effect of personal cancer history and family cancer history on levels of psychological distress
TRANSCRIPT
ARTICLE IN PRESS
0277-9536/$ - se
doi:10.1016/j.so
�Correspondfax: +1401 793
E-mail addr
Michelle_Roger
BPinto@lifespa
(J.M. Nash), G
Peter.C.Trask@
Social Science & Medicine 64 (2007) 411–416
www.elsevier.com/locate/socscimed
Short Report
Effect of personal cancer history and family cancer history onlevels of psychological distress
Carolyn Rabina,�, Michelle L. Rogersb, Bernardine M. Pintoa, Justin M. Nasha,Georita M. Friersona, Peter C. Traska
aThe Miriam Hospital & Brown Medical School, Providence, RI, USAbBrown University, USA
Available online 24 October 2006
Abstract
This study examined the impact of personal and family cancer history on psychological distress. Regression analyses
were conducted on a nationally representative sample of adult individuals who participated in the 2000 National Health
Interview Survey, USA. Effects on distress of a personal cancer history, any family cancer history, or mother, father, sister
or brother with a cancer history were examined. The interaction of personal and family cancer histories and three-way
interactions with gender were also assessed. Analyses indicate that having either a personal or family cancer history is
linked with significantly greater psychological distress and there is evidence of an interaction. Three-way interactions with
gender were not found. Consistent with prior research, results demonstrated that cancer survivors are more distressed than
the general population. Results extend prior research by indicating that having a first-degree relative with cancer increases
risk for distress, and having personal and family cancer histories may exert a synergistic effect on distress.
r 2006 Elsevier Ltd. All rights reserved.
Keywords: Cancer; Cancer history; Family history; Distress; USA
Introduction
Personal and/or family histories of cancer havethe potential to increase psychological distress.Research has shown that cancer survivors experi-ence greater anxiety and depression than the generalpopulation and are more likely to report havingused mental health services in the past year (Amir &
e front matter r 2006 Elsevier Ltd. All rights reserved
cscimed.2006.09.004
ing author. Tel.: +1401 793 8234;
8078.
esses: [email protected] (C. Rabin),
[email protected] (M.L. Rogers),
n.org (B.M. Pinto), [email protected]
[email protected] (G.M. Frierson),
pfizer.com (P.C. Trask).
Ramati, 2002; Hewitt & Rowland, 2002; Hewitt,Rowland, & Yancik, 2003; Hjerl, Andersen, Keid-ing, Mortensen, & Jorgensen, 2002). Less is knownabout psychological distress among individuals witha family cancer history. Some research indicatesthat those with a family cancer history experienceelevated levels of cancer-specific or general distressand that this distress exceeds levels in normativepopulations (Erblich, Bovbjerg, & Valdimarsdottir,2000; Gilbar, 1998; Kash, Holland, Halper, &Miller, 1992; Lloyd et al., 1996; Zakowski et al.,1997). Having a family history of cancer has notbeen consistently associated with elevated distress,however (Butow et al., 2005; Gilbar, 2003; Lloydet al., 1996; Zakowski et al., 1997). Discrepant
.

ARTICLE IN PRESSC. Rabin et al. / Social Science & Medicine 64 (2007) 411–416412
findings may be due to differences in eligibility andstudy design (e.g., whether controls were beingevaluated for a breast symptom; e.g., Gilbar, 2003),the status of the cancer patient (e.g., in treatment,deceased; Erblich et al., 2000; Zakowski et al., 1997)and whether the relative had cared for the cancerpatient (Erblich et al., 2000). One aim of the currentstudy was to determine whether family cancerhistory is actually associated with greater distress(although data were not available to evaluate thepreviously noted moderators). Additional aims wereto investigate the effect of having both personal andfamily cancer histories on distress and determinewhether there were three-way interactions betweenpersonal cancer history, family cancer history, andgender (as research indicates that females with apersonal or family cancer history are more dis-tressed than their male counterparts; Aass, Fossa,Dahl, & Moe, 1997).
The present study examined the responses of anationally representative sample of individuals whoparticipated in the National Health InterviewSurvey (National Center for Health Statistics,2002). We hypothesized that: (1) having a personalcancer history would exert a main effect onpsychological distress, (2) having a family cancerhistory would exert a main effect on psychologicaldistress, (3) having both personal and family cancerhistories would exert an interactive effect onpsychological distress, (4) three-way interactionswith gender would be found with females experien-cing more distress.
Methods
The National Health Interview Survey is con-ducted annually by the National Center for HealthStatistics (2002). Data are collected through ahousehold interview conducted by interviewersemployed and trained by the US Bureau of theCensus. Participation is voluntary (National Centerfor Health Statistics, 2002). A multi-stage areaprobability sampling design permits a representativesampling of households in the United States. Thisinvestigation used data from the 2000 NHIS.
Measures
Cancer history
Respondents were asked if they had ever beentold by a doctor/health professional that they hadcancer or any kind of malignancy. Individuals
responding ‘‘Don’t Know’’ or ‘‘Refused’’ wereexcluded (n ¼ 28). Respondents were also askedwhether their biological mothers, biological fathers,or any full sisters or full brothers were everdiagnosed with cancer. Responses to these itemswere used to categorize respondents according topersonal and family cancer histories. Respondentsreporting only personal or family history of non-melanoma skin cancer were classified as having nocancer history, as in prior NHIS research (Hewittet al., 2003, Hewitt & Rowland, 2002; self ¼ 451,father ¼ 645, mother ¼ 390, brother ¼ 181, sister¼ 150). Respondents reporting that they wereadopted, did not know their biological parent, didnot know whether their parent ever had cancer, didnot have any full brothers or sisters, or refusing torespond to family cancer history questions wereexcluded from the respective analysis. Finally, 747individuals reporting a child with cancer (a uniquelydistressing event) were excluded from analyses.
Distress
Respondents were asked how often over the last30 days they felt sad, nervous, restless, hopeless,everything was an effort, or worthless. Responseswere recorded on a 5-point Likert scale from ‘‘all ofthe time’’ to ‘‘none of the time’’. All six items wererecoded so that higher scores indicated morefrequent negative mood and then summed to createa (non-psychometrically validated) measure ofdistress (coefficient alpha ¼ 0.88; Kessler et al.,2003). As the scores on this continuous measure ofdistress were not normally distributed (and couldnot be normalized through any of a series oftransformations) a dichotomous measure of distresswas also included as an outcome. A cutpoint of 13on the distress measure was used to classifyindividuals as experiencing serious mental healthrisk (‘‘SMHR’’; Kessler et al., 2003).
Analyses
Analyses were conducted with SUDAAN (Re-lease 9.0.0) using Taylor-series variance estimationprocedures to account for the complex samplingdesign and sample weighting of the NHIS. Doing soprovided representative estimates of the civilian,non-institutionalized US population in 2000. Hy-potheses were tested while controlled for age,gender, race/ethnicity, education, marital status,income, and health insurance coverage.

ARTICLE IN PRESSC. Rabin et al. / Social Science & Medicine 64 (2007) 411–416 413
First, using an ordinary least squares (OLS)regression model we examined the effect of personaland family cancer history on distress. Second, usinglogistic regression, we examined the likelihood ofexperiencing SMHR, comparing those with apersonal and family cancer history to those withno reported history. Then, in four separate OLSregression models, we examined the effects ofpersonal and each type of family cancer history(i.e., mother, father, sister, and brother) on distress.Due to sample size constraints, we did not examinethe effects of each type of family cancer history onlikelihood of experiencing SMHR. (We also did notanalyze data on respondents with children diag-nosed with cancer, as having a child with cancer is auniquely distressing event and not comparable tohaving a parent or sibling with cancer.) Finally, wetested whether the combination of personal andfamily cancer histories differentially affected men’sand women’s distress.
Results
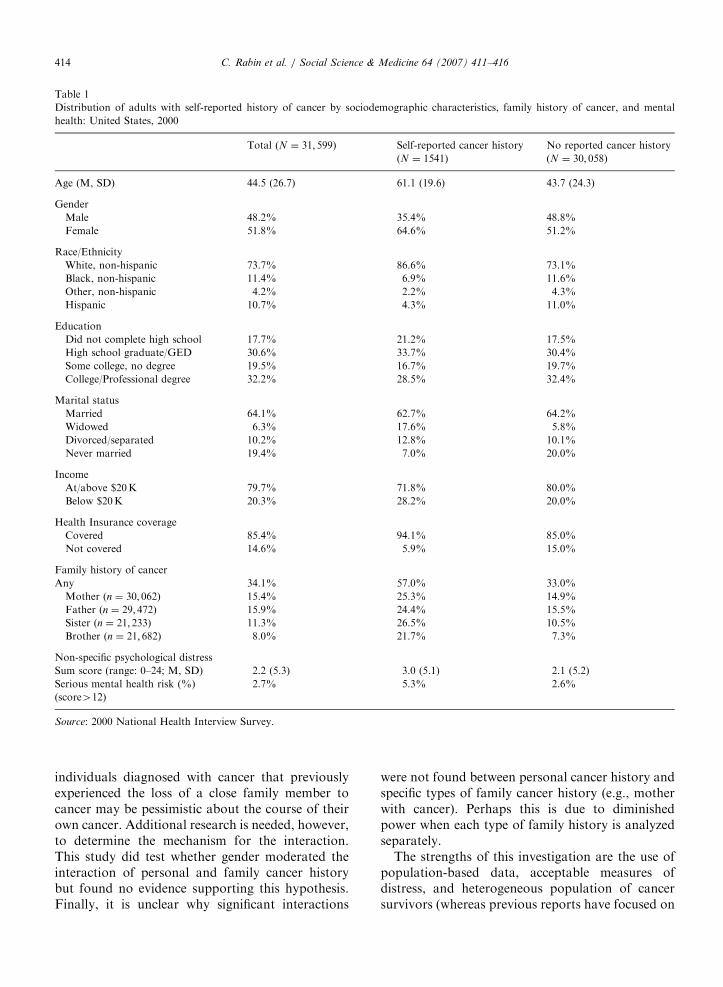
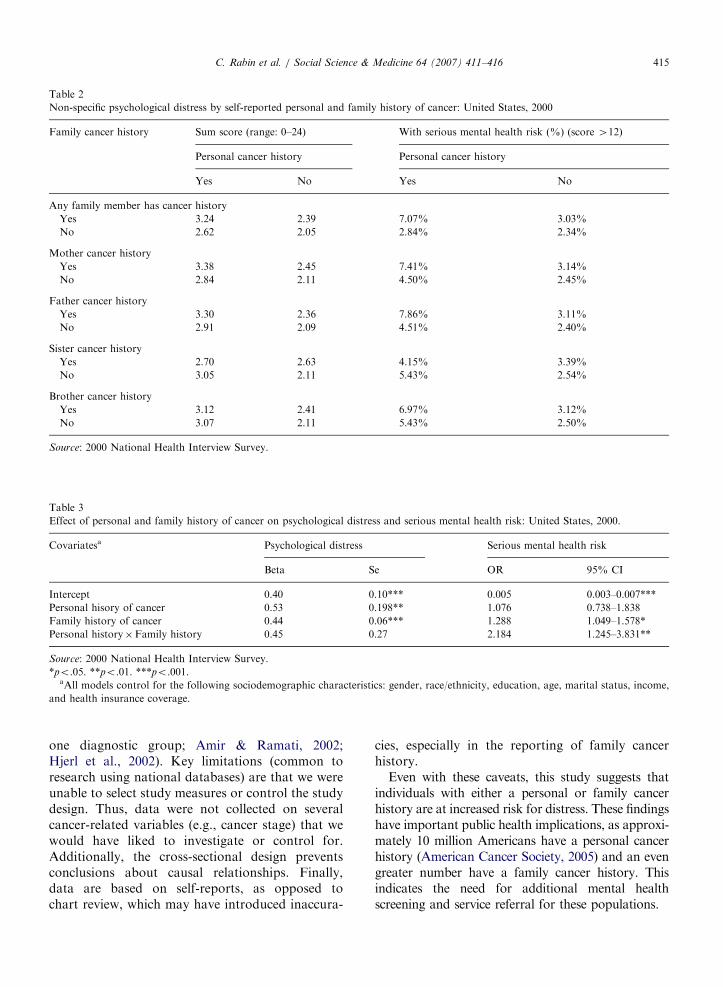
A total sample of 31,599 adults was used foranalyses. Table 1 presents descriptive informationon the sample as a whole, as well as by personalcancer history. Approximately 5% of the US adultpopulation in 2000 were cancer survivors andapproximately 34% had a family cancer history.Females were more likely than males to have apersonal cancer history (65% vs. 35%, po.0001).Those with a personal cancer history were morelikely to meet criteria for SMHR than those without(5.3% vs. 2.6%, po.0001). Table 2 providesdescriptive information on levels of psychologicaldistress by cancer history. Respondents with apersonal and/or family cancer history had higherscores on the continuous measure of psychologicaldistress than respondents not reporting a cancerhistory. Data on SMHR demonstrates a similarpattern.
Table 3 reports the results of analyses performedto determine whether there were significant mainand interactive effects of personal and family cancerhistory on distress (while controlling for socio-demographic characteristics). Consistent with bi-variate analyses, these multivariate analysesdemonstrated that those with a personal cancerhistory reported significantly more distress thanthose without. Similarly, those with a family cancerhistory reported significantly more distress and weremore likely to meet criteria for SMHR than those
without. Those with both personal and familycancer histories were more than twice as likely tomeet criteria for SMHR than others. Femalesreported significantly higher rates of distress thanmales (beta ¼ 0.51, po.0001), but were no morelikely to meet criteria for SMHR (OR ¼ 1.18, 95%CI: 0.99–1.41).
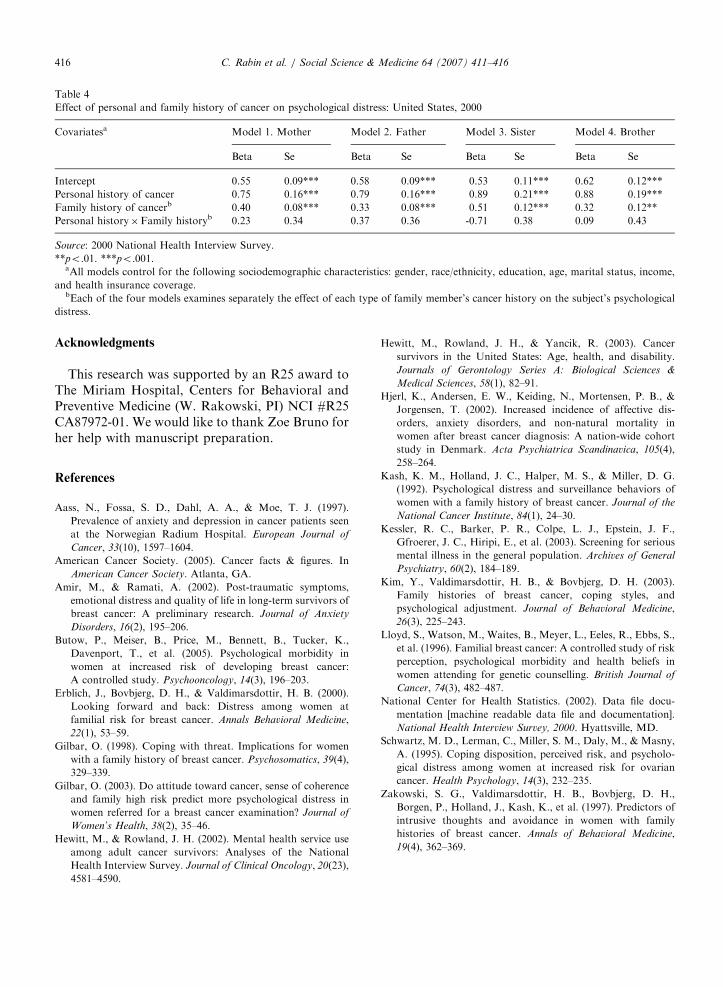
Table 4 presents analyses performed to determinewhether personal cancer history and each of thefour types of family cancer history had interactiveeffects on distress. Personal cancer history contin-ued to have a main effect on distress in each model.Having a mother, father, brother, or sister withcancer was also significantly associated with greaterdistress. None of the interactions between personalcancer history and specific types of family cancerhistory were statistically significant, however. Fi-nally, we tested the three-way interaction betweenpersonal cancer history, family cancer history (i.e.,mother, father, sister, or brother with cancer) andgender on distress. None of the models demon-strated any statistically significant three-way inter-actions.
Discussion
Consistent with prior research, findings from thispopulation-based study demonstrate that those witha personal cancer history report significantly greaterdistress than those without (Amir & Ramati, 2002;Hjerl et al., 2002). Findings also supported thehypothesis that having a family member diagnosedwith cancer would be associated with greaterdistress. Prior research has shown that those witha family cancer history are more likely to bedistressed if they lack adequate coping resourcesor social support (Kash et al., 1992; Kim, Valdi-marsdottir, & Bovbjerg, 2003), feel particularlyvulnerable to cancer themselves (Schwartz, Lerman,Miller, Daly, & Masny, 1995), cared for the cancerpatient (Erblich et al., 2000) or lost a family memberto cancer (Erblich et al., 2000; Zakowski et al.,1997).
This investigation yielded some support for thehypothesized interaction between personal andfamily cancer history. When considering all typesof family cancer history, individuals with bothpersonal and family cancer histories were mostlikely to meet criteria for SMHR. It is possible thatwhen a cancer survivor learns of a relative’sdiagnosis, it elicits the emotions engendered by thesurvivor’s own cancer experience. Conversely,
ARTICLE IN PRESS
Table 1
Distribution of adults with self-reported history of cancer by sociodemographic characteristics, family history of cancer, and mental
health: United States, 2000
Total (N ¼ 31; 599) Self-reported cancer history
(N ¼ 1541)
No reported cancer history
(N ¼ 30; 058)
Age (M, SD) 44.5 (26.7) 61.1 (19.6) 43.7 (24.3)
Gender
Male 48.2% 35.4% 48.8%
Female 51.8% 64.6% 51.2%
Race/Ethnicity
White, non-hispanic 73.7% 86.6% 73.1%
Black, non-hispanic 11.4% 6.9% 11.6%
Other, non-hispanic 4.2% 2.2% 4.3%
Hispanic 10.7% 4.3% 11.0%
Education
Did not complete high school 17.7% 21.2% 17.5%
High school graduate/GED 30.6% 33.7% 30.4%
Some college, no degree 19.5% 16.7% 19.7%
College/Professional degree 32.2% 28.5% 32.4%
Marital status
Married 64.1% 62.7% 64.2%
Widowed 6.3% 17.6% 5.8%
Divorced/separated 10.2% 12.8% 10.1%
Never married 19.4% 7.0% 20.0%
Income
At/above $20K 79.7% 71.8% 80.0%
Below $20K 20.3% 28.2% 20.0%
Health Insurance coverage
Covered 85.4% 94.1% 85.0%
Not covered 14.6% 5.9% 15.0%
Family history of cancer
Any 34.1% 57.0% 33.0%
Mother (n ¼ 30; 062) 15.4% 25.3% 14.9%
Father (n ¼ 29; 472) 15.9% 24.4% 15.5%
Sister (n ¼ 21; 233) 11.3% 26.5% 10.5%
Brother (n ¼ 21; 682) 8.0% 21.7% 7.3%
Non-specific psychological distress
Sum score (range: 0–24; M, SD) 2.2 (5.3) 3.0 (5.1) 2.1 (5.2)
Serious mental health risk (%)
(score412)
2.7% 5.3% 2.6%
Source: 2000 National Health Interview Survey.
C. Rabin et al. / Social Science & Medicine 64 (2007) 411–416414
individuals diagnosed with cancer that previouslyexperienced the loss of a close family member tocancer may be pessimistic about the course of theirown cancer. Additional research is needed, however,to determine the mechanism for the interaction.This study did test whether gender moderated theinteraction of personal and family cancer historybut found no evidence supporting this hypothesis.Finally, it is unclear why significant interactions
were not found between personal cancer history andspecific types of family cancer history (e.g., motherwith cancer). Perhaps this is due to diminishedpower when each type of family history is analyzedseparately.
The strengths of this investigation are the use ofpopulation-based data, acceptable measures ofdistress, and heterogeneous population of cancersurvivors (whereas previous reports have focused on
ARTICLE IN PRESS
Table 2
Non-specific psychological distress by self-reported personal and family history of cancer: United States, 2000
Family cancer history Sum score (range: 0–24) With serious mental health risk (%) (score 412)
Personal cancer history Personal cancer history
Yes No Yes No
Any family member has cancer history
Yes 3.24 2.39 7.07% 3.03%
No 2.62 2.05 2.84% 2.34%
Mother cancer history
Yes 3.38 2.45 7.41% 3.14%
No 2.84 2.11 4.50% 2.45%
Father cancer history
Yes 3.30 2.36 7.86% 3.11%
No 2.91 2.09 4.51% 2.40%
Sister cancer history
Yes 2.70 2.63 4.15% 3.39%
No 3.05 2.11 5.43% 2.54%
Brother cancer history
Yes 3.12 2.41 6.97% 3.12%
No 3.07 2.11 5.43% 2.50%
Source: 2000 National Health Interview Survey.
Table 3
Effect of personal and family history of cancer on psychological distress and serious mental health risk: United States, 2000.
Covariatesa Psychological distress Serious mental health risk
Beta Se OR 95% CI
Intercept 0.40 0.10*** 0.005 0.003–0.007***
Personal hisory of cancer 0.53 0.198** 1.076 0.738–1.838
Family history of cancer 0.44 0.06*** 1.288 1.049–1.578*
Personal history�Family history 0.45 0.27 2.184 1.245–3.831**
Source: 2000 National Health Interview Survey.
*po.05. **po.01. ***po.001.aAll models control for the following sociodemographic characteristics: gender, race/ethnicity, education, age, marital status, income,
and health insurance coverage.
C. Rabin et al. / Social Science & Medicine 64 (2007) 411–416 415
one diagnostic group; Amir & Ramati, 2002;Hjerl et al., 2002). Key limitations (common toresearch using national databases) are that we wereunable to select study measures or control the studydesign. Thus, data were not collected on severalcancer-related variables (e.g., cancer stage) that wewould have liked to investigate or control for.Additionally, the cross-sectional design preventsconclusions about causal relationships. Finally,data are based on self-reports, as opposed tochart review, which may have introduced inaccura-
cies, especially in the reporting of family cancerhistory.
Even with these caveats, this study suggests thatindividuals with either a personal or family cancerhistory are at increased risk for distress. These findingshave important public health implications, as approxi-mately 10 million Americans have a personal cancerhistory (American Cancer Society, 2005) and an evengreater number have a family cancer history. Thisindicates the need for additional mental healthscreening and service referral for these populations.
ARTICLE IN PRESS
Table 4
Effect of personal and family history of cancer on psychological distress: United States, 2000
Covariatesa Model 1. Mother Model 2. Father Model 3. Sister Model 4. Brother
Beta Se Beta Se Beta Se Beta Se
Intercept 0.55 0.09*** 0.58 0.09*** 0.53 0.11*** 0.62 0.12***
Personal history of cancer 0.75 0.16*** 0.79 0.16*** 0.89 0.21*** 0.88 0.19***
Family history of cancerb 0.40 0.08*** 0.33 0.08*** 0.51 0.12*** 0.32 0.12**
Personal history�Family historyb 0.23 0.34 0.37 0.36 -0.71 0.38 0.09 0.43
Source: 2000 National Health Interview Survey.
**po.01. ***po.001.aAll models control for the following sociodemographic characteristics: gender, race/ethnicity, education, age, marital status, income,
and health insurance coverage.bEach of the four models examines separately the effect of each type of family member’s cancer history on the subject’s psychological
distress.
C. Rabin et al. / Social Science & Medicine 64 (2007) 411–416416
Acknowledgments
This research was supported by an R25 award toThe Miriam Hospital, Centers for Behavioral andPreventive Medicine (W. Rakowski, PI) NCI #R25CA87972-01. We would like to thank Zoe Bruno forher help with manuscript preparation.
References
Aass, N., Fossa, S. D., Dahl, A. A., & Moe, T. J. (1997).
Prevalence of anxiety and depression in cancer patients seen
at the Norwegian Radium Hospital. European Journal of
Cancer, 33(10), 1597–1604.
American Cancer Society. (2005). Cancer facts & figures. In
American Cancer Society. Atlanta, GA.
Amir, M., & Ramati, A. (2002). Post-traumatic symptoms,
emotional distress and quality of life in long-term survivors of
breast cancer: A preliminary research. Journal of Anxiety
Disorders, 16(2), 195–206.
Butow, P., Meiser, B., Price, M., Bennett, B., Tucker, K.,
Davenport, T., et al. (2005). Psychological morbidity in
women at increased risk of developing breast cancer:
A controlled study. Psychooncology, 14(3), 196–203.
Erblich, J., Bovbjerg, D. H., & Valdimarsdottir, H. B. (2000).
Looking forward and back: Distress among women at
familial risk for breast cancer. Annals Behavioral Medicine,
22(1), 53–59.
Gilbar, O. (1998). Coping with threat. Implications for women
with a family history of breast cancer. Psychosomatics, 39(4),
329–339.
Gilbar, O. (2003). Do attitude toward cancer, sense of coherence
and family high risk predict more psychological distress in
women referred for a breast cancer examination? Journal of
Women’s Health, 38(2), 35–46.
Hewitt, M., & Rowland, J. H. (2002). Mental health service use
among adult cancer survivors: Analyses of the National
Health Interview Survey. Journal of Clinical Oncology, 20(23),
4581–4590.
Hewitt, M., Rowland, J. H., & Yancik, R. (2003). Cancer
survivors in the United States: Age, health, and disability.
Journals of Gerontology Series A: Biological Sciences &
Medical Sciences, 58(1), 82–91.
Hjerl, K., Andersen, E. W., Keiding, N., Mortensen, P. B., &
Jorgensen, T. (2002). Increased incidence of affective dis-
orders, anxiety disorders, and non-natural mortality in
women after breast cancer diagnosis: A nation-wide cohort
study in Denmark. Acta Psychiatrica Scandinavica, 105(4),
258–264.
Kash, K. M., Holland, J. C., Halper, M. S., & Miller, D. G.
(1992). Psychological distress and surveillance behaviors of
women with a family history of breast cancer. Journal of the
National Cancer Institute, 84(1), 24–30.
Kessler, R. C., Barker, P. R., Colpe, L. J., Epstein, J. F.,
Gfroerer, J. C., Hiripi, E., et al. (2003). Screening for serious
mental illness in the general population. Archives of General
Psychiatry, 60(2), 184–189.
Kim, Y., Valdimarsdottir, H. B., & Bovbjerg, D. H. (2003).
Family histories of breast cancer, coping styles, and
psychological adjustment. Journal of Behavioral Medicine,
26(3), 225–243.
Lloyd, S., Watson, M., Waites, B., Meyer, L., Eeles, R., Ebbs, S.,
et al. (1996). Familial breast cancer: A controlled study of risk
perception, psychological morbidity and health beliefs in
women attending for genetic counselling. British Journal of
Cancer, 74(3), 482–487.
National Center for Health Statistics. (2002). Data file docu-
mentation [machine readable data file and documentation].
National Health Interview Survey, 2000. Hyattsville, MD.
Schwartz, M. D., Lerman, C., Miller, S. M., Daly, M., & Masny,
A. (1995). Coping disposition, perceived risk, and psycholo-
gical distress among women at increased risk for ovarian
cancer. Health Psychology, 14(3), 232–235.
Zakowski, S. G., Valdimarsdottir, H. B., Bovbjerg, D. H.,
Borgen, P., Holland, J., Kash, K., et al. (1997). Predictors of
intrusive thoughts and avoidance in women with family
histories of breast cancer. Annals of Behavioral Medicine,
19(4), 362–369.