evaluation of hiv counseling and testing in anc settings
TRANSCRIPT

Population Council Population Council
Knowledge Commons Knowledge Commons
HIV and AIDS Social and Behavioral Science Research (SBSR)
2009
Evaluation of HIV counseling and testing in ANC settings and Evaluation of HIV counseling and testing in ANC settings and
adherence to short course antiretroviral prophylaxis for PMTCT in adherence to short course antiretroviral prophylaxis for PMTCT in
Francistown, Botswana Francistown, Botswana
Carolyn Baek Population Council
Tracy Creek
Lee Ann Jones
Louis Apicella Population Council
Jennifer Redner Population Council
See next page for additional authors
Follow this and additional works at: https://knowledgecommons.popcouncil.org/departments_sbsr-hiv
Part of the Health Policy Commons, Immune System Diseases Commons, International Public Health
Commons, Maternal and Child Health Commons, Medicine and Health Commons, Public Health
Education and Promotion Commons, Virus Diseases Commons, and the Women's Health Commons
How does access to this work benefit you? Let us know! How does access to this work benefit you? Let us know!
Recommended Citation Recommended Citation Baek, Carolyn, Tracy Creek, Lee Ann Jones, Louis Apicella, Jennifer Redner, and Naomi Rutenberg. 2009. "Evaluation of HIV counseling and testing in ANC settings and adherence to short course antiretroviral prophylaxis for PMTCT in Francistown, Botswana," Horizons Final Report. Washington, DC: Population Council.
This Report is brought to you for free and open access by the Population Council.

Authors Authors Carolyn Baek, Tracy Creek, Lee Ann Jones, Louis Apicella, Jennifer Redner, and Naomi Rutenberg
This report is available at Knowledge Commons: https://knowledgecommons.popcouncil.org/departments_sbsr-hiv/27
Horizons Program
Centers for Disease Control and Prevention
Evaluation of HIV Counseling and Testing in ANC Settings and Adherence to Short Course
Antiretroviral Prophylaxis for PMTCT in Francistown, Botswana
Evaluation of HIV Counseling and Testing in ANC Settings and Adherence to Short Course
Antiretroviral Prophylaxis for PMTCT in Francistown, Botswana
Carolyn Baek1, Tracy Creek2, LeeAnn Jones1, Louis Apicella1, Jennifer Redner1, and Naomi Rutenberg1
Authors’ affiliations at the time of the study:
1Horizons/Population Council 2Centers for Disease Control and Prevention
Acknowledgments The principal investigators for this study were Tracy Creek (Centers for Disease Control and Prevention) and Carolyn Baek and Naomi Rutenberg (Horizons/Population Council, New York). Louis Apicella (Horizons/Population Council, Washington DC) and Jennifer Redner (formerly Horizons/Population Council, Washington DC) provided data support. LeeAnn Jones (Horizons/Population Council, Washington DC) contributed to data analysis and the writing of this report and Ellen Weiss (Horizons/International Center for Research on Women, Washington DC) provided technical and editorial comments. The authors would like to thank Carolyn Wilson and Vanessa Beyleveld from Premiere Personnel in Gabarone, Botswana for their important contributions in data collection. The authors are grateful to the many women in Francistown, Botswana, who were willing to be interviewed in this study. Many thanks are also extended to the providers for their active participation in this study. The authors would like to acknowledge the United States Agency for International Development and the President’s Emergency Plan for AIDS Relief for providing funding support for the evaluation. The authors would also like to acknowledge the Centers for Disease Control and Prevention’s BOTUSA program.
The Horizons Program is implemented by the Population Council in collaboration with the International Center for Research on Women, International HIV/AIDS Alliance, PATH, Tulane University, Family Health International, and Johns Hopkins University. This study and final report were made possible by the President’s Emergency Plan for AIDS Relief and
the generous support of the American people through the United States Agency for International Development (USAID) under the terms of Cooperative Agreement No. HRN-A-00-97-00012-00. The contents are the responsibility of the Horizons Program and do not necessarily reflect the views of USAID or the United States Government. Published in March 2009.
the The Population Council is an international, non-profit, nongovernmental institution that seeks to improve the well-being and reproductive health of current and future generations around
world and to help achieve a humane, equitable, and sustainable balance between people and resources. The Council conducts biomedical, social science, and public health research and helps build research capacities in developing countries. Established in 1952, the Council is governed by an international board of trustees. Its New York headquarters supports a global network of regional and country offices. Copyright © 2009. The Population Council Inc. Suggested citation: Baek, Carolyn, Tracy Creek, LeeAnn Jones, Louis Apicella, Jennifer Redner, and Naomi Rutenberg. 2009. “Evaluation of HIV counseling and testing in ANC settings and adherence to short course antiretroviral prophylaxis for PMTCT in Francistown, Botswana,” Horizons Final Report. Washington, DC: Population Council. This document may be reproduced in whole or in part without permission of the Population Council provided full source citation is given and the reproduction is not for commercial purposes.
Table of Contents
Abbreviations
Executive Summary 1
Introduction 5
Overview of PMTCT in Botswana 5
Evaluation objectives 6
Methods 7
Overview 7
Ethical procedures 7
Eligibility, recruitment, and data collection procedures 8
Development of evaluation instruments and training of interviewers 9
Limitations of the study 9
Results 11
Profile of respondents 11
HIV counseling and testing and post-test information about ARV prophylaxis and therapy 14
Receipt of AZT for prophylaxis and adherence to regimen 23
Operational successes and barriers 30
Community resources 32
Discussion and Recommendations 33
HIV counseling and testing 33
AZT receipt and adherence 35
Community resources 35
Recommendations 36
References 37
Abbreviations AIDS Acquired immune deficiency syndrome ANC Antenatal care ARV Antiretroviral AZT Zidovudine HIV Human immunodeficiency virus MTCT Mother-to-child transmission NRH Nyangabgwe Referral Hospital PMTCT Prevention of mother-to-child transmission WHO World Health Organization
Evaluation of HIV Counseling and Testing in ANC Settings
Executive Summary Worldwide, it is estimated that two million children are infected with HIV (USAID 2005). The vast majority of these infections are the result of mother-to-child transmission (MTCT) of the virus during pregnancy, labor, or breastfeeding. However, there are effective methods for prevention of mother-to-child transmission (PMTCT). Botswana is one of the first countries in the developing world with a national PMTCT program that uses an efficacious and complex regimen to reduce vertical transmission. At the time of this evaluation (August – December 2005), the standard of care for prevention of MTCT of HIV in Botswana included three-drug antiretroviral therapy for HIV-infected women with a CD4 count of < 200; twelve weeks of zidovudine (AZT) for women with CD4>200 (300 mg AZT in the morning and 300 mg AZT in the evening); four weeks of AZT for their infants; single-dose maternal and infant nevirapine (NVP); and 12 months of free infant formula. Botswana’s PMTCT program also provided routine HIV testing for all pregnant women during antenatal care (ANC) to identify HIV-positive women for prophylaxis or treatment. While programs often report the number of individuals beginning AZT and receiving nevirapine for PMTCT, effectiveness is dependent on the level of adherence of individuals to these regimens. To describe adherence of pregnant women to the current PMTCT regimen, the Horizons Program of the Population Council, in collaboration with the Centers for Disease Control and Prevention (CDC) and Premiere Personnel in Botswana, conducted an evaluation to describe HIV-related services provided to women during their pregnancies, document the content of post-test counseling sessions for HIV-positive pregnant women, whether HIV-positive women remembered what had been discussed, the extent of AZT adherence based on self-reports, and the operational successes and barriers to adherence to AZT for PMTCT. Methods Francistown, Botswana’s second largest urban area, served as the study location for this evaluation. Data were collected from August-December 2005 at 10 primary health clinics, one hospital, and during home visits. In order to evaluate post-test counseling content, providers of PMTCT services (n = 43) were interviewed and post-test counseling sessions with HIV-positive pregnant women were observed (n = 22). For evaluation of adherence to AZT for PMTCT, HIV-positive pregnant women at antenatal clinics (n = 122) and HIV-positive women in the postnatal ward (n = 125) were interviewed. Additionally, home visits were conducted with a subset of women interviewed on the postnatal ward to evaluate adherence to the four week infant AZT regimen (n = 34). Key Findings Provider-initiated routine HIV testing in the antenatal care settings has increased coverage, and is both feasible and acceptable. Nearly all HIV-positive pregnant women in this evaluation had tested for HIV during their current pregnancy and only five women approached for the study were not eligible to participate because they did not know their HIV status. In contrast, only a third of women with a previous birth had tested during their
1
previous pregnancy, indicating that Botswana’s 2004 opt-out testing policy has increased testing coverage, enabling health providers to provide PMTCT services to more HIV-positive women. Moreover, almost all HIV-positive women indicated that they wanted to take the HIV test when they were pregnant, demonstrating that not only is HIV testing feasible, but it is also acceptable in this setting. Most HIV-positive pregnant women received one post-test counseling session. More than two-thirds of all HIV-positive women interviewed in this evaluation had one post-test counseling session at the ANC clinic. The median time providers reported spending on a post-test counseling session with HIV-positive women was 28 minutes, with 20 minutes being the most common response. Providers had different notions of what information was essential to communicate to HIV-positive pregnant women, and observed counseling sessions revealed incomplete delivery of important information. When providers were asked what general information they believed was important in post-test counseling for HIV-positive women, many combinations of responses were given and only two responses were mentioned by more than half of the respondents. These were evaluating women for ARV therapy and using condoms. Also, responses were different when stratified by provider type, with results for nurses and midwives varying from those given by HIV counselors. In addition to there being little standardization in provider opinions of essential information, there were also differences found related to AZT adherence counseling. While over half of those providing adherence counseling said they discussed the importance of taking the correct dose and taking it on schedule, far fewer providers reported discussing other important topics, such as the purpose of AZT and side effects. The researchers developed a checklist to assess the quality of post-test counseling sessions for HIV-positive pregnant women. The only item on the checklist discussed in all 22 post-test counseling sessions observed was the meaning of an HIV-positive test result. Almost all of the sessions included the availability of ARV therapy and the need for a CD4 test to determine when AZT should be started. However, specific information offered on PMTCT varied greatly and was incomplete in most cases. Most women recalled that key topics had been discussed during post-test counseling sessions, but gaps remained. The majority of women remembered information on why AZT is needed, how to take AZT, and the importance of taking AZT on schedule. Only 14 percent of participants recalled receiving written materials developed specifically for HIV-positive women.
2
Evaluation of HIV Counseling and Testing in ANC Settings
More than eight out of ten HIV-positive women reported starting ARV prophylaxis during their pregnancy. Of 118 ANC clinic respondents, 81 percent reported that they started taking AZT for PMTCT. No ANC clinic respondents were on lifelong ARV therapy. Of 125 postnatal ward respondents, 16 were on lifelong ARV therapy. Among the remaining 109 respondents, 90 percent reported that they began AZT during their pregnancy for PMTCT. Reported adherence to AZT for PMTCT was generally good, but 30-40% of women missed at least some doses during their pregnancies. Adherence in this evaluation was measured by self-report. Among ANC clinic respondents who began AZT for PMTCT, 71 percent took AZT the morning of their interview, 92 percent had taken the appropriate number of tablets the two days prior to the interview, and 71 percent reported that they had never missed a dose of AZT. Among postnatal ward respondents, 89 percent reported that they took AZT the morning and evening of the last day before they went to the hospital and 59 percent reported that they never missed a dose of AZT during their whole pregnancy. The majority of women reported that adherence to their AZT regimen was easy. Eighty-three percent of all respondents found taking AZT to be either very easy or somewhat easy. Only 5 percent found it to be very difficult. Among women who reported missing doses of AZT, being away from home without medication, running out of pills, and forgetting to take a dose were the most common reasons given for missing doses. The majority of respondents refill their AZT when they have little or none left, and women were given inconsistent supplies of pills. Women reported being given anywhere from one to four weeks worth of AZT tablets at a time. While the majority of women found that picking up AZT was convenient, most respondents waited until they had little to no AZT left before refilling. Running out of pills was the second most often cited reason for missing doses of AZT. Infant AZT was provided consistently at the delivery sites, and the vast majority of women reported adhering to the infant AZT regimen. All 34 postpartum women interviewed reported that they were sent home from the postnatal ward with AZT for their infant. These women were interviewed about adherence to the four-week infant regimen of AZT. All 34 reported administering AZT to the infant at least once during the infants’ first four weeks of life. Two women stopped giving their infant AZT without finishing the four-week regimen. Among the remaining 32 women, 78 percent reported that they had never missed giving their infant a dose of AZT. Among the 28 women who were still giving the regimen, 86 percent reported following the regimen correctly in the four days prior to the interview.
3
Few women were informed about available community resources for support. Less than a third of all respondents were informed about their eligibility to receive a food basket or about where to go to meet other HIV-positive women to receive support. Recommendations The following recommendations emerged from the study: • Standardize post-test counseling content through the use of job aids. The WHO/CDC Testing and
Counseling for PMTCT support tools are designed to provide standardized information and can be customized by country programs. Adoption of these materials would expedite the introduction of standardized counseling. The tools are available at (http://www.who.int/hiv/pub/vct/tc/en/index.html).
• Adapt existing WHO written materials for distribution to HIV-positive mothers and pilot their usefulness in Botswana.
• Include as part of counseling an assessment of each client’s understanding of essential HIV information. Before leaving the counselor’s office, clients should understand at least the need to have their CD4 count checked, the meaning of the CD4 count, and information on PMTCT, including a specific AZT start date, and be aware that the counselor can provide ongoing support and information throughout the pregnancy.
• Encourage provision of at least two post-test counseling sessions for each woman. The same essential information should be covered in both sessions, increasing the likelihood of retention of the information.
• Encourage women to bring partners and other family members to visit the counselor with them, to increase family understanding of HIV and PMTCT and encourage HIV testing for other family members.
• Improve the AZT distribution process by standardizing the time interval for AZT refill pick-up, which would reduce the frequency of refills, and encourage women to refill their AZT before they run out of pills.
• Government health facilities should improve the distribution of information about community resources, such as support groups, health services, and nutritional services, and actively help women to access these services.
4

Evaluation of HIV Counseling and Testing in ANC Settings
Introduction Worldwide, two million children are estimated to be living with HIV and 2000 are thought to be newly infected each day (USAID 2005). These infant infections are primarily a result of mother-to-child transmission (MTCT) of the virus during pregnancy, labor, or breastfeeding. Clinical trials in Thailand in 1998 and in Uganda in 1999 demonstrated that the risk of vertical transmission of HIV can be reduced by nearly 50 percent through administering either a short-course of zidovudine (AZT) to the mother in the last weeks of pregnancy and during labor, or through administering a single dose of nevirapine to the mother at the onset of labor and to infants within 72 hours of birth (Shaffer et al. 1999; Guay et al. 1999). Based on these results, UNICEF supported the initiation of pilot PMTCT programs in 11 countries, including Botswana. PMTCT services include voluntary HIV counseling and testing, improved obstetric practices, provision of antiretroviral (ARV) prophylaxis, counseling and support for safer infant feeding practices, and family planning. The evaluation of the UN-supported programs found that it was feasible to integrate PMTCT services into the ANC/MCH setting in low resource countries (Rutenberg et al. 2003). In order for PMTCT programs to be effective at both an individual and public health level, HIV-positive women need to receive ARV prophylaxis and take the drug as it is prescribed. Measuring adherence is especially important in the face of serious consequences of low adherence to antiretroviral regimens such as failure to prevent viral replication and an increased likelihood of developing viral resistance (Turner 2002). While PMTCT programs routinely report the number and percentage of women who receive short course antiretroviral prophylaxis, there is little data on adherence to prophylactic regimens by women. In a clinical study setting in Lusaka, Zambia, Stringer et al. (2003) found that adherence to single dose nevirapine, the simplest short course regimen, was not ideal, with 26 percent of women failing to take the drug as prescribed. While single-dose nevirapine is the most widely used regimen for PMTCT programs, in major part due to its simplicity, the WHO guidelines regarding antiretroviral drugs for preventing HIV infection in infants recommend that a more efficacious combination regimen (e.g. AZT beginning at 28 weeks and single dose NVP at delivery) should be the standard of treatment (WHO 2006). Within the developing world, Botswana was one of the first countries to introduce a combination regimen in its national PMTCT program. It is thus timely to examine the successes and challenges in Botswana of administering a combination regimen during pregnancy as well as to document levels of adherence to this more complicated regimen. Data on administration and adherence to this combined prophylactic regimen will help guide the incorporation of a complex regimen into current country-specific PMTCT programs. Overview of PMTCT in Botswana Botswana has been hard hit by the AIDS epidemic. HIV surveillance data collected among pregnant women in 2003 showed that overall, 37.4 percent of pregnant women were HIV-positive, and in a third of the districts, more than 40 percent of pregnant women were infected with HIV (NACA 2003). The government of Botswana is strongly committed to fighting AIDS. In addition to being one of the first countries in the world to begin a pilot PMTCT project in 1999, the government quickly moved to scale up these services and became Africa’s first country to have a national PMTCT program, offering services to all pregnant women at no charge. Services have been available in every public antenatal clinic since 2002. At the time of this study, Botswana’s PMTCT program provided routine HIV testing and counseling,
5

twelve weeks of AZT for pregnant women (300 mg AZT in the morning and 300 mg AZT in the evening), four weeks of AZT for infants, single dose nevirapine for mothers and infants, and 12 months of infant formula. In addition to its advanced PMTCT services, Botswana also had the continent’s first nationally scaled-up antiretroviral therapy program, with ARV therapy available in at least 32 towns and villages throughout the country at the time of this evaluation. Pregnant women with CD4 counts under 200 or an AIDS-defining illness qualify to receive ARV therapy through the national ARV program. Evaluation Objectives This evaluation provided an opportunity for policymakers and program managers in Botswana to learn about the quality of post-test counseling and education, and to identify existing problems with ARV prophylaxis adherence and referral for therapy. It was also an opportunity for individuals who are implementing PMTCT activities elsewhere to learn lessons from a well-established program. The objectives of the evaluation were to: 1. Document the content of post-test counseling sessions for HIV-positive pregnant women and the
retention of this information by the women.
2. Describe the extent to which HIV-positive women who are pregnant or on the postnatal ward receive and adhere to ARV prophylaxis.
3. Describe operational successes and the specific barriers that women face in taking ARV prophylaxis,
including logistical, personal, and health-related factors which may prevent them from starting or continuing ARV prophylaxis or therapy.
6

Evaluation of HIV Counseling and Testing in ANC Settings
Methods Overview This evaluation was conducted from August to December 2005 in Francistown, Botswana’s second largest urban area. Data were collected at 9 primary health clinics, one hospital, and during home visits. The primary health clinic evaluation sites were: Area W, Boikhutso, Botswelelo, Gerald, Kagiso, Lapologang, Masego, Tatitown, and Tshwaragano. The hospital evaluation site was Nyangabgwe Referral Hospital (NRH). There was a range of study participants and points of data collection as outlined in Table 1. Table 1 Data sources Study participants Type of data
collection Number Location
HIV-positive pregnant women* (29–36 weeks gestation)
Client interviews 118** Antenatal care clinics
HIV-positive women on the postnatal ward Client interviews 125 Referral hospital
HIV-positive women with infants on four-week AZT prophylaxis
Client interviews 36 Home visits
Providers of PMTCT services Provider interviews 43 Clinics and hospital
HIV-positive pregnant women* during counseling sessions
Observations 22 Antenatal care clinics
*Both HIV-positive and HIV-negative women were interviewed and observed in order to reduce the possibility of identifying women as HIV-positive through their participation in the study. However, since the purpose of the evaluation was to explore adherence, the report only presents data for HIV-positive women. **While 122 interviews were conducted, data from four (3 percent) of these interviews were too incomplete for inclusion in the analysis; therefore data from 118 of these interviews are presented in the results section. Ethical Procedures The evaluation protocol was reviewed and approved by USAID, CDC, the Health Research and Development Committee (HRDC) in Botswana, and the Population Council’s Institutional Review Board. Ethical approval for the study was granted by the latter three institutions. Interviewers were trained on the importance of following ethical guidelines including maintaining confidentiality. Interviewers requested written informed consent from all women who were eligible for the study and only those who gave informed consent were interviewed or observed. There was no compensation for participating in the evaluation. Interviews and observations were conducted in a private space. Participants were not asked their names, except those who agreed to a home visit. For these subjects, names were recorded on a separate sheet, which was linked to the questionnaires by evaluation ID numbers and was kept separate from the questionnaires. Clinic ID numbers were asked of all women on the postnatal ward in order to
7

check their medical records for receipt of AZT and nevirapine at delivery. The study records forms with the clinic ID numbers were destroyed after hospital records were accessed. Completed questionnaires were stored in locked cabinets, and only the research team had access to the data. Eligibility, Recruitment, and Data Collection Procedures All pregnant women who were at 29–36 weeks of gestation or who had recently delivered and were at the postnatal ward, who were 18 years or older, and who already knew their HIV status (positive or negative) were eligible for the study. Only citizens of Botswana were eligible to participate in the evaluation, as foreign women are not eligible for PMTCT or ARV services. Clinic providers identified women who met the eligibility criteria and referred them to the interviewers. For client interviews from antenatal care clinics, interviewers rotated which clinics they were at on a weekly basis to reduce the possibility of interviewer bias. The interviews took place either while women were waiting to be seen by providers or after they received services. By approaching HIV-positive and HIV-negative women, the interviewers did not create the perception that the study was solely about HIV-positive women, thus avoiding possible stigmatization. The interviews of women at the postnatal ward took place as women were resting after having recently delivered. Only HIV-positive women were interviewed in the postnatal ward. Women who experienced complications during delivery that resulted in their being in obvious pain, heavily medicated, or having had a stillbirth were ineligible for the study. Women who had already been interviewed at the antenatal care clinic were also not eligible. Upon completion of the interview in the postnatal ward, interviewers asked women if they would agree to be visited at home approximately four weeks postpartum so that questions could be asked about infant AZT and infant care. All HIV-positive women who were interviewed in the postnatal ward (excluding those who had twins) and lived within a 40km radius of Francistown (a one hour drive) were asked whether they would be willing to participate in an interview at home. Among those who were eligible to take part in the evaluation, a small minority of women did not want to participate (see Table 2).
8
Evaluation of HIV Counseling and Testing in ANC Settings
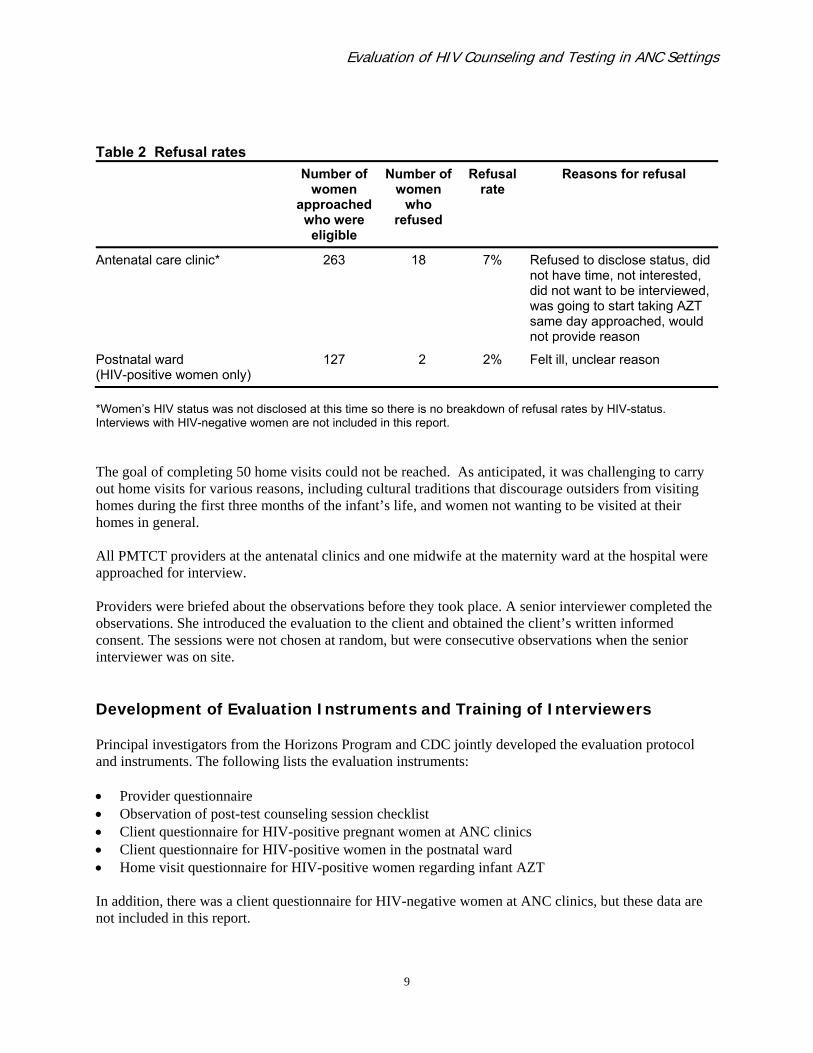
Table 2 Refusal rates Number of
women approached
who were eligible
Number of women
who refused
Refusal rate
Reasons for refusal
Antenatal care clinic* 263 18 7% Refused to disclose status, did not have time, not interested, did not want to be interviewed, was going to start taking AZT same day approached, would not provide reason
Postnatal ward (HIV-positive women only)
127 2 2% Felt ill, unclear reason
*Women’s HIV status was not disclosed at this time so there is no breakdown of refusal rates by HIV-status. Interviews with HIV-negative women are not included in this report. The goal of completing 50 home visits could not be reached. As anticipated, it was challenging to carry out home visits for various reasons, including cultural traditions that discourage outsiders from visiting homes during the first three months of the infant’s life, and women not wanting to be visited at their homes in general. All PMTCT providers at the antenatal clinics and one midwife at the maternity ward at the hospital were approached for interview. Providers were briefed about the observations before they took place. A senior interviewer completed the observations. She introduced the evaluation to the client and obtained the client’s written informed consent. The sessions were not chosen at random, but were consecutive observations when the senior interviewer was on site. Development of Evaluation Instruments and Training of Interviewers Principal investigators from the Horizons Program and CDC jointly developed the evaluation protocol and instruments. The following lists the evaluation instruments: • Provider questionnaire • Observation of post-test counseling session checklist • Client questionnaire for HIV-positive pregnant women at ANC clinics • Client questionnaire for HIV-positive women in the postnatal ward • Home visit questionnaire for HIV-positive women regarding infant AZT In addition, there was a client questionnaire for HIV-negative women at ANC clinics, but these data are not included in this report.
9

Premiere Personnel was the in-country organization that took primary responsibility for data collection and other related field activities. Premiere Personnel translated the questionnaires into Setswana, back translated them into English, and pre-tested them. Premiere Personnel recruited six interviewers who completed training specifically in these instruments prior to beginning data collection. Training was jointly conducted by Premiere Personnel and the Horizons Program. Interviewers for this evaluation were female university graduates. Many of them had previous experience conducting interviews. Data Analysis This was an evaluation that had small sample sizes and employed convenience sampling. As such most of the data presented in this paper is descriptive, and document trends or qualitative findings, and are not necessarily statistically significant. Moreover, only pooled data are analyzed and thus none of the analyses account for possible differences by site. Limitations of the Study This evaluation employed convenience sampling at PMTCT and delivery sites in one city in Botswana, and therefore the extent to which results can be generalized to the larger population of all pregnant or recently delivered women in the country is unknown. However, the findings from the evaluation can be used to provide insights into the quality of counseling received by HIV-positive pregnant women and their initiation of and adherence to PMTCT medical regimens. Adherence was measured by self-report in this evaluation. While self-report tends to overestimate adherence as compared with other adherence measures, it has been shown to correlate well with viral load levels (Turner 2002). As this was a cross-sectional study, measures of adherence such as pill counts and MEMS (Medication Event Monitoring System) were not feasible. Additionally, sample sizes of observations and respondents for some questions were small. It should be noted that for ease of reading, the results are often reported in percentages, but caution should be used in interpreting the data based on these percentages because of the small sample sizes.
10
Evaluation of HIV Counseling and Testing in ANC Settings
Results Profile of Respondents Sociodemographic data of clients The sociodemographic profiles of HIV-positive pregnant women and HIV-positive postnatal ward women are reported in Table 3. The mean age of respondents was 26.5 years in the antenatal clinics and 28.2 years in the postnatal ward. Almost all of the respondents reported having a partner, but few of the respondents were married. Approximately half of the women in both locations were employed and the mean number of meals eaten per day was three. There were some notable differences between the sociodemographic characteristics of the respondents in the antenatal clinics compared to those in the postnatal ward. The following are examples of trends. Postnatal ward women were more likely to be single, to use a shared water source, and to use more wood and less gas as their fuel for cooking. These differences are likely due to the following reasons. NRH is a referral hospital, meaning that patients in the postnatal ward are often referred from smaller towns and rural areas for services that may not be available in these areas. Some of the women interviewed in the postnatal ward came from communal farming areas, cattle posts, and other rural locations. On the other hand, most women attend ANC clinics in their own area. Therefore, the women interviewed in the ANC clinics in Francistown were most likely from Francistown and likely to be better off economically than women from surrounding rural areas. The second possible reason may be related to the timeframe of data collection. Interviews of postnatal ward women at the hospital took place after data collection in the ANC clinics was completed. Consequently, some women who had received care from the Francistown ANC clinics could not be interviewed as they had already participated in the study while pregnant.
11
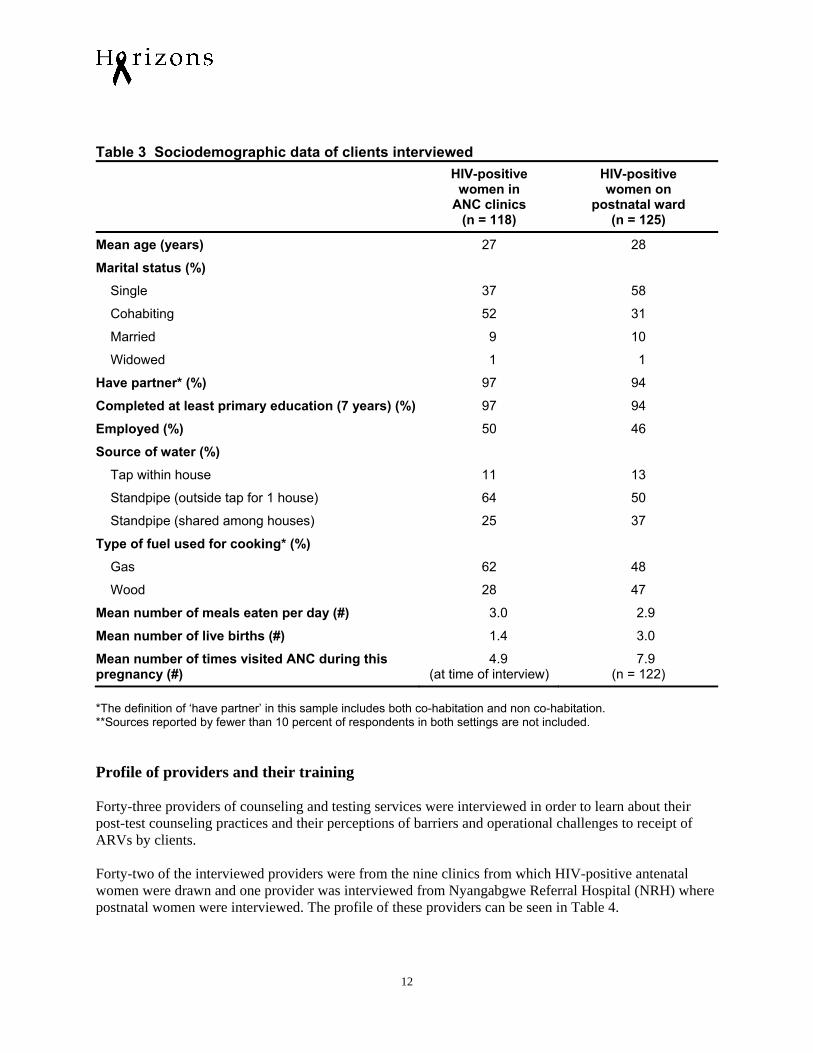
Table 3 Sociodemographic data of clients interviewed HIV-positive
women in ANC clinics
(n = 118)
HIV-positive women on
postnatal ward (n = 125)
Mean age (years) 27 28
Marital status (%)
Single 37 58
Cohabiting 52 31
Married 9 10
Widowed 1 1
Have partner* (%) 97 94
Completed at least primary education (7 years) (%) 97 94
Employed (%) 50 46
Source of water (%)
Tap within house 11 13
Standpipe (outside tap for 1 house) 64 50
Standpipe (shared among houses) 25 37
Type of fuel used for cooking* (%)
Gas 62 48
Wood 28 47
Mean number of meals eaten per day (#) 3.0 2.9
Mean number of live births (#) 1.4 3.0
Mean number of times visited ANC during this pregnancy (#)
4.9 (at time of interview)
7.9 (n = 122)
*The definition of ‘have partner’ in this sample includes both co-habitation and non co-habitation. **Sources reported by fewer than 10 percent of respondents in both settings are not included. Profile of providers and their training Forty-three providers of counseling and testing services were interviewed in order to learn about their post-test counseling practices and their perceptions of barriers and operational challenges to receipt of ARVs by clients. Forty-two of the interviewed providers were from the nine clinics from which HIV-positive antenatal women were drawn and one provider was interviewed from Nyangabgwe Referral Hospital (NRH) where postnatal women were interviewed. The profile of these providers can be seen in Table 4.
12
Evaluation of HIV Counseling and Testing in ANC Settings
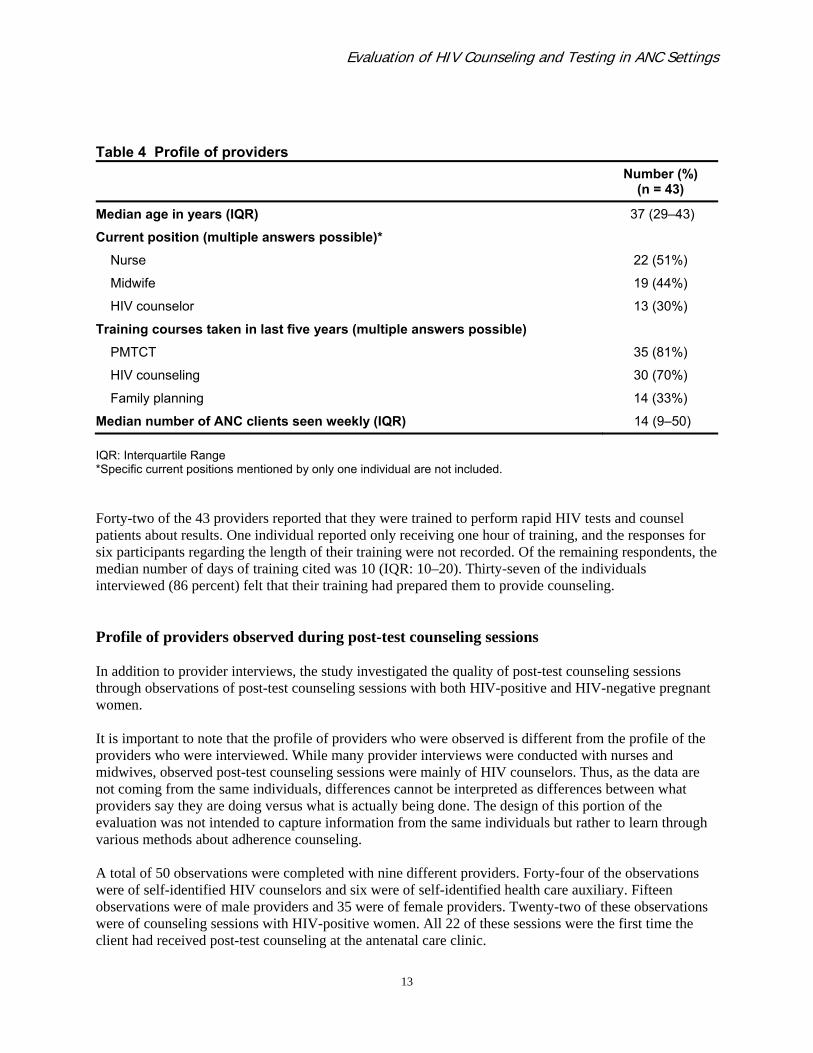
Table 4 Profile of providers Number (%)
(n = 43)
Median age in years (IQR) 37 (29–43)
Current position (multiple answers possible)*
Nurse 22 (51%)
Midwife 19 (44%)
HIV counselor 13 (30%)
Training courses taken in last five years (multiple answers possible)
PMTCT 35 (81%)
HIV counseling 30 (70%)
Family planning 14 (33%)
Median number of ANC clients seen weekly (IQR) 14 (9–50) IQR: Interquartile Range *Specific current positions mentioned by only one individual are not included. Forty-two of the 43 providers reported that they were trained to perform rapid HIV tests and counsel patients about results. One individual reported only receiving one hour of training, and the responses for six participants regarding the length of their training were not recorded. Of the remaining respondents, the median number of days of training cited was 10 (IQR: 10–20). Thirty-seven of the individuals interviewed (86 percent) felt that their training had prepared them to provide counseling. Profile of providers observed during post-test counseling sessions In addition to provider interviews, the study investigated the quality of post-test counseling sessions through observations of post-test counseling sessions with both HIV-positive and HIV-negative pregnant women. It is important to note that the profile of providers who were observed is different from the profile of the providers who were interviewed. While many provider interviews were conducted with nurses and midwives, observed post-test counseling sessions were mainly of HIV counselors. Thus, as the data are not coming from the same individuals, differences cannot be interpreted as differences between what providers say they are doing versus what is actually being done. The design of this portion of the evaluation was not intended to capture information from the same individuals but rather to learn through various methods about adherence counseling. A total of 50 observations were completed with nine different providers. Forty-four of the observations were of self-identified HIV counselors and six were of self-identified health care auxiliary. Fifteen observations were of male providers and 35 were of female providers. Twenty-two of these observations were of counseling sessions with HIV-positive women. All 22 of these sessions were the first time the client had received post-test counseling at the antenatal care clinic.
13
HIV Counseling and Testing and Post-test Information about ARV Prophylaxis and Therapy HIV counseling and testing at the ANC clinic is the starting point for identifying the HIV status of pregnant women, and includes information about ARV prophylaxis and therapy. This section explores the information received and the quality of counseling and testing by HIV-positive pregnant women during post-test counseling as the backdrop to examining adherence. The data presented are from interviews with providers, observations of post-test counseling sessions, and self-reports from HIV-positive women who received at least one post-test counseling session. Provider interviews Information providers believe is important to convey during post-test counseling for HIV-positive women The median time that providers reported spending on a post-test counseling session with an HIV-positive woman was 28 minutes (IQR 20-40), with 20 minutes as the most common response. Half of the providers stated that they have the opportunity to provide post-test counseling with an individual during only one session. Table 5 shows the results when providers were asked what issues they thought a counselor should address during post-test counseling for HIV-positive pregnant women. Despite the limited time spent on individual post-test counseling sessions, providers reported a long and broad list of issues that should be discussed during these sessions. Major themes mentioned included explaining the meaning of the test result, encouraging women to accept their status and live positively, suggestions of how the individual could take care of herself both physically and emotionally, how to prevent vertical transmission, and how to prevent re-infection. While the sample size for each group is small, this evaluation indicates differences in the information that different provider types find important when counseling an HIV-positive pregnant woman.
14

Evaluation of HIV Counseling and Testing in ANC Settings
Table 5 Issues providers thought a counselor should address during post-test counseling sessions with HIV-positive pregnant women*┼
Provider type‡
Nurse/midwife (n = 27)
Number (%)
HIV counselor (n = 13)
Number (%)
Using condoms 21 (77%) 12 (92%)
Evaluation for ARV therapy 13 (48%) 10 (77%)
Avoid reinfection/sexual behavior change 12 (44%) 3 (23%)
Eating well 11 (41%) 2 (15%)
Positive living 10 (37%) 5 (38%)
Accept status 9 (33%) 4 (31%)
Getting partner tested 9 (33%) 3 (23%)
PMTCT 8 (30%) 9 (69%)
Seeking support 6 (22%) 7 (54%)
Meaning of result 6 (22%) 5 (38%)
Disclosure 6 (22%) 4 (31%)
IPT (TB) 4 (15%) 3 (23%)
Condom negotiation 4 (15%) 1 (8%)
Infant formula feeding 3 (11%) 4 (31%) *Multiple responses possible ┼Responses mentioned by less than 10 percent of providers were not included. ‡One provider was a “health care auxiliary” and one was a social worker. These two are not included here. Provider discussion of AZT adherence When providers were specifically asked whether they discuss adherence to AZT with their HIV-positive pregnant clients, 40 out of 42 (95 percent) said that they did. One of the two providers that responded that they did not provide adherence counseling said that you should only discuss AZT adherence when the woman had a very low CD4 count while the other did not counsel on adherence as they did not feel that they were trained adequately to do so. Over half of those providing adherence counseling discussed the importance of taking the correct dose of medication and of taking the medication on schedule. However, as can be seen in Table 6, not only did the responses and combination of responses vary greatly, but they also varied by provider type.
15

Table 6 Issues related to AZT adherence that providers thought should be addressed in counseling sessions with HIV-positive women* Provider type‡
Nurse/Midwife (n = 27) Number
HIV counselor (n = 13) Number
Dosing/schedule 17 4
Timeframe of prophylaxis 2 7
Not missing or skipping doses/not stopping once started
11 1
Importance/purpose of AZT 9 2
Side effects 4 1
Infant regimen 3 1 *Multiple responses possible; responses that were mentioned by less than 10 percent of providers were not included. ‡One provider was a “health care auxiliary” and one was a social worker. These two are not included here. Observed counseling sessions with post-test HIV-positive pregnant women Although the sample size was small, these 22 observations of post-test counseling sessions of HIV-positive pregnant women provide insights regarding the interaction between the counselor and the client, and what kind of information is being provided and discussed. The median length of time for the observed sessions was 15 minutes (IQR 10–20). General information In all of the post-test counseling sessions, providers explained the meaning of a positive HIV test result. However, only half of the sessions included an assessment of whether the client understood the meaning of what was explained. In the vast majority of sessions, providers discussed issues pertaining to a partner’s HIV status, and most discussed positive living and disclosure of results (see Table 7).
16
Evaluation of HIV Counseling and Testing in ANC Settings
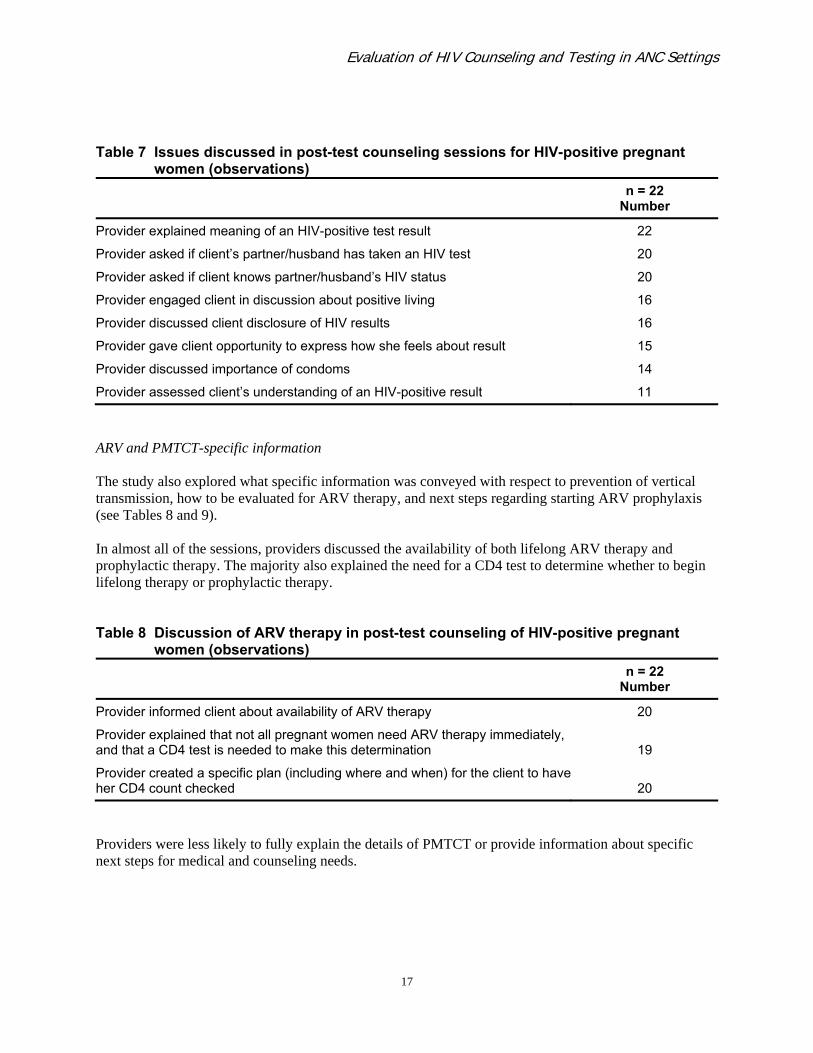
Table 7 Issues discussed in post-test counseling sessions for HIV-positive pregnant women (observations) n = 22
Number
Provider explained meaning of an HIV-positive test result 22
Provider asked if client’s partner/husband has taken an HIV test 20
Provider asked if client knows partner/husband’s HIV status 20
Provider engaged client in discussion about positive living 16
Provider discussed client disclosure of HIV results 16
Provider gave client opportunity to express how she feels about result 15
Provider discussed importance of condoms 14
Provider assessed client’s understanding of an HIV-positive result 11
ARV and PMTCT-specific information The study also explored what specific information was conveyed with respect to prevention of vertical transmission, how to be evaluated for ARV therapy, and next steps regarding starting ARV prophylaxis (see Tables 8 and 9). In almost all of the sessions, providers discussed the availability of both lifelong ARV therapy and prophylactic therapy. The majority also explained the need for a CD4 test to determine whether to begin lifelong therapy or prophylactic therapy. Table 8 Discussion of ARV therapy in post-test counseling of HIV-positive pregnant women (observations) n = 22
Number
Provider informed client about availability of ARV therapy 20
Provider explained that not all pregnant women need ARV therapy immediately, and that a CD4 test is needed to make this determination
19
Provider created a specific plan (including where and when) for the client to have her CD4 count checked
20
Providers were less likely to fully explain the details of PMTCT or provide information about specific next steps for medical and counseling needs.
17
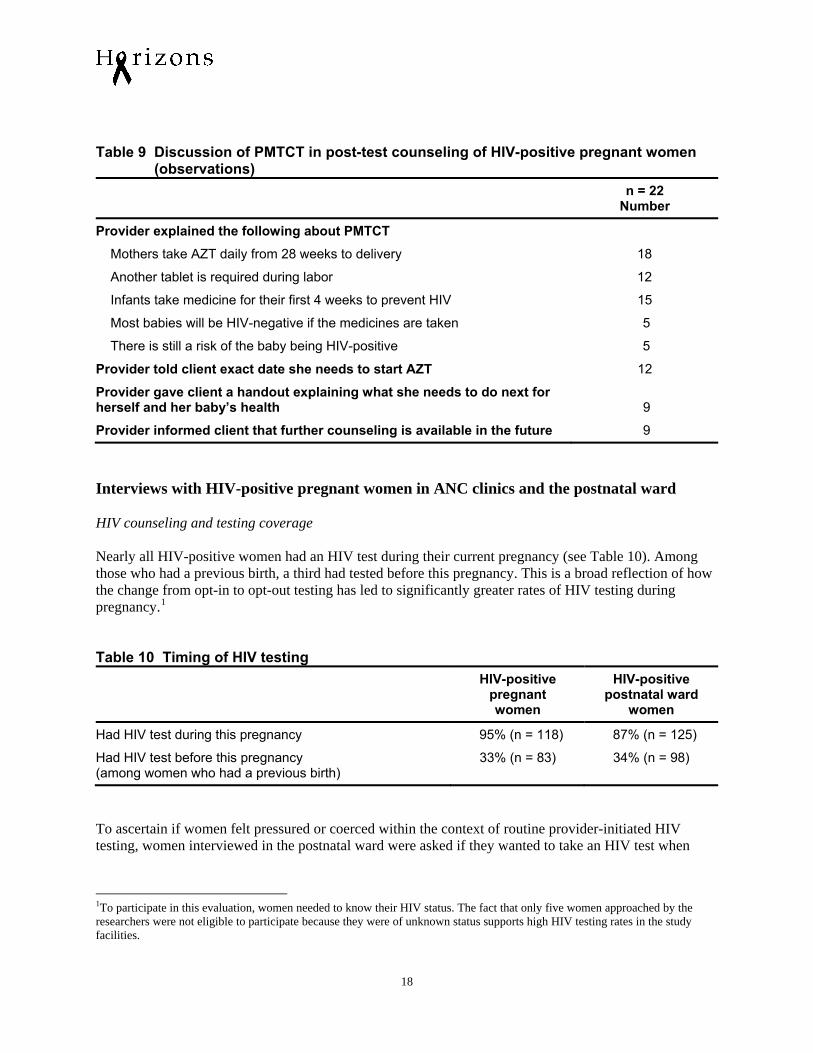
Table 9 Discussion of PMTCT in post-test counseling of HIV-positive pregnant women (observations) n = 22
Number
Provider explained the following about PMTCT
Mothers take AZT daily from 28 weeks to delivery 18
Another tablet is required during labor 12
Infants take medicine for their first 4 weeks to prevent HIV 15
Most babies will be HIV-negative if the medicines are taken 5
There is still a risk of the baby being HIV-positive 5
Provider told client exact date she needs to start AZT 12
Provider gave client a handout explaining what she needs to do next for herself and her baby’s health
9
Provider informed client that further counseling is available in the future 9
Interviews with HIV-positive pregnant women in ANC clinics and the postnatal ward HIV counseling and testing coverage Nearly all HIV-positive women had an HIV test during their current pregnancy (see Table 10). Among those who had a previous birth, a third had tested before this pregnancy. This is a broad reflection of how the change from opt-in to opt-out testing has led to significantly greater rates of HIV testing during pregnancy.1 Table 10 Timing of HIV testing HIV-positive
pregnant women
HIV-positive postnatal ward
women
Had HIV test during this pregnancy 95% (n = 118) 87% (n = 125)
Had HIV test before this pregnancy (among women who had a previous birth)
33% (n = 83) 34% (n = 98)
To ascertain if women felt pressured or coerced within the context of routine provider-initiated HIV testing, women interviewed in the postnatal ward were asked if they wanted to take an HIV test when
1To participate in this evaluation, women needed to know their HIV status. The fact that only five women approached by the researchers were not eligible to participate because they were of unknown status supports high HIV testing rates in the study facilities.
18
Evaluation of HIV Counseling and Testing in ANC Settings
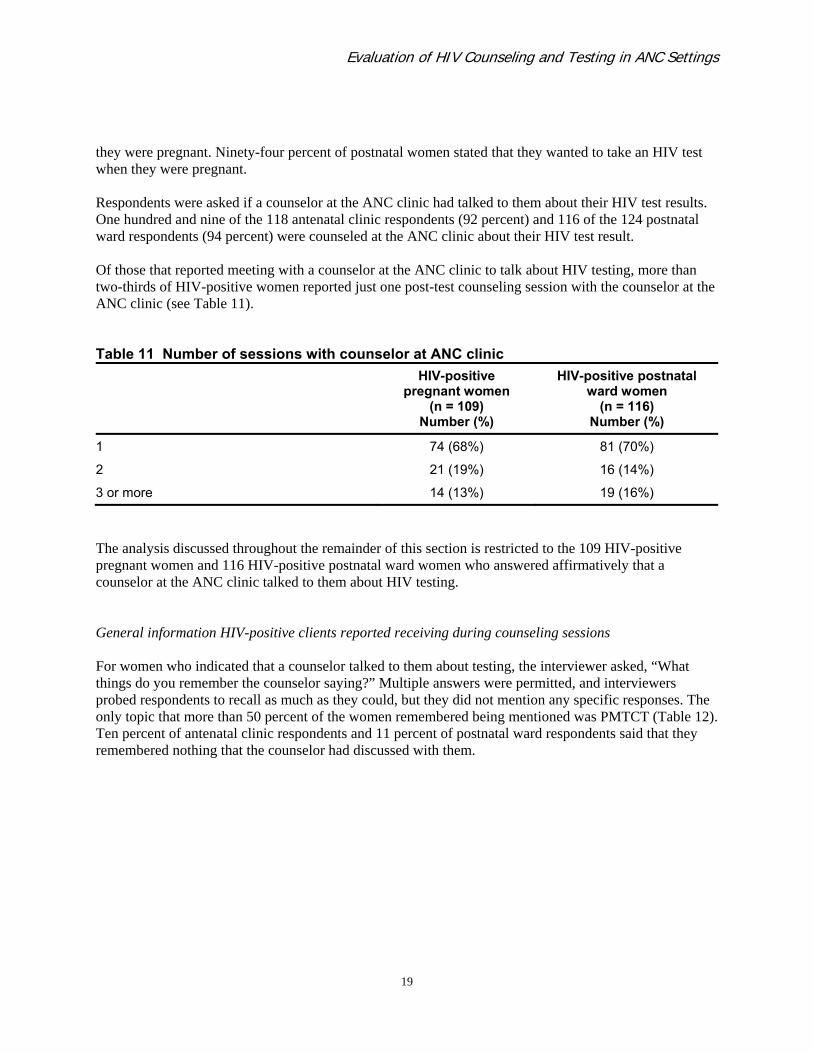
they were pregnant. Ninety-four percent of postnatal women stated that they wanted to take an HIV test when they were pregnant. Respondents were asked if a counselor at the ANC clinic had talked to them about their HIV test results. One hundred and nine of the 118 antenatal clinic respondents (92 percent) and 116 of the 124 postnatal ward respondents (94 percent) were counseled at the ANC clinic about their HIV test result. Of those that reported meeting with a counselor at the ANC clinic to talk about HIV testing, more than two-thirds of HIV-positive women reported just one post-test counseling session with the counselor at the ANC clinic (see Table 11). Table 11 Number of sessions with counselor at ANC clinic HIV-positive
pregnant women (n = 109)
Number (%)
HIV-positive postnatal ward women
(n = 116) Number (%)
1 74 (68%) 81 (70%)
2 21 (19%) 16 (14%)
3 or more 14 (13%) 19 (16%)
The analysis discussed throughout the remainder of this section is restricted to the 109 HIV-positive pregnant women and 116 HIV-positive postnatal ward women who answered affirmatively that a counselor at the ANC clinic talked to them about HIV testing. General information HIV-positive clients reported receiving during counseling sessions For women who indicated that a counselor talked to them about testing, the interviewer asked, “What things do you remember the counselor saying?” Multiple answers were permitted, and interviewers probed respondents to recall as much as they could, but they did not mention any specific responses. The only topic that more than 50 percent of the women remembered being mentioned was PMTCT (Table 12). Ten percent of antenatal clinic respondents and 11 percent of postnatal ward respondents said that they remembered nothing that the counselor had discussed with them.
19
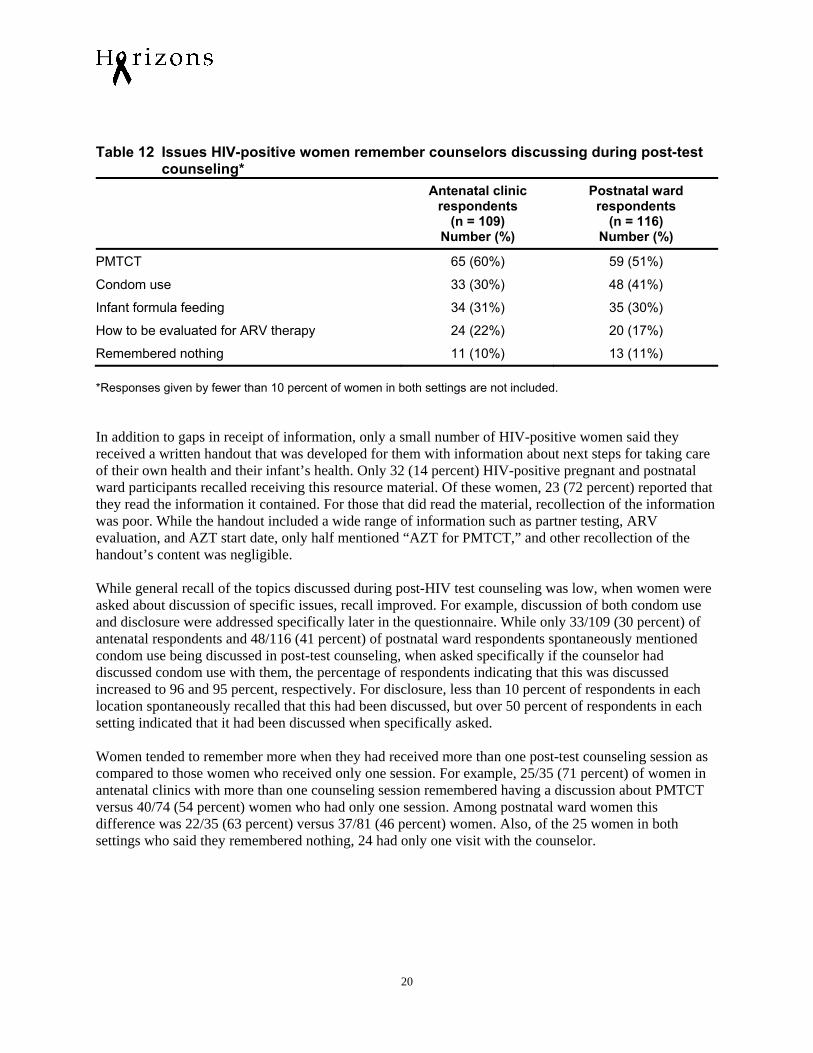
Table 12 Issues HIV-positive women remember counselors discussing during post-test counseling* Antenatal clinic
respondents (n = 109)
Number (%)
Postnatal ward respondents
(n = 116) Number (%)
PMTCT 65 (60%) 59 (51%)
Condom use 33 (30%) 48 (41%)
Infant formula feeding 34 (31%) 35 (30%)
How to be evaluated for ARV therapy 24 (22%) 20 (17%)
Remembered nothing 11 (10%) 13 (11%) *Responses given by fewer than 10 percent of women in both settings are not included. In addition to gaps in receipt of information, only a small number of HIV-positive women said they received a written handout that was developed for them with information about next steps for taking care of their own health and their infant’s health. Only 32 (14 percent) HIV-positive pregnant and postnatal ward participants recalled receiving this resource material. Of these women, 23 (72 percent) reported that they read the information it contained. For those that did read the material, recollection of the information was poor. While the handout included a wide range of information such as partner testing, ARV evaluation, and AZT start date, only half mentioned “AZT for PMTCT,” and other recollection of the handout’s content was negligible. While general recall of the topics discussed during post-HIV test counseling was low, when women were asked about discussion of specific issues, recall improved. For example, discussion of both condom use and disclosure were addressed specifically later in the questionnaire. While only 33/109 (30 percent) of antenatal respondents and 48/116 (41 percent) of postnatal ward respondents spontaneously mentioned condom use being discussed in post-test counseling, when asked specifically if the counselor had discussed condom use with them, the percentage of respondents indicating that this was discussed increased to 96 and 95 percent, respectively. For disclosure, less than 10 percent of respondents in each location spontaneously recalled that this had been discussed, but over 50 percent of respondents in each setting indicated that it had been discussed when specifically asked. Women tended to remember more when they had received more than one post-test counseling session as compared to those women who received only one session. For example, 25/35 (71 percent) of women in antenatal clinics with more than one counseling session remembered having a discussion about PMTCT versus 40/74 (54 percent) women who had only one session. Among postnatal ward women this difference was 22/35 (63 percent) versus 37/81 (46 percent) women. Also, of the 25 women in both settings who said they remembered nothing, 24 had only one visit with the counselor.
20
Evaluation of HIV Counseling and Testing in ANC Settings
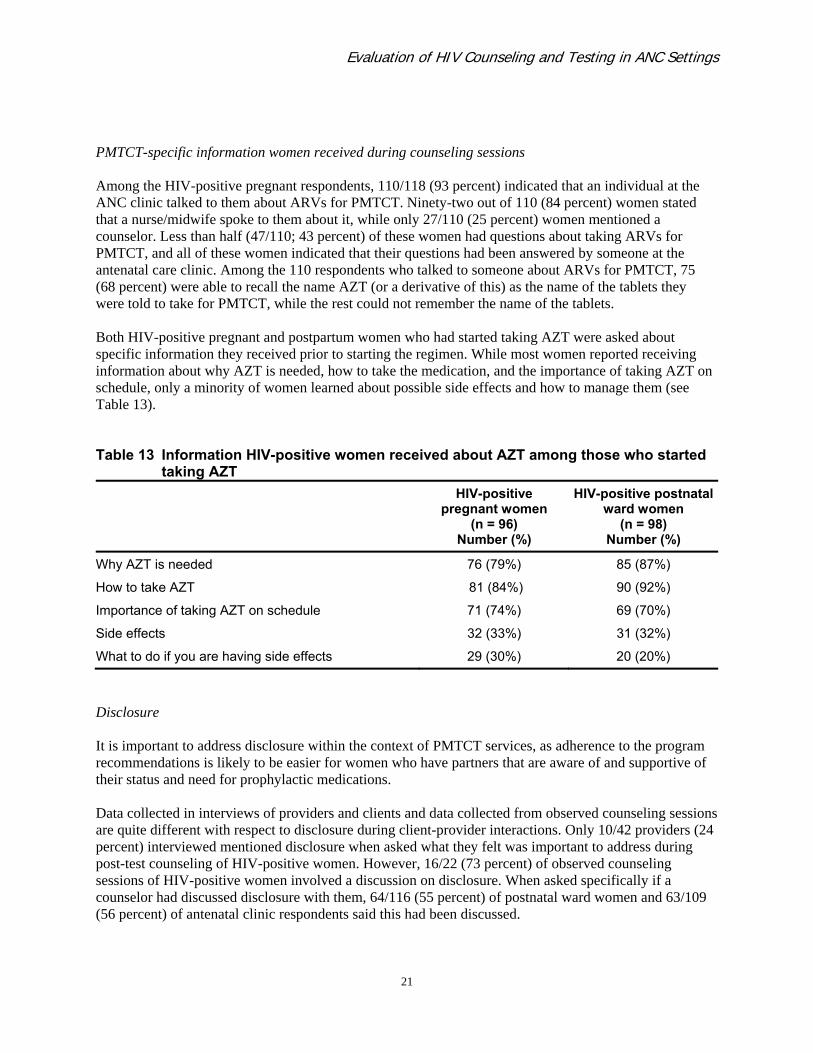
PMTCT-specific information women received during counseling sessions Among the HIV-positive pregnant respondents, 110/118 (93 percent) indicated that an individual at the ANC clinic talked to them about ARVs for PMTCT. Ninety-two out of 110 (84 percent) women stated that a nurse/midwife spoke to them about it, while only 27/110 (25 percent) women mentioned a counselor. Less than half (47/110; 43 percent) of these women had questions about taking ARVs for PMTCT, and all of these women indicated that their questions had been answered by someone at the antenatal care clinic. Among the 110 respondents who talked to someone about ARVs for PMTCT, 75 (68 percent) were able to recall the name AZT (or a derivative of this) as the name of the tablets they were told to take for PMTCT, while the rest could not remember the name of the tablets. Both HIV-positive pregnant and postpartum women who had started taking AZT were asked about specific information they received prior to starting the regimen. While most women reported receiving information about why AZT is needed, how to take the medication, and the importance of taking AZT on schedule, only a minority of women learned about possible side effects and how to manage them (see Table 13).
Table 13 Information HIV-positive women received about AZT among those who started taking AZT HIV-positive
pregnant women (n = 96)
Number (%)
HIV-positive postnatal ward women
(n = 98) Number (%)
Why AZT is needed 76 (79%) 85 (87%)
How to take AZT 81 (84%) 90 (92%)
Importance of taking AZT on schedule 71 (74%) 69 (70%)
Side effects 32 (33%) 31 (32%)
What to do if you are having side effects 29 (30%) 20 (20%)
Disclosure It is important to address disclosure within the context of PMTCT services, as adherence to the program recommendations is likely to be easier for women who have partners that are aware of and supportive of their status and need for prophylactic medications. Data collected in interviews of providers and clients and data collected from observed counseling sessions are quite different with respect to disclosure during client-provider interactions. Only 10/42 providers (24 percent) interviewed mentioned disclosure when asked what they felt was important to address during post-test counseling of HIV-positive women. However, 16/22 (73 percent) of observed counseling sessions of HIV-positive women involved a discussion on disclosure. When asked specifically if a counselor had discussed disclosure with them, 64/116 (55 percent) of postnatal ward women and 63/109 (56 percent) of antenatal clinic respondents said this had been discussed.
21
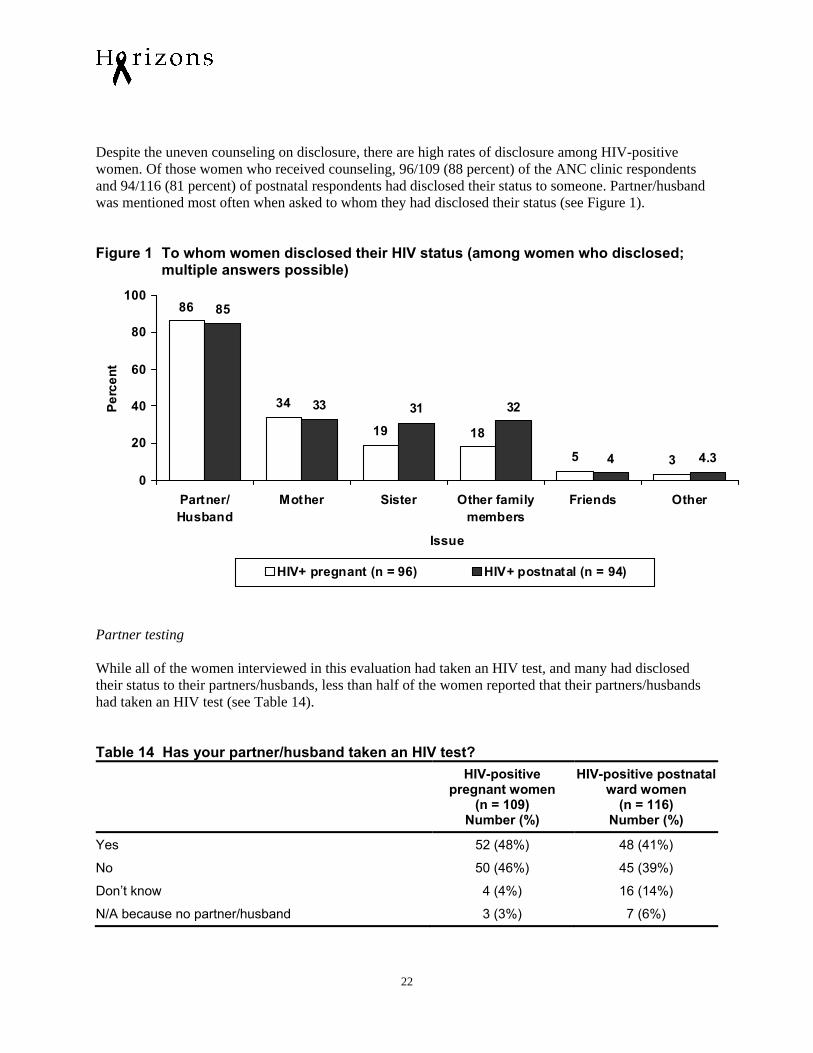
Despite the uneven counseling on disclosure, there are high rates of disclosure among HIV-positive women. Of those women who received counseling, 96/109 (88 percent) of the ANC clinic respondents and 94/116 (81 percent) of postnatal respondents had disclosed their status to someone. Partner/husband was mentioned most often when asked to whom they had disclosed their status (see Figure 1). Figure 1 To whom women disclosed their HIV status (among women who disclosed; multiple answers possible)
86
34
19 18
5 3
85
33 31 32
4 4.3
0
20
40
60
80
100
Partner/Husband
Mother Sister Other familymembers
Friends Other
Issue
Perc
ent
HIV+ pregnant (n = 96) HIV+ postnatal (n = 94)
Partner testing While all of the women interviewed in this evaluation had taken an HIV test, and many had disclosed their status to their partners/husbands, less than half of the women reported that their partners/husbands had taken an HIV test (see Table 14). Table 14 Has your partner/husband taken an HIV test? HIV-positive
pregnant women (n = 109)
Number (%)
HIV-positive postnatal ward women
(n = 116) Number (%)
Yes 52 (48%) 48 (41%)
No 50 (46%) 45 (39%)
Don’t know 4 (4%) 16 (14%)
N/A because no partner/husband 3 (3%) 7 (6%)
22
Evaluation of HIV Counseling and Testing in ANC Settings
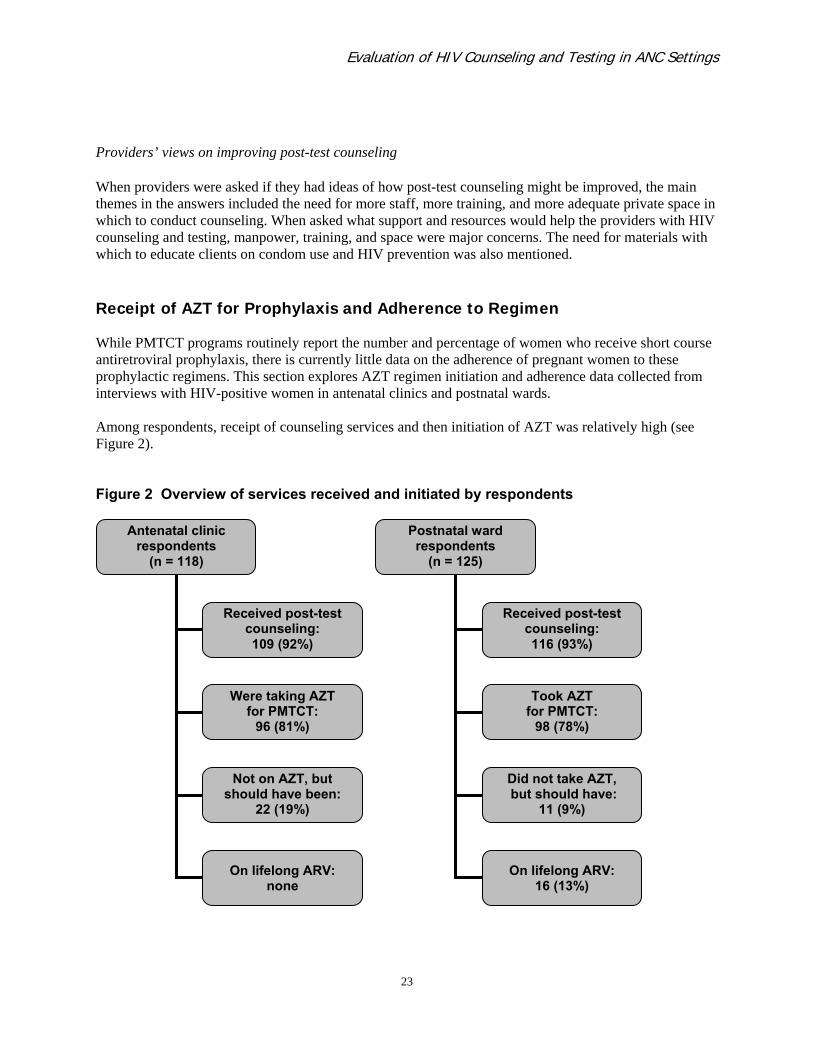
Providers’ views on improving post-test counseling When providers were asked if they had ideas of how post-test counseling might be improved, the main themes in the answers included the need for more staff, more training, and more adequate private space in which to conduct counseling. When asked what support and resources would help the providers with HIV counseling and testing, manpower, training, and space were major concerns. The need for materials with which to educate clients on condom use and HIV prevention was also mentioned. Receipt of AZT for Prophylaxis and Adherence to Regimen While PMTCT programs routinely report the number and percentage of women who receive short course antiretroviral prophylaxis, there is currently little data on the adherence of pregnant women to these prophylactic regimens. This section explores AZT regimen initiation and adherence data collected from interviews with HIV-positive women in antenatal clinics and postnatal wards. Among respondents, receipt of counseling services and then initiation of AZT was relatively high (see Figure 2). Figure 2 Overview of services received and initiated by respondents
Antenatal clinic
respondents (n = 118)
Received post-test counseling: 109 (92%)
Were taking AZT for PMTCT:
96 (81%)
Not on AZT, but should have been:
22 (19%)
On lifelong ARV: none
Postnatal ward respondents
(n = 125)
Received post-test counseling: 116 (93%)
Took AZT for PMTCT:
98 (78%)
Did not take AZT, but should have:
11 (9%)
On lifelong ARV: 16 (13%)
23
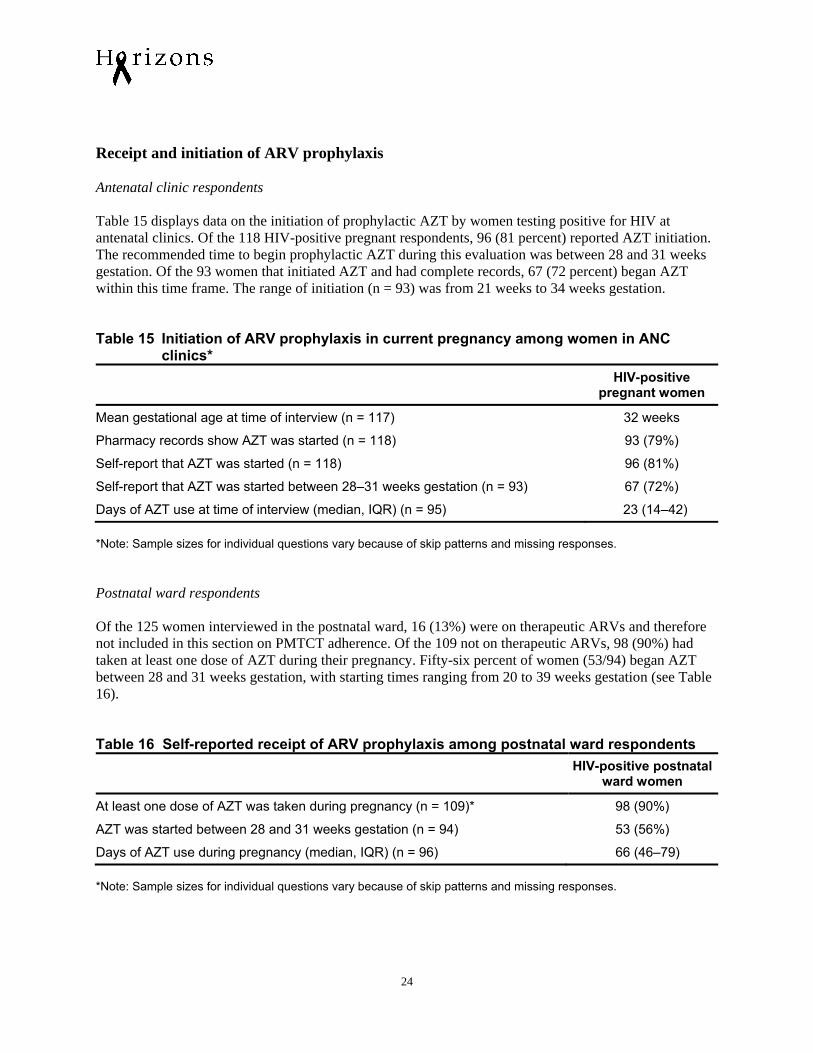
Receipt and initiation of ARV prophylaxis Antenatal clinic respondents Table 15 displays data on the initiation of prophylactic AZT by women testing positive for HIV at antenatal clinics. Of the 118 HIV-positive pregnant respondents, 96 (81 percent) reported AZT initiation. The recommended time to begin prophylactic AZT during this evaluation was between 28 and 31 weeks gestation. Of the 93 women that initiated AZT and had complete records, 67 (72 percent) began AZT within this time frame. The range of initiation (n = 93) was from 21 weeks to 34 weeks gestation. Table 15 Initiation of ARV prophylaxis in current pregnancy among women in ANC clinics* HIV-positive
pregnant women
Mean gestational age at time of interview (n = 117) 32 weeks
Pharmacy records show AZT was started (n = 118) 93 (79%)
Self-report that AZT was started (n = 118) 96 (81%)
Self-report that AZT was started between 28–31 weeks gestation (n = 93) 67 (72%)
Days of AZT use at time of interview (median, IQR) (n = 95) 23 (14–42) *Note: Sample sizes for individual questions vary because of skip patterns and missing responses. Postnatal ward respondents Of the 125 women interviewed in the postnatal ward, 16 (13%) were on therapeutic ARVs and therefore not included in this section on PMTCT adherence. Of the 109 not on therapeutic ARVs, 98 (90%) had taken at least one dose of AZT during their pregnancy. Fifty-six percent of women (53/94) began AZT between 28 and 31 weeks gestation, with starting times ranging from 20 to 39 weeks gestation (see Table 16). Table 16 Self-reported receipt of ARV prophylaxis among postnatal ward respondents HIV-positive postnatal
ward women
At least one dose of AZT was taken during pregnancy (n = 109)* 98 (90%)
AZT was started between 28 and 31 weeks gestation (n = 94) 53 (56%)
Days of AZT use during pregnancy (median, IQR) (n = 96) 66 (46–79) *Note: Sample sizes for individual questions vary because of skip patterns and missing responses.
24
Evaluation of HIV Counseling and Testing in ANC Settings
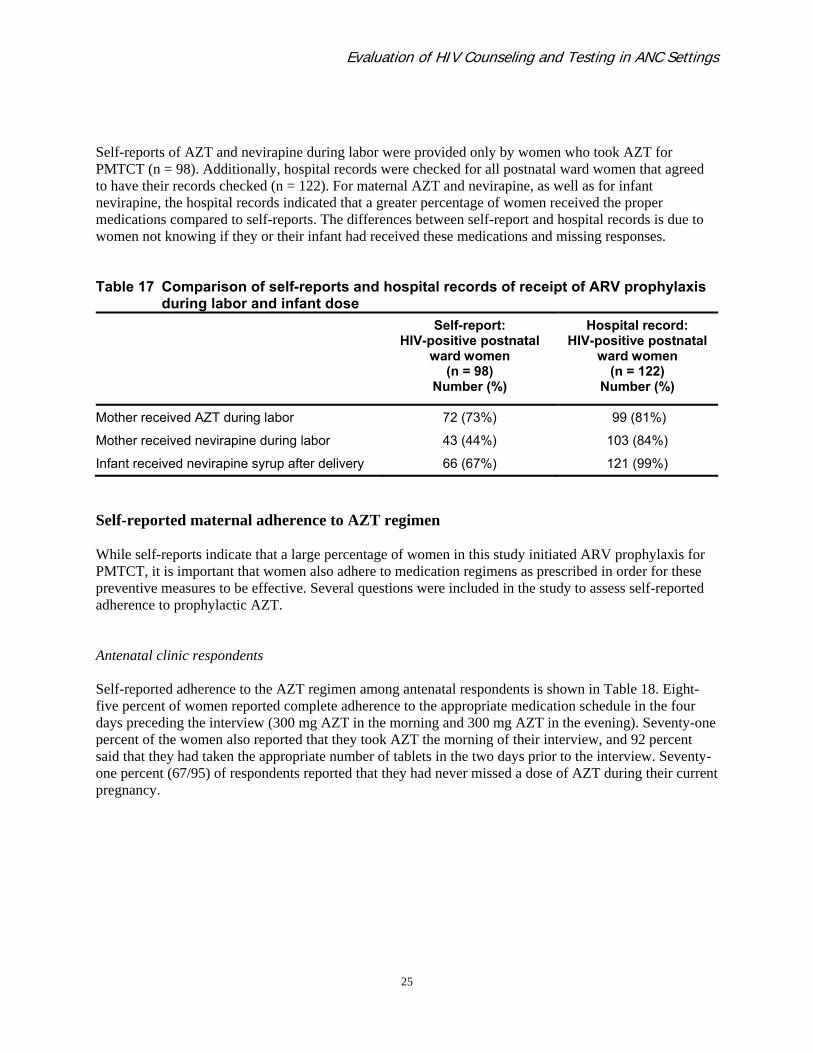
Self-reports of AZT and nevirapine during labor were provided only by women who took AZT for PMTCT (n = 98). Additionally, hospital records were checked for all postnatal ward women that agreed to have their records checked (n = 122). For maternal AZT and nevirapine, as well as for infant nevirapine, the hospital records indicated that a greater percentage of women received the proper medications compared to self-reports. The differences between self-report and hospital records is due to women not knowing if they or their infant had received these medications and missing responses. Table 17 Comparison of self-reports and hospital records of receipt of ARV prophylaxis
during labor and infant dose Self-report:
HIV-positive postnatal ward women
(n = 98) Number (%)
Hospital record: HIV-positive postnatal
ward women (n = 122)
Number (%)
Mother received AZT during labor 72 (73%) 99 (81%)
Mother received nevirapine during labor 43 (44%) 103 (84%)
Infant received nevirapine syrup after delivery 66 (67%) 121 (99%)
Self-reported maternal adherence to AZT regimen While self-reports indicate that a large percentage of women in this study initiated ARV prophylaxis for PMTCT, it is important that women also adhere to medication regimens as prescribed in order for these preventive measures to be effective. Several questions were included in the study to assess self-reported adherence to prophylactic AZT. Antenatal clinic respondents Self-reported adherence to the AZT regimen among antenatal respondents is shown in Table 18. Eight-five percent of women reported complete adherence to the appropriate medication schedule in the four days preceding the interview (300 mg AZT in the morning and 300 mg AZT in the evening). Seventy-one percent of the women also reported that they took AZT the morning of their interview, and 92 percent said that they had taken the appropriate number of tablets in the two days prior to the interview. Seventy-one percent (67/95) of respondents reported that they had never missed a dose of AZT during their current pregnancy.
25
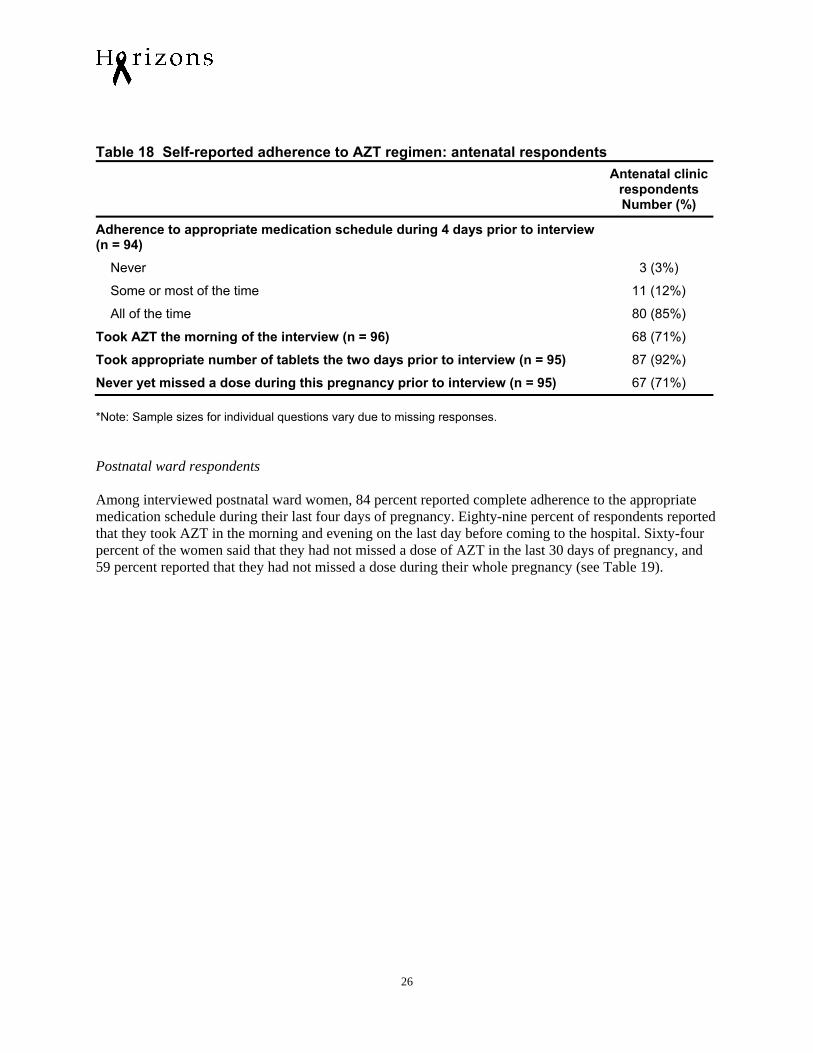
Table 18 Self-reported adherence to AZT regimen: antenatal respondents Antenatal clinic
respondents Number (%)
Adherence to appropriate medication schedule during 4 days prior to interview (n = 94)
Never 3 (3%)
Some or most of the time 11 (12%)
All of the time 80 (85%)
Took AZT the morning of the interview (n = 96) 68 (71%)
Took appropriate number of tablets the two days prior to interview (n = 95) 87 (92%)
Never yet missed a dose during this pregnancy prior to interview (n = 95) 67 (71%) *Note: Sample sizes for individual questions vary due to missing responses. Postnatal ward respondents Among interviewed postnatal ward women, 84 percent reported complete adherence to the appropriate medication schedule during their last four days of pregnancy. Eighty-nine percent of respondents reported that they took AZT in the morning and evening on the last day before coming to the hospital. Sixty-four percent of the women said that they had not missed a dose of AZT in the last 30 days of pregnancy, and 59 percent reported that they had not missed a dose during their whole pregnancy (see Table 19).
26
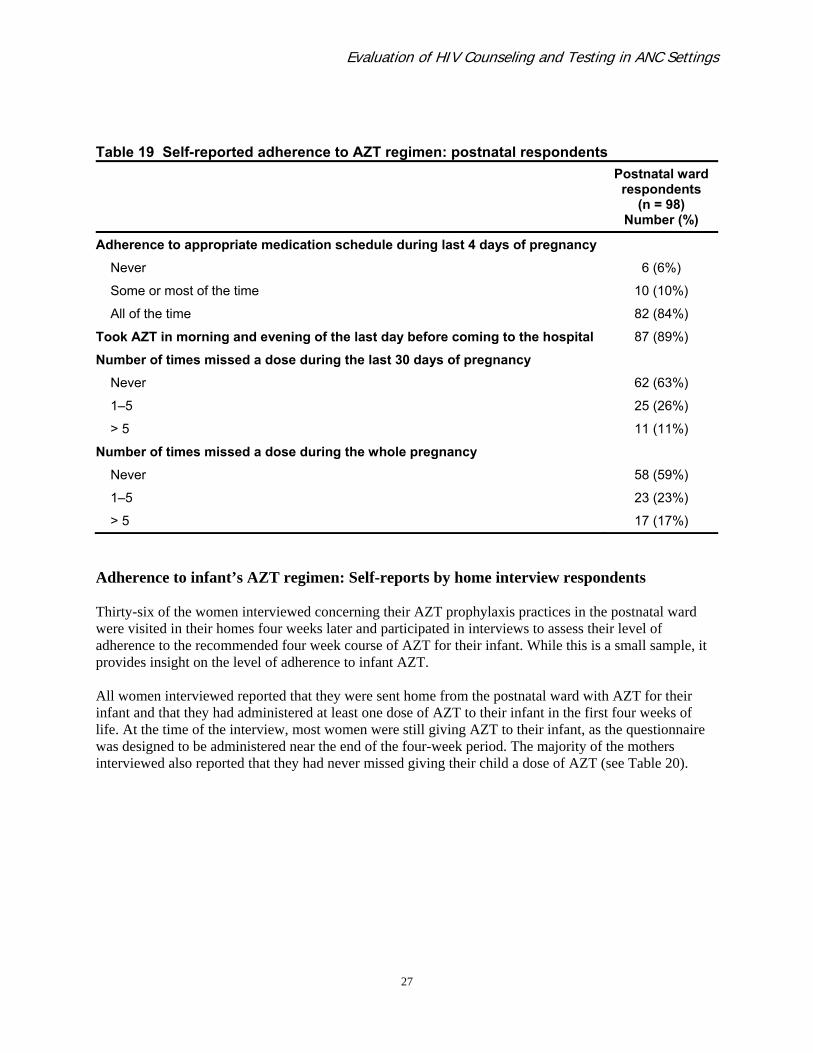
Evaluation of HIV Counseling and Testing in ANC Settings
Table 19 Self-reported adherence to AZT regimen: postnatal respondents Postnatal ward
respondents
(n = 98) Number (%)
Adherence to appropriate medication schedule during last 4 days of pregnancy
Never 6 (6%)
Some or most of the time 10 (10%)
All of the time 82 (84%)
Took AZT in morning and evening of the last day before coming to the hospital 87 (89%)
Number of times missed a dose during the last 30 days of pregnancy
Never 62 (63%)
1–5 25 (26%)
> 5 11 (11%)
Number of times missed a dose during the whole pregnancy
Never 58 (59%)
1–5 23 (23%)
> 5 17 (17%)
Adherence to infant’s AZT regimen: Self-reports by home interview respondents Thirty-six of the women interviewed concerning their AZT prophylaxis practices in the postnatal ward were visited in their homes four weeks later and participated in interviews to assess their level of adherence to the recommended four week course of AZT for their infant. While this is a small sample, it provides insight on the level of adherence to infant AZT. All women interviewed reported that they were sent home from the postnatal ward with AZT for their infant and that they had administered at least one dose of AZT to their infant in the first four weeks of life. At the time of the interview, most women were still giving AZT to their infant, as the questionnaire was designed to be administered near the end of the four-week period. The majority of the mothers interviewed also reported that they had never missed giving their child a dose of AZT (see Table 20).
27
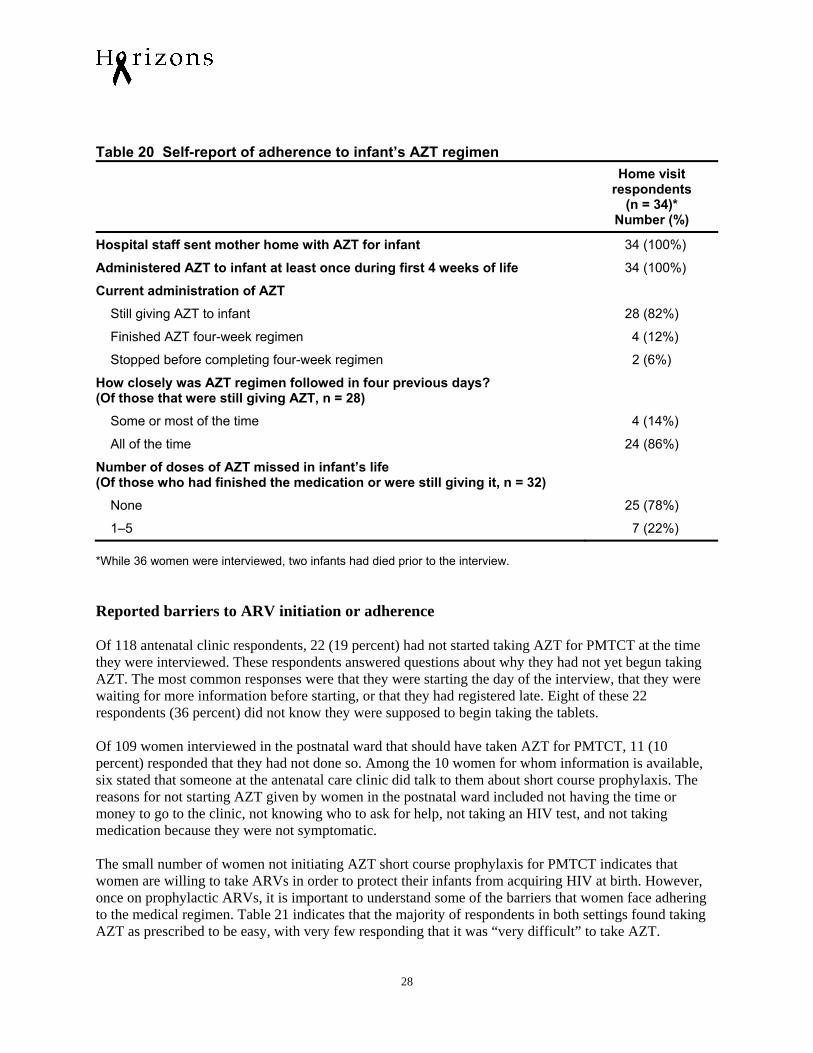
Table 20 Self-report of adherence to infant’s AZT regimen Home visit
respondents (n = 34)*
Number (%)
Hospital staff sent mother home with AZT for infant 34 (100%)
Administered AZT to infant at least once during first 4 weeks of life 34 (100%)
Current administration of AZT
Still giving AZT to infant 28 (82%)
Finished AZT four-week regimen 4 (12%)
Stopped before completing four-week regimen 2 (6%)
How closely was AZT regimen followed in four previous days? (Of those that were still giving AZT, n = 28)
Some or most of the time 4 (14%)
All of the time 24 (86%)
Number of doses of AZT missed in infant’s life (Of those who had finished the medication or were still giving it, n = 32)
None 25 (78%)
1–5 7 (22%) *While 36 women were interviewed, two infants had died prior to the interview. Reported barriers to ARV initiation or adherence Of 118 antenatal clinic respondents, 22 (19 percent) had not started taking AZT for PMTCT at the time they were interviewed. These respondents answered questions about why they had not yet begun taking AZT. The most common responses were that they were starting the day of the interview, that they were waiting for more information before starting, or that they had registered late. Eight of these 22 respondents (36 percent) did not know they were supposed to begin taking the tablets. Of 109 women interviewed in the postnatal ward that should have taken AZT for PMTCT, 11 (10 percent) responded that they had not done so. Among the 10 women for whom information is available, six stated that someone at the antenatal care clinic did talk to them about short course prophylaxis. The reasons for not starting AZT given by women in the postnatal ward included not having the time or money to go to the clinic, not knowing who to ask for help, not taking an HIV test, and not taking medication because they were not symptomatic. The small number of women not initiating AZT short course prophylaxis for PMTCT indicates that women are willing to take ARVs in order to protect their infants from acquiring HIV at birth. However, once on prophylactic ARVs, it is important to understand some of the barriers that women face adhering to the medical regimen. Table 21 indicates that the majority of respondents in both settings found taking AZT as prescribed to be easy, with very few responding that it was “very difficult” to take AZT.
28
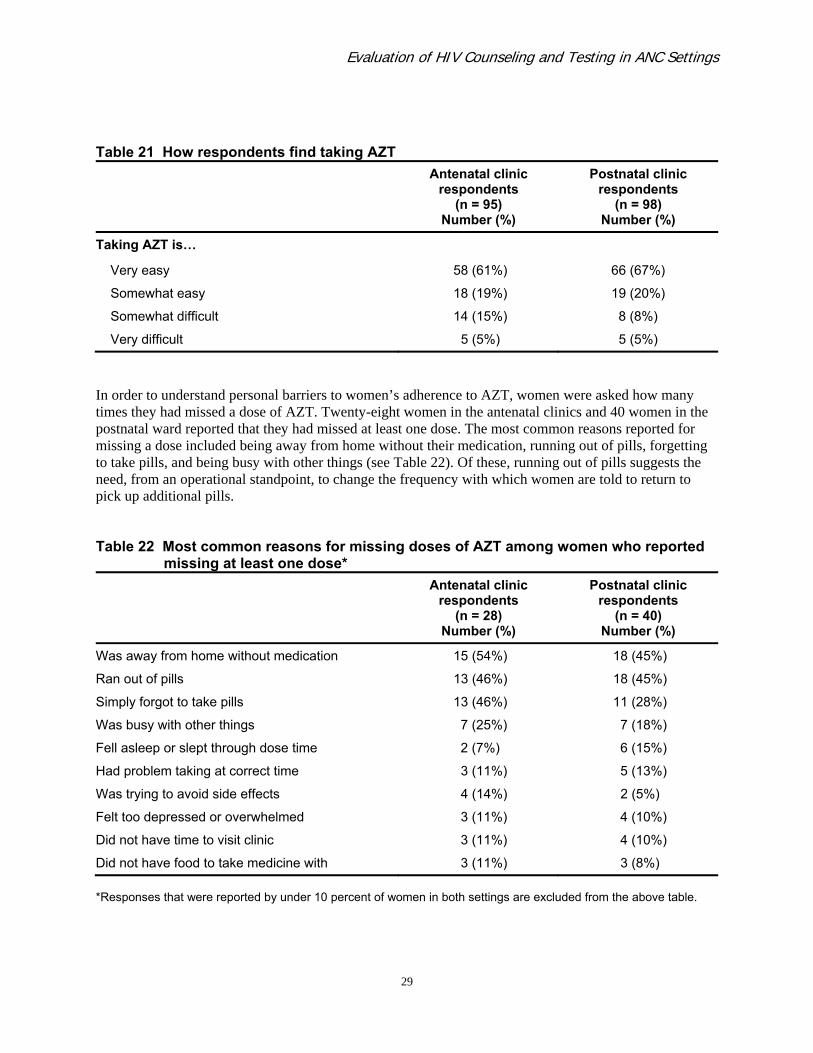
Evaluation of HIV Counseling and Testing in ANC Settings
Table 21 How respondents find taking AZT Antenatal clinic
respondents (n = 95)
Number (%)
Postnatal clinic respondents
(n = 98) Number (%)
Taking AZT is…
Very easy 58 (61%) 66 (67%)
Somewhat easy 18 (19%) 19 (20%)
Somewhat difficult 14 (15%) 8 (8%)
Very difficult 5 (5%) 5 (5%)
In order to understand personal barriers to women’s adherence to AZT, women were asked how many times they had missed a dose of AZT. Twenty-eight women in the antenatal clinics and 40 women in the postnatal ward reported that they had missed at least one dose. The most common reasons reported for missing a dose included being away from home without their medication, running out of pills, forgetting to take pills, and being busy with other things (see Table 22). Of these, running out of pills suggests the need, from an operational standpoint, to change the frequency with which women are told to return to pick up additional pills. Table 22 Most common reasons for missing doses of AZT among women who reported missing at least one dose* Antenatal clinic
respondents (n = 28)
Number (%)
Postnatal clinic respondents
(n = 40) Number (%)
Was away from home without medication 15 (54%) 18 (45%)
Ran out of pills 13 (46%) 18 (45%)
Simply forgot to take pills 13 (46%) 11 (28%)
Was busy with other things 7 (25%) 7 (18%)
Fell asleep or slept through dose time 2 (7%) 6 (15%)
Had problem taking at correct time 3 (11%) 5 (13%)
Was trying to avoid side effects 4 (14%) 2 (5%)
Felt too depressed or overwhelmed 3 (11%) 4 (10%)
Did not have time to visit clinic 3 (11%) 4 (10%)
Did not have food to take medicine with 3 (11%) 3 (8%) *Responses that were reported by under 10 percent of women in both settings are excluded from the above table.
29
For infant adherence, the sample size was small and only seven out of thirty two women (whose infants had finished the medication or were still giving it) said that they had ever missed a dose of AZT for their infant. Reasons for missing doses among these seven women included not understanding how to give the AZT, being away from home, being busy, forgetting, and sleeping through the dose. Operational Successes and Barriers Operational issues associated with clients obtaining ARVs for PMTCT The majority of women found it necessary to pick up AZT once every week or once every two weeks. This is frequent, but most respondents indicated that this frequency and pharmacy hours were convenient. The majority of women did not have to travel more than two kilometers to pick up their medication and were able to travel this distance by walking or public transportation. Once they were at the clinic, almost all respondents felts that the clinic staff protected their privacy. A few women reported that the pharmacy had run out of AZT when it was needed. As reported in the section on personal barriers to medication adherence, running out of pills was the second most common reason for missing a dose of AZT. This is likely due to the fact that almost all women were refilling their AZT often, and half of women did not pick up their refills until they had no remaining medication. Table 23 highlights operational issues associated with obtaining ARVs for PMTCT.
30

Evaluation of HIV Counseling and Testing in ANC Settings
Table 23 Operational factors involved in women accessing AZT for prophylaxis HIV-positive
pregnant women (n = 95)a
Number (%)
HIV-positive postnatal ward women
(n = 98)a
Number (%)
How often AZT picked up:
Once a week 24 (25%) 48 (49%)
Once every two weeks 53 (56%) 30 (31%)
Once a month 6 (6%) 7 (7%)
Other* 12 (13%) 13 (13%)
Picking up AZT is convenient 87 (93%) 94 (96%)
Pharmacy hours are convenient 84 (88%) 96 (98%)
Pharmacy has been out of AZT when it was needed 9 (9%) 19 (19%)
Clinic staff protected privacy 91 (97%) 90 (92%)
Distance traveled to obtain AZT
< 1 km 52 (55%) 55 (56%)
1–2 km 25 (26%) 20 (20%)
3–4 km 9 (9%) 7 (7%)
> 4km 9 (9%) 16 (17%)
Mode of transport used to pick up AZT
Walking 66 (69%) 69 (70%)
Car 7 (7%) 8 (8%)
Public transportation 24 (25%) 20 (21%)
Received extra AZT in case they could not return to clinic in time
14 (15%)
4 (4%)
AZT was refilled when…
None was left 48 (51%) 57 (58%)
One to few days left 43 (45%) 36 (37%)
Week’s supply left 2 (2%) 1 (1%)
Only picked up once 1 (1%) 4 (4%)
aNot all groups of answers add to 100% as some were missing 1–2 responses. *“Other” included answers without timeframes, such as “during ANC visits” or “when finished.”
31
Provider-perceived barriers to clients accessing ARV prophylaxis Follow-up with clients is an important part of any treatment regimen. When specifically asked if they talked to women about PMTCT medications or gave PMTCT medications, all providers responded that they did. All also said that women were educated on how and when to take the medication by nurses, midwives, or counselors. However, only 18 of the 43 respondents (42 percent) said that they followed up with patients to make sure that they took the correct dose at the correct time. Half of those who did not follow up with women cited lack of time and/or manpower as the primary reason. Other reasons included that it is not their duty to follow up, that the women are too difficult to locate for follow-up, and that they trust that the women are adhering properly. Only six of the providers acknowledged that there had been difficulties in administering AZT. Of these six, three said that the difficulties were caused by using 100 mg tablets instead of having access to 300 mg tablets.2 The other three noted that women do not take their AZT properly, they register too late, and that some women refuse to know their HIV status until after they deliver. Community Resources It is important for HIV-positive women to be aware of community resources and support services that can help them cope with their HIV status. During the interviews, HIV-positive women were asked questions about access to and awareness of community resources. Most women did not receive information from clinic staff about their eligibility to receive a food basket or where to go to meet other HIV-positive women (see Table 24). Table 24 Knowledge of community resources among HIV-positive women HIV-positive
pregnant women (n = 118)
Number (%)
HIV-positive postnatal ward women
(n = 125) Number (%)
Learned from someone at the ANC clinic that they are eligible to receive a food basket
32 (27%) 26 (21%)
Learned from someone at the ANC clinic where to go to meet other HIV-positive women to receive support
13 (11%) 27 (22%)
Knows where to go to meet other HIV-positive women 19 (16%) 36 (29%)
Clinics and hospitals were the most commonly mentioned sources of information and services, suggesting that there are not many community resources that these women are aware of.
2Women take 300 mg of AZT two times daily. Use of 100 mg tablets causes staff to count out three times more tablets than if they used 300 mg tablets.
32
Evaluation of HIV Counseling and Testing in ANC Settings
Discussion and Recommendations This evaluation was designed as an opportunity for policymakers and program managers in Botswana to learn about the quality of HIV post-test counseling, education of HIV-positive pregnant women, and any existing problems with ARV prophylaxis adherence. The findings can be used to help design and test activities to improve the quality of counseling that HIV-positive pregnant women receive, to increase the number of women starting ARV prophylaxis or therapy, and to improve adherence to these medications. For stakeholders in other resource-constrained settings, this evaluation demonstrates the feasibility of administering a more complex regimen within ANC/MCH. While different challenges may arise depending on contextual factors, the lessons learned from Botswana can be applied to other settings. HIV Counseling and Testing Testing acceptance was high in this study, and represents a large improvement over findings from a study based on the Botswana AIDS Impact Survey in 2001 (Rakgoasi 2005). While coverage of testing was very high in this sample, the quality of information transmission to HIV-infected women could be improved. As HIV counseling is a woman’s first point of contact with the health system in learning how to cope with her HIV status, receiving a positive result is an emotional experience. This can be compounded when a woman is pregnant and faced with the possibility of passing the virus on to her child. In this study more than two-thirds of women received only one post-test counseling session. Therefore it is particularly important that this session be structured and standardized in order to effectively transmit essential information as well as provide emotional support. When providers were asked what general information they believed was important to convey to HIV-positive women during post-test counseling, there were many different combinations of responses. In addition, only two responses were mentioned by more than half of the respondents; this suggests that providers have very different notions of what is considered essential information. There was also large variation in opinions of what women need to hear regarding AZT adherence. These findings suggest that there are no standardized post-test counseling materials being followed by providers for covering pre-determined key information. Observations of post-test counseling sessions with HIV-positive pregnant women revealed that in most cases the information delivered in these sessions was incomplete. Of all of the information on the post-test counseling check list used to evaluate these sessions, explaining the meaning of an HIV positive test result was the only item discussed in all 22 observations. Nearly all of these 22 observations did include the mention of availability of ARV therapy and initial information about CD4 testing. However, there were severe gaps in the information provided on PMTCT. Moreover, in less than half of observed sessions, providers distributed the handout that explained next steps for safeguarding the health of women and infants, and in a similar proportion of sessions, mentioned that the client could receive further counseling in the future. Results from studies in South Africa and Kenya also point to the need for standardization of counseling as these countries aim to improve and scale up PMTCT services in an effective manner (Chopra et al. 2005;
33

Delva et al. 2006). Delva et al. (2006) point out that, as in our evaluation where the majority of counselors spend only 20–30 minutes on post-test counseling with HIV-positive women, “the limited time dedicated to women receiving antenatal VCT contrasts with the heavy and comprehensive load of health information and advice they are supposed to receive.” These studies as well as ours suggest that there are key gaps in the delivery of information to HIV-positive pregnant women. In this evaluation we were able to examine the views of providers stratified by occupational title. Although the sample size was small, nurses and midwives differed from HIV counselors (possibly due to differences in their training, knowledge base, and experience) in terms of what they deemed to be important to discuss. This indicates the need to standardize training across all providers conducting post-test counseling. As Botswana’s health system includes dedicated HIV counselors, it would be helpful to have clearly delineated roles explaining what information counselors are responsible for relaying to clients and what information nurses/midwives should be responsible for relaying. During the time of this evaluation, there were no standardized tools. The impact of the lack of standardized counseling is reflected in the poor recall of important topics discussed during post-test counseling sessions among the women interviewed in this study. The wide range in topics remembered, the fact that only one topic was mentioned by more than 50 percent of women interviewed in both the antenatal clinics and the postnatal ward, and the fact that 10 percent of women in both groups did not remember anything that was discussed demonstrates a severe gap in the flow of knowledge to these women and their ability to retain information. For future studies, it will be important to assess women’s retention of knowledge as an important indicator of the effectiveness of counseling. While not statistically significant, results from this study suggest that women who have more than one counseling session tended to recall more than women who received only one session, indicating that women may benefit from receiving more than one counseling session. Standardization of counseling and role delineation is especially important in the face of routine opt-out HIV testing in the antenatal clinic setting. Since 2004, the national PMTCT program in Botswana has implemented provider-initiated routine HIV testing. This has led to significant increases in the percentage of women who know their HIV status at delivery and the percentage of women receiving PMTCT interventions, indicating that routine testing has been well accepted (Creek et al. 2007). As uptake of PMTCT interventions increase, there must be concurrent evaluation of the quality of services received to ensure that the interventions are effective. Kiarie et al. (2003) found that to improve compliance with PMTCT regimens there was a need for greater involvement of partners. It is encouraging that in this study, among women who disclosed, partner/husband was the most frequently mentioned individual, with more than 80 percent of HIV-positive women reporting having disclosed to their partner/husband. This suggests that Botswana’s national leadership, public health interventions, and media campaigns have worked to fight the HIV epidemic not only through increased prevention, treatment, and care services, but also through decreasing the fear and stigmatization that are often responsible for a lack of disclosure. HIV serostatus disclosure initiates discussion among sexual partners that can lead to behavior change, a discussion of contraceptives, and increased partner support for accessing PMTCT and other treatment and care programs (Medley et al. 2004). The importance of disclosure in the prevention of vertical transmission of HIV makes it a priority topic for inclusion in any standardized counseling materials. Less than half of the women in this study reported that their partner had tested. The discrepancy in the level of testing between these women and their partners may in part be attributed to routine testing of women offered during antenatal care, while men do not have a comparable opportunity where they are
34

Evaluation of HIV Counseling and Testing in ANC Settings
encouraged to test. This supports the need to implement WHO’s recommendation that HIV counseling and testing be a part of diagnostic assessments and clinical evaluations when individuals present to health care facilities (WHO/UNAIDS 2007). In addition to providing men opportunities for counseling and testing during other diagnostic assessments, the ability to conduct couples testing and counseling in the context of antenatal care could also be explored in order to facilitate disclosure and support between partners (Semrau et al. 2005; Painter 2001). AZT Receipt and Adherence The majority of women did take AZT for PMTCT or were on therapeutic ARVs during their pregnancy. Receipt of maternal AZT and maternal and infant nevirapine at delivery was also high. While it is encouraging that the vast majority of women delivering at the hospital were receiving the medications they and their infant need based on hospital records, it is important to note that many of the women were unaware that they or their infant had received these medications. This indicates the need for increasing awareness of these medications and their purpose among HIV-positive women. Women’s self-reports demonstrated that the majority of mothers and infants were adhering to their respective AZT regimen, but there is room for improvement, as optimal adherence to antiretroviral regimens should be greater than 95 percent (Paterson et al. 2000) This study identified a number of factors that may negatively impact adherence, such as one-off counseling that does not provide essential information, lack of follow-up once women start their AZT regimen, and the need for women to collect medication frequently. While most women lived close to a pharmacy and said that this was convenient, running out of pills was a main reason for missing doses of AZT. This suggests that many missed doses may be averted if a two-week supply was standard and if women were encouraged to refill their AZT before it ran out. Additionally, expanded counseling and follow-up of HIV-positive women should be considered as measures PMTCT services can take to foster adherence to ARVs. While the sample size for infant adherence is small, the fact that only two mothers stopped administering AZT and that most reported high levels of adherence to the schedule indicates that mothers are both willing and able to adhere to a four-week AZT regimen for their infants. As this study relied on self-reports for assessing adherence by women and infants, prospective evaluations that are able to observe adherence through multiple methods are needed. Community Resources Support from health workers, family members, partners, and the community can be important in order to attain the levels of participation and adherence needed to substantially decrease the burden of mother-to-child transmission of HIV. Currently, referral of HIV-positive pregnant women to community resources is poor. This needs to be improved in order to ensure the health and well-being of HIV-positive women and their families.
35
Recommendations The following recommendations emerged from the study: • Standardize post-test counseling content through the use of job aids. The WHO/CDC Testing and
Counseling for PMTCT support tools are designed to provide standardized information and can be customized by country programs. Adoption of these materials would expedite the introduction of standardized counseling. The tools are available at (http://www.who.int/hiv/pub/vct/tc/en/index.html).
• Adapt existing WHO written materials for distribution to HIV-positive mothers and pilot their usefulness in Botswana.
• Include as part of counseling an assessment of each client’s understanding of essential HIV information. Before leaving the counselor’s office, clients should understand at least the need to have their CD4 count checked, the meaning of the CD4 count, and information on PMTCT, including a specific AZT start date, and be aware that the counselor can provide ongoing support and information throughout the pregnancy.
• Encourage provision of at least two sessions with the counselor for each woman. The second session may be able to focus more on PMTCT program reinforcement, support, and adherence, whereas the first may focus more on accepting and understanding the HIV-positive test. To a great extent, though, the same essential information should be covered in both sessions, increasing the likelihood of retention of the information.
• Encourage women to bring partners and other family members to visit the counselor with them, to increase family understanding of HIV and PMTCT and encourage HIV testing for other family members. .
• Improve the AZT distribution process by standardizing the time interval for AZT refill pick-up, which would reduce the frequency of refills, and encourage women to refill their AZT before they run out of pills.
• Government health facilities should improve the distribution of information about community resources, such as support groups, health services, and nutritional services, and actively help women to access these services.
36
Evaluation of HIV Counseling and Testing in ANC Settings
References Botswana National AIDS Coordinating Agency (NACA). 2003. 2003 Second Generation HIV/AIDS Surveillance Technical Report. Gaborone: NACA. Chopra, M. et al. 2005. “Preventing HIV transmission to children: Quality of counseling of mothers in South Africa,” Acta Paediatrica 94(3): 357–363. Creek, T.L. et al. 2007. “Successful introduction of routine opt-out HIV testing in antenatal care in Botswana,” Journal of Acquired Immune Deficiency Syndromes 45(1): 102–7. Delva, W. et al. 2006. “Quality and quantity of antenatal HIV counseling in a PMTCT programme in Mombasa, Kenya,” AIDS Care 18(3): 189–193. Guay, L.A. et al. 1999. “Intrapartum and neonatal single-dose nevirapine compared with zidovudine for prevention of mother-to-child transmission of HIV-1 in Kampala, Uganda: HIVNET 012 randomized trial,” Lancet 354(9181): 795–802. Kiarie, J. N. et al. 2003. “Compliance with antiretroviral regimes to prevent perinatal HIV-1 transmission in Kenya,” AIDS 17: 65–71. Medley, A. et al. 2004. “Rates, barriers and outcomes of HIV serostatus disclosure among women in developing countries: implications for prevention of mother-to-child transmission programmes,” Bulletin of the World Health Organization 82: 299–307. Painter, T.M. 2001. “Voluntary counseling and testing for couples: a high-leverage intervention for HIV/AIDS prevention in sub-Saharan Africa,” Social Science and Medicine 53(2001): 1397–1411. Paterson, D.L. et al. 2000. ”Adherence to protease inhibitor therapy and outcomes in patients with HIV infection,” Annals of Internal Medicine 133(1): 21–30. Rakgoasi, S.D. 2005. “HIV counselling and testing of pregnant women attending antenatal clinics in Botswana, 2001,” Journal of Health, Population and Nutrition 23(1): 58–65. Rutenberg, N. et al. 2003. “Evaluation of United Nations-supported pilot projects for the prevention of mother-to-child transmission of HIV.” New York: UNICEF and Population Council. Semrau, K. et al. 2005. “Women in couples antenatal HIV counseling and testing are not more likely to report adverse social events,” AIDS 19: 603–609. Shaffer, N. et al. 1999. “Randomized placebo-controlled trial of short-course antenatal zidovudine to reduce perinatal HIV transmission, Bangkok, Thailand,” Lancet 353(9155): 773–80. Stringer, J.S. et al. 2003. “Comparison of two strategies for administering nevirapine to prevent perinatal HIV transmission in high-prevalence, resource-poor settings,” AIDS 32(5): 506–13.
37
38
Turner, B.J. 2002. “Adherence to antiretroviral therapy by human immunodeficiency virus-infected patients,” The Journal of Infectious Diseases 185(Suppl 2): S143–51. USAID. 2005. “In focus: Women and AIDS: Prevention of mother-to-child HIV transmission,” Issue Brief. World Health Organization (WHO). 2006. “Antiretroviral drugs for treating pregnant women and preventing HIV infection in infants in resource-limited settings: Towards universal access: recommendations for a public health approach.” Geneva: WHO. WHO/UNAIDS. 2007. Guidance on Provider-Initiated HIV Testing and Counselling in Health Facilities. Geneva: World Health Organization. Geneva: WHO.

Horizons is implemented by the Population Council in collaboration with
International Center for Research on Women (ICRW)International HIV/AIDS AlliancePATHTulane UniversityFamily Health International (FHI)Johns Hopkins University
Horizons is a global operations research program designed to:
Identify and test potential strategies to improve HIV/AIDS prevention, care, and support programs and service delivery.
Disseminate best practices and utilize findings with a view toward scaling upsuccessful interventions.
For more information, please contact:
Horizons Program, Communications Unit4301 Connecticut Avenue, NW Suite 280Washington, DC 20008 USATel: 202-237-9400Fax: 202-237-8410Email: [email protected]/horizons