endoscopic ultrasound-guided fine-needle aspiration of lymph nodes: the hennepin county medical...
TRANSCRIPT

Endoscopic Ultrasound-GuidedFine-Needle Aspiration of LymphNodes: The Hennepin CountyMedical Center ExperienceEdward B. Stelow, M.D.,
1* Rebecca Lai, M.D.,2 Ricardo H. Bardales, M.D.,
1
Shawn Mallery, M.D.,2 Bradley M. Linzie, M.D.,
1 Gretchen Crary, M.D.,1
and Michael W. Stanley, M.D.1
Endoscopic ultrasound (EUS)-guided fine-needle aspiration(FNA) allows for the sampling and diagnosis of lesions of thegastrointestinal system and adjacent tissues. It has also provedhelpful with the sampling of lymphadenopathy both for the stagingof malignancy and for the diagnosis of lymphadenopathy of othercauses. We review our experience with EUS-guided FNA of lymphnodes. The cytology files were searched at Hennepin CountyMedical Center (HCMC) for all cases of lymph nodes sampled byEUS. Clinical history, biopsy site, diagnosis, and follow-up infor-mation (including ancillary testing) were reviewed. Between Jan-uary 1, 2000 and December 5, 2002, 217 lymph nodes from 185different patients were sampled by EUS at HCMC. Biopsy sitesincluded 62 mediastinal, 9 paraesophageal, and 146 intra-abdom-inal lymph nodes. Diagnoses were as follows: metastatic non-small cell carcinoma (n � 69); benign, reactive lymph node (n �76); granulomatous lymphadenopathy (n � 18); malignant lym-phoma (n � 7); atypical–suspicious for malignancy (n � 5);metastatic small cell carcinoma (n � 2); necrotic debris (n � 4),and foreign material (n � 1); 35 cases were nondiagnostic(16.1%) in 22 of 185 patients (11.9%). Ancillary tests includingflow cytometry, cytogenetics, and cultures were performed. EUS-guided FNA of mediastinal and intra-abdominal lymph nodesprovides diagnostic material from which ancillary testing may beperformed. Diagn. Cytopathol. 2004;30:301–306.© 2004 Wiley-Liss, Inc.
Key Words: endoscopic ultrasound; fine-needle aspiration; GItract; lymph node; metastases
Endoscopic ultrasound (EUS) has proved a useful diagnos-tic modality for the investigation of the gastrointestinal (GI)tract and adjacent structures.1–10 With the use of fine-needleaspiration (FNA), this technique can achieve a good yieldwith high sensitivity and specificity for the diagnosis ofmediastinal, GI, pancreatobiliary, hepatic, adrenal, andother abdominal lesions.
The method has also been shown to be helpful with thestaging of malignancy, especially when used preoperativelyto guide therapeutic decisions for esophageal, gastric, pan-creatic and other malignancies.1–3,5,7–9,11 To date, reportsaddressing cytologic findings in EUS-guided lymph nodeFNA have been limited to small numbers of cases discussedin manuscripts that address EUS-guided FNA more gener-ally or have discussed, primarily clinically, the diagnosis ofspecific diseases.4,11–13 We review our experience withEUS-guided FNA of lymph nodes with particular attentionto clinical history, aspiration findings, and the use of ancil-lary techniques.
Materials and MethodsEUS was performed by standard methods. FNA was per-formed by the endoscopists (S.M., R.L.) with 21-gaugeand/or 25-gauge needles. A pathologist (E.B.S., R.H.B.,B.M.L., G.C., M.W.S.) then prepared slides. An air-driedslide was usually made first and stained with Diff-Quik.After immediate assessment, the specimen was triaged.Fixed slides were prepared and stained by the Papanicolaoumethod. Cell blocks (Figs. 1–6) were made by allowingmaterial to clot and then submitting it in formalin for routinehistologic methods as described by Stanley and Lowha-gen.14 Fungal and mycobacterial cultures were obtained inrare cases. Material was rarely submitted for flow cytometryor cytogenetic analysis. Cases were generally reviewed thenext day with cell block histology and ancillary test results.
1Department of Pathology and Laboratory Medicine, Hennepin CountyMedical Center, Minneapolis, Minnesota
2Division of Gastroenterology, Hennepin County Medical Center, De-partment of Medicine, Minneapolis, Minnesota
*Correspondence to: Edward B Stelow, M.D., Department of Pathology(815), Hennepin County Medical Center, 701 Park Avenue, Minneapolis,MN 55415. E-mail: [email protected]
Received 30 May 2003; Accepted 31 July 2003DOI 10.1002/dc.10405Published online in Wiley InterScience (www.interscience.wiley.com).
© 2004 WILEY-LISS, INC. Diagnostic Cytopathology, Vol 30, No 5 301

Histochemistry and immunohistochemical stains were thenperformed at the discretion of the pathologist.
The cytology files at Hennepin County Medical Center(HCMC) were searched for all cases of EUS-guided FNA oflymph nodes between January 1, 2000 and December 5,2002. All EUS and cytology reports were reviewed forclinical history, patient age, location of the adenopathysampled, number of passes performed, diagnoses, ancillarytesting and results, and clinical follow-up. Follow-up infor-mation was pursued only when applicable. Selected slideswere reviewed (Figs. 1–6).
ResultsA total of 217 lymph nodes from 185 different patients weresampled by EUS between January 1, 2000 and December 5,2002 at HCMC. The mean age of patients was 61.0 � 28.8yr (mean � 2 SD). Males outnumbered females by 125:60.Table I shows the clinical history of these patients. Sites
sampled were as follows: 62 mediastinal, 14 paraesopha-geal, 15 perigastric, 27 celiac, 2 perisplenic, 31 peripancre-atic, 47 perihepatic, 15 other intra-abdominal sites, and 4other retroperitoneal sites. The average number of passesper node was 2.2 � 2.4 (mean � 2 SD). 2.8 � 3.4 (mean �2 SD) air-dried Diff-Quik-stained slides and 1.6 � 2.4(mean � 2 SD) alcohol-fixed Papanicolaou-stained slideswere prepared per case. It was found that 120 of 217 caseshad sufficient material for a cell block. Figure 7 shows thefinal diagnoses as determined from the evaluation of allsmears, cell block sections, and ancillary testing.
Ancillary testing was performed on selected cases at thediscretion of both the pathologist and the endoscopist. Withthe exception of special stains and immunohistochemistry
Fig. 1. Typical cellularity of a benign peripancreatic lymph node (Diff-Quik stain, �100).
Fig. 2. Cell block section of same case as Fig. 1 (H&E stain, �40).
Fig. 3. Noncaseating granulomatous inflammation from a mediastinallymph node in a patient later found to have sarcoid (Diff-Quik stain,�100).
Fig. 4. Cell block specimen of and abdominal lymph found by flowcytometry and cytogenetics to be consistent with follicular lymphoma(H&E stain, �100).
STELOW ET AL.
302 Diagnostic Cytopathology, Vol 30, No 5

applied to paraffin-embedded cell block preparations, allo-cation of material for ancillary testing was accomplishedduring EUS based on immediate interpretation of aspiratesmears. Eleven cases were submitted for flow cytometrywith the following results: 1 case was hypocellular andnondiagnostic, 5 cases failed to show a clonal B-cell pop-ulation, and 5 cases showed a clonal B-cell population. Ofthe cases that showed clonal B-cell populations, 2 caseswere cytologically consistent with a large B-cell lymphoma;the 3 other cases were composed predominantly of smalllymphocytes. Of these 3 cases, 1 each showed flow cyto-metric results most consistent with mantle cell lymphoma,small lymphocytic lymphoma, and follicular lymphoma.Material was also submitted for cytogenetic analysis in thefinal case and showed the classic follicular lymphoma trans-location [t(14;18)].
Material was submitted from 13 patients for mycobacte-rial cultures. Four of these grew Mycobacterium tuberculo-sis. Material was submitted from 12 patients for fungalcultures; no noncontaminant organisms were identified.
DiscussionEndoscopic ultrasound-guided FNA has allowed for boththe preoperative staging of malignancy and the sampling oflymphadenopathy of other etiologies.1–13 Both have provedextremely helpful in the management of benign and malig-nant disease processes. This is especially true for patientswith tumors of the esophagus or pancreas, but it has alsobeen helpful with other GI malignancies and lung cancer.
Various studies have reported overall institutional andmulti-institutional findings and have shown that EUS-
Fig. 5. Metastatic pancreatic adenocarcinoma to a peripancreatic lymphnode (Diff-Quik stain, �100).
Fig. 6. Cell block of metastatic “foamy gland” pancreatic adenocarcinomato a peripancreatic lymph node (H&E stain, �400).
Table I. Clinical History of 185 Consecutive Patients With LymphNodes Aspirated by EUS
History No. of patients
Esophageal lesion 44Known carcinoma 38Barrett’s esophagus 3Undiagnosed lesion 3
Pancreatobilliary lesion 61Pancreatic carcinoma 24Other pancreatic lesion 24Bile duct stricture 8Other biliary lesion 5
Other carcinoma or lesion 37Lung cancer or mass 9Gastric carcinoma or mass 7Gastroesophageal junction carcinoma 6Hepatic carcinoma or mass 4Duodenal carcinoma 3Colon carcinoma 3Other carcinoma 5
Adenopathy of unknown cause 43
Fig. 7. Diagnoses of 217 consecutive EUS-guided aspirated lymph nodes.1, reactive lymph node; 2, metastatic non-small cell carcinoma; 3, nondi-agnostic sample; 4, granulomatous lymphadenopathy; 5, lymphoma; 6,suspicious for malignancy; 7, descriptive (necrotic debris [n � 4], foreignmaterial [n � 1]); 8, metastatic small cell carcinoma.
ENDOSCOPIC ULTRASOUND-GUIDED FNA OF LYMPH NODES
Diagnostic Cytopathology, Vol 30, No 5 303
guided FNA is a safe, sensitive, and specific diagnosticmodality.4,10 Similar to our own experience, much of thefollow-up has been clinical, however, as the diagnosis ofsamples collected by EUS often precludes further tissuesampling. For example, patients with GI malignancies andcytologically proven nodal metastases rarely go to surgery,nor do patients with cytologically proven malignancies thatshow sonographic evidence of vascular invasion. For thisreason, diagnostic yield and the rate of nondiagnostic spec-imens may be more helpful markers for the assessment ofthis technique.
Most institutions report overall nondiagnostic samplerates of 2–14%.4,10,11 Undoubtedly, these results may berelated to the skills of the endoscopists and pathologists andto the technical difficulty of cases sampled. At our institu-tion, 16% of the lymph nodes aspirated were considerednondiagnostic. However, only 12% of patients ultimatelyhad nondiagnostic studies, as some patients had multiplenondiagnostic samples and others had diagnostic samplesobtained from adjacent lymph nodes aspirated during asingle EUS procedure.
HCMC serves as both a referral center for EUS-guidedFNA and as a primary care facility for a community richwith immigrants and the indigent. As a result, we see a greatvariety of GI, mediastinal, and abdominal lesions aspiratedby EUS and are asked to diagnose both malignant andnonmalignant processes. A consequence of our position isthat many patients return to other institutions, making fol-low-up difficult to obtain.
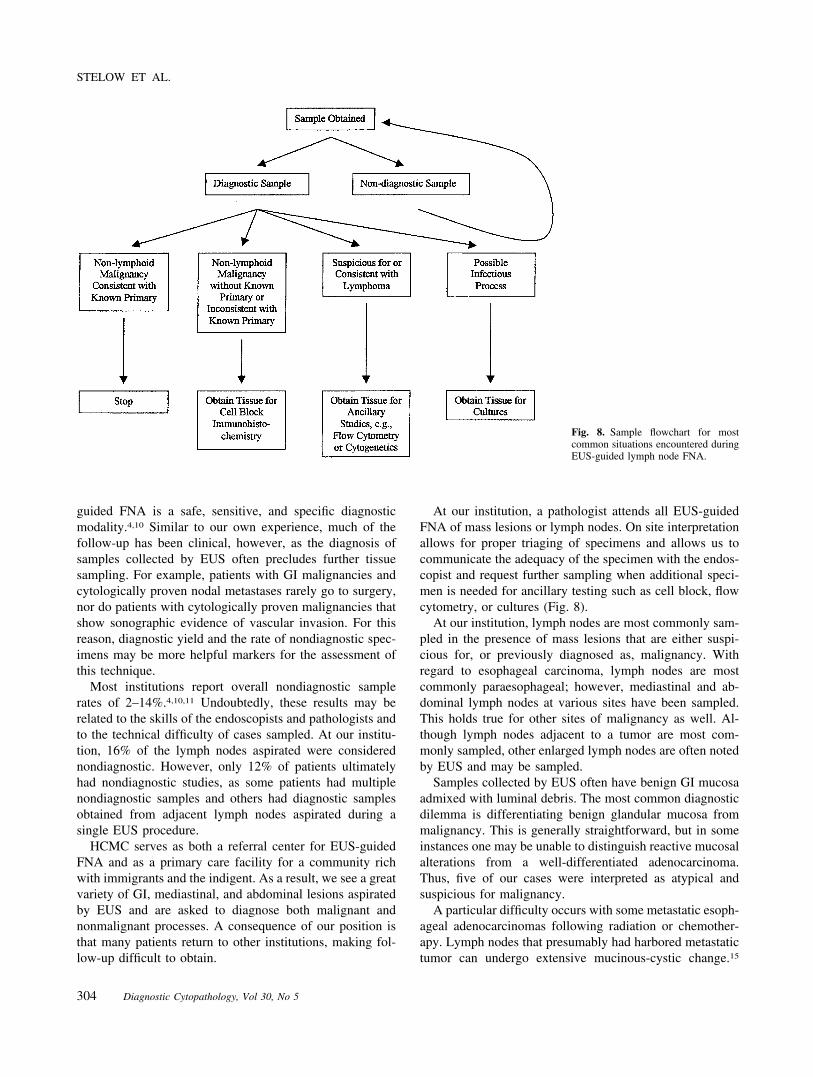
At our institution, a pathologist attends all EUS-guidedFNA of mass lesions or lymph nodes. On site interpretationallows for proper triaging of specimens and allows us tocommunicate the adequacy of the specimen with the endos-copist and request further sampling when additional speci-men is needed for ancillary testing such as cell block, flowcytometry, or cultures (Fig. 8).
At our institution, lymph nodes are most commonly sam-pled in the presence of mass lesions that are either suspi-cious for, or previously diagnosed as, malignancy. Withregard to esophageal carcinoma, lymph nodes are mostcommonly paraesophageal; however, mediastinal and ab-dominal lymph nodes at various sites have been sampled.This holds true for other sites of malignancy as well. Al-though lymph nodes adjacent to a tumor are most com-monly sampled, other enlarged lymph nodes are often notedby EUS and may be sampled.
Samples collected by EUS often have benign GI mucosaadmixed with luminal debris. The most common diagnosticdilemma is differentiating benign glandular mucosa frommalignancy. This is generally straightforward, but in someinstances one may be unable to distinguish reactive mucosalalterations from a well-differentiated adenocarcinoma.Thus, five of our cases were interpreted as atypical andsuspicious for malignancy.
A particular difficulty occurs with some metastatic esoph-ageal adenocarcinomas following radiation or chemother-apy. Lymph nodes that presumably had harbored metastatictumor can undergo extensive mucinous-cystic change.15
Fig. 8. Sample flowchart for mostcommon situations encountered duringEUS-guided lymph node FNA.
STELOW ET AL.
304 Diagnostic Cytopathology, Vol 30, No 5

When they are later sampled, only mucus may be obtained.In the few cases that we have encountered with this change,rare cytologically malignant cells were present, allowing foran accurate and definitive diagnosis of metastatic adenocar-cinoma.
The background of most sampled lymph nodes containsvarying numbers of polymorphous lymphocytes present sin-gly and in large groups that may sometimes mimic epithelialclusters. The amount of lymphoid tissue present is likelydependent on the sampling and on the degree of nodalreplacement by tumor. With biopsies that do not showneoplasm or other changes, the diagnostic threshold forcalling the biopsy benign has not been well delineated; thisholds true even for FNA of superficial lymph nodes. Un-doubtedly, the lower one’s threshold, the greater the chanceof a false-negative diagnosis. Identifying true false-negativecases is difficult in such a situation, where many patientswill not undergo surgical sampling. Furthermore, evenwhen further sampling occurs and lymph nodes are found tocontain metastatic tumor, it is difficult to determine whetherthose lymph nodes were the ones originally sampled byEUS.
We submitted samples for flow cytometry in only 11 ofthe 217 cases, which is much less often than we do whensampling superficial lymph nodes. This is because mostlymph nodes were sampled to rule out metastatic carcinomain patients with known malignancy or with lesions suspi-cious for malignancy at the time of the EUS (only 43 of the185 patients had adenopathy without other lesions). Suffi-cient material was obtained in 10 of 11 cases (91%). Theseresults are comparable with yields from superficial FNA ofpalpable lesions.16 We are aware of only one patient withlymphoma diagnosed on follow-up that was missed byEUS-guided FNA. This case had been interpreted as gran-ulomatous and was worked up for possible infectious etiol-ogies. The patient was later found to have nodular sclerosisHodgkin lymphoma. As with superficial FNA, false-nega-tive cases will occur in patients clinically suspected to havelymphoma.17 Flow cytometry would not have helped in thiscase, and it is known that Hodgkin lymphoma will occa-sionally show only granulomata on aspirates.17
Patients with infectious disease may present with medi-astinal or abdominal adenopathy. Twenty-two of the 217sampled nodes showed granulomatous inflammation or onlynecrotic debris (19 of 185 patients). Mycobacterial (13) andfungal (12) cultures were submitted based on clinical sus-picion. The remaining cases were mostly from patients withknown malignancy in whom there was no suspicion ofinfection. Four cases grew Mycobacterium tuberculosis, anddrug sensitivities were performed in all these. On follow-up,two patients with granulomatous lymphadenitis were foundto have sarcoidosis, and one was (as noted above) found tohave Hodgkin lymphoma. One case, in which initial fungal
cultures were negative, was later found to have generalizedhistoplasmosis.
Although no cases in this series required immunohisto-chemistry, we obtained cell block material in 120 of 217cases. We have found that once directed to obtain materialfor cell block, such as when dealing with submucosal GImesenchymal neoplasms, endoscopists can generally pro-cure sufficient tissue for cell block immunohistochemis-try.18,19 Since assembling this series we have diagnosedmetastatic seminoma in an abdominal lymph node with thehelp of immunohistochemistry.
We have found EUS-guided FNA an effective method forthe sampling of lymph nodes (only 12% of patients hadcompletely nondiagnostic samples) that has assisted mostwith the preoperative staging of malignancy and post-ther-apeutic identification of recurrence. When clinically indi-cated, material for flow cytometry, cytogenetics, immuno-histochemistry, and cultures can be obtained through thismethod with relatively good yields. Our experience indi-cates that many patients who undergo EUS-guided lymphnode FNA will not undergo follow-up surgical excisions.Many have unresectable malignancies, often, as shown bythe FNA itself. Thus, the traditional methods of evaluatingcytodiagnostic efficiency with histologic correlation maynot be applicable. We have noted a similar experience in ourstudy of intraductal papillary mucinous neoplasms of thepancreas, in which many patients with clinically, sono-graphically, and cytologically suspected cases are not sur-gical candidates because of age and comorbidity.20 Thissituation underscores the need for correct cytologic diagno-sis and the use of ancillary testing, which, we believe, isoptimized when the pathologist is involved with the proce-dure.
References1. Akahoshi K, Chijiiwa Y, Nakano I, Nawata H, Ogawa Y, Tanaka M,
Nagai E, Tsuneyoshi M. Diagnosis and staging of pancreatic cancer byendoscopic ultrasound. Br J Radiol 1998;71:492–496.
2. Akahoshi K, Misawa T, Fujishima H, Chijiiwa Y, Maruoka A, OhkuboA, Nawata H. Preoperative evaluation of gastric cancer by endoscopicultrasound. Gut 1991;32:479–482.
3. Chang KJ, Nguyen P, Erickson RA, Durbin TE, Katz KD. The clinicalutility of endoscopic ultrasound-guided fine-needle aspiration in thediagnosis and staging of pancreatic carcinoma. Gastrointest Endosc1997;45:387–393.
4. Chhieng DC, Jhala D, Jhala N, Eltoum I, Chen VK, Vickers S, HeslinMJ, Wilcox CM, Eloubeidi MA. Endoscopic ultrasound-guided fine-needle aspiration biopsy: a study of 103 cases. Cancer 2002;96:232–239.
5. Heintz A, Mildenberger P, Georg M, Braunstein S, Junginger T.Endoscopic ultrasonography in the diagnosis of regional lymph nodesin esophageal and gastric cancer—results of studies in vitro. Endos-copy 1993;25:231–235.
6. Jhala D, Chhieng DC, Chen V, Jhala N, Eltoum I, Eloubeida M. Yieldof endoscopic ultrasound-guided fine needle aspiration in intraabdomi-nal and mediastinal lymphadenopathy (abstract). Acta Cytol 2002;46:999–1000.
7. Palazzo L, Roseau G, Gayet B, Vilgrain V, Belghiti J, Fekete F,Paolaggi JA. Endoscopic ultrasonography in the diagnosis and staging
ENDOSCOPIC ULTRASOUND-GUIDED FNA OF LYMPH NODES
Diagnostic Cytopathology, Vol 30, No 5 305

of pancreatic adenocarcinoma. Results of a prospective study withcomparison to ultrasonography and CT scan. Endoscopy 1993;25:143–150.
8. Rice TW, Boyce GA, Sivak MV. Esophageal ultrasound and thepreoperative staging of carcinoma of the esophagus. J Thorac Cardio-vasc Surg 1991;101:536–543.
9. Rosch T, Lorenz R, Zenker K, von Wichert A, Dancygier H, Hofler H,Siewert JR, Classen M. Local staging and assessment of resectabilityin carcinoma of the esophagus, stomach, and duodenum by endoscopicultrasonography. Gastrointest Endosc 1992;38:460–467.
10. Shin HJ, Lahoti S, Sneige N. Endoscopic ultrasound-guided fine-needle aspiration in 179 cases: the M.D. Anderson Cancer Centerexperience. Cancer 2002;96:174–180.
11. Fritscher-Ravens A, Sriram PV, Bobrowski C, Pforte A, Topalidis T,Krause C, Jaeckle S, Thonke F, Soehendra N. Mediastinal lymphad-enopathy in patients with or without previous malignancy: EUS-FNA-based differential cytodiagnosis in 153 patients. Am J Gastroenterol2000;95:2278–2284.
12. Fritscher-Ravens A, Sriram PV, Topalidis T, Hauber HP, Meyer A,Soehendra N, Pforte A. Diagnosing sarcoidosis using endosonogra-phy-guided fine-needle aspiration. Chest 2000;118:928–935.
13. Ribeiro A, Vazquez-Sequeiros E, Wiersema LM, Wang KK, Clain JE,Weirsema MJ. EUS-guided fine-needle aspiration combined with flowcytometry and immunohistochemistry in the diagnosis of lymphoma.Gastrointest Endosc 2001;53:485–491.
14. Stanley MW, Lowhagen T. Fine needle aspiration of palpable masses.Boston: Butterworth-Heinemann; 1993. p 40–41.
15. Jhala D, Eloubeidi M, Eltoum I, Jhala N, Chhieng. Cytology of lymphnodes in patients status-post chemo- and/or radiation therapy withesophageal cancer: a potential diagnostic pitfall [abstract]. Acta Cytol2002;46:998–999.
16. Nicol TL, Silberman M, Rosenthal DL, Borowitz MJ. The accuracy ofcombined cytopathologic and flow cytometric analysis of fine-needleaspirates of lymph nodes. Am J Clin Pathol 2000;114:18–28.
17. Chhieng DC, Cangiarella JF, Symmans WF, Cohen J. Fine-needleaspiration cytology of Hodgkin disease: a study of 89 cases withemphasis on the false-negative cases. Cancer 2001;93:52–59.
18. Stelow EB, Lai R, Bardales RH, Linzie BM, Mallery S, Stanley MS.Endoscopic ultrasound-guided fine needle aspiration cytology of pe-ripheral nerve sheath tumors. Diagn Cytopathol 2004;30:172–177.
19. Stelow EB, Stanley MW, Mallery S, Lai R, Linzie BM, Bardales RH.Endoscopic ultrasound-guided fine needle aspiration findings of gas-trointestinal leiomyomas and gastrointestinal stromal tumors. Am JClin Pathol 2003;119:703–708.
20. Stelow EB, Bardales RH, Stanley MW, Mallery S, Lai R, Linzie BM,Pambuccian SE. Intraductal papillary mucinous neoplasms of thepancreas: the findings and limitations of cytologic samples obtained byendoscopic ultrasound-guided fine needle aspiration. Am J Clin Pathol2003;120:398–404.
STELOW ET AL.
306 Diagnostic Cytopathology, Vol 30, No 5