expert radiation oncologist interpretations
TRANSCRIPT
7/23/2019 Expert Radiation Oncologist Interpretations
http://slidepdf.com/reader/full/expert-radiation-oncologist-interpretations 1/6
Guidelines
Expert Radiation Oncologist Interpretations
of Involved-Site Radiation Therapy Guidelines
in the Management of Hodgkin LymphomaBradford S. Hoppe, MD, MPH,* and Richard T. Hoppe, MDy
*University of Florida Health Proton Therapy Institute, Jacksonville, Florida; and y Stanford Cancer
Institute, Stanford, California
Received Jan 7, 2015, and in revised form Jan 29, 2015. Accepted for publication Feb 2, 2015.
Summary
Involved-site radiation ther-apy (ISRT) guidelines havebeen developed to replaceinvolved-field radiation ther-apy guidelines that werebased on 2D radiation simu-lation techniques and treat-
ment planning. A survey of expert radiation oncologistscovering 7 different Hodgkinlymphoma cases demon-strated variable in-terpretations of ISRTguidelines. Further guidancefor involved-site field designwill be needed to reducevariability among practicingphysicians.
Purpose: Recently, involved-site radiation therapy (ISRT) guidelines have been devel-oped and published to replace the previous concept of involved-field radiation therapyfor patients with lymphoma. However, these ISRT guidelines may be interpreted indifferent ways, posing difficulties for prospective clinical trials. This study reports sur-vey results regarding interpretation of the ISRT guidelines.Methods and Materials: Forty-four expert lymphoma radiation oncologists wereasked to participate in a survey that included 7 different cases associated with 9 ques-tions. The questions pertained to ISRT contouring and asked respondents to choose
between 2 different answers (no “correct” answer) and a third write-in option allowed.Results: Fifty-two percent of those surveyed responded to the questionnaire. Amongthose who responded, 72% have practiced for >10 years, 46% have treated >20 Hodg-kin lymphoma cases annually, and 100% were familiar with the ISRT concept. Amongthe 9 questions associated with the 7 cases, 3 had concordance among the expertradiation oncologists of greater than 70%. Six of the questions had less than 70%concordance (range, 56%-67%).Conclusions: Even among expert radiation oncologists, interpretation of ISRT guide-lines is variable. Further guidance for ISRT field design will be needed to reduce vari-ability among practicing physicians. 2015 Elsevier Inc. All rights reserved.
Introduction
The radiation treatment fields used for lymphomas haveevolved continuously over the past 50 years. In the 1950s
and 1960s, radiation therapy was used primarily as apalliative therapy, and radiation fields were typicallylimited to symptomatic sites of disease. In the late 1960s,studies by Peters (1) and Kaplan (2) advocated curative
Reprint requests to: Richard T. Hoppe, MD, Stanford CancerInstitute, Radiation Oncology, Rm.CC-G224, 875 Blake WilburDr Stanford CA 94305. Tel: (650) 723-5510; E-mail: [email protected]
Presented in part at the 56th Annual Meeting of the American Societyfor Radiation Oncology, San Francisco CA, September 13-17, 2014.
Conflict of interest: none.Supplementary material for this article can be found at
www.redjournal.org.
Int J Radiation Oncol Biol Phys, Vol. 92, No. 1, pp. 40e45, 2015
0360-3016/$ - see front matter 2015 Elsevier Inc. All rights reserved.http://dx.doi.org/10.1016/j.ijrobp.2015.02.008
Radiation OncologyInternational Journal of
b iol og y p hy si cs
www.redjournal.org

7/23/2019 Expert Radiation Oncologist Interpretations
http://slidepdf.com/reader/full/expert-radiation-oncologist-interpretations 2/6
treatment of lymphoma by irradiating not only all sites of known disease but also adjacent uninvolved sites. Bynecessity, treatment fields became larger, and terms such as“mantle,” “inverted Y,” “extended field” radiation therapy(EFRT), and “total lymphoid irradiation” were introducedto describe these fields, which contrasted with the previouslimited-field treatment now known as “involved-field”
radiation therapy (IFRT).Beginning in the mid-1970s, however, combined-
modality therapy became more common in the treatmentof the lymphomas, and interest in reducing the extent of theradiation fields resurged, leading to a renaissance in the useof IFRT (3-6). In the context of these clinical trials, IFRTwas usually clearly defined. IFRT was based on the AnnArbor-defined lymphoid regions, and radiation treatmentplanning included 2-dimensional (2D) simulation usingbony landmarks to define the borders of those lymphoidregions. Outside its use in prospective clinical trials, IFRTwas more variably defined. In 2001, a survey among in-
ternational expert radiation oncologists confirmed that therewere substantial discrepancies in the definition of fielddesigns for IFRT (7). Subsequently, Yahalom and Mauch(7) published guidelines for the design of IFRT fields basedupon 2D imaging. However, much has changed over thelast decade, including improved diagnostic imaging withphoton emission tomography-computed tomography (PET-CT) and the use of 3-dimensional (3D) treatment planningwith target volume contouring, such as gross tumor volume(GTV), clinical target volume (CTV), internal target vol-ume (ITV), and planning target volume (PTV).
In response to these changes in modern radiation
oncology practices, Girinsky et al (8) developed guidelinesfor “involved-node RT” (INRT) to be used with EuropeanOrganization for Research and Treatment of Cancer-Groupe d’Etude des Lymphomes de l’Adulte (EORTC-GELA) trials. These trials used the International Commis-sion on Radiation Units (ICRU) Report 50/62 dose speci-fications and target delineation of a GTV, a CTV, and aPTV, and that required 3D treatment planning (9). Althoughresults have been quite promising in successfully reducingthe field size without impacting event-free survival (10),most centers throughout the world are unable to meet thestringent criteria of INRT, which require prechemotherapy
evaluation by a radiation oncologist and a PET-CT scanperformed in the radiation treatment position and obtainedbefore chemotherapy. In response, the International Lym-phoma Radiation Oncology Group (ILROG), an interna-tional group of radiation oncologists with special expertisein the treatment of lymphoma, developed the concept of “involved-site” RT (ISRT) and published guidelines to helpbridge the differences between IFRT and INRT.
ISRT guidelines incorporate the prechemotherapy defi-nition of extent of disease based upon clinical studies,including PET-CT, which may or may not be performed inthe treatment position, as well as the postchemotherapy
treatment planning CT. However, defining the CTV relies
upon the quality and accuracy of imaging; knowledge of the spread patterns of the disease, as well as potentialsubclinical extent of involvement and adjacent organ at risk (OAR) constraints, all of which depend on clinical
judgment.Guidelines for ISRT have been published for HL (11),
pediatric HL (12), and nodal non-HL (13). Despite their
wide acceptance, interpretation of the guidelines varies.Consequently, a survey was developed to try to better un-derstand the areas of consensus and lack of consensus forISRT contouring and formed the basis for this report.
Methods and Materials
Forty-two radiation oncologists known to be experienced intreating HL according to their publications or participationin lymphoma-related activities of the American Board of Radiology, the American College of Radiology, Children’s
Oncology Group, or National Cancer Center Network wereasked to participate in completing a 9-question survey thatincluded 7 different cases, emphasizing contouring de-cisions for the definition of radiation treatment volumes.These cases were chosen to represent a range of clinicalscenarios in defining treatment fields by ISRT criteria,including sites of disease and patient age, sex, and re-sponses to chemotherapy. Generally, respondents wereasked to select 1 of 2 different contouring options, althoughthey could also respond with “other,” a write-in option.
The following clinical scenarios were presented,accompanied by pre- and postchemotherapy PET-CT im-
aging (as appropriate) and predefined contouring choices.
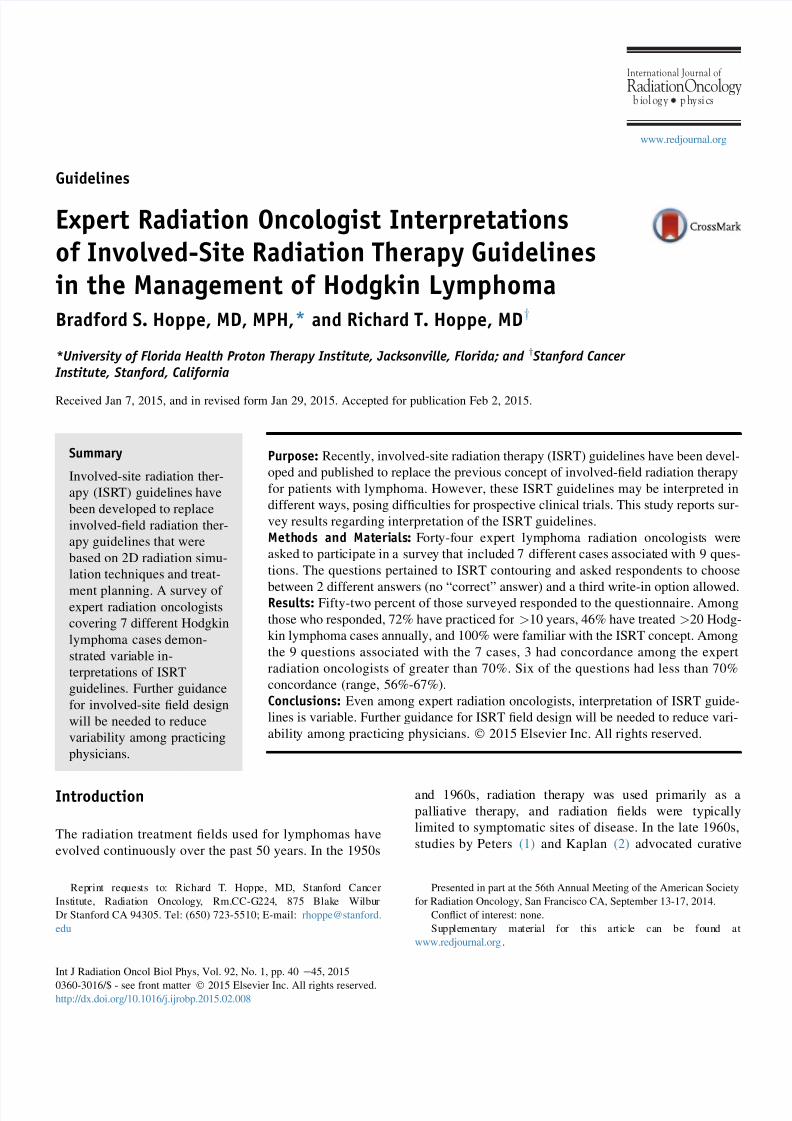
Case 1: stage IA, classical HL of left parotid lymphnode and nodes in levels IIA, IIB, III, IV, and V
A woman with stage IA classical HL involving a left pa-rotid lymph node and nodes in levels IIA, IIB, III, IV, andV, received 2 cycles of doxorubicin, bleomycin, vinblastine,dacarbazine (ABVD) therapy and achieved a completeresponse (CR) by PET and CT. The contouring choiceswere to include elective coverage of the uninvolved neck
nodes in level IB (choice A) or to restrict treatment to levelsIIA-IV (choice B) (Fig. 1).
Case 2: stage IIAE, classical HL of the right parotidgland and ipsilateral high neck
A 48-year-old man with stage IIAE classical HL involvingthe right parotid gland and ipsilateral high neck achieved aCR on PET-CT following 4 cycles of ABVD. The con-touring choices were to define a CTV that included only theinitially involved nodes and postoperative parotid bed(choice A) or to extend the field to include adjacent unin-
volved nodes (choice B).
Volume 92 Number 1 2015 Involved-site RT guidelines for lymphoma 41
7/23/2019 Expert Radiation Oncologist Interpretations
http://slidepdf.com/reader/full/expert-radiation-oncologist-interpretations 3/6
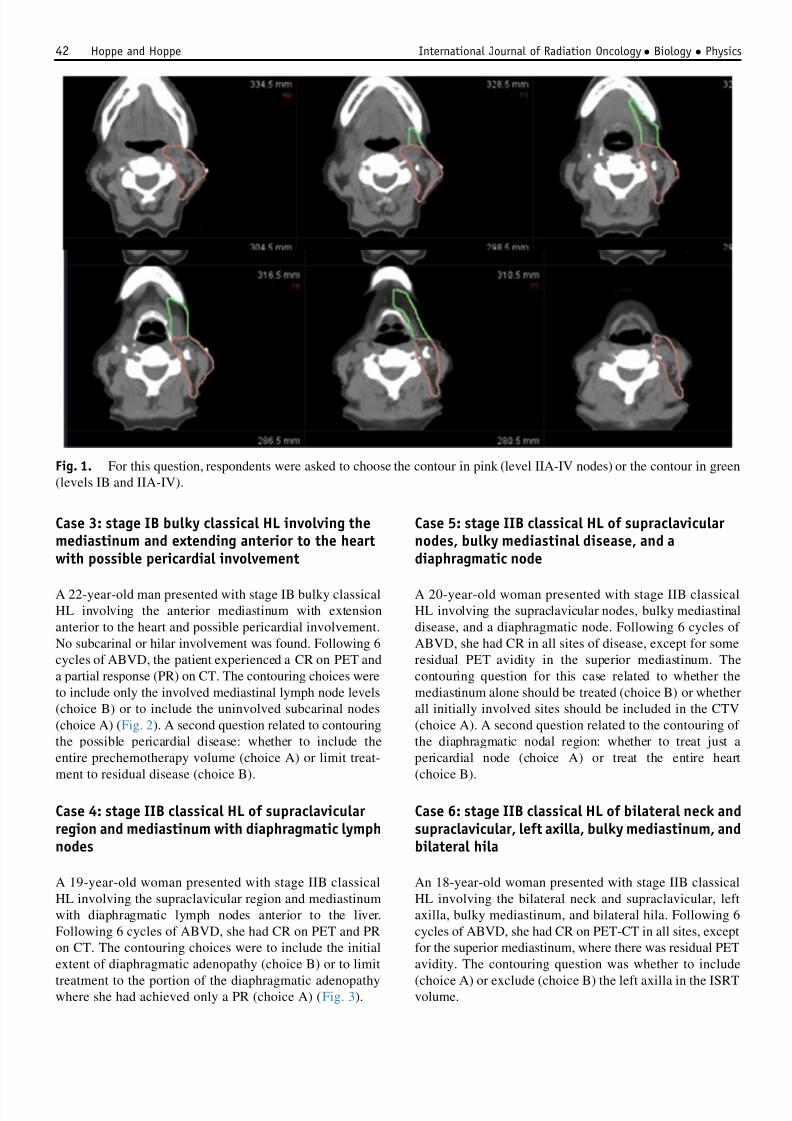
Case 3: stage IB bulky classical HL involving themediastinum and extending anterior to the heartwith possible pericardial involvement
A 22-year-old man presented with stage IB bulky classicalHL involving the anterior mediastinum with extensionanterior to the heart and possible pericardial involvement.No subcarinal or hilar involvement was found. Following 6cycles of ABVD, the patient experienced a CR on PET anda partial response (PR) on CT. The contouring choices wereto include only the involved mediastinal lymph node levels(choice B) or to include the uninvolved subcarinal nodes(choice A) (Fig. 2). A second question related to contouringthe possible pericardial disease: whether to include theentire prechemotherapy volume (choice A) or limit treat-ment to residual disease (choice B).
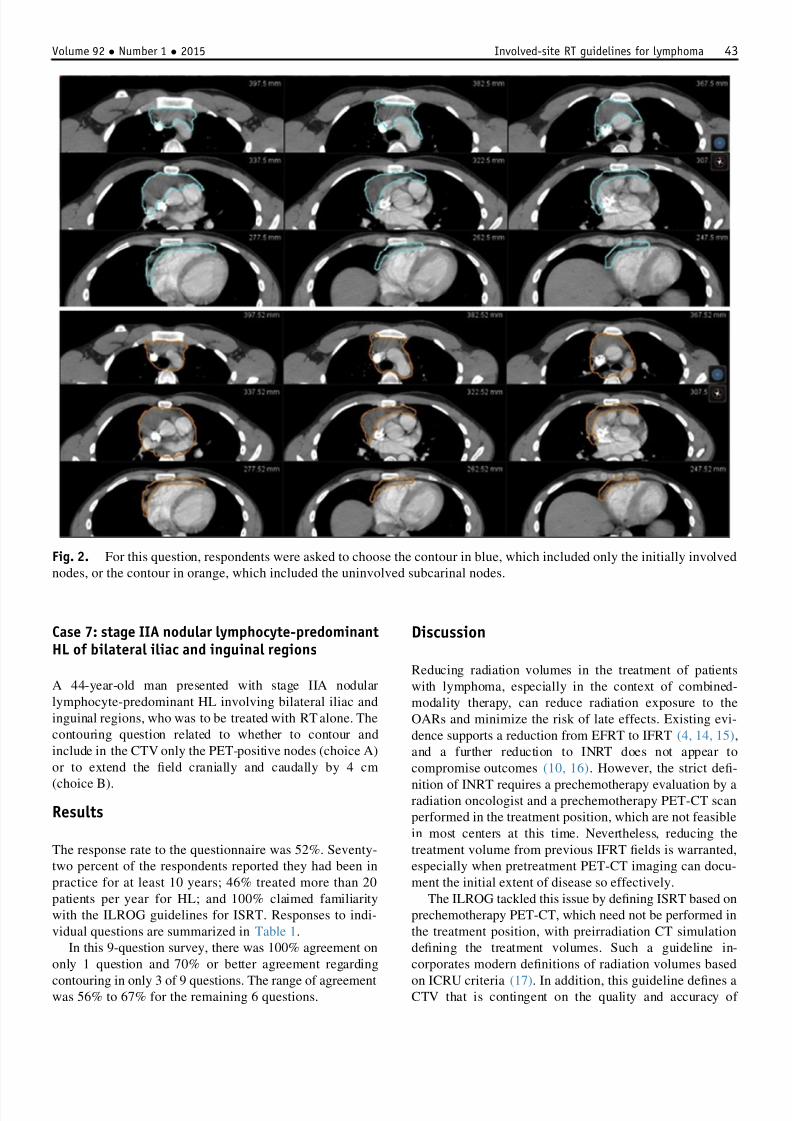
Case 4: stage IIB classical HL of supraclavicular region and mediastinum with diaphragmatic lymphnodes
A 19-year-old woman presented with stage IIB classicalHL involving the supraclavicular region and mediastinumwith diaphragmatic lymph nodes anterior to the liver.Following 6 cycles of ABVD, she had CR on PET and PRon CT. The contouring choices were to include the initialextent of diaphragmatic adenopathy (choice B) or to limit
treatment to the portion of the diaphragmatic adenopathywhere she had achieved only a PR (choice A) (Fig. 3).
Case 5: stage IIB classical HL of supraclavicular nodes, bulky mediastinal disease, and adiaphragmatic node
A 20-year-old woman presented with stage IIB classicalHL involving the supraclavicular nodes, bulky mediastinaldisease, and a diaphragmatic node. Following 6 cycles of ABVD, she had CR in all sites of disease, except for someresidual PET avidity in the superior mediastinum. Thecontouring question for this case related to whether themediastinum alone should be treated (choice B) or whetherall initially involved sites should be included in the CTV(choice A). A second question related to the contouring of the diaphragmatic nodal region: whether to treat just apericardial node (choice A) or treat the entire heart(choice B).
Case 6: stage IIB classical HL of bilateral neck andsupraclavicular, left axilla, bulky mediastinum, andbilateral hila
An 18-year-old woman presented with stage IIB classicalHL involving the bilateral neck and supraclavicular, leftaxilla, bulky mediastinum, and bilateral hila. Following 6cycles of ABVD, she had CR on PET-CT in all sites, exceptfor the superior mediastinum, where there was residual PETavidity. The contouring question was whether to include
(choice A) or exclude (choice B) the left axilla in the ISRTvolume.
Fig. 1. For this question, respondents were asked to choose the contour in pink (level IIA-IV nodes) or the contour in green(levels IB and IIA-IV).
Hoppe and Hoppe International Journal of Radiation Oncology Biology Physics42
7/23/2019 Expert Radiation Oncologist Interpretations
http://slidepdf.com/reader/full/expert-radiation-oncologist-interpretations 4/6
Case 7: stage IIA nodular lymphocyte-predominantHL of bilateral iliac and inguinal regions
A 44-year-old man presented with stage IIA nodularlymphocyte-predominant HL involving bilateral iliac andinguinal regions, who was to be treated with RT alone. Thecontouring question related to whether to contour andinclude in the CTV only the PET-positive nodes (choice A)or to extend the field cranially and caudally by 4 cm
(choice B).
Results
The response rate to the questionnaire was 52%. Seventy-two percent of the respondents reported they had been inpractice for at least 10 years; 46% treated more than 20patients per year for HL; and 100% claimed familiaritywith the ILROG guidelines for ISRT. Responses to indi-vidual questions are summarized in Table 1.
In this 9-question survey, there was 100% agreement ononly 1 question and 70% or better agreement regarding
contouring in only 3 of 9 questions. The range of agreementwas 56% to 67% for the remaining 6 questions.
Discussion
Reducing radiation volumes in the treatment of patientswith lymphoma, especially in the context of combined-modality therapy, can reduce radiation exposure to theOARs and minimize the risk of late effects. Existing evi-dence supports a reduction from EFRT to IFRT (4, 14, 15),and a further reduction to INRT does not appear tocompromise outcomes (10, 16). However, the strict defi-
nition of INRT requires a prechemotherapy evaluation by aradiation oncologist and a prechemotherapy PET-CT scanperformed in the treatment position, which are not feasiblein most centers at this time. Nevertheless, reducing thetreatment volume from previous IFRT fields is warranted,especially when pretreatment PET-CT imaging can docu-ment the initial extent of disease so effectively.
The ILROG tackled this issue by defining ISRT based onprechemotherapy PET-CT, which need not be performed inthe treatment position, with preirradiation CT simulationdefining the treatment volumes. Such a guideline in-corporates modern definitions of radiation volumes based
on ICRU criteria (17). In addition, this guideline defines aCTV that is contingent on the quality and accuracy of
Fig. 2. For this question, respondents were asked to choose the contour in blue, which included only the initially involvednodes, or the contour in orange, which included the uninvolved subcarinal nodes.
Volume 92 Number 1 2015 Involved-site RT guidelines for lymphoma 43
7/23/2019 Expert Radiation Oncologist Interpretations
http://slidepdf.com/reader/full/expert-radiation-oncologist-interpretations 5/6
imaging, knowledge of the spread patterns of the disease aswell as potential subclinical extent of involvement, andadjacent organ (OAR) constraints, all of which dependsomewhat on clinical judgment. These variables may leadto differences in defining the CTV for individual patients.In this study, expert radiation oncologists who werefamiliar with the ILROG guidelines were asked to select
from 2 different contouring options in a series of 9 ques-tions derived from 7 clinical scenarios. Neither option wasconsidered correct but merely intended to evaluate the de-gree of consensus. The 1 question for which there was100% agreement (question 7) likely reflects the concern forpotential cardiac toxicity by extension of the field toinclude the entire heart, especially as there was no peri-
cardial involvement noted. The results indicated that theseguidelines, although generally accepted, can lead to variousinterpretations. Although not tested in this survey, it islikely that even greater variability in interpretation mayexist among general practice radiation oncologists.
Conclusions
Our findings suggest that more education and greater expe-rience are required to improve concordance of volumedefinition. This effort is already under way both throughILROG-sponsored contouring workshops at the annualAmerican Society for Radiation Oncology meeting andworkshops at the International Congress on MalignantLymphoma, in Lugano, Italy, 2013 and 2015. In addition, thisstudy indicates that prospective trials that incorporate ISRTshould use precise definitions for common clinical scenarios.Furthermore, careful quality control review of ISRT fields onprospective clinical trials is warranted, similar to that foundwith the German Hodgkin Study Group (18).
References
1. Peters MV. Prophylactic treatment of adjacent areas in Hodgkin’sdisease. Cancer Res 1966;26:1232-1243.
2. Kaplan HS. The radical radiotherapy of regionally localized Hodg-kin’s disease. Radiology 1962;78:553-561.
3. Rosenberg SA, Kaplan HS. The evolution and summary results of theStanford randomized clinical trials of the management of Hodgkin’sdisease: 1962-1984. Int J Radiat Oncol Biol Phys 1985;11:5-22.
4. Noordijk EM, Carde P, Mandard AM, et al. Preliminary results of theEORTC-GPMC controlled clinical trial H7 in early-stage Hodgkin’s
disease. EORTC Lymphoma Cooperative Group. Groupe Pierre-et-Marie-Curie. Ann Oncol 1994;5(suppl 2):107-112.
5. Engert A, Schiller P, Josting A, et al. Involved-field radiotherapy is equallyeffective and less toxic compared with extended-field radiotherapy after
four cycles of chemotherapy in patients with early-stage unfavorableHodgkin’s lymphoma: Results of the HD8 trial of the German Hodgkin’sLymphoma Study Group. J Clin Oncol 2003;21:3601-3608.
6. Miller TP, Dahlberg S, Cassady JR, et al. Chemotherapy alonecompared with chemotherapy plus radiotherapy for localized inter-mediate- and high-grade non-Hodgkin’s lymphoma. N Engl J Med
1998;339:21-26.
7. Yahalom J, Mauch P. The involved fieldis back:Issues in delineating theradiation fieldin Hodgkin’sdisease. Ann Oncol 2002;13(suppl 1):79-83.
8. Girinsky T, van der Maazen R, Specht L, et al. Involved-node radio-
therapy (INRT) in patients with early Hodgkin lymphoma: Conceptsand guidelines. Radiother Oncol 2006;79:270-277.
9. ICRU. International Commission on Radiation Units and Measure-ments. Prescribing, recording, and reporting photon therapy. (Sup-
plement to ICRU Report 50). |ICRU Report 62. 1999.10. Maraldo MV, Aznar MC, Vogelius IR, et al. Involved node radiation
therapy: an effective alternative in early-stage hodgkin lymphoma. Int J Radiat Oncol Biol Phys 2013;85:1057-1065.
Fig. 3. For this question, respondents were asked tochoose the contour in blue, which included the area of
postchemotherapy residual disease only (outlined in pink),or the contour in red, which included all of the nodesinvolved prior to chemotherapy.
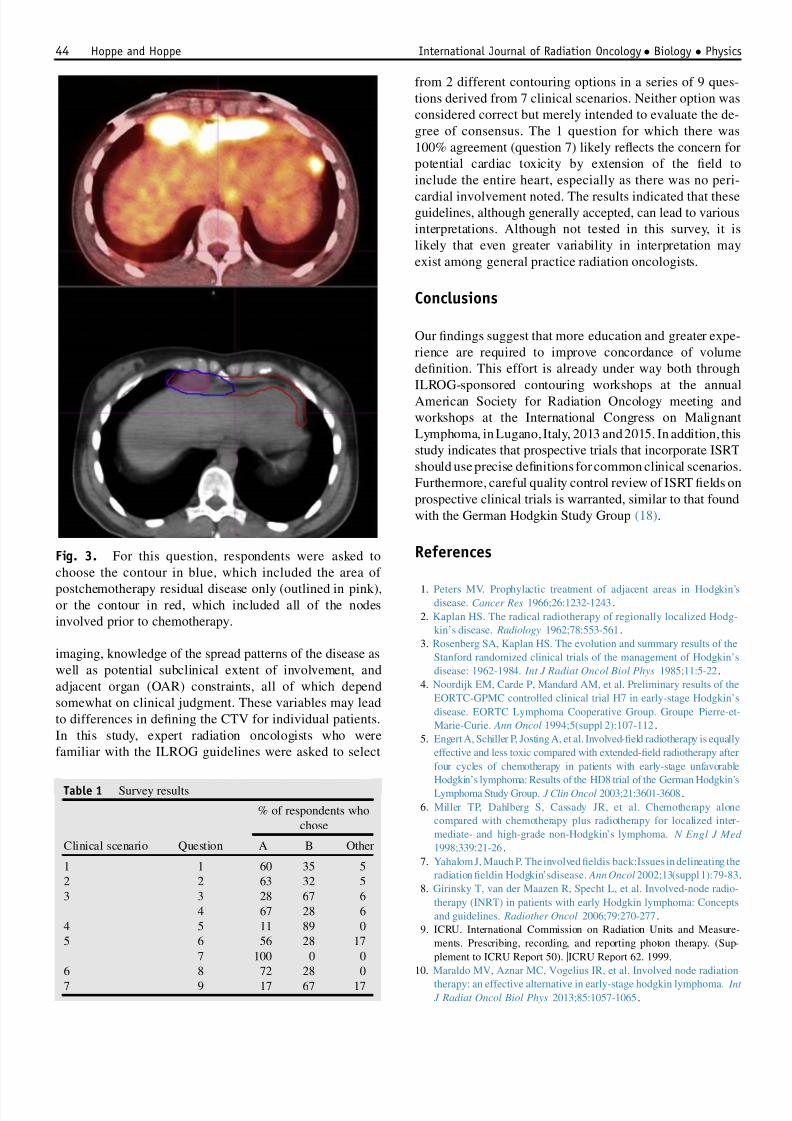
Table 1 Survey results
Clinical scenario Question
% of respondents whochose
A B Other
1 1 60 35 52 2 63 32 53 3 28 67 6
4 67 28 64 5 11 89 05 6 56 28 17
7 100 0 06 8 72 28 0
7 9 17 67 17
Hoppe and Hoppe International Journal of Radiation Oncology Biology Physics44

7/23/2019 Expert Radiation Oncologist Interpretations
http://slidepdf.com/reader/full/expert-radiation-oncologist-interpretations 6/6
11. Specht L, Yahalom J, Illidge T, et al. Modern radiation therapy forHodgkin lymphoma: field and dose guidelines from the InternationalLymphoma Radiation Oncology Group (ILROG). Int J Radiat Oncol
Biol Phys 2014;89:854-862.12. Hodgson DC, Dieckmann K, Terezakis S, et al. Implementation of
contemporary radiation therapy planning concepts for pediatricHodgkin lymphoma: Guidelines from the International LymphomaRadiation Oncology Group. Pract Radiat Oncol 2014;5:85-92.
13. Illidge T, Specht L, Yahalom J, et al. Modern radiation therapy fornodal non-Hodgkin lymphoma-target definition and dose guidelinesfrom the International Lymphoma Radiation Oncology Group. Int J
Radiat Oncol Biol Phys 2014;89:49-58.14. Bonadonna G, Bonfante V, Viviani S, et al. ABVD plus subtotal nodal
versus involved-field radiotherapy in early-stage Hodgkin’s disease:Long-term results. J Clin Oncol 2004;22:2835-2841.
15. Sasse S, Klimm B, Gorgen H, et al. Comparing long-term toxicity andefficacy of combined modality treatment including extended- orinvolved-field radiotherapy in early-stage Hodgkin’s lymphoma. Ann
Oncol 2012;23:2953-2959.16. Hoppe BS, Flampouri S, Zaiden R, et al. Involved-node proton therapy
in combined modality therapy for hodgkin lymphoma: Results of aphase 2 study. Int J Radiat Oncol Biol Phys 2014;89:1053-1059.
17. International Commission on Radiation Units and Measurements.[website] 2014. Available at: http://www.icru.org/ . Accessed February22, 2015.
18. Eich HT, Engenhart-Cabillic R, Hansemann K, et al. Quality controlof involved field radiotherapy in patients with early-favorable (HD10)and early-unfavorable (HD11) Hodgkin’s lymphoma: an analysis of the German Hodgkin Study Group. Int J Radiat Oncol Biol Phys 2008;71:1419-1424.
Volume 92 Number 1 2015 Involved-site RT guidelines for lymphoma 45