especies de malassezia productoras de infecciones sistémicas...
TRANSCRIPT
69
Especies de Malassezia productoras de infecciones sistémicas y superficiales Giusiano, Gustavo; Mangiaterra, Magdalena; Sosa, María de los Angeles; Bustillo, Soledad Departamento Micología. Instituto de Medicina Regional. Universidad Nacional del Nordeste. Av. Las Heras 727. (3500) Resistencia, Chaco. Argentina. E-mail: [email protected] Subsidiado por la Fundación Alberto J. Roemmers. Introducción El género Malassezia, con Malassezia fufur (M. furfur) como especie tipo, fue creado por Baillon en 1889 en honor a Luis Malassez, el primero que lo describió. La denominación de la especie hace alusión a las finas escamas, de consistencia furfurácea o parecida al salvado, que se desprenden de las lesiones (1). La mayoría de las especies del género Malassezia son parte de la biota cutánea normal humana y pueden ser cultivadas desde casi todas las áreas del cuerpo, principalmente de aquellas con abundantes glándulas sebáceas. Esto se debe a que estos hongos tienen un defecto en la síntesis de los ácidos grasos, que se manifiesta en el requerimiento de ácidos grasos exógenos. Esta parece ser la razón por la cual son prevalentes en piel con alta producción seborreica. Bajo la influencia de ciertos factores pueden volverse patógenos y participar en diversas enfermedades tal como pitiriasis versicolor, foliculitis, dermatitis seborreica, algunas formas de dermatitis atópicas, de papilomatosis confluente y reticulada y en infecciones sistémicas. Los factores predisponentes endógenos incluyen piel grasa, hiperhidrosis, factores hereditarios, tratamiento con corticosteroides, malnutrición e inmunodeficiencias. Los factores exógenos más importantes son la temperatura y la humedad relativa ambiente altas. La recurrencia es característica de las infecciones por Malassezia, particularmente en pitiriasis versicolor. La cura permanente es difícil de lograr, por lo que, para evitar la recurrencia, el tratamiento profiláctico es mandato (2,3,4). La aparición de levaduras del género Malassezia como patógenos emergentes en infecciones sistémicas e intrahospitalarias está en relación a pacientes inmunocomprometidos y a niños prematuros, especialmente los que están en unidades de cuidados intensivos (UCI) y reciben alimentación lipídica parenteral. Cuando estos pacientes presnetan datos clínicos o analíticos de sepsis y hemocultivo negativo para microorganismos habituales, es imprescindible la realización de un subcultivo para el aislamiento de Malassezia spp La entrada del organismo al cuerpo se produce a través del catéter venoso desde la piel colonizada. Las levaduras pasan al torrente sanguíneo donde encuentran soporte nutricional en los lípidos de la alimentación. Si bien ésta es la menos frecuente de las infecciones fúngicas nosocomiales, es importante por su alto porcentaje de morbimortalidad (4,5,6). Los recién nacidos sanos a término no están colonizados. La colonización se inicia en los primeros días de vida, alcanzando alrededor del 30% al cabo de un mes. Se ha demostrado que esta tasa aumenta hasta 80% en caso de niños en UCI. La manipulación por parte del personal parece ser el factor más importante de transmisión. La colonización, en el transcurso de la vida, varía paralelamente a la actividad de las glándulas sebáceas, siendo baja en la etapa prepuber, subiendo en la adolescencia hasta alcanzar un 100% en la edad adulta. La taxonomía del género Malassezia ha sido siempre materia de controversia debido a su morfología variable y a sus fastidiosos requerimientos para crecer in-vitro (7). El género Malassezia se encuadra dentro de la clase Basidiomycota, familia Cryptococcaceae. Originalmente incluía una sola especie antropofílica, M. furfur, pero en 1990 Simmons y Guého describieron M. sympodialis y luego Guillot, Midgley & Guého en 1996 por características morfológicas, fisiológicas y estudios moleculares genómicos y ribosomales, discriminaron otras cuatro (2,3,8,9). Actualmente el género consta entonces de 7 especies, de las cuales 6, M. furfur, M. sympodialis, M. slooffiae, M. obtusa, M. globosa y M. restricta, son estrictamente lípido-dependientes y son parte de la biota normal de piel del hombre. La séptima especie, M. pachydermatis (Weidmman) Dodge 1935, está adaptada al estrato córneo de los animales, raramente se ha aislado del ser humano y los lípidos presentes en un medio rico, tal como agar Sabouraud glucosado, son suficientes para asegurar su desarrollo (2,3,4,7,8,9). Estos organismos difieren entre sí en el aspecto de las colonias, las características morfológicas y fisiológicas, sus propiedades antigénicas, el porcentaje molar de G+C, las secuencias RNA/DNA de la subunidad ribosomal 25S, los requerimientos nutricionales de ácidos grasos de cadena larga, la actividad catalasa, la termotolerancia y su supervivevencia in vitro (2,3,4,7,10,11,12). Los metabolitos de estas especies, tal como el ácido dicarboxílico, pueden inducir la despigmentación de la piel intoxicando los melanocitos por inhibición de la tirosinasa. Malassezia furfur (Robin) Baillon 1889, comprende los dos neotipos culturales que históricamente corresponden a Pityrosporum ovale (P. ovale) (Castellani and Chalmers, 1913) y P. orbiculare (Gordon 1951). En 1986 estudios micológicos, inmunológicos y análisis genéticos, confirmaron que estos dos últimos son diferentes estados del complejo ciclo de desarrollo de una sola especie. M. furfur describía sólo la fase micelial de un hongo cuyas fases levaduriformes recibían los nombres de P. ovale y P. orbiculare según su morfología. P.
orbiculare fue asociado a pitiriasis versicolor y P. ovale a pitiriasis capitis y dermatitis seborreica. La fase micelial y las dos fases levaduriformes se incluyen ahora en el taxon M. furfur (7,13,14). M. furfur está
70
involucrada en una amplia gama de afecciones, desde una pitiriasis versicolor a infecciones invasivas, probablemente debido a que tiene mayor capacidad de supervivencia que las otras especies. Malassezia sympodialis (Simmons & Guého, 1990) es la especie más aislada en el hombre, tanto de piel sana como enferma. Ha sido descripta asociada a pitiriasis versicolor, foliculitis y dermatitis seborreica (7,9). Generalmente se encuentra junto a otras especies.
Malassezia slooffiae (Guillot, Midgley & Guèho, 1996), presente en humanos y animales. Por su morfología puede ser confundida con M. furfur o M. sympodialis de las que se diferencia porque no crece en los medios suplementados con Tween 20 al 10%. Hasta el momento no se sabe mucho sobre su patogenicidad (7,9,15). Malassezia obtusa (Midgley, Guillot & Guèho, 1996), es una de las especies que aparece menos frecuentemente en la piel del ser humano. Morfológicamente es parecida a. M. furfur pero difiere en sus características fisiológicas y en la capacidad de crecer a altas temperaturas (7,9,15). Malassezia globosa (Midgley, Guèho & Guillot, 1996), es residente habitual de la piel sana, se distingue porque sus células son esféricas y usualmente no crece a 37ªC (7,9,15). Malassezia restricta (Guèho, Guillot & Midgley, 1996), al igual que M. globosa se halla frecuentemente en la piel. Se distingue de las otras especies por presentar reacción negativa a la catalasa (7,9).
Malassezia spp. es sensible in-vitro a la anfotericina B, al fluconazol e itraconazol y resistente a la 5-fluorocitosina, sin embargo, no hay pruebas de sensibilidad in-vitro que permitan extrapolar esos resultados para su utilización in-vivo. Esta situación hace necesaria la ampliación de los estudios para lograr estandarizar las pruebas de sensibilidad a los agentes antifúngicos existentes. La ecología y el rol patogénico de estas nuevas especies todavía no está definido y hay pocos datos publicados al respecto (3). En el simposio sobre “el rol de las especies de Malassezia en la ecología de la piel humana y como patógeno” realizado en al XIV Congreso Internacional de la Sociedad Internacional de Micología Humana y Animal (ISHAM), se concluyó que la nueva taxonomía debe ser aplicada en estudios epidemiológicos para comprobar si las siete especies de Malassezia tienen relevancia clínica. El objeto de estudio es analizar el rol que juega cada especie de Malassezia en relación a su capacidad de producir infecciones superficiales y sistémicas. Materiales y Métodos
Muestras Las muestras fueron recolectadas entre septiembre de 2001 y septiembre de 2003, en el Departamento de Micología del Instituto de Medicina Regional (UNNE) y en el Servicio de Laboratorio del Hospital Pediátrico “Juan Pablo II” de la ciudad de Corrientes. Se estudiaron: 1.- Cepas provenientes de materiales de lesiones cutáneas obtenidos por raspado con bisturí estéril, de pacientes con pitiriasis versicolor (PV), dermatitis seborreica (DS), foliculitis (FC) y dermatitits atópicas (DA). 2.- Cepas provenientes de puntas de catéteres obtenidas de pacientes pediátricos en Unidades de Cuidados Intensivos (UCI) y en salas de oncología (SO). Metodología Examen microscópico de las muestras de lesiones cutáneas: Las escamas se observaron en fresco con hidróxido de potasio 40% diluido al medio con tinta Parker azul negro permanente. Se realizaron calcos que se colorearon con Azul de metileno y Gram. Cultivo primario Las muestras cutáneas y los catéteres se inocularon en medio de Agar Dixon modificado (7) y se incubaron a 32ºC hasta una semana, con controles diarios. Identificación Las especies de Malassezia se tipificaron en base a sus características macro y micro-morfológicas y a sus propiedades bioquímicas y fisiológicas, según la metodología propuesta por Guillot y col. (7).
• Estudio macromorfológico: descripción de las características de las colonias. • Estudio micromorfológico: se realizaron coloraciones de Gram y Azul de metileno para observación
microscópica.
71
• Características bioquímicas y fisiológicas: a) Actividad catalasa b) Capacidad de asimilación de Tween 20, 40, 60 y 80 c) Hidrólisis de la esculina d) Crecimiento a diferentes temperaturas
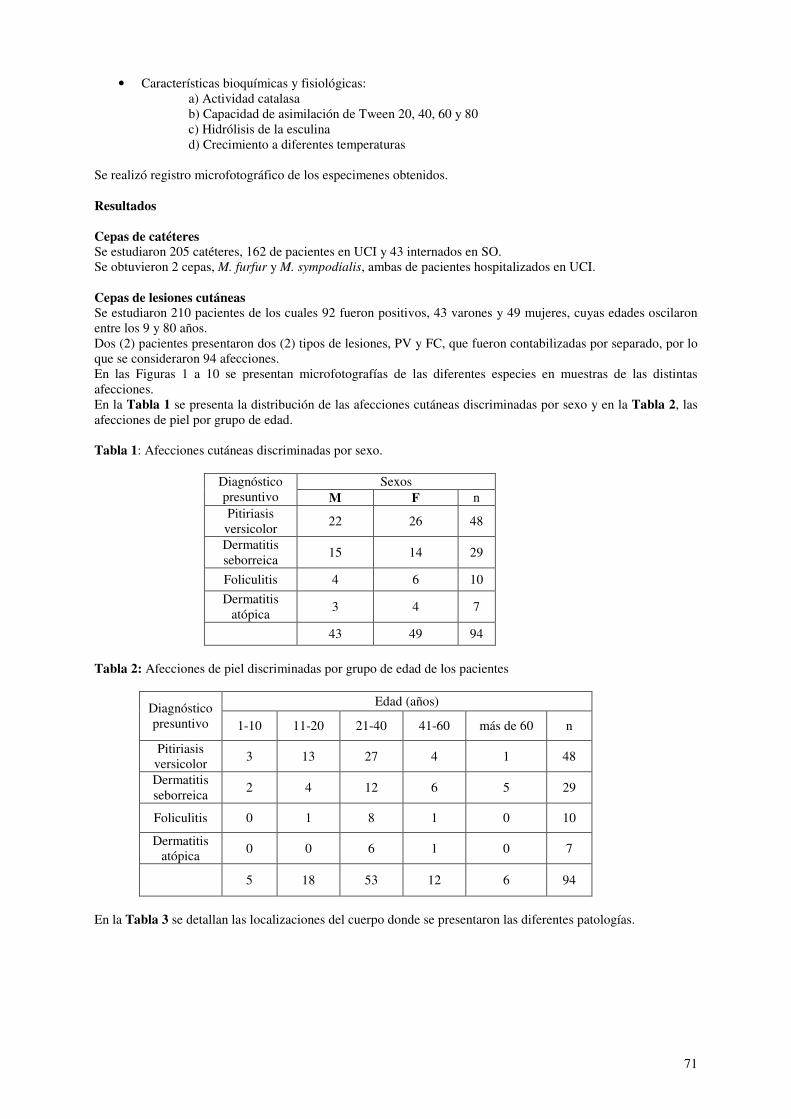
Se realizó registro microfotográfico de los especimenes obtenidos. Resultados Cepas de catéteres Se estudiaron 205 catéteres, 162 de pacientes en UCI y 43 internados en SO. Se obtuvieron 2 cepas, M. furfur y M. sympodialis, ambas de pacientes hospitalizados en UCI. Cepas de lesiones cutáneas Se estudiaron 210 pacientes de los cuales 92 fueron positivos, 43 varones y 49 mujeres, cuyas edades oscilaron entre los 9 y 80 años. Dos (2) pacientes presentaron dos (2) tipos de lesiones, PV y FC, que fueron contabilizadas por separado, por lo que se consideraron 94 afecciones. En las Figuras 1 a 10 se presentan microfotografías de las diferentes especies en muestras de las distintas afecciones. En la Tabla 1 se presenta la distribución de las afecciones cutáneas discriminadas por sexo y en la Tabla 2, las afecciones de piel por grupo de edad. Tabla 1: Afecciones cutáneas discriminadas por sexo.
Sexos Diagnóstico presuntivo M F n Pitiriasis
versicolor 22 26 48
Dermatitis seborreica
15 14 29
Foliculitis 4 6 10
Dermatitis atópica
3 4 7
43 49 94
Tabla 2: Afecciones de piel discriminadas por grupo de edad de los pacientes
Edad (años) Diagnóstico presuntivo 1-10 11-20 21-40 41-60 más de 60 n
Pitiriasis versicolor
3 13 27 4 1 48
Dermatitis seborreica
2 4 12 6 5 29
Foliculitis 0 1 8 1 0 10
Dermatitis atópica
0 0 6 1 0 7
5 18 53 12 6 94
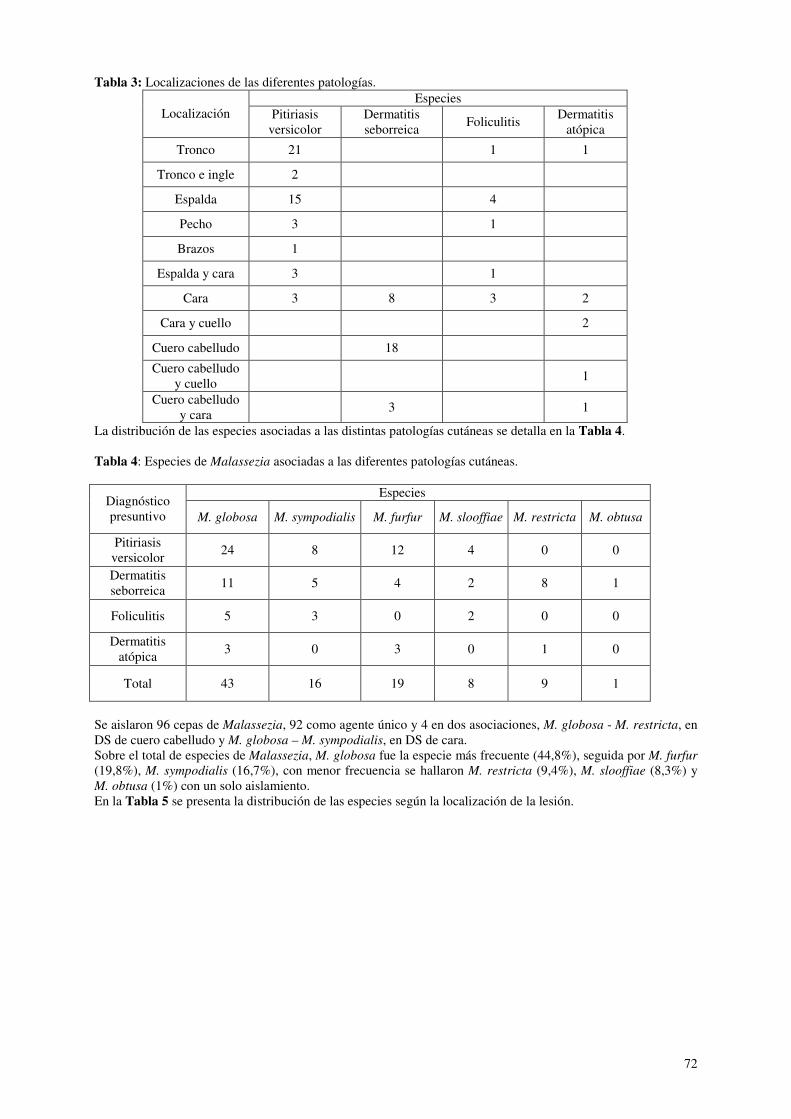
En la Tabla 3 se detallan las localizaciones del cuerpo donde se presentaron las diferentes patologías.
72
Tabla 3: Localizaciones de las diferentes patologías. Especies
Localización Pitiriasis versicolor
Dermatitis seborreica
Foliculitis Dermatitis
atópica
Tronco 21 1 1
Tronco e ingle 2
Espalda 15 4
Pecho 3 1
Brazos 1
Espalda y cara 3 1
Cara 3 8 3 2
Cara y cuello 2
Cuero cabelludo 18
Cuero cabelludo y cuello
1
Cuero cabelludo y cara
3 1
La distribución de las especies asociadas a las distintas patologías cutáneas se detalla en la Tabla 4. Tabla 4: Especies de Malassezia asociadas a las diferentes patologías cutáneas.
Especies Diagnóstico presuntivo M. globosa M. sympodialis M. furfur M. slooffiae M. restricta M. obtusa
Pitiriasis versicolor
24 8 12 4 0 0
Dermatitis seborreica
11 5 4 2 8 1
Foliculitis 5 3 0 2 0 0
Dermatitis atópica
3 0 3 0 1 0
Total 43 16 19 8 9 1
Se aislaron 96 cepas de Malassezia, 92 como agente único y 4 en dos asociaciones, M. globosa - M. restricta, en DS de cuero cabelludo y M. globosa – M. sympodialis, en DS de cara. Sobre el total de especies de Malassezia, M. globosa fue la especie más frecuente (44,8%), seguida por M. furfur (19,8%), M. sympodialis (16,7%), con menor frecuencia se hallaron M. restricta (9,4%), M. slooffiae (8,3%) y M. obtusa (1%) con un solo aislamiento. En la Tabla 5 se presenta la distribución de las especies según la localización de la lesión.
73
Tabla 5: Distribución de las especies según la localización de la lesión. Especies
Localización N M. globosa
M.
sympodialis M. furfur
M.
slooffiae
M.
restricta M. obtusa
Tronco 23 10 5 5 2
Tronco e ingle 2 1 1
Espalda 19 12 3 4 1
Pecho 4 2 1 1
Brazos 1 1
Espalda y cara 4 1 1 2
Cara 16 8 2 3 3 1
Cara y cuello 2 1 1
Cuero cabelludo 18 7 2 2 1 6 1
Cuero cabelludo y cuello
2 2
Cuero cabelludo y cara
3 2 1
Discusión En la actualidad el género Malassezia ha adquirido gran importancia dentro de los patógenos emergentes debido a que en las dos últimas décadas han sido descriptas infecciones sistémicas causadas por estos agentes. La mayoría de los casos están referidos a adultos inmunocomprometidos, neonatos prematuros y pacientes pediátricos en UCI con alimentación lipídica intravenosa a través de catéteres (16,17,18,19). Hasta el momento son escasos los estudios sobre la epidemiología de las nuevas especies de Malassezia como agentes de dermatopatologías, infecciones sistémicas o colonizador de catéteres. Los aislamientos de M. furfur y M. sympodialis que hemos obtenido a partir de catéteres son relevantes y evidencian la importancia de la introducción de cambios en la rutina del laboratorio cuando se trabaja con pacientes de riesgo. Debido a que por sus requerimientos nutricionales estos organismos no desarrollan en los medios de cultivo comunes estas infecciones son subdiagnosticadas. La detección de levaduras lipofílicas tanto en catéteres como en fluidos corporales o en tejidos, es esencial para la instauración de un tratamiento eficaz (20). La asociación de las nuevas especies de Malassezia a patologías dérmicas u otras afecciones, como agente causal o colonizante, ha impulsado el estudio de su ecología y capacidad patogénica. Los hongos de este género tienen un defecto en la síntesis de los ácidos grasos, que se manifiesta en el requerimiento de ácidos grasos exógenos. Esta parece ser la razón por la cual son prevalentes en zonas de la piel con alta producción de sebo, superficies rugosas que pueden contenerlos o atraparlos y en aquellas donde la aplicación de ungüentos y cremas es más frecuente. Aunque se considera que ninguna especie coloniza con frecuencia relativamente significativa un área susceptible más que otra, estudios recientes han mostrado cierta preferencia de las especies de Malassezia por diferentes partes del cuerpo (23,24,25). Hasta el momento es poco el conocimiento que se tiene sobre la prevalencia y la incidencia de Malassezia como información válida para la orientación en las conductas diagnóstica, profiláctica y terapéutica. En nuestro país sólo un estudio referido a dermatopatías, realizado en Buenos Aires, indica predominio general de M.
sympodialis, seguida en menor proporción por M. globosa y M. furfur (21). Esto difiere considerablemente de nuestros hallazgos donde M. globosa fue la especie aislada con mayor frecuencia, seguida por M. furfur y M.
sympodialis. También tuvimos considerables porcentajes de aislamiento de M. restricta y M. slooffiae, especies no mencionadas por esos autores. La diferencia podría deberse a que las ciudades de Buenos Aires y Resistencia están en áreas geográficas disímiles, habiendo en la segunda factores climáticos favorecedores del desarrollo de estos hongos. Está demostrado que el género Malassezia es el agente etiológico de FC, se asocia a DS y exacerba la DA, lo que no se conoce es si alguna especie se asocia particularmente a alguna de estas patologías (24). Los resultados que hemos obtenido sugieren a M. globosa como la principal especie relacionada a la PV, sin bien las otras especies aparecen en porcentajes considerables. Estudios sobre esta afección, realizados en Canadá y en Buenos Aires, revelaron predominio de M. sympodialis (con valores superiores al 50%) seguida por M. globosa y M. furfur (21,22,23). A diferencia de esto, nuestros resultados se correlacionan con diversos informes de
74
Europa y Japón que indican a M. globosa como la principal responsable de esta patología, pero obtienen un muy escaso nivel de recuperación de las otras especies (2,3,24). En la microscopía directa de las muestras hemos observado que la densidad de levaduras varía en las distintas lesiones y es considerablemente más baja en FC y DA. Por el problema estético y el prurito que ocasionan, los pacientes con estas dermatosis son más susceptibles al uso de remedios caseros, detergentes sintéticos, jabones, lociones o shampoos con aditivos. El uso de estas sustancias podría estar asociado con el bajo recuento de hongos y el reducido número de colonias obtenido a partir de este tipo de lesiones. Con respecto a DA las especies de Malassezia fueron halladas en cara, cuero cabelludo y cuello. En la literatura se hace referencia a la presencia de este género en espalda, sitio desde donde nosotros no lo aislamos, y no se informa sobre su presencia en cuero cabelludo. Las especies encontradas con mayor frecuencia asociadas a esta patología fueron M. globosa y M. furfur. En Francia y Japón, en cambio, indican a M. furfur como la más frecuente (24) y en Buenos Aires y Canadá a M. sympodialis (21,23). Es llamativo que en la única patología donde se presentaron las seis especies lipofílicas y las asociaciones fue en DS. M. globosa y M. restricta fueron las especies prevalentes. Esta epidemiología se corresponde con la encontrada en España, pero difiere de los estudios informados en Canadá (3). La edad en que se presentaron con mayor frecuencia todas la afecciones estudiadas es coincidente con la descripta desde siempre para esta afecciones. No se encontraron diferencias respecto a la distribución por sexo. Es posible que la composición lipídica del estrato córneo esté relacionada al crecimiento de determinadas especies de Malassezia en ciertas afecciones y en determinados sitios anatómicos. Nuestros resultados podrían avalar esta afirmación pero se necesitarían estudios más amplios y más complejos Además es importante considerar, como en otras dermatosis fúngicas, la posibilidad, ya sea como agente etiológico como colonizador comensal, de una variación en la prevalencia relacionada con la distribución geográfica (23). Así nuestros datos coinciden mayormente con los informes de Europa y Asia, y difieren considerablemente de lo hallado en Canadá y Buenos Aires, por lo que estaríamos en desacuerdo con una distribución particular para América como indican estos últimos (21). El método de identificación basado en pruebas bioquímicas y fisiológicas por asimilación de Tweens y reacción de catalasa propuesto por Guillot y col. (4) tiene la ventaja de su simplicidad metodológica y conveniencia económica. Tiene ciertas desventajas respecto a la ambigüedad en la lectura de las placas de asimilación, obteniéndose resultados poco específicos para diferenciar entre M. furfur, M. sympodialis y M. slooffiae, principalmente entre las dos primeras (26). Otro de los problemas de esta metodología se presenta frente a las mezclas de especies. Por ejemplo M. restricta, que es catalasa negativa, puede no ser detectada cuando está asociada, ya que siempre se obtiene una reacción de catalasa positiva (23). Este problema puede ser salvado con el uso de métodos de biología molecular, por ejemplo PCR-REA, lo que permitiría la detección de un mayor porcentaje de mezclas (26). La naturaleza fúngica de la pitiriasis versicolor fue reconocida por Eichsted en 1846 y su agente etiológico, el género Malassezia, taxonómicamente ubicado medio siglo después por Baillon. En los últimos años, casi 100 años después, gracias al desarrollo de técnicas de biología molecular, se ha podido consensuar respecto a la clasificación de las especies de este género. Sigue aún en estudio el verdadero rol que juega cada una de las especies en relación a su capacidad de producir infecciones superficiales y sistémicas, su tendencia a colonizar determinados áreas del cuerpo, su mayor o menor virulencia y su susceptibilidad a los antifúngicos. Estudios epidemiológicos y ecológicos basados en esta reclasificación del género y las nuevas técnicas para su estudio, permitirán correlacionar la distribución de Malassezia con factores fisico-químicos, inmunológicos y biogeográficos del hospedero y con ello ampliar el conocimiento sobre la patogenia de éste género emergente (23). Este estudio es una contribución al conocimiento de la ecología y la distribución de las especies de Malassezia en hospederos inmunocomprometidos e inmunocompetenetes.
75
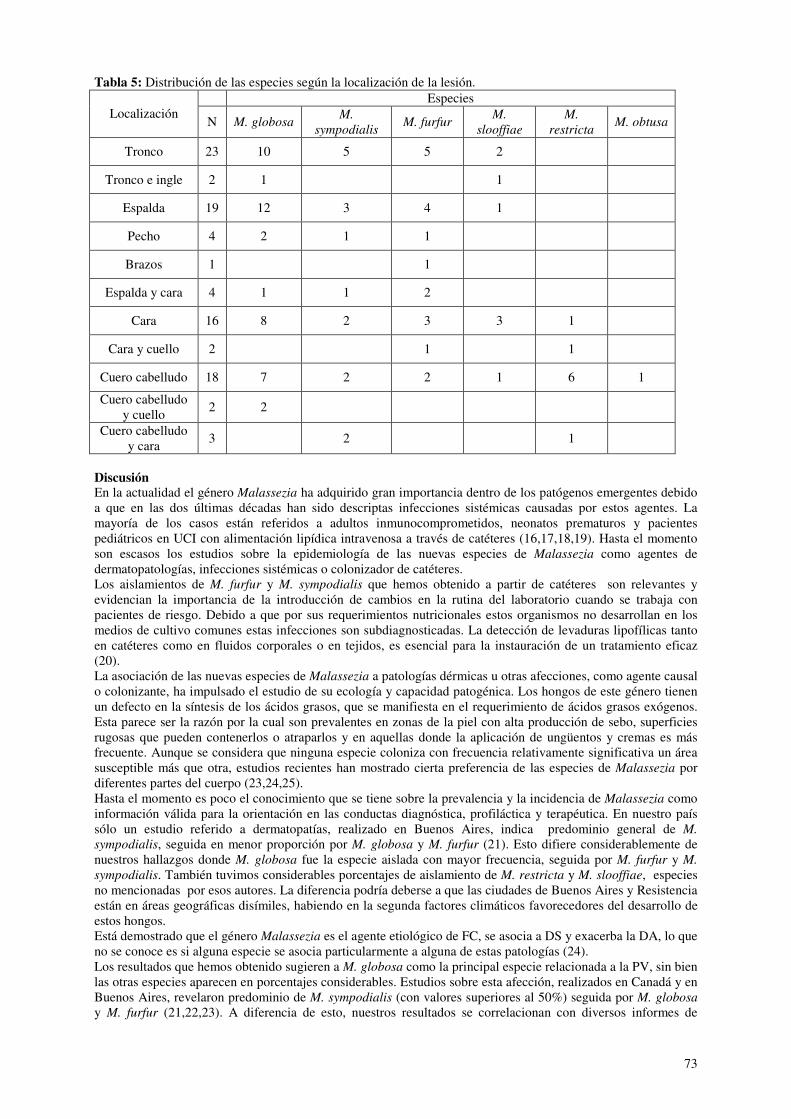
Figura 1: Malassezia furfur en muestra de pitiriais versicolor.
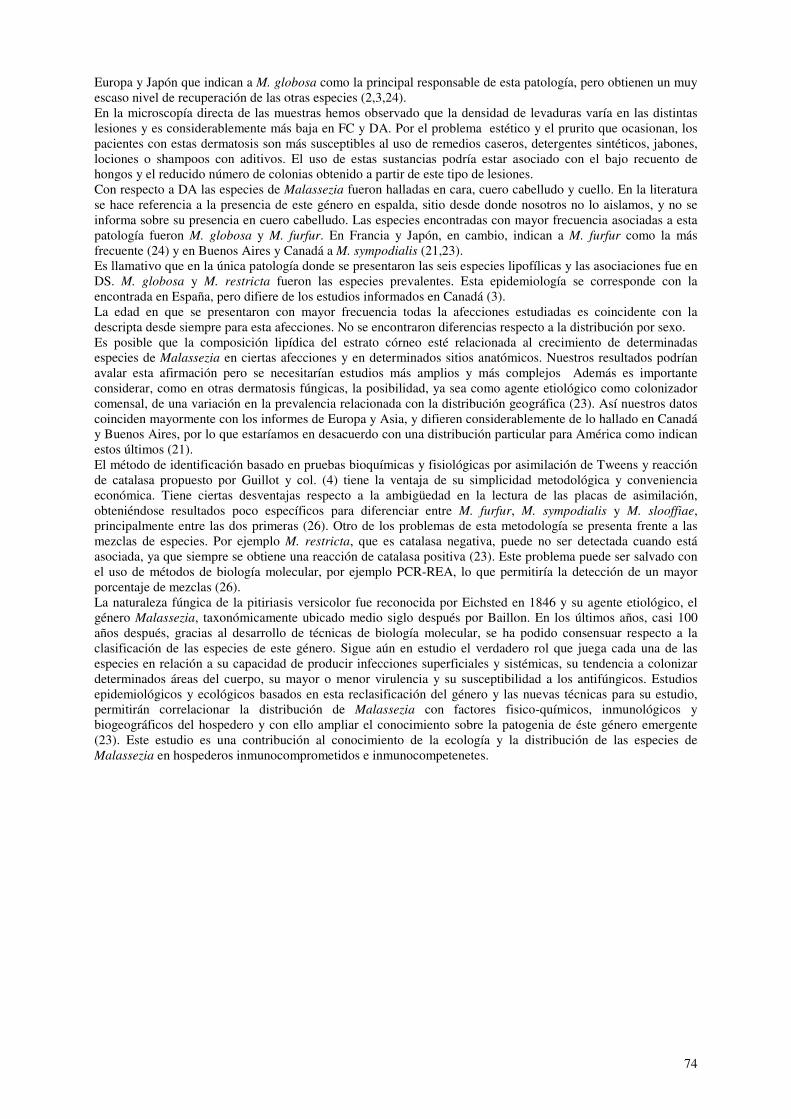
Figura 2: Malassezia sympodialis en muestra de dermatitis seborreica.
76
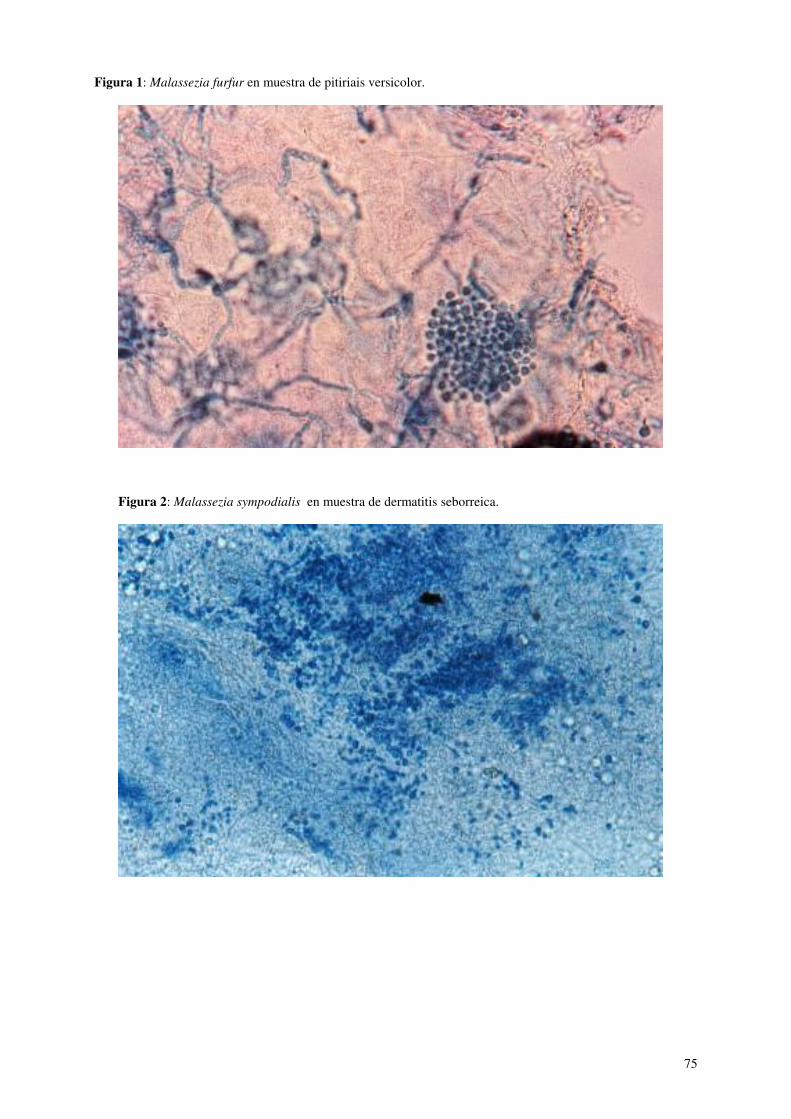
Figura 3: Malassezia obtusa en muestra de dermatitis seborreica.
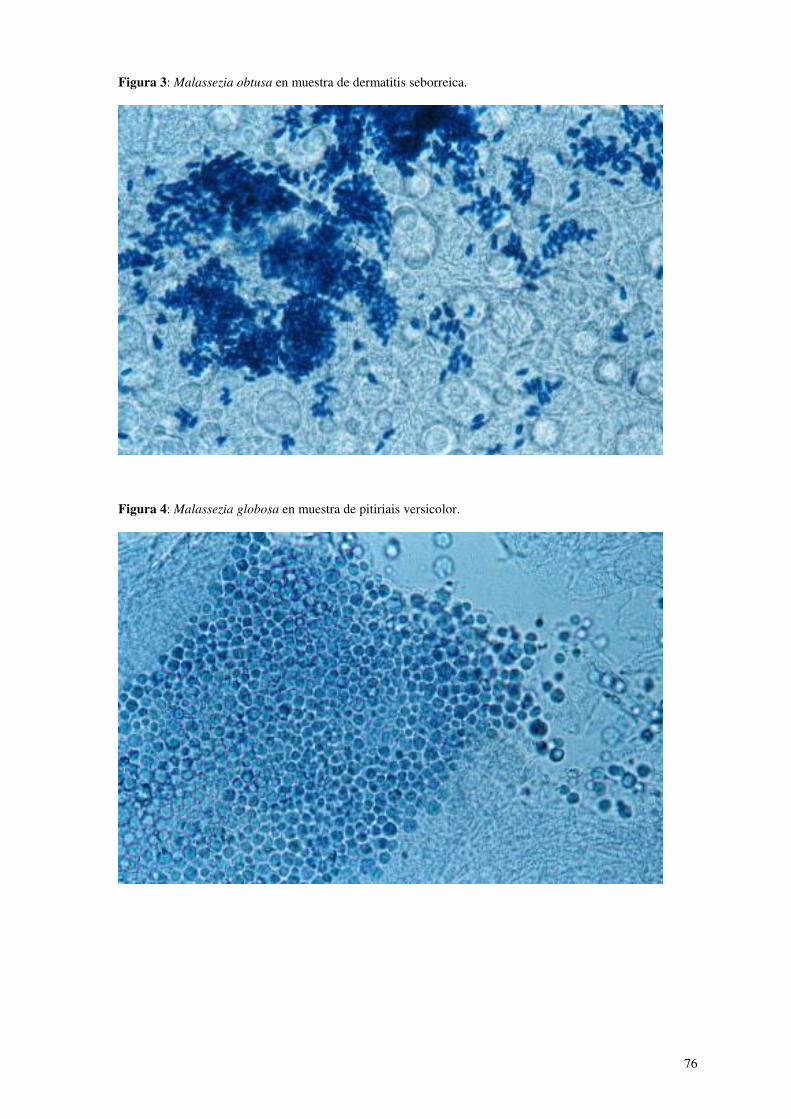
Figura 4: Malassezia globosa en muestra de pitiriais versicolor.
77
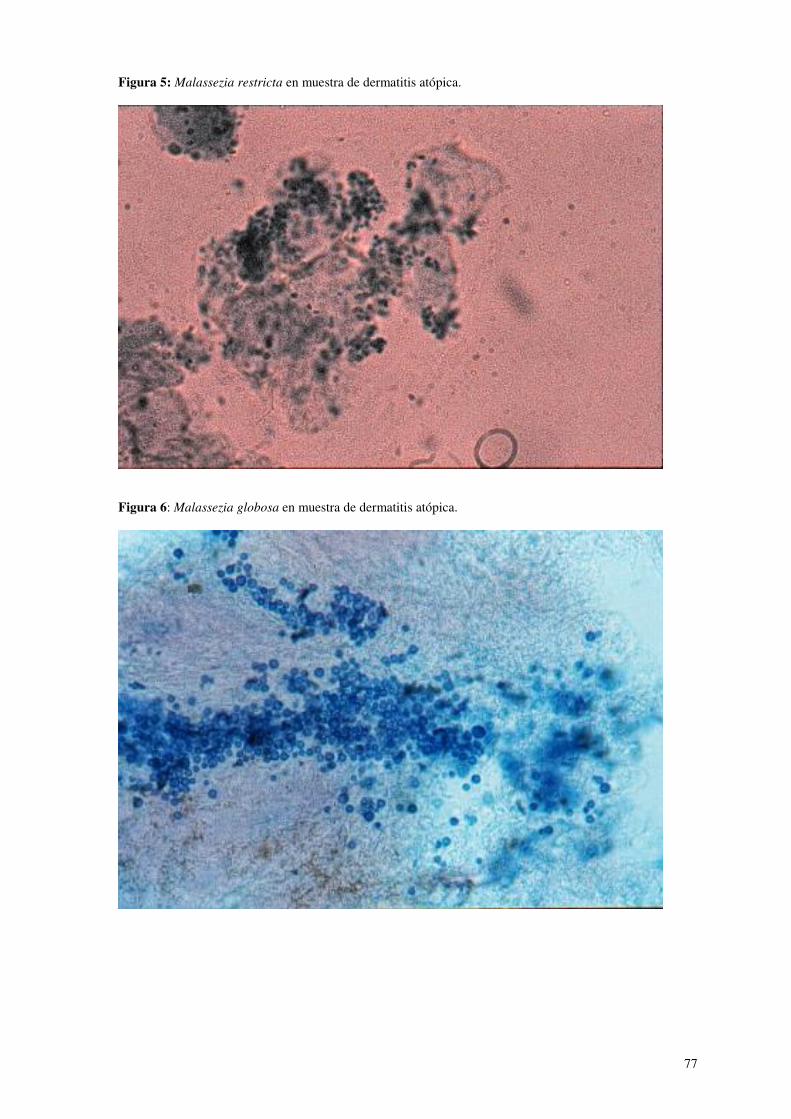
Figura 5: Malassezia restricta en muestra de dermatitis atópica.
Figura 6: Malassezia globosa en muestra de dermatitis atópica.
78
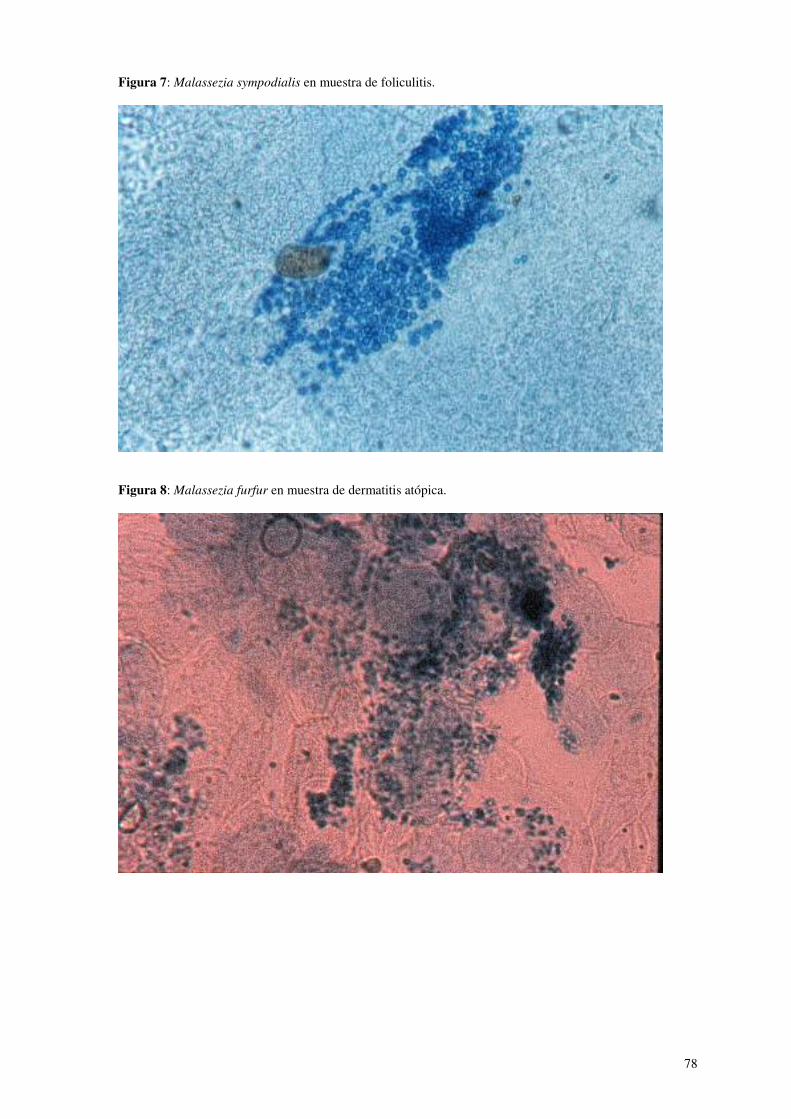
Figura 7: Malassezia sympodialis en muestra de foliculitis.
Figura 8: Malassezia furfur en muestra de dermatitis atópica.
79
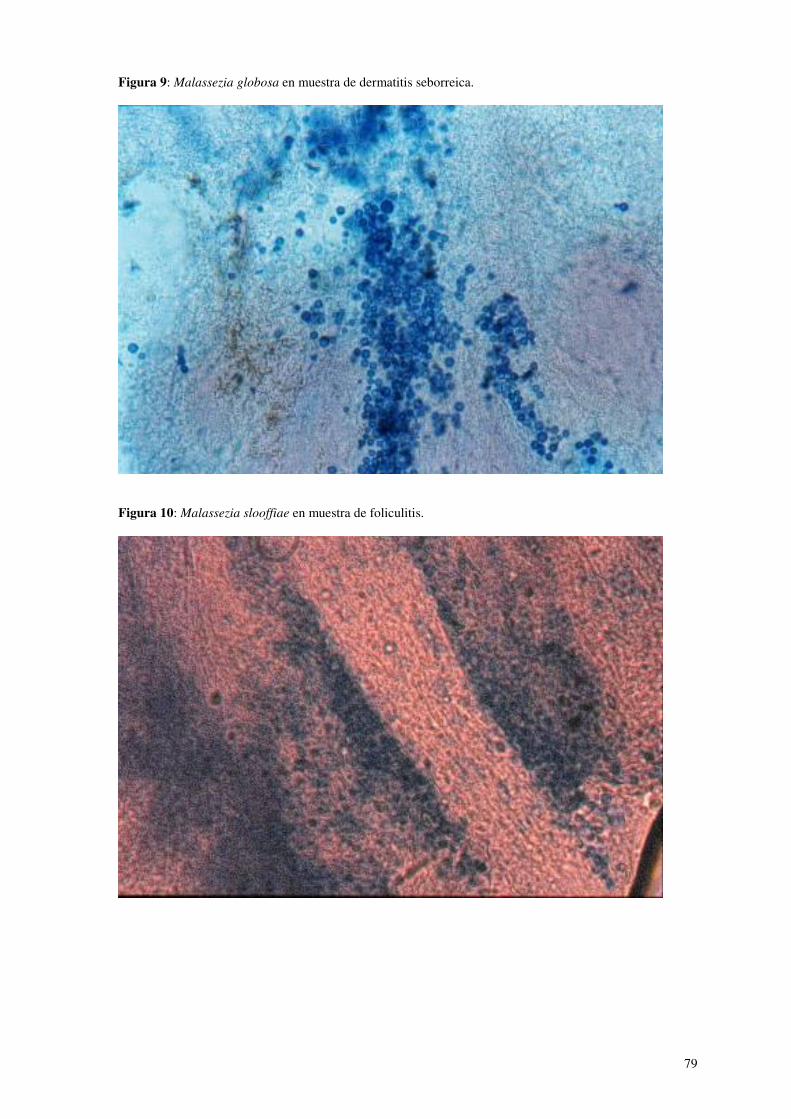
Figura 9: Malassezia globosa en muestra de dermatitis seborreica.
Figura 10: Malassezia slooffiae en muestra de foliculitis.

80
Bibliografía 1. Moreno Giménez JC, 1995. Pitiriasis versicolor. Monografías de Dermatología. Vol VIII, 4, 223-243. 2. Guého E, Midgley G & Guillot J. The genus Malassezia with description of four new species. Antonie
van Leeuwenhoek. 1996; 69: 337-55. 3. Crespo Erchiga V, Ojeda Martos A, Vera Casaño A, Crespo Erchiga A, Sánchez Fajardo F, Guèho E.
Mycology of pityriasis versicolor. J. Mycol. Med. 1999; 9:143-148. 4. Arribi A. Funguemia por levaduras lipofílicas: ¿una rareza o simplemente infravalorada? Enferm. Infecc.
Microbiol. Clin. 1999;17:53-55. 5. Dankner W, Spector S, Flerer J, Davis C. Malassezia funguemia in neonates and adults: complication of
hyperalimentation. Rev Infect Dis. 1987;9:743-753. 6. Marcon MJ, Powell DA. Human infections due to Malassezia spp. Clin Microbiol Rev. 1992;5(2):101-19. 7. Guillot J, Guého E, Lesourd M, Midgley G, Chèvrier G, Dupont B. Identification of Malassezia species.
A practical approach. J Mycol Med. 1996; 6:103-110. 8. Castellani A. Chalmers AJ. Manual of Tropical Medicine. 2nd edition. London, Baillere. Tindall and
Cox. pp 1913 – 1947. 9. Guého E, Boekhout T, Ashbee HR, Guillot J, Van Belkum A, Faergemann J. The role of Malassezia
species in the ecology of human skin and as pathogens. Med. Mycol. 1998, 36, Supplement 1, 220-229. 10. Weidman FD. Exfoliative dermatitis in the Indian rhinoceros (Rinhoceros unicornis), with description of
a new species: Pityrosporum pachydermatis. In: Fox H. ed. Rep. Lab Museum comp Zoo Soc. Philadelphia 1925: 36-45.
11. Midgley G. The diversity of Pityrosporum (Malassezia) yeasts in vivo and in vitro. Mycopathologia 1989; 106:143-153.
12. Cunningham AC, Leeming JP, Ingham E, Gowland G. Differentiation of three serovars of Malassezia
fufur. J Appl Bacteriol 1990; 67:439-446. 13. Ingham E & Cunningham C. Malassezia furfur. J Med Vet Mycol. 1993;31:265-288. 14. Gordon MA. The lipophilic mycoflora of the skin. Invitro culture of Pityrosporum orbiculare n. sp
Mycologia 1951: 43: 524-35. 15. Teun Boekhout, Marga Kamp & Eveline Gueho. Molecular typing of Malassezia species with PFGE and
RAPD 16. González-Cuevas A, Alayeto J, Juncosa T, García-Fructuoso MT, Moreno J, Latorre C. Sepsis neonatal
por Malassezia furfur. Rev Iberoam Micol. 1999;16:157-160. 17. Marimón JM, García-Arenzana JM, Gil A, Paisán L. Infección asociada a catéter por Malassezia furfur en
un niño prematuro. Enferm Infecc Microbiol Clin. 1995;13:572. 18. Redline RW, Dahms BB. Malassezia pulmonary vaculitis in a infant on long-term intralipid theraphy. N
Engl J Med. 1981;305(23):1395-8. 19. Sizun J, Karangawa A, Giroux JD, Masure O, Simitzis AM, Alix D, De Parscau L. Malassezia furfur-
related colonization and infection of central venous catheters. A prospective study in a pediatric intensive care unit. Intensive Care Med. 1994; 20(7):496-9.
20. Midgley G. The lipophilic yeasts: state of the art and prospects. Med Mycol 2000;38:9-16. 21. Canteros C, Soria M, Rivas C, Lee W, López Joffre MC, Rodero L, Perrota D, Körte C, Davel G.
Especies de Malassezia aisladas de patologías de piel en un centro asistencial de la ciudad de Buenos Aires, Argentina. Rev Arg Microbiol 2003;35:156-161.
22. Gupta AK, Kohli Y, Faergemann J, Summerbell RC. Epidemiology of the Malassezia yeast associated with pityriasis versicolor in Ontario, Canada. Med Mycol 2001, 39:199-206.
23. Gupta AK, Kohli Y, Summerbell RC, Faergemann J. Quantitative culture of Malassezia species from different body sites of individuals with or without dermatoses. 2001,39:243-251.
24. Nakabayashi A, Sei Y, Guillot J. Identification of Malassezia species isolated from patients with seborrhoeic dermatitis, atopic dermatitis, pityriasis versicolor and normal subjects. Med Mycol 2000,38:337-341.
25. Kwon-Chung KJ, Bennet JE. Infections caused by Malassezia species. In: Medical Mycology. Philadelphia: Lea and Febiger, 1992:170-182.
26. Giusiano G, Bustillo S, Mangiaterra M, Deluca G. Identificación de especies de Malassezia por PCR-REA. Rev Arg Microbiol 2003,35:162-166.
81
Sertaconazole: updated review of a topical antifungal agent
Alfonso J Carrillo-Muñoz†, G Giusiano, P A Ezkurra and G Quindós †Author for correspondence ACIA, Microbiology Dept, PO Box 10178, E-08080 Barcelona, Spain Tel.: +34 934 297 120 [email protected]
KEYWORDS: dermatophytes, fungi, mycoses, sertaconazole, topical antifungal agent, yeast Sertaconazole is an imidazole-type antifungal agent that has shown considerable in Vitro activity against pathogenic fungi. Various studies carried out in animal models, clinical and toxicologic trials have confirmed the value of sertaconazole in the topical treatment of superficial mycoses in dermatology and gynecology. After several years of clinical experience in the topical treatment of dermatophytosis and Tinea versicolor, the substance has been approved for gynecologic candidiasis in Europe. Sertaconazole has a wide action spectrum that includes yeasts, dermatophyte fungi and it is also active against bacteria, mainly Gram-positive cocci, making it highly efficient in the treatment of polymicrobial infections. The recent approval of the molecule by the US Food and Drug Administration, and the appearance of a new formulation of sertaconazole for the treatment of onychomycoses on a weekly administrative basis are all data relevant to the process of marketing the product. Expert Rev. Anti Infect. Ther. 3(3), xxx–xxx (2005) The development of new antifungal agents has been marked by increasing pathogenicity of many fungal micro-organisms, the most important being emerging pathogens, the reduced sensitivity to traditional antifungal agents and the seriousness of many mycoses. These facts are due to the increase in the population at risk, including AIDS patients, and now with growing importance, receptors of transplanted organs with hematologic diseases and other immunosuppressed persons. From an epidemiologic point of view, the changes taking place in these types of infections have been brought about by new medical treatments for at-risk populations, as well as by changes in the handling of patients, such as the introduction of new systems of cell transplantation, progress in the practice of organ transplants, or the use of new immunosuppressant agents and antimicrobial prophylaxis strategies. Two factors have heavily influenced the impact of invasive mycoses; the progress of base pathologies, and insufficient diagnostic methods and tools that do not allow detection of the infection in its inicial stages. Fungal infections continue to be one of the major causes of death in patients being treated for neoplasia. These immunocompromised patients are frequently infected by fungi of different species belonging to the Candida, Aspergillus or Cryptococcus genera as well as other opportunistic pathogenic fungi. The introduction of highly active antiretroviral therapy (HAART) has brought about a significant decline in the incidence of opportunistic infections among AIDS patients in developed countries. However, the availability of HAART is very limited in underdeveloped countries, with a high rate of HIV infection and opportunistic fungal infections, such as oropharyngeal candidiasis, cryptococcosis, histoplasmosis, penicilliosis or pneumocystosis, which are now an important cause of morbidity and mortality. The advances made in surgical techniques and immunosuppressant treatments have decreased the incidence of invasive candidiasis in receptors of transplanted organs with a high risk of infection by Candida, but at the same time there has been an increase in the frequency of infection by species other than Candida albicans as a pathogen among the Candida genus. The increased use of very aggressive immunosuppressant agents in receptors of the hematopoietic cell transplants has meant a greater incidence of invasive mycoses caused by filamentous fungi (such as aspergillosis, fusariosis or zygomycoses) among these pathogens. Unfortunately, antifungal agents must act against micro-organisms that have metabolic pathways similar to those of the host cell, and this means that the actions with greatest effectiveness are those that exploit asymmetric reactions, that is those that only damage the cell viability of the fungus. This effect is sufficient to reduce the fungal population to concentrations manageable by the host’s different functional defense mechanisms.
82
Many of the required advantages of an antifungal agent, such as wide action spectrum and in vitro and in
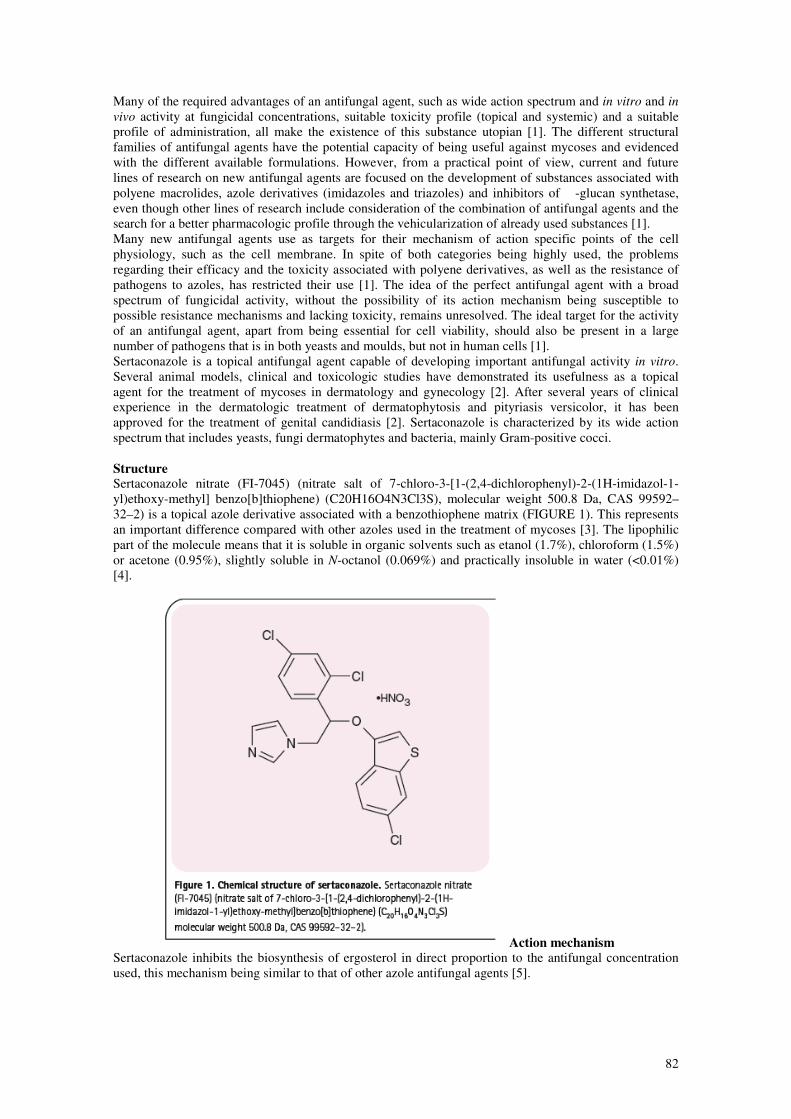
vivo activity at fungicidal concentrations, suitable toxicity profile (topical and systemic) and a suitable profile of administration, all make the existence of this substance utopian [1]. The different structural families of antifungal agents have the potential capacity of being useful against mycoses and evidenced with the different available formulations. However, from a practical point of view, current and future lines of research on new antifungal agents are focused on the development of substances associated with polyene macrolides, azole derivatives (imidazoles and triazoles) and inhibitors of �-glucan synthetase, even though other lines of research include consideration of the combination of antifungal agents and the search for a better pharmacologic profile through the vehicularization of already used substances [1]. Many new antifungal agents use as targets for their mechanism of action specific points of the cell physiology, such as the cell membrane. In spite of both categories being highly used, the problems regarding their efficacy and the toxicity associated with polyene derivatives, as well as the resistance of pathogens to azoles, has restricted their use [1]. The idea of the perfect antifungal agent with a broad spectrum of fungicidal activity, without the possibility of its action mechanism being susceptible to possible resistance mechanisms and lacking toxicity, remains unresolved. The ideal target for the activity of an antifungal agent, apart from being essential for cell viability, should also be present in a large number of pathogens that is in both yeasts and moulds, but not in human cells [1]. Sertaconazole is a topical antifungal agent capable of developing important antifungal activity in vitro. Several animal models, clinical and toxicologic studies have demonstrated its usefulness as a topical agent for the treatment of mycoses in dermatology and gynecology [2]. After several years of clinical experience in the dermatologic treatment of dermatophytosis and pityriasis versicolor, it has been approved for the treatment of genital candidiasis [2]. Sertaconazole is characterized by its wide action spectrum that includes yeasts, fungi dermatophytes and bacteria, mainly Gram-positive cocci. Structure Sertaconazole nitrate (FI-7045) (nitrate salt of 7-chloro-3-[1-(2,4-dichlorophenyl)-2-(1H-imidazol-1-yl)ethoxy-methyl] benzo[b]thiophene) (C20H16O4N3Cl3S), molecular weight 500.8 Da, CAS 99592–32–2) is a topical azole derivative associated with a benzothiophene matrix (FIGURE 1). This represents an important difference compared with other azoles used in the treatment of mycoses [3]. The lipophilic part of the molecule means that it is soluble in organic solvents such as etanol (1.7%), chloroform (1.5%) or acetone (0.95%), slightly soluble in N-octanol (0.069%) and practically insoluble in water (<0.01%) [4].
Action mechanism Sertaconazole inhibits the biosynthesis of ergosterol in direct proportion to the antifungal concentration used, this mechanism being similar to that of other azole antifungal agents [5].
83
However, due to its mixed structure, sertaconazole is capable of causing direct damage to the C. albicans
cell membrana [5–7]. This second, and very important, effect is the basis of its fungicidal effect against C.
albicans [5–7]. The special structure of the cell membrane of fungi is based on the properties of ergosterol, which is capable of regulating the internal fluidity of the membrane. The interaction at some stage of the biosynthetic route of ergosterol may cause a reduction of the levels of this compound and, as a result, affect the integrity of the cell. An intermediary of the biosynthesis of ergosterol (lanosterol) is produced by the interaction of azole compounds with the cytochrome P450 complex (in mono-oxygenase or hydroxylase 14-�-demethylase enzymes). In general, azole derivatives cause inhibition of the biosynthesis of ergosterol and inhibition of filamentation in C. albicans, as well as in some cases, such as with sertaconazole (direct damage to the cell membrane) [7]. The bond between the azole molecule and the iron atom of the hemo group leads to inactivation of the enzyme and the resulting accumulation of lanosterol that damages cellular architecture and membrane fluidity and permeability. Any increase in cell permeability causes the loss of intracellular ATP, destruction of the cytoskeleton and lysis of the cell organelles, while at the same time reducing the number of viable cells by up to 90%. The result of this is the fungicidal effect of sertaconazole when cells are exposed to high concentrations of this drug [5,7]. Under these same conditions, it is also posible to detect an interruption in the process of the formation of hyphae, thus preventing invasion of the host tissue [5,7]. Antifungal action spectrum The relevant antifungal activity of sertaconazole has already been demonstrated in different preclinical studies against a broad spectrum of pathogenic fungi, including yeasts, fungi dermatophytes, opportunistic filamentous fungi and Grampositive bacteria (Streptococcus and Staphylococcus) and Tricomonas spp. (TABLE 1) [8]. The species of fungi included potential producers of dermatomycoses, dermatophytosis and genital candidiasis. A complete comparison of the minimum inhibitory concentrations, which would enable establishing the antifungal power of the substance in vitro is complex, as some of the different results were obtained prior to the appearance of the Clinical and Laboratory Standards Institute (CLSI/NCCLS) documents, which established standard experimental conditions and variables. Nevertheless, it can be deduced from data that there is a wide activity spectrum against pathogenic fungi, an activity that takes place at concentrations far below those reached after the topical application of sertaconazole (TABLE 1). Antifungal activity in vitro The in vitro antifungal activity of sertaconazole has been widely demonstrated by various authors using standard and nonstandard methods under different experimental conditions [10] against pathogenic yeasts [11–16], including Malassezia spp. [17], dermatophyte fungi [12,18–20] and opportunistic filamentous fungi [6,21]. Susceptibility testing enables an excellent statistical base to be obtained indicating the tendency of a substance towards activity or inactivity and also serves as a therapeutic guide when making clinical decisions regarding the prediction of susceptibility or resistance of the isolated strain, the selection of the most clinically active antifungal agents, or indicating the reasons for therapeutic failure on the basis of microbiologic criteria [22,23]. The fungicide activity of sertaconazole has its onset at concentrations of 8–16 µg/ml [24], whereas at lower concentrations, in ranges equivalent to clotrimazole and miconazole, it develops a fungistatic action mechanism [6,13,24,25]. This antifungal activity of sertaconazole is higher than that of other imidazole derivatives, such as bifonazole, econazole or fluconazole [11–13,15,19,25,26]. In the absence of adverse effects as serious as those observed with other imidazoles such as clotrimazole, miconazole, bifonazole or ketoconazole, in comparison, sertaconazole is more active against opportunistic filamentous fungi than miconazole [6,24]. Sertaconazole also proved to be more active against resistant strains of dermatophytes than fluconazole, a triazole derivative used by oral route in the treatment of some dermatophytoses [19]. Sertaconazole is very active against this group of pathogenic fungi with partial inhibition being detected at concentrations below 0.04 µg/ml [6,18,19]. This excellent in vitro antifungal activity of sertaconazole is completed by a low percentage of resistances, placing it in the same range as other topical antifungal agents such as clotrimazole and tioconazole, and lower than those obtained for amphotericin B, itraconazole, fluconazole, econazole, miconazole or ketoconazole [25,26]. On the other hand, it has not been possible to obtain evidence of induced resistance in vitro by exposure of C. albicans and Candida tropicalis to subinhibitory concentrations of sertaconazole [8]. Antibacterial activity in vitro Sertaconazole has demonstrated in vitro antibacterial activity against Staphylococcus aureus, Staphylococcus epidermidis, Streptococcus pyogenes, Streptococcus agalactiae, Listeria monocytogenes,
84
Gardnerella spp. and other bacteria involved in mixed infections. The activity of sertaconazole against Gram-positive bacteria was described at concentrations below 0.97 µg/ml and considered to have in vitro
therapeutic value [8]. Animal models Some experimental models in animals (mouse and guinea pig) have been used to prove the usefulness and efficacy of topical sertaconazole at doses of 2% against vaginal candidiasis and dermatophytosis, when tested in comparison with miconazole (2%) in different treatment regimes [24,27,28]. In the animal model of dermatophytosis, sertaconazole has a proven efficacy after 12 days of treatment similar to that obtained with miconazole. The therapeutic improvement of the clinical and microbiologic symptoms was better for the sertaconazole group treated during 3 days. The same occurred with the model of vaginal candidiasis but with an even better prophylactic and curative effect [24,28]. In the latter model, there was a greater reduction in the cell count of yeasts with the vaginal administration of sertaconazole (97.7 and 77.5% with sertaconazole and miconazole respectively) promising a good clinical efficacy [28]. Clinical efficacy
Anti-inflammatory effect Sertaconazole has been shown to have anti-inflammatory activity when administered at a dose of 2% [29]. This effect is useful in the treatment of some inflammatory forms of dermatophytoses. Dermatology (dermatophytoses & other cutaneous mycoses) A comparison between different clinical studies to establish the efficacy of antifungal agents is difficult due to the differing numbers of patients assessed in these studies. However, it is possible to review comparative multicentric clinical studies between sertaconazole and other azole derivatives (miconazole, sulconazole, clotrimazole, bifonazole or ketoconazole) that support the clinical efficiency of sertaconazole against superficial mycoses in all its different formulations. The cream formulation was effective in a double-blind study carried out with parallel groups of patients suffering from different dermatophytoses (tinea cruris, tinea corporis, tinea pedis, tinea manuum, tinea barbae among other locations). The efficacy of the cream formulation of sertaconazole in a Multicenter Phase III, randomized and comparative study with miconazole in patients infected by Microsporum canis, C. albicans and other dermatophyte fungi, reached ranges of 98.3 versus 94.3%, respectively, after 4 weeks of treatment. This was statistically significant [30]. The ranges of clinical cure for sertaconazole were accompanied by similar mycologic cure rates – being the percentage of therapeutic failure, recurrence or relapses being very low (sertaconazole 4.4 vs. miconazole 11.9% of relapses at 35 days alter beginning the treatment, p < 0.001) [31]. Similar results were obtained for a comparison of the clinical efficacy of sertaconazole with sulconazole, clotrimazole or bifonazole for the treatment of patients suffering from cutaneous candidiasis and dermatophytosis [32]. Apart from its antifungal activity, some properties of sertaconazole, such as reduction of the severity of erythema, reduction of desquamation, pruritus or the formation of pustules, were also useful when determining the clinical cure. The good results obtained with sertaconazole in the treatment of superficial mycoses were previously described in Phase II studies, which also enabled characterizing a high safety profile in a group of 20 patients [31–34]. The effectiveness of the gel formulations (2%) of sertaconazole compared with ketoconazole was demonstrated against seborrheic dermatitis. Clinical signs and the presence of fungal elements were reduced in 61.1% of the 60 patients studied whereas for ketoconazole this occurred in 52.6% of patients [2]. Clinical and mycologic improvement of various superficial infections was achieved with different formulations of sertaconazole in comparison with other compounds belonging to other chemical families of antifungal agents. Furthermore, its efficacy was demonstrated in children after the application of single doses of the 2% cream formulation of sertaconazole [35]. Gynecology (vaginal candidiasis)
In gynecologic mycoses, such as candidal vulvovaginitis, the excellent efficacy of sertaconazole was also demonstrated in comparative studies with clotrimazole and econazole [2,36,37]. The effectiveness of sertaconazole was comparable with that of clotrimazole in terms of clinical and mycologic cure of the 582 patients studied, reaching a cure rate higher than 80% in both groups at 14 days after the application of a single dose of 500 mg as a vaginal tablet. Both antifungal agents were well tolerated with the adverse effect of greatest frequency being the appearance of pruritus and erythema ahead of irritation, sensitization, edema, rubor, leukorrhea and maceration [2].

85
Sertaconazole and econazole demonstrated similar rates of efficacy and safety, but the percentage of recurrence was coger among patients treated with sertaconazole [36]. In a comparative study between the application of a single intravaginal dose in 369 patients suffering from vaginal candidiasis (183 sertaconazole; 186 econazole), the clinical and mycologic cure rate was 70.8 and 64.7%, respectively, for sertaconazole and econazole, after 7 days of treatment and the clinical cure rates were 71.6 versus 64.2%, respectively, for each of the treatments. In spite of these results being similar for both imidazole antifungal agents, it was posible to observe statistically significant differences in favor of sertaconazole in regard to the relapse rates (19.8 and 32.7%, respectively, after 30 days; p = 0.035), a fact probably related to the fungicide capacity of sertaconazole. No differences were found between both medicinal products for local tolerability. Another study evaluated the differences between the treatment of vulvovaginal candidiasis with single intravaginal doses of 300 mg (applied at night) and the combined intravaginal therapy of a single dose of 300 mg together with topical application of sertaconazole cream (2%) to the vulva during 7 days (combined treatment) [37]. The results demonstrated an efficacy of close to 99% with regard to clinical improvement in all patients, but the cure was faster in the combined treatment group of pessary plus cream than in the group of pessary alone at 7 days (76 vs. 68%, respectively). Furthermore, annoying symptoms such as pruritos disappeared sooner in the combined treatment group [37]. Safety profile Acute toxicity studies The acute toxicity of sertaconazole was determined after the administration of single doses by oral, subcutaneous and intraperitoneal route in rats and mice with the median lethal dose (LD50) being higher than 8000 mg/kg in all cases. Due to its reduced absorption, administration is safe even in the event of accidental overdose or ingestion [38]. Subacute toxicity & maximum tolerated dose Studies of repeated administration over a period of 28 days with subacute oral and dermal doses of 50, 150 and 300 mg/kg and maximum tolerable doses on a geometric progression of 50, 75, 112.5, 168 and 250 mg/kg of sertaconazole revealed a reduced number of toxic effects that are not possible to reproduce after the administration of single doses [39]. No histopathologic changes were found in any of the cases [39]. Chronic toxicity studies after oral administration In this regard, the effects produced by sertaconazole are also common to other azole derivatives used for the treatment of mycoses, and were detected at a dose of 50 mg/kg in chronic toxicity studies after repeated and sustained administration by oral route doses of 50, 150 and 300 mg/kg in rats and ferrets [40]. The accumulative effect, which did not produce any associated mortality, was observed in the group treated with bifonazole (10 mg/kg), ketoconazole (60 mg/kg) and miconazole (100 mg/kg). There was a low increase in body weight in animals treated with 300 mg/kg of sertaconazole over 5 weeks (rats) and 150 mg/kg over 11 weeks (ferrets). The histopathologic findings are similar to those produced by other imidazoles and consisted of changes in the pattern of microvacuolization in the hepatocyte cytoplasm related to the induction of microsomal enzymes [40]. The inhibitory effect on the synthesis of adrenal steroidal hormones, also common to other azole antifungal agents and observed after the administration of very high doses, produces changes in the ovaries of treated females (ferrets) and ductal hyperplasia of the mammary gland and endometrium [40]. The effects, although common to other imidazoles, were found at higher concentrations of sertaconazole and this its safety profile is higher, requiring doses of more than 50 mg/kg [40]. The data available for miconazole and clotrimazole show a worse toxicity profile for these substances [40]. In any case, the administration of sertaconazole is not associated with any necrogenic, inflammatory or degenerative changes [40]. Toxicity studies in reproduction Compared with ketoconazole, bifonazole or miconazole, the low toxicologic risk associated with the administration of sertaconazole has been demonstrated by teratologic studies in rats, rabbits and also in peri- and postnatal rats [41].

86
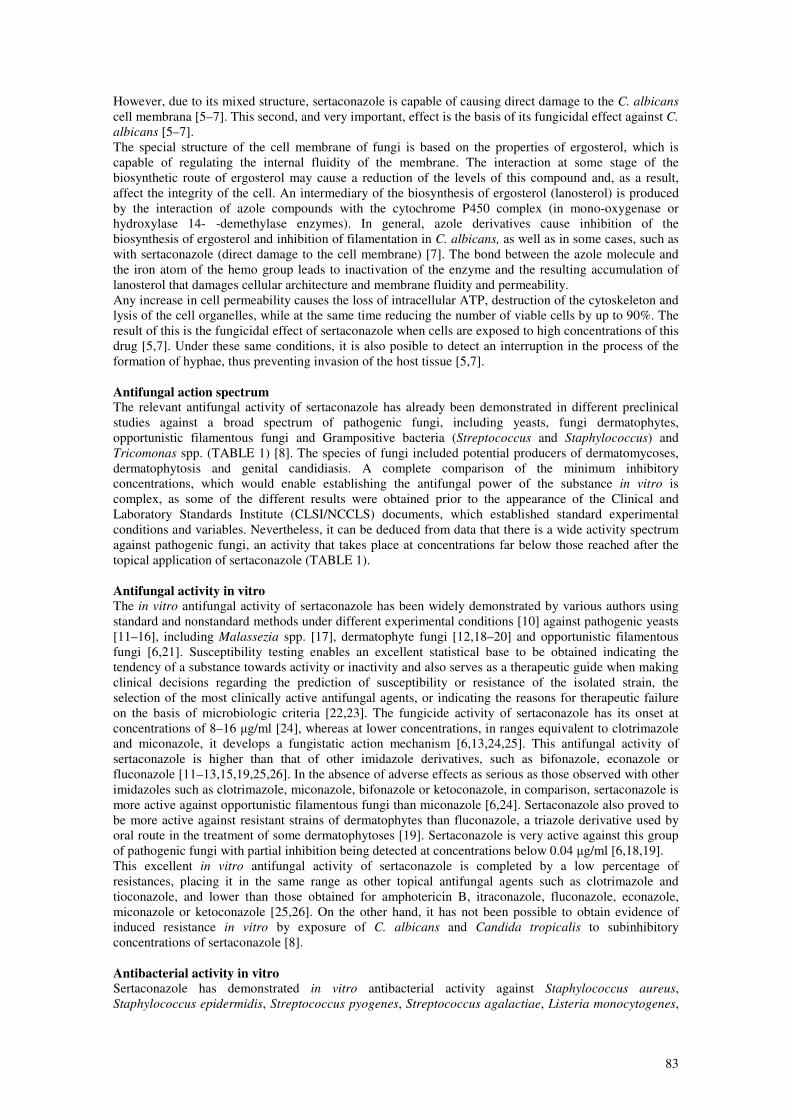
Genotoxicity There was no evidence of induction of signs of promutagenicity, mutagenicity, clastogenicity or interference with the process of chromosomal segregation caused by DNA damage. Neither have genotoxicity studies carried out with sertaconazole demonstrated any increase in the frequency of bacterial retromutation or letal mutations in spermatozoa or spermatids [42]. Skin tolerance & phototoxicity It is possible to state that there is no risk of phototoxicity alter the administration of the 2% cream formulation of sertaconazole in guinea pigs [43]. Trials carried out to detect skin tolerante demonstrated the absence of any irritation [43]. This jeans that sertaconazole may be administered safely without the posible existence of degradation by-products caused by direct exposure to sunlight [43,44]. Sertaconazole does not induce contact dermatitis at therapeutic doses (2% cream) [44,45], although allergic contact dermatitis to sertaconazole was observed in patients who had already presented sensitivity to miconazole and econazole [47]. Pharmacokinetics Sertaconazole penetrates the horny layer of the skin where some pathogenic fungi are capable of developing their effect, and therapeutic concentrations may be found there during a long period of time, which is of interest in clinical practice. However, such high concentrations of sertaconazole cannot be reached in the lower layers, thus avoiding the potential risk of systemic absorption. The concentrations found in plasma in a preclinical study with radioactively marked sertaconazole were below 0.011% 5 h after beginning application of 2% cream to the skin [48]. The cutaneous absorption in humans has been described after topical application at increasing doses [44]. The results of this study showed that the percentage of cutaneous absorption at 24 h after the application was 72% of the dose applied. Analysis of plasma samples did not reveal concentrations of sertaconazole that were detectable at a quantitation limit of 25 ng/ml. No hematologic, cardiac or body temperature changes were observed at 13 days, neither was there any alteration of the blood testosterone levels, thus proving its good safety profile [44]. The antifungal agent is retained in the skin for long periods of time, reaching antifungal concentrations at 72 h after topical applications of once or twice a day [49]. The different vaginal forms in which sertaconazole is available (tablets, pessaries and cream) for the treatment of vulvovaginitis make it possible to reach concentrations above those required to inhibit the development of different species of the genus Candida spp. with a dose of 300 or 500 mg. In addition, these concentrations are maintained in vaginal secretion for several days after a single administration without there being any systemic absorption, thus resolving its necessary presence and persistence in the vaginal mucous membrane [50]. Some of the main pharmacokinetic parameters of sertaconazole in preclinical studies are shown in (TABLE 2) [51]. The fecal and renal routes are the main routes of elimination of the product (61 and 4%, respectively, for endovenous administration; 30 and 0.4% for administration and 17 and 0.6% for the skin) [48]. Tolerability studies Tolerability studies for sertaconazole carried out using animal models and healthy human volunteers showed the absence of evidence of adverse effects associated with the administration of total amounts of 98 g of antifungal agent during 13 days (1–16 g each) [44]. It was also shown with healthy human volunteers that other therapeutically available antifungal agents such as econazole, ketoconazole, bifonazole, clotrimazole and miconazole, produced adverse reactions consisting of the formation of vesicles after the application of their comercial forms [44]. There were no differences between sertaconazole and placebo in regard to photosensitivity [43].
87
Market Sertaconazole is available throughout the world in different dermal and gynecologic formulations. The former include: topical gel, 2% topical cream (recently launched in the USA Ander the name Ertaczo®), powder and solution. In gynecology: pessaries, vaginal cream and vaginal tablets. The dose of sertaconazole active principle contained in each unit is considered sufficient for the complete and individual treatment of each patient. Evolution During the above-mentioned period (1996–2001), there were reports of a reduced percentage of possible adverse effects to treatment in different clinical formulations of sertaconazole (0.5% per 100,000 patients). A total of 88.7% of these reported adverse effects were for use of the 2% cream and consisted of erythema, exudation, urticaria, maculopapular rash, pruritus, contact dermatitis, burning, allergy, flush, wetting, vesication, swelling, pain, hyperpigmentation and decoloration. These adverse effects are the same as those observed after the application of other azole derivatives. Studies have been carried out on the new formulations of sertaconazole to complement the range of infections with the treatment of onychomycoses [52]. The in vitro antifungal activity shown against dermatophyte fungi, producers of infections in the nails, and the higher than inhibitory concentrations reached in the nails, are the basis for the development of a formulation for onychomycoses consisting of adhesive patches that contain concentrations of 1.65 mg/cm2 of sertaconazole. These patches, with an application schedule of one per week during periods of 6 or 12 months, could produce concentrations in the nails of close to 100–150 ng/mg alter the first 2–6 weeks. These concentrations are above the minimum inhibitory concentrations for pathogenic fungi of the nails. Data on the prevalence of fungal infections in the nails and the ease with which the patient could comply with the treatment could be promising in the absence of formulations of similar characteristics of other antifungal agents with a similar antifungal profile and pharmacologic properties, and in this way, be advantageous in front of the oral treatment in some dermatophytoses. Expert opinion Although some topical antifungal agents are available for the management of superficial fungal infections, sertaconazole offers an antifungal activity that occurs at concentrations that are reached and exceeded after topical administration. Some other azole antifungal agents have an affinity for their targets in some fungal pathogens such as dermatophyte fungi lower than that of sertaconazole, and the double mode of action of sertaconazole could be an advantage. Dermal formulation of sertaconazole is retained for a long time in stratum corneum and other sertaconazole qualities such as its anti-inflammatory activity, good tolerance, antibacterial activity and safety profile are helpful for the management of superficial fungal or mixed infections. Successful results are obtained with sertaconazole termal formulations in clinical trials confirming the good in vitro data as predictive for clinical outcome. This contrasts with the longterm therapy profile and the low correlation of the in vitro and clinical outcome reached with other antifungal agents for the management of superficial mycoses (candidosis or dermatophytoses). Frequency of recovering of resistant strains is extremely low in in vitro tests compared with other azole derivatives. Five-year view There is a relative shortage of antifungal agents for the management of fungal infections. Currently, a formidable technical challenge is faced by the pharmaceutical industry in the discovery of new antifungal

88
targets and the development of effective antifungal agents. The number of new antifungal agents at different stages of the development pipeline is high in clear contrast to the fact that during more than 40 years, amphotericin B has been almost the only available therapy for invasive mycoses. Nevertheless, great efforts are now underway to develop investigational programs in azole derivatives for superficial mycoses by topical administration. New trends are focused among the important areas of investigation in antifungal agents, which are: the development of new azole or polyene derivatives, development of new formulations of old antifungal agents, investigation of new chemical structures including those having new genomic targets, and antifungal combination therapy or adjunctive immunotherapies and immune-reconstitution. Although the need for new drugs is obvious, progress in this area is slow and unpredictable. Targets may abound, but the difficulty in translating those targets into meaningful new drugs is well illustrated by the paucity of new classes of compounds over the past 20 years [1]. In this manner, sertaconazole is one of the latest appeared imidazole members. Its wide fungal spectrum, antifungal activity, safety toxicologic profile and pharmacokinetics and mixed mode of action are useful in comparison with other imidazole antifungal agents. Onychomycoses are currently treated by lacquer formulations or their long therapies requiring daily administration. Antifungal compliance is very difficult for infected patients (<51%). Epidemiologic data revealed a significative prevalence of the infection, a high clinical failure over the 25%, due to problems in nail penetration and retention times of active antifungal concentrations. Indeed, some patients are treated with oral therapy (clinical failure or extense affected areas involving nail matrix) with antifungal drugs with lower activity against fungal nail pathogens, without no reduction times of dosage and with more severe reported adverse effects compared with the topical administration of sertaconazole. On the basis of criteria, sertaconazole could be well accepted. By now, is also promising the interest of different companies to license the product. References Papers of special note have been highlighted as: • of interest •• of considerable interest 1. Carrillo-Muñoz AJ, Quindós G, Lopez-Ribot JL. Current developments in antifungal agents:
present and future. Curr.Med. Chem. Anti Infect. Agents. 3(4), 297–323 (2004). 2. Torres J, Márquez M, Camps F. Sertaconazole in the treatment of mycoses: from dermatology to
gynecology. Int. J.Gynaecol. Obstet. 71(Suppl. 1), S3–S20 (2000). 3. Raga MM, Moreno-Manas M, Cuberes MR, Palacín C, Castello JM, Ortíz JA. Synthesis and
antimycotic activity of (benzo[b]thienyl)methyl ethers of 1-(2,4-dichlorophenyl)-2-(1H-imidazol-1-yl)-ethanol and of (Z)-1-(2,4-dichlorophenyl)-2-(1H-imidazol-1-yl)ethanone oxime.Arzneimittelforschung 42(5A), 691–694 (1992).
4. Albet C, Fernández JM, Sacristán A, Ortiz JA. Physicochemical properties, analytical determinations and stability of sertaconazole nitrate. Arzneimittelforschung 42(5A), 695–698 (1992).
5. Agut J, Palacín C, Sacristán A, Ortíz JA. Inhibition of ergosterol synthesis by sertaconazole in Candida albicans. Arzneimittelforschung 42(5A), 718–720 (1992).
6. Drouhet E, DuPont B. In vitro antifungal activity of sertaconazole. Arzneimittelforschung 42(5A), 705–710 (1992).
7. Agut J, Palacín C, Salgado J, Casas E, Sacristán A, Ortíz JA. Direct membranedamaging effect of sertaconazole on Candida albicans as a mechanism of its fungicidal activity. Arzneimittelforschung 42(5A), 721–724 (1992).
8. Palacín C, Sacristán A, Ortiz JA. In Vitro activity of sertaconazole. Arzneimittelforschung 42(5A), 699–705 (1992).
9. Figueras MJ, Cano JF, Guarro J. Ultrastructural alterations produced by sertaconazole on several opportunistic pathogenic fungi. J. Med. Vet Mycol. 33(6), 395–401 (1995).
10. Carrillo-Munoz AJ, Tur-Tur C, Hernández-Molina JM. Comparación de dos métodos para el estudio de la sensibilidad in vitro de sertaconazol a levaduras de origen clínico. Rev. Esp.
Quimioter. 12(1), 58–63 (1999). 11. Carrillo-Munoz AJ, Tur-Tur C, Bornay- Llinares FJ, Arévalo P. Comparative study of the in vitro
antifungal activity of bifonazole, naftifine and sertaconazole against yeasts. J. Chemother. 11(3), 187–190 (1999).
89
12. Carrillo-Munoz AJ, Tur-Tur C. Comparative study of antifungal activity of sertaconazole, terbinafine, and bifonazole against clinical isolates of Candida spp., Cryptococcus neoformans and dermatophytes. Chemotherapy 43(6), 387–392 (1997).
13. Carrillo-Munoz AJ, Tur C, Torres J. In Vitro antifungal activity of sertaconazole, bifonazole, ketoconazole, and miconazole against yeasts of the Candida genus. J. Antimicrob. Chemother.
37(4), 815–819 (1996) 14. Martín-Mazuelos E, Aller AI, Morilla D, Montero O. Antifungal activity of sertaconazole in vitro
against clinical isolates of Candida spp. Chemotherapy 42(2), 112–117 (1996). 15. Carrillo-Muñoz AJ, Torres-Rodríguez JM. In vitro antifungal activity of sertaconazole, econazole,
and bifonazole against Candida spp. J. Antimicrob. Chemother. 36(4), 713–716 (1995). 16. Carrillo-Muñoz AJ, Brió S, Càrdenes D, Bornay-Llinares F. Sertaconazol. Actividad antifúngica
frente a levaduras de interés clínico. Dermatología Peruana. 1, 9–12 (2001). 17. Palacín C, Tarragó C, Ortíz JA. In Vitro activity of sertaconazole against Malassezia furfur and
pachydermatis in different culture media. Methods Find. Exp. Clin. Pharmacol. 20(6), 451–455 (1998).
18. Carrillo-Munoz AJ, Fernández-Torres B, Guarro J. In vitro antifungal activity of sertaconazole against 309 dermatophyte clinical isolates. J. Chemother. 15, 555–557 (2003).
19. Carrillo-Munoz AJ, Fernández-Torres B, Cardenes DC, Guarro J. In vitro activity of sertaconazole against dermatophyte isolates with reduced fluconazole susceptibility. Chemotherapy 49(5), 248–251 (2003).
20. Carrillo-Muñoz AJ, Tur C, Estivill D, Torres JM, Estivill D. In vitro antifungal activity of sertaconazole and bifonazole against dermatophytes. J. Mycolog. Med. 5, 235–238 (1995).
21. Torres JM, Carrillo-Muñoz JM, Madrenys-Brunet N. Minimal inhibitory concentrations of sertaconazole, miconazole and clotrimazole on 14 strains of Scopulariopsis brevicaulis isolated from onychomicosis. J. Mycolog. Med. 3, 225–228 (1993).
22. Espinel-Ingroff A. In vitro antifungal susceptibility methods and clinical applications of antifungal resistance. J. Mycol. Med. 38, 293–304 (2000).
23. Odds FC. Should resistance to azole antifungals in vitro be interpreted as predicting clinical non-response? Drug Resist. Update 1, 11–15 (1998).
24. Palacín C, Sacristán A, Ortíz JA. In Vitro comparative study of the fungistatic and fungicidal activity of sertaconazole and other antifungals against Candida albicans. Arzneimittelforschung
42(5A), 711–714 (1992). 25. Palacin C, Tarragó C, Agut J, Guglietta A. In vitro activity of sertaconazole, fluconazole,
ketoconazole, fenticonazole, clotrimazole and itraconazole against pathogenic vaginal yeast isolates. Methods Find. Exp. Clin. Pharmacol. 23(2), 61–64 (2001).
26. Carrillo-Munoz AJ, Brió S, Quindos G, Palacin C, Guglietta A, Espinel-Ingroff A. Sertaconazole: in vitro antifungal activity against vaginal and other superficial yeast isolates. J. Chemother. 13(5), 555–562 (2001).
27. Palacín C, Sacristán A, Ortíz JA. In vivo activity of sertaconazole in experimental candidiasis in the mouse. Drugs Exp. Clin. Res. 16(9), 469–473 (1990).
28. Palacín C, Sacristán A, Ortíz JA. In vivo activity of sertaconazole in experimental dermatophytosis in guinea-pigs. Arzneimittelforschung 42(5A), 714–718 (1992).
29. Agut J, Tarrida N, Sacristán A, Ortíz JA. Anti-inflammatory activity of topically applied sertaconazole nitrate. Methods Find. Exp. Clin. Pharmacol. 18(4), 233–234 (1996).
30. Alomar C, Bassas S, Casas M et al. Multicentre double-blind trial on the efficacy and safety of sertaconazole 2% cream in comparison with miconazole 2% cream on patients suffering from cutaneous mycoses. Arzneimittelforschung 42, 767–773 (1992).
31. Nasarre J, Umbert P, Herrero E et al. Therapeutic efficacy and safety of the new antimycotic sertaconazole in the treatment of Pityriasis versicolor. Arzneimittelforschung 42(5A), 764–767 (1992).
32. Fonseca et al. Evaluación de la eficacia y seguridad de Sertaconazol en crema en aplicación única diaria en el tratamiento de las dermatomicosis. Piel 12, 183–188 (1997).
33. Pedragosa R, González B, Martín M et al. Therapeutic efficacy and safety of the new antimycotic sertaconazole in the treatment of cutaneous dermatophytosis. Arzneimittelforschung 42(5A), 760–763 (1992).
34. Umbert P, Nasarre J, Bello A et al. Phase II study of the therapeutic efficacy and safety of the new antimycotic sertaconazole in the treatment of superficial mycoses caused by Candida albicans. Arzneimittelforschung 42(5A), 757–760 (1992).
35. Van Esso D, Fajo G, Losada I et al. Sertaconazole in the treatment of pediatric patients with cutaneous dermatophyte infections. Clin. Ther. 17(2), 264–269 (1995).
90
36. Dellenbach P, Thomas JL, Guerin V, Ochsenbein E, Contet-Audonneau N. Topical treatment of vaginal candidosis with sertaconazole and econazole sustainedrelease suppositories. Int. J.
Gynaecol. Obstet. 71(Suppl. 1), S47–S52 (2000). 37. Quereux C, Gelas B, Chevallier T, Petit F, Micheletti MC. Evaluation of the efficacy and speed of
action of sertaconazole nitrate suppository and cream combined treatment for vulvovaginal candidiasis. Gynecol. Obstet. Fertil. 28(3), 238–244 (2000).
38. Grau MT, Romero A, Sacristán A, Ortíz JA. Acute toxicity studies of sertaconazole. Arzneimittelforschung 42(5A), 725–726 (1992).
39. Romero A, Villamayor F, Grau MT, Sacristán A, Ortíz JA. Subacute toxicity and maximum tolerable dose of sertaconazole in repeated administration studies. Arzneimittelforschung 42(5A), 727–732 (1992).
40. Romero A, Villamayor F, Grau MT, Sacristán A, Ortíz JA. Chronic toxicity studies of sertaconazole after oral administration to rats and ferrets. Arzneimittelforschung 42(5A), 732–738 (1992).
41. Romero A, Grau MT, Villamayor F, Sacristán A, Ortíz JA. Reproduction toxicity of sertaconazole. Segment II (teratology) and Segment III (peri-postnatal toxicity). Arzneimittelforschung 42(5A), 739–742 (1992)
42. Romero A, Palacín C, Mosesso P et al. Genotoxicity studies on sertaconazole. Arzneimittelforschung 42(5A), 743–745 (1992).
43. Grau MT, Romero A, Sacristán A, Ortíz JA. Dermal tolerance and phototoxicity studies of sertaconazole. Arzneimittelforschung 42(5A), 746–747 (1992).
44. Farré M, Ugena B, Badenas JM, Márquez M, Roset P, Ortíz JA. Pharmacokinetics and tolerance of sertaconazole in man alter repeated percutaneous administration. Arzneimittelforschung 42(5A), 752–754 (1992).
45. Romero A, Grau MT, Villamayor F et al. Ocular tolerance of sertaconazole gel. Mycoses 39(1–2), 57–60 (1996).
46. Romaguera C, Herrero E, Márquez M, Torres J, Ortíz JA. Study on the sensitizing capacity of the new antimycotic sertaconazole in the treatment of cutaneous mycoses. Arzneimittelforschung
42(5A), 754–756 (1992). 47. Goday JJ, Yanguas I, Aguirre A, Ilardia R, Soloeta R. Allergic contact dermatitis from
sertaconazole with cross-sensitivity to miconazole and econazole. Contact Dermatitis 32(6), 370–371 (1995).
48. Agut J, Moren M, Rego M, Sacristán A, Ortíz JA. Pharmacokinetic evaluation of labelled sertaconazole after termal application. Arzneimittelforschung 42(5A), 748–751 (1992).
49. Palacin C. Antifungal activity of sertaconazole in the cutaneous retention time test. J. Mycol. Med.
5, 35–39 (1995). 50. Azcona et al. Tolerance and kinetic behaviour after single and repeated vaginal administration of
sertaconazole cream and tablets in healthy volunteers. Curr. Ther. Res. 49(6), 1046–1060 (1991). 51. Palacín C, Tarragó C, Ortíz JA. Sertaconazole: pharmacology of a gynecological antifungal agent.
Int. J. Gynaecol. Obstet. 71(Suppl. 1), S37–S46 (2000). 52. Perdomo-López I, Rodríguez-Pérez AI, Yzquierdo-Peiro JM et al. Effect of cyclodextrins on the
solubility and antimycotic activity of sertaconazole: experimental and computational studies. J.
Pharm. Sci. 91(11), 2408–2415 (2002).
Affiliations • Alfonso J Carrillo-Muñoz, MD
ACIA, Microbiology Dept, PO Box 10178, E- 08080 Barcelona, Spain Tel.: +34 934 297 120
• G Giusiano
Universidad Nacional del Nordeste, 2 Mycology Dept, Instituto de Medicina Regional, Resistencia
Argentina. [email protected]
• P A Ezkurra
Universidad del País Vasco, 3 Dept, Immunology, Microbiology and Parasitology, Faculty of Medicine,
Bilbao, Spain. [email protected]
• G Quindós
Universidad del País Vasco, 3 Dept, Immunology, Microbiology and Parasitology, Faculty of Medicine,
Bilbao, Spain

91
Azole Resistance in Neonatal Intensive Care Units in Argentina G. GIUSIANO 1 - M. MANGIATERRA 1 - F. ROJAS 1 - V. GÓMEZ 1 1 Departamento Micología, Instituto de Medicina Regional, Universidad Nacional del Nordeste, Resistencia, Argentina. Correspondence: Prof. Gustavo E. Giusiano, Departamento de Micología, Instituto de Medicina Regional. Universidad Nacional del Nordeste, Av. Las Heras 727, 3500 Resistencia, Chaco, Argentina. Fax: + 54 - 3722- 422793 E-mail: [email protected]
Summary The aim of this study was to determine the antifungal susceptibility profile and to detect resistant strains of yeast species isolated from neonates in Intensive Care Units. 92 strains isolated from 25 bloodstream cultures, 20 venous catheters, 23 suprapubic aspirations and 24 rectal swabs were studied. A Candida
glabrata strain resistant to fluconazole was detected. Candida krusei appeared with its inherent resistance to fluconazole and showed cross-resistance to itraconazole. Two Candida albicans strains were resistant to azoles, one to itraconazole and the other to fluconazole with a high minimum inhibitory concentration (MIC) for itraconazole. All Candida tropicalis strains were susceptible to fluconazole but two of them showed resistance to itraconazole. The detection of resistant strains in neonates whom had not received previous antifungal therapy is noteworthy. The variations in the epidemiology of fungal infections observed and the antifungal resistance detected emphasize the importance of performing a regular surveillance to observe and to assess them.
Key words: Fluconazole, itraconazole, resistance, neonates, Candida. Introduction There are a few specific antifugal agents available for the treatment of systemic mycoses, yet the incidence of such infections, particularly tose caused by Candida species among immunocompromised patients, is generally considered to have become extremely high. Candida sepsis, disseminated candidosis, Candida meningitidis and endocarditis are complications in premature infants that are often lethal. Amphotericin B (AMB) and fluconazole (FCZ) are the conventional antifungal agents for the management of fungal infections in these patients. FCZ is less toxic than AMB, has excellent bioavailability after oral administration, can be administered intravenously, and has broad-spectrum activity 1. Nevertheless, bloodstream infection caused by Candida glabrata (C. glabrata) and C. krusei are more likely to occur in patients who have received FCZ during hospitalization, whereas infections caused by C.
albicans and C. tropicalis are more likely among patients who have not received that agent 1,2. The other Candida species and yeast-like organisms are usually less susceptible to azole compounds and the management of such infections can be problematic 3. The clinical consequences of antifungal resistance can be seen in treatment failures inpatients and in changes in the prevalence of Candida species causing disease. Important changes in the epidemiology of hematogenous candidiasis have been observed, as well as a variation in the incidence of these mycoses according to different geographical regions 2,4,5,6,7. There has been a decrease in candidemias due to C. albicans, an increase in the proportion of infections produced by C. parapsilosis and an emergence of antifungal resistance among Candida species 8,9,10. The aim of this study was to determine the antifungal susceptibility profile and the presence of resistant strains of yeast species isolated from neonatos in Intensive Care Units (NICU). Patients and Methods This study was performed between September 1999 and September 2001 in Resistencia and in Corrientes (58º22’ and 57º54’ W and 27º15’ and 27º55’ S respectively), two cities located in a subtropical area in northeast Argentina 11. Both cities have a population of approximately 350,000 inhabitants. Clinical samples were collected from neonates in NICUs from Resistencia and Corrientes cities. Bloodstream, catheter, rectal swab and urine simples from neonates with signs and symptoms of sepsis before any antifungal therapy were collected and processed at their respective laboratories.
92
Bloodstream cultures collected by punction of peripheral vein were studied by lysis centrifugation 12. Venous catheter tips were collected in sterile recipients and processed by Maki and Cleri methods 13,14. Urine samples were obtained by suprapubic aspiration. All yeasts isolated from these samples were sent to the Mycology Department of the Instituto de Medicina Regional of the Universidad Nacional del Nordeste for reference identification and antifungal susceptibility testing. The Kreeger van Rij methodology was used for yeast identification using physiological, biochemical and morphological tests and the API ID 32C system (bioMérieux, France) 15. All specimens were inoculated onto Dixon Agar and incubated at 32ºC for 7 days with daily examination for isolation of Malassezia
species 16. The broth microdilution method standardized by the National Committee for Clinical Laboratory Standards (NCCLS) Subcommittee on Antifungal Susceptibility Testing in document M27-A was used for in vitro antifungals susceptibility testing 17,18. The activity of amphotericin B (Squibb, NJ), fluconazole (Pfizer) and itraconazole (ITZ) (Janssen Research Foundation, Argentina) was assessed. Candida krusei ATCC 6258 and Candida parapsilosis
ATCC 2119 were used as quality control strains. The MIC of amphotericin B was defined as the lowest drug concentration at which there was a complete absence of growth. The minimum inhibitory concentrations (MICs) of the azoles were defined as the lowest drug concentrations that led to a 50% inhibition of growth in comparison to controls. The microdilution plates were determined spectrophotometrically measuring the absorbance at 405 nanometers. The interpretative breakpoints were established according to recommendations of NCCLS Document M27A. For fluconazole, MICs of ≤8 �g/ml were considered susceptible, MICs between 16 and 32 �g/ml were considered susceptible dose
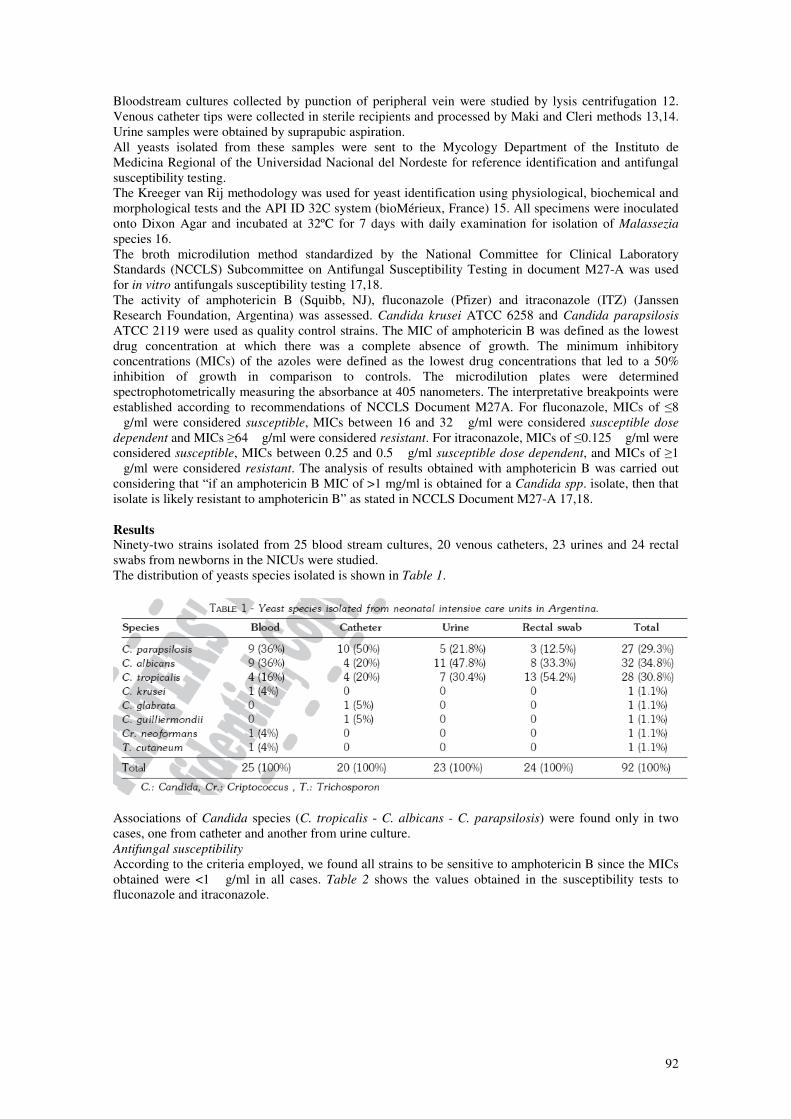
dependent and MICs ≥64 �g/ml were considered resistant. For itraconazole, MICs of ≤0.125 �g/ml were considered susceptible, MICs between 0.25 and 0.5 �g/ml susceptible dose dependent, and MICs of ≥1 �g/ml were considered resistant. The analysis of results obtained with amphotericin B was carried out considering that “if an amphotericin B MIC of >1 mg/ml is obtained for a Candida spp. isolate, then that isolate is likely resistant to amphotericin B” as stated in NCCLS Document M27-A 17,18. Results Ninety-two strains isolated from 25 blood stream cultures, 20 venous catheters, 23 urines and 24 rectal swabs from newborns in the NICUs were studied. The distribution of yeasts species isolated is shown in Table 1.
Associations of Candida species (C. tropicalis - C. albicans - C. parapsilosis) were found only in two cases, one from catheter and another from urine culture. Antifungal susceptibility
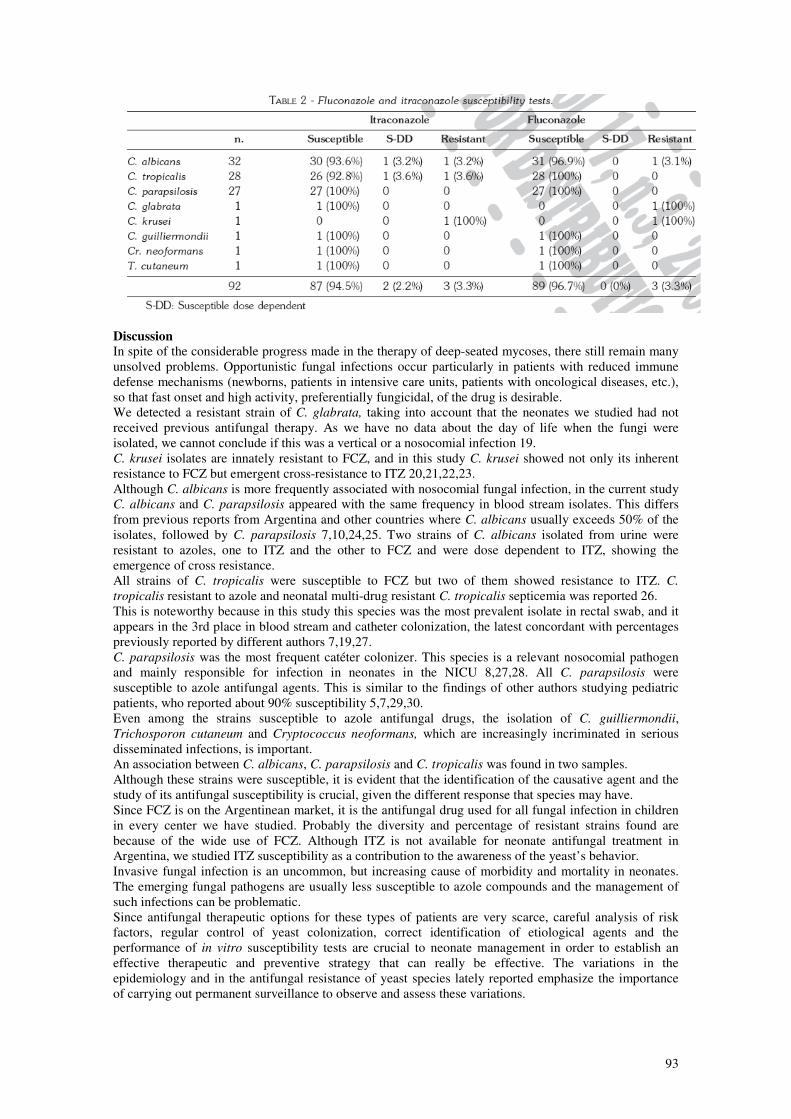
According to the criteria employed, we found all strains to be sensitive to amphotericin B since the MICs obtained were <1 �g/ml in all cases. Table 2 shows the values obtained in the susceptibility tests to fluconazole and itraconazole.
93
Discussion In spite of the considerable progress made in the therapy of deep-seated mycoses, there still remain many unsolved problems. Opportunistic fungal infections occur particularly in patients with reduced immune defense mechanisms (newborns, patients in intensive care units, patients with oncological diseases, etc.), so that fast onset and high activity, preferentially fungicidal, of the drug is desirable. We detected a resistant strain of C. glabrata, taking into account that the neonates we studied had not received previous antifungal therapy. As we have no data about the day of life when the fungi were isolated, we cannot conclude if this was a vertical or a nosocomial infection 19. C. krusei isolates are innately resistant to FCZ, and in this study C. krusei showed not only its inherent resistance to FCZ but emergent cross-resistance to ITZ 20,21,22,23. Although C. albicans is more frequently associated with nosocomial fungal infection, in the current study C. albicans and C. parapsilosis appeared with the same frequency in blood stream isolates. This differs from previous reports from Argentina and other countries where C. albicans usually exceeds 50% of the isolates, followed by C. parapsilosis 7,10,24,25. Two strains of C. albicans isolated from urine were resistant to azoles, one to ITZ and the other to FCZ and were dose dependent to ITZ, showing the emergence of cross resistance. All strains of C. tropicalis were susceptible to FCZ but two of them showed resistance to ITZ. C.
tropicalis resistant to azole and neonatal multi-drug resistant C. tropicalis septicemia was reported 26. This is noteworthy because in this study this species was the most prevalent isolate in rectal swab, and it appears in the 3rd place in blood stream and catheter colonization, the latest concordant with percentages previously reported by different authors 7,19,27. C. parapsilosis was the most frequent catéter colonizer. This species is a relevant nosocomial pathogen and mainly responsible for infection in neonates in the NICU 8,27,28. All C. parapsilosis were susceptible to azole antifungal agents. This is similar to the findings of other authors studying pediatric patients, who reported about 90% susceptibility 5,7,29,30. Even among the strains susceptible to azole antifungal drugs, the isolation of C. guilliermondii, Trichosporon cutaneum and Cryptococcus neoformans, which are increasingly incriminated in serious disseminated infections, is important. An association between C. albicans, C. parapsilosis and C. tropicalis was found in two samples. Although these strains were susceptible, it is evident that the identification of the causative agent and the study of its antifungal susceptibility is crucial, given the different response that species may have. Since FCZ is on the Argentinean market, it is the antifungal drug used for all fungal infection in children in every center we have studied. Probably the diversity and percentage of resistant strains found are because of the wide use of FCZ. Although ITZ is not available for neonate antifungal treatment in Argentina, we studied ITZ susceptibility as a contribution to the awareness of the yeast’s behavior. Invasive fungal infection is an uncommon, but increasing cause of morbidity and mortality in neonates. The emerging fungal pathogens are usually less susceptible to azole compounds and the management of such infections can be problematic. Since antifungal therapeutic options for these types of patients are very scarce, careful analysis of risk factors, regular control of yeast colonization, correct identification of etiological agents and the performance of in vitro susceptibility tests are crucial to neonate management in order to establish an effective therapeutic and preventive strategy that can really be effective. The variations in the epidemiology and in the antifungal resistance of yeast species lately reported emphasize the importance of carrying out permanent surveillance to observe and assess these variations.

94
Acknowledgements: We would like to thank Mrs. Mariana Climent for her help in translation of this work. References 1. Berrouane YF, Herwaldt LA, Pfaller MA. Trend in antifungal use and epidemiology of
nosocomial yeast infections in a university Hospital. J Clin Microbiol 1999; 37: 531-537. 2. Abi-Said D, Anaissie E, Uzun O, Raad I, Pinzcowski H, Vartivarian S. The epidemiology of
hematogenous candidiasis caused by different Candida species. Clin Infect Dis 1997; 24: 1122-1128.
3. Arévalo MP, Carrillo-Muñoz AJ, Salgado J et al. Antifungal activity of the echinocandin anidulafungin (VER002,LY-303366) against yeast pathogens: a comparative study with M27-A microdilution method. J Antimicrobial Chemother 2003; 51:163-166.
4. Pfaller MA, Jones RN, Doern GV et al. Internacional surveillance of bloodstream infections due to Candida Species: frequency of occurrence and antifungal susceptibilities of isolates collected in 1997 in the United States, Canada, and South America for the SENTRY Program. J Clin Microbiol 1998; 36: 1886-1889.
5. Pfaller MA, Jones RN, Doern GV et all. Bloodstream infections due to Candida species: SENTRY antimicrobial surveillance program in North America and Latin America, 1997-1998. Antimicrob Agents Chemother 2000; 44: 747- 751.
6. Rennert G, Rennert HS, Pitlik S, Finkelstein R, Kitzes-Cohen R. Epidemiology of candidemia - a nationwide survey in Israel. Infection 2000; 28: 26-29.
7. Singh K, Chakrabarti A, Narang A, Gopalan S. Yeast colonization & fungaemia in preterm neonates in a tertiary care center. Indian J Med Res 1999; 110: 169-173.
8. Levy I, Rubin LG, Vasishtha S, Tucci V, Sood SK. Emergence of Candida parapsilosis as the predominant species causing candidemia in children. Clin Infect Dis 1998; 26: 1086-1088.
9. Kao AS, Brandt ME, Pruitt WR et al. The epidemiology of candidemia in two United States cities: results of a population-based active surveillance. Clin Infect Dis 1999; 29: 1164-1170.
10. Rangel-Frausto MS, Wiblin T, Blumberg HM et al. National epidemiology of mycoses survey (NEMIS): variation rates of bloodstream infection due to Candida species in several surgical intensive care units and six neonatal intensive care units. Clin Infect Dis 1999; 29, 253-258.
11. Rey W, eds. Atlas total de la República Argentina. Provincia de Corrientes. Buenos Aires. Centro editor de América Latina, 1992: 76-79.
12. Negroni R, Guelfand L. Manual de procedimientos para laboratorios de Micología Médica. 1st ed. Acta Bioquímica Clínica Latinoamericana. Buenos Aires. 1999.
13. Maki DG, Weise CE, Sarafin HW. A semicuantitative culture method for identifying intravenous catheter-related infection. New Engl J Med 1977; 296: 1305-1309.
14. Cleri DJ, Corrado ML, Seligman SJ. Quantitative culture of intravenous catheter and other intravascular inserts. J Infect Dis 1980; 141:781-786.
15. Kreeger-Van Rij NJ. W. The Yeasts: a taxonimic study. Amsterdam. Elsevier Science Publishers. 1984: 47-103.
16. Guillot J, Guého E, Lesourd M, Midgley G, Chévrier G, Dupont B. Identification of Malassezia
species. A practical approach. J Mycol Med 1996; 6: 103-110. 17. National Committee for Clinical Laboratory Standards. Reference Method for Broth Dilution
Antifungal Susceptibility Testing of Yeasts. Approved Standard. M27-A. Wayne, Pennsylvania. 1997.
18. Rex JH, Pfaller MA, Galgiani JN et al. Development of interpretative breakpoints for antifungal susceptibility testing: Conceptual framework and analysis of in vitro-in vivo correlation data for fluconazol, itraconazole and Candida infections. Clin Infect Dis 1997; 24: 235-475.
19. Saiman L, Ludington E, Pfaller M et al. Risk factors for candidemia in Neonatal Intensive care Units patients. The National Epidemiology of Mycosis Survey study group. Pediatric Infect Dis J 2000; 19: 319-324.
20. Pfaller MA, Messer SA, Hollis RJ et al. Trends in species distribution and susceptibility to fluconazole among blood stream isolates of Candida species in the United States. Diagn Microbiol Infect Dis 1999; 33: 217-222.
21. Odds FC. Resistance of clinically important yeasts to antifungal agents. Int J Antimicrob Agents 1996; 6: 145-147.
22. Sanglard D, Odds F. Resistance of Candida species to antifungal agents: molecular mechanisms and clinical consequences. Lancet 2002; 2: 73-85.

95
23. Wingard JR, Merz WG, Rinaldi MG, Johnson TR, Karp JE, Saral R. Increase in Candida krusei
infection among patients with bone marrow transplantation and neutropenia treated prophylactically with fluconazole. N Engl J Med 1991; 325:1274-1277.
24. Rodero L, Boutureira M, Demkura H et al. Infecciones por levaduras: agentes causales y su resistencia a antifúngicos en pacientes pediátricos hospitalizados y en adultos HIV positivos. Rev Arg Microbiol 1997; 29: 7-15.
25. Fairchild KD, Tomkoria S, Sharp EC, Mena FV. Neonatal Candida glabrata sepsis: clinical and laboratory features compared with other Candida species. Pediatr Infect Dis J 2002; 21: 39-43.
26. Dutta S, Narang A. Drug resistant neonatal Candida tropicalis septicemia. Did it cause diaphragmatic hernia? Indian Pediatr 2003; 40: 261-264.
27. Saiman L, Ludington E, Dawson J et al. Risk factors for Candida species colonization of neonatal intensive care units patients. Pediatr Infect Dis J 2001; 20: 1119-1124.
28. Mac Donald L, Baker C, Chenoweth C. Risk factors for candidemia in a children’s hospital. Clin Infect Dis 1998; 26: 642-645.
29. Rodero L, Davel G, Córdoba S et al. Estudio multicéntrico sobre candidiasis nosocomial en la República Argentina. Rev Arg Microbiol 1999; 31: 114-119.
30. Huang YC, Kao HT, Lin TY, Kuo AJ. Antifungal susceptibility and the correlation with clinical outcome in neonatal candidemia. Am J Perinatol 2001; 18, 141-146.