ekg basics # 1 that squigglely line - what does it really mean ?
TRANSCRIPT

EKG Basics # 1EKG Basics # 1
That Squigglely Line - What Does It Really
Mean ?


The EKG ElectrodesThe EKG Electrodes
The tracings on the EKG paper are a reflection of electrical activity of the heart.

A series of body surface electrodes are placed at specific points on the arms, legs and thorax that sense and record the heart’s electrical activity.



The electrodes are assigned a specific polarity - i.e. - either negative or positive.


For any lead, the EKG machine looks at a specific combination of electrodes in order to configure the tracing that we expect to see for Lead I, II, III, aVF, aVR, aVL or for V1-V6.
The electrode we care about the most is the Sensing Electrode which is always given a positive polarity (+). Hence, we call it the Positive Sensing Electrode.

In order to understand what the EKG tracing is saying to us, there are a few general principles to remember for depolarization and repolarization.

Rules Guiding The Tracings On The EKG Paper
Making Sense Out Of Seeming Senselessness - Part I

General Principle # 1 General Principle # 1 For For DepolarizationDepolarization

The Isoelectric LineThe Isoelectric Line

If the wave of depolarization is generally moving toward the positive sensing electrode, that electrode will record a positive deflection above the isoelectric line on the EKG paper


General Principle # 2 General Principle # 2 For For DepolarizationDepolarization

If the wave of depolarization is generally moving away from the positive sensing electrode, then the electrode will record a negative deflection below the isoelectric line on the EKG paper.


General Principle # 3 General Principle # 3 For For DepolarizationDepolarization

If the wave of depolarization moves perpendicular to the line of sight of the positive sensing electrode, the sensing electrode will record a biphasic tracing on the EKG paper.

RepolarizationRepolarization
Rules Guiding The Tracings On The EKG Paper : Making Sense Out Of Seeming Senselessness - Part II

General Principle # 1 General Principle # 1 For For RepolarizationRepolarization

If a wave of repolarization is moving toward the positive sensing electrode, then it will inscribe a negative deflection below the isoelectric line on the EKG paper.

General Principle # 2 General Principle # 2 For For RepolarizationRepolarization

If a wave of repolarization moves away from the positive sensing electrode, then it will inscribe a positive deflection above the isoelectric line on the EKG paper.

General Principle # 3 General Principle # 3 For For RepolarizationRepolarization

If a wave of repolarization that moves perpendicular past the line of sight of the positive sensing electrode, then it will inscribe a biphasic deflection on the EKG paper.

Time And Speed Time And Speed Intervals Of The Intervals Of The
EKG TracingEKG Tracing
The EKG paper is a ruled paper that is usually heat sensitive.

The smallest division on the paper is a one millimeter box.
The largest division on the paper is a five millimeter box.

EKG PaperEKG PaperMarriott’s Practical Electrocardiography, 9th ed., 1994Marriott’s Practical Electrocardiography, 9th ed., 1994
By international convention, the speed of the paper is 25 millimeters per second. This is the speed that makes all of the tracings look appropriate for any lead that is being viewed.

Because the speed of the paper is 25 mm/second, a small 1 mm box is traversed in .04 seconds and a large 5 mm box is traversed in .2 seconds.

1 mm box = .04 seconds5 mm box = .20 seconds

Determination of Determination of Heart RateHeart Rate
Because of the predictable EKG paper speed, we can count the number of boxes traversed over a period of time between heart beats to determine HR.

Methods For Methods For Determining Heart Determining Heart
RateRate

Method # 1 : The Method # 1 : The Cardiac RulerCardiac Ruler
Place the beginning point of a cardiac ruler over an R wave.
Look at the number on which the next R wave falls and that becomes the heart rate for that patient.

Use the following numbers to indicate what the heart rate is between two successive R waves : 300, 150, 100, 75, 60, 50, 43, 37, 33, 30

Method # 2 - A Six Method # 2 - A Six Second TracingSecond Tracing
Obtain a six second tracing (30 five mm boxes) and count the number of R waves and multiply by 10 to obtain the HR/min.

Method # 3Method # 3Count the number of large
boxes between 2 R waves and divide this number into 300
Example :
300/2.5 large boxes = 120 bpm

Method # 4Method # 4Count the number of small boxes
between two R waves and divide this number into 1500
Example :
1500/12.5 small boxes=120 bpm
Amplitude or Amplitude or VoltageVoltage
Amplitude of the deflected wave is measured in millivolts (mV).
The voltage of a wave deflected through one large 5 mm box deflection is 0.5 mV.

The EKG LeadsThe EKG Leads

The Six Limb LeadsThe Six Limb Leads
Three Standard Leads :Lead I
Lead II
Lead III

Standard Limb Leads I, II, IIIStandard Limb Leads I, II, IIIhttp://endeavor.med.nyu.edu/courses/physiology/courseware/ekg_pt1/EKGstdleads.htmlhttp://endeavor.med.nyu.edu/courses/physiology/courseware/ekg_pt1/EKGstdleads.html

The Six Limb LeadsThe Six Limb LeadsThree Augmented Leads :
aVF
aVR
aVL

Augmented Leads aVR, aVL, aVFAugmented Leads aVR, aVL, aVFhttp://endeavor.med.nyu.edu/courses/physiology/courseware/ekg_pt1/http://endeavor.med.nyu.edu/courses/physiology/courseware/ekg_pt1/
EKGaugleads.htmlEKGaugleads.html

The Precordial The Precordial Chest LeadsChest Leads
There are six precordial chest leads:
V1, V2, V3, V4, V5, V6

Precordial Chest Leads V1 - V6Precordial Chest Leads V1 - V6http://endeavor.med.nyu.edu/courses/physiology/courseware/ekg_http://endeavor.med.nyu.edu/courses/physiology/courseware/ekg_
pt1/EKGprecordial.htmlpt1/EKGprecordial.html

The Six Limb LeadsThe Six Limb Leads
The six limb leads look at the heart in the frontal plane.

By international convention, a circle is drawn from the chin to the symphysis pubis to describe the area in which the limb leads view the heart.

The circle is divided along the horizontal X axis and the vertical Y axis.

The top half of this circle is wholly negative with the circle enumerated as 0 to -180 degrees.
The bottom half of this circle is enumerated as wholly positive with the circle enumerated from 0 to +180 degrees.

Hexaxial View In The Frontal PlaneHexaxial View In The Frontal PlaneMarriott’s Practical Electrocardiography, 9th ed., pg 23Marriott’s Practical Electrocardiography, 9th ed., pg 23

The Standard LeadsThe Standard Leads
Lead I : created by making the left arm positive (+) and the right arm negative (-).
Its angle of orientation is + 0

Lead ILead IThayler’s The Only EKG Book You’ll Ever Need, 3rd ed., pg 39, 1999Thayler’s The Only EKG Book You’ll Ever Need, 3rd ed., pg 39, 1999

Lead I looks across the heart from right to left along the +0 axis in the frontal plane.

Lead II : created by making the left leg positive (+) and the right arm negative (-).
Its angle of orientation is +60

Lead IILead IIThayler’s The Only EKG Book You’ll Ever Need, 3rd ed., pg 39, 1999Thayler’s The Only EKG Book You’ll Ever Need, 3rd ed., pg 39, 1999

Lead II looks across the heart from the right shoulder down to the left hip along the + 60 axis in the frontal plane.

Lead III : created by making the left leg positive (+) and the left arm negative (-).
Its angle of orientation is a +120

Lead IIILead IIIThayler’s The Only EKG Book You’ll Ever Need, 3rd ed., pg 39, 1999Thayler’s The Only EKG Book You’ll Ever Need, 3rd ed., pg 39, 1999

Lead III looks at the heart from the left shoulder down through the heart to the right hip along the +120 axis in the frontal plane.
The Augmented LeadsThe Augmented Leads
aVL : created by making the left arm positive (+) and the al other extremities negative (-).
Its angle of orientation is -30

aVL looks across the heart from the right leg up through the heart to the left shoulder along the -30 axis in the frontal plane.
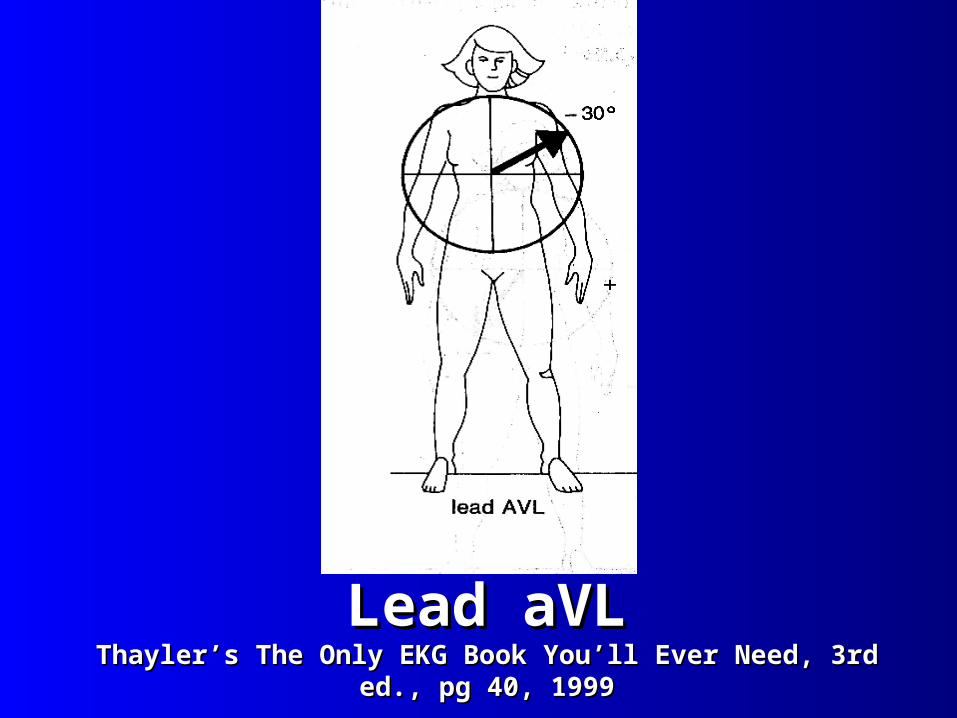
Lead aVLLead aVLThayler’s The Only EKG Book You’ll Ever Need, 3rd ed., pg 40, 1999Thayler’s The Only EKG Book You’ll Ever Need, 3rd ed., pg 40, 1999

aVR : created by making the right arm positive (+) and all other extremities negative (-).
Its angle of orientation is -150

Lead aVRLead aVRThayler’s The Only EKG Book You’ll Ever Need, 3rd ed., pg 40, 1999Thayler’s The Only EKG Book You’ll Ever Need, 3rd ed., pg 40, 1999

aVR looks across the heart from the left hip up through the right shoulder along the -150 axis of the frontal plane.
aVF : created by making the legs positive (+) and all other extremities negative.
Its angle of orientation is +90

Lead aVFLead aVFThayler’s The Only EKG Book You’ll Ever Need, 3rd ed., pg 40, 1999Thayler’s The Only EKG Book You’ll Ever Need, 3rd ed., pg 40, 1999

aVF looks through the heart from the chin down to the feet along the +90 axis in the frontal plane.

Leads Look At Specific Leads Look At Specific Sections Of The HeartSections Of The Heart

The Inferior LeadsThe Inferior Leads
The leads looking at the inferior portion of the heart are : II, III, aVF


The Left Lateral WallThe Left Lateral Wall
Leads looking at the left lateral portion of the heart (left ventricle) are : I, aVL


Lead aVR looks toward the right side of the heart and is considered to be a lead in “no man’s land”.

Since the inferior leads, (Leads II, III, and aVF) will detect the presence of vessel obstructions and MI’s in the inferior wall of the heart, what vessels might be implicated for being occluded ??

Since the lateral wall leads (aVL and Lead I) detect flow obstructions and the presence of MI’s in the lateral wall, what vessels might be implicated for being occluded ??