far lateral and transcondylar approaches
TRANSCRIPT

NEUROSURGERY VOLUME 61 | NUMBER 4 | OCTOBER 2007 SUPPLEMENT 4 | S4-211
CHAPTER 11
FAR LATERAL AND TRANSCONDYLAR APPROACHES
Neurosurgery 61:S4-211–S4-228, 2007 DOI: 10.1227/01.NEU.0000280028.00006.98 www.neurosurgery-online.com
The basic far lateral approach is a low suboccipital approach thatextends up to, but does not include removal of, part of the atlantal oroccipital condyles. The far lateral approach usually includes a suboc-cipital craniectomy or craniotomy with removal of at least half of theposterior arch of the atlas, dissection of the muscles along the postero-lateral aspect of the craniocervical junction to permit an adequate expo-sure of the Cl transverse process and the suboccipital triangle, andearly identification of the vertebral artery either above the posteriorarch of the atlas or in its ascending course between the transverseprocesses of the atlas and axis. The far lateral approach provides accessfor the following three approaches: 1) the transcondylar approachdirected through the occipital condyle or the atlanto-occipital joint andadjoining parts of the condyles, 2) the supracondylar approach directedthrough the part of the occipital bone above the occipital condyle, and3) the paracondylar exposure directed through the area lateral to theoccipital condyle. The transcondylar extension, accomplished bydrilling the occipital condyle, allows a more lateral approach and pro-vides access to the lower clivus and premedullary area. The supra-condylar approach provides access to the region of and medial to thehypoglossal canal and jugular tubercle. The paracondylar approach,which includes drilling of the jugular process of the occipital bone inthe area lateral to the occipital condyle, accesses the posterior part ofthe jugular foramen, and, if needed, the posterior aspect of the facialnerve and mastoid on the lateral side of the jugular foramen.
The basic far lateral approach without drilling of the occipitalcondyle may be all that is required to reach some lesions located alongthe anterolateral margin of the foramen magnum. However, it alsoprovides a route through which the transcondylar, supracondylar, andparacondylar approaches and several modifications of theseapproaches can be completed. The transcondylar exposures can be cat-egorized into several variants. One variant is an atlanto-occipitaltransarticular approach, in which the adjacent posterior part of theoccipital condyle and/or the superior articular facet of C1 is removedto facilitate completion of a circular dural incision, permitting the ver-tebral artery with the surrounding cuff of dura to be mobilized. A moreextensive removal of the articular surfaces and condyles can be per-formed to gain access to extradural lesions situated along the anteriorand lateral margins of the foramen magnum. Another variant, theoccipital transcondylar variant, is directed above the atlanto-occipitaljoint through the occipital condyle and below the hypoglossal canal toaccess the lower clivus and the area in front of the medulla. The supra-condylar approach directed above the occipital condyle can also bevaried, depending on the pathology to be exposed. The supracondylarexposure can be directed above the occipital condyle to the hypoglos-sal canal or both above and below the hypoglossal canal to the lateralside of the clivus. In the transtubercular variant of the supracondylarapproach, the prominence of the jugular tubercle that blocks access tothe brainstem and cistern in front of the glossopharyngeal, vagus, andaccessory nerves is removed extradurally to increase visualization ofthe area in front of the brainstem and to expose the origin of a poste-rior inferior cerebellar artery that arises from the distal part of the ver-tebral artery near the midline. The paracondylar approach also hasseveral variants. In the transjugular variant, the exposure is directedlateral to the condyle through the jugular process of the occipital boneto the posterior surface of the jugular bulb. The approach can also beextended lateral to the jugular foramen into the posterior aspect of themastoid to access the mastoid segment of the facial nerve and the sty-lomastoid foramen.
In the standard posterior and posterolateral approaches, an under-standing of the individual suboccipital muscles is not essential.However, these muscles provide important landmarks for the far lateralapproach and its modifications. In this description, the muscles arereflected separately, but, during an operation, the scalp and musclessuperficial to the muscles forming the suboccipital triangle are reflectedfrom the suboccipital area in a single layer, leaving a musculofascial cuffattached along the superior nuchal line for closure. The procedure hasbeen performed through either a horseshoe type suboccipital flap, a C-shaped retroauricular incision similar to that shown in the section on thejugular foramen, or a hockey stick incision that has a vertical lateral limbbehind the ear with a medial extension along the superior nuchal line.We prefer the horseshoe scalp flap that begins in the midline, approxi-mately 5 cm below the external occipital protuberance, is directedupward to the external occipital protuberance, turns laterally just belowthe superior nuchal line, reaches the mastoid area, and turns down-ward in front of the posterior border of the sternocleidomastoid muscleonto the lateral aspect of the neck below the mastoid tip and where thetransverse process of the atlas can be palpated through the skin. Thescalp flap is reflected downward with the muscular layer that includesthe sternocleidomastoid, trapezius, and splenius, longissimus, and semi-spinalis capitis muscles. The three muscles, the superior and inferioroblique and the rectus capitis posterior, forming the suboccipital trian-gle are reflected separately to expose the vertebral artery.
The vertebral artery, above the transverse foramen of the axis, veerslaterally to reach the transverse foramen of the atlas, which is situatedfurther lateral than the transverse foramen of the axis. The artery,after ascending through the transverse process of the atlas, is locatedon the medial side of the rectus capitis lateralis muscle. From here, theartery turns medially behind the lateral mass of the atlas and theatlanto-occipital joint and is pressed into the groove on the uppersurface of the posterior arch of the atlas, where it courses in the floorof the suboccipital triangle and is covered behind the triangle by thesemispinalis capitis muscle. The first cervical nerve courses on thelower surface of the artery between the artery and the posterior archof the atlas. After passing medially above the lateral part of the pos-terior arch of the atlas, the artery enters the vertebral canal by pass-ing below the lower, arched border of the posterior atlanto-occipitalmembrane, which transforms the sulcus in which the artery courseson the upper edge of the posterior arch of the atlas into an osseofi-brous casing that may ossify, transforming it into a complete orincomplete bony canal surrounding the artery.
The third segment of the vertebral artery, the segment locatedbetween the C1 transverse process and the dural entrance, gives riseto muscular branches and the posterior meningeal artery. The muscu-lar branches arise as the artery exits the transverse foramen of C1 andcourses behind the lateral mass of the atlas to supply the deep mus-cles and anastomose with the occipital and ascending and deep cer-vical arteries. Some of the muscular branches may need to be dividedto mobilize and transpose the vertebral artery. The posteriormeningeal artery arises from the posterior surface of the vertebralartery as it passes behind the lateral mass or above the posterior archof the atlas or just before penetrating the dura in the region of theforamen magnum, but it may also have an intradural origin from thevertebral artery, in which case it pierces the arachnoid over the cis-terna magna to reach the dura. Six to eight percent of posterior infe-rior cerebellar arteries arise extradurally and penetrate the dura withthe vertebral artery.
S4-212 | VOLUME 61 | NUMBER 4 | OCTOBER 2007 SUPPLEMENT 4 www.neurosurgery-online.com
RHOTON
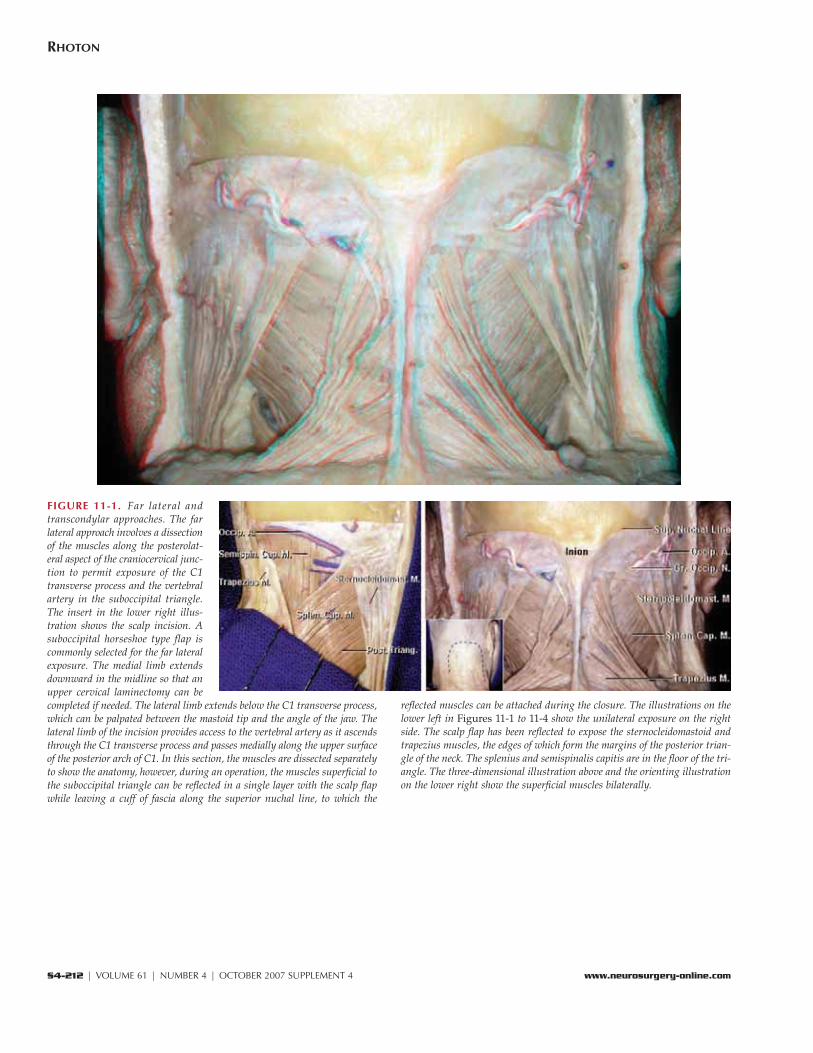
FIGURE 11-1. Far lateral andtranscondylar approaches. The farlateral approach involves a dissectionof the muscles along the posterolat-eral aspect of the craniocervical junc-tion to permit exposure of the C1transverse process and the vertebralartery in the suboccipital triangle.The insert in the lower right illus-tration shows the scalp incision. Asuboccipital horseshoe type flap iscommonly selected for the far lateralexposure. The medial limb extendsdownward in the midline so that anupper cervical laminectomy can becompleted if needed. The lateral limb extends below the C1 transverse process,which can be palpated between the mastoid tip and the angle of the jaw. Thelateral limb of the incision provides access to the vertebral artery as it ascendsthrough the C1 transverse process and passes medially along the upper surfaceof the posterior arch of C1. In this section, the muscles are dissected separatelyto show the anatomy, however, during an operation, the muscles superficial tothe suboccipital triangle can be reflected in a single layer with the scalp flapwhile leaving a cuff of fascia along the superior nuchal line, to which the
reflected muscles can be attached during the closure. The illustrations on thelower left in Figures 11-1 to 11-4 show the unilateral exposure on the rightside. The scalp flap has been reflected to expose the sternocleidomastoid andtrapezius muscles, the edges of which form the margins of the posterior trian-gle of the neck. The splenius and semispinalis capitis are in the floor of the tri-angle. The three-dimensional illustration above and the orienting illustrationon the lower right show the superficial muscles bilaterally.
NEUROSURGERY VOLUME 61 | NUMBER 4 | OCTOBER 2007 SUPPLEMENT 4 | S4-213
FAR LATERAL APPROACHES
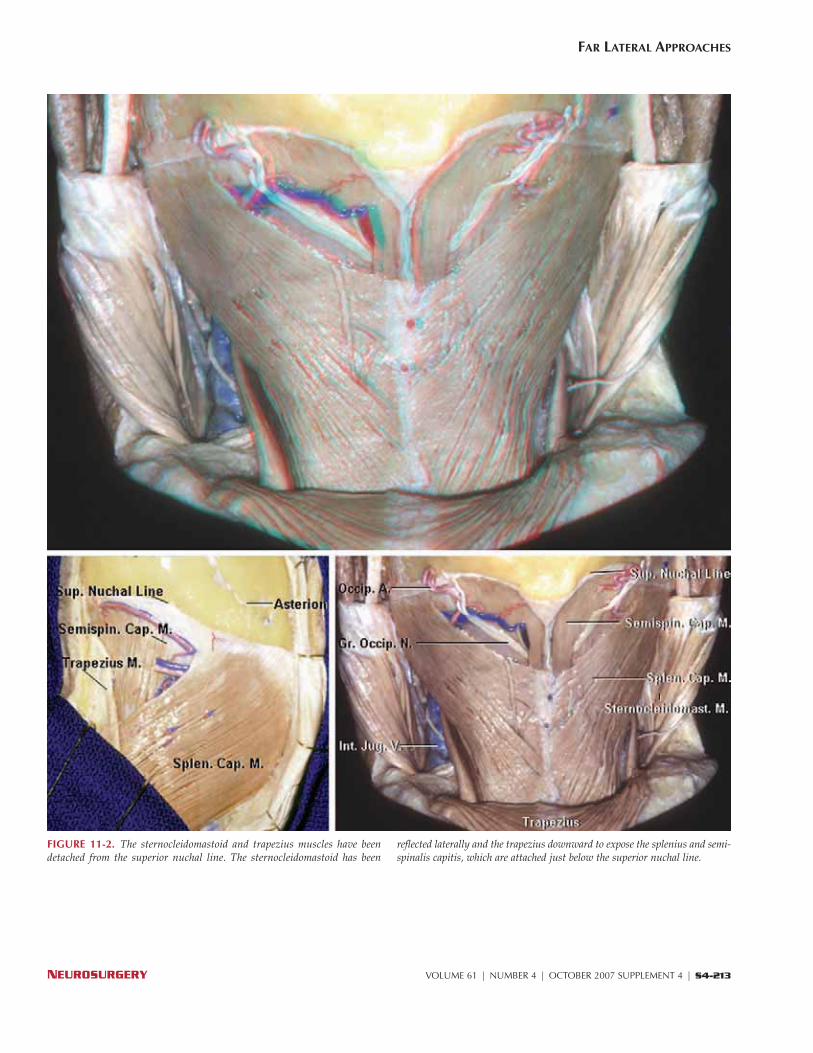
FIGURE 11-2. The sternocleidomastoid and trapezius muscles have beendetached from the superior nuchal line. The sternocleidomastoid has been
reflected laterally and the trapezius downward to expose the splenius and semi-spinalis capitis, which are attached just below the superior nuchal line.
S4-214 | VOLUME 61 | NUMBER 4 | OCTOBER 2007 SUPPLEMENT 4 www.neurosurgery-online.com
RHOTON
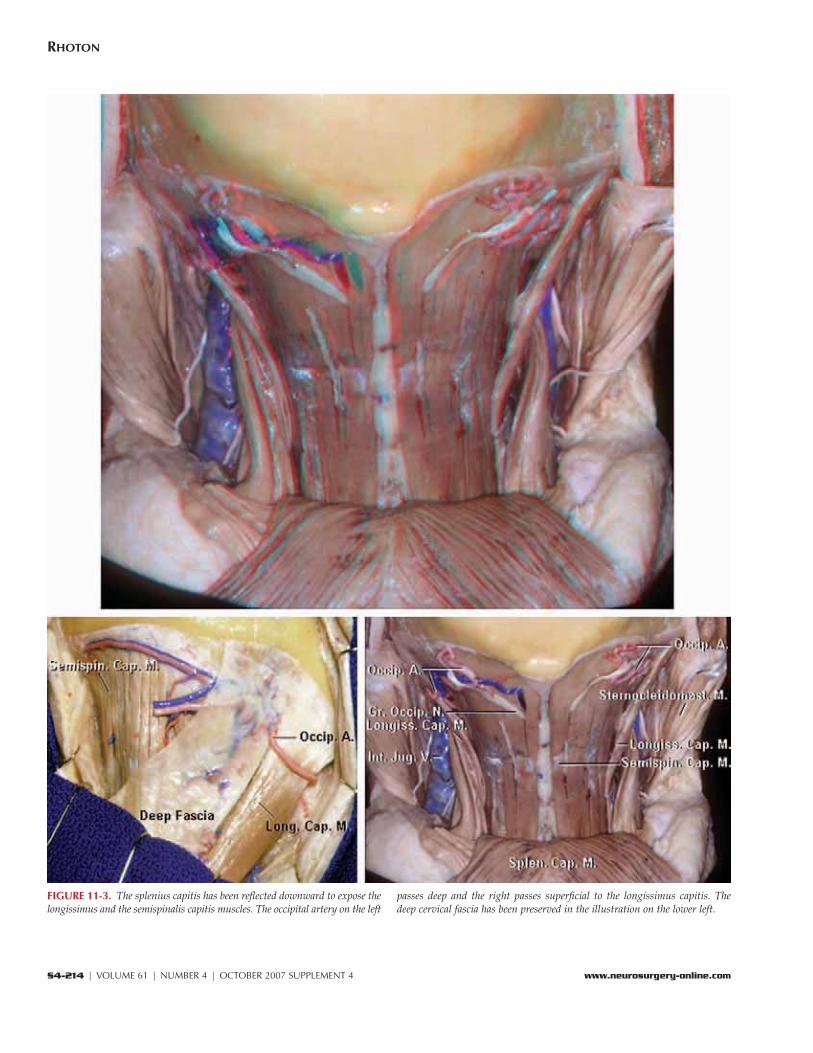
FIGURE 11-3. The splenius capitis has been reflected downward to expose thelongissimus and the semispinalis capitis muscles. The occipital artery on the left
passes deep and the right passes superficial to the longissimus capitis. Thedeep cervical fascia has been preserved in the illustration on the lower left.
NEUROSURGERY VOLUME 61 | NUMBER 4 | OCTOBER 2007 SUPPLEMENT 4 | S4-215
FAR LATERAL APPROACHES
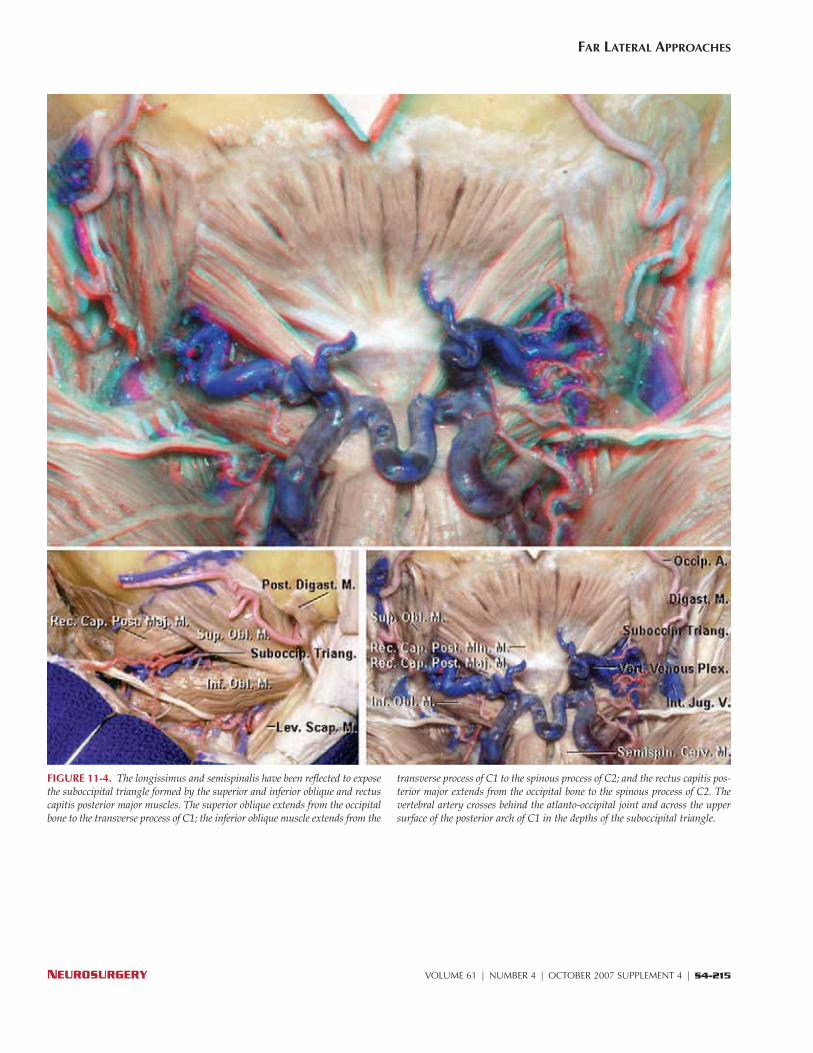
FIGURE 11-4. The longissimus and semispinalis have been reflected to exposethe suboccipital triangle formed by the superior and inferior oblique and rectuscapitis posterior major muscles. The superior oblique extends from the occipitalbone to the transverse process of C1; the inferior oblique muscle extends from the
transverse process of C1 to the spinous process of C2; and the rectus capitis pos-terior major extends from the occipital bone to the spinous process of C2. Thevertebral artery crosses behind the atlanto-occipital joint and across the uppersurface of the posterior arch of C1 in the depths of the suboccipital triangle.
S4-216 | VOLUME 61 | NUMBER 4 | OCTOBER 2007 SUPPLEMENT 4 www.neurosurgery-online.com
RHOTON
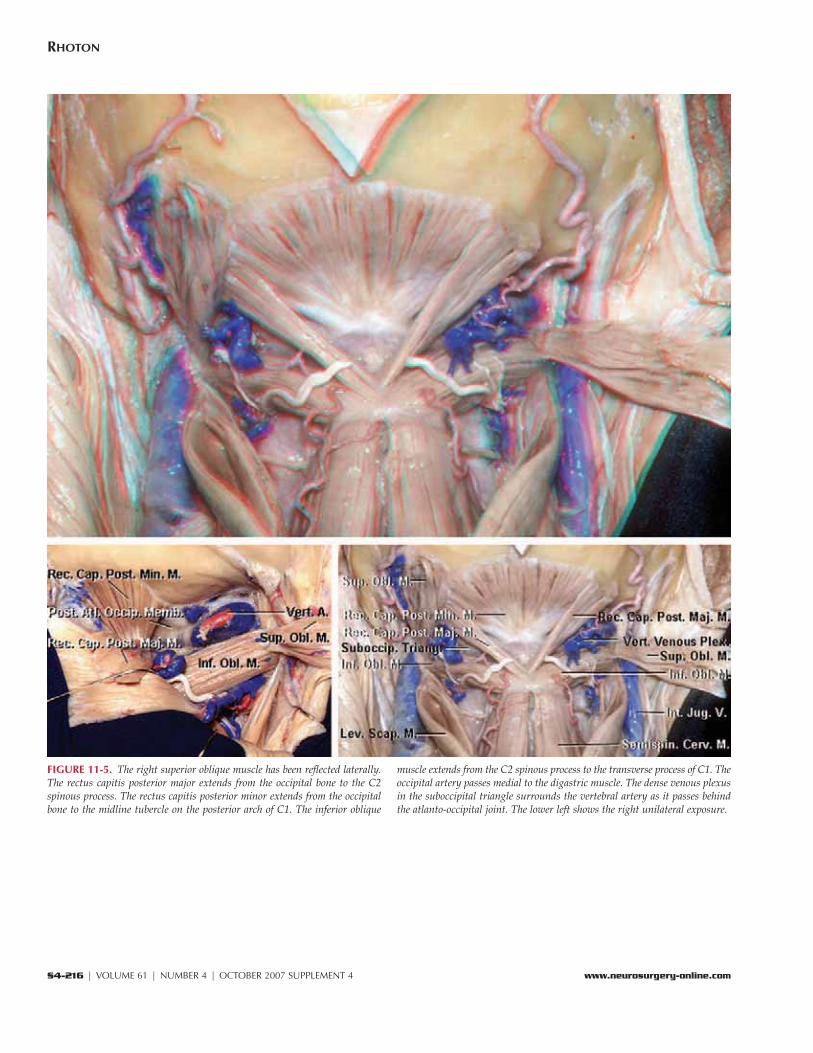
FIGURE 11-5. The right superior oblique muscle has been reflected laterally.The rectus capitis posterior major extends from the occipital bone to the C2spinous process. The rectus capitis posterior minor extends from the occipitalbone to the midline tubercle on the posterior arch of C1. The inferior oblique
muscle extends from the C2 spinous process to the transverse process of C1. Theoccipital artery passes medial to the digastric muscle. The dense venous plexusin the suboccipital triangle surrounds the vertebral artery as it passes behindthe atlanto-occipital joint. The lower left shows the right unilateral exposure.
NEUROSURGERY VOLUME 61 | NUMBER 4 | OCTOBER 2007 SUPPLEMENT 4 | S4-217
FAR LATERAL APPROACHES
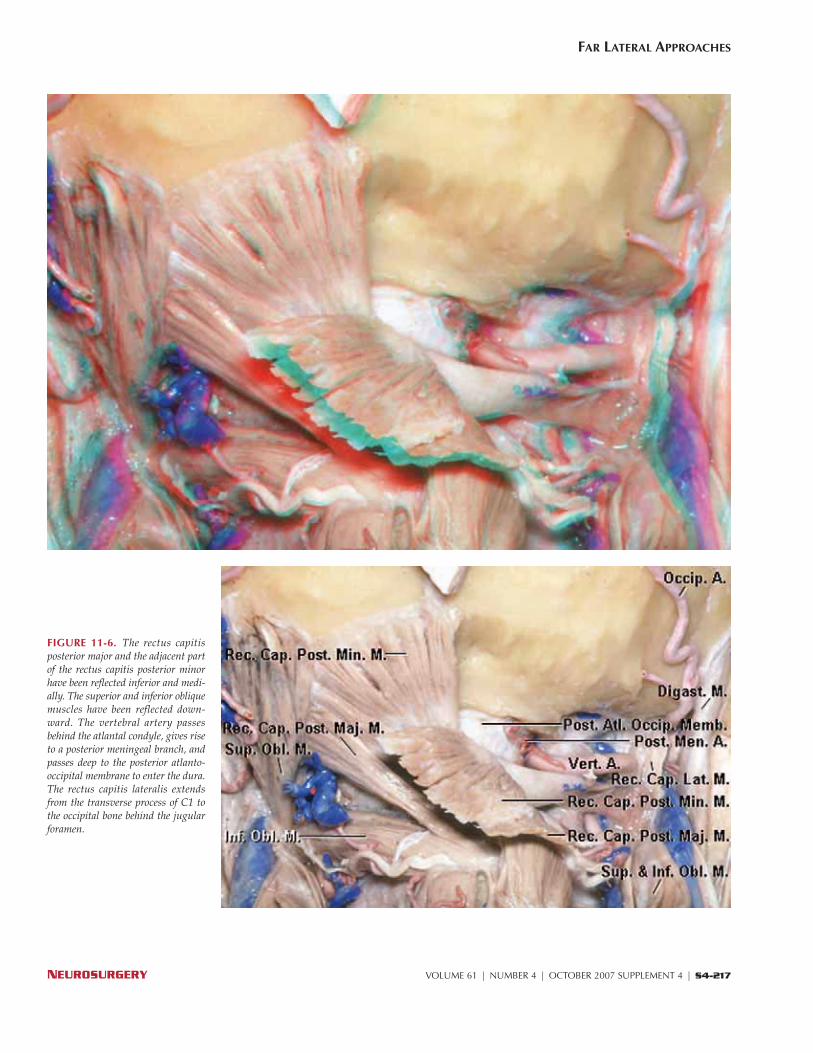
FIGURE 11-6. The rectus capitisposterior major and the adjacent partof the rectus capitis posterior minorhave been reflected inferior and medi-ally. The superior and inferior obliquemuscles have been reflected down-ward. The vertebral artery passesbehind the atlantal condyle, gives riseto a posterior meningeal branch, andpasses deep to the posterior atlanto-occipital membrane to enter the dura.The rectus capitis lateralis extendsfrom the transverse process of C1 tothe occipital bone behind the jugularforamen.
S4-218 | VOLUME 61 | NUMBER 4 | OCTOBER 2007 SUPPLEMENT 4 www.neurosurgery-online.com
RHOTON
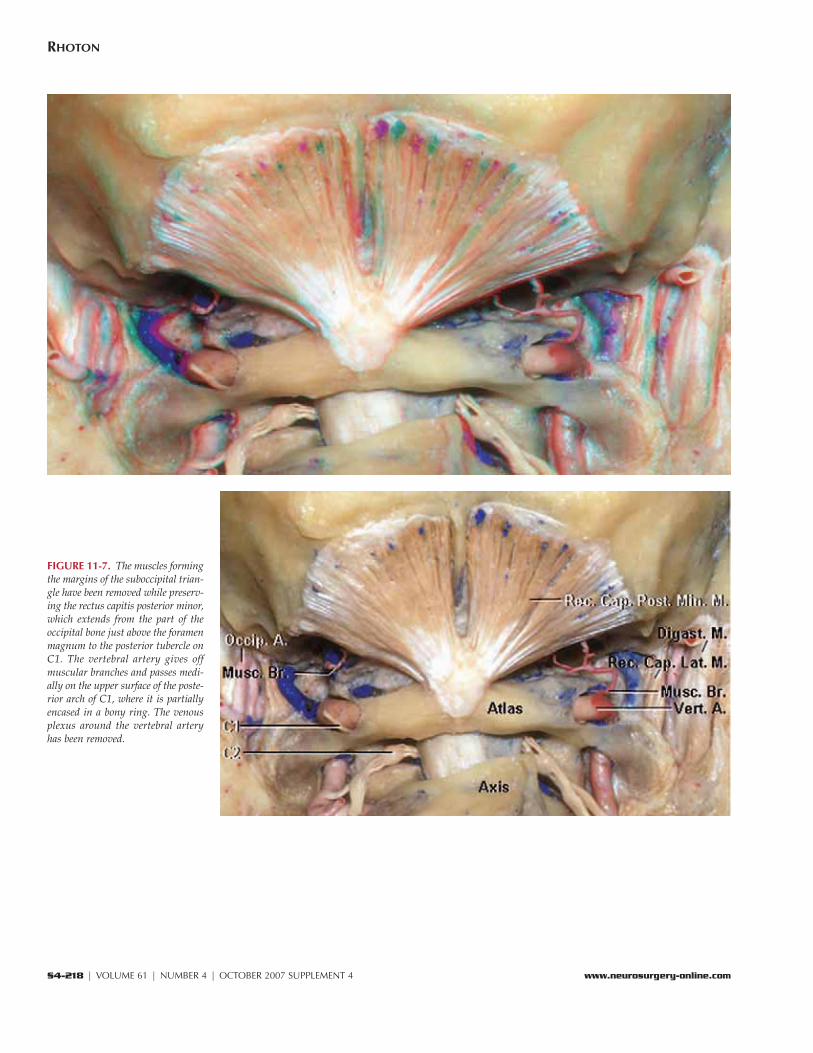
FIGURE 11-7. The muscles formingthe margins of the suboccipital trian-gle have been removed while preserv-ing the rectus capitis posterior minor,which extends from the part of theoccipital bone just above the foramenmagnum to the posterior tubercle onC1. The vertebral artery gives offmuscular branches and passes medi-ally on the upper surface of the poste-rior arch of C1, where it is partiallyencased in a bony ring. The venousplexus around the vertebral arteryhas been removed.
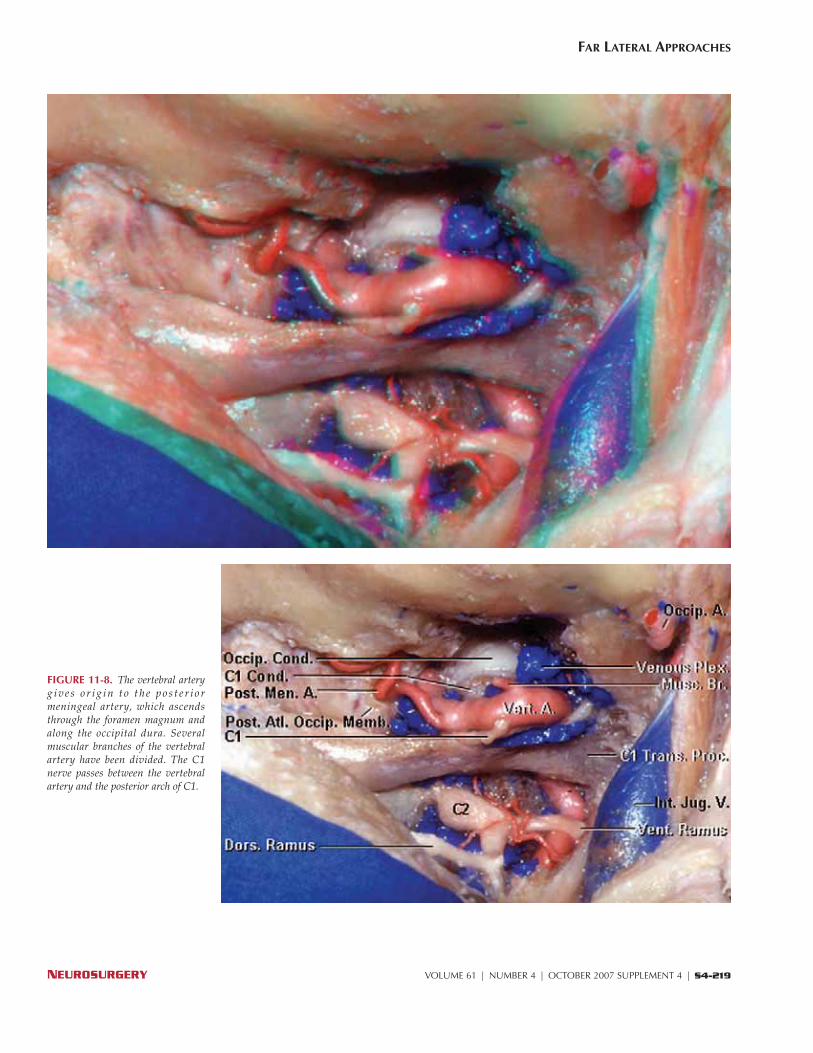
FIGURE 11-8. The vertebral arteryg i v e s o r i g i n t o t h e p o s t e r i o rmeningeal artery, which ascendsthrough the foramen magnum andalong the occipital dura. Severalmuscular branches of the vertebralartery have been divided. The C1nerve passes between the vertebralartery and the posterior arch of C1.
NEUROSURGERY VOLUME 61 | NUMBER 4 | OCTOBER 2007 SUPPLEMENT 4 | S4-219
FAR LATERAL APPROACHES
S4-220 | VOLUME 61 | NUMBER 4 | OCTOBER 2007 SUPPLEMENT 4 www.neurosurgery-online.com
RHOTON
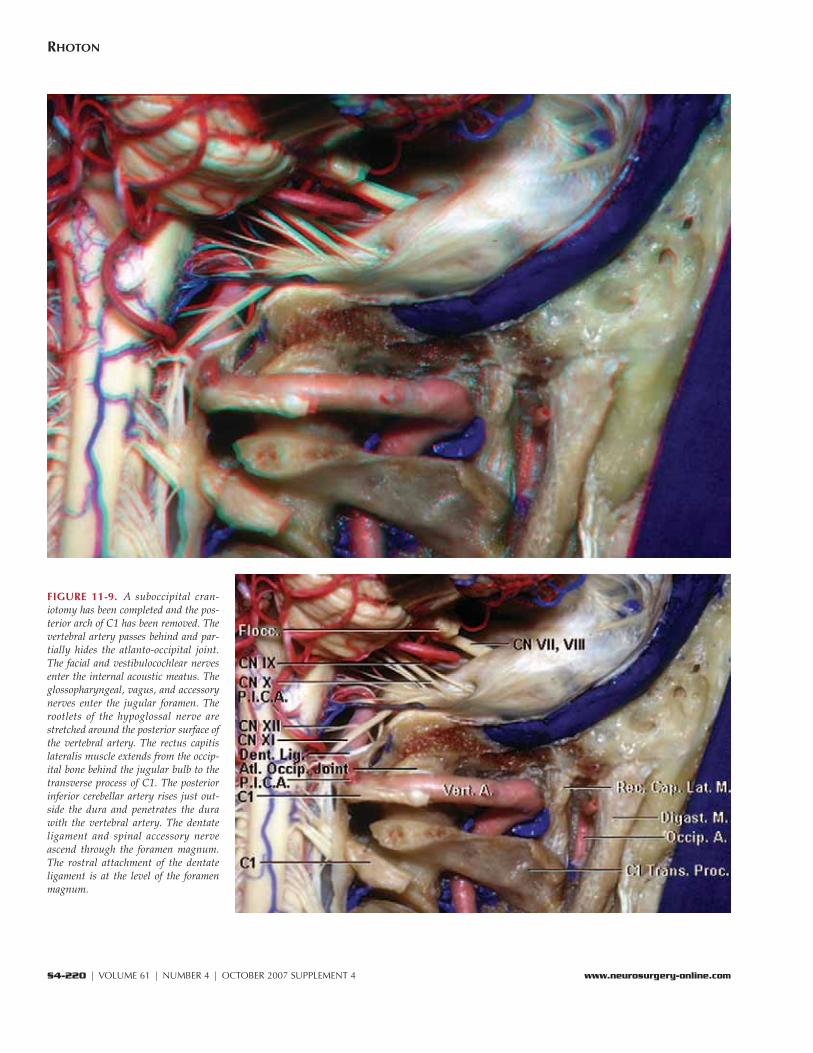
FIGURE 11-9. A suboccipital cran-iotomy has been completed and the pos-terior arch of C1 has been removed. Thevertebral artery passes behind and par-tially hides the atlanto-occipital joint.The facial and vestibulocochlear nervesenter the internal acoustic meatus. Theglossopharyngeal, vagus, and accessorynerves enter the jugular foramen. Therootlets of the hypoglossal nerve arestretched around the posterior surface ofthe vertebral artery. The rectus capitislateralis muscle extends from the occip-ital bone behind the jugular bulb to thetransverse process of C1. The posteriorinferior cerebellar artery rises just out-side the dura and penetrates the durawith the vertebral artery. The dentateligament and spinal accessory nerveascend through the foramen magnum.The rostral attachment of the dentateligament is at the level of the foramenmagnum.
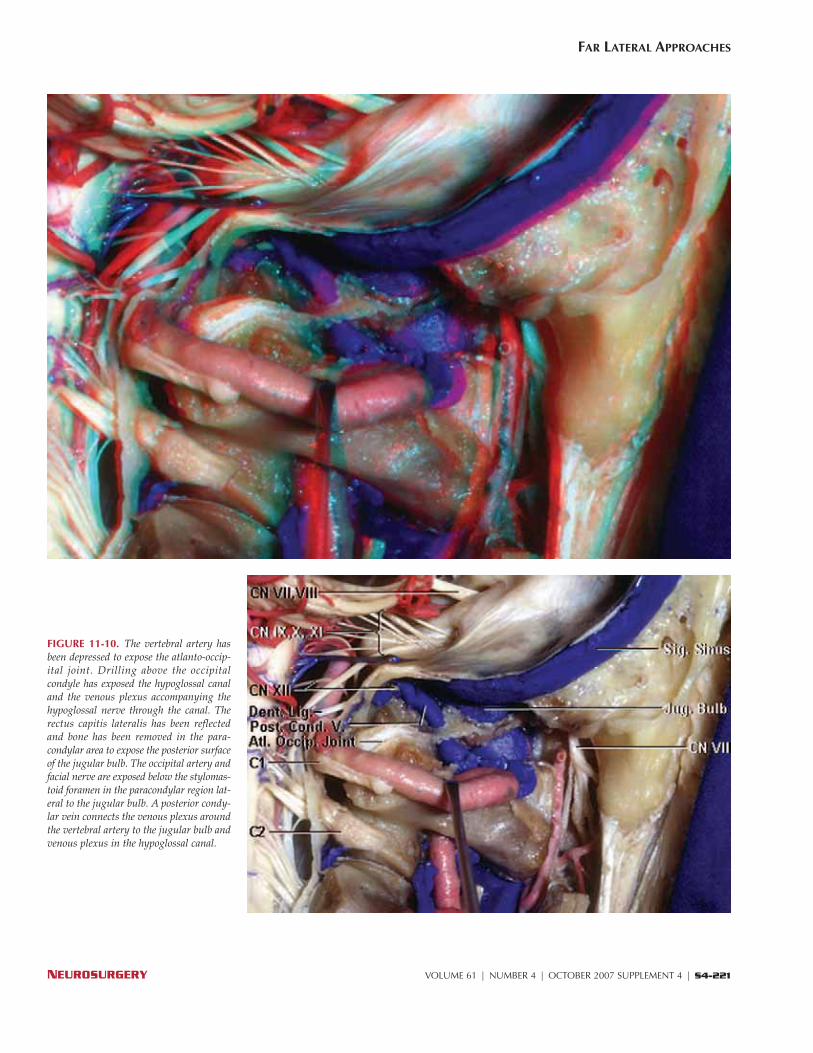
FIGURE 11-10. The vertebral artery hasbeen depressed to expose the atlanto-occip-ital joint. Drilling above the occipitalcondyle has exposed the hypoglossal canaland the venous plexus accompanying thehypoglossal nerve through the canal. Therectus capitis lateralis has been reflectedand bone has been removed in the para-condylar area to expose the posterior surfaceof the jugular bulb. The occipital artery andfacial nerve are exposed below the stylomas-toid foramen in the paracondylar region lat-eral to the jugular bulb. A posterior condy-lar vein connects the venous plexus aroundthe vertebral artery to the jugular bulb andvenous plexus in the hypoglossal canal.
NEUROSURGERY VOLUME 61 | NUMBER 4 | OCTOBER 2007 SUPPLEMENT 4 | S4-221
FAR LATERAL APPROACHES
S4-222 | VOLUME 61 | NUMBER 4 | OCTOBER 2007 SUPPLEMENT 4 www.neurosurgery-online.com
RHOTON
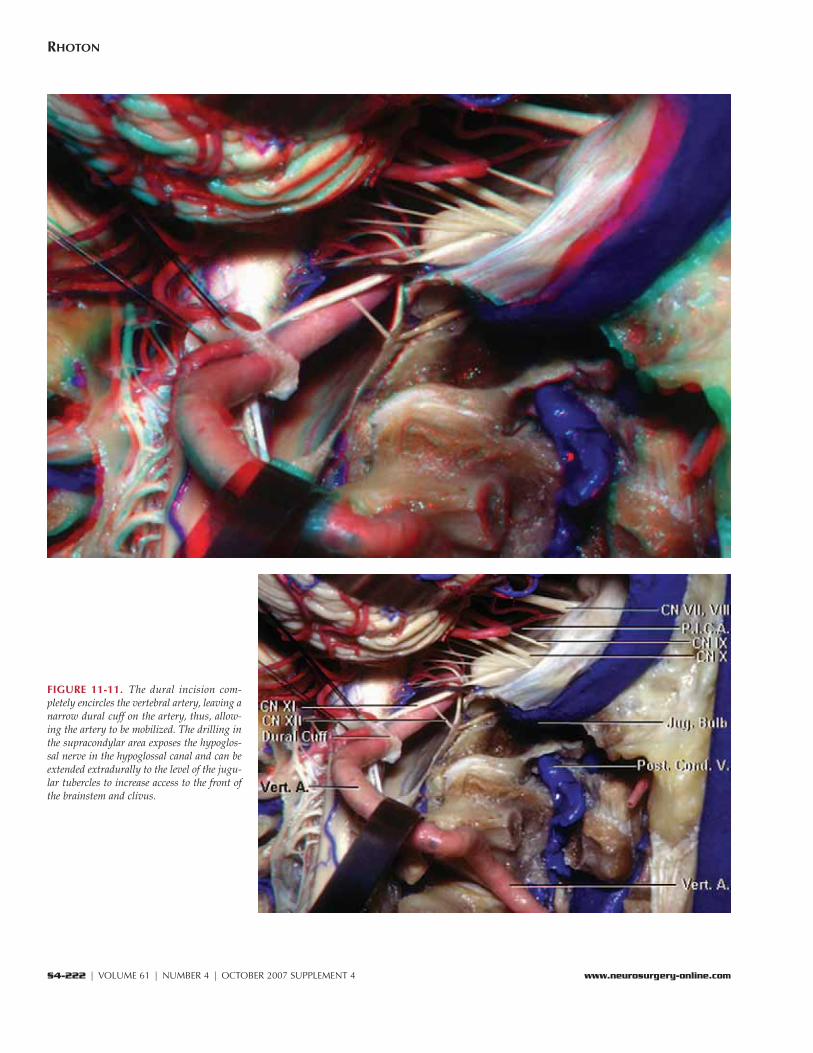
FIGURE 11-11. The dural incision com-pletely encircles the vertebral artery, leaving anarrow dural cuff on the artery, thus, allow-ing the artery to be mobilized. The drilling inthe supracondylar area exposes the hypoglos-sal nerve in the hypoglossal canal and can beextended extradurally to the level of the jugu-lar tubercles to increase access to the front ofthe brainstem and clivus.
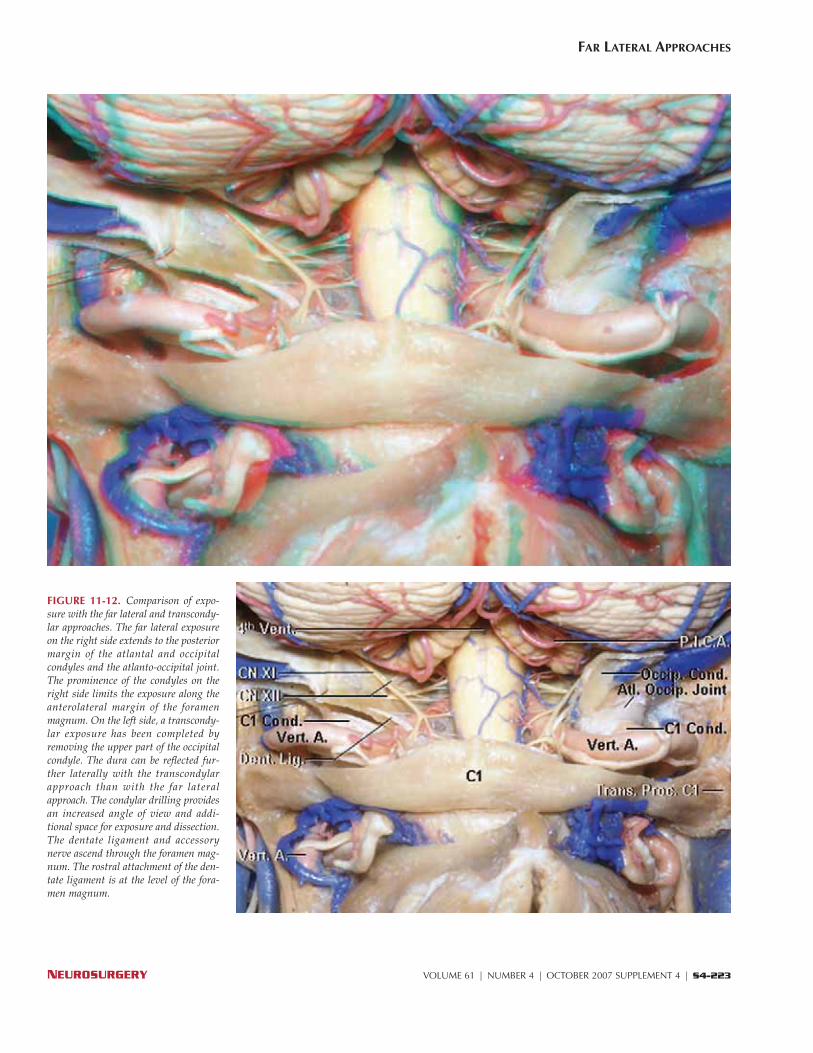
FIGURE 11-12. Comparison of expo-sure with the far lateral and transcondy-lar approaches. The far lateral exposureon the right side extends to the posteriormargin of the atlantal and occipitalcondyles and the atlanto-occipital joint.The prominence of the condyles on theright side limits the exposure along theanterolateral margin of the foramenmagnum. On the left side, a transcondy-lar exposure has been completed byremoving the upper part of the occipitalcondyle. The dura can be reflected fur-ther laterally with the transcondylarapproach than with the far lateralapproach. The condylar drilling providesan increased angle of view and addi-tional space for exposure and dissection.The dentate ligament and accessorynerve ascend through the foramen mag-num. The rostral attachment of the den-tate ligament is at the level of the fora-men magnum.
NEUROSURGERY VOLUME 61 | NUMBER 4 | OCTOBER 2007 SUPPLEMENT 4 | S4-223
FAR LATERAL APPROACHES
S4-224 | VOLUME 61 | NUMBER 4 | OCTOBER 2007 SUPPLEMENT 4 www.neurosurgery-online.com
RHOTON
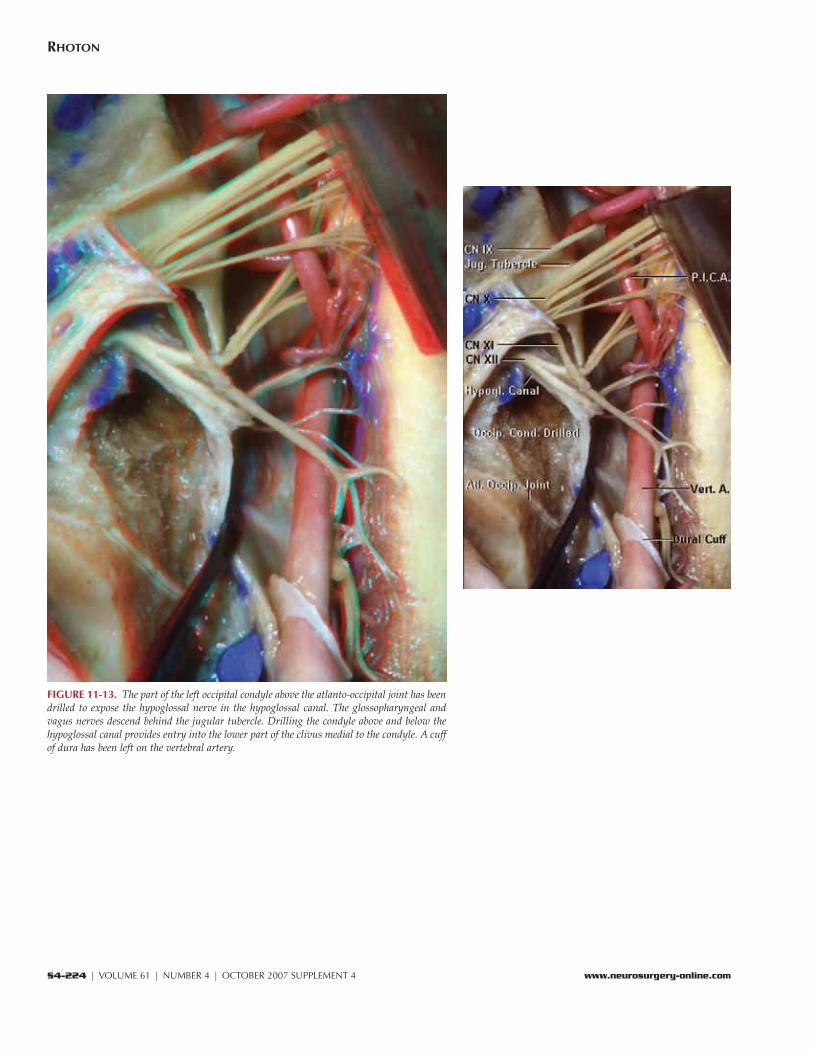
FIGURE 11-13. The part of the left occipital condyle above the atlanto-occipital joint has beendrilled to expose the hypoglossal nerve in the hypoglossal canal. The glossopharyngeal andvagus nerves descend behind the jugular tubercle. Drilling the condyle above and below thehypoglossal canal provides entry into the lower part of the clivus medial to the condyle. A cuffof dura has been left on the vertebral artery.
NEUROSURGERY VOLUME 61 | NUMBER 4 | OCTOBER 2007 SUPPLEMENT 4 | S4-225
FAR LATERAL APPROACHES
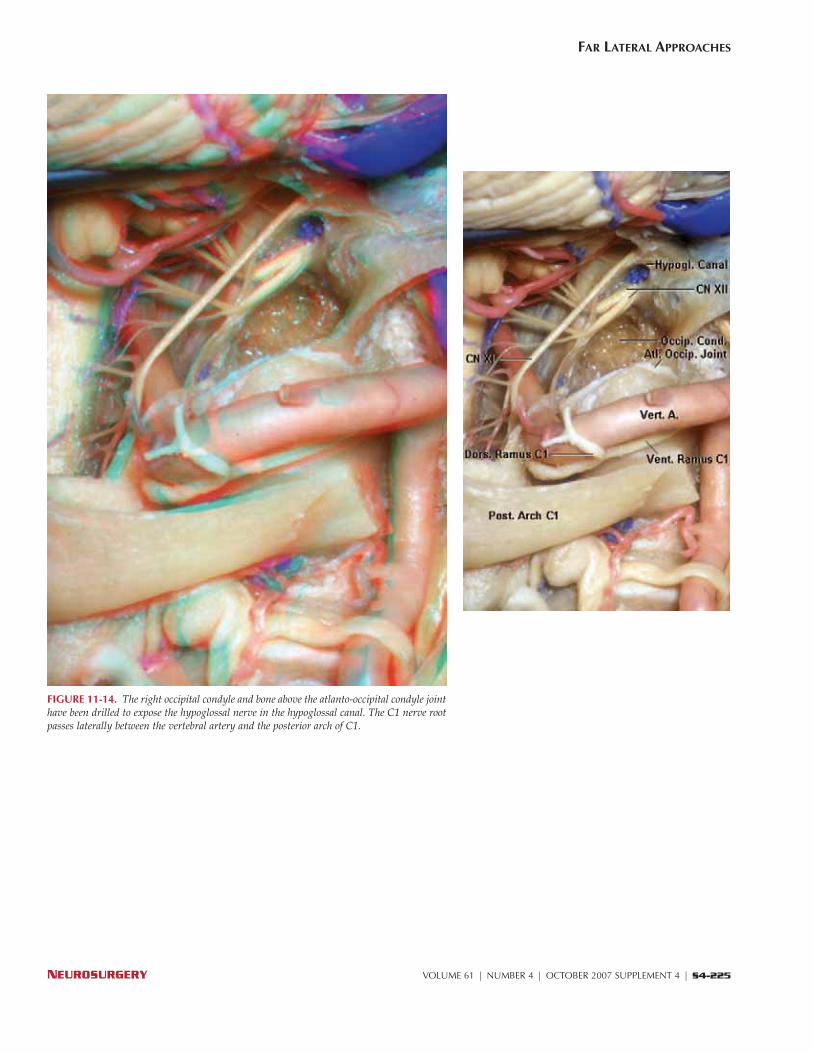
FIGURE 11-14. The right occipital condyle and bone above the atlanto-occipital condyle jointhave been drilled to expose the hypoglossal nerve in the hypoglossal canal. The C1 nerve rootpasses laterally between the vertebral artery and the posterior arch of C1.

S4-226 | VOLUME 61 | NUMBER 4 | OCTOBER 2007 SUPPLEMENT 4 www.neurosurgery-online.com
RHOTON
FIGURE 11-15. Another specimen with the brainstem removed. The boneabove the occipital condyle has been removed to expose the hypoglossal nervein the hypoglossal canal. The glossopharyngeal, vagus, and accessory nervescross the jugular tubercle. The jugular bulb is located lateral to the occipitalcondyle and can be exposed by drilling the occipital bone in the paracondylararea.
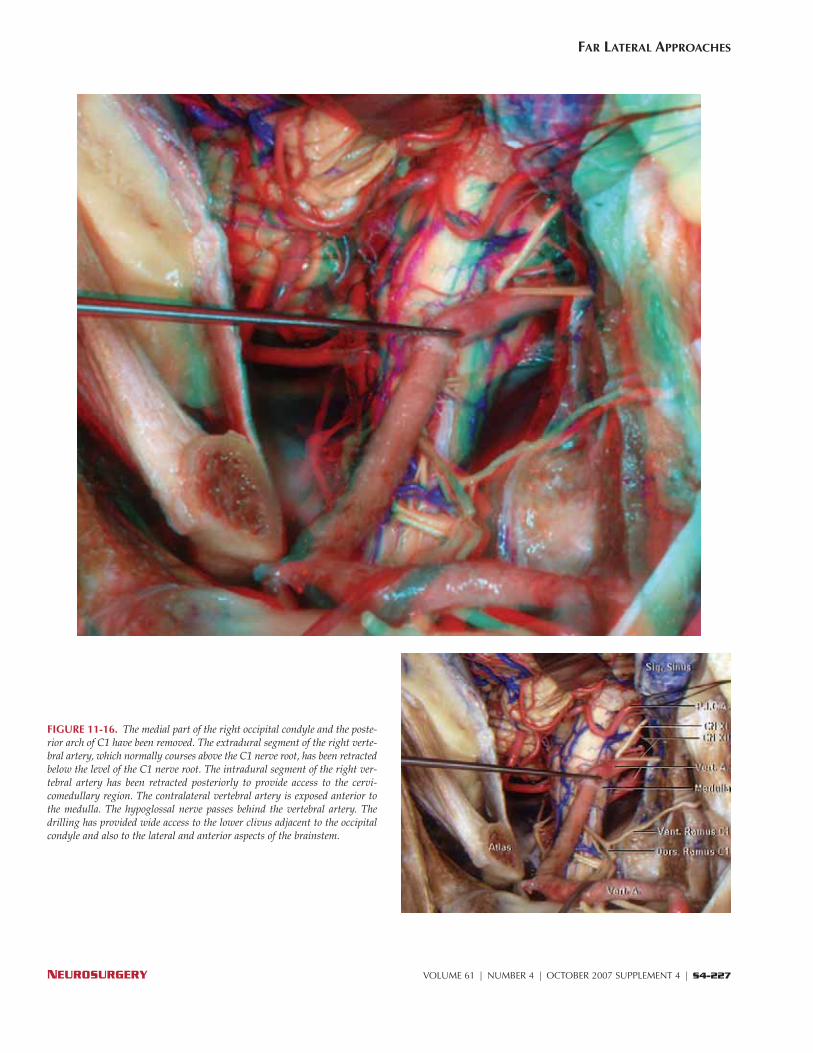
FIGURE 11-16. The medial part of the right occipital condyle and the poste-rior arch of C1 have been removed. The extradural segment of the right verte-bral artery, which normally courses above the C1 nerve root, has been retractedbelow the level of the C1 nerve root. The intradural segment of the right ver-tebral artery has been retracted posteriorly to provide access to the cervi-comedullary region. The contralateral vertebral artery is exposed anterior tothe medulla. The hypoglossal nerve passes behind the vertebral artery. Thedrilling has provided wide access to the lower clivus adjacent to the occipitalcondyle and also to the lateral and anterior aspects of the brainstem.
NEUROSURGERY VOLUME 61 | NUMBER 4 | OCTOBER 2007 SUPPLEMENT 4 | S4-227
FAR LATERAL APPROACHES
S4-228 | VOLUME 61 | NUMBER 4 | OCTOBER 2007 SUPPLEMENT 4 www.neurosurgery-online.com
RHOTON
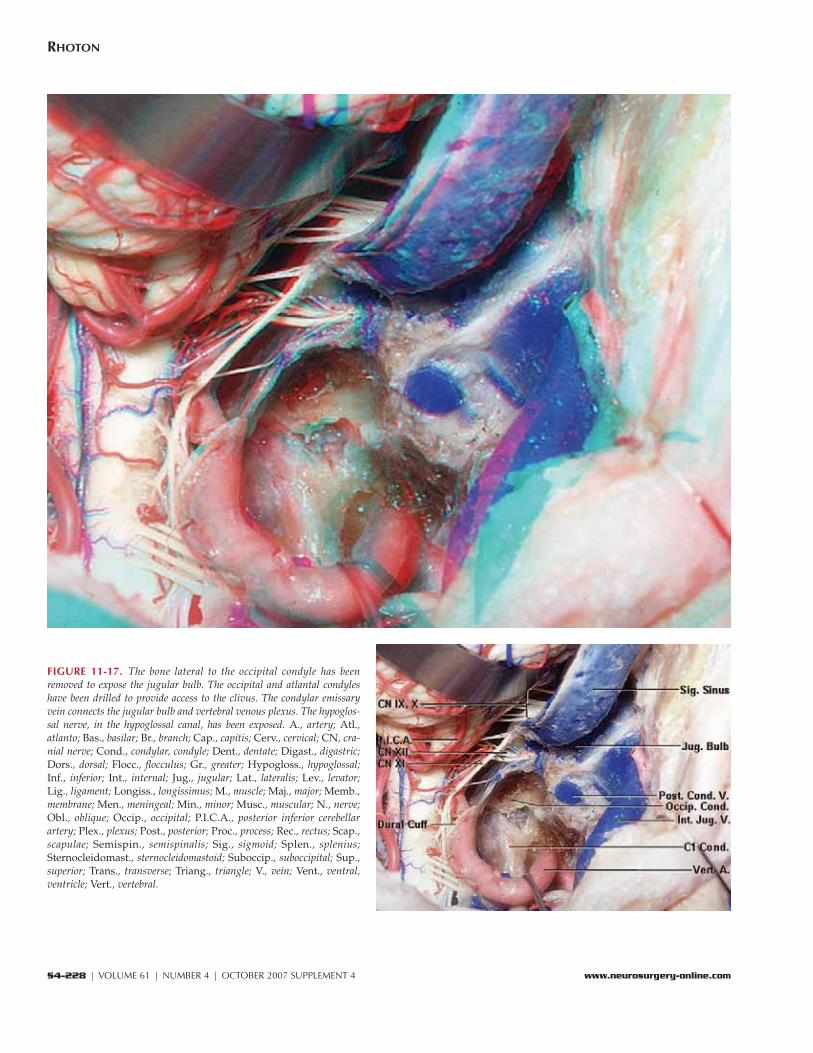
FIGURE 11-17. The bone lateral to the occipital condyle has beenremoved to expose the jugular bulb. The occipital and atlantal condyleshave been drilled to provide access to the clivus. The condylar emissaryvein connects the jugular bulb and vertebral venous plexus. The hypoglos-sal nerve, in the hypoglossal canal, has been exposed. A., artery; Atl.,atlanto; Bas., basilar; Br., branch; Cap., capitis; Cerv., cervical; CN, cra-nial nerve; Cond., condylar, condyle; Dent., dentate; Digast., digastric;Dors., dorsal; Flocc., flocculus; Gr., greater; Hypogloss., hypoglossal;Inf., inferior; Int., internal; Jug., jugular; Lat., lateralis; Lev., levator;Lig., ligament; Longiss., longissimus; M., muscle; Maj., major; Memb.,membrane; Men., meningeal; Min., minor; Musc., muscular; N., nerve;Obl., oblique; Occip., occipital; P.I.C.A., posterior inferior cerebellarartery; Plex., plexus; Post., posterior; Proc., process; Rec., rectus; Scap.,scapulae; Semispin., semispinalis; Sig., sigmoid; Splen., splenius;Sternocleidomast., sternocleidomastoid; Suboccip., suboccipital; Sup.,superior; Trans., transverse; Triang., triangle; V., vein; Vent., ventral,ventricle; Vert., vertebral.