fisiologi geriatri
DESCRIPTION
geriatriTRANSCRIPT

Print Close Window
Note: Large images and tables on this page may necessitate printing in landscape mode. Copyright © The McGraw-Hill Companies. All rights reserved. Harrison's Internal Medicine > Chapter 9. Geriatric Medicine >
Aging Aging is the progressive, universal decline first in functional reserve and then in function that occurs in organisms over time. Aging is heterogeneous. It varies widely in different individuals and in different organs within a particular individual. Aging is not a disease; however, the risk of developing disease is increased, often dramatically, as a function of age. The biochemical composition of tissues changes with age; physiologic capacity decreases, the ability to maintain homeostasis in adapting to stressors declines, and vulnerability to disease processes increases with age. After maturation, mortality rate increases exponentially with age.
Demography of Aging Populations worldwide are aging. Improvements in environmental (e.g., clean water and improved sanitation) and behavioral (nutrition, reduced risk exposures) factors and the treatment and prevention of infectious diseases are largely responsible for the 30-year increase in life expectancy since 1900. In the United States, by 2030, 1 person in 5 will be >65 years. Old people are not evenly distributed geographically. Half of older people in the United States live in nine states, led by California, Florida, New York, and Texas.
Global Aging Between 2000 and 2030, the number of older adults worldwide is expected to increase from 420 to 974 million. At present 59% of older adults live in the developing countries of Africa, Asia, Latin America, the Caribbean, and Oceania. The developing world has the largest absolute number of older adults and is experiencing the largest percentage increase.
Only 13% of those 80 years live in the United States; over 40% of those 80 years live in Asia. Embedded within these figures are additional critically important factors. Women outlive men; only 15% of centenarians are men. Men also remarry more frequently than do women; consequently, older women are frequently single and live alone. Women are more likely to have inadequate financial resources. Women also spend a greater portion of their surviving years being disabled than do men. In the United States, rates of disability decreased during the 1980s and 1990s, but the epidemics of obesity and physical inactivity may reverse these trends. A further concern for countries that already have high proportions of older adults (e.g., Japan, Sweden, Greece, and Italy, whose citizens >65 are 17–18% of their population) is the ratio of the >65 age group to the 15- to 64-year age group—the so-called dependency ratio. This ratio currently ranges from 22% in Europe to 6% in Africa but is expected to rise to >50% in Europe by 2050, with all other areas of the world exceeding 25% by 2050, except Africa.
Life Expectancy Often life-extending therapies are not offered to older patients because of an underestimate of life expectancy. Figure 9-1 shows average life expectancy as a function of age together with values for the lowest and highest quartiles of the population. White women currently have the highest life expectancy. Black women and white men have nearly identical life expectancies, and black men have the poorest life expectancy. At age 85 years, racial differences in life expectancy largely disappear. The average 75-
Page 1 of 21Print: Chapter 9. Geriatric Medicine
2/2/2012mk:@MSITStore:D:\Danny\Kuliah\Blok%2016\Kuliah%20Pakar\fisiologi%20blok%2016\...

year-old is expected to live to age 86 and the average 85-year-old to age 91. Furthermore, where the issue has been examined, age is not a factor in determining the efficacy of a particular intervention. Thus, age alone generally should not be used to withhold life-extending interventions.
Figure 9-1
Upper, middle, and lower quartiles of life expectancy for women and men at selected ages. (From LC Walter, KE Covinsky, JAMA 285:2751, 2001.)
Biology of Aging As we age, we become increasingly unlike one another. For any variable one can measure, the variation in the distribution of values in a population increases with age. While the mean value may trend up or
Page 2 of 21Print: Chapter 9. Geriatric Medicine
2/2/2012mk:@MSITStore:D:\Danny\Kuliah\Blok%2016\Kuliah%20Pakar\fisiologi%20blok%2016\...
down, the age-related increase in the range of values is striking testimony to the diverse manifestations of the aging process. In addition, homeostatic mechanisms are slower to respond to stressors and take longer to restore normal function as we age. The ability to maintain stable function in the face of a change in the environment is called allostasis and it declines with age.
One problem as we age is nosologic; when is a particular change considered a normal age-related alteration and when does it become a disease? Ideas about the range of normal for a particular age continue to evolve. At one time, a 75-year-old with a blood pressure of 170/90 mmHg might have been considered to have an age-related increase in systolic blood pressure that did not require intervention. However, we now know that such a reading is a reflection of increased vascular stiffness, one of the most important risk factors for cardiovascular morbidity and mortality. Similarly, follow-up of individuals with fasting serum glucose levels of 6.1–6.7 mmol/L (110–120 mg/dL) have shown them to be at increased risk of diabetes complications. Accordingly impaired glucose metabolism is now defined as a fasting glucose level > 6.1 mmol/L (>110 mg/dL). Thus, the indications for interventions to alter natural history have changed and will continue to change as we learn more about aging.
Whether age-related changes that produce an aging phenotype have a common origin in a global process that alters cell or organ function or have heterogeneous contributions in different systems or different individuals is unclear. Studies of aging (gerontology) are aimed at understanding the cellular and molecular basis of age-related changes and have two ultimate therapeutic goals: preserving function as long as possible and extending life span. These two goals may not be linked.
The lack of model systems for studying aging has hampered progress. For many years, researchers have studied replicative senescence of normal cells in culture. Why do normal cells have a finite replicative potential in vitro and why do cells from older individuals undergo fewer divisions than cells from younger individuals? Many have hoped that insights from such studies would reveal information about the aging process. However, the link between the failure of cells to divide in a synthetic culture medium and the aging phenotype of a whole organism is tenuous, at best. The body tissues with the greatest replicative potential should identify the organs most susceptible to age-related defective replication. In humans, these organs are the lining of the small intestine and the hematopoietic system. In the absence of disease, no age-related problem is caused by the inability of cells to replicate. Old people do not run out of absorptive surface in the small intestine or fail to make blood cells. Better in vitro models of aging are needed.
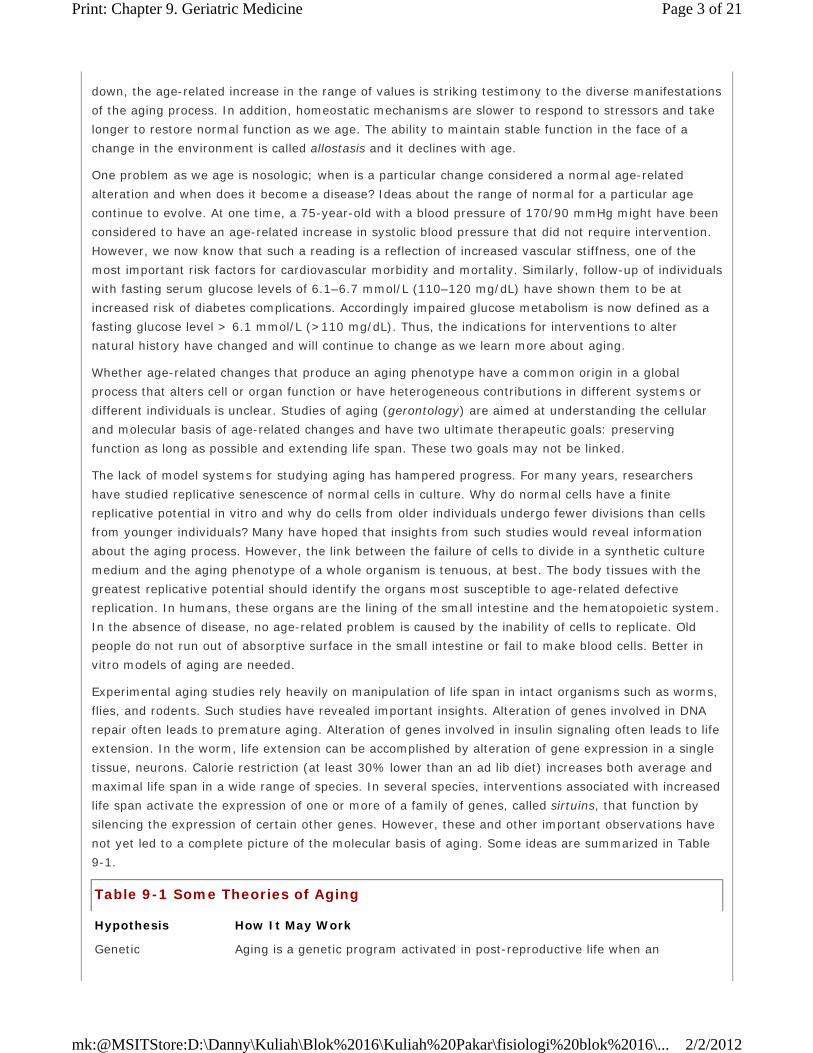
Experimental aging studies rely heavily on manipulation of life span in intact organisms such as worms, flies, and rodents. Such studies have revealed important insights. Alteration of genes involved in DNA repair often leads to premature aging. Alteration of genes involved in insulin signaling often leads to life extension. In the worm, life extension can be accomplished by alteration of gene expression in a single tissue, neurons. Calorie restriction (at least 30% lower than an ad lib diet) increases both average and maximal life span in a wide range of species. In several species, interventions associated with increased life span activate the expression of one or more of a family of genes, called sirtuins, that function by silencing the expression of certain other genes. However, these and other important observations have not yet led to a complete picture of the molecular basis of aging. Some ideas are summarized in Table 9-1.
Table 9-1 Some Theories of Aging
Hypothesis How It May Work
Genetic Aging is a genetic program activated in post-reproductive life when an
Page 3 of 21Print: Chapter 9. Geriatric Medicine
2/2/2012mk:@MSITStore:D:\Danny\Kuliah\Blok%2016\Kuliah%20Pakar\fisiologi%20blok%2016\...
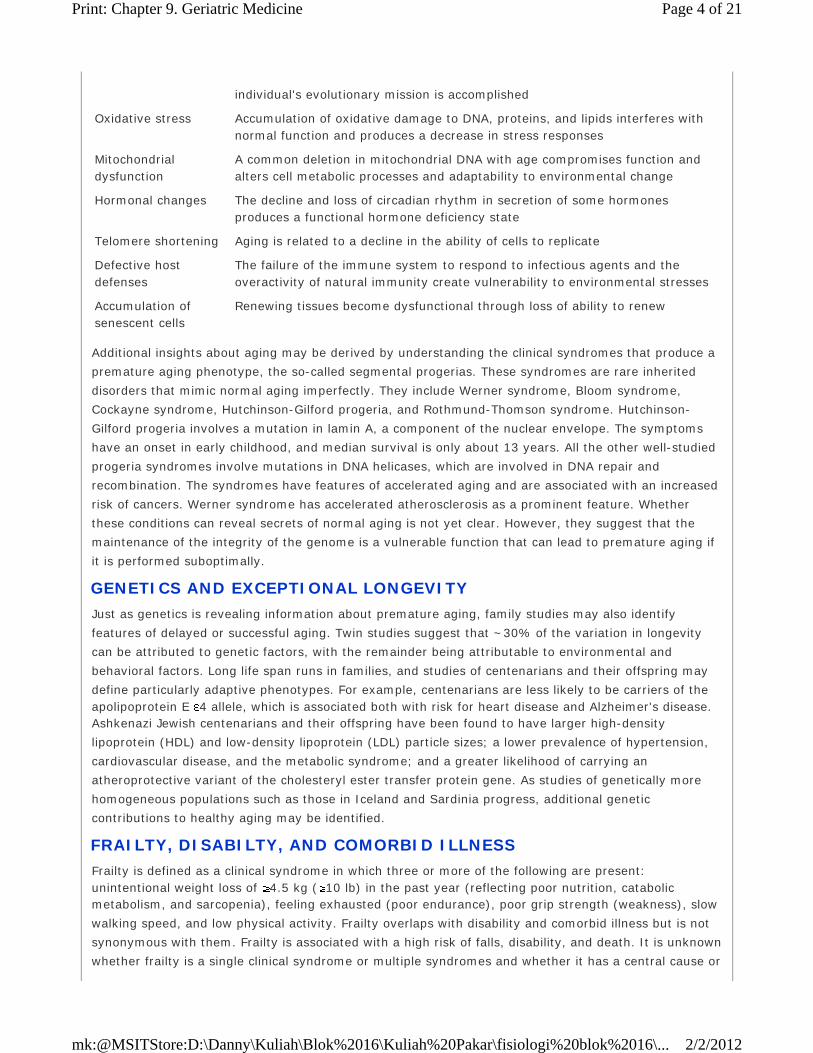
Additional insights about aging may be derived by understanding the clinical syndromes that produce a premature aging phenotype, the so-called segmental progerias. These syndromes are rare inherited disorders that mimic normal aging imperfectly. They include Werner syndrome, Bloom syndrome, Cockayne syndrome, Hutchinson-Gilford progeria, and Rothmund-Thomson syndrome. Hutchinson-Gilford progeria involves a mutation in lamin A, a component of the nuclear envelope. The symptoms have an onset in early childhood, and median survival is only about 13 years. All the other well-studied progeria syndromes involve mutations in DNA helicases, which are involved in DNA repair and recombination. The syndromes have features of accelerated aging and are associated with an increased risk of cancers. Werner syndrome has accelerated atherosclerosis as a prominent feature. Whether these conditions can reveal secrets of normal aging is not yet clear. However, they suggest that the maintenance of the integrity of the genome is a vulnerable function that can lead to premature aging if it is performed suboptimally.
GENETICS AND EXCEPTIONAL LONGEVITY Just as genetics is revealing information about premature aging, family studies may also identify features of delayed or successful aging. Twin studies suggest that ~30% of the variation in longevity can be attributed to genetic factors, with the remainder being attributable to environmental and behavioral factors. Long life span runs in families, and studies of centenarians and their offspring may define particularly adaptive phenotypes. For example, centenarians are less likely to be carriers of the apolipoprotein E 4 allele, which is associated both with risk for heart disease and Alzheimer's disease. Ashkenazi Jewish centenarians and their offspring have been found to have larger high-density lipoprotein (HDL) and low-density lipoprotein (LDL) particle sizes; a lower prevalence of hypertension, cardiovascular disease, and the metabolic syndrome; and a greater likelihood of carrying an atheroprotective variant of the cholesteryl ester transfer protein gene. As studies of genetically more homogeneous populations such as those in Iceland and Sardinia progress, additional genetic contributions to healthy aging may be identified.
FRAILTY, DISABILTY, AND COMORBID ILLNESS Frailty is defined as a clinical syndrome in which three or more of the following are present: unintentional weight loss of 4.5 kg ( 10 lb) in the past year (reflecting poor nutrition, catabolic metabolism, and sarcopenia), feeling exhausted (poor endurance), poor grip strength (weakness), slow walking speed, and low physical activity. Frailty overlaps with disability and comorbid illness but is not synonymous with them. Frailty is associated with a high risk of falls, disability, and death. It is unknown whether frailty is a single clinical syndrome or multiple syndromes and whether it has a central cause or
individual's evolutionary mission is accomplished
Oxidative stress Accumulation of oxidative damage to DNA, proteins, and lipids interferes with normal function and produces a decrease in stress responses
Mitochondrial dysfunction
A common deletion in mitochondrial DNA with age compromises function and alters cell metabolic processes and adaptability to environmental change
Hormonal changes The decline and loss of circadian rhythm in secretion of some hormones produces a functional hormone deficiency state
Telomere shortening Aging is related to a decline in the ability of cells to replicate
Defective host defenses
The failure of the immune system to respond to infectious agents and the overactivity of natural immunity create vulnerability to environmental stresses
Accumulation of senescent cells
Renewing tissues become dysfunctional through loss of ability to renew
Page 4 of 21Print: Chapter 9. Geriatric Medicine
2/2/2012mk:@MSITStore:D:\Danny\Kuliah\Blok%2016\Kuliah%20Pakar\fisiologi%20blok%2016\...

multiple causes. Frail patients often share many physical and biochemical characteristics, and studies are underway to assess whether the syndrome or parts of it are responsive to interventions.
Chronic Diseases and Their Implications The incidence, prevalence, and burden of chronic diseases increase with age, and this increased burden of disease is also associated with an increased risk of disability and decreased ability to recover from disability once it occurs.
THE GLOBAL PERSPECTIVE In 2005, chronic diseases accounted for 20 million deaths worldwide among those 70 years. The major disease contributors were cardiovascular disease (30%), cancer (13%), chronic respiratory disease (7%), and diabetes mellitus (2%). These diseases, driven to a large extent by tobacco use and obesity, are not concentrated in the developed world; rather, they are a large and growing problem in developing/low-income countries that lack the resources to prevent and manage chronic diseases and their consequences.
GENERAL CONSIDERATIONS Hypertension and diabetes mellitus are two common chronic conditions whose prevalence increases with age. In the United States, the National Health and Nutrition Examination Survey estimates that the prevalence of hypertension is between 60 and 84% and the prevalence of diabetes mellitus is between 18 and 21% in adults >65 years. The prevalence of both hypertension and diabetes is projected to increase substantially based on the demographics of aging and obesity. Moreover, rates of uncontrolled blood pressure in older adults are increasing, not decreasing. Both hypertension and diabetes accelerate functional decline in older adults, with hypertension accelerating cognitive decline and diabetes accelerating physical decline. Diabetes is also associated with a greater risk and severity of urinary incontinence (UI) and of falls in older women. Moreover, diabetes and stroke are the conditions most consistently associated with a diminished capacity for functional recovery in the aged.
The incidence of most cancers and cancer-specific mortality both increase with age. The age-adjusted incidence of cancer is ten times higher in the 65+ population than in those <65, and the age-adjusted cancer mortality is 15-fold higher. As a result, the incidence of cancer is expected to increase disproportionately in relation to overall population growth, and this trend is observed in countries throughout the world. Moreover, the majority of cancer survivors (>60%) are 65+ years of age.
In 2000, the leading causes of death among older Americans were heart disease (33%), cancer (22%), and cerebrovascular disease (8%). The death rate from heart disease has continued to decline; in 2006, cancer was the leading cause of death in persons <85 years. The management of chronic disease in older adults is particularly challenging. As examples, both hypertension and diabetes are established risk factors for micro- and macrovascular disease. Randomized clinical trials have demonstrated treatment efficacy, and guidelines for therapy are well established. Yet substantial evidence indicates that both conditions are inadequately treated, particularly in older adults with comorbidity. A portion of the problem is related to the fact that most clinical trials omit patients with comorbidities, making their results difficult to extrapolate to older patients with comorbid illness who are taking several other medications. The risks of drug-drug or drug-food interactions increase as a function of the number of medications used and patient age. In addition, the physician must take into account the impact of the disease and its treatment on the quality of life. Here, current functional status and rate of previous decline are helpful factors in estimating the level of functioning to which the patient may return. In concert with patient preferences and life goals, this information can help physicians and patients make decisions that are optimal at the individual patient level.
Page 5 of 21Print: Chapter 9. Geriatric Medicine
2/2/2012mk:@MSITStore:D:\Danny\Kuliah\Blok%2016\Kuliah%20Pakar\fisiologi%20blok%2016\...

One attempt to develop an evidence-based quality of care framework for older adults cared for in ambulatory settings has been the Assessing Care of Vulnerable Elders (ACOVE) project. Designed to inform the care of persons >65 years who are at high risk for death or functional decline over a 2-year period, based on age, self-rated health, self-report of physical capability, and functional limitations, the ACOVE indicators cover 22 topics, including diseases, syndromes, impairments, and clinical situations that are prevalent, have strong influence on health/quality of life, and are amenable to available interventions. The tool has drawbacks. The indicators are generally focused on the care of one disease or condition at a time, and the total number of indicators is overwhelmingly large (236). However, it appears that better quality of care is associated with improved survival. Better strategies to target clusters of interventions to those who will benefit most are needed.
Approach to: The Geriatric Patient FUNCTIONAL ASSESSMENT While the geriatric patient may have multiple chronic illnesses, functional status is the best indicator of prognosis and longevity. Functional status is defined as how well a person is able to provide for his or her own daily needs. Changes in function may signal a medical illness, advancing cognitive impairment, changes in social support, depression, substance abuse, or a combination of these. These changes should not be accepted as "just part of getting old." Documentation of a patient's baseline functional status is essential so that changes can be identified and addressed.
Table 9-2 lists some suggested brief screening strategies for assessing functional status.
Table 9-2 Suggested Brief Geriatric Assessment Instruments
Domain Instrument Sensitivity Specificity Time (min)
Cutpoint Comments
Cognition
Dementia MMSE 79–100%a
46–100% 9 <24b
Widely studied and accepted
Timed time and change test
94–100% 37–46% <2 <3 s for time and <10 s for change
Sensitive and quick
Delirium CAM 94–100% 90–95% <5 Sensitive and easy to apply
Affective disorders
GDS 5-question form
97% 85% 1 2 Rapid screen
Visual impairment
Snellen chart "Gold standard"
"Gold standard"
2 Inability to read at 20/40 line
Universally used
Hearing impairment
Whispered voice 80–90% 70–89% 0.5 50% correct No special equipment needed
Pure tone audiometry
94–100% 70–94% <5 Inability to hear >2 of 4 40-db tones (0.5, 1, 2, and 3 kHz)
Can be performed by trained office staff
Page 6 of 21Print: Chapter 9. Geriatric Medicine
2/2/2012mk:@MSITStore:D:\Danny\Kuliah\Blok%2016\Kuliah%20Pakar\fisiologi%20blok%2016\...

The first opportunity to assess the functional status of an older adult is when the patient is greeted and taken for a short walk into an examination room. In what way is the greeting received? Does the patient need assistance in getting out of a chair? Does he or she use an assistive device, such as a cane or walker? What is the patient's gait speed? How stable is the patient's gait? Is the patient fatigued after a short walk? These observations provide important initial information about how chronic illnesses affect the life of an older adult.
The basic activities of daily living (ADLs), which comprise activities essential for physical independence, and the instrumental activities of daily living (IADLs), which are necessary for independence in the community, are the most commonly used tools to assess functional status. The ADLs are dressing, bathing, feeding, toileting, transferring, and ambulating. The IADLs are money management, medication administration, using transportation, using the telephone, shopping, housekeeping, and meal preparation. These activities should be reviewed with the patient at the initial encounter and at periodic intervals. Cognitive deficits and psychosocial factors, however, may invalidate a patient's self-report, requiring the assistance of a third party for an accurate assessment. When functional deficits are identified, services provided by community (formal) or familial (informal) supports can be implemented to help the older adult continue to live in the least restrictive setting possible.
Other dimensions of the geriatric functional assessment include assessments of gait and balance, cognition, vision and hearing, dental and nutritional health, and driving ability. The Timed Get Up and Go Test is a valid clinical measure of balance in older adults. The patient is observed and timed as he or she rises from a chair, walks 3 m, turns around, and returns to sit down in the chair. A healthy older adult should be able to complete the test in <10 s. Difficulty performing this test is associated with increased fall risk and warrants further evaluation of mobility.
The screening tools to assess cognition in the older adult assist in identifying dementia and delirium, two common geriatric syndromes, both of which have a major effect on the functional status of the older adult. In addition, history-taking can be inaccurate and misleading if cognitive impairment is not
Dental health
DENTALc
82% 90% <2
(estimated)Score >2
Nutritional status
Weight loss of >4.5 kg (>10 lb) in 6 months or weight <45 kg (<100 lb)
65–70% 87–88% Yes to either
Gait and balance
"Timed Get Up and Go" test
88% 94% <1 >20s Requires no special equipment
aSome studies have found lower sensitivities, but most studies of dementia subjects fall in this range.
bCutoff is dependent on a number of variables including age, education, and racial or ethnic background.
cKA Atchinson, TA Dolan. Development of the geriatric oral health assessment index. J Dent Educ 11:680, 1990; with permission.
Note: MMSE, Mini-Mental Status Examination; CAM, confusion assessment method; GDS, geriatric depression scale.
Source: From CK Cassel et al. Geriatric Medicine: An Evidence-Based Approach, 4th ed. New York, Springer-Verlag, 2003; with permission.
Page 7 of 21Print: Chapter 9. Geriatric Medicine
2/2/2012mk:@MSITStore:D:\Danny\Kuliah\Blok%2016\Kuliah%20Pakar\fisiologi%20blok%2016\...

recognized before a medical evaluation. The Mini-Mental State Examination (MMSE) is the most commonly used test to assess cognitive function (Chap. 26). The Mini-Cog assessment instrument is an alternative to the MMSE and may be superior in assessing culturally diverse populations. The Mini-Cog consists of repeating three unrelated words, followed by a clock-drawing test (CDT) showing a specific time. The times 11:10 or 8:20 are often used. The patient is then asked to recall the three words. The patient receives one point for each recalled word after the CDT and two points for a normal clock. A score of 0–2 is a positive screen for dementia.
Delirium can cause loss of independence, prolonged hospitalizations, and increased health care costs and can be life threatening. It is often undiagnosed by health care providers and not recognized as a symptom of other medical illnesses. The Confusion Assessment Method (CAM) is highly sensitive and specific for identifying delirium. Delirium is diagnosed when the confusional state is both (1) acute in onset with a fluctuating course and (2) associated with inattention, and either (3) manifested by disorganized thinking or (4) an altered level of consciousness. Simple tests of attention include having the patient repeat a series of numbers or stating the months of the year backwards.
While specialists perform full vision and hearing assessments, any provider caring for an older adult should be able to screen for deficits in these areas because they commonly present in older patients, they can lead to loss of patient independence, and they often result from treatable conditions. Basic tests for visual acuity such as the handheld Jaeger card for testing near vision and the wall-mounted Snellen chart for testing far vision are the tests most commonly used in office-based practices. Visual impairment is defined as being unable to read the 20/40 line or worse. Visual acuity itself has not been associated with increased fall risk in most studies; however, binocular vision, depth perception, and contrast sensitivity contribute to postural stability and object recognition. Hearing impairment can lead to decreased physical function, depression, and social isolation. The whisper test and testing with a handheld audioscope are used frequently as screening tests. To perform the whisper test, the examiner covers the opposite ear of the patient being tested, exhales completely, and then whispers an easily answered question from a distance of 60 cm (2 ft) from the ear being tested. Treatment of hearing loss with amplification by a hearing aid has been shown to improve quality of life. Patients demonstrating vision or hearing impairment should be referred for full ophthalmologic and audiologic evaluation. Hearing and vision impairment together are associated with lower functional status than either impairment alone.
Malnutrition is not uncommon in older adults and is associated with increased mortality, morbidity, and admission to nursing homes. In community-dwelling adults, the following definitions of malnutrition may be used: (1) involuntary weight loss [e.g., 4.5 kg ( 10 lb) over 6 months, 4% over 1 year], (2) abnormal body mass index [BMI: weight/height2 (in kg/m2) (e.g., BMI < 22 or BMI > 27], (3) hypoalbuminemia [e.g., 38 g/L ( 3.8 g/dL)], (4) hypocholesterolemia [e.g., <4.1 mmol/L (<160 mg/dL)], or (5) specific vitamin or micronutrient deficiency (e.g., vitamin B12). When any one of these
is present, a multidimensional assessment should be undertaken. The clinician should review the patient's access to food. Are there economic or other barriers to receiving high-quality food? Are there dental problems that might interfere with eating such as loose dentures, missing teeth, or other oral pathology? Many medical illnesses interfere with digestion or absorption of food, increase nutritional requirements, or require dietary restrictions. Is the patient unable to shop, prepare meals, or feed him- or herself? Does the patient have cultural habits or food preferences that could affect his or her nutritional status? Poor appetite may be related to medications, medical illnesses, or depression.
For many older adults, being independent depends on driving an automobile. However, the traffic violation rate per driver is increased in both teenagers and older drivers. One study has identified poor
Page 8 of 21Print: Chapter 9. Geriatric Medicine
2/2/2012mk:@MSITStore:D:\Danny\Kuliah\Blok%2016\Kuliah%20Pakar\fisiologi%20blok%2016\...

design copying on the MMSE, fewer blocks walked, and more foot abnormalities as the best predictors of adverse driving events. While a patient can undergo a formal driving assessment, often done by rehabilitation experts, the clinician can also indirectly assess a patient's driving skills by performing vision, cognition, and motor assessments in the office. Making the decision that an older adult is no longer able to drive is often done by the patient, but when the patient has limited insight into his or her physical and/or cognitive impairments, family, friends, health care providers, and sometimes government employees are responsible for keeping the older patient, as well as other drivers, safe.
Geriatric Syndromes Geriatric syndrome refers to a symptom presentation that is common in older adults; most are multifactorial in origin. Several of these topics are covered in more detail elsewhere in the text.
DEMENTIA AND DELIRIUM Dementia is a syndrome of progressive decline in which multiple intellectual abilities deteriorate, causing both cognitive and functional impairment. While dementia is a state of chronic confusion, delirium is an acute state of confusion. It is important to differentiate delirium from dementia. Early identification and treatment of the underlying causes of delirium can improve outcomes. Delirium may be the only manifestation of a life-threatening illness in the older adult. Both dementia and delirium are characterized by disorientation, memory impairment, paranoia, hallucinations, emotional lability, and sleep-wake cycle reversal. Key features of delirium are acute onset, impaired attention, and an altered level of consciousness. Dementia and delirium are described more fully in Chaps. 365 and 26, respectively.
The main goals of care of a patient with dementia are to maintain an optimal quality of life and to maximize cognitive and physical functioning. Therefore, when an older patient presents with cognitive impairment, a key goal is to identify and treat reversible causes of cognitive impairment, such as infections, electrolyte abnormalities, vitamin deficiencies, thyroid disease, substance abuse, medication, and psychiatric illnesses. The clinician must then ask key questions: (1) Is the patient safe in the community? (2) Is the patient able to perform his or her own ADLs and IADLs? (3) What assistance is needed to maximize the patient's functioning in his or her living situation? The patient may not be able to answer these questions accurately, so an objective, cognitively intact informant will be helpful.
If the patient has dangerous behaviors, such as leaving the stove on or getting lost, a plan of care involving increased patient supervision should be put in place. As dementia progresses, more caregiving services, both formal and informal, will need to be added to support the patient in the community. Formal caregivers are paid care providers. Examples are visiting nurses, home health aides who assist with personal hygiene, homemakers who assist with housework and meal preparation, Meals-on-Wheels, adult day programs, state aging services, and hospice services. Informal caregivers are persons who provide an older adult with unpaid care. Examples are family members, friends, neighbors, or church members.
The primary caregiver of a patient with dementia may need more physician support than the patient. Caring for a disabled spouse or parent is associated with an increased risk of depression or anxiety. Caregivers experiencing mental or emotional strain have an increased risk of dying compared to non-caregivers. Predictors of nursing home admission for patients with Alzheimer's disease include aggression, assault, paranoia, nighttime wandering, and loss of capacity to recognize the caregiver. Adult day care and respite programs may help to alleviate some caregiver burden. Support groups, through organizations such as the Alzheimer's Association, can also help to educate caregivers and decrease stress.
Page 9 of 21Print: Chapter 9. Geriatric Medicine
2/2/2012mk:@MSITStore:D:\Danny\Kuliah\Blok%2016\Kuliah%20Pakar\fisiologi%20blok%2016\...

When patients with dementia exhibit agitated behaviors, medical illnesses, such as infections, pain syndromes, and drug side effects, must be ruled out as causes. These behaviors are, however, often part of a dementing illness. If the agitated behavior is harmful to the patient or others and does not respond to non-pharmacologic therapies, such as redirecting the patient, providing a calm environment, or familiar surroundings, then low doses of psychotropic medication may be helpful. Antipsychotics, anxiolytics, or antidepressants can be used, depending on the type of symptoms. Low-dose risperidone (0.25–1.5 mg/d) or olanzapine (2.5–10 mg/d) can be used if a patient has upsetting delusions or hallucinations. Antidepressants such as citalopram (10–30 mg/d) can be used for depressive symptoms. Patients on antipsychotics should be monitored closely for the development of extrapyramidal side effects, such as tremor, rigidity, and bradykinesia. The lowest dose possible should be used; dosage reductions should be attempted, if possible, at 6-month intervals. Sometimes, as cognitive functioning worsens, patients will no longer have the psychoses or the depression causing the agitated behaviors.
FALLS This discussion of falls excludes falls occurring from seizure, stroke, syncope, or an insurmountable environmental hazard (Chap. 24). Fall rates and risk of injury from falls increase with age. Annually, ~30% of community dwelling adults >65 years fall, while 50% of individuals >80 years fall. Injuries in 20–30% of fallers reduce subsequent mobility and independence, with 3–5% of falls resulting in fracture. Falling is an independent risk factor for nursing home placement. Often the occurrence of a fall does not come to the attention of the health care provider. Given fall frequency and resulting morbidity and mortality from falling in older adults, all older patients should have a fall risk assessment and be asked about falls in the past year.
While most falls are multifactorial, falling is sometimes a symptom of another disease, such as an infection or neurologic disorder, or a medication side effect. In addition, age-related physiologic changes contribute to fall risk. These include decreased proprioception, increased postural sway, and declines in baroreflex sensitivity resulting in orthostatic hypotension. The evaluation of a fall should begin with a history, including the circumstances at the time of the fall, any associated symptoms, and a thorough medication review of both prescription and over-the-counter medications. The physical examination should include postural vital signs, vision evaluation, gait and balance testing, and a musculoskeletal evaluation of joint stability and range of motion. An environmental assessment of the patient's home by a visiting nurse or other health care provider can reveal additional hazards that can increase fall risk, such as clutter, loose carpets, and poor lighting.
Interventions designed to reduce fall rates must also preserve mobility and independence. Physical restraint use has been found to be strongly associated with increased fall risk and increased risk for serious injury from a fall in nursing home residents. The major risk factors for falls are shown in Table 9-3. Several factors associated with increased risk for falling include low creatinine clearance [<1.1 mL/s (< 65 mL/min)], low serum 25-hydroxyvitamin D levels (< 39 nmol/L) and high serum parathyroid hormone levels, insomnia, and fear of falling. Table 9-3 also outlines suggested interventions targeted at common fall risk factors. General exercise and balance training; t'ai chi; psychotropic medication elimination; and multidisciplinary, multifactorial, risk factor screening and intervention have been shown to reduce fall risk.
Table 9-3 Recommended Components of Clinical Assessment and Management for Older Persons Living in the Community Who Are at Risk for Falling
Assessment and Risk Factor Management
Page 10 of 21Print: Chapter 9. Geriatric Medicine
2/2/2012mk:@MSITStore:D:\Danny\Kuliah\Blok%2016\Kuliah%20Pakar\fisiologi%20blok%2016\...

Circumstances of previous fallsa Changes in environment and activity to reduce the likelihood of recurrent falls
Medication use Review and reduction of medications
High-risk medications (e.g., benzodiazepines, other sleeping medications, neuroleptics, antidepressants, anticonvulsants, or class IA antiarrhythmics)a,b,c
Four or more medicationsc
Visiona Ample lighting without glare; avoidance of multifocal glasses while walking; referral to an ophthalmologist Acuity <20/60
Decreased depth perception
Decreased contrast sensitivity
Cataracts
Postural blood pressure (after 5 min in a supine position, immediately after standing, and 2 min after standing)c
Diagnosis and treatment of underlying cause, if possible; review and reduction of medications; modification of salt restriction; adequate hydration; compensatory strategies (e.g., elevation of head of bed, rising slowly, or dorsiflexion exercises); pressure stockings; pharmacologic therapy if the above strategies fail 20 mmHg (or 20%) drop in
systolic pressure, with or without symptoms, either immediately or after 2 min of standing
Balance and gaitb,c Diagnosis and treatment of underlying cause, if possible; reduction of medications that impair balance; environmental interventions; referral to physical therapist for assistive devices and for gait and progressive balance training
Patient's report or observation of unsteadiness
Impairment on brief assessment (e.g., the Get-Up and Go test or performance-oriented assessment of mobility)
Targeted neurologic examination Diagnosis and treatment of underlying cause, if possible; increase in proprioceptive input (with an assistive device or appropriate footwear that encases the foot and has a low heel and thin sole); reduction of medications that impede cognition; awareness on the part of caregivers of cognitive deficits; reduction of environmental risk factors; referral to physical therapist for gait, balance, and strength training
Impaired proprioceptiona
Impaired cognitiona
Decreased muscle strengthb,c
Targeted musculoskeletal examination: examination of legs (joints and range of motion) and examination of feeta
Diagnosis and treatment of the underlying cause, if possible; referral to physical therapist for strength, range-of-motion, and gait and balance training and for assistive devices; use of appropriate footwear; referral to podiatrist
Targeted cardiovascular examinationb
Referral to cardiologist; carotid-sinus massage (in the case of syncope)
Syncope
Arrhythmia (if there is known
Page 11 of 21Print: Chapter 9. Geriatric Medicine
2/2/2012mk:@MSITStore:D:\Danny\Kuliah\Blok%2016\Kuliah%20Pakar\fisiologi%20blok%2016\...

URINARY INCONTINENCE UI is a major problem for older adults, afflicting up to 30% of community-dwelling elders and 50% of nursing home residents. Up to age 80 years, UI affects women twice as commonly as men; after age 80, the sexes are equally affected. In addition to the great impact of UI on a patient's well-being, including embarrassment, social isolation, and depression, UI is also a risk factor for nursing home placement. While certainly not a normal part of aging, advanced age, functional impairment, dementia, obesity, smoking, affective disorder, constipation, certain medical illnesses (such as chronic obstructive pulmonary disease and heart failure), and a history of pelvic surgery are associated with UI. UI is often due to a combination of these risk factors.
Older patients must be asked directly whether they have symptoms of UI, since only half of community-dwelling women with incontinence will discuss their incontinence with a health care provider. UI can then be determined to be either transient or established, although "transient" UI may be misdiagnosed as "established" if left untreated. The "DRIIIPP" mnemonic (Table 9-4) is very useful when evaluating a patient for reversible conditions that may cause or contribute to UI. If these conditions are identified and treated, the older adult benefits from relief of UI and symptoms of other comorbidities.
Leaking of urine occurs in four ways. The bladder can be limited in its ability to empty or in its ability to store urine; or one or both of the urethral sphincters may be unable to allow storage of urine or to allow passage of urine. Impairments can exist in one or in several of the urine storage mechanisms of the lower urinary tract. Four classifications of established UI have been proposed based on this understanding of the lower urinary tract: stress incontinence, urge incontinence, mixed stress and urge
cardiac disease, an abnormal electrocardiogram, and syncope)
Home-hazard evaluation after hospital dischargeb,c
Removal of loose rugs and use of nightlights; nonslip bath-mats, and stair rails; other interventions as necessary
aRecommendation of this assessment is based on observational data that the finding is associated with an increased risk of falling.
bRecommendation of this assessment is based on one or more randomized controlled trials of a single intervention.
cRecommendation of this assessment is based on one or more randomized controlled trials of a multifactorial intervention strategy that included this component.
Source: ME Tinetti: N Engl J Med 348:45, 2003; with permission.
Table 9-4 Reversible Conditions Associated with Urinary Incontinence
Delirium
Restricted mobility—illness, injury, gait disorder, restraint
Infection—acute, symptomatic urinary tract infection
Inflammation—atrophic vaginitis
Impaction—of feces
Polyuria—diabetes, caffeine intake, volume overload
Pharmaceuticals—diuretics, -adrenergic agonists or antagonists, anticholinergic agents (psychotropics, antidepressants, anti-Parkinsonians)
Source: After DB Reuben et al.
Page 12 of 21Print: Chapter 9. Geriatric Medicine
2/2/2012mk:@MSITStore:D:\Danny\Kuliah\Blok%2016\Kuliah%20Pakar\fisiologi%20blok%2016\...

incontinence, and overflow incontinence.
Stress incontinence, which is rare in men, results when the urethral sphincter mechanisms are inadequate to hold urine during bladder filling. Patients describe symptoms of leaking small amounts of urine during activities that increase intraabdominal pressure, such as coughing, laughing, sneezing, lifting, or standing up. Patient history is very sensitive (0.906) but not very specific (0.511) in diagnosing stress incontinence. A stress test in the office can be performed by having the patient stand with a full bladder and cough. The test is positive if urine leakage coincides with the cough. An involuntary bladder contraction induced by the cough may cause leakage several seconds after the cough. The most common causes of stress incontinence in women are insufficient pelvic support due to childbearing, gynecologic surgery, and the decreased effects of estrogen on tissues of the lower urinary tract. Surgical interventions are the most effective treatments; pelvic muscle exercises can be helpful, although treatment failure is higher in patients who have two or more leakages per day.
Urge incontinence, also known as detrusor overactivity (DO), is characterized by uninhibited bladder contractions and is the most common form of UI in older adults. Patients often describe symptoms of an uncontrollable need to void. Urinary frequency and nocturnal incontinence are common, particularly accompanied by loss of larger urine volumes (>100 mL). Urge incontinence may be idiopathic, associated with lesions of the central nervous system, such as a stroke, or be due to bladder irritation from infection, stones, or tumors. The term detrusor hyperactivity with impaired contractility (DHIC) is a type of urge incontinence characterized by involuntary bladder contractions with a weak detrusor muscle leading to incomplete emptying of the bladder. The diagnosis is primarily based on a patient's symptoms in the absence of urinary retention and the leakage of urine with stress maneuvers.
Measurement of postvoid residual (PVR) should be part of an incontinence evaluation in all patients. Under sterile conditions, the patient's bladder is catheterized 5–10 min after the patient has voided. Generally, a PVR > 200 mL suggests detrusor underactivity or obstruction. The patient should be referred for further urologic evaluation.
Initial treatment of urge incontinence should be bladder retraining by encouraging the patient to void every 2 h or based on the patient's symptom frequency. The patient can also try urgency control by sitting or standing quietly while focusing on allowing the urgency to pass before slowly walking to the bathroom to void. If the patient has no incontinence for 2 days, the voiding interval can be increased by 30–60 minutes until the patient is only voiding every 3–4 h. The anticholinergic drugs, oxybutinin and tolterodine, which cause bladder relaxation, can be added to this therapy. Their use in older adults may be limited by anticholinergic symptoms such as urinary retention, confusion, constipation, and dry mouth. Patients using tolterodine have a reduced risk of dry mouth and fewer withdrawals due to side effects, but the efficacy of oxybutinin and tolterodine is similar.
Mixed incontinence refers to UI where symptoms of both stress and urge incontinence are present. A simple, quick questionnaire consisting of three incontinence questions (3IQ) may help to classify urge and stress incontinence in women in the primary care setting. Question one asks if the patient has leaked urine in the past 3 months. Question two familiarizes patients with types of incontinence: stress, urge, or other. Question three asks the patient for the category of incontinence based on her symptoms during the past 3 months: stress, urge, mixed, or other. The 3IQ improved the likelihood of a positive diagnosis of urge incontinence (+likelihood ratio of 3.29) and of stress incontinence (+likelihood ratio of 2.13).
Overflow incontinence is due to either bladder outlet obstruction or an atonic bladder. Male patients, but rarely females, may complain of dribbling after voiding, an incessant urge to urinate, or straining to
Page 13 of 21Print: Chapter 9. Geriatric Medicine
2/2/2012mk:@MSITStore:D:\Danny\Kuliah\Blok%2016\Kuliah%20Pakar\fisiologi%20blok%2016\...
urinate. On physical examination, patients may have a palpable distended bladder. Prostatic hypertrophy, prostate cancer, and urethral strictures are the most common causes of overflow incontinence in men, while a cystocele can cause this problem in women. Detrusor atonicity or underactivity can be caused by spinal cord disease, autonomic neuropathy of diabetes, alcoholism, vitamin B12 deficiency, Parkinson's disease, tabes dorsalis, or chronic outlet obstruction. Urodynamic
testing is helpful in distinguishing urethral obstruction from detrusor underactivity. The most effective treatment for bladder outlet obstruction is surgical removal of the obstruction. Intermittent or indwelling catheterization may be required for nonoperative candidates with obstruction or for patients with detrusor underactivity. For men who have benign prostatic hypertrophy (BPH) and are not in retention, -adrenergic blockers such as terazosin, doxazosin, or tamulosin can decrease symptoms of urinary frequency and nocturia. Finasteride, a 5 -reductase inhibitor, may be useful in combination with doxazosin for decreasing lower urinary tract symptoms due to BPH in men with a total prostate volume of 25 mL.
The diagnosis of functional incontinence describes individuals who have UI and have either cognitive or functional impairments which limit their ability to toilet themselves. However, other treatable causes of UI may be missed if one assumes dementia or immobility is the cause of UI in these patients.
PRESSURE ULCERS Pressure ulcers, also known as pressure sores, bedsores, or decubitus ulcers, occur in older patients with reduced mobility. A pressure ulcer occurs when increased pressure between skin and a bony prominence produces tissue necrosis. While pressure ulcers can occur anywhere, 80% of pressure ulcers occur over the heels, lateral malleoli, sacrum, ischia, and greater trochanters. Shear forces, causing stretching and angulation of blood vessels, and frictional forces, causing separation of the epidermal or dermal layers, can also lead to tissue necrosis and open ulceration. Moisture can increase friction leading to maceration and superficial skin erosions.
Reported incidence data for the United States vary widely by site of care: general acute care, 0.4–38%; long-term care, 2.2–23.9%; and home care, 0–17%. Prevalence rates range from 10–18% in general acute care, 2.3–28% in long-term care, and 0–29% in home care. In older adults and nursing home residents, the development of a pressure ulcer increases mortality by fourfold. Osteomyelitis and sepsis are important, morbid complications of pressure ulcers.
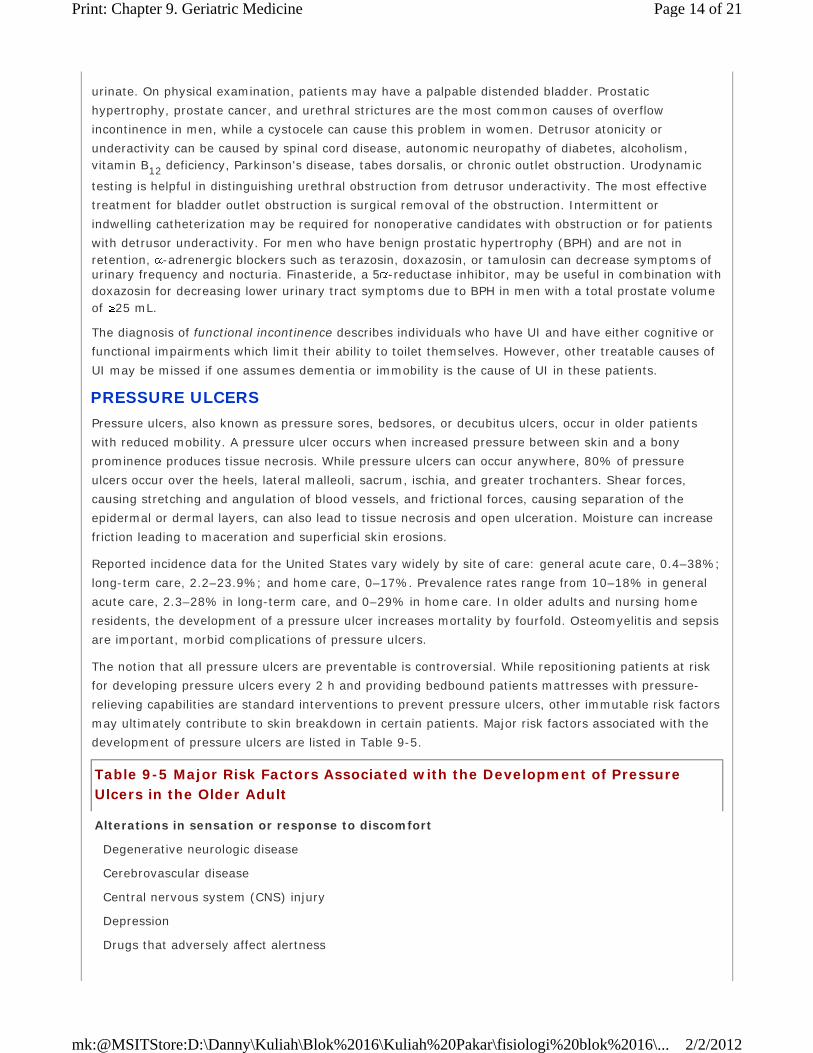
The notion that all pressure ulcers are preventable is controversial. While repositioning patients at risk for developing pressure ulcers every 2 h and providing bedbound patients mattresses with pressure-relieving capabilities are standard interventions to prevent pressure ulcers, other immutable risk factors may ultimately contribute to skin breakdown in certain patients. Major risk factors associated with the development of pressure ulcers are listed in Table 9-5.
Table 9-5 Major Risk Factors Associated with the Development of Pressure Ulcers in the Older Adult
Alterations in sensation or response to discomfort
Degenerative neurologic disease
Cerebrovascular disease
Central nervous system (CNS) injury
Depression
Drugs that adversely affect alertness
Page 14 of 21Print: Chapter 9. Geriatric Medicine
2/2/2012mk:@MSITStore:D:\Danny\Kuliah\Blok%2016\Kuliah%20Pakar\fisiologi%20blok%2016\...

When an ulcer is identified, one must try to identify its etiology. Pressure ulcers lie at sites of pressure. Diabetic ulcers can also be caused by pressure in extremities compromised by neuropathy and vascular disease, including both large and small blood vessels. Venous stasis ulcers develop on the lower extremities with or without edema due to incompetent valves of the veins. Arterial ischemic ulcers develop at sites of decreased blood flow. Since adequate blood supply is necessary for tissue to heal, assessment of pulses and ankle-brachial indices (ABI) for ulcers of the lower extremities can provide prognostic information. An ABI of <0.4 is associated with a low likelihood of wound healing. If the patient is not a surgical candidate for revascularization, the goal of care must be to keep the wound free of infection and to alleviate any related patient discomfort.
When an ulcer is identified as a pressure ulcer, the ulcer should be staged so that the appropriate therapy may be instituted. The staging in Table 9-6 is based on a system developed in 1989 by the National Pressure Ulcer Advisory Panel. Nonblanching erythema constitutes vascular damage and hemorrhage. Stage 1 ulcers can progress to stage 4 ulcers in as little as a day or two, depending on how deeply the necrosis extends. Once a hard, dark eschar develops, the ulcer cannot be staged until the necrotic tissue is removed. Three major steps in pressure ulcer management lead to wound healing: debridement, cleansing, and dressing. Debridement, either surgical or chemical, is necessary to remove necrotic tissue to allow new granulation tissue to grow. Necrotic tissue can also contain bacteria that impede wound healing. Cleansing the wound helps to lower bacteria counts. Normal saline is best, as its use protects new granulation tissue. In foul-smelling, infected wounds, bacteriocidal agents such as 1% povidine-iodine, 0.25% acetic acid, or 0.5% sodium hypochlorite (Dakin's solution) can be used as disinfectants, but not for more than a week at a time as they are cytotoxic to fibroblasts and delay wound healing. A discussion of which dressing to use is beyond the scope of this chapter, but the choice of a dressing should be based on the ulcer stage, whether or not local infection is present, whether or not excessive exudate is present, and whether continued debridement is necessary. Management of pressure ulcers should be interdisciplinary involving physicians, nurses, wound care specialists, occupational or physical therapists, and nutritionists. Usually, stage 1 and 2 pressure ulcers heal in days to weeks, whereas healing of stage 3 and 4 ulcers may be seen at 2–4 weeks, but they often take many months to heal.
Alterations in mobility
Neurologic disease/injury
Fractures
Pain
Restraints
Significant changes in weight ( 5% in 30 days or 10% in the previous 180 days)
Protein-calorie undernutrition
Edema
Incontinence
Bowel and bladder
Source: From American Medical Directors Association (AMDA): Pressure Ulcers. Columbia, MD, American Medical Directors Association, 1996.
Table 9-6 Staging System for Pressure Ulcers
Stage 1
Page 15 of 21Print: Chapter 9. Geriatric Medicine
2/2/2012mk:@MSITStore:D:\Danny\Kuliah\Blok%2016\Kuliah%20Pakar\fisiologi%20blok%2016\...
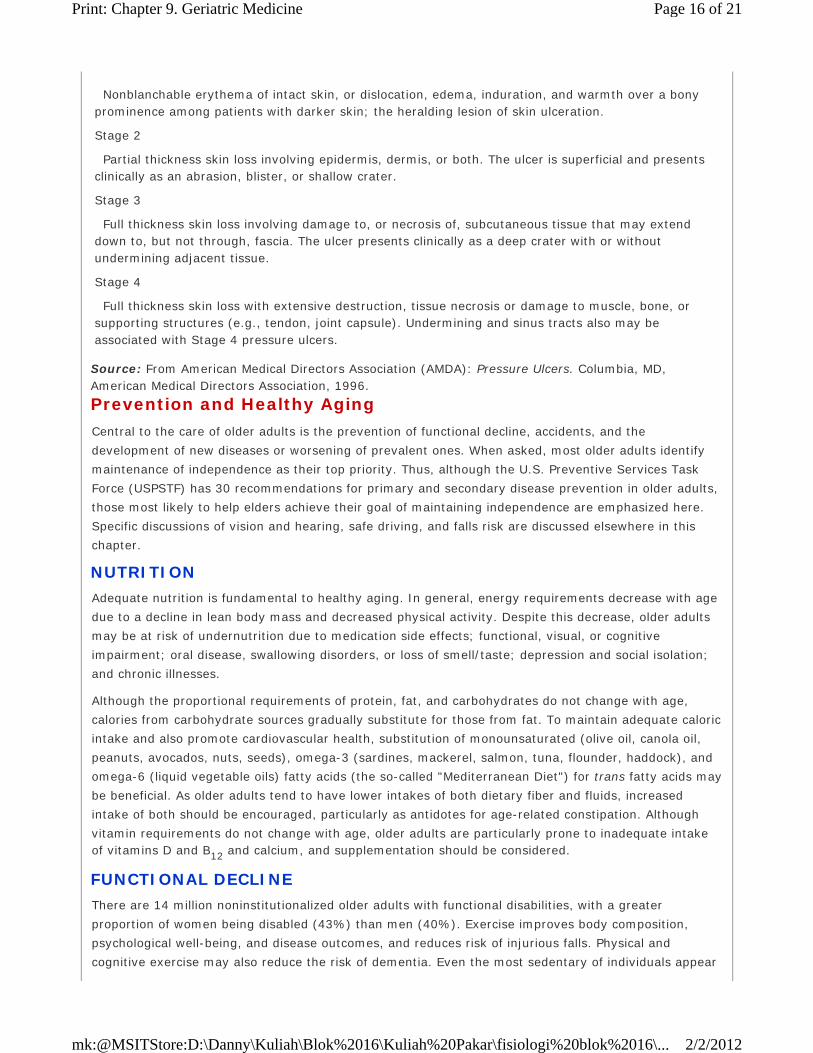
Nonblanchable erythema of intact skin, or dislocation, edema, induration, and warmth over a bony prominence among patients with darker skin; the heralding lesion of skin ulceration.
Stage 2
Partial thickness skin loss involving epidermis, dermis, or both. The ulcer is superficial and presents clinically as an abrasion, blister, or shallow crater.
Stage 3
Full thickness skin loss involving damage to, or necrosis of, subcutaneous tissue that may extend down to, but not through, fascia. The ulcer presents clinically as a deep crater with or without undermining adjacent tissue.
Stage 4
Full thickness skin loss with extensive destruction, tissue necrosis or damage to muscle, bone, or supporting structures (e.g., tendon, joint capsule). Undermining and sinus tracts also may be associated with Stage 4 pressure ulcers.
Source: From American Medical Directors Association (AMDA): Pressure Ulcers. Columbia, MD, American Medical Directors Association, 1996. Prevention and Healthy Aging Central to the care of older adults is the prevention of functional decline, accidents, and the development of new diseases or worsening of prevalent ones. When asked, most older adults identify maintenance of independence as their top priority. Thus, although the U.S. Preventive Services Task Force (USPSTF) has 30 recommendations for primary and secondary disease prevention in older adults, those most likely to help elders achieve their goal of maintaining independence are emphasized here. Specific discussions of vision and hearing, safe driving, and falls risk are discussed elsewhere in this chapter.
NUTRITION Adequate nutrition is fundamental to healthy aging. In general, energy requirements decrease with age due to a decline in lean body mass and decreased physical activity. Despite this decrease, older adults may be at risk of undernutrition due to medication side effects; functional, visual, or cognitive impairment; oral disease, swallowing disorders, or loss of smell/taste; depression and social isolation; and chronic illnesses.
Although the proportional requirements of protein, fat, and carbohydrates do not change with age, calories from carbohydrate sources gradually substitute for those from fat. To maintain adequate caloric intake and also promote cardiovascular health, substitution of monounsaturated (olive oil, canola oil, peanuts, avocados, nuts, seeds), omega-3 (sardines, mackerel, salmon, tuna, flounder, haddock), and omega-6 (liquid vegetable oils) fatty acids (the so-called "Mediterranean Diet") for trans fatty acids may be beneficial. As older adults tend to have lower intakes of both dietary fiber and fluids, increased intake of both should be encouraged, particularly as antidotes for age-related constipation. Although vitamin requirements do not change with age, older adults are particularly prone to inadequate intake of vitamins D and B12 and calcium, and supplementation should be considered.
FUNCTIONAL DECLINE There are 14 million noninstitutionalized older adults with functional disabilities, with a greater proportion of women being disabled (43%) than men (40%). Exercise improves body composition, psychological well-being, and disease outcomes, and reduces risk of injurious falls. Physical and cognitive exercise may also reduce the risk of dementia. Even the most sedentary of individuals appear
Page 16 of 21Print: Chapter 9. Geriatric Medicine
2/2/2012mk:@MSITStore:D:\Danny\Kuliah\Blok%2016\Kuliah%20Pakar\fisiologi%20blok%2016\...

to benefit from increasing physical activity. All patients should be asked about their level of physical activity, e.g., the number of days during an average week that they spend at least 15 min walking, bicycling, swimming, weight training, etc. An exercise prescription may be beneficial. It should consider flexibility, endurance, strength, and balance but should be preceded by attention to musculoskeletal problems, footwear, and risk factors for cardiovascular disease. Guidelines for such a prescription are shown in Table 9-7.
Table 9-7 Recommendations for Optimal Aging and Prevention and Treatment of Disease in Older Adults
Modality Resistance Training
Cardiovascular Endurance Training
Flexibility Training
Balance Training
Dose
Frequency 2–3 days/week 3–7 days/week 1–7 days/week 3–7 days/week
Volume 1–3 sets of 8–12 repetitions, 8–10 major muscle groups
20–60 min per session Major muscle groups 1 sustained stretch (20 s) of each
1–2 sets of 4–10 different exercises emphasizing dynamic posturesa
Intensity 15–18 on Perceived Exertion Scale (70–80% 1 RM), 6 s/repetition, 1–2 min rest between sets
12–14 on Perceived Exertion Scale (50–60% heart rate reserve or maximal exercise capacity)
Progressive neuromuscular facilitation techniqueb
Progressive difficulty as tolerated, at the level that is not yet masteredc
Requirements for safety and maximal efficacy
Slow speed, no ballistic movements, day of rest between sessions
Good form, no substitution of muscles
No breath holding, Valsalva maneuver
Increase weight progressively to maintain relative intensity at high load
If possible, power training (high-velocity, high-
Low-impact activity if arthritis present; high impact more potent for bone remodeling
Weight-bearing, best include hills/stairs if possible
Increase workload progressively to maintain relative intensity
Perceived exertion better than monitoring pulse to gauge intensity
May accumulate short bouts (10 min) of exercise to reach volume goal
One hour/week high-intensity endurance exercise equivalent to 3–4 hours/week moderate-intensity endurance exercise for cardiovascular/metabolic
Static rather than ballistic stretching
Stretch warmed muscles after other exercises are complete, as part of cool-down
Safe environment or monitoring
Dynamic as well as static modes of training
Gradual increase in difficulty as competence is demonstrated
Page 17 of 21Print: Chapter 9. Geriatric Medicine
2/2/2012mk:@MSITStore:D:\Danny\Kuliah\Blok%2016\Kuliah%20Pakar\fisiologi%20blok%2016\...
An exercise program should be initiated gradually. Increasingly, community organizations provide supervised group programs. The National Institute on Aging also has a range of on-line and video resources for older adults.
ACCIDENT PREVENTION In addition to exercise, attention to accident prevention is critical. Falls risk assessment is addressed above. In addition, exercise, particularly directed at balance, resistance, and aerobic training, decreases risk. Seatbelt use should be encouraged. Per mile driven, older adults are at highest risk of serious injury or death as a result of motor vehicle accidents. Assessment of the ability to drive safely is critical to motor vehicle safety (see above). With many older adults riding bicycles, motorcycles, and mopeds, patients should be encouraged to use helmets. Head injuries are common among riders and are particularly devastating to older adults; helmets mitigate this risk.
Although moderate alcohol consumption has been associated with many salutary effects, it is not without consequences for older adults who, because of age-related changes in alcohol distribution, increased brain sensitivity to its effects, and the potential for medication-alcohol interactions, are at risk for alcohol side effects at lower levels of consumption than their younger counterparts. When the definition of at least 12 drinks per year is used, 29% of older adults are classified as regular consumers: 40% of men and 21% of women. The National Institute on Alcohol Abuse and Alcoholism recommends that both men and women aged 65 consume no more than three drinks in a day and no more than seven drinks in a week, while the American Geriatrics Society recommends no more than two drinks on any single drinking occasion. Lower drinking limits or abstinence is recommended for those who take medications that interact with alcohol or who have a health condition exacerbated by alcohol. An
loading) provides benefits of increased strength, power, endurance, balance, and bone density
benefits
aExamples of balance enhancing activities include t’ai chi movements, standing yoga or ballet movements, tandem walking, standing on one leg, stepping over objects, climbing up and down steps slowly, turning, standing on heels and toes, walking on compliant surface such as foam mattresses, maintaining balance on moving vehicle such as bus or train, and dual tasking (addition of a cognitive distractor such as naming animals while balancing), etc.
bProprioceptive neuromuscular facilitation involves stretching as far as possible, then relaxing the involved muscles, then attempting to stretch further, and finally holding the maximal stretch position for at least 20 s.
cIntensity is increased by decreasing the base of support (e.g., progressing from standing on two feet while holding onto the back of a chair to standing on one foot with no hand support); by decreasing other sensory input (e.g., closing eyes or standing on a foam pillow); or by perturbing the center of mass (e.g., holding a heavy object out to one side while maintaining balance, standing on one leg while lifting other leg out behind body, or leaning forward as far as possible without falling or moving feet).
Note: 1 RM, one repetition maximum that is a measure of maximal dynamic strength: the maximal weight one can lift with a particular muscle group one time in good form; the Perceived Exertion Scale of is a self-rating of how hard one’s body is working.
Source: From MAF Singh: J Gerontol: Med Sci 57A:M274, 2002; with permission.
Page 18 of 21Print: Chapter 9. Geriatric Medicine
2/2/2012mk:@MSITStore:D:\Danny\Kuliah\Blok%2016\Kuliah%20Pakar\fisiologi%20blok%2016\...

approach to screening for heavy drinking is first to ask about heavy drinking days in the past year. If a man reports that he consumed five or more drinks in a day, or a woman reports that she consumed four or more drinks in a day, further questioning is warranted. The 10-item AUDIT (Alcohol Use Disorders Identification Test) is a validated strategy for identifying unhealthy drinking.
Disease Prevention and Early Detection IMMUNIZATIONS Although vaccine efficacy declines with age, the risks of no vaccination far outweigh the consequences of less than complete protection. Influenza vaccination is thus recommended annually, and all adults 65 should receive the pneumococcal vaccine at least once. In addition, a one-time revaccination
should be given if the original vaccination was 5 years earlier and persons were 65 years at the time of primary vaccination. Tetanus vaccinations should be administered every 10 years.
BONE HEALTH Some 70% of women 80 years have osteoporosis. Given this substantial risk, the significant morbidity and mortality associated with osteoporotic fractures, and the proven efficacy of bisphosphonates in increasing bone mineral density and preventing fractures, all women >65 years should receive dual-energy x-ray absorptiometry (DEXA) screening at least once. The most appropriate interval between screening tests has not been determined, although a minimum of 2 years is recommended to reliably measure a change in bone density. Although routine measurement of vitamin D levels is not recommended, women who are at high risk for deficiency by virtue of dietary insufficiency and/or lack of sun exposure should be considered for screening.
CANCER SCREENING The effect of cancer screening is not evident for at least 3–5 years; thus, screening is not likely to be of benefit in persons with a limited life expectancy. Individual values and preferences are clearly also important considerations.
Breast Cancer The incidence of breast cancer increases with age and peaks in the eighth decade. The sensitivity and specificity of mammography reaches its maximum in the ninth decade. Over 25% of breast cancer deaths occur in women 80 years. These facts suggest that mammographic screening would be of benefit in older women; however, only two clinical trials have examined the efficacy of mammographic screening in women 70 years, and both were inconclusive. The best supporting observational evidence comes from two Surveillance, Epidemiology, and End Results Medicare studies that found an association between screening mammography and decreased breast cancer mortality. Mammography screening in the 2 years preceding a diagnosis of breast cancer eliminated the age-related disparities in size and stage of the breast tumor at diagnosis.
Annual clinical breast examination (CBE) is a potentially attractive screening alternative to mammography, since the postmenopausal atrophy of breast tissue improves CBE sensitivity in older women compared to younger women. It is also less uncomfortable and cheaper than a mammogram. However, it should be used to complement mammographic screening and reserved as a stand alone strategy only for women who refuse or cannot undergo mammography.
Prostate Cancer Prostate cancer screening in older men is a particularly challenging topic as many more older men die with prostate cancer than from it. Nonetheless, 92% of prostate cancer deaths occur in men who are >65 years. Although prostate cancer can be detected earlier via prostate-specific antigen testing,
Page 19 of 21Print: Chapter 9. Geriatric Medicine
2/2/2012mk:@MSITStore:D:\Danny\Kuliah\Blok%2016\Kuliah%20Pakar\fisiologi%20blok%2016\...

mortality from prostate cancer has not been reduced as a result of screening. The U.S. Preventive Services Task Force has concluded that evidence to recommend for or against screening is lacking. Other organizations such as the American Cancer Society and American Urological Society recommend screening among those with at least a 10-year life expectancy. The matter is complicated by the fact that techniques to treat prostate cancer often greatly affect quality of life. Furthermore, we are not able to reliably predict whether a particular prostate cancer is life-threatening. Given the uncertainties, PSA screening should be reserved for the most robust of older men and only after a thorough discussion of the arguments for and against screening.
Colorectal Cancer Annual or biennial fecal occult blood testing (FOBT) reduces mortality in those up to age 80. Other screening options include sigmoidoscopy (every 5 years), FOBT and sigmoidoscopy (every 5 years), double-contrast barium enema (every 5–10 years), and colonoscopy (every 10 years). No one method has been shown to be superior, and all methods are cost effective. Digital rectal examination (DRE) alone or with a FOBT is not recommended (though DRE is used to screen for prostate cancer). The choice of a colorectal cancer screening strategy is based on many considerations, including procedure risk. Colonoscopy might seem the most attractive option; the colon can be completely visualized and biopsies taken if the examination is positive. If the examination is negative, it does not need to be repeated for 10 years. However, adequate preparation requires lower extremity strength and mobility, and the ability to tolerate substantial fluid losses. Furthermore, the procedure has a small risk of bowel perforation or bleeding. Yet about half of colon cancers occur beyond the reach of a sigmoidoscope.
Lung Cancer Although lung cancer is also a leading killer, no screening interventions have been shown to be effective.
DISEASE RISK MODIFICATION Longitudinal studies are providing evidence that risk factor modification, especially smoking cessation and blood pressure reduction, particularly in mid-life but also up to age 75, results in greater gains in life-years than do medical and surgical therapies, especially in men. In addition, lower levels of risk factors in mid-life are associated with survival free of major morbidity to age 85. Although lifestyle modifications in mid-life are important, modifications even late in life may make a difference. A person is never too old to benefit from smoking cessation.
Older adults are also at risk for obesity, which is becoming more common among successive birth cohorts. Among men, 33.4% of those 65–74 years are obese compared to 20.4% among those >75 years. For women, the comparable figures are 38.8% and 25.1%. Weight loss in obese older adults has the potential advantage of improving mobility and decreasing the severity of comorbidities. Nonetheless, it should be pursued cautiously and be coupled with aerobic and resistance training, since many obese persons are relatively sarcopenic. No data confirm the efficacy and safety of pharmacotherapies for obesity in older persons. Although bariatric surgery has higher perioperative morbidity/mortality in older adults, if successful it can also result in improvements in the severity of comorbidities.
Further Readings Brown JS et al: The sensitivity and specificity of a simple test to distinguish between urge and stress urinary incontinence. Ann Intern Med 144:715, 2006 [PMID: 16702587] Cassel CK et al (eds): Geriatric Medicine: An Evidence-Based Approach, 4th ed. New York, Springer-
Page 20 of 21Print: Chapter 9. Geriatric Medicine
2/2/2012mk:@MSITStore:D:\Danny\Kuliah\Blok%2016\Kuliah%20Pakar\fisiologi%20blok%2016\...
Verlag, 2003 Kirkland JL et al: Adipogenesis and aging: Does aging make fat go MAD? Exp Gerontol 37:757, 2002 [PMID: 12175476] Perls T, Terry D: Understanding the determinants of exceptional longevity. Ann Intern Med 139:445, 2003 [PMID: 12965974] Reuben DB et al: Geriatrics At Your Fingertips: 2006–2007, 8th ed. New York: The American Geriatrics Society, 2006 Tinetti ME et al: Potential pitfalls of disease-specific guidelines for patients with multiple conditions. N Engl J Med 351:2870, 2004 [PMID: 15625341] Walter LC et al: Screening for colorectal, breast, and cervical cancer in the elderly: A review of the evidence. Am J Med 118:1078, 2005 [PMID: 16194635]
Copyright © The McGraw-Hill Companies. All rights reserved. Privacy Notice. Any use is subject to the Terms of Use and Notice. Additional Credits and Copyright Information.
Page 21 of 21Print: Chapter 9. Geriatric Medicine
2/2/2012mk:@MSITStore:D:\Danny\Kuliah\Blok%2016\Kuliah%20Pakar\fisiologi%20blok%2016\...