eh vol12 no1 lakhani
TRANSCRIPT
8/4/2019 EH Vol12 No1 Lakhani
http://slidepdf.com/reader/full/eh-vol12-no1-lakhani 1/8
Electronic Healthcare, Vol. 7, No. 3 Online Exclusive 2008
11
ElectronicHealthcare
ABSTRACT
The establishment of a decision support management and planning process at Bloorview
Kids Rehab in Toronto, Ontario, has driven operational and physical changes at Canada’s
largest children’s rehabilitation, teaching and academic health centre. Decision support
provides Bloorview management with integrated, evidence-based and user-friendly tools to
plan programs and allocate resources; measure organizational, program and staff perform-
ances; and provide timely accountability to the province’s Ministry of Health and Long-Term Care. Not only has Bloorview shifted the internal culture to engage staff in planning
the decision support system and developing meaningful data, but the hospital has also
situated decision support within the hospital’s Planning and Organizational Effectiveness
Department, supporting an integrated model of organizational performance. Users’ and
management’s endorsement of decision support processes is foundational to our organiza-
tional and program effectiveness.
IN CONTEXT: DECISION SUPPORT AND BLOORVIEW KIDS REHAB
At the end of the 20th century and into the early years of the 21st, various decision
support processes specific to healthcare settings and predicated on information
technologies have proliferated in Ontarian, Canadian and North American settings– from local community hospitals to tertiary and quaternary academic health science
centres. Reports indicate that Canada’s business-intelligence market in healthcare grew
10% from 2003 to 2004 (Himmelsbach 2005), with a predicted compound annual
growth rate of 8.1% up to 2008. The use of such information technologies has two
core objectives: (1) to better understand how hospital resources are used and (2) to
demonstrate, in an evidence-based way, an institution’s commitment to quality care
and efficient operations. As argued by Kron (2004), the challenge in healthcare has
never been a lack of data, even prior to the increasingly central role of decision support
Transforming OrganizationalCulture through Decision Supportat Bloorview Kids Rehab
Hakim Lakhani, Lynn Guerriero, Linda Hatton and Christopher Lau
8/4/2019 EH Vol12 No1 Lakhani
http://slidepdf.com/reader/full/eh-vol12-no1-lakhani 2/8
Transforming Organizational Culture through Decision Support at Bloorview Kids Rehab Hakim Lakhani et al.
Electronic Healthcare, Vol. 7, No. 3 Online Exclusive 2008
2
tools and organizational structures in developing and deploying information. There
has traditionally been a wealth of data, “notoriously fragmented and often incomplete,
making analysis and knowledge distillation from such sources an ongoing challenge”
(2004:15).
Nowhere is this challenge – the problem of being data rich but information poor
– more critical to address than in Ontario (though it may be equally critical in various
jurisdictions in Canada and globally). With the installation of the McGuinty Liberals in
2003, the Ministry of Health and Long-Term Care cited its Information Management
Strategy as essential to the province’s transformation of the healthcare system, under
the Canadian universal healthcare model, to one that is more patient-centred, is safer,
provides better access to care and contains costs. At the federal level, Romanow (2002)
also cited health and information technologies as an “essential foundation” of health-
care reform.
Bloorview Kids Rehab in Toronto, Ontario, is in a unique position nationally. We are
the only children’s rehabilitation treatment centre of such size and scope in the country.
We have also undergone fundamental organizational and directional changes over the
past dozen years. Among these have been the merger of Bloorview Children’s Hospital
and the Hugh MacMillan Rehabilitation Centre in 1996; Bloorview’s fully affiliated
status as a teaching hospital of the University of Toronto in 2002, making it Canada’s
first such centre in pediatric rehabilitation and delivering the country’s largest training
program in developmental pediatrics; the founding of our Research Institute in 2004
and the establishment of three research chair positions; and the major rebuilding of
Bloorview’s physical plant, completed in 2006.
Bloorview sees 7,000 clients through 52,000 outpatient visits and 600 in-patient
admissions annually. It has 850 employees, including 300 clinical staff, and approxi-mately 1,000 medical students and medical residents in training. Our nine most
commonly seen types of clients have such conditions as cerebral palsy, acquired brain
injury, muscular dystrophy and developmental disabilities. Clinicians’ and scientists’
growing understanding of the genetics of these conditions and the use of evolving
biotechnology tools are increasing, as are the complexity, acuity and frequency of
certain of these conditions in the pediatric population. Toronto is also the centre of
growth in Canada’s rehabilitation population, growth that is particularly evident in the
age group of 10- to 19-year-olds.
In short, Bloorview must deliver on our vision, “a world of possibility,” through a
broadened scope of practice that builds the province’s capacity in pediatric rehabilita-tion and increasingly emphasizes research and innovation as fundamental to evidence-
informed treatment of disabilities in children – even as we maintain our high degree of
client and family satisfaction and stay responsive to issues of timely care, quality and
cost efficiency.
CHANGING THE CULTURE: DEVELOPING, USING AND SHARING
INFORMATION
“With IBM Cognos software, I can look at everything from workload and over-workload;
8/4/2019 EH Vol12 No1 Lakhani
http://slidepdf.com/reader/full/eh-vol12-no1-lakhani 3/8
Transforming Organizational Culture through Decision Support at Bloorview Kids Rehab Hakim Lakhani et al.
Electronic Healthcare, Vol. 7, No. 3 Online Exclusive 2008
3
to the flow of children through the clinics; to staff sick time; to the allocation of staff to
specific programs. The data analysis I can do from Cognos software is essential in collabo-
rating with my staff during performance reviews and led to an evidence-based proposal for
more operating budget to prevent staff burnout.” (Andrea Tsuji, neuromuscular and spina
bifida programs)
As indicated earlier, the decision to install a constellation of decision support mecha-
nisms at Bloorview Kids Rehab was in line with other healthcare institutions’ moves
in this direction around this period. The way in which Bloorview collaboratively
planned and carried out this process, and the corporate and financial resources that
such a relatively small health centre (albeit mighty in scope) atypically put to decision
support (Kron 2004), have predicted the accolades that Bloorview Kids Rehab has
since received.
Decision support does not have one accepted definition. That of Marakas “as an organ-
ized set of tools intended to impose structure on portions of the decisions-making
situation and to improve the ultimate effectiveness of the decision outcome” (2003:29)
fits with Bloorview’s conception. Decision support is a corporate analytical tool, a core
enabler in implementing organizational strategy and in motivating or redirecting effort
(Longest 2003). At Bloorview, the system builds on and extends beyond information
technology (IT) components. Our efforts and data are focused on utilization manage-
ment, quality improvement, planning and personnel performance management.
From the start, decision support was a senior management, not a project management,
imperative. Reflecting that orientation, the decision support staff of three were situated,
non-traditionally, within the health centre’s Planning and Organizational Effectiveness
Department rather than in corporate services/information systems; hence, there were
structural linkages between, as well as single senior leadership for, decision support,quality, patient safety and risk management. This allowed for the development of a
fully integrated performance measurement and reporting model, with decision support
playing the central role in data and information reporting. As a top-down strategy, it
nevertheless actively engaged both the departments holding data (custodians) and the
data users (e.g., clinical program managers, administration, senior [executive] team
members and the board of trustees) in planning the system, with senior leadership
also participating on the Decision Support Steering Committee. Decision support
continues to add data capability in collaboration with end users and to respond to
information requests in collaboration with data custodians.
Active collaboration is far from a nicety, far from a device of internal relations correct-ness. It is perhaps a less typical approach among organizations establishing a decision
support system, yet it is an identified key to success in implementing new technologies
or their functions (Kron 2004; McGregor 2006). The main return on investment that
Bloorview aimed to gain from decision support was a breaking down of our silos of
information and an improved quality of data. These silos were barriers to integrated
knowledge – and, indeed, barriers to ready access to useable, reliable information –
barriers that exist in many healthcare settings.
8/4/2019 EH Vol12 No1 Lakhani
http://slidepdf.com/reader/full/eh-vol12-no1-lakhani 4/8
Transforming Organizational Culture through Decision Support at Bloorview Kids Rehab Hakim Lakhani et al.
Electronic Healthcare, Vol. 7, No. 3 Online Exclusive 2008
4
BEFORE DECISION SUPPORT
Prior to launching the first phase of IT infrastructure for decision support, Bloorview’s
different departments collected data according to their own metrics, terms of refer-
ence and needs, be they finance, human resources or health records data, for example.
Hospital executives and senior managers were likely to use a “spray and pray” strategy
to these various areas to glean important information for planning and decision-
making. At that time, different departments might have yielded different answers to
the same question. Information silos and data discrepancies at Bloorview were also
exacerbated by the realities of two newly merged organizations, with data at varying
stages of depth. These barriers were reinforced by practical ones – the time it took to
develop one-off reports, time potentially doubly wasted in the duplication of data
collection efforts from one department to another and then the time and effort to
laboriously produce spreadsheets on paper and “pray,” in the case of the data custodian
(or the report writer), that his or her efforts would be user-friendly enough to be read
and considered.
AFTER DECISION SUPPORT: PUTTING PEOPLE AND PROCESSES
TOGETHER WITH TECHNOLOGY
“Everyone up the chain uses the system: staff have access to stats related to their work, and
input their own. We managers are frequent users, both of the Meditech/IBM Cognos system
and the resources of the decision support team. And directors and VPs go into the system to
communicate online with managers, for planning and decision-making and to report to the
ministry.” (Monica Gemeinhardt, manager, child development teams)
Bloorview Kids Rehab developed a comprehensive decision support system that trans-
formed how information is accessed, used and shared. Fundamental to system is that
the technology (Figure 1) is the “glue” for data sharing, rather than the goal itself. Apart
from the more technical aspects of the system, Bloorview embraced the following key features in our decision support to ensure success:
• Recruited in-house expertise who blend IT expertise with the team’s motivation and
experience in understanding Bloorview’s clinical “business”
• Developed an ongoing, collaborative decision support plan and rollout, as described
previously
• Proved the benefit of centralized decision support services and analysis first through
the team’s real-time response to challenging information requests – and only after-
ward demonstrated what the technology itself could do
• Developed a user-driven system, both in terms of data needs and the technology’s
ease of use• Established the foundational data system of modules and the business-intelligence
system – all built on consistent definitions on the data points (“sick time,” “unique
client,” etc.), a system to which all licensed users have access
• Developed “canned” reports that integrate commonly used data for managers’ analysis
and decision-making – for example, from workload, staff performance and client-
satisfaction cubes; the system is also flexible enough for online users to create their
own reports from within a cube and to accommodate senior leadership’s requests for
customized reports
8/4/2019 EH Vol12 No1 Lakhani
http://slidepdf.com/reader/full/eh-vol12-no1-lakhani 5/8
Transforming Organizational Culture through Decision Support at Bloorview Kids Rehab Hakim Lakhani et al.
Electronic Healthcare, Vol. 7, No. 3 Online Exclusive 2008
5
• Continue to commit financially to the infrastructure and technology required by
decision support; a recent Canadian healthcare technology surveys showed that
hospitals commit an average 2.5% of their operating budgets to IT (Zeidenberg
2006; Irving and Nevo 2005) whereas Bloorview is among the few that allocates
>5% annually, of which a significant component is directed to the decision support
system
• Continue internalized training and retraining on the technology, responding to the
style and pace of learners, and using Bloorview’s own data as the training tool, for
greater familiarity and relevance to the end-users: formal group training, just-in-time
one on one and learning from manuals; formal training, per trainee, is equivalent
to >0.03 of a full-time staff position
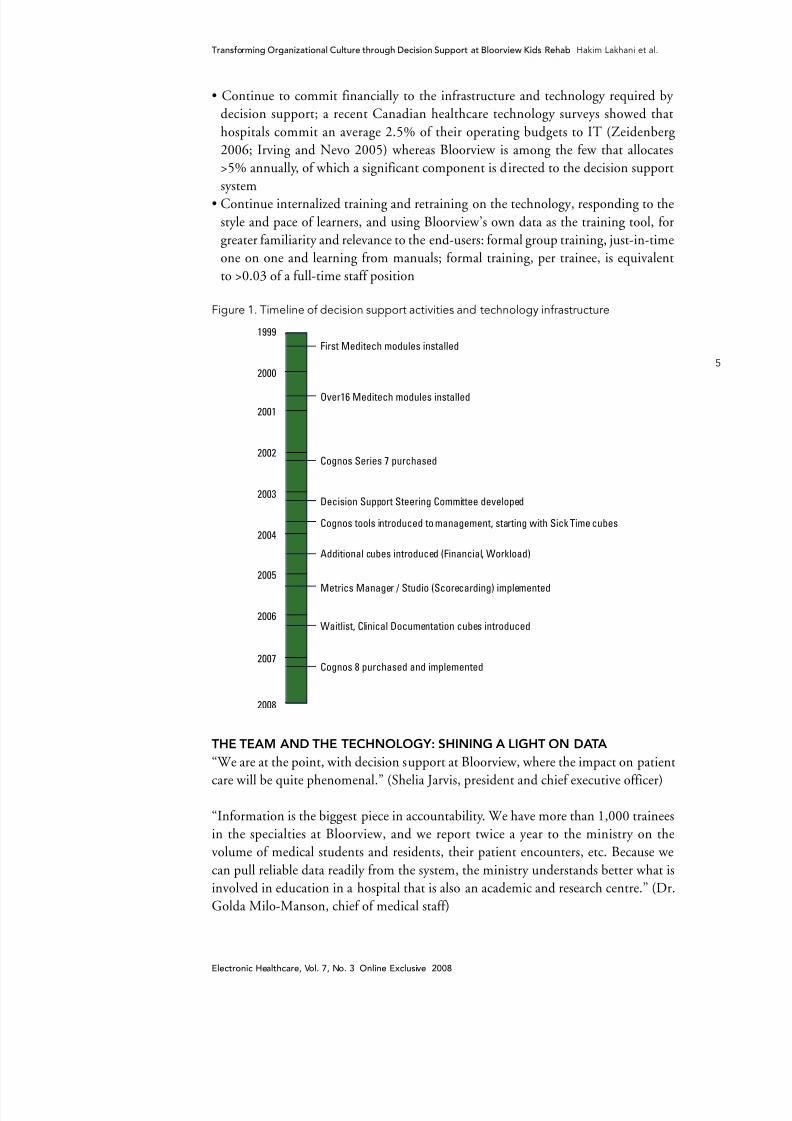
Figure 1. Timeline of decision support activities and technology infrastructure
���
���
���
����
���������
����
�����
����
����
THE TEAM AND THE TECHNOLOGY: SHINING A LIGHT ON DATA
“We are at the point, with decision support at Bloorview, where the impact on patient
care will be quite phenomenal.” (Shelia Jarvis, president and chief executive officer)
“Information is the biggest piece in accountability. We have more than 1,000 trainees
in the specialties at Bloorview, and we report twice a year to the ministry on the
volume of medical students and residents, their patient encounters, etc. Because we
can pull reliable data readily from the system, the ministry understands better what is
involved in education in a hospital that is also an academic and research centre.” (Dr.
Golda Milo-Manson, chief of medical staff)
8/4/2019 EH Vol12 No1 Lakhani
http://slidepdf.com/reader/full/eh-vol12-no1-lakhani 6/8
Transforming Organizational Culture through Decision Support at Bloorview Kids Rehab Hakim Lakhani et al.
Electronic Healthcare, Vol. 7, No. 3 Online Exclusive 2008
6
In September 2007, the Canadian Council on Health Services Accreditation accorded
Bloorview Kids Rehab full accreditation, with no recommendations. The council cited
us in particular for two leading practices: (1) for decision support, transforming a
culture to fact-based decision-making; and (2) for the Growing Up Ready Program,
preparing youth to transition to adult life. Both are recognized as leading-edge practices
nationally and internationally.
The Conference Board of Canada has also recognized Bloorview for the quality and
depth of data in the performance indicators we submit regularly to Bloorview’s Board
of Trustees, and we received the Cognos Performance Leaders Award 2007, citing
Bloorview’s ability to transform the organization from more anecdotal decision-making
to fact-based decision-making.
Other marks of our decision support success include the following:
• Senior leadership, front-line managers, clinicians and staff report that our decision
support team and business-intelligence system have made looking at data easy,
contributing to high use of the system and resulting in more time to actually analyze
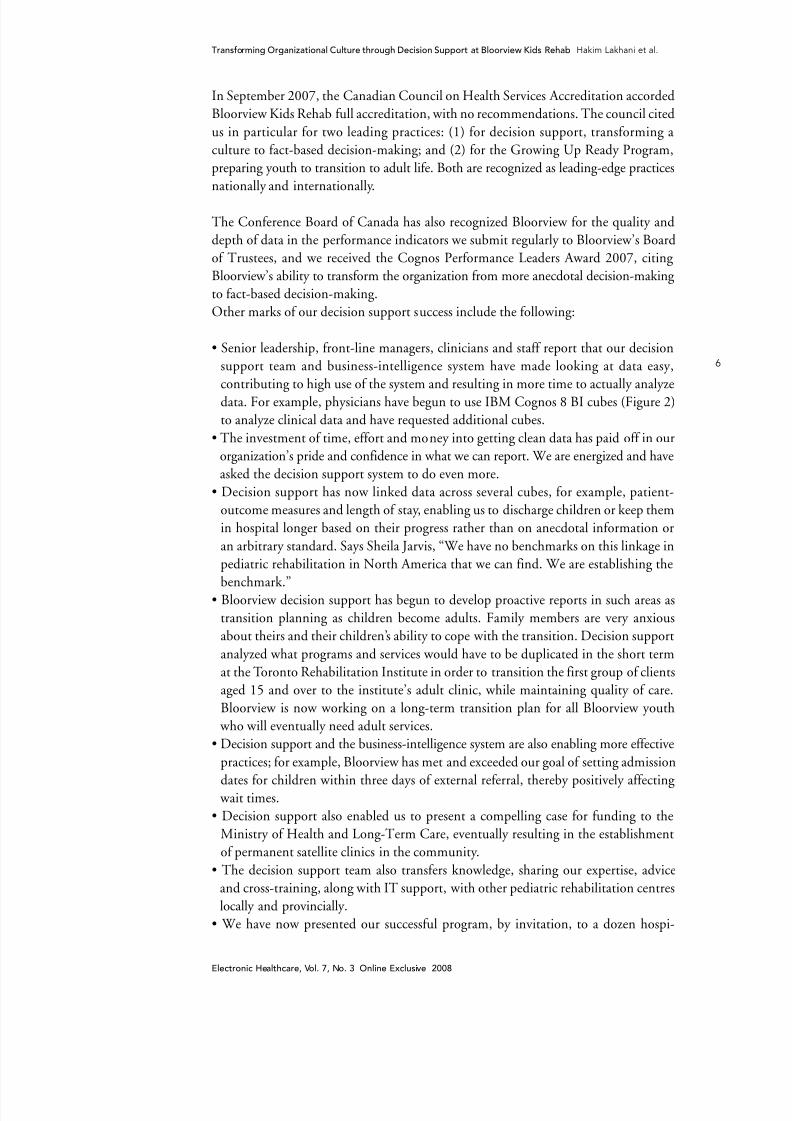
data. For example, physicians have begun to use IBM Cognos 8 BI cubes (Figure 2)
to analyze clinical data and have requested additional cubes.
• The investment of time, effort and money into getting clean data has paid off in our
organization’s pride and confidence in what we can report. We are energized and have
asked the decision support system to do even more.
• Decision support has now linked data across several cubes, for example, patient-
outcome measures and length of stay, enabling us to discharge children or keep them
in hospital longer based on their progress rather than on anecdotal information or
an arbitrary standard. Says Sheila Jarvis, “We have no benchmarks on this linkage in
pediatric rehabilitation in North America that we can find. We are establishing the
benchmark.”• Bloorview decision support has begun to develop proactive reports in such areas as
transition planning as children become adults. Family members are very anxious
about theirs and their children’s ability to cope with the transition. Decision support
analyzed what programs and services would have to be duplicated in the short term
at the Toronto Rehabilitation Institute in order to transition the first group of clients
aged 15 and over to the institute’s adult clinic, while maintaining quality of care.
Bloorview is now working on a long-term transition plan for all Bloorview youth
who will eventually need adult services.
• Decision support and the business-intelligence system are also enabling more effective
practices; for example, Bloorview has met and exceeded our goal of setting admission
dates for children within three days of external referral, thereby positively affecting wait times.
• Decision support also enabled us to present a compelling case for funding to the
Ministry of Health and Long-Term Care, eventually resulting in the establishment
of permanent satellite clinics in the community.
• The decision support team also transfers knowledge, sharing our expertise, advice
and cross-training, along with IT support, with other pediatric rehabilitation centres
locally and provincially.
• We have now presented our successful program, by invitation, to a dozen hospi-
8/4/2019 EH Vol12 No1 Lakhani
http://slidepdf.com/reader/full/eh-vol12-no1-lakhani 7/8
8/4/2019 EH Vol12 No1 Lakhani
http://slidepdf.com/reader/full/eh-vol12-no1-lakhani 8/8
Transforming Organizational Culture through Decision Support at Bloorview Kids Rehab Hakim Lakhani et al.
8
Electronic Healthcare, Vol. 7, No. 3 Online Exclusive 2008
Further goals will include balancing our research, teaching and care missions to ensure
that all these are served, using our decision support data tools; providing more proac-
tive or projective reports on such questions as target lengths of stay or incidence of
specific conditions among children in the community; integrating the electronic health
record for each patient into our decision support system; and developing e-learning
modules on the system.
That such a relatively small centre (though a national standard bearer in our field) is
making this decision support investment in time, money, effort and expertise, matched
in Canadian healthcare by only some much larger entities, speaks to how accountable
Bloorview Kids Rehab is to our mission, on behalf of our kids: to defy disability.
REFERENCES
Canadian Healthcare Technology. <www.canhealth.com/news>. <AU: Please provide author, year of publication, article title and date article was retrieved.>
Erstad, T.L. 2003. “Analyzing Computer Based Patient Records: A Review of Literature.” Journal of Healthcare Information Management 17(4): 51–57.
Himmelsbach, V. 2005. “Signs of Intelligent Life.” Computing Canada 31(8): 12–13.Irving, R., S. Nevo. 2005. “2005-06 Report on IT in Canadian Hospitals: Current Capabilities and Upcoming Acquisitions.” Thornhill, ON: Canadian Healthcare Technology.
Kron, R. 2004. “JHIM Quick Study: Healthcare Business Intelligence and Real-Time Decision SupportSystems.” Journal of Healthcare Information Management 18(3): 14–16.
Longest, B.B., Jr. 2003. “Government Relations in the Healthcare Industry.” In P. Leatt and J. Mapa, eds. Westport, CT: Greenwood Publishing Group. <AU: If this is a chapter in a book, please provide the book title or chapter title (whichever does not appear here).>
Marakas, G.M. 2003. Decision Support Systems in the 21st Century. Upper Saddle River, NJ: PrenticeHall.
McGregor, M. 2006. “What Decision-Makers Want and What They Have Been Getting.” Value inHealth 9(3): 181–85.
Romanow, R. 2002. The Future of Healthcare in Canada. Ottawa: Health Canada. Retrieved November7, 2008. <http://www.hc-sc.gc.ca/english/pdf/romanow/pdfs/HCC_Final_Report.pdf>.
Zeidenberg, J. 2006. Survey ranks top IT projects in hospitals across Canada. Retrieved May 6, 2008.<http://www.canhealth.com/may06.html>
About the AuthorsHakim Lakhani is the Vice President of Organizational Effectiveness at ErinoakKids, Centreof Development and Treatment. At the time of writing this article, he was Senior Director of Organizational Effectiveness at Bloorview Kids Rehab. Hakim founded the Decision Supportdepartment at Bloorview in 2002 and lead the organization through this journey of informationenrichment.
Lynn Guerriero is the Director of the Wait Times Information Program at Cancer Care Ontario. Atthe time of writing this article, she was the Senior Director of Community Programs at BloorviewKids Rehab.
Linda Hatton is the Senior Director of Information Systems at Bloorview Kids Rehab.
Christopher Lau is a Decision Support Analyst at Bloorview Kids Rehab.