family history of renal stones in a population study of stone-formers and healthy subjects
TRANSCRIPT

British Journal of Urologv (197% 51, 249-252
Family History of Renal Stones in a Population Study of Stone-formers and Healthy Subjects
S. LJUNGHALL Department of Internal Medicine, University Hospital, Uppsala, Sweden
Summary-Information on the family history of renal stone disease was obtained from over 2500 middle-aged men in a general health survey. A family history of stones was significantly more common among the stone-formers than among the controls, largely due to an increased frequency of stones among the fathers and brothers of the propositi.
predisposition to stone formation. An increased tendency was also noted, however, among the wives of those whose relatives had stones, which suggests that environmental factors are involved.
their laboratory profiles, but they appeared to be more prone to develop early and frequent recurrences.
This study thus supports previous suggestions that genetic factors play a part in the
Subjects with a family history of renal stones did not exhibit any particular characteristics in
Recent epidemiological studies indicate that renal stone disease is a rapidly increasing problem, already affecting more than 10% of the adult male population (Ljunghall, 1977). Several theories have been postulated for the formation and growth of renal stones but whatever the mechanisms may be which cause the actual crystallisation of salts in the urinary tract, it is likely that both environmental and genetic factors are involved. Thus stone disease appears to be increasing as standards of living rise in the indus- trialised world, but there are considerable geo- graphical variations (Andersen, 1969; Ljunghall, 1978). Comparatively little attention has been paid to familial factors in the occurrence of urinary calculi, although it has been suggested that a polygenic form of inheritance accounts for part of the stone-forming propensity in some patients with calcium stones (McGeown, 1960; Resnick et al., 1968). One problem encountered in genetic studies is the selection of valid patient and control materials, since adequate matching with regard to age, sex and socio-economic factors is essential. Thus patients from specialised stone clinics may not be typical of common stone- formers.
In this study a group of unselected stone-
Received 21 April 1978. Accepted for publication 11 October 1978.
formers, detected in a general health survey, was investigated with regard to the family history of stone disease and compared with a control group of individuals from the same survey. In addition, serum and urinary electrolytes were determined in an attempt to detect factors involved in the stone-forming diathesis.
Material and Methods Two general health surveys, primarily focused on the detection of cardiovascular risk factors, were carried out in the city of, Uppsala between 1970 and 1975. All males born in 1915 and between 1920 and 1924 were invited to participate and 2653 men were examined, a participation rate of 83.2% (Ljunghall and Hedstrand, 1975; Ljunghall and Waern, 1977). These investigations included a detailed self-administered questionnaire con- taining a query on the previous history of renal stones. All patients who answered in the affirma- tive were recalled for interview. Information on the occurrence of renal stone disease among first- degree relatives was obtained through a postal questionnaire sent to all of the stone-formers. The same questionnaire was also sent to a control group consisting of 635 men born in 1915 and 1924 and reported to be stone-free at the survey. This enquiry was answered by 97.6% of the stone-formers and 96.4% of the control group.
249
250 BRITISH JOURNAL OF UROLOGY
A family history of stones was considered to exist if at least one first-degree relative had experienced renal stones, even if the informant did not possess information concerning all of his relatives. On the other hand, the absence of a family history was accepted only if the informant could deny the occurrence of stones in all first-degree relatives. Those who did not possess full informa- tion in this respect were not included in the analysis of the family history. Adequate informa- tion, i.e. either a positive or a negative history, was obtained from 82.2% of the stone-formers and from 83.1070 of the controls. The accuracy of the information was checked by scrutiny of hospital and out-patient records and by re- evaluation of X-ray films. In only 5 cases was the patient’s history of stones found to be in- correct. The analysis of hospital discharge statistics and records did not reveal any further cases of stone disease not already detected by the screen- ing methods described. Serum electrolytes and uric acid were determined in all cases and urinary electrolyte excretion was investigated in all sub- jects born in 1915 (Ljunghall and Waern, 1977).
Conventional statistical methods were used to calculate mean values and SD. Significances of differences between mean values were estimated by Student’s t-test (2-tailed test). The X2-test (for small populations with Yates’s correction) was used for comparison of frequencies. The accepted level of significance was Pc0.05.
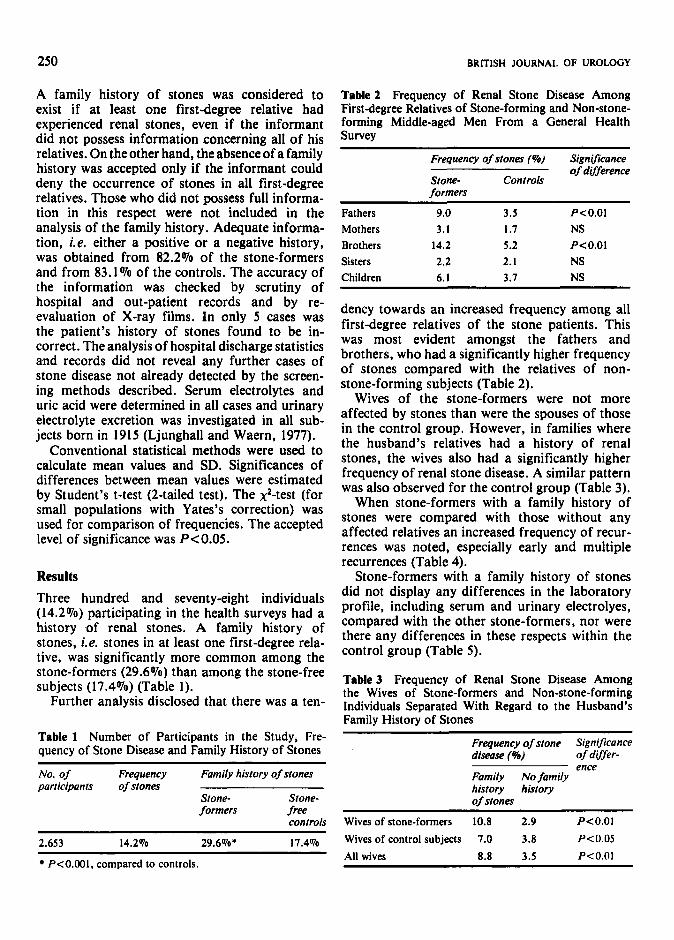
Results Three hundred and seventy-eight individuals (14.2%) participating in the health surveys had a history of renal stones. A family history of stones, i.e. stones in at least one first-degree rela- tive, was significantly more common among the stone-formers (29.6%) than among the stone-free subjects (17.4%) (Table 1).
Further analysis disclosed that there was a ten-
Table 1 Number of Participants in the Study, Fre- quency of Stone Disease and Family History of Stones
No. of Frequency Fomily history of stones porticiponts of stones
Stone- Stone- formers free
controls
2.653 14.2% 29.6%* 17.4%
Table 2 Frequency of Renal Stone Disease Among First-degree Relatives of Stone-forming and Non-stone- forming Middle-aged Men From a General Health Survey
Frequency of stones (%) Significance of difference
Stone- Controls formers
Fathers 9.0 3.5 P<O.Ol Mothers 3.1 1.7 NS Brothers 14.2 5.2 P<O.Ol Sisters 2.2 2.1 NS Children 6.1 3.7 NS
dency towards an increased frequency among all first-degree relatives of the stone patients. This was most evident amongst the fathers and brothers, who had a significantly higher frequency of stones compared with the relatives of non- stone-forming subjects (Table 2).
Wives of the stone-formers were not more affected by stones than were the spouses of those in the control group. However, in families where the husband’s relatives had a history of renal stones, the wives also had a significantly higher frequency of renal stone disease. A similar pattern was also observed for the control group (Table 3).
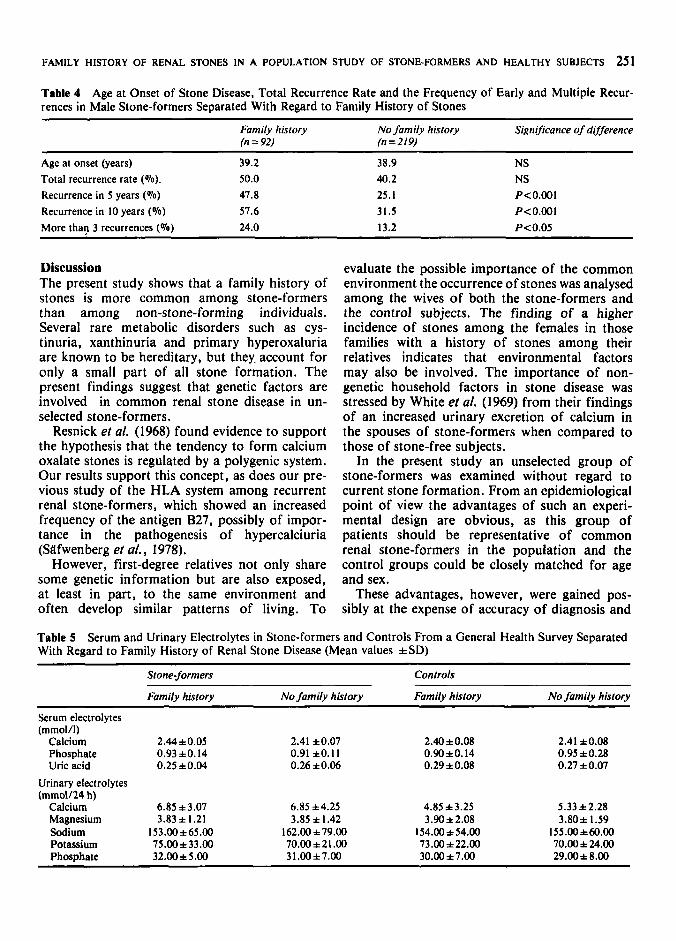
When stone-formers with a family history of stones were compared with those without any affected relatives an increased frequency of recur- rences was noted, especially early and multiple recurrences (Table 4).
Stone-formers with a family history of stones did not display any differences in the laboratory profile, including serum and urinary electrolyes, compared with the other stone-formers, nor were there any differences in these respects within the control group (Table 5) .
Table3 Frequency of Renal Stone Disease Among the Wives of Stone-formers and Non-stone-forming Individuals Separated With Regard to the Husband’s Family History of Stones
Frequency of stone Significonce diseose (%) of differ-
Family No family history history of stones
ence
Wives of stone-formers 10.8 2.9 P<O.Ol Wives of control subjects 7.0 3.8 P<0.05 All wives 8.8 3.5 P<O.Ol P<O.OOl, compared to controls.
FAMILY HISTORY OF RENAL STONES IN A POPULATION STUDY OF STONE-FORMERS AND HEALTHY SUBJECTS 251
Table 4 Age at Onset of Stone Disease, Total Recurrence Rate and the Frequency of Early and Multiple Recur- rences in Male Stone-formers Separated With Regard to Family History of Stones
Family history No family history Significance of difference (n = 92) (n=Z19)
Age at onset (years) 39.2 Total recurrence rate (To). 50.0 Recurrence in 5 years (S) 47.8 Recurrence in 10 years (To) 57.6 More than 3 recurrences (To) 24.0
38.9 40.2 25.1 31.5 13.2
NS NS P<O.001 P<0.001 P<0.05
Discussion The present study shows that a family history of stones is more common among stone-formers than among non-stone-forming individuals. Several rare metabolic disorders such as cys- tinuria, xanthinuria and primary hyperoxaluria are known to be hereditary, but they. account for only a small part of all stone formation. The present findings suggest that genetic factors are involved in common renal stone disease in un- selected stone-formers.
Resnick et al. (1968) found evidence to support the hypothesis that the tendency to form calcium oxalate stones is regulated by a polygenic system. Our results support this concept, as does our pre- vious study of the HLA system among recurrent renal stone-formers, which showed an increased frequency of the antigen B27, possibly of impor- tance in the pathogenesis of hypercalciuria (Siifwenberg et a/., 1978).
However, first-degree relatives not only share some genetic information but are also exposed, at least in part, to the same environment and often develop similar patterns of living. To
evaluate the possible importance of the common environment the occurrence of stones was analysed among the wives of both the stone-formers and the control subjects. The finding of a higher incidence of stones among the females in those families with a history of stones among their relatives indicates that environmental factors may also be involved. The importance of non- genetic household factors in stone disease was stressed by White et al. (1969) from their findings of an increased urinary excretion of calcium in the spouses of stone-formers when compared to those of stone-free subjects.
In the present study an unselected group of stone-formers was examined without regard to current stone formation. From an epidemiological point of view the advantages of such an experi- mental design are obvious, as this group of patients should be representative of common renal stone-formers in the population and the control groups could be closely matched for age and sex.
These advantages, however, were gained pos- sibly at the expense of accuracy of diagnosis and
Table 5 Serum and Urinary Electrolytes in Stone-formers and Controls From a General Health Survey Separated With Regard to Family History of Renal Stone Disease (Mean values iSD)
Stone-formers Controls
Family history No family history Family history No family history
Serum electrolytes (mmol/l)
Calcium 2.44f0.05 2.41 f0.07 2.40f0.08 2.41 *0.08 Phosphate 0.93+0.14 0.91 10.1 I 0.90 f 0 . 14 0.95 *0.28 Uric acid 0.25 *0.04 0.26 *0.06 0.29*0.08 0.27 f 0.07
Urinary electrolytes (mmo1/24 h)
Calcium 6.85 f 3.07 6.85 *4.25 4.85 f3.25 5.33 *2.28 Magnesium 3.83 + I .21 3.85 f 1.42 3.90*2.08 3.80;t 1.59 Sodium 153.00f65.00 162.00 f79.00 154.00*54.00 155.00 ;t60.00 Potassium 75.00*33.00 70.00 f 21 .00 73.00 *22.00 70.00f 24.00 Phosphate 32.Wf 5 . 0 0 3 1 .00 *7.00 30.00 f 7.00 29.00*8.00
252
completeness of information. Previous studies have indicated that the informant’s knowledge of his own stone disease was almost always accurate (Ljunghall, 1977) and this is probably also true of reported cases of stones in his family. On the other hand, it is possible that bias may arise from the fact that stone-formers have an increased interest in stones among their relatives and stone- free subjects may underestimate stone disease in their first-degree relatives. Although ideally an extended survey should obtain firsthand informa- tion from all members of the families, it appears from earlier studies that such a bias was not strong enough to have a significant effect on the results (McGeown, 1960; Resnick ef al., 1968).
Several theories have been put forward to explain stone formation and growth; current opinion on the physicochemical background of stone formation implies a disturbance of the balance between the supersaturating and the inhibitory factors (Robertson et al., 1976).
In previous attempts to identify the factor res- ponsible for the familial predisposition to stone formation, most attention has been directed to calcium metabolism and it has been suggested that hypercalciuria (presumably caused by an increased dietary intake of calcium) is the con- necting link (White ef al., 1969; TransbOl and Frydendal, 1973). None of these investigations, however, studied the calcium intake or the inci- dence of stones among the relatives of stone patients.
We have earlier demonstrated that stone-formers, when compared to matched controls, do not have an increased intake of calcium or vitamin D (Ljunghall and Hedstrand, 1976) and in the present study there were no differences in the serum or urinary calcium between stone patients and the control group when separated with regard to the family history of stones. Although hyper- calciuria is commonly found among recurrent stone-formers, as in the present study, it seems unlikely that the familial diathesis for stone formation is mediated primarily through a raised urinary calcium.
Whatever the biochemical cause for the increased frequency of stone formation in these families may be, it appeared that this group of patients had clinical characteristics in common with a high recurrence rate, particularly early and multiple recurrences. Detailed metabolic investigations have failed to disclose patients with an increased
BRITISH JOURNAL OF UROLOGY
This study suggests that patients with a family history of stone disease should be regarded as being at risk. Early clinical and metabolic evalua- tion is worthwhile and attempts at prevention of stone formation are justified early in the course of the disease.
References Andersen, D. A. (1969). Historical and geographical differ-
ences in the pattern of incidence of urinary stones con- sidered in relation to possible aetiological factors. In Renal Stone Research Symposium, ed. Hodgkinson, A. and Nordin, B. E. C. Pp. 7-31. London: Churchill Livingstone.
Ljunghall, S. (1977). Renal stone disease. Studies of epide- miology and calcium metabolism. Scandinavian Journal of Urology and Nephrology, Supplement 41, 6-39.
Ljunghall, S. (1978). Regional variations in the incidence of urinary stones. British Medical Journal, I, 439.
Ljunghall, S. and Hedslnnd, H. (1975). Epidemiology of renal stones in a middle aged male population. Acta Medica Scandinavica, 197, 439-445.
Ljunghall, S. and Hedstnnd, H. (1976). Renal stones and coronary heart disease. Acta Medica Scandinavica. 199. 481 -485.
Ljunghall, S. and Waern, A. U. (1977). Urinary electrolytes in renal stone formers and healthy subjects. Scandinavian Journal of Urology and Nephrology, Supplement 41, 55-15.
McGeown, M. (1960). Heredity in renal stone disease. Clinical Science, 19,465-47 I.
Powis, S. J., Black, J., Macdougall, J. A. and Clews, J. W. (1974). Management of patients with urinary calculi. British Medical Journal, 1, 355-357.
Resnick, M., Pridgen, D. B. and Goodman, H. 0. (1968). Genetic predisposition to formation of calcium oxalate renal calculi. New England Journal of Medicine, 278,
Robertson, W. G., Peacock, M., Marshall, R. W., Marshall, D. H. and Nordin, B. E. C. (1976). Saturation-inhibition index as a measure of the risk of calcium oxalate stone formation in the urinary tract. New. England Journal of Medicine, 294, 249-252.
Siifwenberg, J., Backman, U.. Danielson, B. G., Johansson, G. and Ljunghall, S. (1978). HLA and kidney stones. Scandinavian Journal of Urology and Nephrology. (In press.)
Transbiil, 1. and Frydendal, N. (1973). Endocrine and meta- bolic aspects of urology. Aetiology of stone formation in 145 renal stone patients. Acta Chirurgica Scandinavica, Supplement 433, 137-153.
While, R. W., Cohen, R. D.. Vince, F. P., Williams. G., Blandy, J. and Tresldder, C. G. (1969). Minerals in the urine of stone-formers and their spouses. In Renal Stone Research Symposium, ed. Hodginson, A. and Nordin, B. E. C. Pp. 289-296. London: Churchill Livingstone.
I 3 13-1 3 18.
The Author S. Ljunghall, MD, Assistant Professor and Registrar, Depart-
ment of Internal Medicine, University Hospital, S-750 14 tendency to stone formation (Powis ef al., 1974). Uppsala, Sweden.