ehrs: improving efficiency & maximizing potential
TRANSCRIPT
e-bookDigital publication
Important information about EHRs from the publishers of Medical Economics
This e-book is brought to you by
EHRs:
Improving efficiency & maximizing potential

2 MedicalEconomics.comMedical econoMics
Go to modernmedicine.com/EHRbestpractices for more practical tips and to access Medical Economics’ content related to the implementation and use of EHRs.
07 Top 50 EHRs: EHR Capability Checklist
10 Top 50 EHRs: Top 50 EHRs
13 Top 50 EHRs: Scorecard
22 EHR 2.0: 4 ways vendors are building better systems
26 EHRs: 5 ways to put data into action
30 How to optimize your patient portal
34 E-prescribing rates soar among physicians
35 E-prescribing is benefi tting healthcare system, but barriers to adoption remain
37 Ways to optimize EHR documentation at your medical practice
41 Utilize your EHR system to boost practice revenue
insiDe
About this ebook The information contained in this e-book is an aggregation of published works from Medical Economics. It was created to off er physicians a useful guide as it relates to implementation of technology in their practice. For more insights on this and other topics, visit our Resource Center at: medicaleconomics.modernmedicine.com/EHRbestpractices.
EHRs: Improving e� ciency & maximizing potential As the evolution of health information technology forges for-ward, electronic health record (EHR) systems will continue to transform the practice of medicine. Tomorrow’s practice won’t be confi ned by four walls and 15-minute appointment slots, but will have the ability to infl uence, guide and educate patients in real-time at home or at work while changing the way healthcare teams operate to achieve successful outcomes.
In this e-book, Medical Economics showcases recent cover-age of important EHR topics to help you improve your effi cien-cy and maximize the impact of technology on your practice.
Th is coverage includes the results of our exclusive national physician survey providing usability ratings of the top EHR sys-tems in fi ve key areas, including Meaningful Use attestation, clinical support, technical support, impact on quality of care, and patient portals. Th is also features the top 50 EHR compa-nies displayed alphabetically to off er a predictive metric for a company’s longevity in the market on as well as a capabilities checklist to use when selecting (or changing) an EHR system. Other key EHR topics include ways to maximize revenue, data, documentation, and patient portal use.
3 Medical econoMicsMedicalEconomics.com
You know the drill: faxes, forms, phone calls, web portals, and the long wait before you get the prescription approved. No more. Simplify the whole process with CompletEPA®, a real-time, end-to-end electronic prior authorization solution that’s integrated within your EHR. As the solution for a majority of health plans, only CompletEPA delivers approved prescriptions before your patient even leaves the office.
Ask your EHR to get CompletEPA For more information, visit Surescripts.com/CompletEPA
Prior Authorization without the Frustration
Copyright © 2014 by Surescripts, LLC. All rights reserved.
4 MedicalEconomics.comMedical econoMics
We believe healthcare will get better with improved information. As the nation’s most comprehensive health information network, we integrate with existing software systems to connect providers, health plans, pharmacies and healthcare technology partners—helping improve the efficiency and effectiveness of America’s healthcare system.
Copyright © 2014 by Surescripts, LLC. All rights reserved.
E-PRESCRIBING
Medication History
Immunization Reporting
Electronic Prior Authorization
E-Prescribing of Controlled Substances
Unleashing the Potential of Healthcare.
Surescripts services are accessible to you through your EHR vendor.
We believe healthcare will get better with improved information. As the nation’s most comprehensive health information network, we integrate with existing software systems to connect providers, health plans, pharmacies and healthcare technology partners—helping improve the efficiency and effectiveness of America’s healthcare system.
Copyright © 2014 by Surescripts, LLC. All rights reserved.
E-PRESCRIBING
Medication History
Immunization Reporting
Electronic Prior Authorization
E-Prescribing of Controlled Substances
Unleashing the Potential of Healthcare.
Surescripts services are accessible to you through your EHR vendor.

Introducing the Medical Economics app for
iPad and iTunes
The leading business resource for physicians
is now available in an app!
Download it for free today at www.MedicalEconomics.com/MedicalEconomicsApp
7Medical econoMicsMedicalEconomics.com
e-bookDigital publication
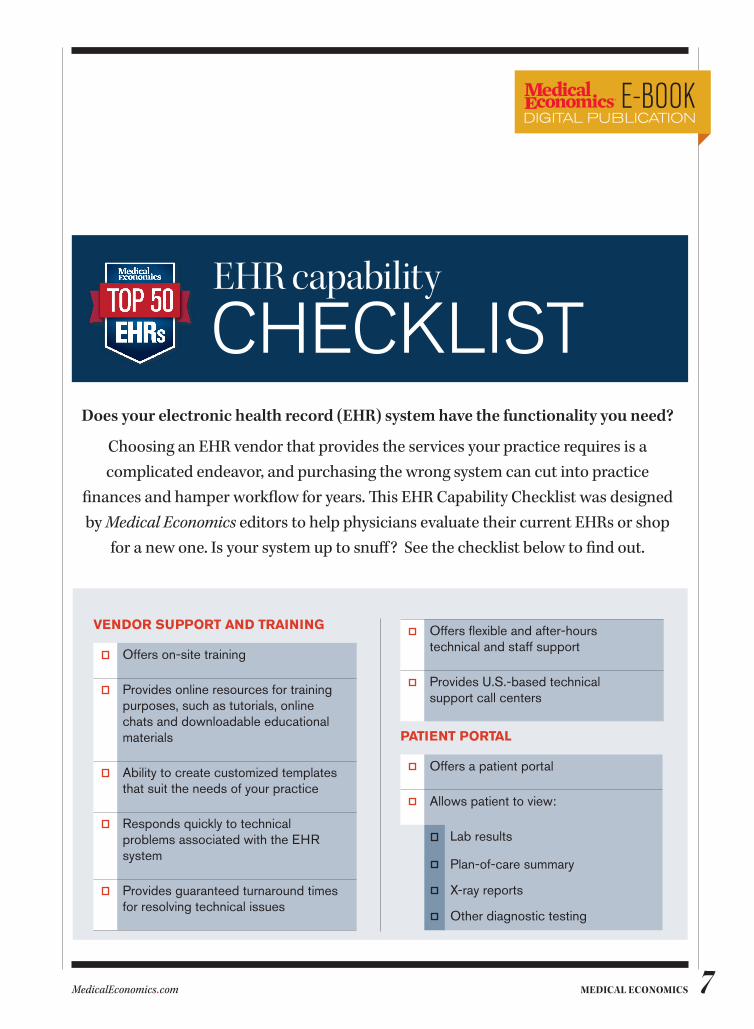
Does your electronic health record (EHR) system have the functionality you need?
Choosing an EHR vendor that provides the services your practice requires is a complicated endeavor, and purchasing the wrong system can cut into practice
fi nances and hamper workfl ow for years. Th is EHR Capability Checklist was designed by Medical Economics editors to help physicians evaluate their current EHRs or shop
for a new one. Is your system up to snuff ? See the checklist below to fi nd out.
EHR capability
CHECKLIST
VENDOR SUPPORT AND TRAINING
Offers on-site training
Provides online resources for training purposes, such as tutorials, online chats and downloadable educational materials
Ability to create customized templates that suit the needs of your practice
Responds quickly to technical problems associated with the EHR system
Provides guaranteed turnaround times for resolving technical issues
Offers fl exible and after-hours technical and staff support
Provides U.S.-based technical support call centers
PATIENT PORTAL
Offers a patient portal
Allows patient to view:
Lab results
Plan-of-care summary
X-ray reports
Other diagnostic testing
8 MedicalEconomics.comMedical econoMics
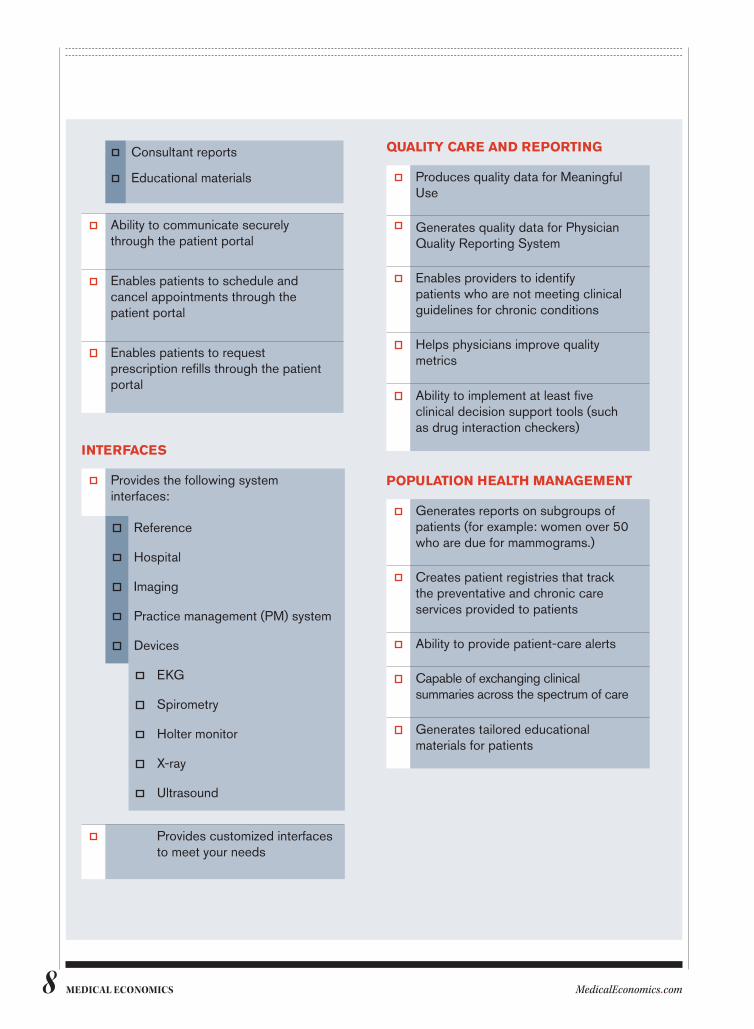
Consultant reports
Educational materials
Ability to communicate securely through the patient portal
Enables patients to schedule and cancel appointments through the patient portal
Enables patients to request prescription refills through the patient portal
INTERFACES
Provides the following system interfaces:
Reference
Hospital
Imaging
Practice management (PM) system
Devices
EKG
Spirometry
Holter monitor
X-ray
Ultrasound
Provides customized interfaces to meet your needs
QUALITY CARE AND REPORTING
Produces quality data for Meaningful Use
Generates quality data for Physician Quality Reporting System
Enables providers to identify patients who are not meeting clinical guidelines for chronic conditions
Helps physicians improve quality metrics
Ability to implement at least five clinical decision support tools (such as drug interaction checkers)
POPULATION HEALTH MANAGEMENT
Generates reports on subgroups of patients (for example: women over 50 who are due for mammograms.)
Creates patient registries that track the preventative and chronic care services provided to patients
Ability to provide patient-care alerts
Capable of exchanging clinical summaries across the spectrum of care
Generates tailored educational materials for patients
9 Medical econoMicsMedicalEconomics.com
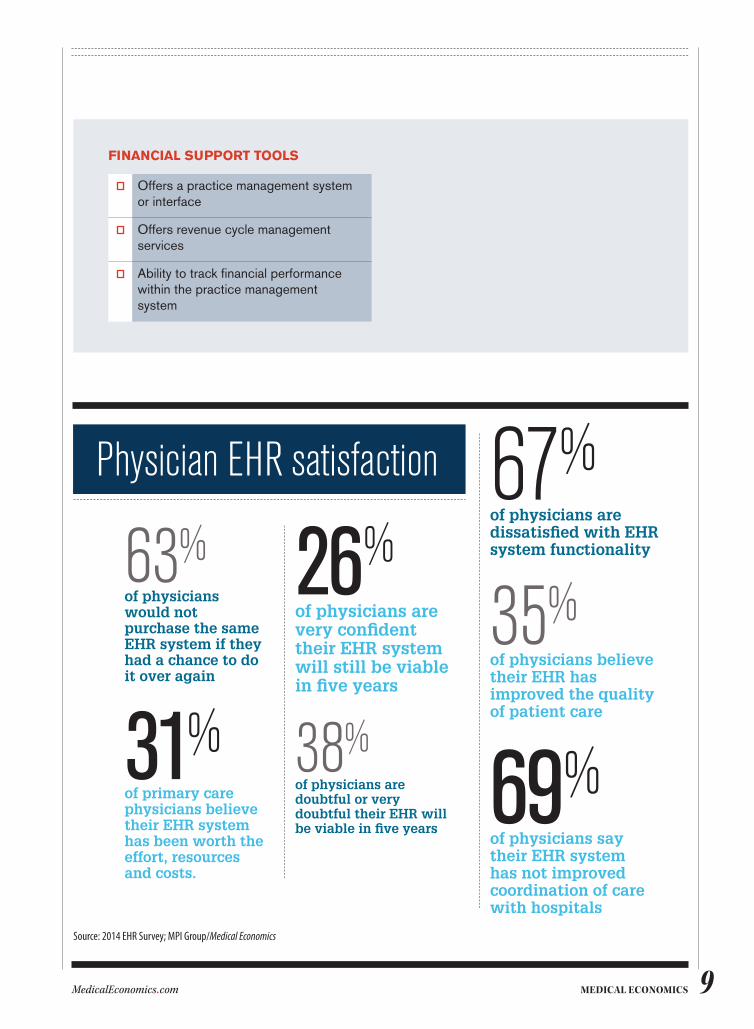
26%of physicians are very confident their EHR system will still be viable in five years
38%of physicians are doubtful or very doubtful their EHR will be viable in five years
67%of physicians are dissatisfied with EHR system functionality
35%of physicians believe their EHR has improved the quality of patient care
69%of physicians say their EHR system has not improved coordination of care with hospitals
63%of physicians would not purchase the same EHR system if they had a chance to do it over again
31%of primary care physicians believe their EHR system has been worth the effort, resources and costs.
Physician eHR satisfaction
Source: 2014 EHR Survey; MPI Group/Medical Economics
FINANCIAL SUPPORT TOOLS
Offers a practice management system or interface
Offers revenue cycle management services
Ability to track financial performance within the practice management system

MedicalEconomics.comMedical econoMics10
e-bookDigital publication
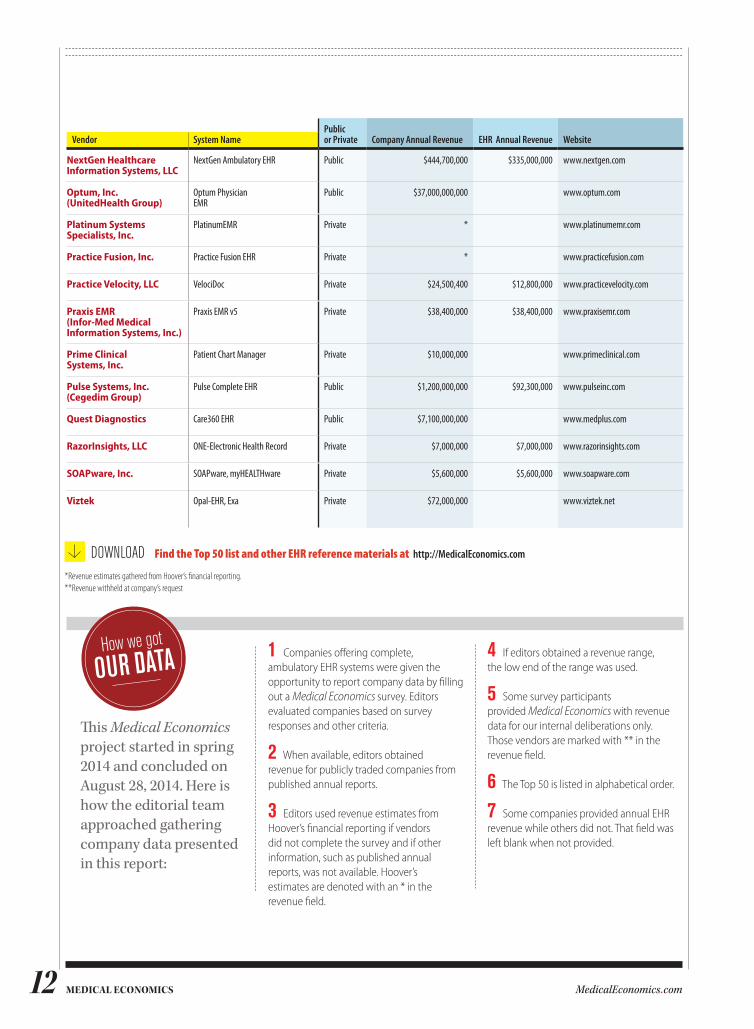
Top 50 EHRsMedical Economics is unveiling this exclusive report on the top 50 electronic health record (EHR) vendors in an eff ort to help physicians make purchasing
decisions. Companies are listed in alphabetical order.
Public or Private Company Annual Revenue EHR Annual Revenue WebsiteVendor System Name
4Medica 4medica iEHR Private $6,000,000 $2,000,000 www.4medica.com
AdvancedMD (ADP) AdvancedMD EHR Public $12,000,000,000 www.advancedmd.com
Advanced Data Systems Corp.
MedicsDocAssistant EHR/EMR Private * www.adsc.com
Allscripts Healthcare Solutions, Inc.
Touchworks EHR, Allscripts Professional EHR
Public $1,400,000,000 $870,000,000 www.allscripts.com
Amazing Charts, LLC Amazing Charts Private ** www.amazingcharts.com
Aprima Medical Software Aprima EHR Private ** www.aprima.com
athenahealth athenaClinicals Public $595,000,000 www.athenahealth.com
Benchmark Systems, Inc. Benchmark Clinical Private $10,000,000 $3,000,000 www.benchmark-systems.com
Bizmatics, Inc. PrognoCIS EMR Private $6,000,000 $6,000,000 www.bizmaticsinc.com
CareCloud Corp. CareCloud Charts Private $11,000,000 $11,000,000 www.carecloud.com
Cerner Corp. PowerChart Ambulatory Public $2,900,000,000 www.cerner.com
CompuGroup Medical, Inc. (CGM US)
CGM CLINICAL, CGM webEHR, CGM ENTERPRISE EHR
Public $50,000,000 $40,000,000 www.cgmus.com
CPSI CPSI Medical Practice EMR Public $200,860,000 www.cpsi.com
*Revenue estimates gathered from Hoover’s fi nancial reporting.**Revenue withheld at company’s request

11 Medical econoMicsMedicalEconomics.com
Public or Private Company Annual Revenue EHR Annual Revenue WebsiteVendor System Name
CureMD CureMD All-in-One EHR Private $91,800,000 $62,200,000 www.curemd.com
Cyfluent Cyfluent Private $5,000,000 $2,000,000 www.cyfluent.com
DocuTAP, Inc. DocuTAP Private ** www.docutap.com
e-MDs , Inc. Solution Series, Cloud Solutions
Private ** www.e-mds.com
eClinicalWorks eClinicalWorks Private $280,000,000 $252,000,000 www.eclinicalworks.com
Endosoft (Utech Products, Inc.)
EndoVault Private * www.endosoft.com
Epic Systems Corp. EpicCare Ambulatory, EpicCare Inpatient
Private $1,660,000,000 $1,660,000,000 www.epic.com
GE Healthcare (GE Corp.) Centricity Practice Solution / Centricity EMR
Public $146,000,000,000 www.gehealthcare.com
Glenwood Systems, LLC GlaceEMR Private $7,500,000 $7,500,000 www.glenwoodsystems.com
Greenway Health, LLC PrimeSUITE, Intergy,SuccessEHS
Private $350,000,000 www.greenwayhealth.com
HealthFusion, Inc. MediTouch Private $35,000,000 $35,000,000 www.healthfusion.com
Integrated Systems Management, Inc.
Omni EHR Private * www.omnimd.com
iPatientCare, Inc. iPatientCare Private $39,000,000 $39,000,000 www.ipatientcare.com
Kareo, Inc. Kareo EHR Private $48,000,000 $48,000,000 www.kareo.com
MacPractice, Inc. MacPractice MD, MacPractice 20/20, MacPractice DC, MacPractice DDS
Private $15,000,000 $15,000,000 www.macpractice.com
McKesson Specialty Health (McKesson Corp.)
iKnowMed (SM) EHR, iKnowMed (SM) Generation 2
Public $122,460,000,000 www.mckesson.com
MD On-Line, Inc. (MDOL) MDOL EMR Private ** www.mdon-line.com
MEDENT MEDENT Private $42,000,000 $30,000,000 www.medent.com
Medical Informatics Engineering, Inc.
WebChart EHR Private * www.mieweb.com
MEDITECH MEDITECH Private $597,840,000 www.meditech.com
Meditab Software, Inc. IMS Clinical Private $35,000,000 $20,000,000 www.meditab.com
MicroFour, Inc. PracticeStudioX16 Private $13,650,000 $12,000,000 www.practicestudio.net
Modernizing Medicine, Inc.
Electronic Medical Assistant (EMA) Private $17,300,000 $17,300,000 www.modmed.com
MTBC ChartsPro Public * www.mtbc.com
Nextech Nextech Private ** www.nextech.com
*Revenue estimates gathered from Hoover’s financial reporting.**Revenue withheld at company’s request
12 MedicalEconomics.comMedical econoMics
Public or Private Company Annual Revenue EHR Annual Revenue WebsiteVendor System Name
NextGen Healthcare Information Systems, LLC
NextGen Ambulatory EHR Public $444,700,000 $335,000,000 www.nextgen.com
Optum, Inc. (UnitedHealth Group)
Optum Physician EMR
Public $37,000,000,000 www.optum.com
Platinum Systems Specialists, Inc.
PlatinumEMR Private * www.platinumemr.com
Practice Fusion, Inc. Practice Fusion EHR Private * www.practicefusion.com
Practice Velocity, LLC VelociDoc Private $24,500,400 $12,800,000 www.practicevelocity.com
Praxis EMR (Infor-Med Medical Information Systems, Inc.)
Praxis EMR v5 Private $38,400,000 $38,400,000 www.praxisemr.com
Prime Clinical Systems, Inc.
Patient Chart Manager Private $10,000,000 www.primeclinical.com
Pulse Systems, Inc. (Cegedim Group)
Pulse Complete EHR Public $1,200,000,000 $92,300,000 www.pulseinc.com
Quest Diagnostics Care360 EHR Public $7,100,000,000 www.medplus.com
RazorInsights, LLC ONE-Electronic Health Record Private $7,000,000 $7,000,000 www.razorinsights.com
SOAPware, Inc. SOAPware, myHEALTHware Private $5,600,000 $5,600,000 www.soapware.com
Viztek Opal-EHR, Exa Private $72,000,000 www.viztek.net
This Medical Economics project started in spring 2014 and concluded on August 28, 2014. Here is how the editorial team approached gathering company data presented in this report:
1 Companies offering complete, ambulatory EHR systems were given the opportunity to report company data by filling out a Medical Economics survey. Editors evaluated companies based on survey responses and other criteria.
2 When available, editors obtained revenue for publicly traded companies from published annual reports.
3 Editors used revenue estimates from Hoover’s financial reporting if vendors did not complete the survey and if other information, such as published annual reports, was not available. Hoover’s estimates are denoted with an * in the revenue field.
4 If editors obtained a revenue range, the low end of the range was used.
5 Some survey participants provided Medical Economics with revenue data for our internal deliberations only. Those vendors are marked with ** in the revenue field.
6 The Top 50 is listed in alphabetical order.
7 Some companies provided annual EHR revenue while others did not. That field was left blank when not provided.
*Revenue estimates gathered from Hoover’s financial reporting.**Revenue withheld at company’s request
DownloaD Find the Top 50 list and other EHR reference materials at http://MedicalEconomics.com
How we got
ouR data
13Medical econoMicsMedicalEconomics.com
e-bookDigital publication
EH R S C O R EC A R D
by KEN TERRY Contributing editor
Exclusive survey gathers physician usability ratings of the top EHR systems in fi ve key areas
SATISFACTIONWITH
EHR SYSTEMSGROWS AMONG PHYSICIANS
Considering the dissatisfaction that many physicians have expressed about electronic health records (EHRs), you might think that most doctors hate these systems. But, ac-cording to an exclusive Medical Economics survey, 55% of physicians are fairly or very satisfi ed with their EHRs, and 54% believe they have helped improve the quality of care.
Forty-fi ve percent of respondents said that EHRs have had a positive fi nancial im-pact on their practices. Most of that is proba-bly related to the Meaningful Use incentives from the government, says Michelle Holmes, MBA, a Seattle-based principal with ECG Management Consultants. “I don’t think it’s the norm for people to say the profi tability of their practice is better after EHR implemen-tation than before it, from a productivity and cost perspective.”
About 80% of Medical Economics’ respon-dents had EHRs, and only 11% of those said they were planning to replace their system within the next 12 months. On the other hand, only 55% said they would recommend their EHR to colleagues. Th e satisfaction of physicians with particular aspects of their EHRs varied a great deal, and the market leaders were not necessarily the most popu-lar among their customers.
Since the survey sample was skewed to-ward small and medium-sized private prac-tices, this doesn’t surprise Holmes. Th e phy-sicians in these practices probably selected the cheap and free products from smaller vendors, she notes. “Th ey’re not using a system that someone else selected on their behalf.”
Internist Edward Gold, MD, an experi-

14 MedicalEconomics.comMedical econoMics
enced EHR user who practices in a 59-doc-tor group based in Emerson, New Jersey, says many physicians prefer the inexpensive EHRs “because they’re simple, and they’re meant to be easy to use. But they don’t ac-complish all the things that need to be ac-
complished for Meaningful Use. They don’t give you the reports you need for the medi-cal home, the reports you need to belong to an ACO. They don’t have the interoperability or the connectivity that’s required. They’ll do for keeping an office record, but they just
eHR usabiliTy RaTingsThe performance of an electronic health record (EHR) system can mean the difference between a thriving practice and a struggling one. These systems impact every aspect of medical care, from the care physicians provide to patients to the practice’s ability to get paid for the work it does.
For this exclusive EHR Scorecard, Medical Economics asked thousands of physicians to rate their systems, on a scale of 0 to 10, in the key areas that matter most to them.
Demographic information on the survey respondents can be found on page 34.
Quality of careThe effect your EHR has on the quality of care your practice provides
An EHR system can either enhance or hinder the care a physician provides to his or her patients. The promise of EHRs is that they will help physicians and the healthcare system provide high-value care, but that remains largely unfulfilled. Some systems are closer to this ideal than others. The vendors that focus on helping physicians navigate today’s healthcare challenges will thrive.
Rank System Base Score
1 SOAPware 24 8.0
2 MEDENT 67 7.2
3 Healthfusion 29 6.9
4 e-MDs 156 6.5
5 Epic 986 6.3
6 Amazing Charts 114 6.3
7 Advanced MD 27 6.2
8 Practice Fusion 255 6.1
9 Modernizing Medicine 42 6.1
10 athenahealth 221 6.0
11 eClinicalWorks 540 5.8
12 Aprima 48 5.7
13 Care360 (Quest) 54 5.6
14 McKesson [All systems} 105 5.2
15 GE 256 5.1
16 Greenway* 227 5.0
17 Vitera* 108 5.0
18 Nextech 23 4.9
19 Cerner 211 4.6
20 Allscripts [All systems] 552 4.5
*Greenway and Vitera merged in late 2013 to become Greenway Health.
15 Medical econoMicsMedicalEconomics.com
provide the basics.”This coverage highlights five EHR usabil-
ity areas important to physicians: Quality of care, Meaningful Use, patient portals, tech-nical support and clinical support. (See EHR system scores on pages 25, 26, 28, 30 and 32.)
AttestAtion toolsOf the respondents who used EHRs, 78% had attested to Meaningful Use in the past year. Sixty-eight percent said the ability of their EHR to enable them to attest to mean-ingful use was “good” or “excellent.”
Internist Kenneth Kubitschek, MD, a partner in North Carolina Internal Medicine in Asheville, North Carolina, and Gold both said their EHRs made it fairly easy to attest in Meaningful Use stage 1. But like most doctors, they’re having trouble with some stage 2 requirements for reasons that have little to do with the quality of their EHRs. Their challenges include getting patients
to use patient portals and exchanging care summaries at transitions of care in an en-vironment where interoperability remains limited.
One area in which EHRs seem to have made progress is clinical decision support (CDS). Sixty-eight percent of our respon-dents had a positive opinion of their ability to use their EHR to implement at least five CDS support tools, which is required for Meaningful Use stage 2.
Holmes notes that the CDS tools in cur-rent EHRs go well beyond pop-up alerts in electronic prescribers that warn doctors about drug interactions, wrong dosages, and so forth. CDS is built into the documen-tation templates of many EHRs, she points out. For example, there may be prompts regarding out-of-range information on vital signs.
Some of the prompts regarding practice guidelines, such as initial medications sug-gested for a patient with newly diagnosed
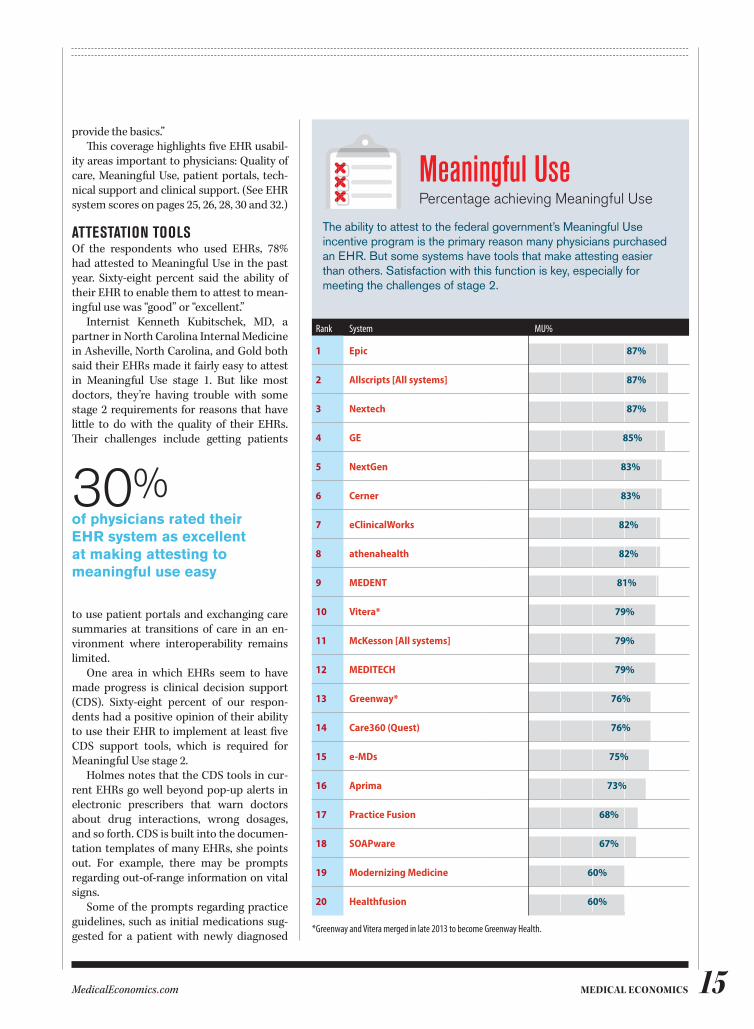
Meaningful use Percentage achieving Meaningful Use
The ability to attest to the federal government’s Meaningful Use incentive program is the primary reason many physicians purchased an EHR. But some systems have tools that make attesting easier than others. Satisfaction with this function is key, especially for meeting the challenges of stage 2.
Rank System Base MU%
1 Epic 986 87%
2 Allscripts [All systems] 552 87%
3 Nextech 23 87%
4 GE 256 85%
5 NextGen 399 83%
6 Cerner 211 83%
7 eClinicalWorks 540 82%
8 athenahealth 221 82%
9 MEDENT 67 81%
10 Vitera* 108 79%
11 McKesson [All systems] 105 79%
12 MEDITECH 102 79%
13 Greenway* 227 76%
14 Care360 (Quest) 54 76%
15 e-MDs 156 75%
16 Aprima 48 73%
17 Practice Fusion 255 68%
18 SOAPware 24 67%
19 Modernizing Medicine 42 60%
20 Healthfusion 29 60%
*Greenway and Vitera merged in late 2013 to become Greenway Health.
30%of physicians rated their EHR system as excellent at making attesting to meaningful use easy
16 MedicalEconomics.comMedical econoMics
diabetes, are quite helpful, Kubitschek says. But many care planning prompts, such as suggested recommendations to an over-weight patient, are unnecessary, he adds.
Peter Basch, MD, medical director for ambulatory health and health IT policy at MedStar Health in Washington, D.C., ob-serves that EHRs certified for Meaningful Use must contain certain types of CDS tools. These include reminder alerts, he says. But he feels that vendors have much further to go in this direction. For one thing, alerts that are fired improperly can lead to alert fatigue. Also, he notes, smart features could be de-veloped to suggest diagnostic tests for a particular problem and to find out whether similar tests had been performed earlier.
ConneCting with pAtientsAbout six in ten respondents gave a “good” or “excellent” rating to the usability of their
patient portal and the ease of updating EHR data on the portal. This is important to many practices because of Meaningful Use stage 2. The government incentive program requires that eligible professionals provide 50% of patients with online access to their records. They must also ensure that 5% of their patients view, download or transmit their health information online. And they have to demonstrate that they can exchange secure messages with patients.
The main barrier to achieving these goals is not the technology, Holmes notes. “Most portals aren’t difficult for the practice or the patient to use. The hurdle is getting people to use them.”
Aside from that, Kubitschek says, his patient portal works very well. “When I do my labs and other stuff, the information
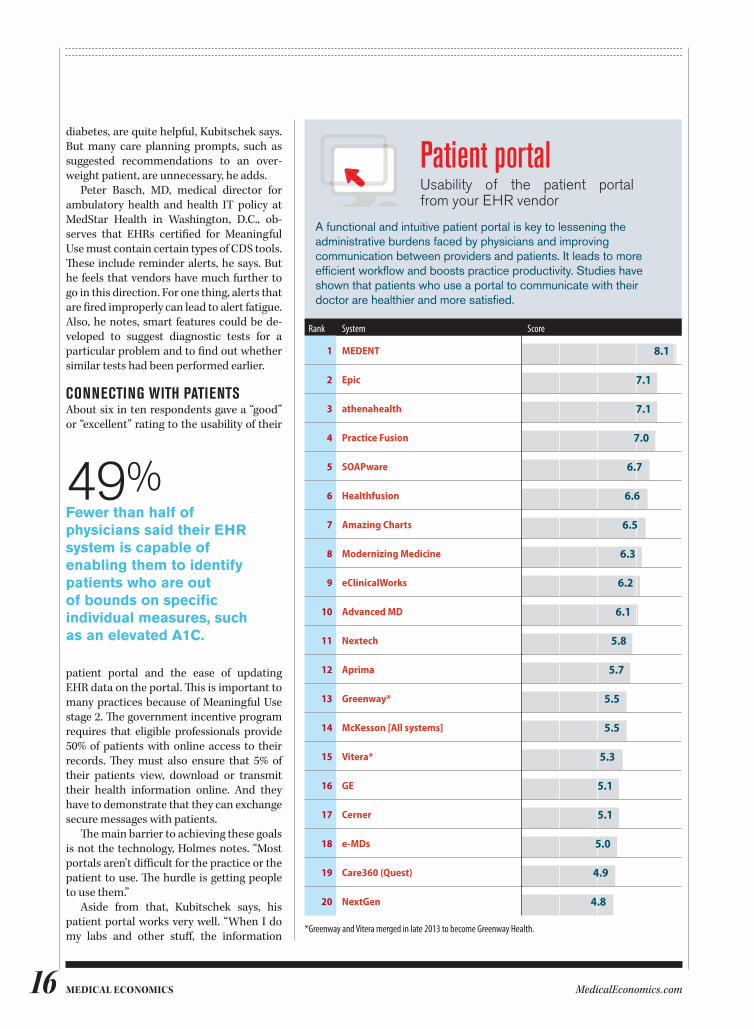
Patient portalUsability of the patient portal from your EHR vendor
A functional and intuitive patient portal is key to lessening the administrative burdens faced by physicians and improving communication between providers and patients. It leads to more efficient workflow and boosts practice productivity. Studies have shown that patients who use a portal to communicate with their doctor are healthier and more satisfied.
Rank System Base Score
1 MEDENT 67 8.1
2 Epic 986 7.1
3 athenahealth 221 7.1
4 Practice Fusion 255 7.0
5 SOAPware 24 6.7
6 Healthfusion 29 6.6
7 Amazing Charts 114 6.5
8 Modernizing Medicine 42 6.3
9 eClinicalWorks 540 6.2
10 Advanced MD 27 6.1
11 Nextech 23 5.8
12 Aprima 48 5.7
13 Greenway* 227 5.5
14 McKesson [All systems] 105 5.5
15 Vitera* 108 5.3
16 GE 256 5.1
17 Cerner 211 5.1
18 e-MDs 156 5.0
19 Care360 (Quest) 54 4.9
20 NextGen 399 4.8
*Greenway and Vitera merged in late 2013 to become Greenway Health.
49%Fewer than half of physicians said their EHR system is capable of enabling them to identify patients who are out of bounds on specific individual measures, such as an elevated A1C.
17 Medical econoMicsMedicalEconomics.com
uploads automatically as soon as I sign it. And the patients are getting it, because we’re talking to them. It has their problems, aller-gies, medications, and immunizations. We get messages back and forth from the pa-tients. I’ve been pretty pleased with it.”
Another benefit, he adds, is that patient messages come right into an EHR inbox, and physicians can decide to whom those should be directed. He has his nurse triage the patient communications. He can then reply directly to a patient message or send it back to his nurse, and can choose whether to save it to the chart.
Vendor Customer serViCeAbout 60% of the respondents rated the quality and amount of EHR training and the
vendor’s ability to solve technical problems as “good” or “excellent.” Around the same percentage gave a thumbs-up to the quality of the interface between their EHR and prac-tice management system (PMS), if they had non-integrated systems.
On the other hand, many respondents gave their vendors fair or poor scores for their ability to solve technical problems (30%), the level of support the practice re-ceived in configuring the EHR (29%), the quality and amount of training (28%), and the ability to customize their EHR (36%).
Basch believes that increasing transpar-ency and competition have induced vendors to offer packages of software, training and implementation that are better than they
70%of physician respondents who do not have an EHR system have no plans to purchase one.
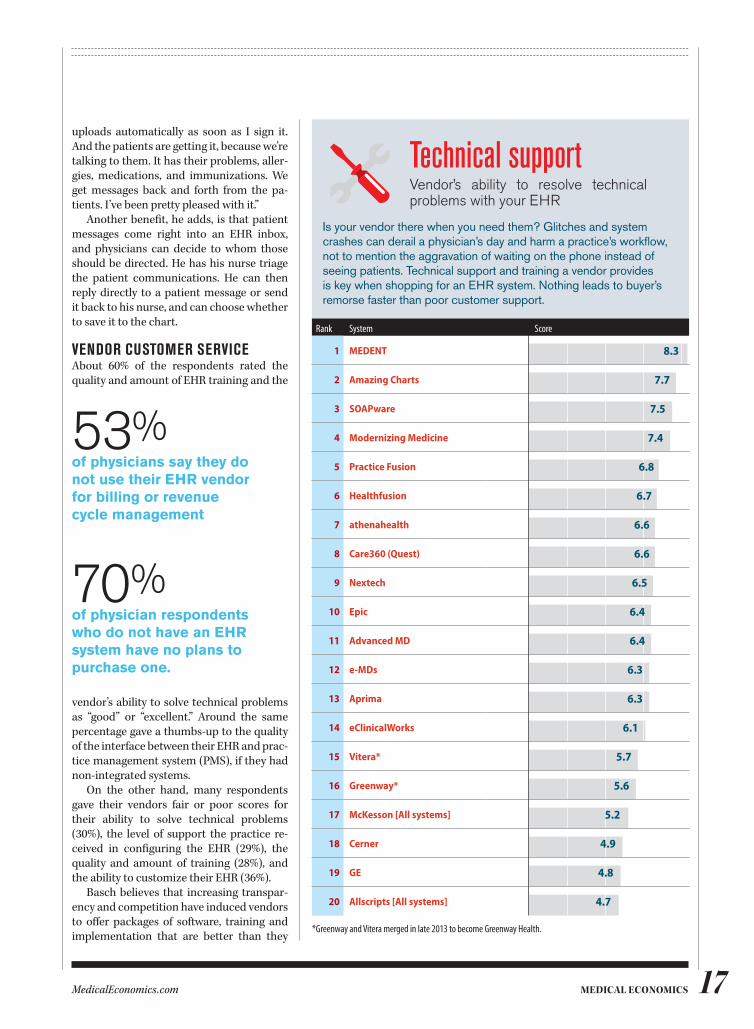
technical supportVendor’s ability to resolve technical problems with your EHR
Is your vendor there when you need them? Glitches and system crashes can derail a physician’s day and harm a practice’s workflow, not to mention the aggravation of waiting on the phone instead of seeing patients. Technical support and training a vendor provides is key when shopping for an EHR system. Nothing leads to buyer’s remorse faster than poor customer support.
Rank System Base Score
1 MEDENT 67 8.3
2 Amazing Charts 114 7.7
3 SOAPware 24 7.5
4 Modernizing Medicine 42 7.4
5 Practice Fusion 255 6.8
6 Healthfusion 29 6.7
7 athenahealth 221 6.6
8 Care360 (Quest) 54 6.6
9 Nextech 23 6.5
10 Epic 986 6.4
11 Advanced MD 27 6.4
12 e-MDs 156 6.3
13 Aprima 48 6.3
14 eClinicalWorks 540 6.1
15 Vitera* 108 5.7
16 Greenway* 227 5.6
17 McKesson [All systems] 105 5.2
18 Cerner 211 4.9
19 GE 256 4.8
20 Allscripts [All systems] 552 4.7
*Greenway and Vitera merged in late 2013 to become Greenway Health.
53%of physicians say they do not use their EHR vendor for billing or revenue cycle management
18 MedicalEconomics.comMedical econoMics
were. Holmes, in contrast, speculates that many physicians rate their vendors highly because they don’t know how much of the support work is being done by their organi-zation’s IT staff or by “super-users” in their own offices.
Gold and Kubitschek both give their ven-dors fairly high marks for training and tech-nical support. But Gold notes that training varies greatly among EHR suppliers. “The basic problem that most doctors have with EHRs has to do with the inadequacy of train-ing. The lower level EHR vendors will give you six hours of training online. The more training you get, the more it costs, and doc-tors don’t like costs. Doctors never invest enough in training,” he says.
His own group he adds, is big enough to afford its own IT person, who trains new staff and provides ongoing training to the
doctors and staff members. “It’s never once and done,” he points out. “In a higher-end system, there are so many bells and whistles that people are unaware of that could make their lives a lot easier. It’s a continuous pro-cess of educating people.”
QuAlity reportingSeventy-nine percent of EHR users said their systems could generate quality reports. That’s about the same percentage of respon-dents who said they’d attested to Meaning-ful Use, which requires quality measures.
But these statistics obscure the difficul-ties that some users have in using their EHRs to report on quality measures, Gold says. “In some systems, it’s easy to generate reports,” he notes. “Others require the involvement of the vendor, which charges the physicians to do this.” Moreover, if doctors and practice staff aren’t specifically trained to produce re-ports, it might be very challenging for them. Gold himself finds it fairly simple, he adds, because his system provides a dashboard for this purpose.
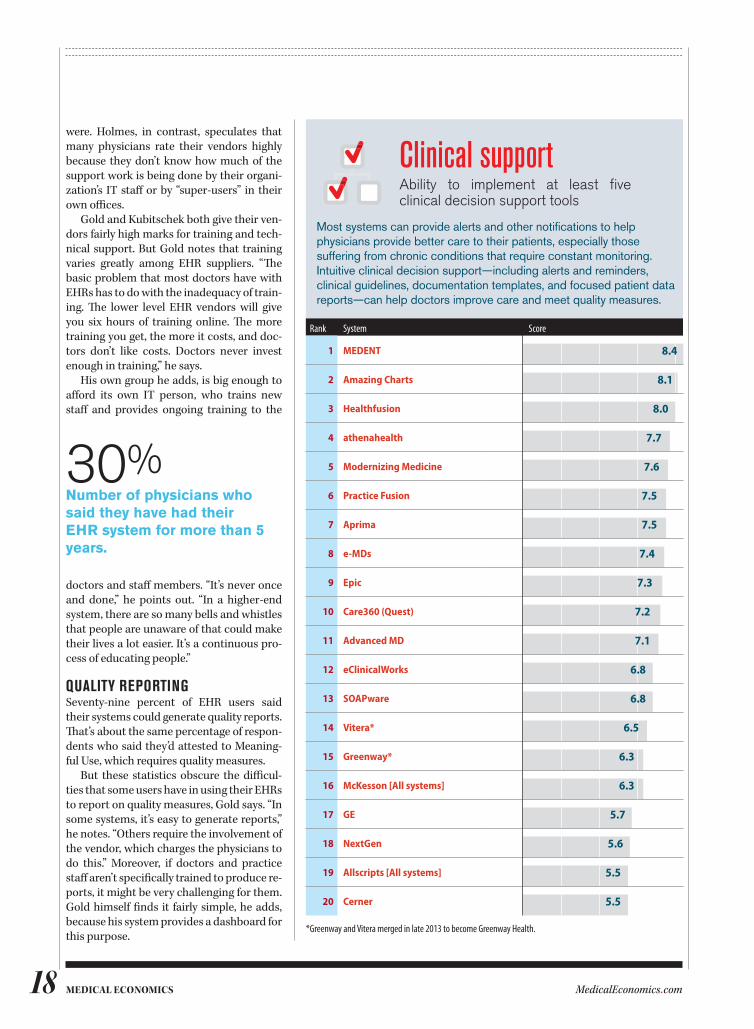
30%Number of physicians who said they have had their EHR system for more than 5 years.
Clinical supportAbility to implement at least five clinical decision support tools
Most systems can provide alerts and other notifications to help physicians provide better care to their patients, especially those suffering from chronic conditions that require constant monitoring. Intuitive clinical decision support—including alerts and reminders, clinical guidelines, documentation templates, and focused patient data reports—can help doctors improve care and meet quality measures.
Rank System Base Score
1 MEDENT 67 8.4
2 Amazing Charts 114 8.1
3 Healthfusion 29 8.0
4 athenahealth 221 7.7
5 Modernizing Medicine 42 7.6
6 Practice Fusion 255 7.5
7 Aprima 48 7.5
8 e-MDs 156 7.4
9 Epic 986 7.3
10 Care360 (Quest) 54 7.2
11 Advanced MD 27 7.1
12 eClinicalWorks 540 6.8
13 SOAPware 24 6.8
14 Vitera* 108 6.5
15 Greenway* 227 6.3
16 McKesson [All systems] 105 6.3
17 GE 256 5.7
18 NextGen 399 5.6
19 Allscripts [All systems] 552 5.5
20 Cerner 211 5.5
*Greenway and Vitera merged in late 2013 to become Greenway Health.
19Medical econoMicsMedicalEconomics.com
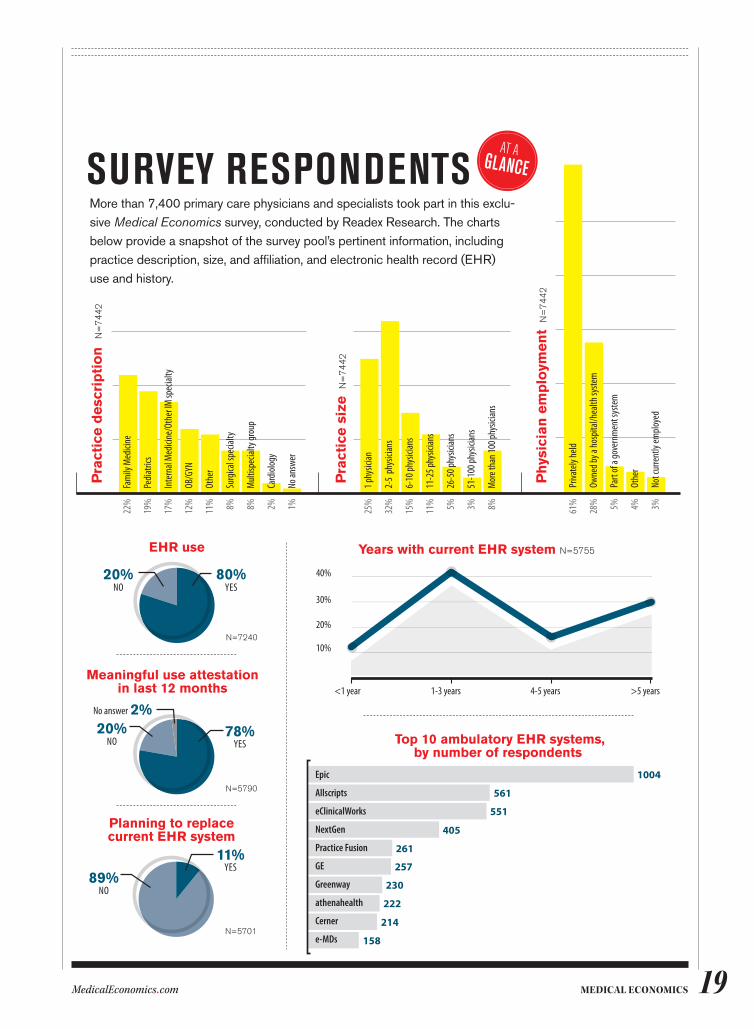
More than 7,400 primary care physicians and specialists took part in this exclu-sive Medical Economics survey, conducted by Readex Research. The charts below provide a snapshot of the survey pool’s pertinent information, including practice description, size, and affiliation, and electronic health record (EHR) use and history.
aT aglanCE
Years with current EHR system N=5755
<1 year 1-3 years 4-5 years >5 years
40%
30%
20%
10%
Pra
ctic
e d
esc
rip
tio
n
N=
74
42
Fam
ily M
edici
ne
Pedia
trics
Inte
rnal
Med
icine
/Oth
er IM
spec
ialty
OB/G
YN
Othe
r
Surg
ical s
pecia
lty
Mult
ispec
ialty
grou
p
Card
iolog
y
No an
swer
22%
19%
17%
12%
11% 8% 8% 2% 1%
Pra
ctic
e s
ize
N
=7
44
2
25%
32%
15%
11% 5% 3% 8%
1 phy
sician
2-5
phys
ician
s
6-10
phys
ician
s
11-2
5 phy
sician
s
26-5
0 phy
sician
s
51-1
00 ph
ysici
ans
Mor
e tha
n 100
phys
ician
s
Ph
ysic
ian
em
plo
ymen
t N
=7
44
2
61%
28% 5% 4% 3%
Priva
tely
held
Owne
d by a
hosp
ital/h
ealth
syste
m
Part
of a
gove
rnm
ent s
yste
m
Othe
r
Not c
urre
ntly
emplo
yed
EHR use
80%20%NO YES
N=7240
Meaningful use attestation in last 12 months
78%20%2%
YESNO
No answer
N=5790
Planning to replace current EHR system
11%
89%YES
NO
N=5701
Top 10 ambulatory EHR systems, by number of respondents
Epic
Allscripts
eClinicalWorks
NextGen
Practice Fusion
GE
Greenway
athenahealth
Cerner
e-MDs
1004
561
551
405
261
257
230
222
214
158
surVey respondents

20 MedicalEconomics.comMedical econoMics
Fairly high numbers of respondents said their EHRs could generate clinical reports on subgroups of patients (63%), identify pa-tients who were out of bounds on specific measures, such as diabetic patients with elevated A1c levels (49%), and send alerts to providers and care managers about pa-tient care gaps (45%). Eighty-seven percent of EHR users said their systems could do at least one of these tasks.
Do many physicians use this data and the related workflow features to improve care and manage population health? Basch doubts it. The business case for using health IT to improve quality, he says, is still lacking in most practices.
For Kubitschek and his colleagues, how-ever, the challenge is much more immedi-ate. They’re too busy attesting to Meaningful Use stage 2 and getting all their quality re-ports right to worry about using the data for quality improvement, he says.
usAbility Nearly two-thirds of respondents gave above-average scores to their EHRs on two markers for usability: ease of ordering tests and medications, and ease of moving be-tween sections of EHRs. And 53% of respon-dents rated their vendor’s ability to custom-ize their EHRs as “good” or “excellent.”
Regarding customization, Holmes be-lieves that most physicians can’t readily dis-tinguish between what their own IT people or other staffers do and what their vendor does. But employed physicians have a more difficult time getting things changed in their EHR than do private practice doctors, she says, because of the former’s need for orga-nizational approval. So she thinks the us-ability scores reflect “the amount of control that physicians have over their systems in smaller practices.”
That doesn’t explain the popularity of cloud-based EHRs, which allow little cus-tomization. Holmes thinks that practices that choose those products see other ad-vantages in them. Among other things, she says, they’re generally simpler to implement, learn and navigate than are more complex client-server programs.
Basch gives credit to EHR vendors for improving the usability of their products in some ways. For example, he notes, phy-sicians can order a test or a prescription anywhere in the workflow in many systems,
rather than having to be at a certain point in the process.
Kubitschek, says that the usability of EHRs has vastly improved since he start-ed using one in 1995. While the vendors haven’t made much progress in the past three years because of their focus on Mean-ingful Use, he says, he’s recently seen some innovations that have made his EHR more user-friendly.
prACtiCe mAnAgement systemsBecause finances are the lifeblood of prac-tices, the practice management system component of EHRs—or the standalone PMS bolted to an EHR—is vitally impor-tant. But just 61% of respondents gave good or excellent scores to the ability of their system to post electronic remittance advice
EHR usabIlIty REPoRt
survey methodologyThe findings cited in this report are based on a survey conducted by Readex Research and sponsored by Medical Economics. Through the use of an online survey, the purpose of this research project was to better understand use and performance regarding ambulatory electronic health record (EHR) systems currently available to medical professionals.
Data was collected via an online survey from June 10, 2014 to June 27, 2014. The survey was closed for tabulation with 7,442 responses. However, a majority of the study’s results are based upon the 5,790 employed respondents who indicated their practice has an ambulatory EHR system.
As with any research, the results should be interpreted with the potential of non-response bias in mind. It is unknown how those who responded to the survey may be different from those who did not respond. In general, the higher the response rate, the lower the probability of estimation errors due to non-response and thus, the more stable the results.
The margin of error for percentages based on 5,790 responses is ±1.3 percentage points at the 95% confidence level. The margin of error for percentages based on smaller sample sizes will be larger.
54%More than half of physician respondents say their EHR has had a positive impact on the quality of care they provide.
11%Number of physicians who said they have had their EHR system for less than 1 year.
45%of physicians reported that the overall performance of their EHR system was average to poor.

21 Medical econoMicsMedicalEconomics.com
(ERA) correctly; 53% did the same for their system’s ability to provide feedback on cod-ing errors.
“I thought those numbers should be higher,” Holmes says. “If you have a PMS that can’t post an ERA correctly, you have a prob-lem. That’s core functionality that’s been there for years.”
Some practices are still clinging to old billing systems that are no longer supported by their vendors, she notes. In addition, a substantial portion of the practice universe isn’t even using ERA yet, according to a re-cent report.
optimizAtionThe bulk of responses to questions about the respondents’ EHRs ranged from neutral to slightly positive. To Holmes, this indi-cates that much more is buried beneath the
surface of the survey results. For example, she says, she’d like to know how much IT support the respondents had available to them and how much of the EHR’s function-ality they’re actually using.
Basch takes a more optimistic view. Considering all of the difficulties doctors encounter in learning how to use an EHR and changing how they work, he says, “I’d expect people to feel neutral to slightly positive.”
The determining factor in how an indi-vidual physician or a group feels about an EHR—assuming it has decent functional-ity—is the degree to which the doctors have optimized their system so that it helps them become more efficient and deliver better care. Says Basch, “If you take a less than op-timal tool and try to optimize it, you can get better results.”

MedicalEconomics.comMedical econoMics22
e-bookDigital publication
While vendors have focused most of their development efforts on meaningful use and ICD-10 readiness, innovations are on the way to improve system functionality for physicians
by KEN TERRY Contributing editor
ehr 2.0:4 ways vendors are building better systems
Physicians continue to express dissatisfac-tion with the usability and the workflow features of electronic health records (EHRs), yet these information systems don’t seem to improve. One reason, experts say, is that vendors have poured most of their research and development budgets into meeting the requirements for meaningful use (MU) and the International Classification of Diseases-10th revision (ICD-10).
“They have only so much of a devel-opment budget, and anything that’s required by government regulations might take away from something else,” says Doug Thompson, MBA, senior re-search director for The Advisory Board Company, a healthcare consulting firm.
The poor usability of ambulatory care EHRs also can be attributed to shifts in the marketplace, notes David Kibbe, MD, president and chief executive officer of DirectTrust, a trade association for secure messaging networks. During the past few years, he says, the big EHR vendors have increasingly focused on hospital systems at the expense of ambulatory EHRs, partly
because the bulk of MU incentive payments have gone to hospitals.
At the same time, he points out, more and more physicians have gone to work for hos-pitals, and “the employed providers have be-come disenfranchised in terms of their choice of information technology. Their choices, par-ticularly in primary care, count for very little in the decisions made by those big corporate entities with respect to EHRs.”
Thompson believes that EHR vendors have improved their product designs over time. But today’s EHRs are more complicated because of their increased functionality, he adds, and can be difficult to customize.
Small to medium-sized physician practic-es may not be equipped to deal with the tech-nical aspects of these systems. “They’re prob-ably stuck with EHRs that are not customized enough, that are not easy to use, and that they don’t understand very well,” he says.
Despite all of this, however, some inno-vations are starting to enhance the usability of EHRs. These include refinements in natu-ral language processing, advances in EHRs designed for mobile devices, the addition of
23 Medical econoMicsMedicalEconomics.com
context to clinical decision support (CDS), and the spread of direct clinical messaging. Read on to find out how these developments could benefit you, either now or in the future.
1/ Natural language processingThe biggest problem that physicians have with EHRs is the way that these applications force them to enter data.
Encounter documentation with point-and-click templates can be excruciatingly slow and difficult. Physicians don’t like to type, and many doctors also have trouble using speech recognition programs, Thomp-son points out. Even if they can overcome these barriers, free text does not create the structured data that is required for MU and quality improvement.
The ideal scenario for doctors would be to speak to the computer and have it convert their speech into structured data that would automatically go into the proper fields in the EHR. That technology, known as “natural language processing” (NLP), has been under development for years. The speech recogni-tion engines used in transcription have be-come fairly accurate, but the ability of com-puters to “understand” medical terms in the context of speech and categorize them is still fairly limited.
Greenway Health, an ambulatory EHR vendor, is making use of NLP in its Prime Speech module, which it co-developed with M*Modal, a vendor of speech recognition software. Prime Speech allows physicians to “dictate and place content into existing custom clinical templates,” according to Gre-enway’s website. But Jim Ingram, MD, chief medical officer of Greenway, admits that Prime Speech is not yet able to transform speech into discrete data automatically.
Prime Speech can take information from the Greenway EHR’s patient “face sheet”—including medications, allergies, and prob-lems—and export it into the “speech docu-ment” that a doctor dictates into. The NLP application can slot the past medical history data into one of six categories that are part of the visit note. As the physician dictates, he can pull parts of the medical history into the ap-propriate sections as he goes along.
“Vital signs go into the physical exam section, for example, and the problem list would go into the assessment section,” In-gram says.
For now, Prime Speech cannot extract newly entered data from the note and export it back to the correct fields in the face sheet, but Ingram says that’s where the technology is heading. In the future, Prime Speech will also assist evaluation and management cod-ing and trigger clinical alerts.
Other vendors, including Allscripts and eClinicalWorks, have integrated aspects of NLP into their EHRs. But so far, none of these companies has had a breakthrough that would significantly improve EHR usability.
2/ MobilityMost physicians now use smartphones and/or computer tablets at work, and they would like to be able to use their EHRs on these mobile devices.
The leading vendors have accommodat-ed them to some degree by allowing their applications to run on an iPad or a smart-phone, says Kenneth Kleinberg, MD, man-aging director for health IT at The Advisory Board. But more progress has been made in ambulatory care than in acute care EHRs, and there’s a significant difference between iPad-native EHRs and mobile versions based on EHRs designed for desktops and laptops.
One problem with trying to use the desk-top model of an EHR on a mobile device is that the latter’s screen is smaller, so some in-formation may be cut off, Kleinberg notes. In addition, if a clinician tries to use the pop-up virtual keyboard on an iPad, it can cover up essential information, including alerts.
Allscripts, Epic, and Cerner—along with a number of smaller EHR vendors—have all created native apps for iPads, Kleinberg says. Allscripts’ approach is to pick the 20% of functions that physicians use 80% of the time and include that in its iPad-native Wand EHR, “recognizing that they’ll prob-ably have to return to the desktop to com-plete their work.” Allscripts Wand gives physicians the ability to review and add to documentation, prescribe electronically, and communicate with staff.
Not all vendors with mobile-native EHRs have focused on the Apple iOS. Some, like Meditech and Siemens, have used the HTML5 browser approach to format their EHRs to run on any platform, including iOS, Android and Windows. But some parts of the EHR functionality can get lost with HTML5, Kleinberg says.
Some physicians have told Kibbe that
EHR vendors have improved their product designs over time. But today’s EHRs are more complicated because of their increased functionality, and can be difficult to customize.
24 MedicalEconomics.comMedical econoMics
they prefer the touch screens on iPads to us-ing a mouse to point and click on desktops or laptops. Kleinberg acknowledges that this can be an advantage, but points out that typing is still much more difficult on an iPad than on a desktop. That’s why speech recognition is an important technology for mobile devices, he says.
While NLP hasn’t yet achieved its mobile use potential, Kleinberg believes it’s moving in the right direction.
“When you talk to the device, it’s navigat-ing to the right template. Some systems can recognize the field you’re talking about just from what you’re saying. You can go between tabs using speech; you can do almost all of it using speech,” Kleinburg says.
Noting that cloud storage of data files is essential when using mobile devices, Klein-burg adds: “I believe you can do everything you need to do on an iPad, especially the large ones they have now.”
3/ Clinical decision supportIdeally, EHR alerts and reminders can help prevent harm to patients or remind physi-cians to provide essential care. Other kinds of CDS built into the EHR’s structure can help doctors follow evidence-based guide-lines.
The drawback of alerts and reminders—the most visible form of CDS--is that they can pop up unnecessarily or erroneously. “In most systems, they’re at a very simple level,” says Dean Sittig, Ph.D., a professor at the University of Texas Health Sciences Center in Houston. “Most doctors would say they’re overly simplistic and are often wrong.”
Frequently, alerts are based on insuffi-cient information. For example, the program might tell the doctor that Valium should not be prescribed to the elderly, although the patient in question is not old. As a result of such mistakes, Sittig says, physicians ignore the vast majority of alerts in EHRs. “They think they’re almost all wrong, or that they don’t matter, or that they don’t apply.”
In some cases, he points out, the EHR alerts create confusion because they don’t include the context of why a physician made a particular medical decision. For example, perhaps the physician is prescribing a small dose of Valium to an elderly patient to ease his or her anxiety before an MRI test.
“A lot of the decision support we give is of that type: It’s true and it’s right, but it doesn’t
pertain to this patient,” Sittig says. “To get the decision support to pertain to the pa-tient, you usually need more context about that patient.”
Intermountain Healthcare, based in Salt Lake City, Utah, has developed a context-sensitive alerting system over many years, Sittig notes. As a result, he says, “Its physi-cians accept decision support more than 95% of the time.”
Intermountain is replacing its home-grown EHR with a system from Cerner, which plans to integrate Intermountain’s context-sensitive alerts into its own EHR, he says. But most other vendors aren’t mov-ing in this direction because they haven’t seen customer demand for it.
Meanwhile, researchers are seeking
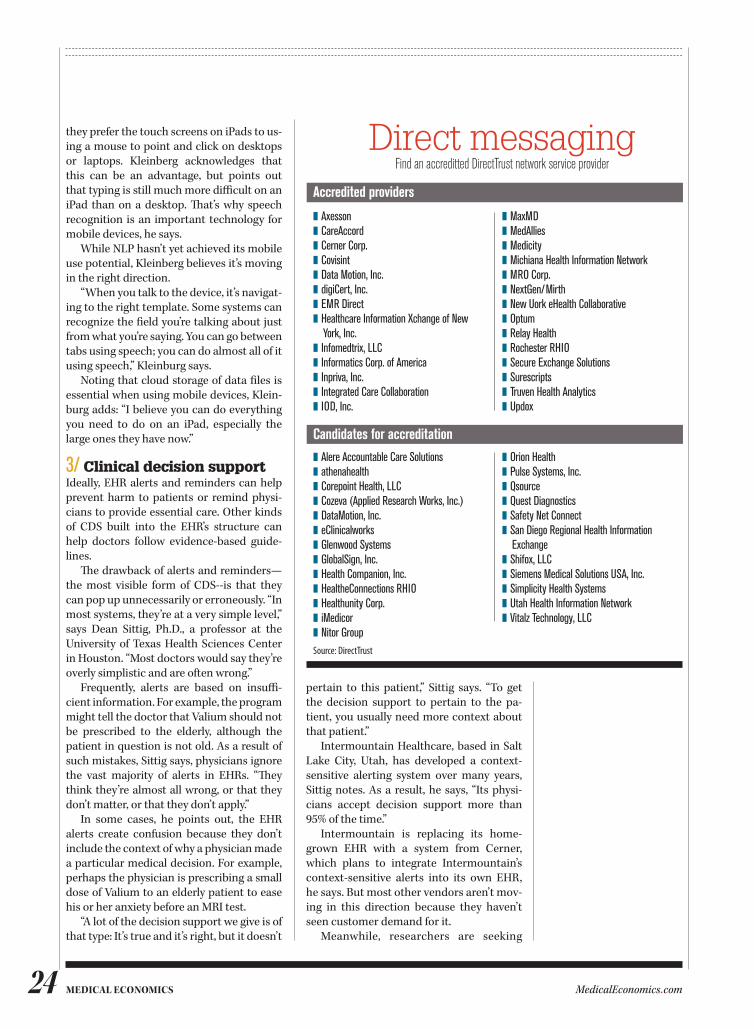
Direct messagingFind an accreditted DirectTrust network service provider
Accredited providers
Source: DirectTrust
❚ Axesson❚ CareAccord❚ Cerner Corp.❚ Covisint❚ Data Motion, Inc.❚ digiCert, Inc.❚ EMR Direct❚ Healthcare Information Xchange of New York, Inc.❚ Infomedtrix, LLC❚ Informatics Corp. of America❚ Inpriva, Inc.❚ Integrated Care Collaboration❚ IOD, Inc.
❚ MaxMD❚ MedAllies❚ Medicity❚ Michiana Health Information Network❚ MRO Corp.❚ NextGen/Mirth❚ New Uork eHealth Collaborative❚ Optum❚ Relay Health❚ Rochester RHIO❚ Secure Exchange Solutions❚ Surescripts❚ Truven Health Analytics❚ Updox
Candidates for accreditation
❚ Alere Accountable Care Solutions❚ athenahealth❚ Corepoint Health, LLC❚ Cozeva (Applied Research Works, Inc.)❚ DataMotion, Inc.❚ eClinicalworks❚ Glenwood Systems❚ GlobalSign, Inc.❚ Health Companion, Inc.❚ HealtheConnections RHIO❚ Healthunity Corp.❚ iMedicor❚ Nitor Group
❚ Orion Health❚ Pulse Systems, Inc.❚ Qsource❚ Quest Diagnostics❚ Safety Net Connect❚ San Diego Regional Health Information Exchange❚ Shifox, LLC❚ Siemens Medical Solutions USA, Inc.❚ Simplicity Health Systems❚ Utah Health Information Network❚ Vitalz Technology, LLC

25 Medical econoMicsMedicalEconomics.com
ways to improve alerts. A recent paper that Sittig co-authored proposes a system for improving CDS by using web-based monitoring tools and an interactive dash-board for evaluating alert and response appropriateness.
To avoid alert fatigue, Thompson points out, some vendors have designed their sys-tems to present information to doctors about medication safety and dosing at the point of prescribing. Only if a prescribing de-cision is truly dangerous would “the flashing light go on,” he says.
4/ InteroperabilityDespite billions of government dollars poured into EHR incentives and health in-formation exchanges, a recent Health Affairs article notes, the amount of data exchanged among providers is still very modest.
To jump-start these communications, which are vital to care coordination, the government joined with the private sector a few years ago to create the Direct secure messaging protocol. Direct is supposed to be embedded in all EHRs that have been certified for use in the second stage of the MU program. It can be used to meet the stage 2 requirement that providers ex-change care summaries at transitions of care.
The use of Direct is starting to grow and is expected to increase rapidly in 2015, Kibbe says. His own organization, DirectTrust, per-forms an important function in this field. By accrediting health information service pro-viders (HISPs), which carry secure messages between physicians with Direct addresses, DirectTrust enables the HISPs to trust each other enough to exchange secure messages. As of the end of July, the two dozen HISPs in the DirectTrust community were serving 13,000 healthcare organizations and had provided over 400,000 Direct addresses, ac-cording to Kibbe.
Direct messaging can increase the use-fulness of EHRs by enabling physicians to attach documents, such as care summaries, notes, and lab results, to messages they ex-change with their colleagues. Hospitals can also use Direct to send discharge summaries and notices of admission and discharge to doctors.
From a workflow standpoint, having Di-rect embedded in their EHRs is a boon to physicians, because they don’t have to leave
the EHR to view or download information from other providers.
But there are also disadvantages. For example, Direct can’t be used to search for information across the community. Sec-ondly, it’s designed only for point-to-point exchanges. Also, the data in the attached documents can’t flow into the structured fields of the receiving EHR.
Greenway has found that to be a problem for ob/gyn customers, who want the EHR to consume data attached to Direct messages, and vice versa, notes Mark Janiszewski, the company’s senior vice president of prod-uct management. To make this happen, he notes, Greenway has built limited interfaces for medications, problems and allergies for use with with EHRs from vendors such as Epic, Cerner, McKesson, Meditech, and CPSI.
works in progressWhile the innovations described above are all works in progress, they seem destined to benefit physicians in the long run. In the meantime, Thompson points out, there are some significant differences among EHRs, including ease of customization, whether they allow physicians to move easily among templates, and how many clicks are required to accomplish a particular task.
If you’re shopping for your first EHR or considering a switch, pay close attention to what these systems can actually do, and don’t depend on demonstrations by experi-enced users. Try them out yourself and visit other practices to see how specific EHRs are being used.
Meanwhile, keep your eye on the innova-tions that will eventually make EHRs more usable. They may be arriving sooner than you expect.
To avoid alert fatigue, some vendors have designed their systems to present information to doctors about medication safety and dosing at the point of prescribing.
MedicalEconomics.comMedical econoMics26
e-bookDigital publication
Physicians share strategies to improve quality metrics, chronic care
by KEN TERRY Contributing editor
EHRs: 5 ways to put data into action
Physician frustration over the functionality of electronic health record (EHR) systems has been escalating. While the source of physi-cian unhappiness stems from the belief that expensive technology should make their work life easier, the reality is that this technol-ogy requires greater physician involvement at a time when many practices struggle to main-tain adequate patient volumes and remain fi-nancially solvent.
The disquiet over the current state of technology was well documented in a recent Medical Economics survey of nearly 1,000 physicians in which 45% of responding physi-cians said patient care had grown worse since they implemented an EHR system. Nearly a quarter of internists said the quality of care was significantly worse.
While the message came through loud and clear in this survey, what can we learn from the silent minority about using data in their EHRs—including their Meaningful Use quality reports—to improve the quality of care they deliver?
Jennifer Brull, MD, a solo family practi-tioner (FP) in Plainville, Kansas, shares of-
fice space, staff and services with four other FPs, four midlevel practitioners, and a nurse midwife. When she and her colleagues first implemented an EHR in 2007, she screened only 43% of her eligible patients for colorectal cancer; in the next few years, with the help of EHR reminders, she raised that rate to 90%. She also used the EHR to increase her pa-tients’ recommended mammography rate from 65% to 99%.
Chronic care also benefited from her practices’ EHR use. In 2012, Brull and her colleagues were regularly testing only 14% of their patients with diabetes for micro-albumin. After educating their staff in the process and turning on an alert in their EHR, they raised that number to 95% within nine months. In 2012, only 11% of their heart fail-ure patients had received a recommended echocardiogram within the previous two years; by the end of 2013, the network had in-creased that to 68%.
Most of the data you need to improve the quality of care is in your EHR, says Rosemarie Nelson, a Medical Group Management As-sociation consultant based in Syracuse, New

27 Medical econoMicsMedicalEconomics.com
York. “But in some cases, the tools to make the data useful are not there,” she notes. Even when those functions are present, she adds, clinicians don’t necessarily use them.
If you find EHR documentation a bit over-whelming and resent the time it takes away from patient care, you might view the idea of using your EHR for quality improvement as a non sequitur. But some studies show that EHRs also do improve patient care and safety. Moreover, we’re entering a new era of value-based reimbursement, in which part of your income will be based on your quality scores. So it’s worth considering how your EHR can help you raise those scores.
EHR ChallengesEHRs were not originally designed for qual-ity improvement, but rather for improving efficiency and documentation so that doc-tors could get a return on their investment. But with the advent of Meaningful Use, ven-dors had to rewrite their software to pro-duce quality reports in order to get certified for Meaningful Use. At the same time, physi-cians started to pay more attention to qual-ity improvement.
The Breakaway Group, a health informa-tion technology consulting firm owned by Xerox, surveyed physician practices with EHRs in 2009 and found that fewer than 20% of them were trying to understand how EHRs affected quality of care. Today, partly because of Meaningful Use, “people are be-ing forced to answer some of those ques-tions,” says Heather Haugen, PhD, managing director of the Breakaway Group.
EHR vendors are offering better tools for quality reporting than they did a few years ago, Nelson notes. But the quality of these tools varies considerably, and some of them must be purchased as add-ons, she says.
The leading EHRs include health main-tenance alerts that remind physicians about some of their patients’ preventive and chronic care gaps when they see them. In some systems, however, users have to build their own alerts, Nelson says.
If an EHR includes prebuilt alerts, you may be able to customize or add to them. Brull says this is not a big chore in her EHR. She has customized about 25% of the health maintenance alerts—most of them in less than five minutes each.
Certified EHRs must be able to extract quality data for Meaningful Use. While the
clinical quality measures are very limited, they can be used in quality improvement, Nelson says. In some EHRs, for example, you can get a list of diabetic patients with an HbA1c >8 by clicking on the percentage of patients in that category.
Unfortunately, Brull says, “That’s where it stops in our EHR software. You can’t click on the patient’s name and go to their chart, which is the most actionable next step.”
The other problem with the reports in Brull’s EHR, she says, is that they can’t be customized. That is one reason why her group has acquired web-based registry soft-ware that interfaces with its EHR. This ap-plication, which also has population health management features, can generate a wide range of custom reports.
“The ability to customize reports is some-thing the EHR vendors are working on,” Hau-gen says. “But it’s definitely not there. What most practices do, if they want to get this information, is hire people who can write those custom reports.”
Of course, many practices can’t afford to pay a technical expert to program these re-ports, so it doesn’t get done, she adds.
Registry functionsRegistries, which track the services provid-ed to patients along with indicators of their health status and due dates for recommend-ed care, are not yet being widely used in healthcare, Haugen says. But some vendors have begun to incorporate registry func-tions into their EHRs, according to Nelson.
Several vendors, for example, offer the ability to query the database for a range of dates, she says. For example, the EHR could supply a list of patients with uncontrolled hypertension who haven’t been seen in three months and don’t have an appointment in the next three months.
Brull’s EHR can’t do this, but her group can use the web-based dashboard of its out-side registry for that purpose. “If I have a pa-tient with high blood pressure (BP) who fails to come see me for a prolonged period of time, they won’t show up on my EHR report, but they will show up on my registry report as a patient with hypertension who has not had their BP checked in an interval of time,” she says.
Making the data actionableSeeking to capitalize on the new opportuni-
5 ways to put data into action1. Use EHRs as reminders
2. Customize health maintenance alerts
3. Use registry functionality
4. Share results with the healthcare team
5. Maximize benefits of structured data
28 MedicalEconomics.comMedical econoMics
ties for value-based reimbursement, a grow-ing number of healthcare organizations are using EHRs and other kinds of health IT applications to identify patients who have care gaps. But relatively few of them are able to ensure that those gaps are filled, Haugen says.
In large part, that’s because EHRs lack the functionality to make the data actionable. For example, even if the EHR has a built-in registry, it may not be able to upload a list of patients who need a specific service to an automated messaging system or send a message to those patients through the EHR’s patient portal, Nelson says.
Brull agrees. There’s a “registry proces-sor” function in her group’s EHR that lets the practice email a list of patients who need services, she says. But even if the network could send such emails securely, she notes, it’s not easy to construct the end-to-end pro-cess with the outside registry. “All the pieces are there, but they’re not ‘click here and do this.’ You have to know what you’re doing,” she says.
Instead, the group exports the registry report data to an Excel file that includes pa-tient demographic information, including addresses and phone numbers. Since regu-lar mail hasn’t proved to be effective, the staff either calls patients or contacts them via the patient portal, “but it’s not an auto-mated process,” Brull notes.
The large group approachIn a large group practice the challenges are somewhat different. The EHR usually oper-ates on a central server, and the quality re-ports are programmed by the organization’s IT department. The organization may also have a mechanism for contacting patients who are not in compliance with their pro-viders’ care plans.
Robert Segal, MD, works for Scottsdale Healthcare in Scottsdale, Ariz. His ambu-latory EHR is used by hundreds of physi-cians that are employed by the healthcare system. When the system decides that it wants the doctors to focus on a particular quality area, a report-writing team creates the requisite reports, and data on individ-ual doctors’ performance is sent to them monthly.
In the near future, Segal says, the organi-zation will begin giving the physicians com-parative quality reports. He welcomes those
because they will show him where he stands in relation to his peers and how he can im-prove his quality scores.
While some healthcare organizations use this approach, others don’t even share the quality data with their doctors, Haugen says. She cites the example of a large hospi-tal group that was collecting quality data for Meaningful Use but was not communicat-ing it to the physicians. They told her, “We’d like to see the data but no one is showing it to us.”
Haugen comments, “In some respects, small practices are doing this better because their ability to affect the process is some-times much more immediate.”
Structured data is keyAlthough doctors don’t like to hear it, their ability to use their EHRs to improve qual-ity depends on whether they enter key data into the system in structured form. If the data is not in codified fields, it doesn’t show up in reports or health maintenance alerts.
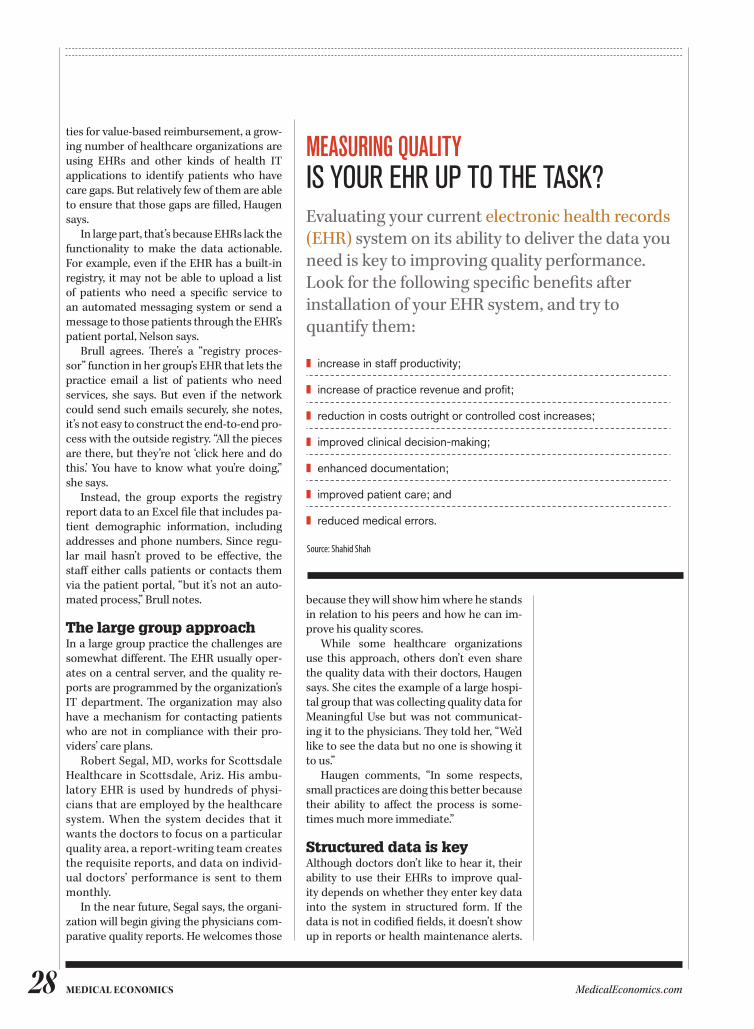
❚ increase in staff productivity;
❚ increase of practice revenue and profit;
❚ reduction in costs outright or controlled cost increases;
❚ improved clinical decision-making;
❚ enhanced documentation;
❚ improved patient care; and
❚ reduced medical errors.
MEasuRIng QualIty IS YOUR EHR UP TO THE TASk?Evaluating your current electronic health records (EHR) system on its ability to deliver the data you need is key to improving quality performance. Look for the following specific benefits after installation of your EHR system, and try to quantify them:
Source: Shahid Shah
29Medical econoMicsMedicalEconomics.com
Consequently, those reports and alerts may not be reliable.
Haugen, a strong proponent of struc-tured data entry, acknowledges that this is a sore point for doctors. But not all data has to be structured to improve quality, she says. What practices need to do is fi nd “a happy medium between what data must be struc-tured and what can be unstructured,” she notes. Vendors must also do their part to make it easier for physicians and their staff s to enter the data, she adds.
Nelson suggests that practices work on improving clinical documentation if they want to improve quality. Also, she says, the
physicians in a group should standardize their EHR templates and enter data the same way. If one doctor uses a template that suits him or her, but nobody else uses it, quality improvement will suff er.
In the end, you’ll get out of the EHR what you put into it. If big chunks of data are miss-ing, you can’t use the information to deliver better care. Also, remember that the EHR is only a tool; process improvement is up to you and your staff .
“We can track the quality of care with the EHR, but the EHR doesn’t change the care we’re providing,” Haugen observes. “So we have a big step to take beyond the EHR.”
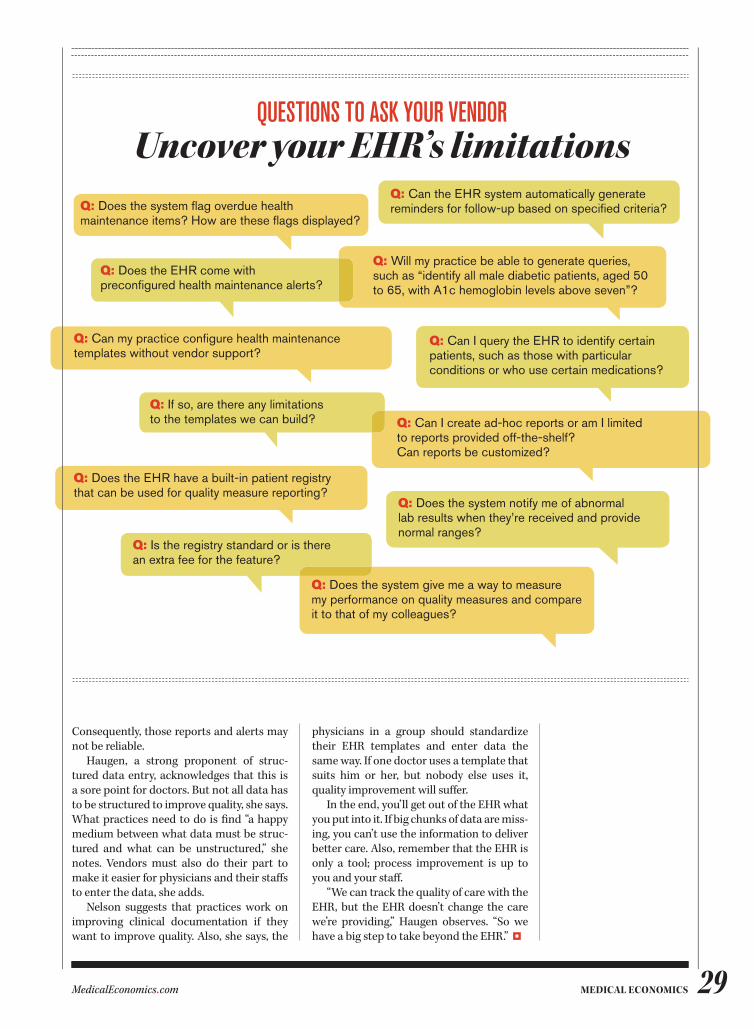
QuEstIons to asK youR VEndoRUncover your EHR’s limitations
Q: Does the system give me a way to measure my performance on quality measures and compare it to that of my colleagues?
Q: Does the system notify me of abnormal lab results when they’re received and provide normal ranges?
Q: Can I create ad-hoc reports or am I limited to reports provided off-the-shelf? Can reports be customized?
Q: Can I query the EHR to identify certain patients, such as those with particular conditions or who use certain medications?
Q: Will my practice be able to generate queries, such as “identify all male diabetic patients, aged 50 to 65, with A1c hemoglobin levels above seven”?
Q: Can the EHR system automatically generate reminders for follow-up based on specifi ed criteria?Q: Does the system fl ag overdue health
maintenance items? How are these fl ags displayed?
Q: Does the EHR come with preconfi gured health maintenance alerts?
Q: Can my practice confi gure health maintenance templates without vendor support?
Q: If so, are there any limitations to the templates we can build?
Q: Does the EHR have a built-in patient registry that can be used for quality measure reporting?
Q: Is the registry standard or is there an extra fee for the feature?
MedicalEconomics.comMedical econoMics30
e-bookDigital publication
Getting patients to use the EHR patient portal is a key part of meaningful use stage 2
by ANDREA DOwNING PECK Contributing editor
How to optimize your patient portal
If you are a physician looking to optimize the use of your practice’s patient portal, you may be the most effective marketing tool and an important reason for the technology’s suc-cess –or failure–to build practice efficiencies and patient loyalty.
About 25% of physicians or their care teams last year communicated with patients using a portal, according to Manhattan Re-search’s 2014 “Taking the Pulse” survey. That number is likely to go higher as Medicare-el-igible providers attesting for meaningful use Stage 2 (MU2) use secure messaging to com-municate “relevant health information” with patients.
Launching a campaign to extol a portal’s 24/7 convenience and timesaving services is essential for driving up patient adoption numbers, but providers ultimately wield the greatest influence when encouraging pa-tients to register and use the technology.
When Jose Polanco, MD, joined Blackstone Valley Community Health Care (BVCHC) in Pawtucket, Rhode Island, as medical director in 2012, physicians were beginning to pro-mote the portal in the exam room, a formula that helped push portal registration from
roughly 2,000 patients to today’s total above 3,300.
“It makes a huge difference because peo-ple want to talk to their provider,” Polanco says. “If your physician tells you, ‘You can email directly with me,’ it’s very powerful. People will walk out [of the exam room] and do the registration.”
In addition to supplying providers with small portal registration information cards to give to patients, BVCHC trained a cross-sec-tion of staff members ( front desk, medical as-sistants and nurses) at each of its three clinics in the portal registration procedure and hired an engagement coordinator to do outreach and targeted enrollment for the portal.
Minimizing portal painPatient engagement strategist Jan Olden-burg, a senior manager for healthcare and consumer advisory service at Ernst &Young LLP, acknowledges that the portal has been a problem for many practices, particularly if the impact on workflow has not been con-sidered from registration through ongoing use.
“Getting portal use up should be thought

31 Medical econoMicsMedicalEconomics.com
of as a team sport in the office,” Oldenburg says. “It has to be embedded in the work-flow and everybody in the office has a role in making this happen. I recommend put-ting in scripts for everyone—from the per-son who does the registration to the person who rooms the patient, for the nurse, the doctor, phlebotomist. Everybody has a role in getting a patient registered and giving them permission to use the capabilities and reminding them this is another way to make the clinic accessible to them.”
Oldenburg says providers also should find ways to make a portal rollout “fun” for both patients and staff by marketing the por-tal at community health fairs, offering prizes to staff members who register the most pa-tients or holding monthly prize drawings for patients who sign up. An awareness cam-paign also can include “theme” days such as
Hawaiian Fridays when staff show pa-tients how to “surf ” their way to the portal.
“Stop thinking about the portal as drudg-ery, but as something cool and innovative,” she says. “Promote it as a part of how we do business.”
Zachary Landman, MD, senior research-er, Institute for Strategy and Competitive-ness at Harvard Business School, says regis-tering patients is only half the battle.
“In the beginning, a lot of physicians and people who designed portals were under the impression that if you build it, they will come,” says Landman, former chief medical officer at DoctorBase. “You can have initial registration levels pretty high, but getting people to log on, access and use the portals has turned out to be a more difficult con-cept.”
Landman offers a simple method for transforming patients into active users. “It’s quite easy,” Landman says. “As a clinician, you just have to use it. The number one way to engage your patients is to use the portal to engage your patients. Reach out to them. Encourage them to put more of their data into the portal so it becomes not something the patient checks one a year when they get a lob, but a dynamic process and a relation-ship building tool between not only the phy-sician, whose time is constrained, but the entire care team.”
BVCHC’s providers help drive traffic to the portal by sending patients pre-formulat-ed email messages that alert them if a pre-scription refill has been sent to a pharmacy
or a lab has returned normal. In addition, at the end of each office visit, they send a “Pa-tient Plan” document to the patient’s por-tal that includes a visit summary as well as goals and educational information.
“By sending something to the portal, we’re making it more meaningful for the pa-tient to visit their account,” Polanco says.
Until recently, however, BVCHC’s Next-Gen portal was available only in English, effectively excluding the practice’s large Spanish-speaking patient population from the site.
“We were going up against a very strong barrier for the first three to four years,” says
4 tips to market your patient portal
1 Get the entire staff involved Everyone in the practice should be involved in promoting the benefits of using the patient portal. The front office can display signs and posters, staff members can distribute brochures to patients, and providers can discuss the use of the portal during patient visits.
2 Simplify registration Have a staff member assist patients with registering for the portal. If you can overcome the registration barrier, patients will be more likely to use the portal.
3 EngageA portal that provides mostly administrative functions, such as scheduling appointments and obtaining lab results, will be helpful but not as interesting to patients. Patients will be more likely to use a portal that is designed to address their personal needs. Portals that include interactive and personalized tools will be more engaging.
4 A two-way streetOne of the best ways to convince patients to use the portal is to communicate with them through it. Communication should go both ways. If a patient sends the physician a secure message through the portal, reply using the portal function (using case-by-case discretion, of course).
Source: HealthIt.gov

32 MedicalEconomics.comMedical econoMics
Nicole Gendron, BVCHC communications manager and project manager for portal implementation. “Only in the last year has it become available in Spanish. We are hoping this will drive up our enrollment numbers.”
Embracing secure messagingMany physicians remain reluctant to adopt portal technology out of fear that secure messaging with patients will cause them to lose control over their personal time or ex-pose them to increased liability. But Daniel Brown, MD, of Family Medicine Associates in South Attleboro, Massachusetts, has em-braced email communication with his pa-tients and has been rewarded for it.
“It ends up being one of those unpredict-able factors that increase the bond between provider and patient by increasing the level of trust or comfort,” he says. “I especially love receiving comments that say, ‘Wow! I can’t believe how fast you got back to me.’ The portal is a very, very significant factor not only in my satisfaction as a provider but also the satisfaction of my patients.”
Brown, whose 12-provider private prac-tice has registered 75% of its patients for the portal, responds to patient messages periodically during the evenings and week-ends, a habit he believes ultimately makes his workweek more efficient and enjoyable.
“If I check five or six times over the course of a weekend and take care of 15 or 20 mes-sages that may have come in, that makes Monday morning a lot easier, “ he explains. “If some nights, I go back and see if anything has come in, it will make tomorrow morning a lot easier.”
Occasionally, a patient will send him a never-ending email, a problem Brown solves with a no-nonsense reply.
“I tell patients upfront that if I get a long message from you, my response will be: ‘I’m your doc, not your pen pal. Too much here for this format. Let’s have you come into the office,” he says.
Brown, who uses athenaCommunicator, says the portal and related add-on services produce benefits that go beyond decreasing phone calls and reducing mailing costs.
“The portal helps increase my efficiency and productivity by helping to shape a pa-tient’s next visit or by not tying up a spot in office for someone who has a new prob-lem, a higher reimbursed visit, rather than a quickie follow-up just to find out that cream worked and the rash is gone,” he says.
Salvatore S. Volpe, MD, a Staten Island, New York-based internist and Medical Eco-nomics editorial board member, suggests providers attend more Health Information Management Systems Society meetings so they can see firsthand the money-saving ad-vantages today’s rapidly improving portals offer.
Volpe estimates his eClinicalWorks por-tal saved him “at least half a full-time em-ployee” by streamlining appointments and reducing calls to the office for medical refills and referral requests. He also praises use of a mobile app that enables patients to share their health information with any doctor with Internet access.
While debate continues over charging patients for portal access, Volpe agrees with the providers who view the technology as a part of doing business and a product that can pay for itself.
“I decided I wasn’t going to charge people for it,” says Volpe. “It introduced efficiencies into my office, which covered whatever ad-ditional cost there were to have a portal.”
IT MAkES A HUGE DIffERENCE BECAUSE PEOPLE WANT TO TALk TO THEIR PROVIDER. If YOUR PHYSICIAN TELLS YOU, ‘YOU CAN
EMAIL DIRECTLY WITH ME,’ IT’S VERY POWERfUL.”— JOSE POLANCO, MD, MEDICAL DIRECTOR, BLACkSTONE VALLEY COMMUNITY HEALTH CARE, PAWTUCkET, RHODE ISLAND

33 Medical econoMicsMedicalEconomics.com
Financial considerations have stopped him from opening the portal’s secure mes-saging feature to patients, however.
“Once Medicare starts reimbursing, I’ll build it into my workflow,” he says, “But until it gets reimbursed, it is hard enough to do patient-centered medical home and not get reimbursed from CMS [Centers for Medi-care and Medicaid Services]. To add this ad-ditional feature would be very hard.”
The future of the portalAs portals continue to evolve, Ernst & Young’s Oldenburg hopes physicians “re-frame” their view of the technology and no longer see it as “one more thing that is being thrown at them.”
“It is something that can be transfor-mative in the way they practice medicine and transformative for their relationships with patients and the loyalty they build,” she says.
But Joanne Rohde, chief executive officer of Axial Exchange in Raleigh, North Caro-
lina, believes patients will not fully embrace portals until the technology becomes a gate-way to self-care, not simply an alternative to phoning their doctor’s office.
“Patients definitely want to get more in-volved in their own healthcare, but patient portals right now aren’t necessarily the right mechanisms to do so,” she says. “Patient portals as mandated by MU2 are doing ad-ministrative tasks, such as appointments and refills. They aren’t making sure you are managing your blood pressure. They are not making sure you understand your dis-ease state. That’s what the industry needs to move toward for self-care.”
Rohde is hopeful Apple’s new “Health” app, a partnership with Epic and Mayo Clinic, may provide the kick-start healthcare needs.
“The key is getting both the patient and the physician to step on the treadmill, be-cause we are in an Internet-enabled world and healthcare is the last industry not to be,” she says.
THE PORTAL HELPS INCREASE MY EffICIENCY AND PRODUCTIVITY
BY HELPING TO SHAPE A PATIENT’S NEXT VISIT.”— DANIEL BROWN, MD, fAMILY MEDICINE ASSOCIATES, SOUTH ATTLEBORO, MASSACHUSETTS
MedicalEconomics.comMedical econoMics34
e-bookDigital publication
Seventy percent of physicians now use elec-tronic prescribing through their electronic health record, and in 2013, the number of pre-scriptions sent electronically topped 1 billion, according to the latest report from the Office of the National Coordinator for Health Infor-mation Technology (ONC).
The report, which analyzed data from Surescripts, looked at the volume ofe-pre-scriptions from December 2008 to April 2014, after the Medicare Improvements for Patients and Providers Act (MIPPA), an e-prescribing incentive program, was passed. The report found a ten-fold increase in providers’e-pre-scribing rates during that timeframe.
Minnesota had the largest increase, with only 4% of its physicians e-prescribing in 2008
and 100% of physicians doing so in 2014. As of April, Indiana had a 95% e-prescribing rate, followed by Massachusetts at 94% and South Dakota at 90%.
The report credits the jump in e-prescrib-ing to the MIPPA. Before it’s implementation, the rate among physicians was at 7% in De-cember 2008. The number of pharmacies that accepted e-prescriptions also increased dur-ing that period, from 76% in 2008 to 96% in 2014.
The global e-prescribing market is grow-ing at a rapid pace. It’s projected to balloon from $250.2 million to $887.8 million by 2019, according to a report released in June by Transparency Market Research.
ONC report shows 7 in 10 physicians are using EHRs for patient prescriptions
by ALISON RITCHIE Contributing editor
E-prescribing rates soar among physicians
35 Medical econoMicsMedicalEconomics.com
e-bookDigital publication
E-prescribing is bringing substantial benefits to the nation’s healthcare system, but signifi-cant barriers remain to its more widespread adoption, a new research study concludes.
The study, in the form of a systematic re-view, examined the findings of 47 articles looking at e-prescribing—which the authors define as “the computer-based electronic generation transmission, and filling of a pre-scription”—from a variety of clinical and fi-nancial perspectives. The results appear in an article titled “Electronic Prescribing: Im-proving the Efficiency and Accuracy of Pre-scribing in the Ambulatory Care Setting” in the Spring 2014 issue of Perspectives in Health Information Management.
The benefits found in the review include:
Improved patient safety: E-prescrib-ing makes prescriptions more legible, de-creases the time needed to prescribe and dispense medications, and reduces medica-tion errors and adverse drug events (ADEs) due to the presence of medication decision support (MDS) systems. One study of 12
community-based practices found that er-ror rates dropped from 42.5 to 6.6 per 100 prescriptions one year after the adoption of e-prescribing.
Greater efficiency: Though it takes about 20 seconds longer per patient to enter a prescription into a computer than to write it by hand, “this time is offset by the time saved because of the fact that less clarifica-tion is needed for electronic prescriptions,” the authors say. At the pharmacy, meanwhile, prescriptions received electronically produce less paperwork and fewer issues that need to be resolved compared with paper prescrip-tions.
Cost savings: The authors cite a study by the clinical network Surescripts showing an estimated $140 billion to $240 billion in savings and improved health outcomes over 10 years, mainly due to better medication ad-herence and reduced ADEs. The Surescripts study also found a 10% increase in the num-ber of e-prescriptions filled compared with written prescriptions.
In addition, e-prescribing systems that use MDS can help doctors choose lower-cost al-
by JEFFREY BENDIx Senior editor
E-prescribing is benefitting healthcare system, but barriers to adoption remain

36 MedicalEconomics.comMedical econoMics
ternatives to brand-name drugs can reduce prescription drug costs. The authors cite a 2005 study involving 19 physicians that found a 17.5% decrease in prescriptions for high-cost drugs compared with the control group, leading to a savings of nearly $110,000 over 12 months.
Barriers to the greater use of e-prescribing include:
Implementation costs: “New technol-ogy requires training and information tech-nology support for installation and upkeep,” the authors note. “A practice must take these costs into account when deciding whether to implement an e-prescribing system and
when choosing a stand-alone system or one that is integrated into an EHR system.”
Alert fatigue: Faced with numerous alerts each time they enter a prescription, many providers stop reading the alerts, with the result that they may ignore a potentially dangerous interaction.Privacy issues: Without effective firewalls and other safeguards, prescription data trans-mitted electronically may be breached, lead-ing to HIPAA violations and fines. In addition, “most information breaches actually occur as a result of employees’ actions, so continuous training on security is imperative and can in-cur additional costs,” the authors write.
37 Medical econoMicsMedicalEconomics.com
e-bookDigital publication
Voice recognition software, scribes allow physicians to focus on the patient, rather than the computer screen
by BETH THOMAS HERTz
Ways to optimize EHR documentation at your medical practice
Electronic health record (EHR) systems are built to help physicians improve their practic-es. But EHRs may also come between a physi-cian and a patient during an encounter. Many physicians believe they spend more time typ-ing into a computer instead of looking their patients in the eye. The bottom line: EHRs re-quire physicians to rethink their documenta-tion strategies.
When physicians are trying to decide what is best, Peter Basch, MD, chair of the Ameri-can College of Physician’s Medical Informat-ics Committee, advises them to look at their overall goals.
“The issue is not just typing. The issue is understanding where we are in the evolu-tion of having a computer in the room with a patient,” he says. “Is there is value in having a third party in the room with the doctor and patient? That third party is information that helps us deliver better, safer and perhaps even less expensive healthcare.”
He compares the new paradigm to a pilot using a checklist prior to takeoff.
“A good pilot doesn’t just make eye contact with the copilot or stare out the window. A
good pilot also attends to other appropriate information for helping to better assure a safe flight,” Basch says. “The same is true in medi-cal care. We quickly forget why the computer is there. It’s not a punishment for not taking typing in eighth grade. The primary purpose is not the documentation. The primary pur-pose is, at least in my opinion, how we better interact with the information.”
Options are available to physicians look-ing for a way to improve their doucmentation strategies. They range from typing furiously, while potentially ignoring the patient, to us-ing scribes, voice recognition technology, or even continuing to take notes by hand and entering them into the computer later.
How EHR is used is keyNo matter what input method is used, physi-cians must prevent the computer from im-peding communication with patients, Basch says.
“Triangulate the screen so that the doc-tor, patient, and family can see it and use it as a tool to improve education, safety, and outcomes,” he suggests. “Do not keep the
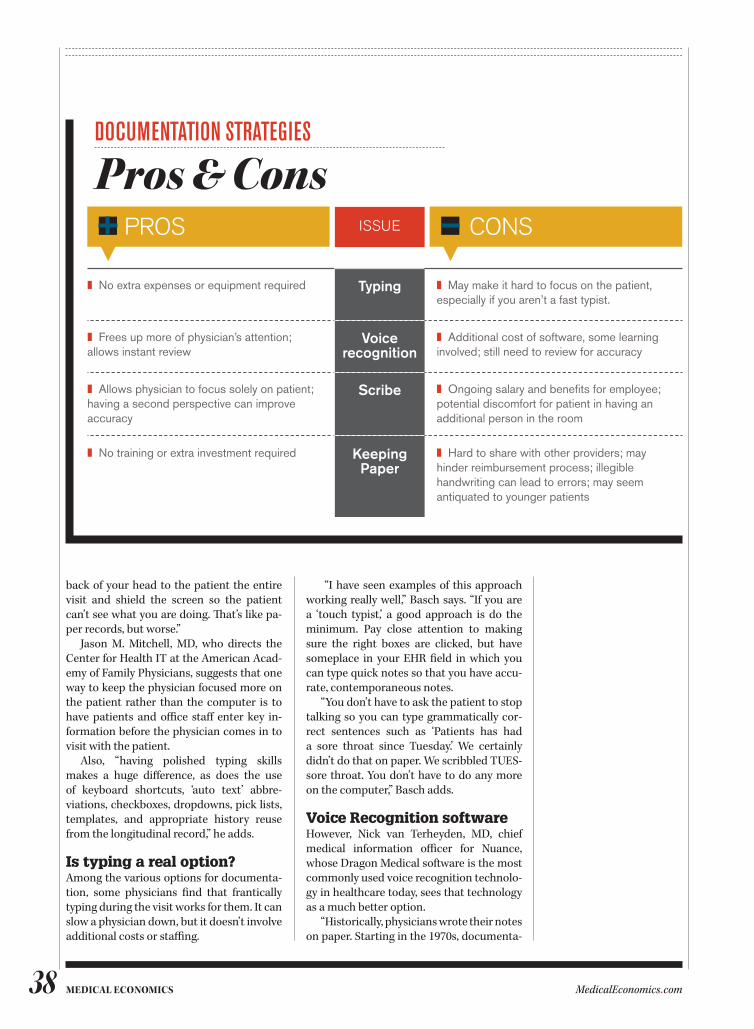
38 MedicalEconomics.comMedical econoMics
back of your head to the patient the entire visit and shield the screen so the patient can’t see what you are doing. That’s like pa-per records, but worse.”
Jason M. Mitchell, MD, who directs the Center for Health IT at the American Acad-emy of Family Physicians, suggests that one way to keep the physician focused more on the patient rather than the computer is to have patients and office staff enter key in-formation before the physician comes in to visit with the patient.
Also, “having polished typing skills makes a huge difference, as does the use of keyboard shortcuts, ‘auto text’ abbre-viations, checkboxes, dropdowns, pick lists, templates, and appropriate history reuse from the longitudinal record,” he adds.
Is typing a real option?Among the various options for documenta-tion, some physicians find that frantically typing during the visit works for them. It can slow a physician down, but it doesn’t involve additional costs or staffing.
“I have seen examples of this approach working really well,” Basch says. “If you are a ‘touch typist,’ a good approach is do the minimum. Pay close attention to making sure the right boxes are clicked, but have someplace in your EHR field in which you can type quick notes so that you have accu-rate, contemporaneous notes.
“You don’t have to ask the patient to stop talking so you can type grammatically cor-rect sentences such as ‘Patients has had a sore throat since Tuesday.’ We certainly didn’t do that on paper. We scribbled TUES-sore throat. You don’t have to do any more on the computer,” Basch adds.
Voice Recognition softwareHowever, Nick van Terheyden, MD, chief medical information officer for Nuance, whose Dragon Medical software is the most commonly used voice recognition technolo-gy in healthcare today, sees that technology as a much better option.
“Historically, physicians wrote their notes on paper. Starting in the 1970s, documenta-
doCuMEntatIon stRatEgIEs
PROS ISSUE CONS
Pros & Cons
❚ No extra expenses or equipment required Typing ❚ May make it hard to focus on the patient, especially if you aren’t a fast typist.
❚ Frees up more of physician’s attention; allows instant review
Voice recognition
❚ Additional cost of software, some learning involved; still need to review for accuracy
❚ Allows physician to focus solely on patient; having a second perspective can improve accuracy
Scribe ❚ Ongoing salary and benefits for employee; potential discomfort for patient in having an additional person in the room
❚ No training or extra investment required Keeping Paper
❚ Hard to share with other providers; may hinder reimbursement process; illegible handwriting can lead to errors; may seem antiquated to younger patients

39 Medical econoMicsMedicalEconomics.com
tion had to be legible in order for them to be paid. This gave rise to a large transcription industry,” he says.
Early voice recognition technology could create a first draft, but it had to be cleaned up by a medical editor. However, today’s technology can create a highly accurate transcript that the physician can review in real time and share immediately with other providers if needed, he says.
Most physicians can learn to use voice recognition very quickly, he says. The tech-nology lets users specify the dialect with which they speak and their medical special-ty, and creates a profile to assist them. Some physicians may find they need to adjust their style of dictation, though.
Van Terheyden’s brother is a physician who realized through using voice recogni-tion that he wasn’t as fluent as he thought he was when he dictated, and worked to im-prove how he presents information.
“He is now proud of his clinical notes,” van Terheyden says.
Such improved clinical notes offer a com-plete narrative of the patient’s story. More intricate details from the visit that may have been missed in the past are captured.
“We all look at lab results and vital signs, but we are really interested in the details of how patients present,” he says. “Eighty per-cent of my diagnostic process comes from the patient history, about 15% from my ex-amination, and about a 5% contribution from the investigations and tests that con-firm or refute my findings.
“If you only capture information from drop-down lists and checked boxes, you lose some of the fine details,” he adds. “Speech preserves it.”
As a bonus, patients can review the dic-tated notes on the computer screen with the physician and correct any errors. “Who has the most vested interest in the successful outcome of the interaction? The patient,” he says. “They can make a wonderful, positive contribution.”
Voice recognition is a time saver for many physicians, he says. One physician he knows works in several locations, one of which does not have speech recognition capabilities. This physician often works an extra hour or more a day to complete his documentation at that location.
Van Terheyden notes that there are many pricing models for voice recognition tech-
nology, based on how many patients the pro-vider sees and the activities he or she needs to document. Some EHR systems come with the technology built in, so physicians do not see it as a separate cost. For others, the soft-ware needs to be added. Most systems will work with piggybacked voice recognition software, although not all.
Many primary care practices can save enough money from eliminating transcrip-tion to recoup the cost of the software and microphone in three to six months, he adds.
Also, voice recognition turns dictation into actionable data tagged against a medi-cal vocabulary, van Terheyden says. This gives providers real-time feedback, such as suggesting a diagnosis that might be indi-cated by the constellation of symptoms. It can also help ease the transition to the In-ternational Classification of Diseases—10th Revision (ICD-10) because it prompts the physician to enter details, such as laterality, up front.
Basch notes that some physicians use voice recognition in a hybrid manner, using a minimal template with key boxes and us-ing voice recognition to add a narrative that accurately reflects what the patient said.
“This is a very powerful thing, particu-larly for patients who have had bad experi-ences with other doctors,” he says.
ScribesAnother documentation strategy is hiring scribes. Scribes can be highly accurate and serve as a backstop for catching physician errors. However, they have several disadvan-tages, namely their ongoing salary, which they likely will expect to increase each year. Also, having a third person in the exam room can make some patients reticent to discuss their condition in a frank manner.
Basch recalls that when he was in train-ing decades ago, the most efficient doctor he ever saw was an ear, nose, and throat spe-cialist who used a scribe. The scribe would tell the doctor the key points from the last visit or remind him of things he wanted to recheck, while he examined the patient and offered comments aloud.
“Certainly that is a way to do it but since it is expensive, it is not for everybody,” Basch says. “If you hire the right person and they know medical terminology, it can be a time saver. But know that you are still signing the notes, so you still need to review them.

40 MedicalEconomics.comMedical econoMics
Mitchell says that the usefulness of scribes can depend on the physician’s prac-tice style.
“Significant benefit comes from a bidi-rectional interaction of the physician and the EHR. Data validation tools, data reuse mechanisms, and clinical decision support tools are all dependent on the provider di-rectly interacting with the EHR. This is com-plicated by putting a scribe between the physician and the EHR,” he says.
“Some systems (SOAPware, for exam-ple) are introducing the concept of ‘virtual scribes’ as a part of the EHR itself. This keeps the physician interacting with the record and the patient and benefiting from the data management and decision support tools that EHRs have to offer,” Mitchell adds.
Still attached to paper?Despite the spread of EHRs, paper charts are still very much in use. Basch, who has been in practice for 33 years, says they appeal particularly to older physicians who feel un-skilled in rapid typing or proper use of voice recognition.
“If this is an issue for you, don’t struggle with it,” he says. “Work with colleagues, a physician champion, your organization, or a vendor to come up with alternate
mechanisms for data entry in the room with a patient so you can focus on the things that you need to. See if you can get a tablet that supports handwriting recognition. Or even stick with paper. In contrast to what some say, paper doesn’t kill. Paper usually cuts. Medical errors can kill.”
Using paper in the exam room and input-ting your notes later is better than leaving medicine, he says. “If you are a talented per-son, don’t give up.”
Mobile platforms can provide a mid-point for some physicians. For example, iPads can accept dictation and allow inter-action. A software program that Nuance makes, called Florence, helps physicians access information from complex medical records. Instead of navigating a menu tree to find lab results, they can just say, “Show me the lab results.”
Mitchell agrees that physicians must use whatever tools are necessary to provide the best care to their patients. “The wrong EHR badly implemented and poorly used by a physician can cause far more harm than effective use of a paper chart. However, the right EHR, well implemented and skillfully used by a physician is far better than a paper chart,” he says.
41 Medical econoMicsMedicalEconomics.com
e-bookDigital publication
Value-based incentives can help practices offset EHR costs and derive a return on investment
by KEN TERRY
Utilize your EHR system to boost practice revenue
It’s difficult for small practices to get a return on investment (ROI) from their electronic health record (EHR) systems, even if they re-ceive government Meaningful Use payments, health information technology consultants say. Still, it’s possible for practices to achieve ROI if they participate in alternative delivery models that help them garner value-based re-imbursement.
The two traditional sources of ROI are increased efficiency and higher charges, based on better documentation. Using an EHR to increase efficiency requires major changes in office processes, and the gov-ernment has recently increased its scru-tiny of certain documentation techniques that help practices justify higher charges.
As a result, says Michelle Holmes, a prin-cipal with ECG Management Consultants in Seattle, Washington, not many small practic-es can achieve ROI on their EHRs in a fee-for-service world.
“The big Meaningful Use incentive dol-lars were in the early years,” she notes. “So at this point, the practices’ spend is greater
than what they take in, unless they’re doing something in addition to the EHR implemen-tation.”
Nevertheless, Holmes and other experts say, it’s possible for practices to achieve ROI if they participate in alternative delivery models that help them garner value-based reimbursement. These include accountable care organizations (ACOs) that participate in shared savings programs; Patient-centered Medical Homes, which many insurers incen-tivize; and pay-for-performance programs that pay quality bonuses.
All of these models, to varying extents, require the use of EHRs. Therefore, Holmes notes, not having an EHR represents an
“opportunity cost” that can be quantified and weighed against the cost of installing a system.
Most practices are still not receiving much, if any, income from value-based re-imbursement. But ACOs and medical homes are increasing, and some physicians are be-ginning to see the possibility of achieving ROI.

42 MedicalEconomics.comMedical econoMics
Nephrology group counts on ACOSimon Prince, MD, is part of a seven-doctor nephrology practice in Manhasset, New York. The physicians have attested to Mean-ingful Use for two consecutive years, but those payments covered only 20% to 25% of what they invested in their EHR, Prince says.
While the EHR has made the practice more efficient in some ways, in other ways it has decreased efficiency and productivity, he says. For example, documentation of patient encounters takes him longer than it used to. On the other hand, improved documentation has led to fairer reimbursement, in his view.
With these and other factors included in the analysis, he says, the ROI on his EHR “is around a wash,” at best. But the group’s participation in an independent practice as-sociation that has turned into an ACO could change the picture in the long run, he says.
The ACO, which Prince leads, includes 325 doctors in 100 practices. It participates in the Medicare Shared Savings Program (MSSP) and is one of 29 ACOs that qualified for bo-nuses in that program’s first year. The ACO also holds shared-savings contracts with sev-eral private payers.
To participate in the ACO, a practice must either have an EHR or plan to acquire one within 12 months. The EHR is necessary partly because the Centers for Medicare and Medicaid Services (CMS) factors the per-centage of ACO members who have achieved Meaningful Use into its bonus calculations. Also, some of the quality measures in the MSSP require clinical data that’s easier to collect with EHRs.
Prince believes that once the MSSP bo-nuses start flowing, they will help him and his colleagues in the ACO achieve ROI on their EHRs. He’s not sure those bonuses will be sub-stantial, but he believes that value-based pay-ments will continue to increase for practices that participate in the Medicare and health-plan shared savings programs.
Meanwhile, he points out, the ACO has barely begun to take advantage of its EHRs. The 30 EHRs used by member practices can-not yet exchange information with each oth-er; when they do, it will be much easier to co-ordinate care. Currently, he notes, the ACO’s population health management software uses claims data, combined with clinical data that practices enter on a web portal and lab data feeds.
Incentives payfor small practice’s EHRJeffrey Kagan, MD, of Newington, Connecti-cut, practices internal medicine with one other physician and a nurse practitioner (NP). The group’s EHR cost about $120,000, including interest payments. Meaningful Use incentives will cover most of that.
Learning the EHR slowed the doctors and the NP initially, but productivity has rebound-ed, and they see more patients now than they did before implementing the system. More-over, Kagan notes, “We’re billing at higher lev-els than we did before.”
So even though the practice is paying about $5,000 a year for software maintenance and may have to buy some new computers, it has achieved ROI on its EHR, he says.
Kagan, a Medical Economics editorial board member, expects further ROI from participation in an ACO and from pay-for- performance. The EHR allows his practice to pull quality data that it sends to the ACO. In turn, the ACO reports on the physicians’ performance to CMS’ Physicians Quality Re-porting System (PQRS), which pays bonuses for reporting.
In addition, when insurance companies ask Kagan to fill out quality improvement forms, he can use the EHR to complete them, which results in small additional payments. While Kagan is not yet getting pay-for-per-formance bonuses from the health plans, he says, “I think that’s coming.”
Other sources of ROIAs Kagan’s story shows, it’s still possible to get ROI from a combination of meaningful use incentives, efficiency, and higher charg-es. But it’s getting harder to pull off.
“Some people do get ROI, but it requires real change,” observes Rosemarie Nelson, a Medical Group Management Association healthcare consultant in Syracuse, New York and Medical Economics editorial consultant. “People want to keep what they do the same, so they try to retrofit the technology into their current processes. But in order to take advan-tage of what the technology offers, your pro-cesses must change.”
Nelson says she has seen practices that don’t take advantage of their EHR’s ability to track test orders against results to see if they came back. Instead, nurses print out the or-ders and put them in a tickler file. Nor do they use patient portals that enable patients to
ehr return on inVestment
According to a survey of 49 community practices in an EHR pilot program:
$43,743the amount the average physician is expected to lose over five years using an EHR
27%number of practices that would have received a positive return on investment, according to results of the survey.
Source: Health Affairs, March, 2013

43 Medical econoMicsMedicalEconomics.com
self-register and enter their chief complaint and family/social history before scheduled visits.
Holmes agrees that process redesign is es-sential if practices want to increase efficiency. But because of the tight MU deadlines, she says, “people aren’t taking enough time to implement these systems in a way that might increase efficiency.”
The amount of additional revenue prac-tices can realize by coding higher depends on whether they were undercoding before they got their EHRs, Holmes notes. But even if they could raise their charges by improv-ing documentation, CMS is looking closely at physicians who copy parts of past notes into current notes or who document by ex-ception. The threat of being accused of fraud has thrown a chill into physicians, she says. As a result, many are coding more conserva-tively.
Other factorsAnother key factor in ROI is the 5-year cost of an EHR system. Vendors of web-based EHRs claim that their products are cheaper than site-based systems because they have a lower upfront cost. But Nelson says that the research she’s seen shows that the differenc-es in 5-year costs are “insignificant.”
Holmes contends, however, that there is a difference in cost that depends on the size of the practice. Larger groups can get econo-mies of scale by hosting their own EHR, but small practices can’t. Therefore, the latter are probably better off with a cloud-based EHR, she says.
Costlier EHRs have sophisticated features not found in modestly-priced systems, in-cluding business intelligence and advanced reporting features that can be useful in popu-lation health management.
Holmes doesn’t think that small practices need these features.
“That’s one way to look at the ROI,” she points out. “How much are you paying for the stuff you’re actually using? If you’re paying $1 million for the EHR, but you’re only using the features and functions you could have gotten in a simpler EHR for $250,000, you may have overpaid.”
Nelson sees the cost/benefit ratio in terms of how well a practice implements its EHR. “A really good Amazing Charts implementation probably has a way better ratio than a poorly implemented NextGen,” she says.
Finally, don’t forget about the practice management system that comes with most EHRs. If that doesn’t work well, you’re going to feel the pain in your bottom line.
For a variety of reasons, including the chal-lenge of maintaining an interface, it makes sense to buy an integrated EHR/practice management system, rather than separate systems, Nelson notes. And if you outsource your billing, you should hire a service that uses the practice management system that comes with your EHR, she adds.
If you’re not getting ROI on your EHR, don’t despair; that EHR could be the ticket to future revenue streams. But to enjoy those added revenues, you’ll have to start partici-pating in the programs and alternative care delivery systems available to you.
Also, don’t worry if you and your col-leagues can’t yet use your EHRs to optimize your income from these new models. As Prince explains, “We’re succeeding despite the challenges that we have with getting any data out of our EHRs. We find that the ROI from that perspective is limited for now, but the potential is there.”
estimAting A return on inVestmentWhen constructing a business plan for the purchase or switch of an electronic health record (EHR) system, most practices need to consider four cost centers:
❚ hardware,
❚ software,
❚ implementation and training,
❚ support and maintenance.
ROI is calculated by: Gross revenues collected
– Direct costs of an EHR
– Indirect costs of operating EHR
– Financing costs associated with purchases
= Net profit (or loss)

Copyright 2014, Advanstar Communications Inc. All rights reserved. Reproduction in whole or in part is prohibited without prior written permission of the publisher.