early changes in serum creatinine level and estimated glomerular filtration rate predict pancreatic...
TRANSCRIPT
at SciVerse ScienceDirect
Pancreatology 13 (2013) 207e211
Contents lists available
Pancreatology
journal homepage: www.elsevier .com/locate/pan
Original article
Early changes in serum creatinine level and estimated glomerular filtration ratepredict pancreatic necrosis and mortality in acute pancreatitisCreatinine and eGFR in acute pancreatitis
Michal Lipinski a,*, A. Rydzewski b,c, G. Rydzewska a,c
aDepartment of Gastroenterology, Central Clinical Hospital of The Ministry of Interior, Woloska 137, 02-507 Warsaw, PolandbDepartment of Internal Medicine and Nephrology, Central Clinical Hospital of The Ministry of Interior, 02-507 Warsaw, Polandc The Jan Kochanowski University Humanities and Sciences, Kielce, Poland
a r t i c l e i n f o
Article history:Received 14 December 2012Accepted 12 February 2013
Keywords:PancreatitisCreatinineGlomerular filtration rateeGFRPredictionPancreatic necrosisMortality
* Corresponding author. Tel.: þ48 22 508 12 40; faE-mail address: [email protected] (M. L
1424-3903/$ e see front matter Copyright � 2013, IAhttp://dx.doi.org/10.1016/j.pan.2013.02.002
a b s t r a c t
Aim: The aim of the study was to evaluate the significance of serum creatinine level (SCL) and estimatedglomerular filtration rate (eGFR) measured in an early phase of acute pancreatitis (AP) for prediction ofpancreatic necrosis (PNec) and mortality.Methods: One hundred and forty-seven patients with AP were retrospectively reviewed in the study.Serum creatinine level and estimated glomerular filtration rate (calculated using the abbreviatedModification of Diet in Renal Disease equation) on admission and 48 h thereafter were analyzed for eachpatient. These parameters were compared with contrast-enhanced computed tomography images per-formed within 96 h from admission (n ¼ 103). Usefulness of SCL and eGFR for prediction of PNec andfatal outcome of AP was evaluated using a receiver operator characteristic curve analysis and comparisonof average parameter values.Results: We confirmed pancreatic necrosis in 41 (39.8%) of 103 patients using computed tomographyexamination. Both creatinine and estimated glomerular filtration rate measured on admission (p < 0.001,p < 0.001 respectively) and 48 h later (p ¼ 0.001, p < 0.001 respectively) were significantly associatedwith the presence of pancreatic necrosis.Moreover, serum creatinine level and eGFR measured on the 1st day proved to be a good predictor offatal outcome. Both, mortality and presence of pancreatic necrosis were significantly higher in the groupwith elevated serum creatinine level and low eGFR values.Conclusions: SCL and eGFR on admission are useful indicators of PNec and mortality.Copyright � 2013, IAP and EPC. Published by Elsevier India, a division of Reed Elsevier India Pvt. Ltd. Allrights reserved.
1. Introduction
Acute pancreatitis is a common, and potentially lethal acuteinflammatory process with diverse clinical course. The incidence ofAP is about 30e40 cases per 100 000 individuals. Severe clinicalcourse (20%), accompanied by development of a systemic inflam-matory response syndrome (SIRS) andmultiple organ failure (MOF)constitute main reasons of complications and on occasion death(10e20%) [1,2]. It is uncertain why some cases of AP result in organfailure and others do not, or at which point in the inflammatoryprocess would an intervention influence disease progression.
Early prediction of acute pancreatitis severity using a simple,single laboratory test would be very helpful for guiding disease
x: þ48 22 508 10 40.ipinski).
P and EPC. Published by Elsevier I
management from the very beginning and potentially improvingthe outcome. Many biochemical parameters (including C-reactiveprotein (CRP), procalcitonin, trypsinogen-activation peptide (TAP))were evaluated with regard to their value for assessment ofAP severity [3e5]. C-reactive protein, one of the most valuableparameters, is not specific for pancreatitis, and its elevation isobserved 48 h after the onset of the disease. Therefore, it is desir-able to find a rapid and inexpensive marker, which would effec-tively predict the outcome at an early stage of the disease.
Hypoperfusion plays amajor role in the pathogenesis not only ofpancreatic necrosis (PNec) but also of MOF, which are the maincauses of death in severe acute pancreatitis. Knowledge of bodywater balance disruption (which is the primary cause of hypo-perfusion) in AP and resulting deviations in laboratory tests ispotentially useful for clinical purposes, both diagnostic and thera-peutic [6].
ndia, a division of Reed Elsevier India Pvt. Ltd. All rights reserved.

Table 1Relation between eGFR estimated on the 1st day of hospitalization and presence ofpancreatic necrosis.
p value <0.001 Pancreatic necrosis [n]
eGFR 1st day (ml/min) >90% 17% [41](0e90)% 64% [62]
M. Lipinski et al. / Pancreatology 13 (2013) 207e211208
Current guidelines recommend intensive fluid resuscitation inthe early phase of AP. This guidance is based on reports stating thatpancreatic microcirculatory disturbance acts as an initiating factorfor local tissue injury as well as for the development of systemiccomplications in experimental models of AP [7,8].
Fluid resuscitation based on dynamic predictors of fluidresponsiveness is safer and more effective [9].
Moreover, early recognition of patients requiring intense fluidresuscitation can help identify patients who need scrupulous careor management in an intensive care unit.
Acute renal failure (ARF) is reported in 14e16% cases of AP[10,11] and carries a bad prognosis, particularly for older patientsand for those with MOF and local pancreatic complications. Re-ported mortality rate in AP accompanied by ARF is as high as 81%[12,13].
High serum creatinine is already known as an unfavorableprognostic factor in AP [14]. However, eGFR e a parameter moreaccurately reflecting renal functione has never been evaluated as apredictor of PNec and fatal AP. Estimated GFR may be an evenmoresensitive indicator of hypoperfusion, as it takes age and sex intoaccount and therefore, could be more accurate for prognosis of APseverity.
It is worth emphasizing that another parameter, which mayreflect intravascular volume depletion and inadequate fluid resus-citation in patients e bloodureanitrogen (BUN) e was also identi-fied as an early predictor of mortality in AP [15].
We assume that limited visceral blood flow, which results fromsevere intravascular volume depletion and associated stressresponse, leads to PNec.
This hypothesis was verified based on a cohort of retrospectivelyevaluated patients.
2. Aim
The aim of this study was to evaluate the significance of SCL andeGFR measured in an early phase of AP for prediction of PNec andfatal disease outcome.
3. Materials and methods
3.1. Patients
We conducted a retrospective study on 147 patients (93 menand 54 women, mean age 52, range 18e85 years) hospitalizedbetween 2001 and 2009. All patients admitted to the Departmentof Gastroenterology of the Central Clinical Hospital of the Ministryof Interior (Poland) with a diagnosis of acute pancreatitis and dis-ease onset within last 48 h were included in this study (n ¼ 147).The following study exclusion criteria were used; chronic kidneydisease and time from the first symptoms to admission exceeding48 h. The diagnosis was established on the basis of clinical picture,acute abdominal pain and at least 4-fold elevation of serumamylase and/or lipase levels. Relatively frequently, the diagnosis ofpancreatic necrosis was confirmed on CT examination due to thefact that the study took place at a tertiary referral center, where themost severe forms of acute pancreatitis from all over the countryare referred.
3.2. Study design
A contrast enhanced CT examination was performed in patientswith severe prognosis of AP (n ¼ 103) on days 4e7 followingthe onset of the disease in order to demonstrate the presence ofpancreatic necrosis. Prognosis of AP was assessed based onRanson score and CRP level. Obtaining at least 3 points in Ranson
score and/or CRP level over 150 mg/l predicted severe course ofAP. SCL and eGFR on admission and 48 h thereafter wereanalyzed for each patient. Estimated GFR was calculated using theabbreviated Modification of Diet in Renal Disease equation.
Elevated SCL was defined as creatinine �1.0 mg/dl, while eGFRvalues below 90 mL/min/1.73 m2 were considered abnormal.
Usefulness of SCL and eGFR for prediction of PNec was assessedby CT diagnosis of interstitial/necrotizing pancreatitis. The dataobtained on admission and after 48 h were analyzed with regard totheir predictive value for fatal outcome.
3.3. Statistical analysis
The Chi-square test and the Fisher exact test were used tocompare the distribution of patients’ characteristics. The receiveroperating characteristic (ROC) curve was used to represent thediagnostic accuracy. Student’s t-test was used to compare averagevalues across groups with p-value of 0.05 determining significance.
4. Results
PNec was confirmed in 41 (39.8%) out of 103 patients withperformed CT examinations. Both SCL and eGFR (Table 1)measured on admission (p < 0.001, p < 0.001, respectively) andafter 48 h (p ¼ 0.001, p < 0.001, respectively) were significantlyassociated with PNec.
Average values of SCL and eGFRwere compared between patientgroups without and with PNec. Average values of creatinine onadmission � SD were: 0.93 � 0.88 mg/dl and 1.20 � 0.44 mg/dlrespectively (p ¼ 0.06). Average concentrations of creatinine (�SD)48 h after admissionwere: 0.95� 0.75mg/dl and 1.27� 0.81mg/dl,respectively (p ¼ 0.04). Average values (�SD) of eGFR on admissionwere: 105.6 � 52.5 mL/min and 75.5 � 29.6 mL/min respectively(p ¼ 0.001, Table 2). Estimated GFR values below 90 mL/min/1.73 m2on the first day of hospitalization predicted PNec with asensitivity, specificity, and positive and negative predictive valuesof 78.1%, 71%, and 64% and 83% respectively.
Average values (�SD) of eGFR 48 h following admissionamounted to101.8 � 41.0 mL/min and 82.3 � 41.4 mL/min respec-tively (p ¼ 0.021). Statistical analysis of mean serum creatininelevels and eGFR on the 1st and the 3rd day of AP allows theconclusion that reduced eGFR on the 1st day of illness is the bestpredictor of pancreatic necrosis.
Changes in eGFR values within the first 3 days of hospitalizationand their influence on the occurrence of pancreatic necrosis werealso analyzed. Among patients with reduced eGFR on the 1st day ofhospitalization and subsequent eGFR normalization at day 3(n ¼ 12), pancreatic necrosis was confirmed in 6 cases. However, ina group of patients with normal eGFR on the first day and eGFRreduction on the 3rd day (n¼ 8), pancreatic necrosis was confirmedin only one case (Table 3). The overall mortality rate was 4.8%(7 patients).
One of themost important goals of the analysis was to assess thepossibility of using the values of SCL and eGFR obtained onadmission as predictive factors for fatal acute pancreatitis.
Accuracy of CRP, SCL and eGFR measured on the 1st day ofhospitalization in predicting mortality in AP was estimated using
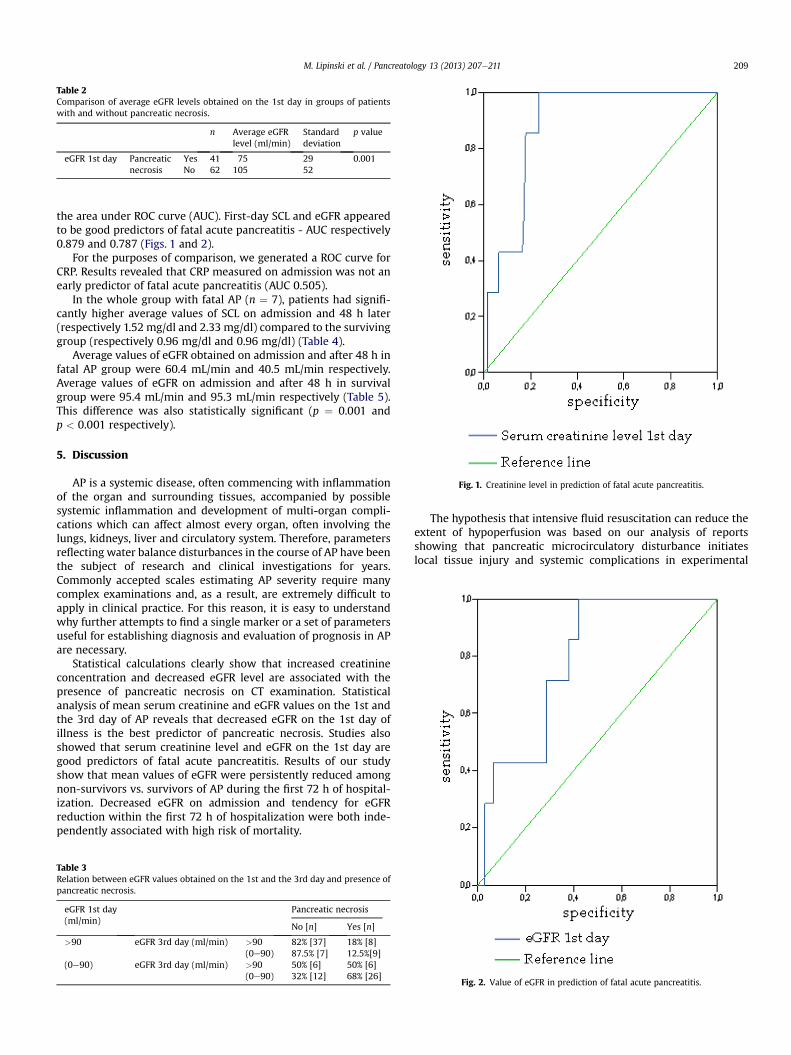
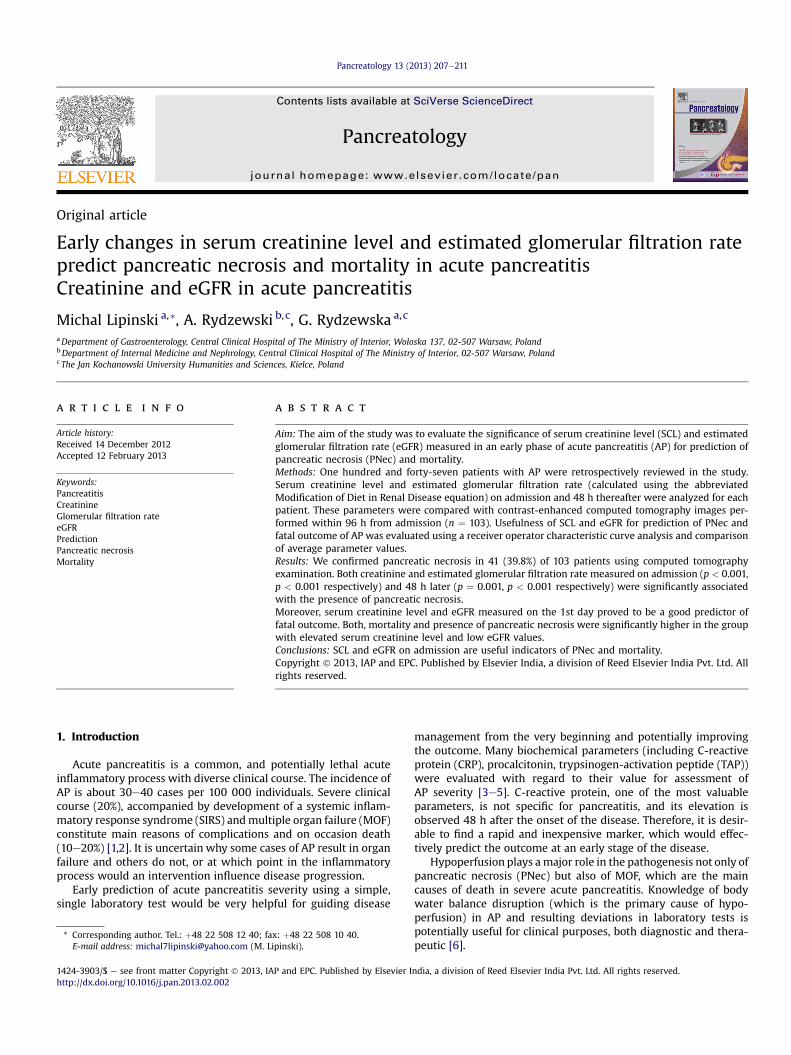
Fig. 1. Creatinine level in prediction of fatal acute pancreatitis.
Table 2Comparison of average eGFR levels obtained on the 1st day in groups of patientswith and without pancreatic necrosis.
n Average eGFRlevel (ml/min)
Standarddeviation
p value
eGFR 1st day Pancreaticnecrosis
Yes 41 75 29 0.001No 62 105 52
M. Lipinski et al. / Pancreatology 13 (2013) 207e211 209
the area under ROC curve (AUC). First-day SCL and eGFR appearedto be good predictors of fatal acute pancreatitis - AUC respectively0.879 and 0.787 (Figs. 1 and 2).
For the purposes of comparison, we generated a ROC curve forCRP. Results revealed that CRP measured on admission was not anearly predictor of fatal acute pancreatitis (AUC 0.505).
In the whole group with fatal AP (n ¼ 7), patients had signifi-cantly higher average values of SCL on admission and 48 h later(respectively 1.52 mg/dl and 2.33 mg/dl) compared to the survivinggroup (respectively 0.96 mg/dl and 0.96 mg/dl) (Table 4).
Average values of eGFR obtained on admission and after 48 h infatal AP group were 60.4 mL/min and 40.5 mL/min respectively.Average values of eGFR on admission and after 48 h in survivalgroup were 95.4 mL/min and 95.3 mL/min respectively (Table 5).This difference was also statistically significant (p ¼ 0.001 andp < 0.001 respectively).
5. Discussion
AP is a systemic disease, often commencing with inflammationof the organ and surrounding tissues, accompanied by possiblesystemic inflammation and development of multi-organ compli-cations which can affect almost every organ, often involving thelungs, kidneys, liver and circulatory system. Therefore, parametersreflecting water balance disturbances in the course of AP have beenthe subject of research and clinical investigations for years.Commonly accepted scales estimating AP severity require manycomplex examinations and, as a result, are extremely difficult toapply in clinical practice. For this reason, it is easy to understandwhy further attempts to find a single marker or a set of parametersuseful for establishing diagnosis and evaluation of prognosis in APare necessary.
Statistical calculations clearly show that increased creatinineconcentration and decreased eGFR level are associated with thepresence of pancreatic necrosis on CT examination. Statisticalanalysis of mean serum creatinine and eGFR values on the 1st andthe 3rd day of AP reveals that decreased eGFR on the 1st day ofillness is the best predictor of pancreatic necrosis. Studies alsoshowed that serum creatinine level and eGFR on the 1st day aregood predictors of fatal acute pancreatitis. Results of our studyshow that mean values of eGFR were persistently reduced amongnon-survivors vs. survivors of AP during the first 72 h of hospital-ization. Decreased eGFR on admission and tendency for eGFRreduction within the first 72 h of hospitalization were both inde-pendently associated with high risk of mortality.
Table 3Relation between eGFR values obtained on the 1st and the 3rd day and presence ofpancreatic necrosis.
eGFR 1st day(ml/min)
Pancreatic necrosis
No [n] Yes [n]
>90 eGFR 3rd day (ml/min) >90 82% [37] 18% [8](0e90) 87.5% [7] 12.5%[9]
(0e90) eGFR 3rd day (ml/min) >90 50% [6] 50% [6](0e90) 32% [12] 68% [26]
The hypothesis that intensive fluid resuscitation can reduce theextent of hypoperfusion was based on our analysis of reportsshowing that pancreatic microcirculatory disturbance initiateslocal tissue injury and systemic complications in experimental
Fig. 2. Value of eGFR in prediction of fatal acute pancreatitis.

Table 4Comparison of average creatinine levels obtained on the 1st and the 3rd day be-tween groups with fatal vs. non-fatal outcome.
Creatinine 1 day(mg/dl)
Creatinine 3 day(mg/dl)
Non-fataloutcome
n 140 140Average values[standard deviation]
0.96 [0.66] 0.96 [0.58]
Fatal outcome n 7 7Average values[standard deviation]
1.52 [0.63] 2.33 [1.32]
p value ¼0.001 <0.001
M. Lipinski et al. / Pancreatology 13 (2013) 207e211210
models of AP [7,8]. According to the American College of Gastro-enterology, “Aggressive intravenous fluid replacement is of criticalimportance to counteract hypovolemia caused by third space los-ses, vomiting, diaphoresis, and greater vascular permeabilitycaused by inflammatory mediators” [2].
Novel management options focus on adequate initial fluidresuscitation, which maintains microcirculation and therefore, hasthe potential to reduce ischemia, resultant reperfusion injury [16]and development of SIRS and MOF [17]. A few recently publishedstudies suggest that intensive fluid resuscitation may have a posi-tive impact on preventing pancreatic necrosis [18], as well asreduced incidence of SIRS and organ failure at 72 h [19]. Additionalrapid, early fluid resuscitation (more than one-third of the total72-h fluid volume within 24 h from presentation) translated tolower in-hospital mortality [20].
On the other hand, overly aggressive fluid resuscitation can beharmful in patients with renal or cardiac disease and in those ofadvanced age. One of the studies found that patients receiving 4 l ormore of intravenous fluids within the first 24 h were more likely todevelop respiratory complications and require intensive carecompared with those who received less than 4 l [21]. Other authorsreported that rapid hemodilution in severe AP was associated withincreased incidence of sepsis and in-hospital mortality [22].Controversially, hemodilution was divided into rapid and slowbased on hematocrit values below or above 35% within 48 h ofonset of SAP.
There is evidence of a pathophysiological role of hypovolemia indetermination of AP severity and the importance of fluid replace-ment for disease prognosis. One of them can be found in the Ransonscore e where 4 out of 11 points indicating severity of AP aredirectly related to fluid resuscitation (urea, net fluid sequestration,base deficit, and decreased hematocrit). Moreover, BUN e a simplemarker of hypovolemia and catabolism e was reported as a prog-nostic factor for AP mortality [15]. Early prediction of AP severityusing a single laboratory test for assessment of fluid loss would bevery helpful in assessment of prognosis and goal-orientedresuscitation.
The presented results suggest that intensive fluid resuscitationin the first days of acute pancreatitis can reduce the extent ofhypoperfusion and organ necrosis. Estimated GFR measured before
Table 5Comparison of average eGFR levels obtained on the 1st and the 3rd day betweengroups with fatal vs. non-fatal outcome.
eGFR 1(ml/min)
eGFR 3(ml/min)
Non-fataloutcome
n 140 140Average values [standard deviation] 95 [43] 95 [39]
Fatal outcome n 7 7Average values [standard deviation] 60 [24] 41 [19]
p value ¼0.01 <0.001
therapeutic intervention (especially before fluid therapy) in acutepancreatitis may be a good parameter to assess the need forintensive hydration. Low eGFR values on the first day of acutepancreatitis may suggest the need for intensive fluid resuscitation.Low eGFR values on the 3rd day of acute pancreatitis may indicatepersisting inadequate hydration, poor vascular filling and conse-quent hypoperfusion of the pancreas. Moreover, as shown above,persistently reduced eGFR on the 3rd day of acute pancreatitis isassociated with a high risk of fatal acute pancreatitis.
Knowledge of body water balance distortions in AP andresulting abnormalities in laboratory tests is potentially useful forboth diagnostic and therapeutic purposes. Simple assessment andaccessibility of parameters (indicators for hypoperfusion) makethem valuable prognostic factors. It is worth stressing that aprognosis of PNec and fatal outcome can be established with highsensitivity on the basis of studied parameters (creatinine andeGFR) already on the 1st day of AP. Early assessment of prognosismay guide prompt and appropriate therapy for severe AP. It can beexplained in most cases by an increase in serum creatinine in AP,i.e. hypovolemia present already on the 1st day of AP. At the sametime, increase in CRP level as late as on the 3rd day of AP is a well-known phenomenon. Moreover many scores for prediction of APseverity are complicated, difficult to use and consist countlessfactors.
In summary, early changes in SCL and in eGFR predict PNecand mortality in AP. We demonstrated that measurement ofcreatinine and eGFR calculation, as the most accurate means ofassessment of renal function, is helpful in predicting PNec andmortality during the first 72 h of hospitalization. Our study con-firms a strong association between eGFR assessment on admissionand after 48 h and the risk of PNec and mortality. Early identifi-cation of patients requiring intense fluid resuscitation mayimprove survival.
The eGFR level in AP has not been studied to date. A few pub-lished reports regarding the role of serum creatinine in prognosis ofthe course and complications of AP are not clear enough [23]. Thescope of our study was broadened to include eGFR, as a parameterthat is thought to better reflect disturbances in water balance thancreatinine. As a result, we recommend using eGFR for prediction ofsevere AP.
Disclosure statement
Authors have no conflicts of interest.
References
[1] Toouli J, Brooke-Smith M, Bassi C, Carr-Locke D, Telford J, Freeny P, et al.Guidelines for the management of acute pancreatitis. J Gastroenterol Hepatol2002;17(Suppl.):S15e39.
[2] Banks Peter A, Freeman Martin L, the Practice Parameters Committee of theAmerican College of Gastroenterology. Practice guidelines in acute pancrea-titis. Am J Gastroenterol 2006;101:2379e400.
[3] Gurleyik G, Cirpici OZ, Aktekin A, Saglam A. The value of Ranson and APACHEII scoring systems, and serum levels of interleukin-6 and C-reactive protein inthe early diagnosis of the severity of acute pancreatitis. Ulus Travma Derg2004;10(2):83e8.
[4] Mofidi R, Suttie SA, Patil PV, Ogston S, Parks RW. The value of procalcitonin atpredicting the severity of acute pancreatitis and development of infectedpancreatic necrosis: systematic review. Surgery 2009 Jul;146(1):72e81.
[5] Neoptolemos JP, Kemppainen EA, Mayer JM, Fitzpatrick JM, Raraty MG,Slavin J, et al. Early prediction of severity in acute pancreatitis by urinarytrypsinogen activation peptide: a multicentre study. Lancet 2000 Jun 3;355(9219):1955e60.
[6] Brown A, Orav J, Banks PA. Hemoconcentration is an early marker for organfailure and necrotizing pancreatitis. Pancreas 2000 May;20(4):367e72.
[7] Bassi D, Kollias N, Fernandez-del Castillo C, Foitzik T, Warshaw AL,Rattner DW. Impairment of pancreatic microcirculation correlates with theseverity of acute experimental pancreatitis. J Am Coll Surg 1994 Sep;179(3):257e63.

M. Lipinski et al. / Pancreatology 13 (2013) 207e211 211
[8] Mann O, Kaifi J, Bloechle C, Schneider CG, Yekebas E, Kluth D, et al. Therapeuticsmall-volume resuscitation preserves pancreatic microcirculation in acute exper-imental pancreatitis of graded severity in rats. Pancreatology 2009;9(5):652e61.
[9] Mao EQ, Tang YQ, Fei J, Qin S, Wu J, Li L, et al. Fluid therapy for severe acutepancreatitis in acute response stage. Chin Med J (Engl) 2009 Jan 20;122(2):169e73.
[10] Mole DJ, Olabi B, Robinson V, Garden OJ, Parks RW. Incidence of individualorgan dysfunction in fatal acute pancreatitis: analysis of 1024 death records.In: Presented in part at the European Pancreatic Club meeting, Newcastle-upon-Tyne; 5e6 July 2007.
[11] Kes P, Vucicevi�c Z, Ratkovi�c-Gusi�c I, Fotivec A. Acute renal failure complicatingsevere acute pancreatitis. Ren Fail 1996;18(4):621e8.
[12] Tran DD, Oe PL, de Fijter CWH, Van der Meulen J, Cuesta MA. Acute renalfailure in patients with acute pancreatitis: prevalence, risk factors andoutcome. Nephrol Dial Transplant 1993;8:1079e84.
[13] Kess P, Vucicevic Z, Ratkovic-Gusic I, Fotivec A. Acute renal failure compli-cating severe acute pancreatitis. Nephron 1996;73:488e9.
[14] Muddana V, Whitcomb DC, Khalid A, Slivka A, Papachristou GI. Elevatedserum creatinine as a marker of pancreatic necrosis in acute pancreatitis. Am JGastroenterol 2009 Jan;104(1):164e70.
[15] Wu BU, Johannes RS, Sun X, Conwell DL, Banks PA. Early changes in blood ureanitrogen predict mortality in acute pancreatitis. Gastroenterology 2009 Jul;137(1):129e35.
[16] Knoefel WT, Kollias N, Warshaw A, Waldner H, Nishioka NS, Rattner DW.Pancreatic microcirculation changes in experimental pancreatitis of graderseverity in rat. Surgery 1994;116:904e13.
[17] Panek J, Zasada J, Po�zniczek M. Microcirculatory disturbance in the course ofacute pancreatitis. Przegl Lek 2007;64(6):435e7.
[18] Wall I, Badalov N, Baradarian R, Iswara K, Li JJ, Tenner S. Decreased mortalityin acute pancreatitis related to early aggressive hydration. Pancreas 2011May;40(4):547e50.
[19] WarndorfMG,KurtzmanJT,BartelMJ, CoxM,Mackenzie T,RobinsonS, et al. Earlyfluid resuscitation reduces morbidity among patients with acute pancreatitis.Clin Gastroenterol Hepatol 2011 Aug;9(8):705e9 [Epub 2011 Apr 8].
[20] Gardner TB, Vege SS, Chari ST, Petersen BT, Topazian MD, Clain JE, et al.Faster rate of initial fluid resuscitation in severe acute pancreatitis diminishesin-hospital mortality. Pancreatology 2009;9(6):770e6 [Epub 2010 Jan 21].
[21] Eckerwall G, Olin H, Andersson B, Andersson R. Fluid resuscitation andnutritional support during severe acute pancreatitis in the past: what have welearned and how can we do better? Clin Nutr 2006;25:497e504.
[22] Mao EQ, Fei J, Peng YB, Huang J, Tang YQ, Zhang SD. Rapid hemodilution isassociated with increased sepsis and mortality among patients with severeacute pancreatitis. Chin Med J 2010;123(13):1639e44.
[23] Lankisch PG, Weber-Dany B, Maisonneuve P, Lowenfels AB. High serumcreatinine in acute pancreatitis: a marker for pancreatic necrosis? Am J Gas-troenterol 2010 May;105(5):1196e200.