enrollment forms packet (efp) · enrollment forms packet (efp) ... @k12.com texas virtual academy...
TRANSCRIPT
Enrollment Forms Packet (EFP)Please review the information below. Based on your student(s) grade and applicable circumstances, you are required to submit documentation in order to complete this step in the enrollment process. You can fax, scan and email, or mail the required paperwork .
Important Note: Please send copies, do not mail the original documents
Fax (preferred): Scan and Email: Mail: 1-877-257-4612 [email protected] Texas Virtual Academy 2300 Corporate Park Drive, Ste 200
Herndon, VA 20171
Texas Virtual Academy Enrollment Processing Center2300 Corporate Park Drive, Ste 200 Herndon, VA 20171Ph. 877.554.1084Fx. 877.257.4612www.k12.com/txva
Required For? Item Description Provided by?
Required for all Students
Proof of Prior Texas Public
You must submit a proof of prior public in a Texas public school. Items (Report Card, Transcript, and/ Verifica-tion of Enrollment Form filled out by your previous Texas public school for the 2012-2013 School year. * Verification of Enrollment Form provided in this packet. This form must be filled out by your students previous school personnel.
Provided by you
Proof of Age Official Birth Certificate (not the hospital issued certificate) Provided by you
Legal Guardian Drivers License or State ID Please submit a copy of the Legal Guardian’s Drivers License or State ID. Provided by you
Proof of Residency Two forms of Proof of Residency: Current Utility bill showing service address, Mortgage statement/Rental contract including signature page, recent tax statement. Provided by you
Proof of Internet Proof of Internet service. Provided by you
RES Student Enrollment Application Complete this form and submit. Provided in this
packet
Immunization Record Current Immunization Record Provided by you
Home Language Survey Complete this form and submit. Provided in this packet
Occupational Survey Complete this form and submit. Provided in this packet
Ethnicity and Race Questionnaire Please write your student’s name, as it was entered on the application. Provided in this
packet
Student Record ReleaseBy filling out this form, you are giving our school permission to request your student’s official records from their previous school after the approval process. If your child was Homeschooled please indicate it on the form, fill out the top portion and sign it.
Provided in this packet
State Compensatory Form Complete this form and submit (Example page included for instructions on how to complete this form) Provided in this
packet
Affidavit of Student Residency Complete this form and submit. Provided in this
packet
ESL Parent Permission Letter Complete this form and submit Provided in this
packet
Special Education Complete this form and submit. Provided in this packet
504 Plan Complete this form and submit. Provided in this packet
Student Health History Complete this form and submit. Provided in this packet
At Risk Indicators Complete this form and submit. Provided in this packet
Recommended for 3rd, 5th and 7th Graders
Vision and Screening Hearing Please submit proof that your student has completed their vision and hearing screening from previous school. Provided by you
Recommended for 6th and 9th Graders Spinal Screenin Please submit proof that your student has completed their spinal screening from previous school. Provided by you
Recommended for All Students
Report Card The most recent Report Card Provided by you
Social Security Card Please note do not send actual card, please submit a copy Provided by You
Recommended for all rising 10 -11th Grade Students
TranscriptsYou will need to request an unofficial transcript from your student’s current school, which will show your stu-dent’s academic standing. This is required in order to place all 10th through 11th graders. Once your student is approved, we will receive the official transcript directly from the school.
Provided by you
Recommended for stu-dent with an IEP or other Special Education needs
IEP A copy of your student’s current IEP (Individualized Education Plan). Because the IEP expires yearly, please submit the current IEP. * Highly recommended to submit with enrollment documents. Provided by you
Evaluation Report The Evaluation Report is valid for 3 years. If you do not have a copy of your student’s ER, you can request a copy from your student’s current school. * Highly recommended to submit with enrollment documents. Provided by you
Recommended for students that have a 504 plan
504 Accommodation Plan A copy of your student’s current 504 Accommodation Plan. Because the 504 expires yearly, please submit the current 504. * Highly recommended to submit with enrollment documents. Provided by you

2013-14
STUDENT ENROLLMENT APPLICATION
(PLEASE PRINT)
Student’s Name _____________________________________________ Application Date ____ / ____ / ______
Last First MI
Address _________________________________________________________________________________
City _______________________________________ State _____________________ ZIP________________
Home Phone _______________ Cell Phone ________________ Social Security # ______ - ____ - ______
Gender (circle one): M F Date of birth ____ / ____ / ____ Age ______ Last grade completed _______
School District in which student resides: ____________________________ ___________________ School Name ISD *Local school the student is zoned to attend in relation to current residence and current grade level.
Last School Attended:
School Name_______________________________________ Phone (______) ______ - ______________
Address _________________________________________________________________________________
City _______________________________________ State ___________________ ZIP________________
Father’s name ___________________________________________________ Living with student? __________
Employer ________________________________________________________________________________
Address _________________________________________________________________________________
City ________________________________ State ____ Zip _________ Home Phone _________________
Work phone (______) ______ - __________ Cellular phone/Pager/Etc. (______) ______ - ____________
Driver’s License # ____________________ (State)________ Email_________________________________
Mother’s name __________________________________________________ Living with student? ___________
Employer ________________________________________________________________________________
Address _________________________________________________________________________________
City ________________________________ State ____ Zip ________ Home Phone __________________
Work phone (______) ______ - __________ Cellular phone/Pager/Etc. (______) ______ - ____________
Driver’s License # ____________________ (State)_________ Email________________________________
Alternate Contact (Name) _________________________________ (Relationship)________________________
Home Phone____________________ Work Phone__________________ Cell Phone___________________
Emergency Contact (Name) __________________________________ (Relationship)______________________
Home Phone____________________ Work Phone___________________ Cell Phone__________________
How were you (was your student) referred to ResponsiveEd? __________________________________________ ________________________________________________________________________________________ Legal Alert: Is anyone legally restricted from contact with your student? (Circle one) Yes No Are copies of documents on file? (Circle one) Yes No
[Please continue on back]
For Administrative Use Only:
Official Enrollment Date _____/ _____/ _____ Official Withdrawal Date _____/ _____/ _____ (Official enrollment date is first day of attendance; official withdrawal date is indicated on withdrawal form and attendance records.)

2013-14
A person who knowingly falsifies information on a form required for a student’s enrollment in Responsive Education Solutions shall be liable to RES if the student is not eligible for enrollment and is enrolled on the basis of false information. For the period in which the student is enrolled, the person is liable for the maximum tuition fee the District may charge or the amount the District has budgeted per student as maintenance and operating expense, whichever is greater. Texas Education Code § 25.031(g)
Student signature_______________________________________________________ Date____/ _____ / _____
(Custodial) Parent/Guardian signature ______________________________________ Date____ / _____ / _____
I affirm that I have seen and reviewed enrollment and residency information of the above student.
Registrar signature _____________________________________________________ Date____ / _____ / _____
Affidavit of Student Residency Student (Last Name) (First Name) (Middle Name)
Student lives with the following person(s):
_______________________________________ and/or_________________________________________ First and Last name of Father/Stepfather/Grandfather/Other First and Last name of Mother/Stepmother/Grandmother/Other (Circle one) (Circle one)
At the Following Address:
__________________________________________________________________ _________________ Street Address City Zip Phone Texas Education Code § 25.001 authorizes Texas school districts to obtain evidence that a person is eligible to attend the public schools of the district at the time of enrollment. To be eligible for continued enrollment in Responsive Education Solutions, the parent or guardian of a student must show proof of residency at the time of enrollment . To comply with residency requirements, the parent or guardian of a student must return this document to Responsive Education Solutions with an original of at least two of the following documents showing name and verifiable current address. (Documents showing evidence of any alteration will not be accepted.) Parent / Guardian must provide at least two (2) of the following documents: _______ Current Utility Bill in parent/guardian’s name _______ Current Texas Driver’s License with current residential address _______ Executed lease agreement _______ Deed of Sale ________ Tax Statement ____________________________________________ ____________________________ Signature of Parent or Guardian Date I affirm that I have seen and reviewed the verification of residency. _______________________________________, ____________________________ __________________________ Signature of School Official Position Date
Notice of Compulsory Attendance Law This notice is to advise you that according to Section 25.085 of the Texas Education Code, children between the ages of six (6) and their 18th birthday are required to attend school on a daily basis unless specifically exempted by Section 25.086. A child who is required to attend school under this section shall attend school each day for the entire period the program of instruction is provided. The law places the responsibility on parents or those who stand in parental relationship to see that children attend school regularly. Any parent or person failing to require his child to attend school as required by law may be subject to a fine–an offense under this section is a Class C Misdemeanor and is punishable by a fine of UP TO $500 for each offense. Section 25.095 states that a parent will be notified in writing if a child is absent 10 days or parts of days during a six-month period or three (3) or more days or parts of days during a four-week period. Responsive Education Solutions will enforce these laws as stated by the Education Code and will report all offenses to the local authorities. By signing below I am acknowledging the receipt of this notification.
Photo / Video Release I, (Name of parent / guardian) _______________________________, do hereby give or grant permission to and assign all rights in and to any photographs, motion pictures, video footage, and/or audio recordings that may be taken of my child during his/her attendance at Responsive Education Solutions that may be used for promotional or training purposes. I hereby authorize the above-named entities to reproduce, copy, exhibit, publish, and distribute any and all photographs, motion pictures, video footage, and/or audio recordings for the sole purpose of promoting the RES learning system or training and professional development of staff. I certify that I am over the age of twenty-one (21). (Signed) ___________________________________________________ parent / guardian PLEASE NOTE: Signing this form is not a condition of enrollment. ResponsiveEd, however, greatly appreciates your cooperation.

2013-14
AT-RISK INDICATORS/DOCUMENTATION
Student Name ______________________________________________ Date __________________
A student at risk of dropping out of school includes each student who is under 21 years of age and who:
(Check yes or no)
YES NO 1. Is in prekindergarten, kindergarten or grade 1, 2, or 3 and did not perform satisfactorily on a readiness test or assessment instrument administered during the current school year. 2. Is in grade 7, 8, 9, 10, 11, or 12 and did not maintain an average equivalent to 70 on a scale of 100 in two or more subjects in the foundation curriculum during a semester in the preceding or current school year or is not maintaining such an average in two or more subjects in the foundation curriculum in the current semester. 3. Was not advanced from one grade level to the next for one or more school years.
4. Did not perform satisfactorily on an assessment instrument [TAAS/TAKS] administered to the student under TEC Subchapter B, Chapter 39, and who has not in the previous or current school year subsequently performed on that instrument or another appropriate instrument at a level equal to at least 110 percent of the level of satisfactory performance on that instrument. 5. Is pregnant or is a parent. 6. Has been placed in an alternative education program in accordance with TEC §37.006 during the preceding or current school year. 7 Has been expelled in accordance with TEC §37.007 during the preceding or current school year. 8. Is currently on parole, probation, deferred prosecution, or other conditional release.
9. Was previously reported through the Public Education Information Management System (PEIMS) to have dropped out of school. 10. Is a student of limited English proficiency, as defined by TEC §29.052. 11. Is in the custody or care of the Department of Protective and Regulatory Services or has, during the current school year, been referred to the department by a school official, officer of the juvenile court, or law enforcement official. 12. Is homeless, as defined by 42 U.S.C. Section 11302, and its subsequent amendments; or 13. Resided in the preceding school year or resides in the current school year in a residential placement facility in the district, including a detention facility, substance abuse treatment facility, emergency shelter, psychiatric hospital, halfway house, or foster group home. The student is at-risk. (Check Yes or No) Principal Signature: __________________________________________ Date: __________________________ Parent/Guardian Signature: ___________________________________ Date: __________________________

Texas Education Agency
Texas Public School Student/Staff Ethnicity and Race Data Questionnaire
The United States Department of Education (USDE) requires all state and local education institutions to collect data on ethnicity and race for students and staff. This information is used for state and federal accountability reporting as well as for reporting to the Office of Civil Rights (OCR) and the Equal Employment Opportunity Commission (EEOC). School district staff and parents or guardians of students enrolling in school are requested to provide this information. If you decline to provide this information, please be aware that the USDE requires school districts to use observer identification as a last resort for collecting the data for federal reporting. Please answer both parts of the following questions on the student’s or staff member’s ethnicity and race. United States Federal Register (71 FR 44866). Part 1. Ethnicity: Is the person Hispanic/Latino? (Choose only one.)
Hispanic/Latino – A person of Cuban, Mexican, Puerto Rican, South or Central American, or other Spanish culture or origin, regardless of race
No Hispanic/Latino Part 2. Race: What is the person’s race? (Choose one or more.)
American Indian or Alaska Native – A person having origins in any of the original peoples of North and South America (including Central America) and who maintains a tribal affiliation or community attachment
Asian – A person having origins in any of the original peoples of the Far East, Southeast Asia, or the Indian subcontinent including, for example, Cambodia, China, India, Japan, Korea, Malaysia, Pakistan, the Philippine Islands, Thailand, and Vietnam
Black or African American – A person having origins in any of the black racial groups of Africa
Native Hawaiian or Other Pacific Islander – A person having origins in any of the original peoples of Hawaii, Guam, Samoa, or other Pacific Islands
White – A person having origins in any of the original peoples of Europe, the Middle East, or North Africa
________________________________ Student/Staff Name (please print)
________________________________ Parent or Guardian/Staff Signature
________________________________ Student/Staff Identification number
________________________________ Date
Texas Education Agency – March 2009

2013-14
All questions must be answered completely. PLEASE PRINT Las preguntas deberán ser respondidas por completo. FAVOR ESCRIBIR EN LETRA DE MOLDE
Schools are required by Texas law to determine the following information for all students. Please help us meet this requirement by answering every question and signing and dating the form. A parent, guardian or student may sign when the student is in ninth grade or higher; otherwise, a parent or guardian must sign. 1. In what month and year did the student first enroll in a school in the United States? ___________ _________ Month Year 2. In what city, state, and country was the student born? ____________________ ___________ ___________ City State Country 3. What language is spoken in your home most of the time?______________________________ 4. What language does the student speak most of the time?______________________________ 5. Does the parent of guardian need to communicate with the school in a language other than English? _______ If yes, write the name of the language. ________________________________________________________
Student / Estudiante___________________________________________________ Age / Edad __________ Campus / Escuela ____________________________________________________ Grade / Grado ________
Home Language Survey
Cuestionario del Idioma en el Hogar OR…
Bajo la Ley de Texas se requiere que las escuelas determinen la siguiente información por cada estudiante. Por favor, ayúdenos por contestar cada pregunta y por firmar y notar la fecha. Cuando el estudiante esté cursando el noveno grado o uno más alto, pueden firmar el padre, la madre, el guardián, o el estudiante. De otra manera, solamente pueden firmar los padres o los guardianes. 1. ¿En qué mes y año se inscribió el estudiante por primera vez en Los Estados Unidos? ___________ _________ Mes Año 2. ¿En qué ciudad, estado, y país nació el estudiante? ____________________ ___________ ___________ Ciudad Estado o provincia País 3. ¿Cuál es el idioma que más se habla en su casa? ______________________________ 4. ¿Cuál es el idioma que más habla el estudiante? ______________________________ 5. Necesitará el padre, la madre, o el guardián comunicarse con la escuela utilizando un idioma que no sea el Inglés? Subraye la respuesta correcta. Sì No Si es así, favor escribir el nombre del idioma. __________________________________
Signature (Firma)_________________________________________ Date (Fecha)___________

2013-14
School Year: 20___ - 20___
Occupational Survey Your Children May Be Eligible for Extra Services
IMPORTANT: Please complete the survey below and return it to your school office. Name of Student_____________________________________________Grade________________ Within the past three (3) years, has your child(ren) traveled or moved alone with a parent, relative, guardian, or a spouse so that a family member could look for or do temporary or seasonal agricultural work or employment?
Yes ____ No ___
Signature of Parent/Guardian_____________________________ Date ___________________________ If No, please stop here and hand this survey back to your school district. If YES, please () the type of employment and complete the following contact information below. ___a. Farming ___b. Ranching ___c. Fencing ___d. Dairying ___e. Fishing
___f. Picking fruit or vegetables ___g. Cotton farming/ginning ___h. Combining/harvesting grain ___i. Driving tractors, machinery ___j. Tree growing or harvesting ___k. Food processing in plants
___l. Plant nursery ___m. Poultry production ___n. Clearing land ___o. Picking pecans, etc. ___p. Bailing hay ___q. Other similar work
Contact Information
Name of Child(ren)____________________________________________________________________
___________________________________________________________________________________
Father/Guardian __________________________ Mother/Guardian______________________________ Home Address________________________________________________________________________ Street City State ZIP Home Phone (____) _________________________ Other Phone (____) __________________________

2013-14
School Year: 20___ - 20__ Formulario De Trabajo
Sus Hijos Podrían Recibir Servicios Extras IMPORTANTE: Por favor complete este formulario y regréselo a la escuela. Nombre de Estudiante ______________________________ Grado/Curso _________________ ¿Durante los últimos tres (3) años, viajó o se fue su hijo/a a vivir solo/a con sus padres, algún guardián legal, o esposo/a para que alguno de la familia buscara o encontrara trabajo temporal en la agricultura?
Sí ____ No ___
Firma de Padres/Guardían __________________________________Fecha _______________________ Si contestó No, no es necesario seguir completando este formulario. Sólo regréselo a la escuela, a la brevedad. Si contestó Sí, por favor indique con un () y complete la siguiente información de contacto abajo. ___a. En la cosecha ___b. En ranchos/
ranchería ___c. En las cercas ___d. En lecherías ___e. En la pesca
___f. Recogiendo frutas/verduras ___g. En el algodón ___h. Cosechando granos ___i. En el manejo de tractores, maquinaria ___j. Plantando árboles ___k. Procesando comida en fábricas
___l. En guardería de plantas ___m. En producción de aves ___n. Limpiando terrenos ___o. Recogiendo nuez, etc. ___p. Recogiendo paja ___q. Algún otro trabajo similar
Referencia
Hijo(s)______________________________________________________________________________
____________________________________________________________________________________
Padre/Guardián ____________________________Madre/Guardián_____________________________ Domicilio____________________________________________________________________________ Calle Ciudad Estado ZIP Teléfono del hogar (____) _____________________ Otro teléfono (____) _________________________
2013-14
ESL PARENT PERMISSION LETTER
I, _____________________________, (print name of parent/guardian) hereby give
permission for my child, ________________________________, (print name of child) to
receive extra help in English as a Second Language as part of a Responsive Education
Solutions English as a Second Language (ESL) program if he/she is found to be limited
in either oral or cognitive and academic English proficiency skills. If any language other
than English is spoken at home, Responsive Education Solutions will evaluate my
student’s oral English language skills with a short Oral Language Proficiency Test and
his/her academic and cognitive English with a Norm-Referenced test of Language Arts
and Reading skills as required by Texas State Law.
[Para aquellos que hablan Español (For those who speak Spanish):]
Yo, _____________________________(nombre del padre, madre, o guardián)
Doy permiso para que mi hijo/a ________________________________(nombre del
niño/a) reciba instrucción en el Programa de Inglés como Segundo Idioma si en él/ella
se encuentre una proficiencia limitada en el idioma de Inglés.
Please sign below (Favor de firmar abajo): ________________________________________________ ____________________ Parent/Guardian Name (Nombre del Padre, Madre, o Guardián) Date (Fecha)
_______________________________________________________ Parent/Guardian Phone Number (Número de teléfono del Padre, Madre, Guardián):

STUDENTNAME:___________________________________________________DATEOFBIRTH:________________________________
201σ‐201τSTUDENTENROLLMENTPACKET PAGE5OF11
SPECIALEDUCATIONWasStudentreceivingSpecialEducation servicesatthelastschoolStudentattended?CheckOne: Yes No
If“Yes,”thenpleasecompletethefollowing:
Checkallthatapply:
ContentMastery/ResourceRoom
Counseling
SpeechTherapy
Occupational/PhysicalTherapy
BehaviorAdjustmentClass
Other:PleaseSpecify:WhatisStudent’sdisability?_________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
If“No,”thenpleasecompletethefollowing:
Has Student ever received Special Education services? Check One: Yes No If “Yes,” please specify school name, year, and disability/condition (if known):___________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
__________________________________________________________________Parent/GuardianSignature
___________________________Date

STUDENTNAME:___________________________________________________DATEOFBIRTH:________________________________
201σ‐201τSTUDENTENROLLMENTPACKET PAGE6OF11
SECTION504WasStudentreceivingSection504and/orDyslexia services/accommodationsatthelastschoolStudentattended?CheckOne: Yes No
If“Yes,”thenpleasecompletethefollowing:
Checkallthatapply:
InstructionalServices
InstructionalAccommodations
Testing/AssessmentAccommodations
Other:PleaseSpecify:
WhatisStudent’sdisability?_________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
If“No,”thenpleasecompletethefollowing:
Has Student ever received Section 504 and/or Dyslexia services? Check One: Yes No If “Yes,” please specify school name, year, and disability/condition (if known):___________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
__________________________________________________________________Parent/GuardianSignature
___________________________Date

2013-14
STUDENT HEALTH HISTORY
Date ____________________________ Student: __________________________________________________________ Phone # (_______) - _______ -_______ LAST FIRST MIDDLE
Social Security # ______ - _____ - ______ D.O.B. ____ /_____ /_______ Campus________________________________ Student resides with Parent(s) ____________________ Spouse ____________________ Other ______________________ NAME NAME NAME Is student pregnant? Yes ___ No ___ If yes, expected due date ___ / ___ / ___ Doctor _____________________________ NAME AND PHONE #
Please list student allergies to medicine, food, environmental, or other that you are aware of or suspect:
___________________________________________________________________________________________________ Please identify if student has had the following diseases by writing the age he/she had the disease on the line:
Chickenpox ________ Measles ________ Mumps ________ AGE AGE AGE
Please check any of the following illnesses, injuries, or conditions which student has had or currently has: PLEASE INDICATE IF IT IS A PAST OR PRESENT CONDITION / DOCTORS / CURRENT MEDICATION REQUIREMENTS AND PURPOSE. FAVOR DE INDICAR SI LA CONDICION ES PASADO O PRESENTE / DOCTORES / MEDICACION REQUIRIDO Y SU PROPOSITO.
___ Asthma or Lung Problems _________________________________________________________________ ASMA / PROBLEMAS DEL PULMON
___ Diabetes/Hepatitis _______________________________________________________________________ DIABETES / HEPATITIS
___ Ear/Nose/Throat _________________________________________________________________________ OIDO / NARIZ / GARGANTA
___ Epilepsy/Seizures________________________________________________________________________ EPILEPSIA / ATAQUES EPILEPTICOS
___ Fracture/Dislocation/Strain _________________________________________________________________ FRACTURAS / LUXACIONES
___ Hearing Aid/Orthopedic Braces _____________________________________________________________ APARATO AUDITIVO / ORTHOPEDICO
___ Head Injury _____________________________________________________________________________ GOLPES DE LA CABEZA
___ Heart Problems __________________________________________________________________________ PROBLEMAS DEL CORAZON
___ Kidney Problems _________________________________________________________________________ PROBLEMAS DEL RINON
___ Ulcers/Digestive _________________________________________________________________________ ULCERAS / PROBLEMAS DIGESTIVOS
___ Skin/Toes ______________________________________________________________________________ PROBLEMAS DE LA PIEL
___ Surgery ________________________________________________________________________________ CIRUGIAS
___ Other: i.e., ADHD/AIDS etc. _________________________________________________________________ OTRAS PROBLEMAS: EJEMPLO, PROBLEMAS CON ATENCION A SIDAS, ETC.
Is student currently under the care of a doctor for any problem not discussed above? Please provide details on back. SI ESTA RECIBIENDO ATENCION MEDICA POR QUALQUIER OTRA RAZON, FAVOR INDICAR CON QUIEN Y PARA QUE. NECESITAMOS LOS DETALLES.

2012-2013
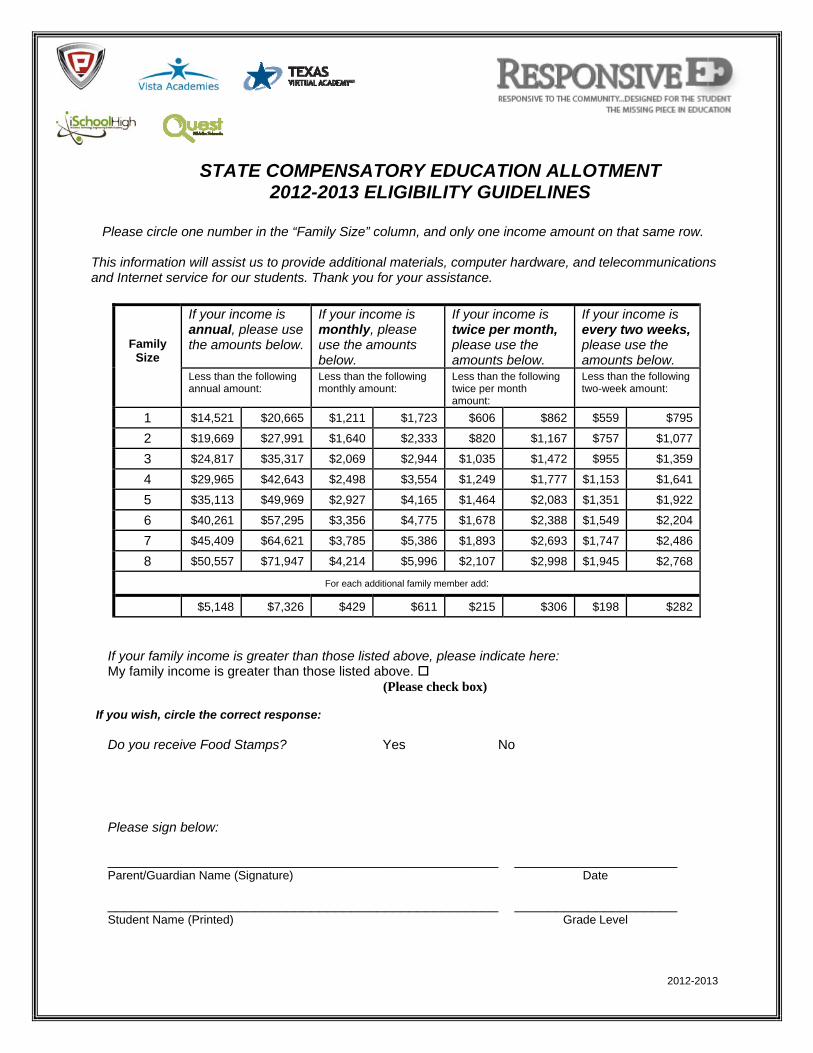
STATE COMPENSATORY EDUCATION ALLOTMENT 2012-2013 ELIGIBILITY GUIDELINES
Please circle one number in the “Family Size” column, and only one income amount on that same row. This information will assist us to provide additional materials, computer hardware, and telecommunications and Internet service for our students. Thank you for your assistance.
Family Size
If your income is annual, please use the amounts below.
If your income is monthly, please use the amounts below.
If your income is twice per month, please use the amounts below.
If your income is every two weeks, please use the amounts below.
Less than the following annual amount:
Less than the following monthly amount:
Less than the following twice per month amount:
Less than the following two-week amount:
1 $14,521 $20,665 $1,211 $1,723 $606 $862 $559 $795
2 $19,669 $27,991 $1,640 $2,333 $820 $1,167 $757 $1,077
3 $24,817 $35,317 $2,069 $2,944 $1,035 $1,472 $955 $1,359
4 $29,965 $42,643 $2,498 $3,554 $1,249 $1,777 $1,153 $1,641
5 $35,113 $49,969 $2,927 $4,165 $1,464 $2,083 $1,351 $1,922
6 $40,261 $57,295 $3,356 $4,775 $1,678 $2,388 $1,549 $2,204
7 $45,409 $64,621 $3,785 $5,386 $1,893 $2,693 $1,747 $2,486
8 $50,557 $71,947 $4,214 $5,996 $2,107 $2,998 $1,945 $2,768
For each additional family member add:
$5,148 $7,326 $429 $611 $215 $306 $198 $282
If your family income is greater than those listed above, please indicate here: My family income is greater than those listed above.
(Please check box) If you wish, circle the correct response:
Do you receive Food Stamps? Yes No Please sign below: ________________________________________________ ____________________ Parent/Guardian Name (Signature) Date ________________________________________________ ____________________ Student Name (Printed) Grade Level

2013-14
STUDENT RECORD RELEASE
DATE ____________________
To Releasing School Counselor or Registrar:
School Name: _________________________________________________ School Address: _________________________________________________ City, State, Zip: _________________________________________________ School Telephone: (______)_______________ Fax Number: (______)_______________ The following student has withdrawn from your school.
_____________________________ _________________ ______________________
Student Date of Birth Student ID #
Please forward the following information on the above student:
___ Official Transcript ___ Academic Records
___ Testing Scores/Assessment ___ Health Records
___ Special Ed Classification / Documents 504 Evaluation and Plan
___ Copy of Social Security Card ___ Copy of Birth Certificate
Copy of Original Home Language Survey and LPAC records ___ Other
Please respond to the following address:
Texas Virtual Academy
Attn: Student Records Dept.
1800 Lakeway Drive, Suite 100
Lewisville TX, 75057
972.420.1404 – Office
888.506.6777 – Fax
__________________________________ ___________________
Signature of Guardian or Registrar Date

2013-14
EMERGENCY INFORMATION ________________________________________ ______________________ Student’s Name (PRINTED) Date of Birth In case the services of a physician are required before parent/guardian can be reached, the school officials of Responsive Education Solutions are hereby authorized to take whatever action is deemed necessary for the health of my child. I also authorize ResponsiveEd school officials to directly contact the physician named below in case of an emergency. I will not hold Responsive Education Solutions or its staff responsible for emergency care and/or transportation for my child, and I will assume responsibility for any costs related to such services provided to my child. Physician’s Name: _______________________________________________________ Physician’s Phone Number: ________________________________________________ Emergency Contact Person (other than parent/guardian): ______________________________________________________________________ Emergency Contact Person’s Telephone Number: ______________________________________________________________________ I also hereby give ResponsiveEd faculty/staff permission to give the following medication to my child as indicated below. (Examples: Tylenol or acetaminophen 200 mg for headache, Ibuprofen 200 mg for headache, etc.) Medication & Dosage: ______________________________________________________________________ Medication & Dosage: ______________________________________________________________________ ________________________________________ Date: _____________________ Parent/Guardian Signature

Texas Virtual Academy Information as Reported to PID
Student Legal Name:
Student SSN or State ID: ____________________ DOB: _________________ Grade: ___________
RECEIVING SCHOOL ‐‐ PLEASE COMPLETE THE INFORMATION BELOW:
Above Student Enrolled On: _______ Above Student Did Not Enroll
Above Student Enrolled, but has withdrawn.
Enrollment Date: _____________ Withdraw Date: _______________
School Name: School Official:
Address:
First Middle
Verification of Enrollment
Last
Must be completed by previous school personnel only
Address:
Signature
Telephone: Today's Date
Is student enrolled at this school under a different name?
Yes NoIf yes, indicate name:
Is student enrolled at this school under a different SSN or State ID?
Yes NoIf yes, indicate number:
Is student enrolled at this school under a different date of birth?
Yes NoIf yes, date of birth:
Registrar Phone: (972) 420‐1404
Texas Virtual Academy
1800 Lakeway Drive, Ste 100 Fax: (888) 506‐6777
Lewisville, TX 75057
PLEASE FAX INFORMATION TO TEXAS VIRTUAL ACADEMY

2012-2013 Texas Minimum State Vaccine Requirements for Students Grades K-12
This chart summarizes the vaccine requirements incorporated in the Texas Administrative Code (TAC), Title 25 Health Services, Sections 97.61 to 97.72. This chart is not intended as a substitute for consulting the TAC, which has other provisions and details. Click here for complete TAC language.
The Department of State Health Services (DSHS) is granted authority to set immunization requirements by the Texas Education Code, Chapter 38, Health & Safety, Subchapter A, General Provisions.
IMMUNIZATION REQUIREMENTS
A student shall show acceptable evidence of vaccination prior to entry, attendance, or transfer to a child-care facility or public or private elementary or secondary school in Texas.
Vaccine Required (Attention to notes and footnotes)
Minimum Number of Doses Required by Grade Level NOTES
K - 3rd 4th- 6th 7th 8th - 10th 11th - 12th
Diphtheria/Tetanus/Pertussis (DTaP/DTP/DT/Td/Tdap)1
5 doses or 4 doses
5 doses or 4 doses
3 dose primary
series and 1 Tdap/Td
booster within last
5 years
3 dose primary series and 1 Tdap/Td booster
within last 10 years
5 doses of diphtheria-tetanus-pertussis vaccine; one dose must have been received on or after the 4th birthday. However, 4 doses meet the requirement if the 4th dose was received on or after the 4th birthday. For students aged 7 years and older, 3 doses meet the requirement if one dose was received on or after the 4th birthday. For 7th grade: 1 dose of Tdap is required if at least 5 years have passed since the last dose of tetanus- containing vaccine. For 8th- 12th grade: 1 dose of Tdap is required when 10 years have passed since the last dose of tetanus-containing vaccine. Td is acceptable in place of Tdap if a medical contraindication to pertussis exists.
Polio1 4 doses or
3 doses 4 doses or
3 doses 4 doses or
3 doses 4 doses or
3 doses 4 doses or
3 doses
4 doses of polio; one dose must be received on or after the 4th birthday. However, 3 doses meet the requirement if the 3rd dose was received on or after the 4th birthday.
Measles, Mumps, and Rubella1,2 (MMR)
2 doses 2 doses 2 doses
2 doses
The first dose of MMR must be received on or after the 1st birthday. For K - 3rd grade, 2 doses of MMR are required. For 4th - 12th grade, 2 doses of a measles-containing vaccine, and one dose each of rubella and mumps vaccine is required.
Hepatitis B2 3 doses 3 doses 3 doses 3 doses 3 doses For students aged 11-15 years, 2 doses meet the requirement if adult hepatitis B vaccine (Recombivax) was received. Dosage and type of vaccine must be clearly documented. (Two 10 mcg/1.0 ml of Recombivax).
Varicella1,2,3 2 doses 1 dose 2 doses 1 dose
The first dose of varicella must be received on or after the first birthday. For grades K – 3rd and 7th - 10th 2 doses are required. 1 dose is required for all other grade levels. For any student who receives the first dose on or after 13 years of age, 2 doses are required.
Meningococcal 1 dose
Hepatitis A1,2 2 doses The first dose of hepatitis A must be received on or after the first birthday.
1 Receipt of the dose up to (and including) 4 days before the birthday will satisfy the school entry immunization requirement. 2 Serologic confirmation of immunity to measles, mumps, rubella, hepatitis B, hepatitis A, or varicella or serologic evidence of infection is acceptable in place of vaccine. 3 Previous illness may be documented with a written statement from a physician, school nurse, or the child's parent or guardian containing wording such as: "This is to verify that (name of student) had varicella disease (chickenpox) on or about (date) and does not need varicella vaccine." This written statement will be acceptable in place of any and all varicella vaccine doses required.

Exemptions The law allows (a) physicians to write a statement stating that the vaccine(s) required would be medically harmful or injurious to the health and well-being of the child or household member, and (b) parents/guardians to choose an exemption from immunization requirements for reasons of conscience, including a religious belief. The law does not allow parents/guardians to elect an exemption simply because of inconvenience (for example, a record is lost or incomplete and it is too much trouble to go to a physician or clinic to correct the problem). Schools and child-care facilities should maintain an up-to-date list of students with exemptions, so they may be excluded in times of emergency or epidemic declared by the commissioner of public health. Instructions for requesting the official exemption affidavit that must be signed by parents/guardians choosing the exemption for reasons of conscience, including a religious belief, can be found at www.ImmunizeTexas.com. Original Exemption Affidavit must be completed and submitted to the school or child-care facility. For children claiming medical exemptions, a written statement by the physician must be submitted to the school or child-care facility. Provisional Enrollment All immunizations should be completed by the first date of attendance. The law requires that students be fully vaccinated against the specified diseases. A student may be enrolled provisionally if the student has an immunization record that indicates the student has received at least one dose of each specified age-appropriate vaccine required by this rule. To remain enrolled, the student must complete the required subsequent doses in each vaccine series on schedule and as rapidly as is medically feasible and provide acceptable evidence of vaccination to the school. A school nurse or school administrator shall review the immunization status of a provisionally enrolled student every 30 days to ensure continued compliance in completing the required doses of vaccination. If, at the end of the 30-day period, a student has not received a subsequent dose of vaccine, the student is not in compliance and the school shall exclude the student from school attendance until the required dose is administered. Documentation Since many types of personal immunization records are in use, any document will be acceptable provided a physician or public health personnel has validated it. The month, day, and year that the vaccination was received must be recorded on all school immunization records created or updated after September 1, 1991.
Texas Department of State Health Services • Immunization Branch • MC-1946 • P O Box 149347 • Austin, TX 78714-9347 • (800) 252-9152 Stock# 6-14 Rev. 01/24/2012
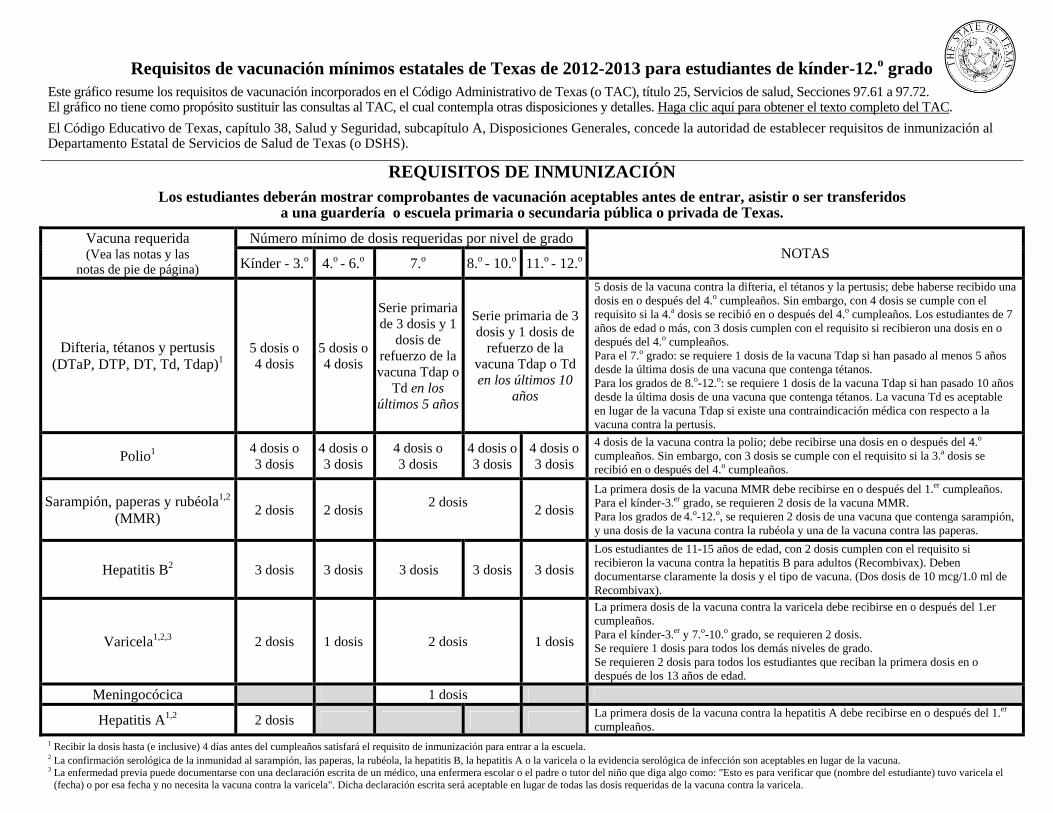
Requisitos de vacunación mínimos estatales de Texas de 2012-2013 para estudiantes de kínder-12.o grado
Este gráfico resume los requisitos de vacunación incorporados en el Código Administrativo de Texas (o TAC), título 25, Servicios de salud, Secciones 97.61 a 97.72. El gráfico no tiene como propósito sustituir las consultas al TAC, el cual contempla otras disposiciones y detalles. Haga clic aquí para obtener el texto completo del TAC.
El Código Educativo de Texas, capítulo 38, Salud y Seguridad, subcapítulo A, Disposiciones Generales, concede la autoridad de establecer requisitos de inmunización al Departamento Estatal de Servicios de Salud de Texas (o DSHS).
REQUISITOS DE INMUNIZACIÓN Los estudiantes deberán mostrar comprobantes de vacunación aceptables antes de entrar, asistir o ser transferidos
a una guardería o escuela primaria o secundaria pública o privada de Texas.
Vacuna requerida (Vea las notas y las
notas de pie de página)
Número mínimo de dosis requeridas por nivel de grado NOTAS
Kínder - 3.o 4.o - 6.o 7.o 8.o - 10.o 11.o - 12.o
Difteria, tétanos y pertusis (DTaP, DTP, DT, Td, Tdap)1
5 dosis o 4 dosis
5 dosis o 4 dosis
Serie primaria de 3 dosis y 1
dosis de refuerzo de la vacuna Tdap o
Td en los últimos 5 años
Serie primaria de 3 dosis y 1 dosis de
refuerzo de la vacuna Tdap o Td en los últimos 10
años
5 dosis de la vacuna contra la difteria, el tétanos y la pertusis; debe haberse recibido una dosis en o después del 4.o cumpleaños. Sin embargo, con 4 dosis se cumple con el requisito si la 4.a dosis se recibió en o después del 4.o cumpleaños. Los estudiantes de 7 años de edad o más, con 3 dosis cumplen con el requisito si recibieron una dosis en o después del 4.o cumpleaños. Para el 7.o grado: se requiere 1 dosis de la vacuna Tdap si han pasado al menos 5 años desde la última dosis de una vacuna que contenga tétanos. Para los grados de 8.o-12.o: se requiere 1 dosis de la vacuna Tdap si han pasado 10 años desde la última dosis de una vacuna que contenga tétanos. La vacuna Td es aceptable en lugar de la vacuna Tdap si existe una contraindicación médica con respecto a la vacuna contra la pertusis.
Polio1 4 dosis o 3 dosis
4 dosis o 3 dosis
4 dosis o 3 dosis
4 dosis o 3 dosis
4 dosis o 3 dosis
4 dosis de la vacuna contra la polio; debe recibirse una dosis en o después del 4.o cumpleaños. Sin embargo, con 3 dosis se cumple con el requisito si la 3.a dosis se recibió en o después del 4.o cumpleaños.
Sarampión, paperas y rubéola1,2 (MMR)
2 dosis 2 dosis 2 dosis
2 dosis
La primera dosis de la vacuna MMR debe recibirse en o después del 1.er cumpleaños. Para el kínder-3.er grado, se requieren 2 dosis de la vacuna MMR. Para los grados de 4.o-12.o, se requieren 2 dosis de una vacuna que contenga sarampión, y una dosis de la vacuna contra la rubéola y una de la vacuna contra las paperas.
Hepatitis B2 3 dosis 3 dosis 3 dosis 3 dosis 3 dosis
Los estudiantes de 11-15 años de edad, con 2 dosis cumplen con el requisito si recibieron la vacuna contra la hepatitis B para adultos (Recombivax). Deben documentarse claramente la dosis y el tipo de vacuna. (Dos dosis de 10 mcg/1.0 ml de Recombivax).
Varicela1,2,3 2 dosis 1 dosis 2 dosis 1 dosis
La primera dosis de la vacuna contra la varicela debe recibirse en o después del 1.er cumpleaños. Para el kínder-3.er y 7.o-10.o grado, se requieren 2 dosis. Se requiere 1 dosis para todos los demás niveles de grado. Se requieren 2 dosis para todos los estudiantes que reciban la primera dosis en o después de los 13 años de edad.
Meningocócica 1 dosis
Hepatitis A1,2 2 dosis La primera dosis de la vacuna contra la hepatitis A debe recibirse en o después del 1.er cumpleaños.
1 Recibir la dosis hasta (e inclusive) 4 días antes del cumpleaños satisfará el requisito de inmunización para entrar a la escuela. 2 La confirmación serológica de la inmunidad al sarampión, las paperas, la rubéola, la hepatitis B, la hepatitis A o la varicela o la evidencia serológica de infección son aceptables en lugar de la vacuna. 3 La enfermedad previa puede documentarse con una declaración escrita de un médico, una enfermera escolar o el padre o tutor del niño que diga algo como: "Esto es para verificar que (nombre del estudiante) tuvo varicela el
(fecha) o por esa fecha y no necesita la vacuna contra la varicela". Dicha declaración escrita será aceptable en lugar de todas las dosis requeridas de la vacuna contra la varicela.
Exenciones La ley permite que (a) los médicos redacten una declaración en la que expongan que la vacuna o vacunas requeridas serían médicamente dañinas o perjudiciales para la salud y el bienestar del niño o de una persona que vive en la casa y que (b) los padres o tutores elijan una exención de los requisitos de inmunización por razones de conciencia, incluso creencias religiosas. La ley no permite que los padres o tutores elijan una exención simplemente por inconveniencia (por ejemplo, si se pierde un registro o éste está incompleto y sería mucha molestia ir con un médico o clínica para corregir el problema). Las escuelas y las guarderías deben mantener una lista actualizada de los estudiantes con exenciones, de forma que se les pueda excluir durante emergencias o epidemias declaradas por el director de salud pública. Encontrará instrucciones para solicitar la declaración jurada de exención oficial que debe ser firmada por los padres o tutores que elijan la exención por razones de conciencia, incluso creencias religiosas, en www.ImmunizeTexas.com. La declaración jurada de exención original debe rellenarse y presentarse a la escuela o guardería. En el caso de los niños que soliciten exenciones médicas, deben presentar una declaración escrita del médico a la escuela o guardería. Inscripción provisional Todas las inmunizaciones se deben finalizar antes de la primera fecha de asistencia. La ley exige que los estudiantes estén completamente vacunados contra las enfermedades señaladas. Un estudiante se puede inscribir provisionalmente si el estudiante cuenta con registro de inmunización que indique que el estudiante ha recibido al menos una dosis de cada vacuna apropiada para la edad específica que esta regla exija. Para seguir inscrito, el estudiante debe completar las dosis posteriores requeridas de cada serie de vacunas conforme al calendario y tan rápidamente como sea médicamente posible y proveer comprobante suficiente de la vacunación a la escuela. Una enfermera escolar o un administrador escolar revisará el estado de inmunización de un estudiante inscrito provisionalmente cada 30 días para garantizar el cumplimiento ininterrumpido en la finalización de las dosis de vacunas requeridas. Si, al final del periodo de 30 días, un estudiante no ha recibido una dosis posterior de la vacuna, el estudiante no está cumpliendo y la escuela excluirá al estudiante para que no asista a la escuela hasta que se administre la dosis requerida. Documentación Dado que se usan muchos tipos de registros de inmunización personales, cualquier documento es aceptable si un médico o el personal de salud pública lo ha validado. Debe registrarse el mes, día y año en que se recibió la vacuna en todos los registros de inmunización escolares creados o actualizados después del 1 de septiembre de 1991.
Texas Department of State Health Services • Immunization Branch • MC-1946 • P O Box 149347 • Austin, TX 78714-9347 • (800) 252-9152 Stock No. 6-14 Rev. 01/24/ 2012