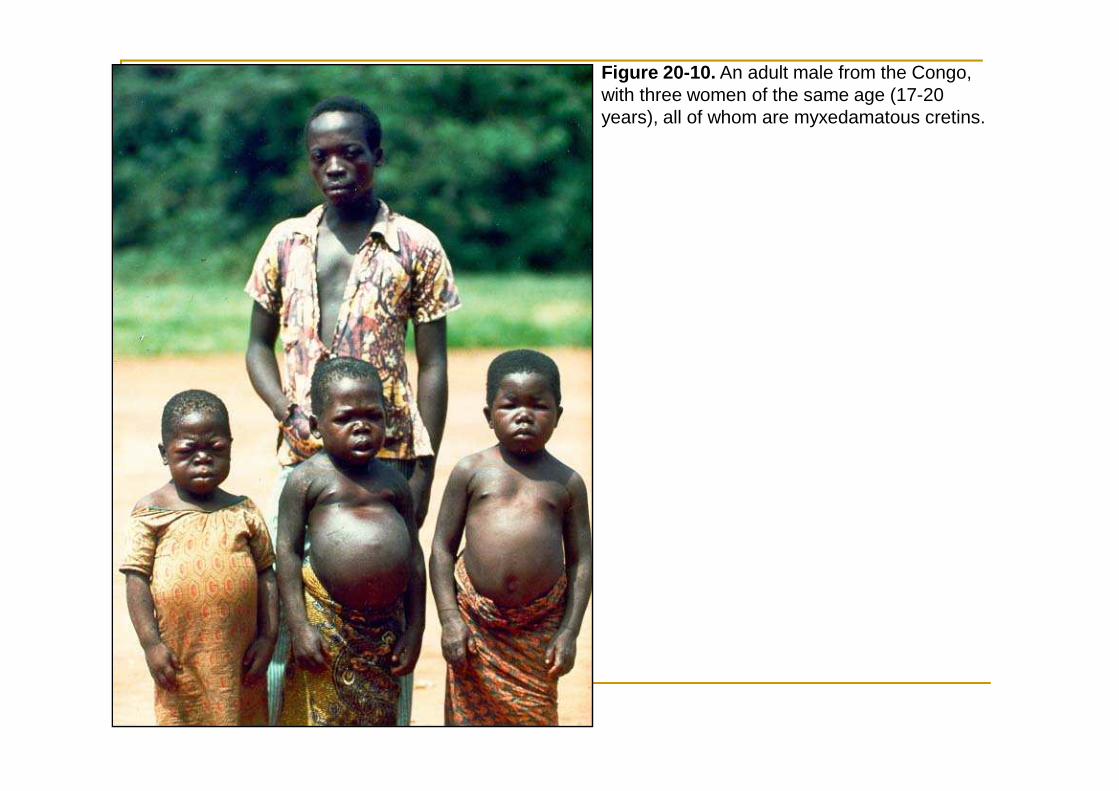
Figure 20-10. An adult male from the Congo, with three women of the same age (17-20 years), all of whom are myxedamatous cretins.
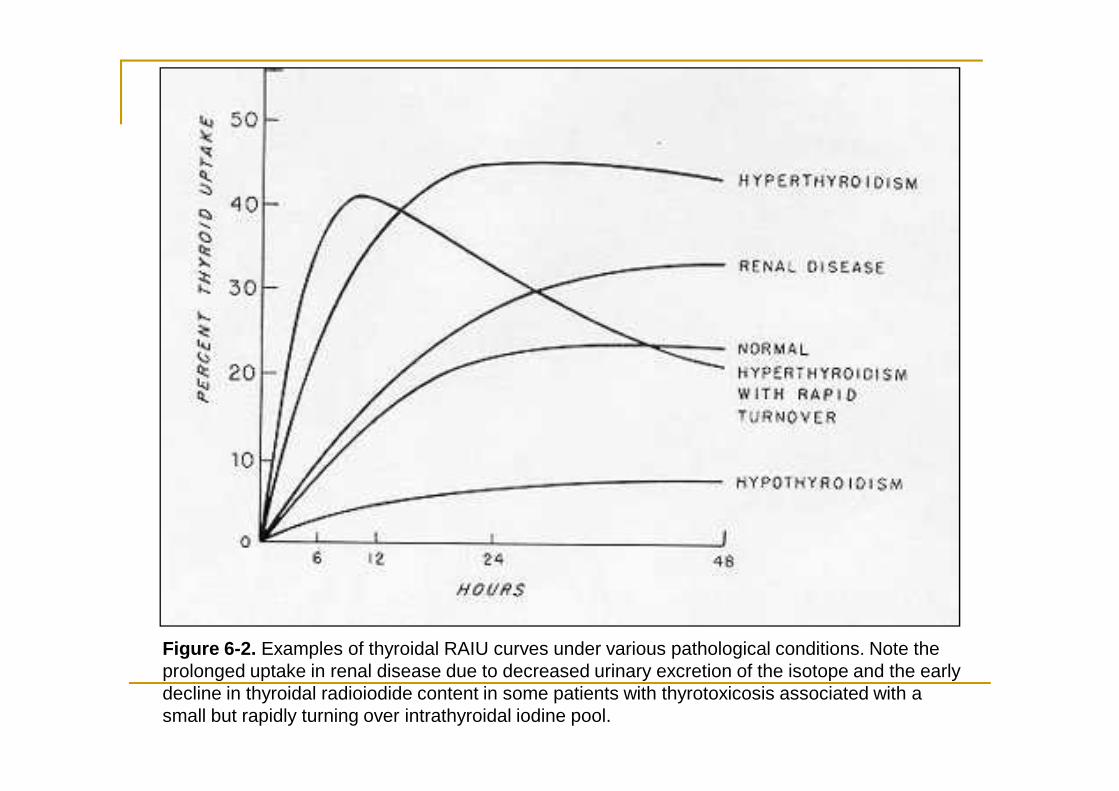
Figure 6-2. Examples of thyroidal RAIU curves under various pathological conditions. Note the prolonged uptake in renal disease due to decreased urinary excretion of the isotope and the early decline in thyroidal radioiodide content in some patients with thyrotoxicosis associated with a small but rapidly turning over intrathyroidal iodine pool.
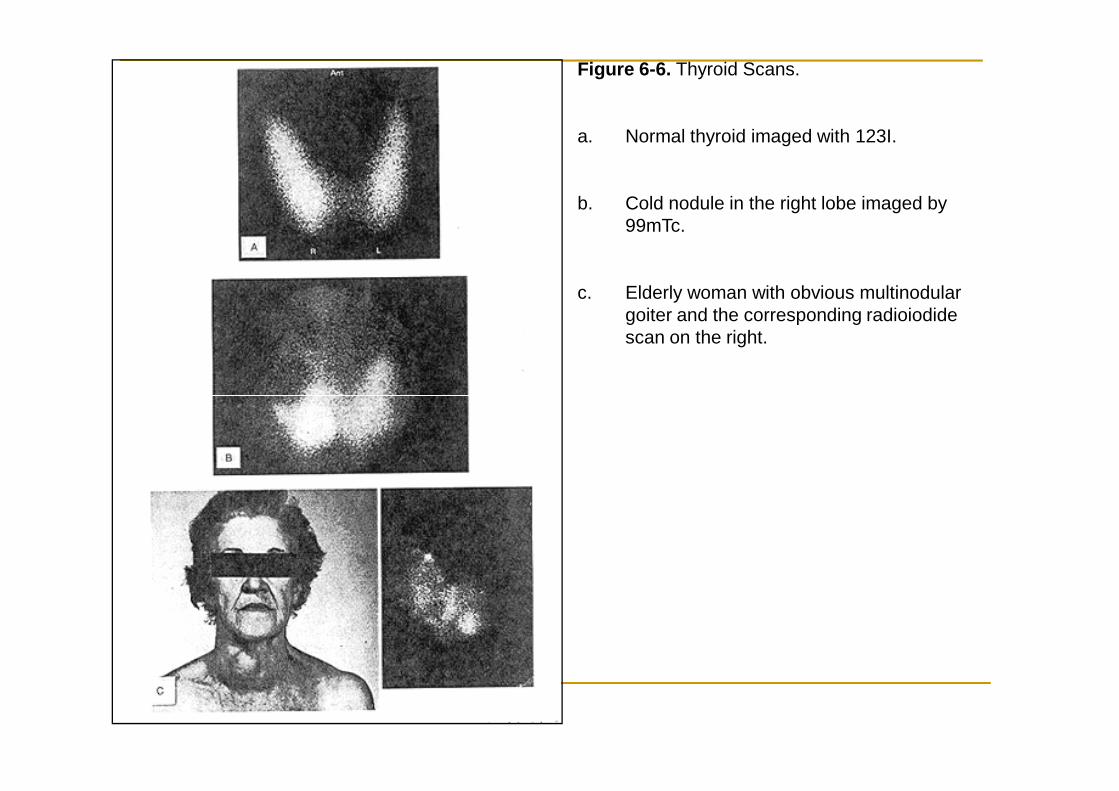
Figure 6-6. Thyroid Scans.
a. Normal thyroid imaged with 123I.
b. Cold nodule in the right lobe imaged by 99mTc.
c. Elderly woman with obvious multinodular goiter and the corresponding radioiodide scan on the right.
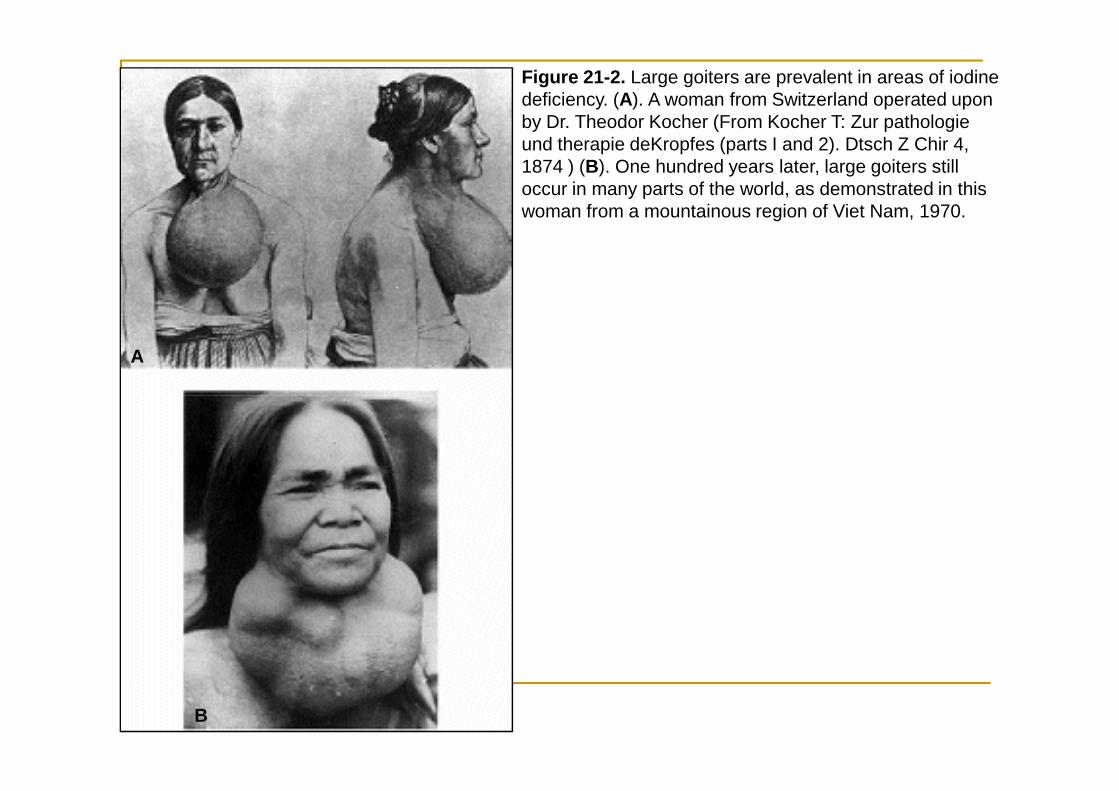
Figure 21-2. Large goiters are prevalent in areas of iodine deficiency. (A). A woman from Switzerland operated upon by Dr. Theodor Kocher (From Kocher T: Zur pathologie und therapie deKropfes (parts I and 2). Dtsch Z Chir 4, 1874 ) (B). One hundred years later, large goiters still occur in many parts of the world, as demonstrated in this woman from a mountainous region of Viet Nam, 1970.
A
B
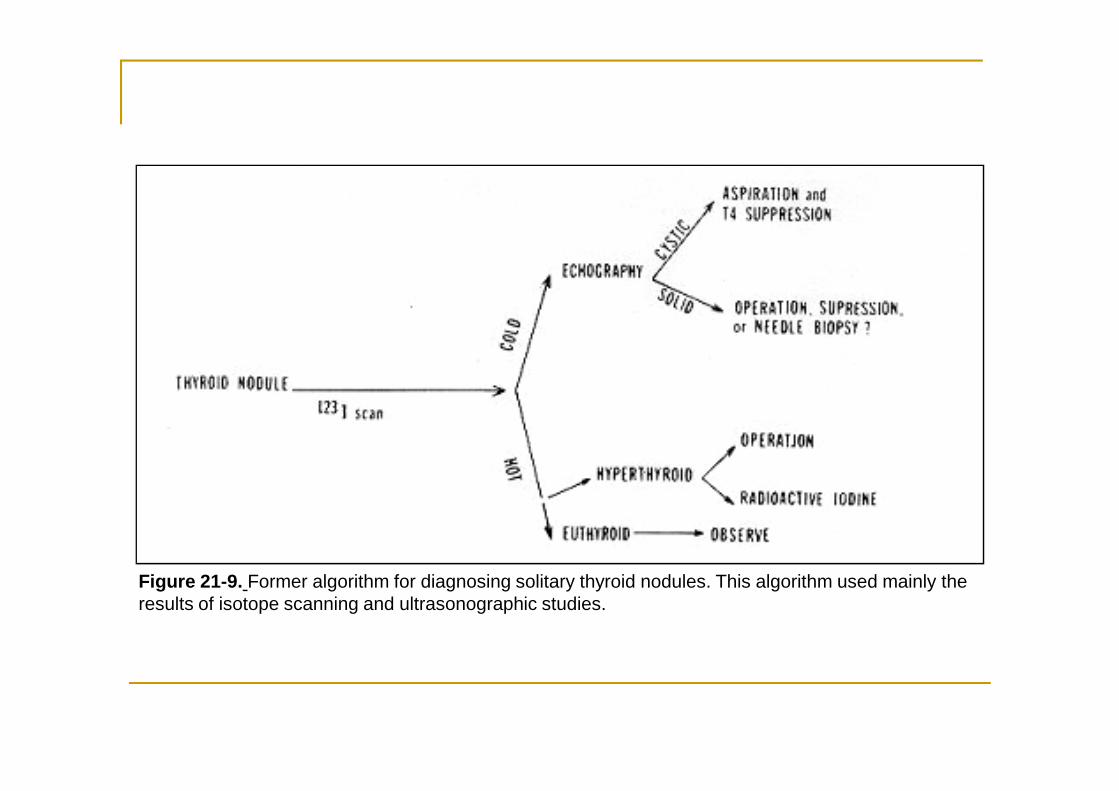
Figure 21-9. Former algorithm for diagnosing solitary thyroid nodules. This algorithm used mainly the results of isotope scanning and ultrasonographic studies.
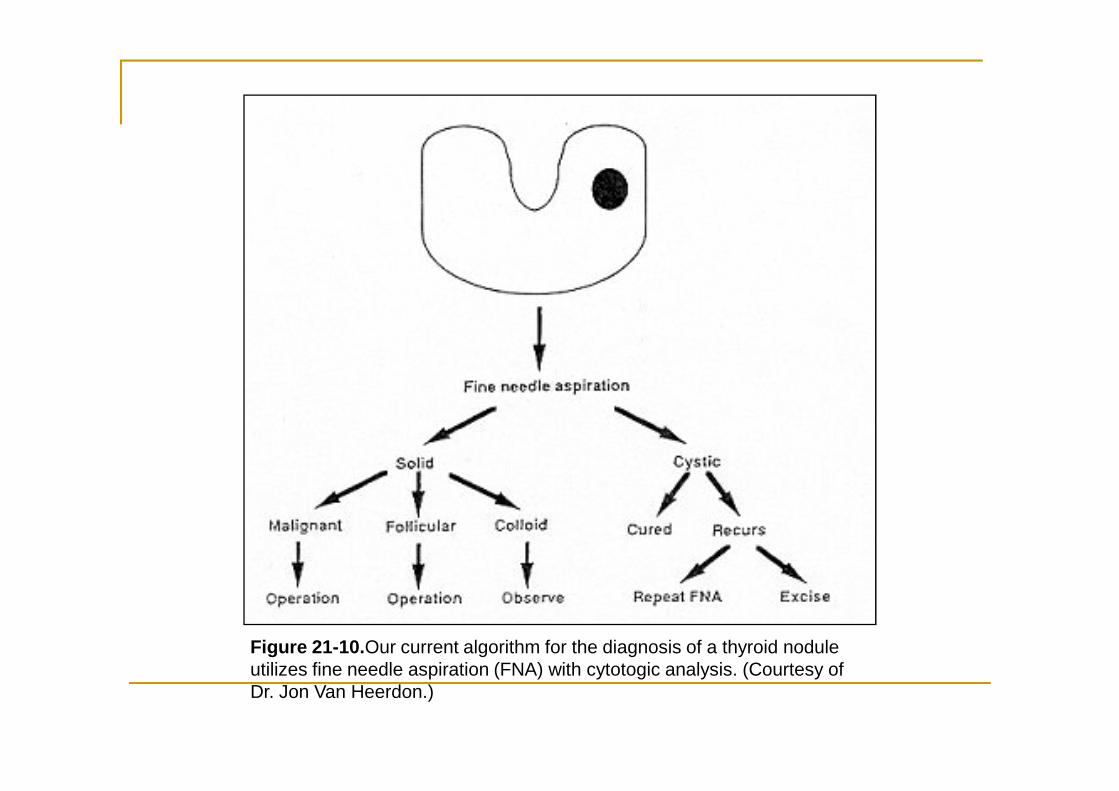
Figure 21-10.Our current algorithm for the diagnosis of a thyroid nodule utilizes fine needle aspiration (FNA) with cytotogic analysis. (Courtesy of Dr. Jon Van Heerdon.)
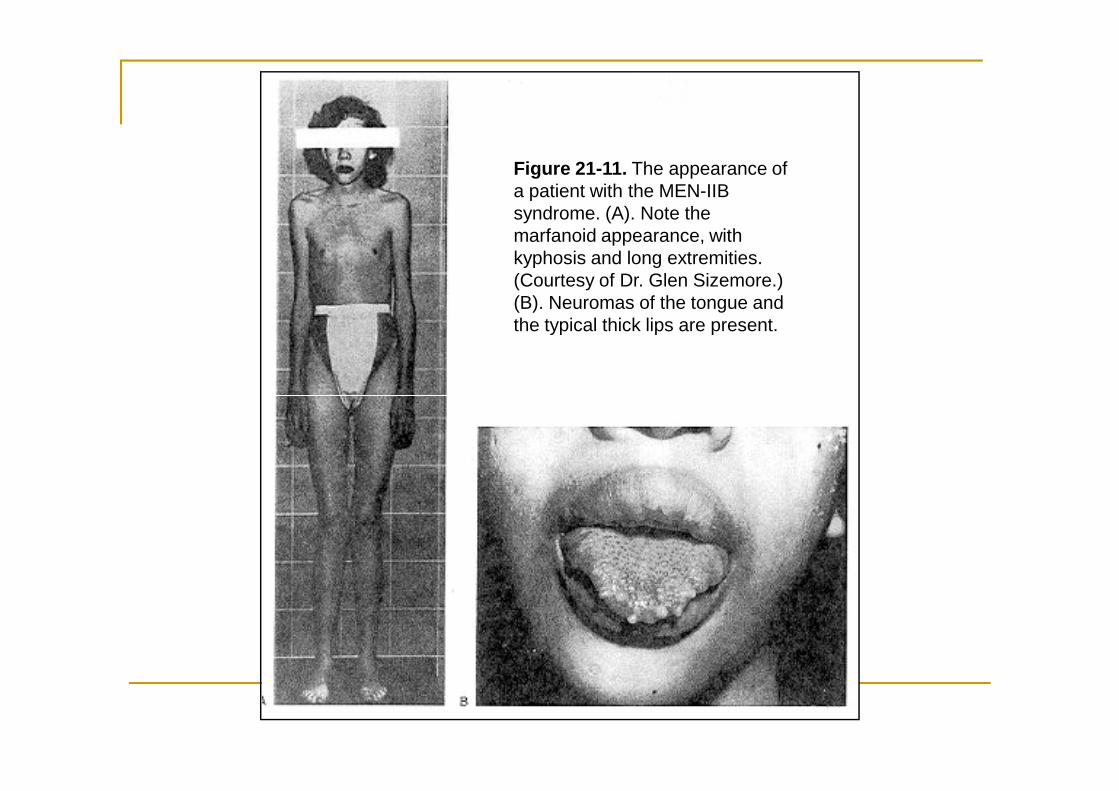
Figure 21-11. The appearance of a patient with the MEN-IIB syndrome. (A). Note the marfanoid appearance, with kyphosis and long extremities. (Courtesy of Dr. Glen Sizemore.) (B). Neuromas of the tongue and the typical thick lips are present.