economic and health needs of wisconsin migrant … and health needs of wisconsin migrant farm...
TRANSCRIPT

Rural Health Policy
Economic and Health Needs of Wisconsin Migrant Farm Workers
Doris P. Slesinger, PhD, and Cynthia Ofstead, MS
ABSTRACT Migrant farm workers play an essential role in the planting and harvesting of crops in our agricultural production system. In the United States today, about 6 percent of the paid farm labor force "follow the crops" across the nation. This article reports on the economic and health care needs of migrant farm workers who travel from the border areas of Texas to Wisconsin each year. Surveys conducted in 1978 and 1989 show that this population remains in serious need of health care and access to financial assistance programs.
During the 11-year interval between surveys, little change occurred in the health care status or use patterns of Wisconsin migrant workers, although housing and sanita y conditions in the work environment improved somewhat due to the passage of new federal regulations. This article discusses the problems and barriers that migrants continue to face and offers recommen- dations for government action.
U rban poverty in the United States has preoccupied scholars and reformers for many decades (Wilson & Aponte, 1985). In recent years, rural poverty has begun to draw the attention of
both academics and policy-makers (Duncan, 1992; Tickamyer & Duncan, 1990). Despite these recent efforts, the poverty status of one group-migrant workers-remains largely unexamined.
Migrant workers differ from other poverty groups. The safety nets available to most of the urban and rural poor are characteristically unavailable to migrant workers (Slesinger & Pfeffer, 1992). Migrants have always been a special population whose persis- tent poverty is reason for renewed concern as we begin a new era of economic restructuring and welfare reform.
Migrant farm workers play an essential role in the planting, weeding, and harvesting of American food crops. Early in the development of American agriculture, when private farmlands grew too large for individual families to work, day workers, field
hands, and migrant workers were hired to plant seed or gather crops. Since that time, seasonal and migrant workers have earned low annual incomes, endured substandard living conditions, and often lived in poverty.
About 2.5 million persons work as hired farm workers in the United States. Most are seasonal employees, distinct from migrant workers in several ways. While migrant and seasonal farm workers often perform the same tasks, seasonal farm workers live at home year-round while migrant farm workers move around the country in search of farm work. Most seasonal farm workers use their farm labor income to supplement income from other work throughout the year, while migrants depend on farm labor income for most of their yearly income. Sea- sonal employees work and are paid as individual's, while migrants usually travel in families and are often paid as family units. In 1985,159,000 (about 6%) of the paid farm labor force were migrant workers (Oliviera & Cox, 1988).
Another classification separates "casual" workers
The journal of Rural Health 138 Vol. 9, No. 2

(those employed in farm work for less than 25 days per year) from those whose primary source of income is farm labor (those employed in farm work 150 days or more per year). Migrants are more likely than other farm laborers to derive their primary income from farming. In 1981, for example, 37 percent of migrant workers worked 150 days or more compared to 27 percent of nonmigrants (Pollack & Jackson, 1983, p.19).
National statistics concerning migrant workers are sparse. The Economic Research Service of the U.S. Department of Agriculture (USDA) sponsored a ”Hired Farm Working Force” survey as a supplement to the Current Population Survey (CPS) conducted by the U.S. Bureau of the Census. The survey was conducted annually in December from 1945 through 1977 and biennially from 1977 to 1987. About 1,500 of the 60,000 households in the CPS sample included at least one hired farm worker (Daberkow & Whitener, 1986, p.11). The survey showed that the number of migrant workers, defined by the USDA as “...indi- viduals who travel across county or state boundaries and stay overnight to do farm work for cash wages or salary” (Pollack &Jackson 1983, p.17), has been declining since the 1940s.
~~
Methods
To examine specific characteristics of the migrant work force, Slesinger conducted two studies of migrant workers in Wisconsin. The first, conducted in 1978, was based on a 10 percent random statewide sample of migrant workers, using lists of names randomly selected from employers’ payroll files during July and August, the peak seasonal employ- ment months. Bilingual researchers interviewed migrant workers face-to-face at their residences throughout Wisconsin (Slesinger, 1979; Slesinger & Cautley, 1981). In 1989, Slesinger initiated a second study using the same sampling method and a slightly revised version of the 1978 interview instrument. Because severe budget restrictions precluded a statewide survey in 1989, the follow-up study was limited to three counties-Columbia, Dane, and Waushara-containing approximately one third of the migrants expected in the season (Slesinger & Ofstead, 1990).
The three counties included in the 1989 sample are an approximate representation of the state as a whole. To ensure a reliable comparison of data from the two survey years, the current analysis compares
the 1989 respondents (n=113) to the 1978 (n=145) cases located in the same three counties as those surveyed in 1989.
views were timed to coincide with the peak of migrant worker presence in the state, based on migrant population estimates provided by the Department of Labor, Industry, and Human Rela- tions (DLIHR) (Note 1). Almost all migrants who spend any portion of the year in Wisconsin have arrived in the state by early July and remain through the end of August. A small number of additional workers arrive in September to work in the shaping and harvesting of Christmas trees; these workers were not sampled either in 1978 or 1989. In each year, the difficult task of sampling a highly mobile popula- tion was facilitated by complete cooperation from employers in the three counties. In addition, few sampled workers refused to be interviewed (eight in 1978; four in 1989).
The 1978 results showed differences in the characteristics of migrants who labored in the fields compared to those who worked in canneries. There- fore, the 1989 sampling plan included both field workers (50%) and cannery workers (42%) as well as persons doing both field and cannery work. Most migrants in Waushara County work in the harvest of cucumbers, sweet peppers, and other vegetables. Some migrants in Columbia and Dane Counties also do field work, but the majority work in canneries packing corn, beans, peas, and other vegetables.
migrant health clinic would affect health care use patterns, the sample also provided variation in the workers’ residential proximity to the clinic, with about one half the sampled workers residing in Waushara (the county in which the clinic was lo- cated) and one half in Columbia and Dane Counties (more than 50 miles away). Later analysis showed,
In both survey years, the sampling and inter-
Based upon the hypothesis that distance from a
This study was supported by the Wisconsin Rural Health Research Center at Marshfield Medical Foundation with funds from the Health Resources and Services Administration; matching funds from the Graduate School at the University of Wisconsin-Madison; and Agency for Health Care Policy and Research grant no. HS06524. We are indebted to David Benson, Andrew Chesnut, Mary Clark, and Erika Smith, bilingual interviewers; Iulia Salomon, translator; and Eleanor Cautley, research specialist, who assisted in sampling design, interviewer training, and coding and analysis problems. The collection of the data presented in this report relied upon the interest and cooperation of both the employers of migrant workers and the respondents. This article is a revised version of one preseuted in 2990 at the Rural Sociological Society meeting in Norfolk, VA. For further information, contact: Doris P. Slesinger, PhD, Department of Rural Sociology, University of Wisconsin-Madison, 313 Agriculture Hall, 2450 Linderi Drive, Madison, WI 53706.
Slesinger and Ofstead 139 Spring 1993

however, that distance from the clinic was not related to utilization in a systematic way.
tics of the migrant work force in these counties in 1978 and 1989, making special note of income, poverty status, housing conditions, health status, and barriers to obtaining health care. It also discusses the failure of many public assistance "safety nets" to support the needs of migrant workers, and recom- mends renewed policy reform efforts to help elimi- nate rural poverty.
This article compares and contrasts characteris-
- Findings
Sample Demographic Characteristics. In 1978, men comprised 60 percent of the 1,350 migrant workers residing in Columbia, Dane, and Waushara counties. By 1989, the proportion of men had in- creased to about 72 percent of the 1,665 workers. At both times, ages ranged from 16 to older than 60 years, and all workers 60 years and older were men. Since 1978, the average age has declined by about one year for men and nearly two years for women.
Educational achievement among migrants has improved since 1978, although respondents still fall far below national averages. The number of function- ally illiterate men (those who completed fewer than five years of school) declined from 27 percent in 1978 to 16 percent in 1989 (Z=1.84, P=0.06). The number of functionally illiterate women remained at about 19 percent. The proportion of men completing high school remained low, with only 8 percent of men age 25 years or older in both years completing high school. The number of women completing high school rose from 4 percent in 1978 to 14 percent in 1989 [Z=1.64, P=O.lOl. Nationally, about 76 percent of all persons 25 and older, and 51 percent of Hispanics 25 years and older, have completed high school (Bureau of the Census, 1988).
In both 1978 and 1989, more than 94 percent of Wisconsin's migrant workers were of Mexican ancestry. In 1989,71 percent of respondents had been born in Mexico, 26 percent in Texas, and 3 percent in other parts of the United States. Sixty-two percent of workers sampled in 1989 were married, 35 percent had never been married, and 4 percent were di- vorced. Of those who were never married, 95 percent were younger than 30 years. Married worker house- holds in 1989 included some couples without ex- tended family, but most also included children,
Figure 1. Percent of Wisconsin Migrant Farm Workers Employed and Employed Specifically in Agriculture, by month- August 1988 to July 1989.
aa
60
..4
G
PF
40
20
Aug Scp Oct Nav Dec Jan k b Mar Apr May Sun Jul 1988 1989
grandchildren, parents, or other relatives. Eleven percent of households contained members of three generations.
Employment. The 1989 respondents had worked as migrants from one to 31 years, averaging six years. One of three migrants was working in Wisconsin ffor the first time in 1989. Of those who had worked in Wisconsin before, more than 80 percent worked for the same grower or canner who had previously employed them or their family members.
Wisconsin in June or July and stayed through Sep- tember or October. All workers lived away from their home states in July and August, and about 90 percent were back home from December through March. Figure 1 displays the total proportion of migrants who were employed in agriculture for each month of the previous year. The proportion employed begins to increase slowly in April and May during the planting and nursery season, reaching 80 percent in June. All respondents were employed in July and August, but during the lowest period of employment, from December through March, almost 60 percent were unemployed. In winter and nonpeak months of
More than 75 percent of the migrants arrived in
VOl. 9. No. 2 The Journal of Rural Health 140
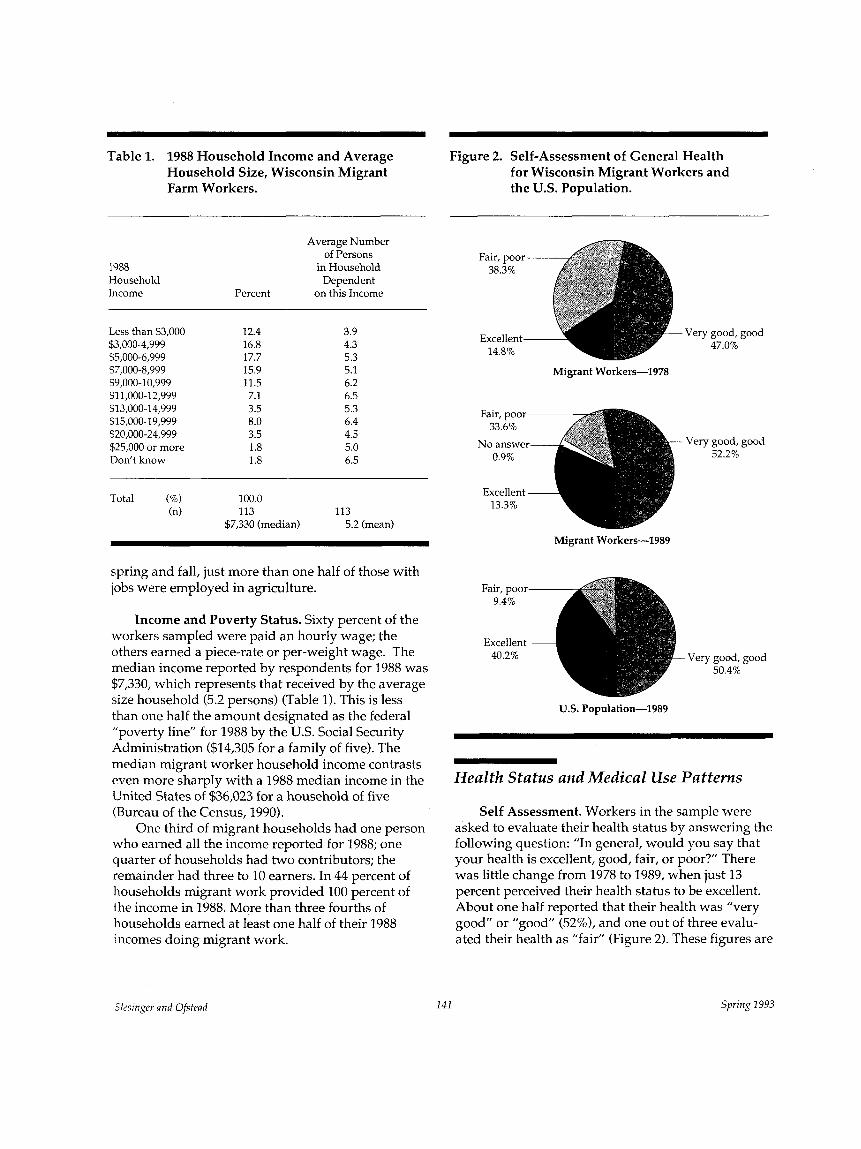
Table 1. 1988 Household Income and Average Household Size, Wisconsin Migrant Farm Workers. the U.S. Population.
Figure 2. Self-Assessment of General Health for Wisconsin Migrant Workers and
1988 llousehold Income Percent
Average Number of Persons
in Household Dependent
on this Income
Less than $3,000 12.4 $3,000-4,999 16.8 $5.000-6.999 17.7
3.9 4.3 5.3
$i000-8;999 15.9 5.1 $9,000-10,999 11.5 6.2 $1 1,000-12,999 7.1 6.5
Fair, poor- 38.3%
Excellent- 14.8%
Very good, good 47.0%
Migrant Workers-1978
$13,000-14,999 3.5 5.3 $15,000-19,999 8.0 6.4 $20,000-24,999 3.5 4.5 $25,000 or more 1.8 5.0 Don’t know 1.8 6.5
Very good, good 52.2%
Total (%) 100.0 (n) 113 113
$7,330 (median) 5.2 (mean) Migrant Workers-1989
spring and fall, just more than one half of those with jobs were employed in agriculture.
Income and Poverty Status. Sixty percent of the workers sampled were paid an hourly wage; the others earned a piece-rate or per-weight wage. The median income reported by respondents for 1988 was $7,330, which represents that received by the average size household (5.2 persons) (Table 1). This is less than one half the amount designated as the federal ”poverty line” for 1988 by the U.S. Social Security Administration ($14,305 for a family of five). The median migrant worker household income contrasts even more sharply with a 1988 median income in the United States of $36,023 for a household of five (Bureau of the Census, 1990).
who earned all the income reported for 1988; one quarter of households had two contributors; the remainder had three to 10 earners. In 44 percent of households migrant work provided 100 percent of the income in 1988. More than three fourths of households earned at least one half of their 1988 incomes doing migrant work.
One third of migrant households had one person
Fair, poor 9.4%
Excellent 40.2% Very good, good
50.4%
U.S. Population-1989
Health Status and Medical Use Patterns
Self Assessment. Workers in the sample were asked to evaluate their health status by answering the following question: ”In general, would you say that your health is excellent, good, fair, or poor?” There was little change from 1978 to 1989, when just 13 percent perceived their health status to be excellent. About one half reported that their health was ”very good” or ”good” (52%), and one out of three evalu- ated their health as “fair” (Figure 2). These figures are
%singer and Ofstead 141 Spring 1993

strikingly different from those reported for the US. population as a whole: 40 percent of all Americans describe their health as ”excellent,” 50 percent as “very good or good,” and less than 10 percent as “fair or poor” (Department of Health and Human Services [DHHSI, 1990).
Medical Conditions. The 1989 respondents were read a list of 25 common medical conditions and were asked whether each condition bothered them “very much, some, or not at all.” Women reported greater occurrence of backache, headache, and nervousness than did men who reported more dental problems, stomachaches, and sleeping troubles. Some problems may be linked to the extensive travel, frequent relocation, and long hours of back-bending required of many migrants. Backache was the most frequently reported condition for both sexes, affecting nearly 33 percent of the sampled workers.
The 1978 study had suggested that language proficiency was a key to perceived health problems and use of health care facilities, and this was corrobo- rated in 1989. Workers who spoke only Spanish gave their general health a lower assessment than did others and they reported a higher incidence of many morbid conditions. The indications of poorer health among those who speak only Spanish may be associ- ated with age; Spanish speakers tended to be older on average than those who speak at least some English. The fact that many of the conditions that Spanish speakers report suffering are related to stress also suggests that migrants without English language skills may find the experience of working in a non- Spanish setting especially taxing, both physically and emotionally.
Fifteen percent of sampled workers reported chronic conditions or illnesses. The most frequently mentioned problems were gastric ulcer, hearing problems, gallbladder trouble, diabetes, cough, and sore throat. Women were more likely than men, and Spanish speakers more likely than English speakers, to report chronic problems.
Medical Utilization Patterns. In both 1978 and 1989, about 60 percent of workers said they had been to a doctor or clinic in the past year. Twenty-eight percent had general physical exams or checkups, pap smears, or pelvic exams. Common ailments, such as stomachaches, flu, joint or muscle problems, and skin rash or inflammation, were responsible for most other visits. A few respondents mentioned gallblad- der trouble and diabetes. One of 10 migrants spent at
least one day in the hospital in the past year. Twenky- nine percent of workers surveyed in 1978, and 27 percent in 1989, had never had a physical exam when they were not sick.
Dental Care. Migrant workers are far less likely than the average American to receive dental care. While more than 98 percent of the U.S. population older than age 15 have seen a dentist at least once (National Center for Health Statistics, 1989, p. 1101, only 75 percent of the survey respondents in each year had done so. Three or more years had elapsed since the most recent dental visits of one fifth of migrants surveyed in 1978 and one fourth of those surveyed in 1989. In both years men were less likely than women to have received dental care.
About one half of the respondents said they needed dental care at the time of the interview, although only about 7 percent of those needing care were actually seeing a dentist. Lack of money and having ”too much work” were the most common reasons given for not seeking care. Fifteen percent of respondents felt uncomfortable or fearful about dental care. Some were waiting to return to Texas or Mexico to get attention.
Vision Care. Twenty percent of the interviewed workers wore glasses at least some of the time. A significantly higher proportion of women (34%) than men (14%) wear glasses (chi square=5.50, d.f.=l, P<0.05). More than 43 percent had never had their eyes checked. As with dental care, men and those who only spoke Spanish in both studies were less likely to have had an eye examination. Lack of money and time, and fear or discomfort were reasons most often given for not seeking eye care.
Overall, there was almost no change during the 11-year period in the proportion of migrant workers who had never had routine physical, dental, and vision checkups (Figure 3). The only change-in vision care utilization-was in a negative direction. Clearly, a significant portion of the migrant popula- tion does not receive routine preventive health care.
Problems in Obtaining Medical Care. Migrant workers face a number of problems getting medical care. Their mobility can make it difficult to find care and maintain continuity of treatment. Migrants in Wisconsin generally live in rural areas and may have to travel considerable distances to reach medical care. Furthermore, because migrants earn most of their yearly incomes during a few months, any intenup-
V O l . 9, No. 2 The lournal of Rural Health 142

Figure 3. Proportion of Wisconsin Migrant Farm Workers Who Never Had Routine Physical, Dental, or Eye Checkups -1978,1989.
Table 2. Reasons for Not Seeing a Doctor During the Past Year Reported by Wisconsin Migrant Farm Workers, by Sex, 1989.
1 0 0 1 Percent Answering "Yes"
Reason Total Men Women
43.3
Routine Dental Eye physical checkup examination
1978
1989
I'm never sick I don't like to bother the doctor
unless it's necessary I can't afford it The doctor is too far away I'm unable to get there at the
time service is offered I would lose pay/income from
work It takes too long to get an
appointment I can't speak English I'm afraid of what the doctor
might find I don't know what doctor to go to I feel uncomfortable with doctors I have no transportation I believe in sources of healing
other than doctors
44.2 45.7 40.6
25.7 17.3 46.9 19.5 16.0 28.1 17.7 9.9 37.5
15.9 11.1 28.1
15.0 13.6 18.8
13.3 8.6 25.0 12.4 7.4 25.0
12.4 6.2 28.1 8.8 6.2 15.6 8.8 4.9 18.8 7.1 3.7 15.6
3.5 0.0 12.5
tion in their work is unwelcome.
accustomed to seeking medical care from Spanish- speaking practitioners on both sides of the U.S.- Mexico border. Migrants who speak only Spanish or limited English have difficulty communicating symptoms and conditions to an English-speaking practitioner. Language barriers also may limit the degree to which patients can understand and follow treatment regimens.
To assess obstacles to health care, respondents in both studies were asked to identify the major reasons that had kept them from seeing a health professional in the past year. Table 2 lists the most frequently cited reasons.
Women in general reported more problems in seeking medical care. Difficulties related to lack of resources and transportation were particularly prevalent among women, as was reluctance to bother the doctor.
The survey also assessed the extent to which language constitutes a barrier to health care for
Many workers from south Texas and Mexico are
migrant workers. In 1989, only 8 percent of the sample (14% of non-English speakers) said language created problems for them when seeking health care in Wisconsin. On the other hand, more than one half the sample (81% of non-English speakers) needed someone to interpret when they went to a medical provider. About one third of the respondents had seen Wisconsin providers who spoke Spanish, and one half (67% of those who spoke only Spanish) received written instructions in Spanish from their Wisconsin providers. One fourth of those who speak some English and 70 percent of those who speak only Spanish needed help reading instructions written in English. Only a few workers (2%) felt that discrimina- tion against migrant workers prevented them from getting health care in Wisconsin.
Payment of Medical Costs. Of the 66 percent of workers who used Wisconsin health care providers in 1989, more than 50 percent said migrant health funds paid for their care (Table 3). An additional 17 percent used medical assistance (Title 19 or Medicaid), and 14 percent paid out of pocket. This pattern is similar to
Slesingev and Ofstead 143 Spring 1993

Table 3. Form of Payment of Medical Bills in Wisconsin, 1978 and 1989.
Form of Payment
Migrant health funds Medical assistance Out of pocket Medicare Insurance
Through employer Paid independently
Other Don’t know
1989 Percent
1978 Percent P’
54.0 17.5 14.3 3.2 3.2 1.6 1.6 3.2 4.8
51.4 ns 13.9 ns 23.7 ns 4.0 ns
17.0 0.006 13.0 4.0
16.2 0.0
Total (%) 100.0 100.0 (n) 63 127
1. Two-sample, difference of proportions test.
the 1978 findings with one significant change-a decrease in the proportion of workers whose bills were paid by private health insurance from 17 percent in 1978 to 3 percent in 1989 (Z=2.76; P<O.Ol).
Housing And Environmental Health
While employed in agricultural labor in Wiscon- sin, most migrant workers live in camps or dormito- ries provided by their employers. The structural and sanitary conditions of migrant housing vary greatly. Wisconsin employers most frequently provide two to four unit bungalows, stationary trailers or mobile homes, reconverted farmhouses or barns, and dormi- tories. A few workers each year rented their own apartments or houses, lived with relatives or friends in Wisconsin, or rented hotel rooms.
About one half of the workers surveyed were “very satisfied” with the housing provided by employers. One half were ”somewhat satisfied,” and 2 percent were not satisfied. Table 4 shows the percent of workers in both survey years reporting the absence of various housing facilities.
One in three workers surveyed in 1989 said their units did not have indoor plumbing, an improvement over 1978 when well more than one half lacked these facilities. One in five 1989 respondents had no hot
Table 4. Migrant Farm Worker Housing Lacking Various Facilities, Wisconsin, 1978 and 1989.
Facility 1989 1978 P1
Hot running water Cold running water Bath, shower Flush toilet Working refrigerator Gas or electric burner Gas or electric oven Electricity in house Windows in every room Screens on all windows
and doors
67.6 59.4 67.6 74.3 8.4 8.4
12.7 3.8
24.3
3.1
20.4 15.9 31.0 32.7 16.8 16.8 17.7 1.8 0.9
0.0
<0.001 <0.001 <0.001 <0.001 <0.05 <o.os IIS ns
<0.001
IIS
(n) 145 113
1. Two-sample, difference of proportions test.
running water, compared to two thirds in 1978. Almost all 1989 units had electricity, though about 17 percent lacked cooking and refrigeration facilities. All units had screened windows in every room by 1989. These figures indicate important improvements in migrant housing conditions in the 11 years since 1978, although it appears that about one third of the units still lack bathrooms. For the latter, a separate bath house and laundry room was provided.
Sanitary Facilities in the Work Place. About 80 percent of 1989 respondents said their work places provided a place to wash hands; 96 percent of their worksites had toilets, and 86 percent provided drink- ing water while at work. As Table 5 shows, cannery workers have greater access to sanitary facilities than do field workers. A major improvement in field sanitary conditions has occurred since 1978, mainly due to a 1986 Occupational Safety and Health Admin- .istration (OSHA) code requiring that employers of 10 or more migrants provide toilet facilities, drinking water, and hand-washing water in the fields.
Exposure to Chemicals. Survey questions as- sessed whether migrants suffered from exposure to dangerous chemicals at work. The risks of pesticides and herbicides did not figure prominently in the
The Journal of Rural Health 144 Vol. 9, No. 2

Table 5. Presence of Sanitary Facilities by Field or Cannery Work Place, Wisconsin Migrant Farm Workers, 1978 and 1989.
1978 1989
Facilities Field Cannery Total' Field Cannery Total2
Percent Percent Percent Percent Percent Percent P3
Drinking water Toilet Place to wash hands
54.8 95.0 66.9 74.1 100.0 85.8 0.0005 44.1 100.0 63.6 93.1 100.0 95.6 <0.0001 34.4 100.0 55.2 62.1 100.0 79.6 <0.0001
Total (n) 93 27 145 58 47 113
1.
2.
3.
Total includes 23 workers who worked in both field and cannery work; 87 percent had access to drinking water, 100 percent to toilets, and 87 percent to places to wash hands. Total includes eight workers who worked in both field and cannery work; all workers reported access to drinking water, toilets, and places to wash hands. Two-sample, difference of proportions test. Significance is between percents in total groups.
responses of workers interviewed. Only 8 percent said they may have suffered health problems due to pesticides. Similarly, a very small proportion (4%) reported pesticide-related problems in 1978. In considering these figures, it is important to note that the effects of poisons and chemicals on the body may not produce immediate symptoms, and the link between pesticide exposure and subsequent health problems is often unrecognized.
Discussion
Since the turn of the century, migrant workers have been coming to Wisconsin on a seasonal basis to work in the canning, harvesting, and processing of agricultural products. While the demand for their labor has fluctuated during past years due to changes in technology and the agricultural economy, migrant workers continue to provide an important, short-term labor supply to Wisconsin growers and food proces- sors during the crucial summer months. Because much of their total yearly income is earned during the agricultural season, migrants are often willing to work long hours, double shifts, and seven days a week when crops reach their peak.
For many migrants, the income earned during three or four months in Wisconsin provides a mea-
sure of economic security during long months of unemployment or partial employment in their home states. Still, the annual incomes of migrants surveyed in our study indicate that many live in poverty. Low levels of income, coupled with the living conditions imposed by migrant life (e.g., seasonal cross-country travel, temporary housekeeping in migrant camps, intermittent periods of long and heavy labor, and periodic separation from home communities), mean that many members of this work force require access to different forms of public support. Individuals and families need support services to gain access to legal, economic, and emotional resources in the communi- ties where they work. Migrant children often miss portions of the school term in their home communi- ties and need supplemental education programs. Migrants often need public financial assistance, in the form of health insurance, food stamps, or monetary transfers. Finally, workers and their families need information about access to health care.
Many low-income people have felt the sting of government cutbacks in public assistance during the past decade. Migrant workers face additional barriers to successfully gaining help. Long patterns of exclu- sion from programs such as unemployment insur- ance and from the legal right to bargain collectively and demand improvements are part of the problem. Structural characteristics of migrant work, including
&singer and Ofstead 2 45 Spring 1993

the irregularity of employment, the location of employment in remote rural areas, and the complex- ity of migrants’ fluctuating state of residence further complicate the problem. The barriers built into public aid bureaucracies confront migrant workers as they do all applicants, presenting special problems for those who do not speak English or whose national citizenship.is unclear.
for migrant workers involve unemployment insur- ance. Two key difficulties arise with current unem- ployment insurance programs. First, unemployment insurance was constituted in 1938 as a joint federal- state program. Because migrants often earn money from multiple employers in numerous states and pass their months of unemployment in home states such as Texas or Florida, the application and payment procedure can be complex and inhibiting. Second, in many states, including Wisconsin, many farms that employ migrant labor have too few employees to be required to pay for unemployment insurance cover- age (Note 2). As analysts point out, agriculture is traditionally portrayed as a unique, family-oriented industry made up of small operations that could be ”destroyed if burdened by the social legislation aimed at industrial employers” (Johnson, 1985, p. 51). Although some states have more stringent guidelines (Note 3), the federal government still exempts employers with fewer than 10 workers from manda- tory unemployment insurance payments.
About 60 percent of migrants in the 1989 survey said they were unemployed for at least one month in the year prior to their interview, although just less than 40 percent received unemployment compensa- tion payments.
Another concern relates to health insurance coverage. Although some large food processing firms provide employees with health insurance coverage, most farms do not. Migrant workers usually rely on government clinics or insurance programs for the medically indigent. Like unemployment insurance, Medicaid is a joint federal and state program under administrative control by the states, and states differ in residency requirements and levels of benefit. Migrant workers may have difficulty obtaining benefits when their stay in an area is short or when employment exigencies force them to relocate before their Medicaid cards become valid.
As in many other states, Wisconsin’s medical assistance program requires a statement of earned income from applicants. Migrants may meet the ”means test” for benefits when they enter the state
Some of the worst problems in public assistance
after a period of travel or unemployment but may earn enough income to be ineligible by the time they meet the 60-day residency requirement. Chronically ill persons, or children needing routine health care, may go long periods without adequate access to treatment. Thirty-five percent of migrants interviewed received public medical aid funds at some point during the past year, but only about one sixth of those who obtained health care in Wisconsin used medical assistance to pay those bills.
With regard to all types of public assistance, complex patterns of state residence constitute one problem for migrant workers. National citizenship and national origin can further complicate the situation. A California study (Mines & Kearney, 1982) showed that migrant workers who are U.S. citizens are more likely to use public assistance programs than are settled Mexican immigrants (including those who have permanent residence and a legal right to work and live in the United States). ”Citizen families owe their higher incomes to welfare and social insurance programs,” claimed the researchers, and they credited “familiarity with government agencies” and greater facility with the English language for this difference in utilization (Mines & Kearney, 1982, p. 37). Migrants without legally documented rights to employment are more economically vulnerable than either of these groups and have recourse to few institutional re- sources in dealing with health or other crises.
The current structure of public assistance insur- ance programs seems particularly ill suited to the needs of migrant workers. Major structural reforms are needed to alleviate the economic vulnerability of migrant workers. While an infusion of funding would improve the situation temporarily, program structures must be examined in light of migrants’ special needs. One avenue that deserves further exploration is standardization of the administration and regulation of programs like unemployment insurance and Medicaid. Unless the specific conditions and needs of the migrant labor force are explicitly recognized, difficulties will persist.
be problematic for migrant workers, other types d legislation and social programs do exist to address migrants’ particular needs. Since the mid-l960s, federal programs have provided educational benefits for migrant children, and federal funds have sup- ported health programs that target the migrant population. Since the late 1970s, Wisconsin laws have provided additional economic and legal protection for migrant workers. The 1977 Wisconsin Migrant Labor
While current public assistance programs tend to
The Journal of Rural Health 146 Vol. 9, No. 2

Law requires written contracts for migrant workers, stipulates that migrant agricultural laborers be paid at least minimum wage, and mandates the inspection and certification of employer-provided migrant housing. A sanitary code passed first in Wisconsin, and later by the federal government, requires employ- ers to provide drinking water, toilets, and hand- washing facilities at both field and cannery work sites. As has been seen, environmental health conditions improved significantly in the years between this study’s two surveys.
use of health services must include attention to the year-round conditions of their lives. The fact that 27 percent of the workers interviewed had never had a physical examination when not ill, that 26 percent had never been to a dentist, and that 43 percent had never had an eye examination demonstrates that the migrant population is underserved both at home and while migrating. Many workers who felt they needed health care, but were not getting it, said lack of money impeded them. Many reported the inconvenience of obtaining health care, especially while working. While it is beyond the scope of this study to assess the quality and availability of health care in the communi- ties where migrants reside in winter, the information collected indicates that the three- or four-month period that migrants spend in Wisconsin provides an opportunity for needed health services.
The primary source of health care for migrants in Wisconsin is Family Health/La Clinica, located in the middle of the state. This clinic offers free or low cost medical and dental services on site, provides vouchers to pay for referrals to hospitals or specialists, and issues vouchers to migrants working too far from the clinic to obtain care there. The clinic is staffed with Spanish-speaking professionals and maintains some evening and weekend hours during the peak agricul- tural season. In addition, La Clinica provides health information through outreach workers and expanded health services using a mobile van. Most of the fund- ing for La Clinica comes from federal migrant health funds, with additional funding from Title V maternal and child health funds, and the Women, Infants and Children Nutritional Supplement Program (WIC). During the 1980s, the federal allocation of migrant health funds was subject to budget cuts (as were state and federal funds for some migrant social service and education organizations). Satellite clinics are no longer in operation, some forms of noncritical care (such as some dental procedures) are no longer offered, and outreach and mobile unit staffs have been scaled
Efforts to improve migrant workers’ access to and
down. According to La Clinica’s staff, a shortage of funds has made it increasingly difficult to meet the health care needs of migrant workers in Wisconsin.
Conclusions
Many factors contribute to a population’s health. For migrant workers, persistent poverty may be the underlying problem most urgently requiring public attention. Enforcement of minimum wage standards should be guaranteed to agricultural workers in every state. Along with wage improvements, programs to support year-round employment for migrants are needed to ensure an annual income above poverty level.
National universal health insurance would make consistently available health care a strong alternative to the patchwork of services now available to mi- grants. Some states have good migrant health services, others have next to none. When health service provi- sion is the responsibility of individual states or coun- ties, migrants doing the same type of work may have no access to health services in some places, to minimal services in others, and to adequate services elsewhere. A universal national health plan could cover these workers, regardless of where they are located when they need a doctor, and regardless of their income or employment status at any given point in the agricul- tural year.
In the meantime, it is crucial that society strengthen its commitment to public programs and service agencies established to assist migrants in overcoming problems related to economic disadvan- tage, such as educational and health deficits. Efforts to improve the conditions of migrant workers include public policies re-establishing sufficient levels of funding to these agencies and stronger legislative measures to ensure that migrants have access to resources that can help them improve their lives.
Notes
1. In 1978 approximately 4,080 migrants worked in Wisconsin. That year, 1,350 worked in the three counties analyzed here. In 1989, a total of approximately 3,913 migrants worked in Wisconsin, of which 1,665 worked in the three counties included in this study. Agricultural employers are included if they paid more than $20,000 in cash wages during any quarter of the current or preceding calendar year, or if they employed 10 or more workers in agricultural labor for some part of a day in a
2.
Slesinger and Ofstead 147 Spring 1993

minimum of 20 different weeks in the current or preceding calendar year. To be eligible, employees must have worked at least 17 weeks in unemployment insurance covered employ- ment during the 52 weeks immediately preceding the initial claim for benefits. Martin’s study (1988) of unemployment insurance coverage shows that increasing numbers of farm workers are protected by unemployment insurance due to the increasing consolida- tion and concentration of farming operations, not due to legislative reform.
3.
References
Bureau of the Census. (1988). The Hispanic population in the United States (Current Population Reports, Series P-20, No. 431). Washington, DC: US. Government Printing Office.
Bureau of the Census. (1990). Trends in income, by selected character- istics: 1947-2988, (Current Population Reports, Series P-60, No. 167). Washington, DC U.S. Government Printing Office.
sources: A n update (Agriculture Handbook No. 658). Washing- ton, DC: US. Department of Agriculture, Economic Research Service.
Department of Health and Human Services. (1990). Health, United States, 2989. Washington, DC: U.S. Government Printing Office.
Auburn House.
Hills, MI: National Migrant Workers Council, Inc.
Daberkow, S.G., & Whitener, L.A. (1986). Agricultural labor data
Duncan, C. (Ed.). (1992). Rural poverty in America. Westport, C T
Johnson, H. (1985). Health for the nation’s harvesters. Farmington
Martin, P.L. (1988). Harvest of confusion: Migrant workers in U.S
Mines, R., & Kearney, M. (1982). The health of Tulare County agriculture. Boulder, C O Westview Press.
farmworkers. Sacramento, CA: California Department of Health Services.
National Center for Health Statistics. (1989). Health, United Staffs, 1988 (DHHS Publication No. PHS 89-1232). Washington, IDC: U.S. Government Printing Office.
(Agricultural Economic Report No. 582). Washington, DC: U.S. Department of Agriculture, Economic Research Senwe.
Pollack, S.L., & Jackson, W.R. (1983). The hired farm working fwa of 1982 (Agricultural Economic Report No. 507). Washington, DC: U.S. Department of Agriculture, Economic Research Service.
Slesinger, D.P. (1979). Health needs of migrant workers in Wisconsm. Madison, W I Department of Rural Sociology, University of Wisconsin.
Hispanic migrant farmworkers in Wisconsin. Public Health Reports, 96(3), 255-263.
Slesinger, D.P., & Ofstead, C. (1990). Migrant agricultural works in Wisconsin, 2989: Social, economic, and health characteristics Madison, W I Department of Rural Sociology, University of Wisconsin.
Slesinger, D.P., & Pfeffer, M. (1992). Migrant farm workers. In C. Duncan (Ed.), Rural poverty in America (pp. 135-153). W e s p r t , C T Auburn House.
Tickamyer, A.R., & Duncan, C. (1990). Poverty and opportunity structure in America. Annual Review of Sociology, 16,6746.
Wilson, W.J., & Aponte, R. (1985). Urban poverty. Annual R e a m of Sociology, 11,231-258.
Oliviera, V.J., & Cox, E.J. (1988). The agricultural workforce of2985
Slesinger, D.P., & Cautley, E. (1981). Medical utilization patterms of
The Journal of Rural Health 148 Vol. 9,. No. 2