evolving concepts of median nerve decompression in the...
TRANSCRIPT
Peripheral Nerve Surgery 0749-071’9./86 $0.00 +.20
Evolving Concepts of Median NerveDecompression in the Carpal Tunnel
Frederick R. Heckler, M.D.,*and Michael E. Jabaley, M.D. ~
Compression neuropathies, formerlythought to be rare, have been recognizedwith increasing frequency over the past 25years by clinicians who deal with problemsof the hand. This apparent increase in in-cidence in fact reflects a profound increasein awareness and accuracy of diagnosis--both factors which are based on a clearerunderstanding of the anatomy, pathophys-iology, and subsequent clinical appearanceof each of these fascinating clinical entities.Of all the compression neuropathies, me-dian nerve compression at the wrist (carpaltunnel syndrome) is the most frequently en-countered and best understood. As our un-derstanding has evolved, there has alsogrown an appreciation for the subtleties andnuances that accompany this entity, and thishas been mirrored in a number of modifi-cations in treatment, both surgical and oth-erwise.
We wish to review the salient features andcurrent understanding of compression neu-ropathies of the median nerve at the wrist,with emphasis on points that have provedparticularly valuable in our own clinicalpractices. We will also stress those points oftechnique that reflect a shift from early prac-tices. Such a personal review is necessarilybiased, and we will attempt to add balanceby including a selected (rather than ency-
clopedic) listing of both complementary andopposing viewpoints from the published lit-erature on the subject.
ANATOMY
The carpal tunnel or canal is a closedspace whose dorsal, radial, and ulnarboundaries are the bones of the carpus andwhose volar limit is the transverse carpalligament. The transverse carpal ligament at-taches to the pisiform and hamate on itsulnar aspect and to the seaphoid tubercleand trapezium on its radial edge. Thus, allthe boundaries of the canal are either bonyor ligamentous and.are nonyielding in char-acter. The nine extrinsic flexor tendons ofthe fingers and thumb pass through the car-pal tunnel surrounded by the synovial mem-branes of the ulnar and radial bursae andaccompanied by the median nerve.
PATHOPHYSIOLOGY
The common denominator of the variousspecific etiologies of carpal tunnel syndromeis a relative volumetric increase in the con-tents contained within the carpal tunnel.This can be accomplished either by an actual
*Chief, Division of Plastic Surgery, Allegheny General Hospital; and Associate Professor of Surgery, Plastic, University ofPittsburgh, Pittsburgh, Pennsylvania
~Clinical Professor, Division of Plastic Surgery, University of Mississippi Medical Center, Jackson, Mississippi
Hand Clinics--Vol. 2, No. 4, November 1986 723
724 Frederick R. Heckler and Michael E. Jabaley
increase in volume or decrease in dimen-sions. Since all the boundaries of the carpaltunnel are nonyielding, an increase in con-tent results in increased pressure within thecanal and subsequently upon all of the struc-tures contained therein. Increased pres-sures within the carpal tunnel, long as-sumed to be present in symptomaticpatients, have been clearly demonstrated byGelbermanI5 and Lundborg31 using directmeasurements.
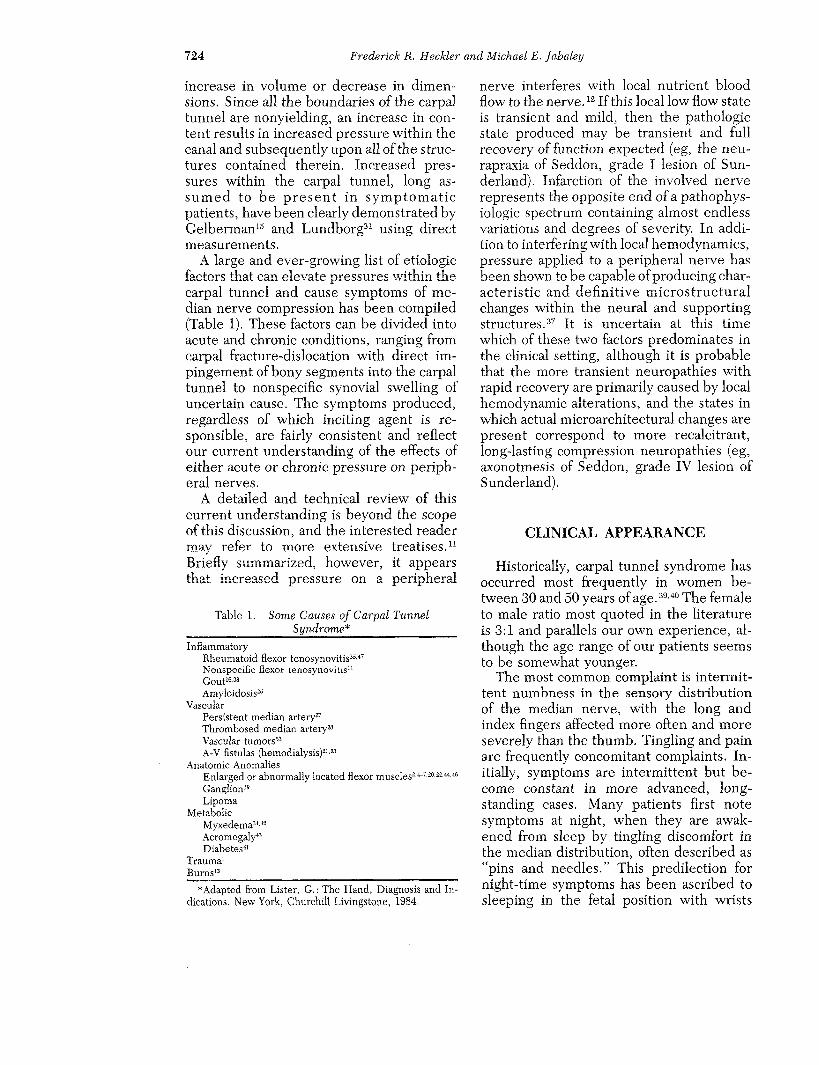
A large and ever-growing list of etiologicfactors that can elevate pressures within thecarpal tunnel and cause symptoms of me-dian nerve compression has been compiled(Table 1). These factors can be divided intoacute and chronic conditions, ranging fromcarpal fracture-dislocation with direct im-pingement of bony segments into the carpaltunnel to nonspecific synovial swelling ofuncertain cause. The symptoms produced,regardless of which inciting agent is re-sponsible, are fairly consistent and reflectour current understanding of the effects ofeither acute or chronic pressure on periph-eral nerves.
A detailed and technical review of thiscurrent understanding is beyond the scopeof this discussion, and the interested readermay refer to more extensive treatises,n
Briefly summarized, however, it appearsthat increased pressure on a peripheral
Table 1. Some Causes of Carpal TunnelSyndrome*
InflammatoryRheumatoid flexor tenosynovitisas.4rNonspecific flexor tenosynovitis~Gout~6.asAmyloidosis~
VascularPersistent median arterya
Thrombosed median artery~
Vascular tumors~a
A-V fistulas (hemodialysis)~l.~a
Anatomic AnomaliesEnlarged or abnormally located flexor musclese,~-~,~’°,z~,~4,46
GanglionI~
LipomaMetabolic
Myxedemaa<~
Acromegaly4a
Diabetes~1
Traumat
Burns~a
*Adapted from Lister, G.: The Hand, Diagnosis and In-dications. New York, Churchill Livingstone, 1984.
nerve interferes ~vith local nutrient bloodflow to the nerve, lz If this local low flow stateis transient and mild, then the pathologicstate produced may be transient and fullrecovery of function expected (eg, the neu-rapraxia of Seddon, grade I lesion of Sun-derland). Infarction of the involved nerverepresents the opposite end ofa pathophys-iologic spectrum containing almost endlessvariations and degrees of severity. In addi-tion to interfering with local hemodynamics,pressure applied to a peripheral nerve hasbeen shown to be capab!e of producing char-acteristic and definitive microstructuralchanges within the neural and supportingstructures. 3r It is uncertain at this timewhich of these two factors predominates inthe clinical setting, although it is probablethat the more transient neuropathies withrapid recovery are primarily caused by localhemodynamic alterations, and the states inwhich actual microarchitectural changes arepresent correspond to more recalcitrant,long-lasting compression neuropathies (eg,axonotmesis of Seddon, grade IV lesion ofSunderland).
CLINICAL APPEARANCE
Historically, carpal tunnel syndrome hasoccurred most frequently in women be-tween 80 and 50 years of age.ao,4° The femaleto male ratio most quoted in the literatureis 8:1 and parallels our own experience, al-though the age range of our patients seemsto be somewhat younger.
The most common complaint is intermit-tent numDness in the sensory distributionof the median nerve, with the long andindex fingers affected more often and moreseverely than the thumb. Tingling and painore frequently concomitant complaints. In-itially, symptoms are intermittent but be-come constant in more advanced, long-standing eases. Many patients first notesymptoms at night, when they are awak-ened from sleep by tingling discomfort inthe median distribution, often described as"pins and needles." This predilection fornight-time symptoms has been ascribed tosleeping in the fetal position with wrists

Evolving Concepts of Median Nerve Decompression 725
flexed, to direct pressure on the wrists bythe head, and to changes in total body fluiddistribution resulting from lying horizon-tally. For unclear reasons, the discomfort isoften relieved by shaking the hand or hang-ing it in a dependent position.
In contrast to night symptoms, many pa-tients will note the onset of symptoms atwork or while performing repetitive tasks.Furthermore, activities such as repeated fistclenching or prolonged gripping, as ingrasping a steering wheel, will initiatesymptoms, while cessation of such activitiesbrings relief. The pain of carpal tunnel syn-drome may occasionally radiate proximally,causing confusion with other pain com-plexes of the forearm, elbow, and shoulder,z4Careful questioning and examination willusually pinpoint the site of symptomatic or-igin at the wrist, even when the patient hasnot noted this as the source. Carpal tunnelsyndrome should thus be considered in thedifferential diagnosis of almost any obscuresymptom complex involving pain in theupper extremity.
Progression of the intermittent episodicnature of the symptoms in carpal tunnel syn-drome to either more prolonged or evenconstant discomfort or numbness usuallysignals more severe disease, although thedegree of actual nerve damage found at sur-gery, as well as the potential for recoveryof function, seems to be more related to theseverity of compression than to its longevity.Put another way, marked compression for arelatively short period of time has the po-tential to produce more neural damage thanminimal compression over a lon~e~ p~r~o~of time.
Weakness and atrophy of the median-in-nervated thenar muscles tend to occur laterin the course of the disease, usually aftersensory loss has been present for a pro-longed period. The patient’s perception ofthis motor palsy is often that of weakness ofgrasp, particularly pinch, and a clumsinessand loss of dexterity in manipulating smallobjects. In our own clinical practice, motorweakness in carpal tunnel syndrome pa-tients has been seen with less and less fre-quency. This is probably o~ving to a morewidespread recognition of the classical
symptom complex within the general med-ical community. As a result, patients are re-ferred for treatment much earlier in thecourse of this disease than was previouslythe case.
Not a11 patients’ symptoms involve theentire median nerve sensory distribution inthe hand. Indeed, our own patients mostcommonly complain of symptoms in only aportion of the sensory area subserved by themedian nerve--usually the long and indexfingers or the long and ring fingers (ie, thoseareas served by one of the common digitalnerves).
EXAMINATION
Sensory Disturbances
Sensory disturbances, as detected by al-terations in appreciation of touch as well asabnormal static and moving two-point dis-crimination, should always be sought andany abnormality in distribution of normalsweating noted. The 30 and 256 CPS tuningforks are also useful. Objective evidence ofsensory loss, however, is commonly notpresent as the modern-day patient will pre-sent for evaluation before such severeneural damage has occurred.
Tinel’s Sign
Tinel’s sign can be elicited in the majorityof patients. Tapping with the finger or areflex hammer over the course of the me-dian nerve at the wrist, just proximal to theflexor retinaculum, will transiently repro-duce the numbness and tingling of whichthe patient complains. Excessively firm per-cussion of the nerve may produce paresthe-sias even in normals. Simultaneous evalu-ation of the opposite wrist (if it is normal)may help identify such situations. The pres-ence of Tinel’s sign in patients with symp-toms of carpal tunnel syndrome has beenquite reliable confirmatory evidence in ourexperience and has been present in ap-proximately 80 per cent of our patients. Theabsence of Tinel’s sign does not, however,
726 Frederick R. Heckler and Michael E. ]abaIey
rule out the presence of carpal tunnel syn-drome.
Phalen’s Wrist Flexion Test
Phalen’s wrist flexion test39 is anotherhelpful confirmatory sign. The wrist isplaced in unforced but acute flexion for 60seconds. This posture causes an increase inmeasured pressure within the carpal canal,particularly marked in carpal tunnel syn-drome patients.l~ The test is positive whenmaintenance of the flexed posture repro-duees or exacerbates the patient’s symptomsof numbness or paresthesias. We have foundthis test to be positive in over 70 per centof our carpal tunnel patients. Like the Ti-nel’s sign, absence of a positive Phalen’s testdoes not completely rule out carpal tunnelsyndrome, but its presence is strong con-firmatory evidence.
Motor involvement, as evidenced bymuscle weakness or even obvious thenaratrophy, is not commonly noted in modernhand surgery practices. When present,however, it is best detected by viewing thethenar eminence in profile and comparingit with the asymptomatie hand. A flatteningof the thenar eminence can sometimes beseen relatively early (the so-called shelfsign) and is due to selective atrophy of theabductor pollieis brevis muscle.
The abductor pollieis brevis is the thenarmuscle that is most easily tested in terms ofpure median motor function (cross-inner-vation of this particular unit by branchesfrom another nerve is exeeptionaiiy rare).The patient places his or her hand on a flatsurface, palm up, in the "military salute"position (addueted against the second me-tacarpal) and is asked to palmarly abduct thethumb against the resistance of the exam-iner’s finger. Contraction of the abductorpollieis brevis can be easily visualized, andstrength can be compared with the oppositehand. Atrophy of the opponens pollieis andflexor pollieis brevis occurs relatively late inpatients with median nerve compression.
Occasionally, muscle faseieulation can beseen in the thenar muscles and is a valuablesign because it is an early sign of motor
involvement. Pulp-to-pulp pinch strength isalso useful and should be measured and re-corded. Direct evaluation of opposition isperformed by the popular technique of hav-ing the patient place the tips of the thumband either the ring or small finger togetherand resist attempts to break this pinch cir-cle. This examination has seemed to us tobe less reliable and less specific than theabductor pollieis brevis evaluation becausethe patient may use the adductor pollieisand ulnar-innervated portion of the flexorpollieis brevis and thus still be able to dem-onstrate considerable pinch power.
ELECTRODIAGNOSIS
Sophisticated eleetrodiagnostie tech-niques are available to assist in diagnosis ofperipheral nerve compression syndromes,and their applications are most widely de-veloped and best understood in relation tocompression neuropathies of the mediannerve at the wrist.3°,33,48,~z
Slowing of sensory conduction across thewrist has proven to be the most sensitive ofsuch tests, with prolongation of the distalsensory latency above 3.5 msee being pres-ent in 85 to 95 per cent of surgically con-firmed cases. The motor analogue of slowedsensory conduction, a delayed distal motorlatency, may also be measured but is asomewhat less sensitive index. Lastly, elee-tromyographie evaluation of the thenarmuscles may show signs of denervation, butonly in more advanced eases where actualaxonotmesis has already occurred.
We do not routinely use eleetrodiagnostiestudies when evaluating patients for mediannerve compression. Our experience has par-alleled that of other authorsis in this regard.In patients with fairly typical symptoms andlocalizing wrist signs (positive Phalen’s testor Tinel’s sign), eleetrodiagnosis has notcontributed additional information of clini-cal value. Patients with typical symptomsand confirmatory physical findings have uni-formly gained symptomatic relief from sur-gical therapy even if eleetrodiagnosis hasbeen interpreted as normal or minimally ab-normal. Conversely, false-negative clinical

Evolving Concepts of Median Nerve Decompression 727
diagnoses (patients with absent clinical find-ings but abnormal eleetrodiagnosis) havenot been encountered. Further, there hasbeen no good correlation noted between thedegree of eleetrodiagnostie abnormalitiesand either the severity of symptoms or theamount of nerve abnormality noted at sur-gery. 17.45 For these reasons, we do not rou-tinely evaluate eleetrophysiologie parame-ters in patients with clinical presentation ofcarpal tunnel syndrome. Rather, we reservesuch additional (and expensive) tests for pa-tients with questionable diagnoses, those inwhom the site of compression cannot beclinically localized with reasonable certaintyor who are suspected of having multiplecompression loci, and those whose symp-toms may reflect systemic disease or gen-eralized neural degenerative disease ratherthan a localized mechanical process. The lat-ter situations can be readily suspected froma careful general history and physical ex-amination and diagnosed by further appro-priate blood tests. In the final analysis, thepatient’s own cerebral "computer" remainsthe most sensitive detector of early signs ofnerve compression.
TREATMENT
Treatment of median nerve compressionmav be either surgical or nonsurgicaI. Asexperience accumulates, the indication foreach modality becomes increasingly clear.
Nonsurgical Treatment
Nonsurgieal treatment of carpal tunnelsyndrome is most appropriate when symp-toms are mild or intermittent, relativelyshort in duration, or when the inciting agentis expected to be transient in nature. Themost common such situation is carpal tunnelsyndrome of pregnancy, where symptomsare related to fluid retention and edema.Resolution of symptoms is almost universalfollowing the end of the pregnancy, and allattempts should be made to alleviate thepatient’s discomfort with nonoperativemeans. These include splinting, local ste-
roid injection, diuretics, and other meansof edema control.
Patients whose symptoms appear to havebeen precipitated by a recent change inwork habit can also often benefit by cessa-tion or alteration of the provoking activity.and nonsurgical therapy. Nonsurgical treat-ment modalities used include: (1) oral anti-inflammatory agents, (2) splinting and ele-vation, and (3) local steroid injection. Sys-temic administration of diuretics and steroidpreparations has been described, but,most cases, we have not thought that theuse of such systematically potent agents wasappropriate or advisable.
When consulted by a patient with mild,intermittent symptoms of median nervecompression at the wrist and confirmatoryclinical findings, our general therapeutic ap-proach is a graded one. We first try to de-termine if any particular occupational orrecreational activity appears to be the in-citing cause and, if so, recommend its tem-porary cessation. Simultaneously, the pa-tient is fitted for a removable volar splintthat extends from just proximal to the MPflexion crease to the proximal forearm andholds the wrist in neutral or slight dorsi-flexion. The ideal position of immobilizationseems to be one in which the thumb met-acarpal is slightly abducted and flexed. Thisposition drops the nerve away from thetransverse carpal ligament and makes theligament less tense. The splint is worn atnight (if the patient’s symptoms occur onlyat night) and during the day, if indicated. simultaneous trial of oral anti-inflammatoryagents, such as salicylates or ibuprofen, mayalso be helpful. We formerly used strongeranti-inflammatory agents such as indometh-acin, but now prefer to avoid them becauseof their potential for harmful side effects.
If nonoperative treatment is to be suc-cessful at all, clear-cut improvement or evenrelief of all symptoms will usually occurwithin 1 week. Patients who note no sig-nificant relief with splinting at 1 week willusually not benefit from persistence in suchefforts. In patients who do not respond tothis regimen, we next proceed to local ste-roid injection.
Steroid instillation into the carpal canal is

728 Frederick It. Heckler and Michael E. Jabaley
indicated in patients with intermittentsymptoms and in whom objective findingssuch as loss of two-point discrimination orthenar atrophy are not present. It can alsobe used as a provocative test to confirm thediagnosis. Other relative indications for ste-roid injections include those patients inwhom surgical therapy is contraindicated byeither age or poor general medical condi-tion. These latter situations should be quiterare, since the magnitude of the surgicaltreatment for carpal tunnel syndrome ismodest in terms of systemic stress and caneasily be carried out using local anesthesiaif necessary.
jority of our patients are seen relativelyearly in the course of this disease. Of thosewho respond favorably, however, onlyabout half (20 per cent) gain permanent re-lief. Patients whose symptoms are not re-lieved or who have recurrence of symptomsafter steroid injection should be consideredcandidates for surgical intervention. We donot favor repeated steroid instillations be-cause of the risk of tendon rupture or in-advertent nerve injury, and also because thegreat majority of patients who have recur-rent symptoms postinjection will eventuallyrequire surgery anyway.
Technique of Steroid Injection
A mixture of 0.5 mL of soluble steroidand 0.5 mL of Xyloeaine is used. The in-jection is carried out at the level of the distalwrist crease with a short 25-gauge needleangled distally to enter the carpal tunnel.This site of injection is less painful than di-rect injection through the transverse carpalligament. Our preferred skin puncture siteis just ulnar to the palmaris longus tendonas it crosses the distal wrist flexion crease.Injection here places the needle ulnar to themedian nerve but still locates the tip withinthe carpal tunnel. Injection of steroid prep-arations (or anything else) directly into themedian nerve can be deleterious and shouldbe avoided. Ifparesthesias are elicited whenthe needle enters the canal, it should bewithdrawn slightly and redirected prior toinjection to avoid such complications. Theinjection itself may temporarily aggravatesymptoms since a temporary increase intotal volume content of the carpal canal re-sults. As long as the needle itself elicits noparesthesias, one may be confident of thesafety of proceeding with injection. Splint-ing is continued following steroid instilla-tion.
We have noted relief of symptoms follow-ing carpal tunnel injection in approximately40 per cent of our patients so treated, afigure somewhat higher than that usuallyquoted. 14.39 This discrepancy may reflect thenature of our referral population: the ma-
Surgical Treatment
Surgical intervention in carpal tunnelsyndrome is indicated in patients in whomnonoperative treatment has failed, in pa-tients who show evidence of thenar muscleweakness or atrophy, in patients with re-producible, objective abnormalities on sen-sory examination, and in almost all patientswhose subjective symptoms are constantrather than intermittent. Some surgeonsrecommend a trial of conservative treatmentfor patients in these last two categories, butour own observations suggest that the greatmajority of these, too, will eventually re-quire surgical management.
Acute Carpal Tunnel Syndrome.1,13Symptoms of acute compression of the me-dian nerve at the wrist have been reportedsubsequent to a number of traumatic situ-ations, including wrist and forearm frac-tures, dislocation of the wrist, crush inju-ries, burns, high-pressure injectioninjuries, and in reperfusion following tran-sient profound ischemia (as with revascu-larization). The symptoms and clinical find-ings are similar to those described for casesof carpal tunnel syndrome in general exceptthat those findings ofchronicity, particularlythenar muscle atrophy, are not present. Ur-gent decompression of the carpal canal(along with fasciotomies of any other in-volved compartment of the extremity) is in-dicated whenever post-traumatic acute car-pal tunnel syndrome symptoms are morethan transient and mild. When in doubt, it
Evolving Concepts of Median Nerve Decompression 729
is better to proceed with nerve decompres-sion since the risk of permanent nerve dam-age seems greater in such patients.
SURGICAL TECHNIQUE FORMEDIAN NERVE DECOMPRESSION
It can be said that the ideal operation fora given pathologic or pathophysiotogie con-dition might be one that maximizes poten-tial therapeutic benefit to the patient whileminimizing potential complications andother adverse effects. The ideal operationfor carpal tunnel syndrome should have asits goals: (1) the complete decompression the median nerve and its branches, and (2)the avoidance of surgical complications in-eluding injury to the median nerve, itsmotor branch, its major and minor sensorybranches, and its palmar cutaneous branch.Injury to the vascular structures in the area,namely the superficial palmar arch and itsbranches, must also be avoided.
The skin incision used in the ideal carpaltunnel operation should allow complete ex-posure of the transverse carpal ligament andcarpal canal, should be anatomically placedto avoid major cutaneous nerve injury,should avoid trespassing on flexion creases,and should heal kindly with a good cosmeticresult. The surgical approach carried outthrough this incision should be adaptable toconcomitant procedures or unexpectedfindings, should permit complete visuali-zation of the structures at risk, and shouldbe technically simple. When necessary, itshould permit proximal or distal extension.In our hands, the operative approach to bedescribed comes closer than any other tofulfilling these ideal criteria.*
Anesthesia
General anesthesia, regional block (eitheraxillary or intravenous), and local infiltration
*This particular operative technique was first demon-strated to one of the authors by l~obert Hornet, M.D., in1975. With minor changes, it has been used continuouslyby both authors since 1975,
anesthesia~9 are all equally effective. Mostof our patients undergo surgery as outpa-tients and we have used regional or localanesthesia almost exclusively, dependingupon patient preference. A proximal he-mostatie tourniquet must always be used topermit the precise dissection and identifi-cation of anatomic structures, which is thekey to complication-free surgery.
Preoperative Markings
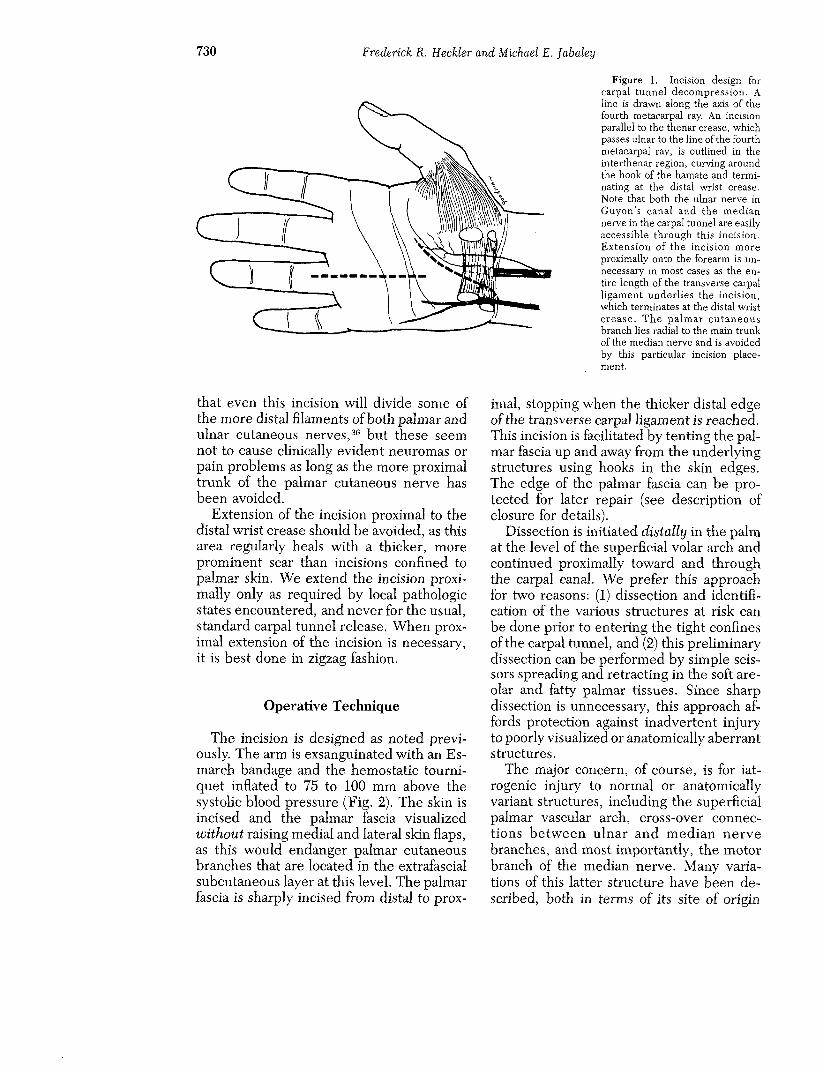
Taleisnik5I has demonstrated the courseof the palmar cutaneous branch of the me-dian nerve and the proper positioning ofpalmar incisions to avoid damaging it. Neu-romas of the palmar cutaneous branch canbe markedly symptomatic and disabling; thekey to their avoidance is proper incisionplacement.8 A mark is drawn on the palmarskin directly in line with the fourth meta-carpal ray and is extended proximally to thedistal wrist crease (Fig. 1). The trunk of thepalmar cutaneous nerve, in its course be-tween the thenar and hypothenar emi-nences, usually lies well radially to this line.Incisions in this area should, therefore,preferentially be kept ulnar to Taleisnik’sline.
We prefer an incision parallel to thethenar crease which, as it crosses the prox-imal palm, is kept ulnar to the line of thefourth metacarpal ray, and which thencurves toward the ulna around the hook ofthe hamate, terminating at the distal wristcrease. In the routine ease, it is unnecessaryto incise proximal to this crease. Such anincision permits complete exposure of thetransverse carpal ligament, allows direct vis-ualization of all structures at risk during di-vision of the transverse carpal ligament,avoids major cutaneous nerve trunks, andfollows normal anatomic creases, therebypermitting favorable healing and minimalscarring. It is important that the incisioncurve around the hook of the hamate ratherthan passing directly over it (such a searlocation tends to cause prolonged local post-operative tenderness, probably because ofits positioning directly over bone at a fre-quently traumatized site). It is fair to note
730 Frederick R. Heckler and Michael E. ]abaley
Figure I. Incision design forcarpal tunnel decompression, Aline is drawr~ along the axis o£ thefourth metacarpal ray. An incisionparallel to the thenar crease, whichpasses ulnar to the line of the fourthmetacarpal ray, is outlined in theinterthenar region, curving aroundthe hook of the hamate and termi-nating at the distal wrist crease,Note that both the ulnar nerve inGuyon’s canal and the mediannerve in the carpal tunnel are easilyaccessible through this incision.Extension of the incision moreproximally onto the forearm is un-necessary in most cases as the en-tire length of the transverse carpalligament underlies the incision,which terminates at the distal wristcrease. The palmar cutaneousbranch lies radial to the main trunkof the median nerve and is avoidedby this particular incision place-ment.
that even this incision will divide some ofthe more distal filaments of both palmar andulnar cutaneous nerves,a6 but these seemnot to cause clinically evident neuromas orpain problems as long as the more proximaltrunk of the palmar cutaneous nerve hasbeen avoided.
Extension of the incision proximal to thedistal wrist crease should be avoided, as thisarea regularly heals with a thicker, moreprominent scar than incisions confined topalmar skin. We extend the incision proxi-mally only as required by local pathologicstates encountered, and never for the usual,standard carpal tunnel release. When prox-imal extension of the incision is necessary,it is best done in zigzag fashion.
Operative Technique
The incision is designed as noted previ-ously. The arm is exsanguinated with an Es-march bandage and the hemostatic tourni-quet inflated to 75 to 100 mm above thesystolic blood pressure (Fig. 2). The skin incised and the palmar fascia visualizedwithout raising medial and lateral skin flaps,as this would endanger palmar cutaneousbranches that are located in the extrafascialsubcutaneous layer at this level. The palmarfascia is sharply incised from distal to prox-
imal, stopping when the thicker distal edgeof the transverse carpal ligament is reached.This incision is facilitated by tenting the pal-mar fascia up and away from the underlyingstructures using hooks in the skin edges.The edge of the palmar fascia can be pro-tected for later repair (see description ofclosure for details).
Dissection is initiated distally in the palmat the level of the superficial volar arch andcontinued proximally toward and throughthe carpal canal. We prefer this approachfor two reasons: (1) dissection and identifi-cation of the various structures at risk canbe done prior to entering the tight confinesof the carpal tunnel, and (2) this preliminarydissection can be performed by simple scis-sors spreading and retracting in the soft are-olaf and fatty palmar tissues. Since sharpdissection is unnecessary, this approach af-fords protection against inadvertent injuryto poorly visualized or anatomically aberrantstructures.
The major concern, of course, is for iat-rogenic injury to normal or anatomicallyvariant structures, including the superficialpalmar vascular arch, cross-over connec-tions between ulnar and median nervebranches, and most importantly, the motorbranch of the median nerve. Many varia-tions of this latter structure have been de-.scribed, both in terms of its site of origin
Evolving Concepts of Median Nerve Decompression 731
and its course.2~ For this reason, it is essen-tial to visualize the motor branch during thisdissection, and the easiest and most con-sistent place to do this is in the palm at thesite where the nerve approaches and entersthe thenar muscles. This site, just distal tothe distal edge of the transverse carpal lig-ament, is quite consistent, and most motorbranches, regardless of site of origin or var-iations in course, can be located here. Evenif one of the rare situations is encounteredwhere the motor branch enters the thenarmuscles at another point, the surgeon willat least be alerted to this situation prior tobeginning dissection in the tight carpalcanal where visualization is more difficult.
After incision of the palmar fascia distalto the ligament, the first structure to belocated is the superficial vascular arch.Gentle, blunt spreading with scissors in thepalmar fat allows easy visualization of thearch and its common digital branch to thering-long finger interspace. This latterstructure in turn serves as a handy guide tothe common digital branch of the mediannerve to these same fingers lying just ad-jacent to it. Most commonly, this is the ul-narmost median nerve, and dissection caneasily be continued proximally, again byspreading the palmar fat. Since no sharpdissection is required, risk to local struc-tures is minimal. Regardless, proximal dis-section should be done under direct visionsince branches from the ulnar nerve to themedian digital nerves are sometimes pres-ent and must not be injured.
As dissection proceeds proximally, thedistal edge of the transverse carpal ligamentis encountered. Simultaneously, it can benoted that the main median trunk has beenreached.
Division of the transverse carpal ligamentis not initiated yet. Rather, dissection is car-ried in a radial direction, again using onlyblunt separation of fatty perineural tissues,and the motor median branch is specificallyidentified. Identification of the motorbranch is facilitated by placing traction onthe thenar edge of the skin incision at rightangles to the palmar surface, a maneuverthat makes the motor branch stand out inits course to the thenar muscles. Once iden-
tiffed at its site of muscular entry, the originof the motor branch from the main trunk,normal or variant, is easily noted.
At this relatively early point in the op-eration, the surgeon has identified and caneasily protect all important structures at riskand has done so prior to initiating sharpdivision of the transverse carpal ligament.Division of the ligament can now proceedwith relative assurance. We prefer to inserta hemostat between the ligament and themedian nerve, visualize the exposed seg-ment of nerve, and then incise that portionof the median nerve until complete divisionof the ligament is accomplished. In addi-tion, the antebraehial fascia is incised for ashort distance proximal to the wrist crease.This latter maneuver can be accomplishedby elevating rather than cutting the over-lying skin and fat, thereby avoiding injuryto cutaneous nerve branches containedtherein.
This particular incision easily allows si-multaneous evaluation and release of Gu-yon’s canal, if indicated. This passageway isalso most easily located in retrograde fash-ion by tracing the vessels of the superficialpalmar arch back toward the ulnar arteryinto Guyon’s canal. Here, the ulnar nerveand artery can be directly visualized anddecompressed, if necessary.
Closure of the incision is in one layerusing nonabsorbable sutures in the’skin.The divided transverse carpal ligament isnot sutured or reapproximated, but thereseems to be a good reason for suturing theoverlying palmar fascia. The transverse ear-pal ligament holds the pillars of the handtogether to form the proximal transversearch, and an effort should be made to pre-serve this arch.
Intraneural Neurolysis
This procedure has been advocated as anadjunct to carpal tunnel decompression.9 Itinvolves epineurotomy with dissection andlysis of fibrosis between fascicles and fas-cicular groups. Loupe or microscopic mag-nification is required and the latter is pre-ferred. Such extensive dissection carries its
732 Frederick ~. Heckler and Michael E. Jabaley
F
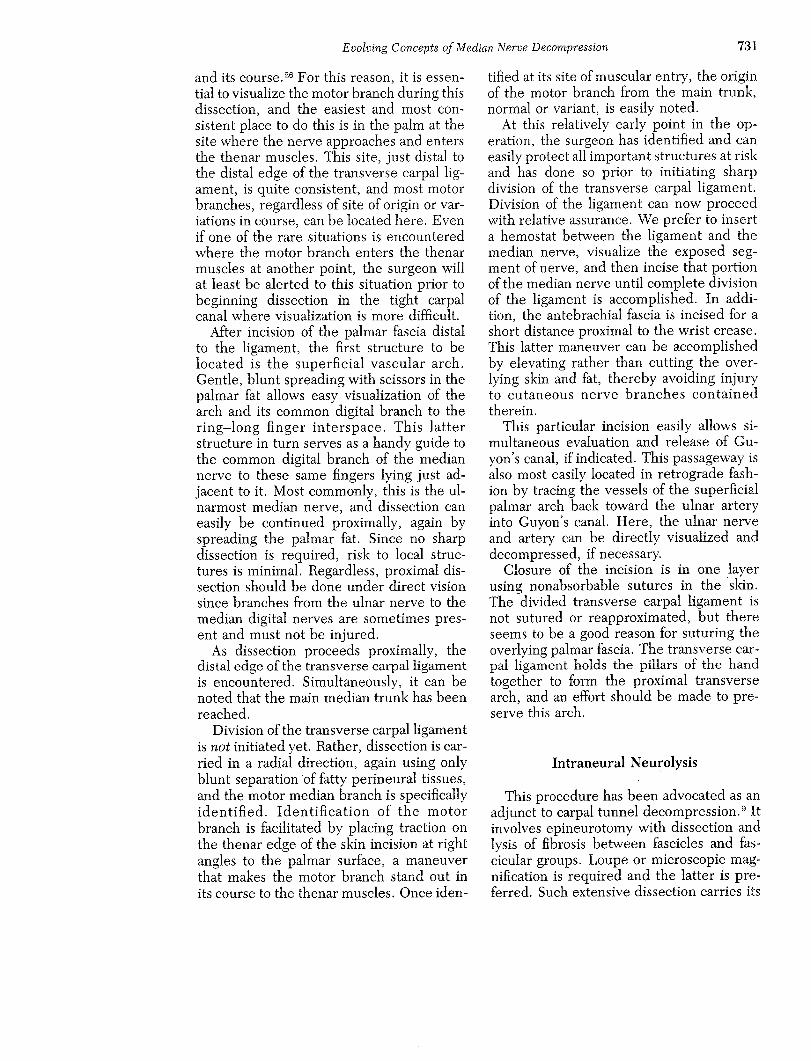
Figure 2. Operative technique.A, The operative incision has been designed as noted in Figure 1. The anticipated positions of the transverse carpal ligament,the median nerve, and the palmar cutaneous branch are also outlined. Most compressions of the median nerve occur beneaththe distal portion of the ligament (that area which lies in the center of this incision). B, The skin incision is made and carrieddown through the subcutaneous fat to the palmar fascia. This fascia is tented up with hooks and then incised. C, The commondigital nerve leading to the long-ring finger interspace is easily located by a bIunt spread technique in the loose palmar fat.Dissection will be continued proximally along the ulnar side of this common digital branch until the thickened distal edgeof the transverse carpal ligament is reached. Note that no sharp dissection is required in this area, thereby minimizing riskto vital structures during the dissection. D, Before beginning dissection into the tight confines of the carpal tunnel, bluntdissection is next immediately carried to the radial side of the main trunk of the median nerve. Traction upward on thethenar edge of the skin incision will allow easy localization of the motor branch o£ the median nerve (here demonstratedwith the curved hemostat). Having visualized this structure as well as the main trunk of the median nerve, the commondigital nerve branches, and the superficial palmar vascular arch and its branches, all vital structures at risk have now beenseen and can easily be protected. E, The surgeon next proceeds with relative assurance into the tight confines of the carpaltunnel, incising the transverse carpal ligament from distal to proximal. This is done by placing a hemostat between themedian nerve and the transverse carpal ligament and incising the ligament by proceeding proximally along the ulnar borderof the median nerve. F, A few centimeters of antebrachial fascia are incised subcutaneously proximal to the distal wristcrease by elevating the overlying skin and fat.
Evolving Concepts of Median Nerve Decompression 733
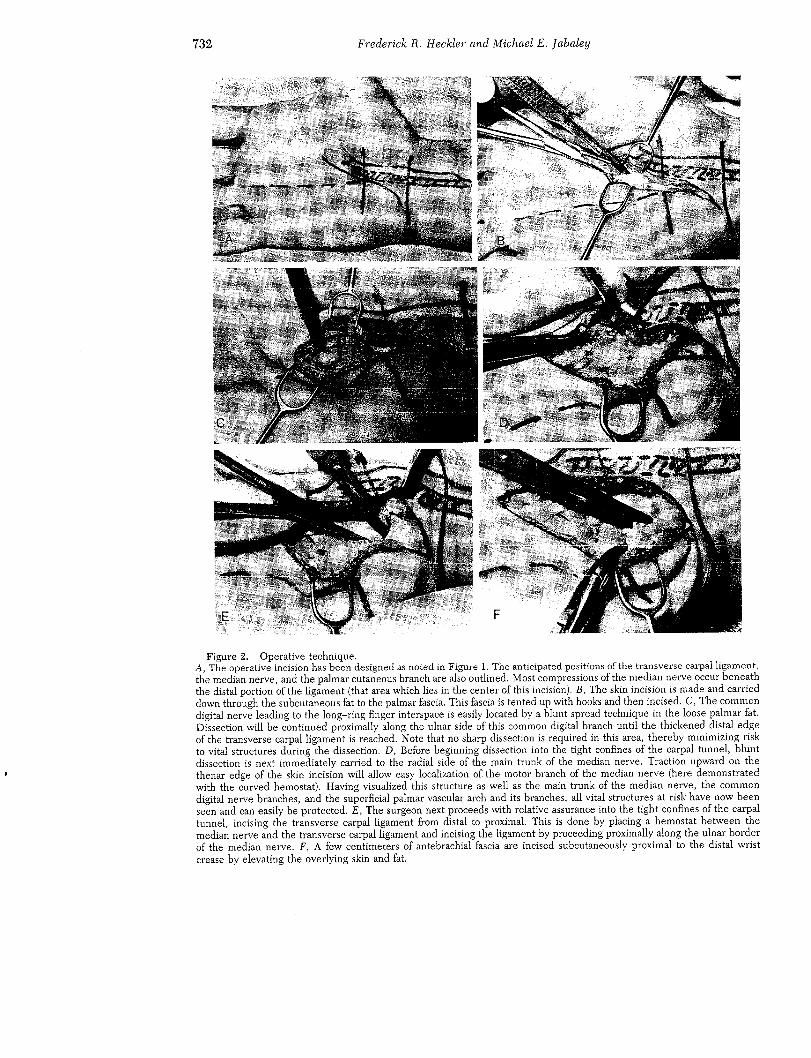
Figure 2. G, The completed dissection, showing the wide exposure oi’the median nerve and all other regional structuresincluding the common digital branches, the thenar motor branch, and the median main trunk. Note that this incision giveswide access to all structures of concern without extension proximal to the wrist crease. H, Guyon’s canal is easily exploredthrough the same incision by tracing the sllper~cial palmar vascular arch vessels proximally toward the ulnar artery. The tipof" the hemostat is entering Guyon’s canal. I, A different patient, viewed from the thenar side (fingers to the right, i’orearmto the left), in whom carpal tunnel release as well as release of Cuyon’s canal has been carried out. Note the ease of totalexposure of both structures. The probe is in Cuyon’s canal, which is being decompressed. ], A typical postoperative resultat 3 months. As long as the incision is confined to the palm and follows natural crease lines, an excellent cosmetic result isexpected.
734 Frederick 1:1. Heckler and Michael E. JabaIey
o~vn risks of both direct mechanical nerveinjury and additional postoperative scarringowing to the dissection itself, and one mustalways be sure that the potential benefit out-weighs the risk before undertaking internalneurolysis.
Indications for internal neurolysis are lim-ited to those conditions in which there isscarring or fibrosis of the external and/orinternal epineurium. These conditions pro-duee constriction within the nerve, whichis unlikely to be relieved by ligament di-vision alone. Indications include: (1) muscleatrophy, (2) fixed sensory loss, (3) severeeausalgia, (4) previous unsuccessful opera-tion, or (5) a history, such as crush fracture,suggesting that neurolysis will be necessary.It can be seen from the foregoing that in-ternal neurolysis is indicated only in themore advanced eases. When it is indicated,we do not carry out complete internal neu-rolysis, but rather approach only the in-volved fascicles. An example would be a pa-tient who has a fixed sensory loss withabnormal two-point discrimination in thelong finger, but only intermittent symptomsin the remainder of the median nerve dis-tribution. In such a situation, the involvednerve branch is located distally and then itsfascicles traced proximally through the maintrunk of the nerve in the carpal canal. Theremainder of the nerve is not disturbed,thereby limiting the risk of postdisseetionfibrosis or injury to intraneural blood ves-sels.
and encouraged throughout the recupera-tive course. Sutures are removed in 6 to 9days. Patients are advised to avoid stren-uous activity for 6 weeks. There seems tobe no problem in resuming activities thatinvolve fingertip opposition, but the grip-ping of objects, such as hammer handles orpliers, may be painful for several weeks.
It is important to recognize that recoveryfrom median nerve compression is based onthe pathologic condition of the nerve anddoes not always occur at the same rate ofspeed. If the changes in the nerve are bio-chemical and not structural (neurapraxia),then recovery will be prompt and may benoticeable in a matter of days or weeks.Conversely, if axonotmesis is present and asegmental demyelination has occurred, thepatient should be told that recovery mayrequire 6 months or longer. In either ease,patients should be aware that gradual im-provement may occur for 2 to 3 years andsubtle improvement should be anticipatedfor at least that long. It should be borne inmind that not all fibers or fascicles areequally injured and not all recover at thesame rate or to the same degree.
The rehabilitation process can be helpedby early initiation of range-of-motion exer-cises, edema control, and sear massage.Strengthening exercises should be addedwhen pain and early inflammation have sub-sided.
POSTOPERATIVE CARE
At the completion of wound closure, avolar splint is applied that extends from justproximal to the MP flexion crease to theproximal forearm and that holds the wristin slight extension and the thumb in op-position. This posture is maintained for 2weeks and for a third week at night only. Aflexed posture of the wrist must be avoidedduring the initial healing phase to preventprolapse of the contents of the carpal canalthrough the open transverse carpal liga-ment. Active finger flexion and thumb mo-tion are initiated within 24 hours of surgery
SPECIAL SITUATIONS
The motor branch of the median nervemay occasionally traverse the transversecarpal ligament independently in a separatefibrous canal, and the palmar cutaneousnerve commonly does this. For this reason,it is possible to have an isolated compressionneuropathy of either of these nerves, eitheras part of or completely independent of thecarpal tunnel syndrome.49,5° Specific explo-ration and, if necessary, decompression ofeach respective nerve should be carried outwhen isolated thenar weakness is the pre-senting symptom, when thenar weakness ispresent in any carpal tunnel patient, and
Evolving Concepts of Median Nerve Decompression 735
when palmar cutaneous sensory symptoms scribed,a but we do think that their meritsare present, have not received adequate emphasis.
CONCLUSIONS
Carpal tunnel decompression has becomeone of the most commonly performed handoperations and one of the most successful.When diagnosis is made relatively early, im-provement or complete relief of symptomsis the rule. Complications are infrequent,and few reports in the literature offer anal-yses of postoperative problems.1°,3z Suchcomplications, when they do occur, can becatastrophic, for they involve important sen-sory or motor branches of the median nerve.The absence of large reported series of com-plications does not necessarily mean thatthey do not occur. Several patients havebeen referred to us over a 10-year periodwith incorrectly placed incisions and post-operative palmar cutaneous nerve neuro-mas. Two patients have been seen with sur-gical injuries to the median motor branch,and we are aware of three patients withmajor hematomas requiring reoperation fol-lowing laceration of the palmar vessels dur-ing carpal tunnel release. Finally, we havereoperated on a number of patients withincompletely divided ligaments, a problemthat may be the result of blind ligamentdivision through a transverse wrist incision.
We strongly believe that the key to avoid-ance of such problems is to approach sur-gery of the carpal tunnel as a nerve dissec-tion and decompression rather than as aligament release. Such a change in mind setwill engender the modest adjustments intechnique requisite to complication-freenerve surgery. The requisites to such sur-gery are complete visualization and subse-quent protection of all structures at risk.Only some forms of longitudinal incisionwill allow such visualization, and the pre-viously popular transverse wrist incision ismentioned only to be condemned.
The surgical approach described hasproven to be easy to use, easy to teach, andreliable. No originality is claimed for eitherthe incision or the surgical approach de-
REFERENCES
1. Adamson, J., Snouji, S., Horton, C., et al.: The acutecarpal tunnel syndrome. Plast. I~econstr. Surg.,47:332, 197i.
2. Aghasi, M., l~zetelny, V., and Axer, A.: The flexor dig-itorum sublimis as a cause of bilateral carpal tunnelsyndrome and trigger wrist. J. Bone Joint Surg.,62A:134, 1980.
3. Ariyan, S., and Watson, H.K. : The palmar approach forthe visualization and release of the carpal tunnel: Ananalysis of 429 cases. Plast. Reconstr. Surg., 60:539,1977.
4. Ashby, B.S.: Hypertrophy of the palmaris longus mus-cle. J. Bone Joint Surg., 46B:230, 1964.
5. Baekhouse, K., and Churchill-Davidson, D.: Anoma-lous palmaris longus muscle producing carpal tunnel-like compression. Hand, 7:22, I975.
6. Brones, M.F., and Wilgis, S.: Anatomical variations ofthe palmaris longus causing carpal tunnel syndrome:Case reports. Plast. Reconstr. Surg., 62:798, 1978.
7. Butler, B., and Bigley, E.: Aberrant index (first) lumbri-cal tendinous origin associated with carpal tunnel syn-drome: A ease report. J. Bone Joint Surg., 53A:I60,1971.
8. Carroll, R., and Green, D.: The significance of the pal-mar cutaneous nerve at the wrist. Clin. Orthop.,83:24, 1972.
9. Curtis, I~.M., and Eversmann, W.: Internal neurolysisas an adjunct to the treatment of carpal tunnel syn-drome. ~. Bone Joint Surg., 55A:733, 1973.
10. Das, S., and Brown, H,: In search of complications incarpal tunnel decompression. Hand, 8:243, 1976.
11. Da~vson, D., Hallett, M., and Millender, L.: Entrap-ment Neuropathies. Boston, Littlc, Brown and Com-pany, 1983.
12. Eversmann, W., and Ritsick, J.: Intraoperative changesin motor nerve conduction latency in carpal tunnelsyndrome. ~. Hand Surg., 3:77, 1978.
13. Fissette, J., Onkelinx, A., and Fandi, N.: Carpal andGuyon tunnel syndrome in burns at the wrist. J. HandSurg., 6:13, 1981.
14. Gelberman, t~., Aronson, D., and Weisman, M.: Carpaltunnel syndrome: ItesuIts of a postoperative trial ofsteroid injection and splinting. ]’. Bone joint Surg.,62A:1181, 1980.
15. Gelberman, R., Hergenroeder, P., Hargens, A., et al.:The carpal tunnel syndrome: A study of carpal canalpressures. J. Bone Joint Surg., 63A:380, 1981.
16. Green, E., Dilworth, J., and Levitin, P.: Tophaceousgout: An unusual cause of bilateral carpal tunnel syn-drome. J.A.M.A., 237:2747, 1977.
i7. Goodwill, C.J. : The carpal tunnel syndrome: Long termfollow-up showing relation of latency measurementsto response to treatment, Ann. Phys. Med., 8:i2,1965.
18. Grundberg, A.: Carpal tunnel decompression in spiteof normal electromyography. Am. J. Hand Surg.,8:348, 1983.
19. Harvey, F., and Bosanquet, J.: Carpal tunnel syndromecaused by simple ganglion. Hand, 13:164, 1981.
20. Hayes, C.W.:Anomalous flexor digitorum sublimiswithincipient carpal tunnel syndrome. Plast. Reconstr.Surg., 53:479, 1974.
736 Frederick R. Heckler and Michael E. Jabaley
21. Holtman, B., and Anderson, C.: Carpal tunnel syn-drome following vascular shunts for hemodialysis.Arch. Surg., 112:65, 1977.
‘29.. Jabaley, M.E.: Personal observations on the role of thelumbrical muscle in carpal tunnel syndrome. J. HandSurg., 3:8’2, i978.
23. Kenzora, J.: Dialysis carpal tunnel syndrome. Or-thopedics, 1:195, i978.
24. Kummel, B., and Zazanis, G.: Shoulder pain as thepresenting complaint in carpal tunnel syndrome.Clin. Orthop., 92:’227, 1973.
‘25. Kyle, R.A., and Bayrd, E.: Amyloidosis: Review of’236cases. Medicine, 54:27i, 1975.
226. Lanz, U.: Anatomical variations of the median nerve inthe carpal tunnel. J. Hand Surg., 2:44, i977.
2227. Lavey, E., and Pearl, R.: Patent median artery as acause of carpal tunnel syndrome. Ann. Plast. Surg.,7:236, 1981.
‘28. Levy, M., and Pauker, P.: Carpal tunnel syndrome dueto thrombosed persisting median artery: A case re-port. Hand, I0:65, 1978.
29. Lichtman, D., Florio, R., and Mack, G.: Carpal tunnelrelease under local anesthesia: Evaluation of the out-patient procedure. J. Hand Surg., 4:544, I979.
30. Loong, S.: The carpal tunnel syndrome: A clinical andelectrophysiologic study of 250 patients. Proc. Aust.Assoc. Neurol., 14:5i, 1977.
3i. Lundborg, C., Gelberman, R., Minteer-Convery, M.,et al.: Median nerve compression in the carpal tun-nel--functional response to experimentally inducedpressure. J. Hand Surg., 7:9.52, 1982.
32. MacDonald, R., Lichtman, D., Hanlon, J., et al.: Com-plications of surgical release for carpal tunnel syn-drome. J. Hand Surg., 3:70, 1978.
33. Melvin, J., Schuchmann, J., and Lanese, R.: Diagnosticspecificity of motor and sensory nerve conduction var-iables in the carpal tunnel syndrome. Arch. Phys.Med. Rehabil., 54:69, 1973.
34. Murray, I., and Simpson, J.: Acroparesthesias in myxe-dema: A clinical and e!ectromyographic study. Lan-cet, 1:1360, I958.
85. Nakano, K.: Entrapment neuropathies in rheumatoidarthritis. Orthop. Clin. North Am., 6:‘243, 1975.
36. Nalebuff, E., and Smith, J.: Preservation of the terminalbranches of the median palmar cutaneous nerve incarpal tunnel syndrome. Orthopedics, 2:370, i979.
37. Ochoa, J.: Nerve fiber pathology in acute and chroniccompression. In Omer, G., and Spinner, M. (eds.):Management of Peripheral Nerve Problems. Phila-delphia, W.B. Saunders, 1980.
38. O’Hara, L., and Levin, M.: Carpal tunnel syndromeand gout. Arch. Intern. Med., 120:180, 1967.
39. Phalen, G.S.: The carpal tunnel syndrome: Seventeenyears experience in diagnosis and treatment of sixhundred fifty-four hands. J. Bone Joint Surg.,48A:‘21I, i966.
40. Phalen, G.S.: The carpal tunnel syndrome: Clinicalevaluation of 598 hands. Clin. Orthop., 83:229, i972.
41. Phillips, t~.S.: Carpal tunnel syndrome as a manifesta-tion of systemic disease. Ann. IRheurn. Dis., 26:59,1967.
422. Purnell, D., Daly, D., and Lipscomb, P.: Carpal tunnelsyndrome associated with myxedema. Arch. Intern.Med., 108:751, 1961.
43. Schiller, F., and Kolb, F.O.: Carpal tunnel syndromein acromegaly. Neuroiogy, 4:371, 1954.
44. Schultz, R., Endler, P., and Huddleston, H.: Anoma-lous median nerve and an anomalous muscle belly ofthe first lumbrieal associated with carpal tunnel syn-drome. J. Bone Joint Surg., 55A:1744, 1973.
45. Shivde, A., Dreizin, I., and Fisher, M.: The carpaltunnel syndrome: A clinical-electrodiagnostie analy-sis. Electromyogr. Clin. Neurophysiol., 21:143, 1981.
46. Smith, R.J.: Anomalous muscle belly of flexor digitorumsublimis causing carpal tunnel syndrome. J. BoneJoint Surg., 53A:I’215, 197i.
47. Smukler, N.M., Patterson, J., Lorenz, H., et al.: Theincidence of carpal tunnel syndrome in patients withrheumatoid arthritis. Arthritis Rheum., 6:2298, 1963.
48. Spindler, H., and Dellon, A. L. : Nerve conduction stud-ies and sensibility testing in carpal tunnel syndrome.J. Hand Surg., 7:‘260, i9822.
49. Spinner, M.: Injuries to the Major Branches of the Pe-ripheral Nerves of the Forearm. Edition 22. Philadel-phia, W.B. Saunders, 1978, pp. ‘203-206.
50. Stellbrink, G.: Compressionofthepalmarbranchofthemedian nerve by atypical palmaris !ongus muscle.Hand Chirurgie, 4:455, 1979~.
51. Taleisnik, J.: Palmar cutaneous branch of the mediannerve. J. Bone Joint Surg., 55A:1212, 1973.
52. Thomas, I.E., Lambert, E., and Cseuz, E.: Electro-diagnostic aspects of the carpal tunnel syndrome.Arch. Neurol., 16:635, 1967.
53. Tomkins, D.G.: Median neuropathy in the carpaltunnelcaused by tumor-like conditions. J. Bone Joint Surg.,49A:737, 1957.
320 East North AvenuePittsburgh, Pennsylvania 152~2-9986