emergencies in pediatric dental practice
DESCRIPTION
emergencies in pediatric dental practiceTRANSCRIPT

Emergencies in pediatric dental practice
Made by
Fatima Gilani
Under the guidance of
M.K.Jindal

Contents
•Duties and responsibilities of a dentist during dental emergency•Critical steps in preparation of emergency•Fundamental steps in emergency management•Treatment protocols in pediatric emergency•Emergency drugs and equipment•Basic life support•Emergency situations in pediatric dental practice•Management of unconsciousness/fainting/syncope•Management of respiratory difficulty•Management of altered consciousness/hyper and hypoglycemic states•Management of seizures•Management of drug related emergencies/ allergy/ anaphylaxis / drug
toxicity
•Management of bleeding
•Management of chest pain
•Management of cardiac arrest

Duties and responsibilities of a dental professional during medical emergencies in pediatric dental practiceA medical emergency is defined as an unforeseen difficulty experienced by the patient.It can occur anywhere even in a dental office.Emergencies may due to a variety of causes, including a child’s pre-existing medical condition, an airway obstruction caused by dental material or problems related to a sedation procedure.Prompt and organized therapy can usually save a life.It is the responsibility of the pediatric dental surgeon to be prepared to recognize a medical emergency & render appropriate care.Many medical emergencies that occur in a dental office are fear-related. therefore, if fear and apprehension are reduced, the chances of having a medical emergency are also reduced.

Medical risk determination
The best treatment for medical emergencies is prevention
By consulting the physician of the patient, emergency complications can be minimized or the severity of the complication can be reduced.
Hospitalization may be required sometimes due to seriousness of the illness for the dental procedure to be carried out.
Emergencies may be related directly to dental therapy or they may occur by chance in the dental office environment.
A best practice dictates that dental personnel must be prepared to provide effective basic life support and seek emergency medical services in a timely manner

Rationale in Emergency
Management Recognize that a problem exists .
Diagnose the problem correctly .
Activate the emergency medical service (EMS)
system immediately.
Keep the patient alive until better trained personnel
arrives .
Remain calm and act swiftly and definitely.
Never administer drugs without definite indication

Medico legal aspects
For medico legal aspects, a written record of the
following should be kept:
Time of onset
Vital signs elicited during the emergency
Time, Name, Dose and Route of drugs
administered
Effects of drugs and therapy provided
Time of initiation of Cardiopulmonary
Resuscitation
Status of the patient at the time of transfer to
Emergency Medical Services system

Steps in the preparation of the emergency in dental office
The ability to perform Basic Life Support
A functioning dental office emergency team
Ready access to emergency assistance
The availability of emergency drugs and
other equipments


Emergency plan
All staff members should have specific assigned duties
Contingency plans should be in place in case a staff member is absent
All staff members should receive appropriated training in the management of
medical emergencies.
All clinical staff members should be trained in Basic Life Support system for
health care providers.
The dental office should be Equipped with emergency equipment and the
supplies should be appropriate for that practice
Emergency drills should be conducted at least quarterly.
Emergency telephone numbers should be placed prominently near each
telephone.
Oxygen tanks and oxygen delivery system should be checked regularly;
other emergency respiratory support equipment should be present; in a good
working order and located according to the emergency plan.
All medical emergency medications should be checked and replacements
should be ordered for specific drugs before their expiratory dates.
One staff member should be assigned the task of ensuring that the above
procedures are completed or not.

Dental Office Emergency System
Team member 1
• Remain with the victim
• Activate office emergency system
• Basic life support system necessary
Team member 2
• Bring emergency equipment to the scene
Team member 3
• Activate emergency medical support system
• Meet and escort Emergency medical support system to office
• Assist with BLS
• Prepare emergency drugs for administration
• Monitor and record vital signs

TREATMENT PROTOCOLS IN PEDIATRIC EMERGENCY
POSITION
(P)
AIRWAY MAINTENANCE
(A)
BREATHING (B)
CIRCULATION ( C )
DEFINITIVE CARE
(D ) EMERGENCY GUIDELINES

EMERGENCY GUIDELINES
POSITION (P)
For a conscious patient: Whatever
position is comfortable for the patient.
For an unconscious patient: All
unconscious patients are placed in a
position to increase cerebral flow with
minimal interference with ventilation.– Place the patient in a supine position
– Head at the same level as the body
– Feet slightly elevated (10-15 angle)

Airway maintenance (A)
The anatomical factors that increases the risk
of airway obstruction in infants are:
Smaller infant mouth, nose and air passages
Larger infant tongues relative to oral cavity
Narrow trachea, glottis opening
Narrowest cricoid cartilage ring
Non palpable cricothyroid membrane.

Breathing (B)During the immediate assessment of breathing, it is vital to diagnose and treat life
threatening breathing problems immediately, i. Clinical signs include Sweating, Central Cyanosis, use of the accessory muscles of
respiratory and abdominal breathing.ii. Seeing the victim’s chest moving does not always mean that the victim is
breathing, but means that an attempt to breathe is made. “LOOK-LISTEN-and-FEEL” technique is used.
iii. Count the respiratory rate, normal rate is 12-20breath/min and a child’s resp. rate is 20-30 breath/min. increase in the breathing rate denotes illness, a warning that a patient may deteriorate and may need medical help
iv. Listen to the patients breath sounds a short distance from their face.v. If the patient’s depth or rate of breathing is inadequate,use bag and mask or
pocket mask ventilation with sufficient oxygen.vi. The rescue breathe is delivered at the rate of 10-12 breaths/min (1breath/5-
6seconds) vii. Acc. To Melamed, hearing and feeling the exchange of air against the rescuer’s
cheek is the only option of a successful spontaneous ventilation.viii. Hyperventilation and panic attacks are relatively common in general dental
practice that will be resolved with simple reassurance.


Circulation (C)
Simple faints or vasovegal episodes are the most likely cause of
circulation problems in general dental practice.
i. Look at the color of the hands and fingers: Are they blue, pink,
pale or mottled?
ii. Assess the limb temp. by feeling the patient’s hand: Are they cool
or warm?
iii. Measure the capillary refill time, apply cutaneous pressure for 5
seconds on a fingertip held at heart level with enough pressure to
cause blanching, check the time how long it takes for the skin to
return to the color of the surrounding skin after releasing the
pressure

iv. The normal refill time is less than 2 sec, increase in
refill time indicates poor peripheral perfusion.
v. Counter the patient’s pulse rate
vi. Palpation of carotid artery preferred in children and
adults, brachial pulse preferred in infants
vii. Weak pulses in a patient with a decreased
conscious level and slow capillary refill time
suggest a low blood pressure
viii. In absence of palpable pulse, chest compression
should be started immediately.

DEFINITIVE CARE
Definitive care involves treating the
specific emergency situation, which is
usually carried out in a hospital.

Emergency drugs and equipment
General principles in using Emergency DrugsTo manage a medical emergency in a dental practice following
drugs should be available :- Glyceryl trinitrate(GTN) spray ( 400 micro gram/dose) Salbutamol aerosol inhaler (100 micro gram/actuation) Adrenaline inj. (1:1000; 1mg/ mL) Aspirin injection (300mg) Glucagon injection 1 mg Oral glucose sol/tab/gel/powder Midazolam 10mg (buccal) Oxygen

Whenever possible, drugs in solution
should be in a prefilled syringe.
The use of intravenous (I V) drugs in dental
practice should be discouraged.
Inhalational, sublingual buccal and
intranasal routes should be preferred.
All drugs should be kept in an “emergency
drug” container.
Oxygen cylinders should be of sufficient
sizes to be easily portable, but also allow
adequate flow

Specific drugs
I. OXYGEN: It is of primary importance in any medical emergencies in
which hypoxemia might be present. These emergencies include CVS ,Respiratory System ,CNS In the hypoxemic patients, breathing enriched with oxygen
elevates the arterial oxygen which increases the oxygen tension and alters the Hb saturation in these patients
Hypoxemia leads to anaerobic metabolism and metabolic acidosis, that diminishes the efficacy of these emergency drugs

2) Epinephrine Single most important injectable drug. Drug of choice for CVS & respiratory systems of acute allergic
reactions. Pharmacological actions include bronchodilation, and increased
systemic vascular resistance, myocardial contractility and cerebral flow.
For better response in case of acute allergic reaction epinephrine should be administered immediately after recognizing the condition.
Epinephrine should be available in preloaded syringes or auto injector to use immediately.
Because of its bronchodilating effects, used in case of acute asthmatic attacks that are not relieved by sprays or aerosols.

3) Diphenhydramine
Histamine blockers reverse the actions of histamine by occupying H1 receptor sites on the effector cell and are effective in patients with mild or delayed onset of allergic reactions.

4) Glucose
Glucose preparations are used by the clinicians to treat hypoglycemia resulting from fasting in a diabetic patient or in a non-diabetic patient with hypoglycemia.
In a conscious patient oral carbohydrates such as orange juice, choc bar act rapidly in circulating blood sugar.
In an unconscious patient if the dentist suspects acute hypoglycemia, oral drugs should not be administered to avoid airway obstruction.

5) Aspirin
The antiplatelet properties of aspirin decreases myocardial mortality by preventing further clot formation when administered while evolving myocardial infarction.
Contraindications to its use include allergy to aspirin and severe bleeding disorders.

6) Bronchodilator
Inhalation of a Beta2 adrenergic receptor agonist such as metaproterenol or albuterol are used to treat bronchospasm that is experienced during an asthmatic attack or anaphylaxis.
Albuterol is an excellent choice because it is associated with fewer cardiovascular adverse effects than other bronchodilator.

Emergency Equipments for dental office
Portable oxygen cylinder with regulator. Oxygen source with flowmeter Nasal cannula Non-rebreathing mask with oxygen reservoir Nasal blood Bag-valve-mask device with oxygen reservoir Oropharyngeal airways Magill forceps Automated external defibrillator Suction devices- powered and manual backup Suction tips and catheters- yankauer 8,10,14 F Intubation equipment-laryngoscope handle with batteries, extra
bulb



Stylets (small and large )-which should never extend beyond the distal end of the endotracheal tube
Adhesive tape to secure the endotracheal tube Needle cricothyrotomy kit Intraosseous needles- 15 or 18 gauge Catheters,short,over the needle 18,20,22,24 gauge Butterfly needles-23gauge Pediatric drip chambers and tubing Isotonic fluids (normal saline or lactated ringer’s solution ) Automatic blood pressure cuff- infant , child , adult Nasogastric tubes -8,10,14 F Sphygmomanometer with adult small, medium and large
cuffs Wall clock with second hand.

Basic life support for a child
Assess consciousness and position the patient Assess and open the airway: Head tilt-chin lift (unless there
has been trauma) Assess and ensure breathing :– Initial rescue breathing-provide two breaths at 1
second/breath– Create a mouth-to-mouth seal and pinch the nose closed– Subsequent 20 breath/min for rescue breathing only– Activate EMS only

Assess and ensure circulation :– Pulse check –palpate the carotid artery/brachial artery, the pulse is
checked for not less than 5 sec. and no more than 10 sec.– Compress if the pulse is less than 60 and the are signs of poor
systemic perfusion– Depth of compressions-one third deep of thoracic cavity– Rate compressions-100per min.– Compressions to ventilations ratio for children – 30:2 for single
rescuer and 15:2 if two rescuers are present– Location-lower one third of sternum– Technique- use the heel of one hand Activate the EMS after 20 cycles (1 min.) of compressions +
ventilations Administer oxygen at 15 L/min and monitor /record vital signs

Emergency situations encountered in a pediatric dental practice
They are classified as follows :1. Unconsciousness Syncope Orthostatic hypotension Adrenal insufficiency2. Respiratory difficulty Airway obstruction Hyperventilation Asthma Chf 3. Seizures 4. Cardiac arrest

5. Drug related emergencies Allergy Toxic overdose.6. Bleeding problems Bleeding disorders Clotting disorders Liver disorders Drug induced7. Altered consciousness Diabetes mellitus Cerebrovascular disorders8. Chest pains Angina pectoris Myocardial infarction

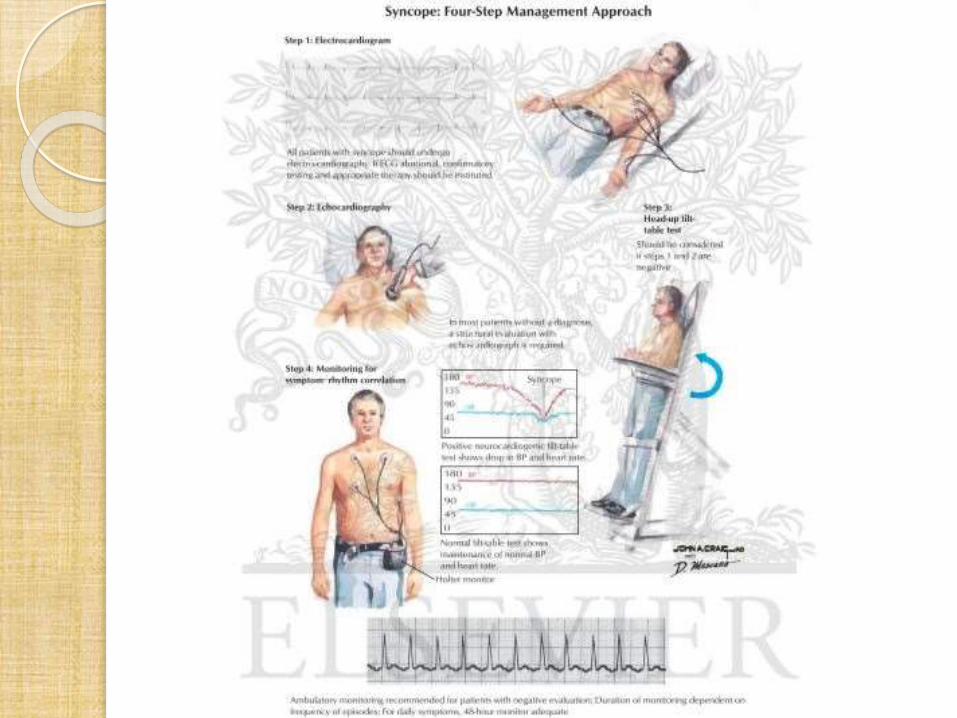
Management of unconsciousness/fainting/syncope
Unconsciousness is rarely noticed in younger children except in the presence of disease
Psychogenic reactions are infrequent in this age group, because children are unable to express their feelings towards dentist.
Causes of fainting are : Vasovegal syncope Orthostatic hypotension Adrenal insufficiency


Vasovegal syncope
It is a loss of consciousness secondary to stress and anxiety. Defined as transient loss of consciousness due to cerebral
ischemia caused by less blood supply to brain.Sign and symptoms
Warm feeling, pale, feeling faint or sick, nausea, bradycardia,hypotension,tachycardia
Fall in BP Gasp for breath Cold clammy skin Eyes dilate Some muscle rigidity Most common in males who try to be macho


Management of syncope
Lie the patient flat in trendelenburg position Relieve any compression on the neck and maintain an airway Raise patient’s leg Use ammonia stimulant Cold towel on forehead and back of the neck Give supplemental oxygen When consciousness is regained, patient should be kept flat and
reassured Once pulse and blood pressure recover, slowly raise patient to
seated position

ORTHOSTATIC HYPOTENSION
Drugs that can trigger orthostatic hypotension are: Anti hypertensive's Antidepressants Narcotics Antiparkinson drugsSigns and symptoms Poor physical condition Obesity Medications Prolonged supine position Not precipitated by stress

Management
Place the patient in supine position Airway maintenance Slowly elevate the patient monitor

Acute adrenal insufficiency
More dangerous than orthostatic hypotension or vasovegal syncope.
Def. of glucocorticosteroid hormone can cause unconsciousness
MANAGEMENT OXYGEN AND SUPPORTIVE THERAPY DECADRON (IV OR IM) 1-4mg (child ) 4-6mg (adult)

Management of respiratory difficulty
Causes : Airway obstruction Hyperventilation Asthma CHF FOREIGN BODY : UPPER AIRWAY OBSTRUCTIONSevere or complete upper airway obstruction due to a foreign body rapidly progresses to unconsciousness
MANAGEMENT 1. Partial obstruction2. Complete obstruction3. Unconscious obstruction


Hyperventilation
Prolonged rapid deep breathing often seen in anxious patients, that leads to metabolic changes and result in unconsciousness.
Fall in arterial co2 that causes cerebral vasoconstriction and resp. alkalosis

MANAGEMENT Reassure patient If conscious patient, rebreath into paper bag to increase inspired
co2 If unconscious patient, maintain airway until patient regains
consciousness. Place in stable side position and reassure patient, while
rebreathing into paper bag

Asthma Asthma manifests as wheezing, with rapid and full pulse,
prolonged expirations.MANAGEMENT Acute severity-patient unable to speak incomplete sentences,
pulse rate more than 110/min, resp. rate more than 45/min. Life-threatening asthma- ‘silent chest’ ,cyanosis, sweating,
hypercarbic flush, bradycardia/hypertension, confusion, Agitation.


Congestive heart failureIn this condition, blood is pooled in the venous system and cause
difficulty in breathing.SIGNS AND SYMPTOMS Pallor Sweating Narrow BP Sleeps semi-sitting Dyspnoea Cyanosis Frothly pink sputum

Treatment
Place in an upright position Administer oxygen Record vitals Call for professional help Bloodless phlebotomy: rotating tourniquets from arm-
to-leg-to-leg altering blood flow back to heart.

Management of seizures
Epilepsy Stages of epilepsy Aura prodrome Ictal phase– Rigidity– Cyanosis– Cheek or tongue biting – Urinary/fecal incontinence– Loss off consciousness Postictal – Disorientation, confusion, amnesia– Somnolence– guilt

Sign and symtoms

Management
Remove dangerous objectives from the mouth and around the patient, e.g. dental cart
Loosen tight clothing Avoid restraining the patient Mouth should not be forced open, nor attempts should be
made to insert anything into the mouth Turn the victim into a stable side-position as soon seizure
stops, open and maintain a clear airway and avoid aspiration, check for breathing.
Most tonic clonic seizures stops within a minute and almost always within 2 min.
Allow the victim to sleep under supervision. On recovery, give reassurance.


Diazepam IV 0.03 mg/kg slow infusion can be administered – Child up to 5 yrs: 0.2-0.5mg slowly every 2-5 min – Child 5 yrs and up: 1 mg every 2-5 min Midazolam nasal spray or buccal placements in case of recurrent
attacks Transfer to hospital if:– First fit– Tonic phase lasts longer than 5 min.– Repeated seizure– Any post seizure respiratory difficulty– Patient has suffered an injury– Post seizure confusion greater than 5 min.

Management of drug-related emergencies/ allergy/anaphylaxis/drug toxicity
Drug allergy/anaphylaxisPotential for drug allergy in dentistry Local anaesthetic -amide solution-overdose/toxicity vs allergy,
vasoconstrictor-cardiac effects Antibiotic-penicillin like drugs Analgesic-ASA, NSAIDs allergy Latex allergy Stressing a medically compromised patientSIGNS OF ALLERGIESMODERATE Hives and itching Skin rash Pallor, light headed Pilomotor erection Palpitation, tachycardia


Severe Asthmatic breathing due to bronchial constriction Large drop in BP These two things indicate allergy is developing into anaphylactic shockAnaphylaxis Develops after re-exposure to a sensitizing antigen within min It is a potentially life-threatening immune reaction to a foreign body Hypersensitivity reactions mediated by immunoglobulin E and IgG4 subclass of
antibodiesSIGNS AND SYMPTOMS Chemical release of mediators from mast cellss causes:– Vasodilation– Increased capillary permeability – Airway constriction– Hypotension– Bronchospasm– Angioedema– Urticaria,rhinitis,conjunctivitis,abdominal pain,vomitting,diarrhoea


Management
Assess the degree of cardiovascular collapse (pulse and BP) Assess the degree of air way obstruction Stop administration of drug Patient supine Check pulse, BP Assess breathing difficulty ( stridor, wheeze, cannot speak) Give O2 Monitor consciousness, airway, breathing, circulation, pulse, BP

If shocked, angioedema or bronchospasm: Raise legs if low BP– Twinject is the new device, for administration of epinephrine Repeat IM adrenaline every 5 min while waiting for
ambulance.There are no contraindications to epinephrine when given for
anaphylactic shock (death can occur with anaphylactic shock)
Up to 3 injections of epinephrine may be needed before arrival of emergency medical technician team
Oxygen If you have doubt, give the epinephrine Call for emergency medical service

Management of bleeding
If bleeding occurs, search for bleeding or bruises, nose bleeds, spontaneous bruising and menstrual bleeding in females
Duration off bleeding is more important than frequency Reasons of bleeding could be manifold- bleeding disorders,
clotting disorders, disorders of liver and effects of drugs. Causes of bleeding in oral cavity includes bleeding/platelet
disorders, clotting disorders, drugs and toxins and liver disorders
MANAGEMENT Pressure application for min 5 min. If bleeds from sockets and compression is ineffective, pack the
socket with gel foam for 7 days Suturing


Hemophilic patients form loose, friable clots that may be readily dislodged or quickly dissolved, antifibrinolytics prevent lysis of clots within oral cavity
They are used as an adjunct to factor concentrate replacement to prevent or control oral bleeding with or without factor replacement.
Epsilon aminocaproic acid (EACA) administration :– 100mg/kg every 6hrs for 7 days to prevent secondary
hemolysis for children– 5g every 6hrs for 5-7 days for children greater than 30
kg.

Management of chest pain
Myocardial infarction Myocardial infarction usually begins with varying degree of
atheromatous coronary occlusion M.I is usually initiated by rupture or erosion of a thin cap,
that over lies the atheromatous plaques. Platelet adhesion and aggregation then occurs over the
ruptured surface. The hemodynamic effects of this thrombus formation may
lead to prolonged ischemic symptoms and pain at rest. If the clot occludes the coronary artery, a myocardial
infarction occurs.


Sign and symptoms :
Persisting central chest pain, with possible radiation to the left or right arms, jaw or neck
Pain is no longer improved with Glyceryl trinitrate Nausea, vomiting A sense of impending doom Restlessness Shortness of breath Pallor, cold sweaty skin Pump failure: hypotension raised venous pressure, tachycardia
and possibly pulmonary edema.

Sign and symtoms

Management
If myocardial infarction is suspected Reassure the victim, keep them warm Sit them up, if breathless Lay them flat, if they are faint Give GTN tablets or sprays, one tablet chewed or one spray
under the tongue Repeat in 5 min, if pain unrelieved activate EMS Give high flow oxygen by face mask Give 300mg aspirin, chewed or sucked, if patient not
allergic Continue monitoring level of consciousness and be
prepared to initiate adult collapse guidelines, if patient becomes unconscious

ANGINA PECTORIS Symptoms of myocardial infarction are similar to that of angina
pectoris, but pain is usually relieved by nitroglycerine. BP is usually raised in Angina while in Myocardial infarction it is
lowMANAGEMENT OF CARDIAC ARREST
Heart does not pump blood in cardiac arrest namely cardiac standstill and ventricular fibrillationSIGN
Gasping for air Pupils dilate Syncope No pulse, BP breathing


Principle Of Cardio Pulmonary Resuscitation When the heart stops, there is still blood (oxygen) in the
tissues This is what gives us the few min. before permanent tissue
damage begins to occur The survival rate for an individual after cardiac arrest,
receiving CPR is 2%-5% If an automated external fibrillator (AED) is utilized, that
survival rate jumps to 86% Most cardiac arrests on children are due to lack of adequate
respiration, therefore open the airway first, before you attempt CPR or attempt to call emergency
Most cardiac arrests on adults are due to a diseased heart, so call emergency first, and then do CPR


AUTOMATED EXTERNAL DEFIBRILLATOR Easy to use If used within min of cardiac arrest, survival rate is
86 % Survival rate decreases with each passed minute by
10% AEDs cause the heart to go to flat-line and then the
body will adjust to the normal heart rhythm The AED is 90% accurate in reading and diagnosing
the patient’s correct cardiac condition AEDs cost is high


Use of AED

Precautions: Do not touch the patient, while AED is reading the heartbeat/rhythm- can confuse the machine
After shocking the patient, do CPR for 2min. If you witness the cardiac arrest(CA), Shock the
patient right away If you do not witness the CA, do 2 min of CPR
and then shock

THANK YOU