envisioning the opportunities - jones & bartlett learning · envisioning the opportunities ......
TRANSCRIPT

1
1Envisioning theOpportunities
� Introduction
Physicians face unprecedented challenges today prac-ticing medicine in the United States. With practicesfounded overwhelmingly on their love of medicine, theyhave an unwavering desire to provide excellent care toa society in great need. However, the average physiciancontinually struggles to balance how to deliver the high-est-quality care with the need to survive economically.He or she faces the dual pressures of reduced reim-bursement and higher overhead and expenses.
With the desire to deliver excellent care as the un-derpinning of their profession, physicians must lookfor options in the way they practice medicine and forother sources of revenue. This book explores ancillaryservices as opportunities for physicians who are underpressure to make economic sense of their work in anincreasingly demanding field.
What is an ancillary service? An “ancillary service”is any service a physician practice provides over andabove its basic offerings and general professional fees.
Developing and providing ancillary services is ameans for physicians to realize a better return on theirinvestments of time, resources, and capital. Many physi-cians have increased their net incomes significantlythrough these services. Types of ancillary services varyby specialty, yet most physician practices could offeradditional services, perform other procedures, do moretests, and so on, within the sphere of their existing prac-tices. Some “ancillaries” can be done by current prac-titioners; others can be performed by “interim” orpart-time providers. Some ancillary services can be of-fered at “satellite” or freestanding locations.
For example, scores of surgeons are using ambu-latory surgery centers (ASC) instead of, or in additionto, using traditional hospital facilities to perform sur-gical procedures. ASCs can either be physician ownedor jointly owned by hospitals and physicians. Other in-vestors can share in the ownership as well. An ASC caneither be freestanding or an operating room in an ex-isting building. Using these facilities can be very prof-itable for the physicians and time saving because ofeasy access.
C H A P T E R

2 | Chapter 1: Envisioning the Opportunities
This chapter provides an overview of ancillary serv-ices and gives a vision of why physicians should engagein additional services beyond the basics. This vision be-comes the foundation for exploring specific compo-nents of developing a successful ancillary programstrategy. The objective is to provide physicians and otherreaders with useful tools for achieving their goals andobjectives for their medical practices.
� Overview of Ancillary ServicesExpanding on the previous definition, “ancillary serv-ices” are those services offered by a physician practiceor a hospital, beyond its core services, that generate ad-ditional revenue. An example of ancillary services wouldbe an orthopedic surgeon who provides consultationsand evaluations of diseases and injuries affecting thebones and skeletal system. Most of this physician’s rev-enue is from professional fees charged for performingsurgical procedures. Historically, those surgical proce-dures have been performed within the local or area hos-pital’s operating room (OR) facilities. Physicians arebecoming more accustomed to performing these serv-ices at independent, stand-alone ASCs or, in some in-stances and depending upon the specialty, at their ownoffices.
Hospitals, on the other hand, have traditionallyemphasized inpatient care along with their operatingroom and other surgical services. Although continu-ing in this mode, hospitals are also looking at serv-ices that they can provide other than room, board,and professional care. They have developed outpa-tient centers, including ASCs, which allow them toprovide at least some of these services outside thehospital’s walls.
The following are a few examples of ancillary services:
� X-ray services laboratory� Anesthesia (in certain settings)� Physical therapy� Diagnostic testing� Diabetes and weight management programs� Wellness centers
� Retail product sales (e.g., eyeglasses, hearingaids, etc.)
� Freestanding ASCs� Dialysis centers� Antiaging centers� Skin care centers� Infusion therapy centers� Catheterization laboratories� Sleep centers� Endoscopy centers� Antiaddiction centers� Psychotherapy centers� Weight loss centers� Geriatric centers� Urgent care centers� Pain management
Practically every physician specialty has the opportu-nity to add ancillary services. Figure 1-1 (following) isa partial list of services by specialty, and some exam-ples of ancillary services that might fit well with thosespecialties.
Ancillary services can assist with the ultimate goalof providing quality medical care, often in the physician’soffice, and generate a profit for his or her efforts. The or-thopedic surgeon, for example, can establish a success-ful private practice by providing patients with pre- andpostoperative care and consultation. That same ortho-pedic surgeon may establish an ASC “attached” to theoutpatient practice. For example, any single room withinthe physical plant can be converted to a surgical suite,operate under a different tax identification number, andbe used by the physician to offer more convenient serv-ices to benefit both the physician and his or her patients.The orthopedic surgeon performs all surgical proceduresat the ASC unless the procedure requires an overnighthospital stay. Even then, if the hospital is nearby, the sur-geon may use the ASC and then transport the patient tothe hospital for overnight care.
This is an excellent example that can be found du-plicated throughout the United States. Forming ASCsand establishing other ancillary services is not donewithout constraints, however. Many states govern suchventures by requiring prior approval, which usuallymeans that the entity must receive licensure through

Overview of Ancillary Services | 3
satisfying the requirements for a “certificate of need”(CON). This authorization provides the physician, oranyone else developing the ancillary service, with theright to build and operate based on the fact that thecommunity needs the service. Some states do not haveCON regulations; therefore, launching an ancillary ven-ture is quite easy. Other states have very stringent re-quirements; others lie somewhere in between. Some
states allow single specialty, small ASCs or ancillaryservices, as in the example of the orthopedic practicementioned previously, to be built as long as the cost iswithin a certain threshold.
The ancillary service, like the orthopedic surgeon’sASC, often benefits the patient by offering convenience,the same or reduced costs, and as good or better qual-ity and continuity of care.
Ancillary Services by Specialty
Ancillary Services Examples by Specialty Provider
Anesthesiology Pain management center The Cleveland Clinic Pain Management Centers,
Neurological Associates Pain Management Center
Nephrology Renal center Silver Cross Renal Center,
The Gloria York Renal Center
Orthopedics X-rays, physical therapy, diagnostic The Cleveland Clinic Rehabilitation Institute,
center, ASC Vision Surgery & Laser Center, LLC
Cardiology Stress testing, nuclear testing, Minneapolis Heart Institute,
cardiorespiratory care, catheterization Hendrick HeartSaver Network Heart
laboratory Catheterization Lab
Radiology Mammography diagnostic center, Women’s Diagnostic Center,
basic radiology imaging centers Radiology Associates
Internal medicine Lab, X-rays, diabetes management, spa, Diabetes Management and Training Centers, Inc.,
retail products IN TOUCH diabetes management software program
from LifeScan
Dermatology Retail products, skin care centers The Cosmetic Skin and Surgery Center,
Essentials Skin Care Center
Hematology/oncology Infusion centers, radiation centers Lourdes Ambulatory Infusion Center,
Synchrotron Radiation Center
Neurology Sleep study centers Carilion Sleep Center,
The Center for Sleep Disorders at Johnson City
Medical Center
Pulmonology Hospitalist program, sleep study center Ochsner Clinic Hospitalist Program,
Cheshire Center for Sleep Studies
Family Practice X-rays, lab, diabetes management Geriatrics Center of Excellence (COE) at Cambridge
programs, geriatrics centers Health Alliance
Gastroenterology Endoscopy center Three Rivers Endoscopy Center
Endocrinology Nutrition education programs Friedman Foundation
General Surgery ASC Virtua Ambulatory Surgery Center
Urology ASC, continence centers The Hennepin Faculty Associates Continence Center
Pediatrics Lab, X-rays (subspecialty may have East Tennessee Children’s Hospital
asthma and allergy center, etc.)
Figure 1-1

4 | Chapter 1: Envisioning the Opportunities
� Why Consider Ancillary Services ?Physicians, hospitals, other providers, and investorsthat are considering whether to invest in ancillary serv-ices should base their decisions on the following im-portant issues:
� Declining third-party reimbursement for stan-dard services
� Their need to diversify and increaserevenue
� In reaction to the final Stark regulations� To broaden their ability to offer ancillary
services� To achieve more control over all aspects of pa-
tient care available� Their desire to improve their quality of care, usu-
ally with improved efficiency� To augment revenue and enhance bottom line
results
Unless most of these factors apply, reconsiderationof the entire proposed venture is recommended.
Physicians who develop ancillary services are un-der continual pressure to maintain the highest standardof quality care, and yet are regularly forced to take lessreimbursement for their services. Physicians’ costs ofproviding services is ever increasing, as labor, rent, mal-practice coverage, supplies, and other practice expenseshave climbed steadily over the last 10 years. During thesame period, reimbursement, (i.e., what the physiciangets paid for his or her services) has not increased com-mensurately. Even when adjusted for inflation, increasesin revenue have fallen far behind expenses in most ar-eas of the country. Increased expenses and lower reim-bursements place huge hardships on physicians—tothe extent that many have questioned whether to con-tinue to practice medicine. Sadly, many have left theprofession in which they invested so much, and othersare finding the need to diversify.
The Stark laws and other federal regulations haveinhibited physicians and hospitals since their intro-duction, but the 2003 final Stark rulings provide newopportunities that broaden the ability of health careproviders to offer and invest in ancillary services.
Although economic factors are among a physician’stop priorities for considering investing in or develop-ing ancillary services, quality of care is of equal con-cern and the major “driver” in the decision. Quality ofcare cannot be compromised.
In the same way one would ask questions about fi-nancial issues, the following are specific questions toconsider relative to quality of care and an ancillary serv-ice venture:
� Will the service add to or detract from patientcomfort and security?
� Will patients be compliant with the care plan?� Does the physician have the ability to supervise
the delivery of ancillary services?� Will care be of comparable quality to the tradi-
tional way the service is provided?� Will the service be reimbursed by third-party
payers?� What are the revenue possibilities on a per case
or per procedure basis?� Is there a possibility of an acceptable return on
investment?
Although other questions should be answered, theseare the most important and should be top priorities indetermining whether an ancillary service makes busi-ness and clinical sense.
There are several guidelines to follow before de-ciding to develop an ancillary service. First, do ex-haustive “due diligence” on financial, management, andlegal compliance matters. Each of these three facets willbe addressed more comprehensively in subsequent chap-ters of this book. A feasibility study and business plan(i.e., the due diligence process) is an essential compo-nent of your planning. You will also require competentmanagement of your entity or your service. Otherwise,the ancillary service initiative will get off to a slow startor fail completely. Your ancillary service venture mustcomply fully with all the rules and regulations that gov-ern it throughout the establishment of the entity andduring all operational phases. The consequences of non-compliance are significant.
Start with a clear business plan and prepare a com-prehensive budget with a series of “pro forma” (as if)

Why Consider Ancillary Services ? | 5
projections. Preparation and planning is the subject ofChapter 4.
Gather an experienced team to structure the trans-action and operate the business. This team should in-clude representatives from your existing managementstaff and outside resources, such as consultants, attor-neys, accountants, and other advisors who can assistin various areas and stages of the process. Some will becalled on in the preplanning and planning stages, andothers need to be on board for the management of theentity.
Another concept that is important during the de-velopment phase of the ancillary service is to have anidea for the source of patients, or customers. Part of thedue diligence (as addressed in Chapter 3) will includedevising an effective plan to market the services.Understanding referral sources is essential, especiallyfor ancillary services like an ASC that are dependentupon the referrals of other physicians (as well as thosewho are owners of the venture) for success, if not sur-vival. A demographic analysis of your existing patientbase can also be a huge factor to consider in planningand marketing your services.
You will also need to hire competent outside assis-tance including knowledgeable legal counsel. Seek anattorney who has years of experience in health care law.Another important consideration is to hire an experi-enced health care consultant familiar with the com-plexities of outpatient medical practice and ancillaryventures, especially at the beginning or preopeningphases. After the venture is up and running and a stronginternal management team is in place, your need for anoutside consultant should be limited if you get off to agood start. You may, however, decide to outsource allor some aspects of your management. Some consider-ations for possible functions to outsource are billing,coding, and compliance.
If establishing an ancillary service involves con-struction or modification of a facility, you must meetall the requirements for structural planning and coor-dination of design. The investors must take the time tothink through all aspects and stages to anticipate needs,problems, and challenges. Otherwise you will regretmistakes and be compelled to make changes as a resultof a lack of efficiency or misuse of space.
Another rule to follow as the ancillary venture isconsidered is the need to develop an implementationtimeline and assign specific responsibilities to thosethat are taking part in the preopening and preplanningprocesses. Individuals should be assigned due dates aswell as responsibilities to assure the process will be com-pleted effectively. It is highly unlikely that timelineswill be met unless specific assignments are made.
Thus, the key components of ancillary service de-velopment include the design of that service to serve aspecific medical need of a targeted population whoseprofile shows a high demand for the service. The serv-ice should be located in an area where demographicsidentify it as having a high density of the targeted pop-ulation. It is both acceptable and advisable to have theancillary service mirror the existing outpatient prac-tice, if indeed the physician is the investor.
Other good options for investment in the ancillaryservice include joint ventures among hospitals andphysicians as well as private investors. Hospitals andphysicians are often at odds with each other and notamenable to working together. However, when a hos-pital and physicians are committed to working togetherbased on a fair and objective business plan, and neitherparty takes advantage of the other, the community ben-efits greatly. The result will be the success of the jointventure, as it is much easier for both parties to focus onproviding quality care when they know they are not try-ing to compete with each other. The community thenenjoys the benefits.
Another option is to hire a management group toset up and run the ancillary venture within the prac-tice location. Many competent management companiesprovide these services. Some will want to share own-ership, which may or may not be a good idea for thephysicians or hospitals. Each situation should be re-viewed upon its own merits.
Some providers have the opinion that no one cantake as good care of a business as the owner. This view-point often proves true when services are turned over toa management company where there is the risk of it man-aging in absentia. On the other hand, a managementcompany may provide expertise that is needed in spe-cialized areas of service. In this regard each situationshould also be considered based upon its own merits.

6 | Chapter 1: Envisioning the Opportunities
Still another option in creating an ancillary serviceis to have a member of the medical group become themedical director of the ancillary service, and in so do-ing stay closely involved in the clinical services beingperformed and the quality of those services.
Day-to-day management and oversight may also beadministered to some extent by personnel from the ex-isting staff. This is usually only a temporary arrange-ment and should not be a long-range solution. From abusiness standpoint, it is best not to comingle staffamong business entities; however, it does make sensein some instances to have crossover tasks, as when thefunctions are complementary.
� Current Environment and PlayersAncillary services are the hot topic among virtually allparticipants in the provider service chain, which in-cludes hospitals, physicians, private companies and in-vestors, and various combinations of the foregoing.
Hospitals have long strived to determine the bestmodel, both economically and in terms of patient care.The practice of medicine generally is based upon tra-ditional delivery models, not on appropriateness of thedelivery. The consequences of inappropriate deliverycan result in the difference between life and death.Continuing with historical ways of taking care of pa-tients can stymie thinking, lead to operations that fos-ter inefficiency, and constrain the quality of patient care.Delivery models should, therefore, be carefully couchedwithin the context of “this is the way we do it” versus“this is the way we might be able to change it” to de-rive at the “right way.”
Hospitals, which traditionally are bureaucratic andslow to change, have been looking “outside the box”for ways to deliver services, including ancillary serv-ices. Conventional wisdom says not to redesign a program until there is a problem. Nevertheless, in thefast-moving health care environment, waiting for abona fide problem results in being at a disadvantage.It takes time to plan dramatic changes, especially whena hospital has a heavy investment in equipment andsupporting services, such as personnel. One area wherehospitals are rethinking their delivery systems is car-
diovascular services (CV). CV services is one of themajor service lines within most hospital’s provision ofcare, and our country’s aging population supports thisfor the future. Therefore, hospitals must focus on thisprogram now and consider it in the context of servicesthat can be performed outside of the four walls of thehospital. Although CV surgeries are rarely, if ever, per-formed outside of the operating room because of theseriousness of the procedures, many other services thatsupport CV care are performed outside of the hospitalfacility. For example, interventional cardiology is a ma-jor consideration in lieu of surgery, a trend which likelywill continue based on technology and clinical out-comes. Hospitals, as a result, are compelled to considerpulling out some of their most profitable and stablecomponents of revenue, that is, cardiology and catheter-ization lab services. Traditional delivery must change.Physicians, cardiologists, and others are thinking aboutperforming noninvasive and noninterventional cardi-ology within their own freestanding facilities. Althoughinterventional cardiology is not accepted in an ancil-lary, stand-alone setting, less serious procedures per-formed away from the hospital are the “rule of the day”for many cardiologists. At a minimum, hospitals mustplan for these scenarios as they inventory the skills,talents, and services they will provide or want to pro-vide in the future. Not surprisingly, such considera-tion must include the physician as either a competitoror, preferably, as a partner.
Now, more than ever, hospitals must organize pro-grams based on the considerations of ancillary servicesfor their maximum positive impact on patient services,and to achieve good physician and medical staff rela-tions. This calls for a commitment to design a CV an-cillary services program. Throughout this book, areasare considered with a degree of specificity that bothhospitals and others must consider in this context. Ifhospitals do these things correctly, they can protect atleast a significant portion of what before has been ex-clusively their revenue stream. Sharing in revenue thatused to be solely theirs may be disappointing; nonethe-less it is becoming the rule of the day.
“If done properly, there are numerous opportuni-ties and examples (some in place, some yet to be de-signed) that can change the way we care for patients.

Current Environment and Players | 7
Given the rising cost of health care and our current de-mand for health services, this entire situation takes onsome urgency. It is not only about cardiovascular sur-gery, but all cardiac services, and not only about hos-pitals, but how those hospitals provide a potpourri ofservices to a community, at the hospital, but also inother locations, not only about cardiovascular special-ists, but also about the competing imperatives of somany constituencies that characterize the health carelandscape—constituencies who should have the pa-tient as their ultimate concern.
“If a man…make a better mouse-trap than his neigh-bor, tho’ he build his house in the woods, the world willmake a path to his door.”—Ralph Waldo Emerson (at-tributed)1
As discussed, physicians are another major playerin the current health care environment. Physicians areone of the major components in the development ofancillary services. It is amazing that physicians havegone as long as they have in allowing private industryand hospitals to build, manage, and operate ancillaryservice entities. ASCs have only been in existence thelast 10 to 15 years. Prior to that time, there was rarely,if ever, a thought given to performing surgeries outsideof the hospital operating room , mostly because of thetechnology required and what was perceived to be bestfor the patient. Technology is a driver in this dynamic,and without advances in technology it is unlikely an-cillary services would be a topic of discussion. However,without question, technology has moved the physicianinto a more entrepreneurial position. Inherent to theirtraining, physicians learn the skills to perform surger-ies or most other ancillary services. It makes perfectsense for physicians to adopt a more entrepreneurialattitude in the development of such ventures.
Using the previous example of CV services, mostcardiologists are trained to perform highly technicaland life-or-death services. Although not surgeries perse, CV services are often invasive or semi-invasive pro-cedures. The patient’s life is on the line (if not at thattime, certainly later as the diagnosis for his or her heartcondition is defined). As a result, physicians have al-ways borne the liability or the risk for performing suchservices. To relocate the delivery of these services to anoutpatient catheterization laboratory is really not chang-
ing the level of liability for the physician, or if so, onlyslightly. Often the cardiologist believes that he or shecan perform such services in his or her own lab underbetter controls, and with as good if not better qualityoutcomes. Therefore, in some respects, the risk may ac-tually be perceived to be less.
From an economic standpoint, the physician seesthe ability to garner a portion of the revenue “pie” thatwas never before available. The technical or facility fee,which is a genuine component of the services beingrendered, can now be a part of the physician’s base ofrevenue. This is not only alluring, it is in some respectsessential for the maintenance of a level of income com-mensurate with the risk for providing such services bythe physician.
Thus, physicians will continue to be strong and ac-tive players in the market place, relative to ancillaryservices—they are not going away. They will be a partof the process and, logically speaking, this is not sur-prising considering they will still be the ones provid-ing the key components of clinical care.
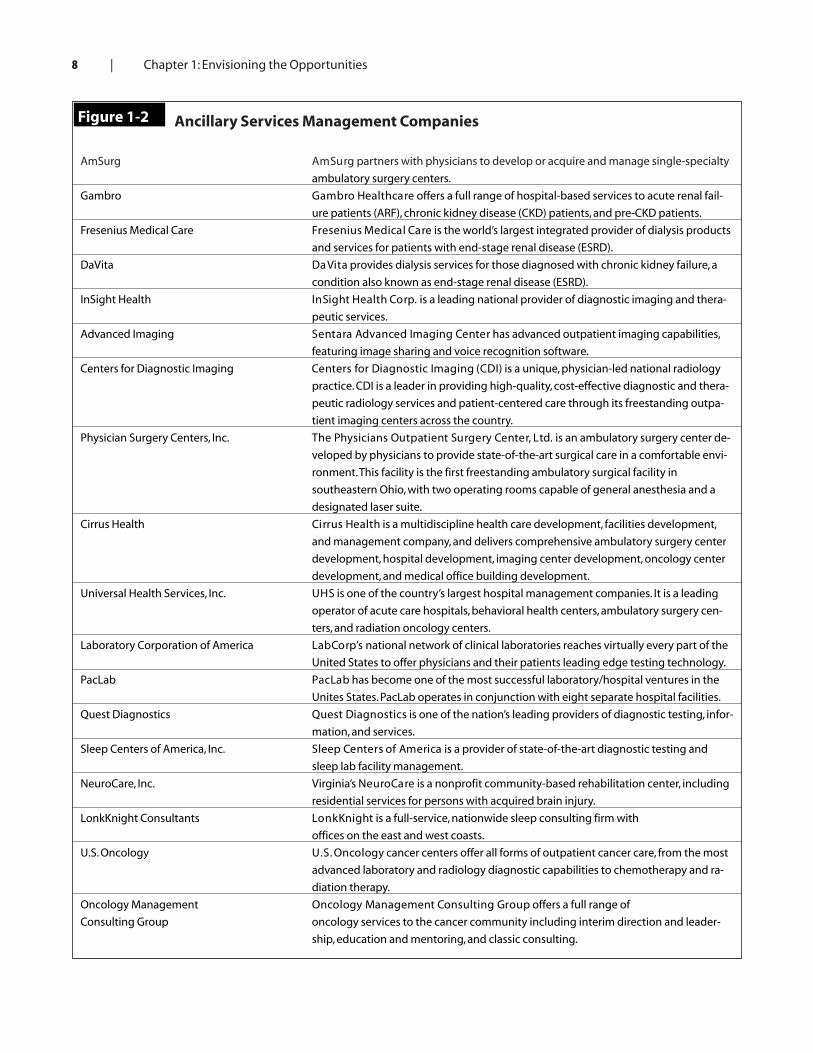
Private companies and investors are not new to thescene either. For-profit hospitals have been around formany years, and some of the best hospitals in the UnitedStates are operated by for-profit entities that are publiccompanies listed on the New York Stock Exchange. In addition, many other companies specialize in the provision and/or investment in these ancillary serv-ices. Figure 1-2, “Ancillary Services ManagementCompanies,” shown following, is a list of some of thepublicly held and privately held entities and their mar-ket focus.
Figure 1-2 shows there are numerous private com-panies that specialize in the development of ancillaryservices, which take on different shapes and forms. Forexample, some private entities will build, develop, andmanage AS centers. They may also partner with physi-cians, or simply contract for professional services.Hospitals can also be partners in these ventures.
The business model of a private investor deliver-ing care can be questioned. The inevitably concern iswhether proper care is being provided, or if quality isbeing sacrificed for the “almighty dollar.” Most privateinvestor companies deliver excellent care and insist onmeeting the highest possible standards for the delivery
8 | Chapter 1: Envisioning the Opportunities
Ancillary Services Management Companies
AmSurg AmSurg partners with physicians to develop or acquire and manage single-specialty
ambulatory surgery centers.
Gambro Gambro Healthcare offers a full range of hospital-based services to acute renal fail-
ure patients (ARF), chronic kidney disease (CKD) patients, and pre-CKD patients.
Fresenius Medical Care Fresenius Medical Care is the world’s largest integrated provider of dialysis products
and services for patients with end-stage renal disease (ESRD).
DaVita DaVita provides dialysis services for those diagnosed with chronic kidney failure, a
condition also known as end-stage renal disease (ESRD).
InSight Health InSight Health Corp. is a leading national provider of diagnostic imaging and thera-
peutic services.
Advanced Imaging Sentara Advanced Imaging Center has advanced outpatient imaging capabilities,
featuring image sharing and voice recognition software.
Centers for Diagnostic Imaging Centers for Diagnostic Imaging (CDI) is a unique, physician-led national radiology
practice. CDI is a leader in providing high-quality, cost-effective diagnostic and thera-
peutic radiology services and patient-centered care through its freestanding outpa-
tient imaging centers across the country.
Physician Surgery Centers, Inc. The Physicians Outpatient Surgery Center, Ltd. is an ambulatory surgery center de-
veloped by physicians to provide state-of-the-art surgical care in a comfortable envi-
ronment.This facility is the first freestanding ambulatory surgical facility in
southeastern Ohio, with two operating rooms capable of general anesthesia and a
designated laser suite.
Cirrus Health Cirrus Health is a multidiscipline health care development, facilities development,
and management company, and delivers comprehensive ambulatory surgery center
development, hospital development, imaging center development, oncology center
development, and medical office building development.
Universal Health Services, Inc. UHS is one of the country’s largest hospital management companies. It is a leading
operator of acute care hospitals, behavioral health centers, ambulatory surgery cen-
ters, and radiation oncology centers.
Laboratory Corporation of America LabCorp’s national network of clinical laboratories reaches virtually every part of the
United States to offer physicians and their patients leading edge testing technology.
PacLab PacLab has become one of the most successful laboratory/hospital ventures in the
Unites States. PacLab operates in conjunction with eight separate hospital facilities.
Quest Diagnostics Quest Diagnostics is one of the nation’s leading providers of diagnostic testing, infor-
mation, and services.
Sleep Centers of America, Inc. Sleep Centers of America is a provider of state-of-the-art diagnostic testing and
sleep lab facility management.
NeuroCare, Inc. Virginia’s NeuroCare is a nonprofit community-based rehabilitation center, including
residential services for persons with acquired brain injury.
LonkKnight Consultants LonkKnight is a full-service, nationwide sleep consulting firm with
offices on the east and west coasts.
U.S. Oncology U.S. Oncology cancer centers offer all forms of outpatient cancer care, from the most
advanced laboratory and radiology diagnostic capabilities to chemotherapy and ra-
diation therapy.
Oncology Management Oncology Management Consulting Group offers a full range of
Consulting Group oncology services to the cancer community including interim direction and leader-
ship, education and mentoring, and classic consulting.
Figure 1-2

Current Environment and Players | 9
of their services. Many will get the best doctors, sur-geons, and other health care providers to perform serv-ices. In general, investor entities do not sacrifice quality.
Without question, the motivation of these entitiesis to show a profit on the bottom line of their incomestatements. However, we should also question whetheror not this is also the motivation with other providerinvestors, including physicians and hospitals. Everyone,including private investor companies are focused onquality outcomes. Without quality outcomes, they willnot survive simply because the market will not allowit. Further, managed care companies will not contractwith entities of questionable quality. The conclusion isthat private investor-owned ancillary services are as re-liable as others; although there are exceptions to everyrule. This is also true for hospital and physician-ownedentities.
The private investor in health care is here to stay.Health care makes up at least one fifth of the entire USgross national product (GNP). We are talking abouttrillions of dollars. The assumption is that private in-vestors will always be a part of the delivery of care,which is good, particularly when one considers the costof the delivery of these services. “Profit” is not a four-letter word in the health care industry. It is the drive forprofit that has yielded the tremendous advances in tech-nology which make the health care delivery system inthe United States unparalleled anywhere else in theworld.
The current environment includes three majorplayers: hospitals, physicians, and private companiesand investors. These can be combined in a joint in-vestor entity or in a competitive environment for thedevelopment, operation, and management of ancil-lary services.
Market conditions also have an effect on the envi-ronment. In the early 1990s it was assumed that a morerestrictive form of managed care would be pervasiveand that this would eventually envelop the entire payerside of the US health care delivery system. Capitationseemed to be the trend and if not for capitation, providers(hospitals and physicians) would be under a system di-rected by the government or private insurance carriersas to where they could perform and what they coulddo. The patient side of care assumed a similar dynamic.
Predictions were that patients would only be directedto certain physicians and facilities for providers to bereimbursed for even a portion of their services. Further,the rule of the day was that contracts would encompassentire populations and all health care for that popula-tion would be controlled by those contracts. Althoughsuch drastic measures did not fully materialize, manyaspects of this model are characteristic of our currenthealth care delivery system.
Market conditions are definitely less extreme thanexpected in the early 1990s; however, health careproviders are greatly restricted. Further, the marketplaceputs providers under pressure to provide the same qual-ity of care as their competitors. Just because capitationand global contracting have not become as pervasive aspredicted does not diminish the many remaining re-strictions on health care providers. Correspondingly, pa-tients are also restricted in their access to services. Accessto health care services is still largely driven by a market-based environment; that is, the desired combination oflow cost and high quality remains the strongest force inthe marketplace. Physicians, hospitals, and private in-vestors in ancillary services must understand and adaptto the low-cost, high-quality paradigm or their venturewill likely fail, regardless of how well the ancillary serv-ice is managed and operated.
Many books have been written about the dynam-ics of managed care and how to exist in such an envi-ronment. The purpose of this book is not to focus onmanaged care, yet it would be remiss if it did not pointout the importance of this phenomenon as a major con-sideration in the decision-making process for puttingtogether an ancillary service.
Further, many of the attitudes of payers and mar-ket conditions themselves are confined to local condi-tions, with one area of the country varying greatly fromanother. Each situation, therefore, must stand on itsown merit and consideration. One general plan will notapply throughout the country because of the conflict-ing dynamics at work from one area to another.
The evaluation process should begin with payer at-titudes and relations, which are primary reasons whyphysicians are such an important component of the an-cillary service initiative. Physicians and hospitals havethe relationships with the payers, and presumably good

10 | Chapter 1: Envisioning the Opportunities
relationships will carry over to the ancillary service. Thisis especially true if that service is well planned and coor-dinated, and if the payer is convinced it will provide equalservice and quality of care in a cost-efficient manner as ahospital or other venture. Thus, the payer relations ele-ment should be completed early on in the evaluationprocess to understand the opportunity for performingprocedures within the specified ancillary service.
� Characteristics of SuccessfulVentures
Examples of ancillary services are listed previously inthis chapter. As with any other business initiatives, someare very successful, others providing the same serviceline are less successful, and some fail totally. What thenare the characteristics of successful ventures? A suc-cessful outcome is an outgrowth of four important stagesin the implementation of the ancillary service. Thesefour stages of implementation are as follows:
1. Planning2. Development3. Operations4. Continued assessment
When looking at each of these stages in greater de-tail, keep in mind that the successful development andimplementation of each of these stages is the prescrip-tion for success.
The Planning StageThe planning stage is completed before any investmentand, to some extent, before any long-term commitmentis made for the ancillary initiative. The first order ofbusiness is to develop a flexible and customized busi-ness plan. Moreover, prior to the business plan a feasi-bility analysis also may be needed depending upon thesituation. If, for example, the potential investors or par-ticipants in the ancillary service are somewhat uncer-tain as to the overall viability of the ancillary servicedevelopment, more detailed feasibility analysis shouldbe completed first. Chapter 3, “Preparing the FeasibilityStudy,” addresses the feasibility study in detail.
Both the business plan and the feasibility analysiscall for a demographic review prior to completion toanalyze the market for the types of ancillary servicesthat are both needed and wanted. The demographicanalysis will relate key elements, such as competition,socioeconomic standing, population (current and ex-pected growth rates), and other pertinent informationrelative to such an analysis.
For example, an orthopedic practice is flourishingwithin a certain area near a hospital. However, withinthat area the surgeon is starting to see an erosion of vol-ume as more primary care physicians move to outlyingareas within the service area. Further, most of the com-peting surgeons in his specialty are concentrated in thesame area as his practice. The question that then arisesis where a surgery center should be placed. Should itbe near the campus of the orthopedic surgeon’s exist-ing practice, or should it be in an outlying area, per-haps where the community is growing and thedemographics indicate positive trends? The answers tothese questions would come through a demographicanalysis that is either a part of the business plan or thefeasibility study. Consider the information in Chapters3 and 4 for a detailed analysis of both a feasibility studyand business plan.
Although it takes considerable time, the impor-tance of the demographic study cannot be underes-timated. It may cause the potential investor physician(in this scenario) to completely reverse the locationdecision, yet the time would be well spent when con-trasted to spending time, energy, and capital to builda surgery center in an area that would soon becomeoversaturated or where the patient population wasshifting elsewhere. A venture like a surgery center isa long-term venture that must stand the test of timeover an extended period of at least 5 to 10 years andperhaps longer.
Another integral part of the planning stage shouldbe the preparation of the “pro forma” income statementand cash flow projection. These are examined in muchgreater detail in Chapter 3. It is essential to understandthat the very core of any ancillary initiative lies in therevenue and expense assumptions, which must be basedon realistic figures and calculations. Financial projec-tions are often best completed by an outside independent

Characteristics of Successful Ventures | 11
party (along with the business plan and demographicstudies) as a level of independence is essential.
Sample revenue assumptions should be brokendown based upon individual procedures and specificprocedures that will be performed. Likewise, expensesshould be documented based upon a line-by-line pro-jection of each of the overhead components. Later chap-ters in this book address how proforma income andcash flow statements are completed.
Development StageThe second phase of implementation is the develop-ment stage, which follows the completion of the initialfeasibility study (at a minimum) and business plan, andwhen it is assured that the ancillary venture is a go.Several areas should be addressed, including the fol-lowing:
� Establishing a legal entity� Procuring financing as necessary� Securing a location� Purchasing necessary equipment and supplies� Completing third-party reimbursement creden-
tialing requirements� Hiring and training staff� Setting up scheduling, billing, and reporting
functions� Instituting regulatory compliance protocols� Developing written policies and procedures� Establishing a management structure (both
provider and nonprovider)
In essence, the development stage is that periodprior to opening wherein key decisions related to theplanning, operations, and ongoing organizational struc-ture of the ancillary service entity will be completed. Itis an area of critical importance and must be well-thought. Most of the remainder of this book is devotedto a detailed discussion of each of the areas within thedevelopment stage. To complete these areas effectively,we recommend an organized outline of the task be com-pleted, assignment of the individuals who are respon-sible for the tasks, and a timeline for completion. Figure1-3, the “Development Plan Worksheet” (following),provides a sample list of initiatives that are to be com-
pleted with columns for assignments and timelines.As in Figure 1-3, we suggest three major initiatives
within the development stage.First are the “structural initiatives,” which consider
the legal structure, equity, ownership, pertinent agree-ments that memorialize the ownership, and the ad-ministrative processes.
Next, are the “organizational and management ini-tiatives” that define the organizational chart, the indi-vidual physicians and job descriptions, an outline ofreporting responsibilities and protocols, managementconsulting, legal and accounting assistance, adminis-trative processes and the marketing plan, and other re-lated documentation and functions.
Finally, the “operational start-up initiatives” sum-marize the major areas of operational start-up projectsthat must be completed prior to the actual opening.Naturally, variations occur within each situation. Someancillary services may be able to rely to a large extenton the existing practice structure and infrastructure,and some of these areas may not even be necessary assuch. However, given the fact that all of these tasks willneed to be done in one form or another, it is best to stayorganized and make sure that nothing is overlooked.
The Operating StageOnce the ancillary service business is up and running,the operational aspects that will make it a success shouldnot be neglected. Requirements include constant mon-itoring and management of clinical operations, pro-viding continuing clinical and productivity training forstaff members, monitoring of coding and submissionof collection of claims, monitoring of compliance withregulatory agencies, and constant analysis of financialperformance. Monthly financial reports should be com-pleted and interpreted regarding performance. Strategicplanning should be ongoing. Once the ancillary serv-ice is operative and has some track record of perform-ance, the historical data will serve as a basis for gooddecisions in the future, and will help in strategic plan-ning relative to expansion, divestiture, dilution, or evencontraction.
Continued AssessmentThe final stage in the successful implementation of the

12 | Chapter 1: Envisioning the Opportunities
Development Plan Worksheet
Task Person(s) Responsible Completion Timeline
Structural Initiatives
Decide on legal structure
Agree upon equity ownership
Complete pertinent agreements
Complete operating agreement
Complete buy/sell agreement
Complete employment agreements for providers and technologists
Define administrative processes and structural form (administrative
services as a part of the institute versus an independent management
services organization)
Organizational/Management Initiatives Person(s) Responsible Completion Timeline
Outline organizational chart
Define individual physicians and develop job descriptions
Outline reporting responsibilities and protocols
Procure management consulting, legal, and accounting assistance
Determine administrative processes and responsibilities
(i.e., billing, personnel management, compliance, etc.)
Develop a marketing plan
Design marketing materials as a part of the marketing plan
Operational Start-Up Initiatives Person(s) Responsible Completion Timeline
Determine effective date for opening the institute
Select and register the corporate structure
Apply for hospital privileges
Apply to managed care organizations
Negotiate office lease
Design renovations
Order equipment
Select furniture
Select information system, including paperless office applications
Design and order telephone system
Select an insurance agent/broker
Determine insurance coverage needed
Determine supply needs
Decide on vendors (clinical and nonclinical)
Determine office form needs including business cards, stationary, etc.
Establish office policies and procedures
Design organization structure/determine staffing needs
Analyze compliance with regulations (coding, billing,
documentation, HIPAA)
Apply for necessary accreditation, business licenses, and other
appropriate certification for the institute
Figure 1-3

Conclusion | 13
ancillary service is continued assessment. All of thefactors that were reviewed, analyzed, and decided uponprior to opening must be continually assessed, such asthe following:
� Ownership structure� Management structure� Review of Stark rules and compliance and other
regulatory laws, including new regulations� Continued equipment needs� Facility layout� Staff� Proper coding� Revenue goals� Expense structure� Ongoing training� Service offerings relative to strategic plans and
needs� Return on investment
Running an ancillary business is not unlike run-ning a medical practice, a hospital, or some other non-health care business. It requires a well-charted course,both prior to opening and after the business is up andrunning.
� Successful Planning ProcessesThe need for planning cannot be overemphasized forany venture prior to the actual decision to move for-ward and before investing time and resources. The plan-ning should be done in organized phases of work. Eventhough the ancillary service may be derived from anexisting physician practice, it should have a separateidentity. A definition of its mission, vision, and valuesis appropriate, which is included in the business planand strategic planning processes outlined in later chap-ters.
Prior to completing the decision to move forwardwith the ancillary service venture, the investors shouldnot only take the time to define the type of entity (mis-sion, vision, values, etc.) but to realistically identify itscapabilities and its goals and objectives. It is a mistaketo believe that because the ancillary service is an ad-
junct to a successful practice that it too will automati-cally be successful. For example, a primary care physi-cian who is operating a successful family practice andhas extra space may believe that the opening of an ur-gent care clinic will be an automatic success; however,this is not necessarily true. Competition may alreadyexist in this very specialized arena that will be more for-midable than thought. Further, the commitment withan urgent care center to extended hours, additional staff,diagnostic equipment, and so forth entails not only asignificant investment of time, but a financial invest-ment as well. Therefore, what seems to be (and mayvery well be) a very logical ancillary venture for the pri-mary care physician may encounter several obstaclesto success.
Therefore, it is important that realistic and frankdiscussions take place among the investors as to whetheror not the ancillary service will indeed be viable. Outsideresources who can lend an independent viewpoint canmake a viable contribution to the overall project’s prob-ability of success.
� ConclusionThe practice of medicine is both a profession and a busi-ness. Ancillary services present a viable way for physi-cians, hospitals, and independent investors to enhanceexisting services and operations. Virtually any medicalspecialty can offer a type of ancillary service as a wayto generate additional revenue and improve the qual-ity of health care offered to patients. Ancillary serviceswill often offer advantages to patients through con-venience and reduced cost.
Although there are many concerns and considera-tions to review before deciding to invest in an ancillaryservice venture, it makes good sense to approach an-cillaries as an added opportunity for the existing med-ical practice or hospital’s services.
Consideration of regulatory matters is essential,and a multitude of resources for this purpose are avail-able. Chapter 2, “Facing Legal and Regulatory Issues”is a helpful start. Consult an experienced health careattorney for counsel for your specific situation beforeentering into a venture. A complete due diligence process

14 | Chapter 1: Envisioning the Opportunities
is appropriate, followed by a detailed business plan andpro forma income and cash flow statements. Prior tothe completion of the business plan, and before a deci-sion is made to enter into the ancillary service venture,a feasibility analysis may be necessary. Questions thatshould be answered include the source of the patients(or customers), the opportunities for revenue growthand expansion, and competition within the area.Demographics and the overall socioeconomic standingwithin the area in which the service will be providedare essential to know and understand prior to goinginto the actual ancillary service venture.
This chapter provides a basic outline of the key el-ements that should be considered prior to deciding toundertake an ancillary health care service venture andfurther, it reviews key functions that are necessary priorto and after opening.
The remainder of this book will consider many ofthese same specific elements. It will closely review andanalyze the various key components that need to takeplace prior to the actual opening of the ancillary serv-ice venture.
It will also explore some specific case examples,based on the following criteria:
� Type of ancillary service—Ambulatory servicecenter
� Location—Atlanta, GA (major metropolitan areain the Southeast)
� Specialties—Pain management, orthopedic sur-gery, urology, otolaryngology, ophthalmology(multispecialty)
� Number of operating rooms—Two, plus separateendoscopy
� Makeup of the ASC—Stand-alone building withattached (separately owned) medical office building
� Ownership structure—49% by physician whorepresent the previously noted surgical specialties(the physician ownership could be equal or non-equal among the physicians’ 49%; 51% owned bya local partnering hospital
� Organizational and administrative structure—ASC manager, surgical nurse manager, billing of-fice manager
� Medical director—One of the physician ownersStaff—Approximately _______
� Expansion capacity—Ability to expand to an ad-ditional two ORs
� Total initial square footage—ASC: 8000; MOB:10,000
� Total initial investment of construction and ini-tial equipment—$3 to $4 million
� Diagnostic equipment—X-ray, CT/MRI units,other
Endnotes1. Ronald N. Riner, MD. (2003). Article title. The Journal of Invasive
Cardiology, 15(3), 155.