emotional stroop performance predicts disorganization in schizophrenia
TRANSCRIPT

www.elsevier.com/locate/schres
Schizophrenia Research
Emotional Stroop performance predicts
disorganization in schizophrenia
Laura K. Phillipsa,T, Patricia J. Deldinb, Martina M. Voglmaierc, Sarah Rabbittd
aDepartment of Psychology, Harvard University, 33 Kirkland Street Rm. 1205, Cambridge, MA, 02138, USAbDepartment of Psychology, University of Michigan, Ann Arbor, 525 E. University, 2252 East Hall, Ann Arbor, MI, 48109, USA
cDepartment of Psychiatry, Harvard Medical School, Cambridge Health Alliance, 1493 Cambridge St., Cambridge, MA 02139, USAdClinical and Research Program in Pediatric Psychopharmacology, Massachusetts General Hospital,
185 Alewifebrook Parkway, Cambridge, MA 02138 USA
Received 29 October 2004; received in revised form 6 February 2005; accepted 16 February 2005
Available online 1 April 2005
Abstract
An examination of emotional processing in individuals with schizophrenia may aid in understanding the heterogeneous
disease states of schizophrenia. An emotional Stroop test, comprising conditions separated by both emotional valence (positive,
negative) and arousal (low, high), was administered to disorganized (N =12) and non-disorganized (N =15) schizophrenic and
schizoaffective participants, and 22 non-patient controls. Results indicate that the performance of disorganized versus non-
disorganized participants differed particularly on the negative, high arousal condition. Understanding which symptom
dimensions accompany aberrant emotion processing might be useful in understanding the mechanisms involved in the
exacerbation of symptoms, particularly disorganization. Such information may lead to improved treatment and prevention
strategies for schizophrenia spectrum diagnoses.
D 2005 Elsevier B.V. All rights reserved.
Keywords: Disorganization; Schizophrenia; Stroop; Emotion
1. Introduction
Rather than comprising a single disease entity,
schizophrenia may be a cluster of heterogeneous
syndromes that differ in underlying structure (e.g.,
0920-9964/$ - see front matter D 2005 Elsevier B.V. All rights reserved.
doi:10.1016/j.schres.2005.02.009
T Corresponding author. Tel.: +1 617 496 8563; fax: +1 617 495
3728.
E-mail address: [email protected] (L.K. Phillips).
Andreasen et al., 1995). Efforts have beenmade toward
the clarification of subtypes, encompassing more
homogenous manifestations of the illness and perhaps
common pathophysiology. At the descriptive level, the
positive and negative symptom dimensions of schizo-
phrenia can be broken down further into three
syndromes. Negative symptoms, such as affective
flattening, withdrawal, and avolition are included in a
bpsychomotor povertyQ dimension. Positive symptoms
can be divided into breality distortion,Q comprising
77 (2005) 141–149

L.K. Phillips et al. / Schizophrenia Research 77 (2005) 141–149142
hallucinations and delusions, and bdisorganization,Qdescribing attentional, conceptual, and behavioral
disorganization (see Liddle, 1987; Andreasen et al.,
1995, for review).
A number of theorists have attempted to refine the
construct of disorganization. Based on the results of
semantic priming studies, disorganization has been
explained as a deficit in the ability to integrate
contextual information (Hardy-Bayle et al., 2003)
and in the capacity to maintain a mental set (Rosenthal
et al., 1960). In addition, the phenomena associated
with disorganization have been explained by deficits
in working memory (Daban et al., 2003), sensory
motor ability, IQ (Basso et al., 1998), selective
attention (Ngan and Liddle, 2000), and theory of
mind (Hardy-Bayle et al., 2003). Lastly, individuals
diagnosed with higher levels of disorganization have
displayed higher levels of arousal (Lapidus and
Schmolling, 1975) and emotional reactivity (Bur-
bridge and Barch, 2002).
Evidence for the last relationship, between the
disorganization syndrome and abnormalities of
arousal and emotional reactivity, is becoming increas-
ingly evident. Docherty et al. (1994) categorize
individuals as affectively reactive if they produce
more speech errors, in the form of referential
communication failure, when discussing affectively
negative topics than when discussing affectively
positive topics. This disruption in language produc-
tion is speculated to reflect a differential responsivity
to negative valence (Docherty et al., 1994). Specifi-
cally, language reactivity, during the discussion of
stressful events, is greater in participants who scored
higher on positive symptoms (includes both the
positive and disorganization dimensions) (Docherty
and Herbert, 1997), while unrelated to deficit symp-
toms (Cohen and Docherty, 2003). Similarly, Bur-
bridge and Barch (2002) found that symptoms under
the disorganization dimension predicted affective
reactivity in language. Finally, in a study where
individuals with schizophrenia rated slides on pleas-
antness and arousal, higher levels of disorganization
was associated with lower ratings on the pleasant
slides and with a more negative mood post study
participation (Quirk et al., 1998). Thus, both aberrant
emotional processing and emotional reactivity may be
characteristic of individuals meeting criteria for the
disorganized dimension of schizophrenia.
1.1. The emotional Stroop
In the current study, we examined whether aberrant
emotional processing is evident in individuals with
schizophrenia or schizoaffective disorder who score
higher on levels of disorganization. Specifically, we
compared the emotional Stroop performance of those
within the schizophrenia spectrum group who scored
higher in disorganization with those who scored
lower. The emotional Stroop is a variant of the
standard color Stroop (see Williams et al., 1996, for
review). In this task, words with positive or negative
emotional valence are printed in colored ink, and the
participant is asked to name the color of the word
while attempting to ignore the meaning of the word.
Interference is measured by the delay in response time
and errors in naming the color of the word. Increased
response time in color naming reflects increased
attention allocated toward the meaning of the word,
as well as difficulty disengaging attention from it.
Few studies have examined emotional Stroop
effects in schizophrenia, and none has specifically
addressed the Stroop in the disorganized subtype. This
is a surprising oversight given that a possible
dysfunctional affective system, as suggested by the
associated differential responsivity to negative
valence (as cited above), may be more likely to be
associated with aberrant processing on this task.
Epstein et al. (1999) employed an emotional Stroop
test to measure responsivity to threatening verses
neutral information. Although controls showed
increased mesolimbic activity to threat but not neutral
stimuli, individuals with schizophrenia showed
increased mesolimbic activity in both threatening
and neutral contexts, reflecting heightened responsiv-
ity to neutral information. Bentall and Kaney (1989)
found that individuals with persecutory delusions
showed an increased response time to words with
hostile content versus neutral words. Thus, it remains
unclear whether a Stroop effect in schizophrenia is an
effect of emotionality, negativity, arousal, or specific
to hostile information.
1.2. Purpose of the current study
The purpose of the current study was to determine
whether the disorganization symptom dimension is
associated with abnormalities in emotional Stroop
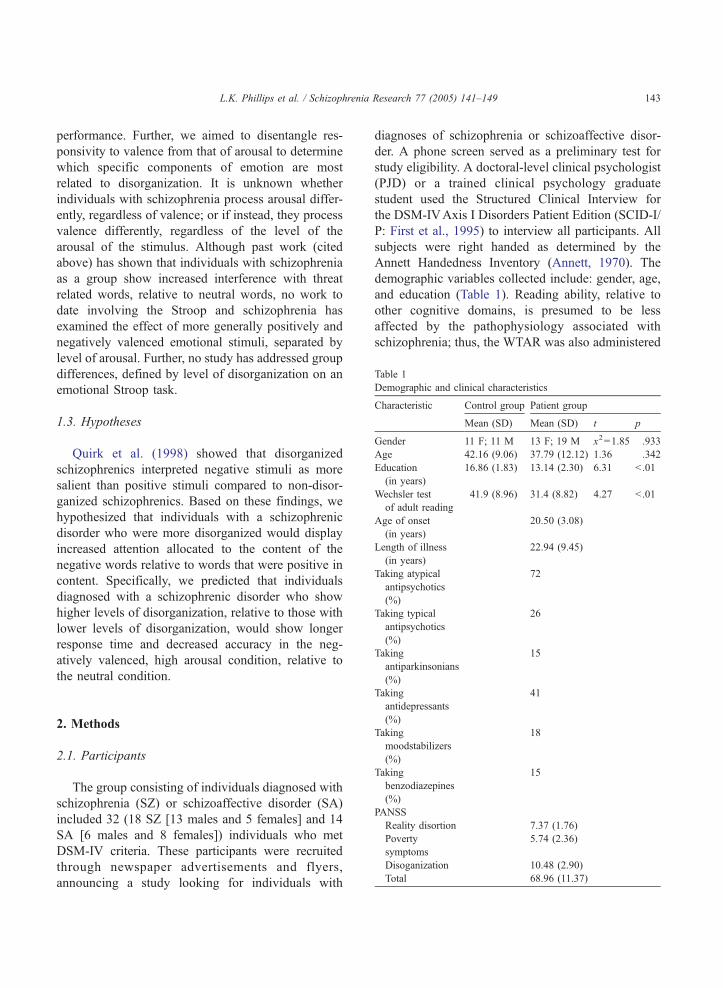
Table 1
Demographic and clinical characteristics
Characteristic Control group Patient group
Mean (SD) Mean (SD) t p
Gender 11 F; 11 M 13 F; 19 M x2=1.85 .933
Age 42.16 (9.06) 37.79 (12.12) 1.36 .342
Education
(in years)
16.86 (1.83) 13.14 (2.30) 6.31 b .01
Wechsler test
of adult reading
41.9 (8.96) 31.4 (8.82) 4.27 b .01
Age of onset
(in years)
20.50 (3.08)
Length of illness
(in years)
22.94 (9.45)
Taking atypical
antipsychotics
(%)
72
Taking typical
antipsychotics
(%)
26
Taking
antiparkinsonians
(%)
15
L.K. Phillips et al. / Schizophrenia Research 77 (2005) 141–149 143
performance. Further, we aimed to disentangle res-
ponsivity to valence from that of arousal to determine
which specific components of emotion are most
related to disorganization. It is unknown whether
individuals with schizophrenia process arousal differ-
ently, regardless of valence; or if instead, they process
valence differently, regardless of the level of the
arousal of the stimulus. Although past work (cited
above) has shown that individuals with schizophrenia
as a group show increased interference with threat
related words, relative to neutral words, no work to
date involving the Stroop and schizophrenia has
examined the effect of more generally positively and
negatively valenced emotional stimuli, separated by
level of arousal. Further, no study has addressed group
differences, defined by level of disorganization on an
emotional Stroop task.
1.3. Hypotheses
Quirk et al. (1998) showed that disorganized
schizophrenics interpreted negative stimuli as more
salient than positive stimuli compared to non-disor-
ganized schizophrenics. Based on these findings, we
hypothesized that individuals with a schizophrenic
disorder who were more disorganized would display
increased attention allocated to the content of the
negative words relative to words that were positive in
content. Specifically, we predicted that individuals
diagnosed with a schizophrenic disorder who show
higher levels of disorganization, relative to those with
lower levels of disorganization, would show longer
response time and decreased accuracy in the neg-
atively valenced, high arousal condition, relative to
the neutral condition.
Taking
antidepressants
(%)
41
Taking
moodstabilizers
(%)
18
Taking
benzodiazepines
(%)
15
PANSS
Reality disortion 7.37 (1.76)
Poverty
symptoms
5.74 (2.36)
Disoganization 10.48 (2.90)
Total 68.96 (11.37)
2. Methods
2.1. Participants
The group consisting of individuals diagnosed with
schizophrenia (SZ) or schizoaffective disorder (SA)
included 32 (18 SZ [13 males and 5 females] and 14
SA [6 males and 8 females]) individuals who met
DSM-IV criteria. These participants were recruited
through newspaper advertisements and flyers,
announcing a study looking for individuals with
diagnoses of schizophrenia or schizoaffective disor-
der. A phone screen served as a preliminary test for
study eligibility. A doctoral-level clinical psychologist
(PJD) or a trained clinical psychology graduate
student used the Structured Clinical Interview for
the DSM-IVAxis I Disorders Patient Edition (SCID-I/
P: First et al., 1995) to interview all participants. All
subjects were right handed as determined by the
Annett Handedness Inventory (Annett, 1970). The
demographic variables collected include: gender, age,
and education (Table 1). Reading ability, relative to
other cognitive domains, is presumed to be less
affected by the pathophysiology associated with
schizophrenia; thus, the WTAR was also administered

L.K. Phillips et al. / Schizophrenia Research 77 (2005) 141–149144
because of its utility as a measure of potential IQ
(Ginsberg, 2003).
Per participant report, all but one of the individuals
diagnosed with schizophrenia or schizoaffective dis-
order were taking psychotropic medication (twenty-
eight individuals on atypical antipsychotics, ten on
typical neuroleptics, six on benzodiazepines, sixteen
on antidepressants, six on antiParkinsonian agents,
and seven were taking a mood stabilizer, Table 1). The
schizophrenia/schizoaffective group experienced a
mean age of onset of 20.50 years (SD=3.08) and an
average duration of illness of 22.9 years (SD=9.45).
All interviews were audiotaped and administered with
2 interviewers present who came to a consensus on all
clinical ratings.
A median split was used to divide those individuals
diagnosed with schizophrenia and schizoaffective
disorder, who scored higher on the disorganization
cluster of the Positive and Negative Symptom Scale
(PANSS; Kay et al., 1987), from those who scored
relatively lower. These two groups (disorganized,
n =12; non-disorganized, n =15) differed significantly
on all four items of disorganization (F =10.7,
p b .001, eta = .81), conceptual disorganization
( p b .01) mannerisms and posturing ( p b .01), diffi-
culty in abstract thinking ( pb .01), and poor attention
( p b .01). The two groups did not differ on any of the
demographic variables [gender ( p = .93), age
( p =.34), education ( p =.80), WTAR ( p =.61), diag-
nosis ( p =.62), duration of illness ( p= .16), age of
onset ( p =.94), medication status ( p =.39), or type of
antipsychotic medication (typical versus atypical)
( p =.21)].
The control group consisted of twenty-two partic-
ipants (11 males and 11 females), who were recruited
through newspaper advertisements and flyers in the
Boston area. They were interviewed, with the use of the
SCID, by the same clinician and graduate students.
There were no significant differences between the
groups on gender and age, and all subjects were right
handed as determined by the Annett Handedness
Inventory (Annett, 1970). However, individuals in the
schizophrenia/schizoaffective group, on average,
experienced fewer years of education and had lower
WTAR scores compared to those in the control group.
Exclusionary criteria, for both groups, included:
learning disabilities, head injuries resulting in loss of
consciousness for more than 10 min, anorexia
nervosa, seizure disorders, and other primary neuro-
logical disorders. Additional criteria for the control
group included no current or past history of Axis I
psychiatric disorder. The group with schizophrenia
disorders had no other history of Axis I mood
disorder.
All study procedures were approved by the
Harvard Institutional Review Board. The details of
the study were explained to all participants, and after
all questions were addressed, written informed con-
sent was obtained. Participants were compensated US
$10 for each hour of their participation.
2.2. Procedures
2.2.1. Questionnaires
After establishment of each participant’s eligibil-
ity, we administered the Positive and Negative
Symptom Scale (PANSS; Kay et al., 1987), the
Annett Handedness Inventory (Annett, 1970), and
the Wechsler Test of Adult Reading (WTAR: The
Psychological Corporation, 2001). The PANSS varia-
bles were divided into three symptom clusters:
reality distortion, poverty symptoms, and disorgani-
zation (similar to Liddle, 1987; Burbridge and Barch,
2002). Reality distortion included delusions and
hallucinations. Poverty symptoms included blunted
affect, motor retardation, and lack of spontaneity.
Disorganization encompassed conceptual disorgani-
zation, mannerisms and posturing, difficulty in
abstract thinking, and poor attention.
2.2.2. Emotional Stroop color-naming paradigm,
modified
Participants were presented with five blocks of 15
words from the Affective Norms for English Words
(ANEW) list (Bradley and Lang, 1999). Words were
displayed in four different colors: blue, red, green,
and brown. The specific colors were selected
because each contains only one syllable. Participants
were instructed to name the color of the ink of the
words as quickly as possible. The conditions differed
by valence and arousal (see Appendix for word list),
consisting of words that were: neutral (e.g., constant);
negative, low arousal (e.g., weak); positive, low
arousal (e.g., sincere); negative, high arousal (e.g.,
furious); and positive, high arousal (e.g., ecstatic). The
conditions appropriately differed according to ratings

L.K. Phillips et al. / Schizophrenia Research 77 (2005) 141–149 145
of valence and arousal and were matched on
frequency and length. Valence and arousal ratings,
taken from the ANEW word list, were on a scale of 1–
5, with 1 being the most positive and of the highest
arousal (neutral: valence=2.94, arousal=3.41; nega-
tive low: valence=4.06, arousal=3.30; positive low:
valence=1.84, arousal=3.13; negative high: valence=
4.22, arousal=2.01; and positive high: valence=1.73,
arousal=1.91).
Each block consisted of 2 practice stimuli followed
by 60 scored stimuli presented on an Apple Macin-
tosh. A word was never repeated more than once. A
custom-made program, through the use of SuperLab,
controlled the interstimulus interval. Each word
remained on the screen until the participant
responded, with a 1000 ms interval between the
participant’s response and the next stimulus presenta-
tion. Automatic collection of response times was
performed through a computer microphone with a
voice-activated trigger. We used Adobe Photoshop to
create stimuli in the font Times, 150 pixels. Partic-
ipants pressed the space bar to initiate the presentation
of stimuli. The vocal responses were manually
recorded by the experimenter with the use of a list
of correct responses, and the participants’ vocal
responses were tape-recorded to ensure accuracy of
coding. Blocks, word order, and color of words were
pseudo-randomly counterbalanced with the following
restrictions: the neutral condition occurred in an equal
number of times in each of the five possible order
positions and the color of the words was never
repeated more than 3 times in succession.
2.3. Data analyses, scoring of the emotional Stroop
First, difference scores were obtained by subtract-
ing the response time to the neutral Stroop condition
from those of each of the emotional Stroop conditions
A repeated measures multivariate analysis of variance
(MANOVA) was performed, with diagnosis (schizo-
phrenia, schizoaffective, control) as the between
subjects factor and valence (positive, negative) and
arousal (low, high) as within subjects factors, in order
to determine if there were any differences among the
three diagnostic groups. This was followed by
pairwise comparisons to assess differences between
the two psychiatric groups to ensure that diagnosis
was not a confound of any group differences between
those individuals who are more versus less Disor-
ganized. Correlations among each of the four emo-
tional Stroops and each of the symptom clusters
(reality distortion, poverty symptoms, and disorgani-
zation) were examined.
A repeated measure multivariate analysis of
variance (MANOVA), with group (disorganized,
non-disorganized) as the between subjects factor and
response time to valence (positive, negative) and
arousal (low, high) as within subjects factors, was
performed to examine valence versus arousal affects
between the groups. This was followed by planned
comparisons, in order to examine differences between
the groups (disorganized, non-disorganized) in
response time to each of the emotional Stroop
conditions (negative valence, low arousal; negative
valence, high arousal; positive valence, low arousal;
positive valence, high arousal). The above analyses
were repeated for accuracy data, where an error
equaled reading the actual word (rather than naming
its color) or naming the color incorrectly. Lastly, a
binary stepwise logistic regression analysis was
performed to determine if response times on the
emotional Stroop conditions could correctly classify
those with the highest scores on the disorganization
dimension from those with the lowest.
3. Results
Although there were no significant differences
among the three diagnostic groups (schizophrenia,
schizoaffective, control) (p=.09) or between the two
psychiatric groups on any of the emotional Stroop
conditions, significant differences emerged in response
time to emotional stimuli between those individuals who
scored higher on levels of disorganization and thosewho
scored lower (Fig. 1). Response time to the negative,
high arousal condition correlated with the dimension of
disorganization (r=.47, p=.02); neither reality distor-
tion nor poverty symptoms correlated with any of the
emotional Stroop conditions. The repeated measures
analysis revealed that group differences existed across
both valence and arousal. When the conditions were
collapsed across levels of arousal, those who scored
higher on disorganization showed increased response
times for negative and decreased response times for
positive blocks, relative to those who showed lower
-80
-40
0
40
80
Non-Disorganized Disorganized
Res
po
nse
Tim
e in
ms.
(dif
fere
nce
sco
res:
em
oti
on
al c
on
dit
ion
s -
neu
tral
)
Neg LowNeg HighPos LowPos High
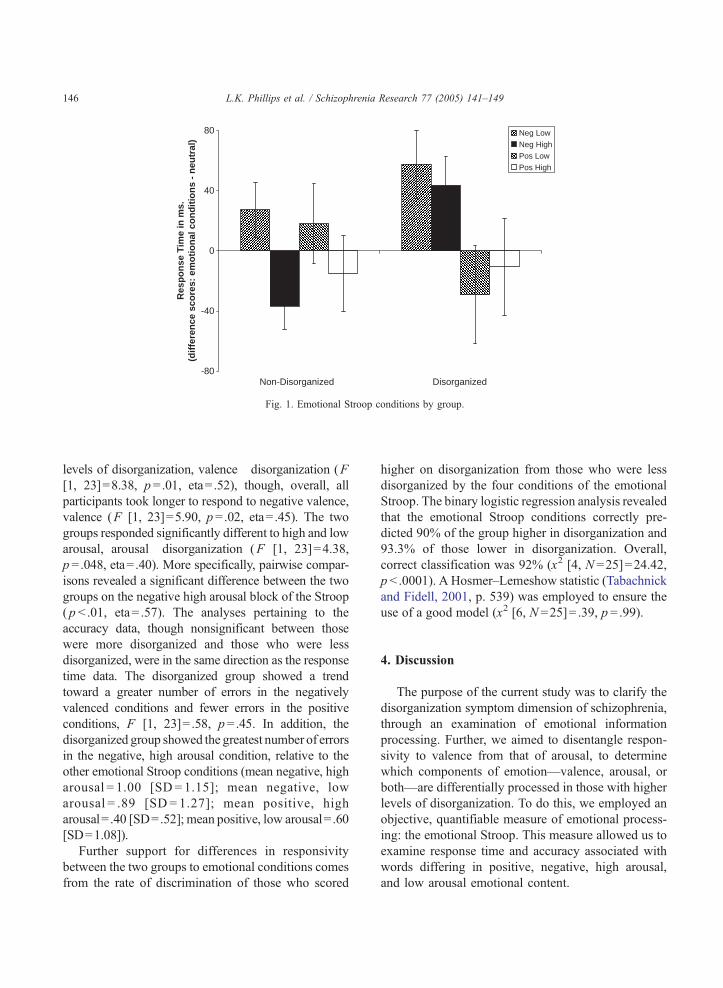
Fig. 1. Emotional Stroop conditions by group.
L.K. Phillips et al. / Schizophrenia Research 77 (2005) 141–149146
levels of disorganization, valence�disorganization (F
[1, 23]=8.38, p=.01, eta= .52), though, overall, all
participants took longer to respond to negative valence,
valence (F [1, 23]=5.90, p=.02, eta= .45). The two
groups responded significantly different to high and low
arousal, arousal�disorganization (F [1, 23]=4.38,
p=.048, eta= .40). More specifically, pairwise compar-
isons revealed a significant difference between the two
groups on the negative high arousal block of the Stroop
( p b .01, eta= .57). The analyses pertaining to the
accuracy data, though nonsignificant between those
were more disorganized and those who were less
disorganized, were in the same direction as the response
time data. The disorganized group showed a trend
toward a greater number of errors in the negatively
valenced conditions and fewer errors in the positive
conditions, F [1, 23]= .58, p=.45. In addition, the
disorganized group showed the greatest number of errors
in the negative, high arousal condition, relative to the
other emotional Stroop conditions (mean negative, high
arousal = 1.00 [SD= 1.15]; mean negative, low
arousal = .89 [SD = 1.27]; mean positive, high
arousal= .40 [SD=.52]; mean positive, low arousal= .60
[SD=1.08]).
Further support for differences in responsivity
between the two groups to emotional conditions comes
from the rate of discrimination of those who scored
higher on disorganization from those who were less
disorganized by the four conditions of the emotional
Stroop. The binary logistic regression analysis revealed
that the emotional Stroop conditions correctly pre-
dicted 90% of the group higher in disorganization and
93.3% of those lower in disorganization. Overall,
correct classification was 92% (x2 [4, N =25]=24.42,
p b .0001). A Hosmer–Lemeshow statistic (Tabachnick
and Fidell, 2001, p. 539) was employed to ensure the
use of a good model (x2 [6, N =25]= .39, p =.99).
4. Discussion
The purpose of the current study was to clarify the
disorganization symptom dimension of schizophrenia,
through an examination of emotional information
processing. Further, we aimed to disentangle respon-
sivity to valence from that of arousal, to determine
which components of emotion—valence, arousal, or
both—are differentially processed in those with higher
levels of disorganization. To do this, we employed an
objective, quantifiable measure of emotional process-
ing: the emotional Stroop. This measure allowed us to
examine response time and accuracy associated with
words differing in positive, negative, high arousal,
and low arousal emotional content.

L.K. Phillips et al. / Schizophrenia Research 77 (2005) 141–149 147
Individuals diagnosed with schizophrenia or
schizoaffective disorder, as a whole, did not respond
differently from the control group in response time or
accuracy to words with valenced and arousing
content. Once the individuals diagnosed with schiz-
ophrenia or schizoaffective disorder were separated
according to level of disorganization symptomatol-
ogy, group differences within the schizophrenia/
schizoaffective group emerged. Specifically, the
disorganized group displayed increased response
time to negative and decreased response time to
positive content. In addition, the disorganized group
responded with increased response times particularly
to the negative high arousal condition, relative to the
neutral condition. Similarly, though not significant,
individuals who were disorganized showed the
highest number of errors in the negative conditions
and the fewest in the positive conditions. Further, the
high rate of accuracy in discrimination of disorgani-
zation by the emotional Stroops suggests that there
may be an overlap in the mechanisms associated
with disorganization with those that contribute to
aberrant emotional processing, particularly to that of
negative affective content. Similar to that mentioned
in the above analyses, it was the words with negative
content with higher arousal ratings that most
distinguished those individuals who were more
disorganized from those who were less.
Emotion and cognition are highly integrated
processes. Together, they contribute to the monitoring
and control of thought and behavior (Gray, 2004).
Differences in the processing of negative, more highly
arousing stimuli, by individuals who are more
disorganized, may be associated with the disinhibition
of cognitive control that is found in this population.
The impact of arousal levels on cognition is evi-
denced by the disruptive influence increased arousal
can have on certain cognitive function, such as
selective attention (Burbridge and Barch, 2002).
Indeed, thought disorder and disorganization in
schizophrenia have been associated with diminished
inhibitory function, coupled with heightened arousal
and increased emotional intensity. In addition, rather
than increasing attention to task relevant information,
abnormal emotional processing may interfere and
result in the loss of perspective that has been observed
in individuals who are disorganized (Harrow et al.,
1989).
Aberrant emotional processing, evident in this
disorganized sample, may be associated with an
increased sensitivity to emotional stress. Indeed,
cortisol change, indexing novelty or stress, has been
associated with disorganization symptom severity
(Walder et al., 2000). Further, since stress sensitivity
has been a predecessor of psychotic episodes, under-
standing which symptoms accompany abnormalities
in emotional processing might be useful in under-
standing the mechanisms involved in the exacerba-
tion of symptomatology. Such information has the
potential to lead to improved treatment and preven-
tion strategies.
There were significant differences between the
schizophrenia/schizoaffective group and the healthy
control group on demographic variables, such as
education, WTAR, and medication status. However,
given there were no significant differences among
the three groups on emotional Stroop performance,
and given other confounds raised by matching on
such variables (Meehl, 1970), we believe that the
demographic differences do not pose significant
challenge to our conclusions. Further, because there
were no significant differences between those higher
in Disorganization and those lower on any of the
demographic variables (gender, age, education,
WTAR, handedness, age of onset, length of illness,
medication status, and diagnosis) differential per-
formance on the Stroop is probably unrelated to
demographic differences.
One limitation of this study is the multiple inter-
pretations associated with performance on the Stroop
test. We are unable to determine whether increased
response time indicates increased attention toward a
stimulus or difficulty disengaging from a stimulus.
While it is especially compelling that stimuli in the
form of words, considered less ecologically valid than
faces, pictures, or film clips, elicited differential
responses among the groups, follow up work with
other forms of emotional stimuli would be helpful to
understanding the relationship between emotional
responsivity and symptoms of disorganization. Addi-
tional work aimed at examining aberrant processing in
those who are disorganized might include independent
measures of different aspects of emotional responsivity
and affective arousal, such as skin conductance and
facial electromyography (EMG). Lastly, it would be
interesting to examine emotional processing in the
Neutral
Impartial
Placid
Passable
L.K. Phillips et al. / Schizophrenia Research 77 (2005) 141–149148
relatives of individuals who are disorganized in order to
determine whether aberrant emotional processing and/
or levels of disorganization are heritable components of
the disease process.
MediumCustomary
Everyday
Neutral
Temperate
Indifferent
Centered
Tolerable
Pacifist
Passive
Acknowledgements
This work was supported by Harvard University
Restricted Funds. The authors would like to thank
Richard J. McNally for his help with revising initial
drafts of this paper.
ModerateConstant
Appendix A. Words selected from affective norms
for English word list
Negative, low arousal Positive, low arousal
Pessimistic Reliable
Dreary Dependable
Alienated Kind
Inadequate Understanding
Weak Loved
Unwanted Considerate
Glum Carefree
Dishonest Pleasant
Hopeless Secure
Somber Sincere
Sluggish Peaceful
Gloomy Harmonious
Unremarkable Valued
Desolate Generous
Plain Sociable
Negative, high arousal Positive, high arousal
Furious Sparkling
Devastated Cheerful
Tormented Animated
Annoyed Optimistic
Reckless Passionate
Frightened Delighted
Irritable Spirited
Ruthless Witty
Desperate Excited
Wicked Splendid
Jealous Jovial
Tense Ambitious
Horrified Euphoric
Greedy Creative
Suffering Exuberant
References
Andreasen, N.C., Arndt, S., Alliger, R., Miller, D., Flaum, M., 1995.
Symptoms of schizophrenia: methods, meanings, and mecha-
nisms. Arch. Gen. Psychiatry 52, 341–351.
Annett, M., 1970. A classification of hand preference by association
analysis. Br. J. Psychol. 61, 303–321.
Basso, M.R., Nasrallah, H.A., Olson, S., Bornstein, R., 1998. Neuro-
psychological correlates of negative, disorganized, and psychotic
symptoms in schizophrenia. Schizophr. Res. 31, 99–111.
Bentall, R.P., Kaney, S., 1989. Content specific information
processing and persecutory delusions: an investigation using
the emotional Stroop test. Br. J. Med. Psychol. 62, 355–364.
Bradley, M.M., Lang, P.J., 1999. Affective norms for English words
(ANEW): instruction manual and affective ratings. Technical
Report C-1, The Center for Research in Psychophysiology.
University of Florida.
Burbridge, J.A., Barch, D.M., 2002. Emotional valence and
reference disturbance in schizophrenia. J. Abnorm. Psychology
111, 186–191.
Cohen, A.S., Docherty, N.M., 2003. Affective reactivity of speech
and emotional experience in patients with schizophrenia.
Schizophr. Res. 69, 7–14.
Daban, C., Amado, I., Bayle, F., 2003. Disorganization syndrome is
correlated to working memory deficits in medicated schizo-
phrenic patients with recent onset schizophrenia. Schizophr. Res.
61, 323–324.
Docherty, N.M., Herbert, A.S., 1997. Comparative affective
reactivity of different types of communication disturbances in
schizophrenia. J. Abnorm. Psychology 106, 325–330.
Docherty, N.M., Evans, I.M., Sledge, W.H., 1994. Affective
reactivity of language in schizophrenia. J. of Nerv. Ment. Dis.
182, 98–102.
Epstein, J., Stern, E., Silbersweig, D., 1999. Mesolimbic activity
associated with psychosis in schizophrenia: symptom-specific
PET studies. Annals of the New York Academy of Sciences 877,
562–574.
First, M.B., Spitzer, R.L., Gibbon, M., Williams, J.B.W., 1995.
Structured Clinical Interview for the DSM-IV Axis I Disor-
L.K. Phillips et al. / Schizophrenia Research 77 (2005) 141–149 149
ders—patient Edition (SCID I-P, Version 2.0). American
Psychiatric Press, Washington, DC.
Ginsberg, J.P., 2003. Wechsler test of adult reading. Appl. Neuro-
psychol. 10, 182–184.
Gray, J.R., 2004. Integration of emotion and cognitive control. Curr.
Dir. Psychol. Sci. 13, 46–48.
Hardy-Bayle, M.-C., Sarfati, Y., Passerieux, C., 2003. The cognitive
basis of disorganization symptomatology in schizophrenia and
its clinical correlates: toward a pathogenetic approach to
disorganization. Schizophr. Bull. 29, 459–471.
Harrow, M., Lanin-Kettering, I., Miller, J.G., 1989. Impaired
perspective and thought pathology in schizophrenic and
psychotic disorders. Schizophr. Bull. 15, 605–623.
Kay, S.R., Fiszbein, P.S., Opler, L.A., 1987. The positive and
negative syndrome scale (PANSS) for schizophrenia. Schizophr.
Bull. 13, 261–276.
Lapidus, L.B., Schmolling, P., 1975. Anxiety, arousal, and
schizophrenia: a theoretical integration. Psychol. Bull. 82,
689–710.
Liddle, P.F., 1987. Syndromes of chronic schizophrenia: a reexami-
nation of the positive–negative dichotomy. Br. J. Psychiatry 151,
145–151.
Meehl, P.E., 1970. Nuisance variables and the ex post facto design.
In: Radner, M., Winokur, S. (Eds.), Minnesota Studies in the
Philosophy of Science. University of Minnesota Press, Minne-
apolis, MN, pp. 373–402.
Ngan, E.T.C., Liddle, P.F., 2000. Reaction time, symptom profiles
and course of illness in schizophrenia. Schizophr. Res. 46,
195–201.
Quirk, S.W., Strauss, M.E., Sloan, D.M., 1998. Emotional response
as a function of symptoms in schizophrenia. Schizophr. Res. 32,
31–39.
Rosenthal, D., Lawlor, W.G., Zahn, T.P., 1960. The relationship of
some aspects of mental set to degree of schizophrenic
disorganization. J. Person. 28, 26–38.
Tabachnick, B.G., Fidell, L.S., 2001. Logistic regression. In:
Tabachnick, B.G., Fidell, L.S. (Eds.), Using Multivariate
Statistics, 4th ed. A Pearson Education Company, Needham
Heights, MA, p. 539.
The Psychological Corporation, 2001. Wechsler Test of Adult
Reading (WTAR) Manual. Author, San Antonio, TX.
Walder, D.J., Walker, E.F., Lewine, R.J., 2000. Cognitive function-
ing, cortisol release, and symptom severity in patients with
schizophrenia. Biol. Psychiatry 48, 1121–1132.
Williams, J.M.G., Mathews, A., MacLeod, C., 1996. The emo-
tional Stroop task and psychopathology. Psychol. Bull. 120,
3–24.