dyspepsia in healthy blood donors
TRANSCRIPT
Digestive Diseases and Sciences, Vol. 39, No. 5 (May 1994), pp. 1090-1098
Dyspepsia in Healthy Blood Donors Pattern of Symptoms and Association with
Helicobacter pylori
GERALD HOLTMANN, HARALD GOEBELL, MARIANNE HOLTMANN, and NICHOLAS J. TALLEY
Whether Helicobacter pylori is causally linked to dyspepsia remains controversial The aims of this study were to assess in healthy blood donors the prevalence of dyspepsia and dyspepsia subgroups, determine if H. pylor i /s associated with different categories o f dyspeptic symptoms, and evaluate the association between dyspepsia and nicotine, alcohol, and analgesic use. Consecutive blood donors (N = 180) who had no clinical evidence of organic disease were included. Abdominal symptoms were measured by means of a standardized questionnaire that has been previously validated. Subjects with dyspepsia (defined as pain localized to the upper abdomen) were further subdivided into those with ulcer-like, dysmotility-like, reflux-like, or nonspecific dyspepsia. A total o f 65 subjects reported abdominal pain or discomfort during the prior 12 months [36.1%, 95% confidence interval (CI) 29.1-43.1]; 44 subjects (24. 4%, 95% C118. 2-30. 7) had dyspepsia. Dysmotility-like, reflux-like, and ulcer-like symptoms were reported by 19. 4% (95% CI 13.7-25.2), 17.2% (95% C1 11.7-22.7), and 16.7% (95% C1 11.2-22.1) of subjects with dyspepsia, respectively. Fifty-seven subjects (31.7%, 95% C1 24. 9-38. 5) were H. pylori positive; 26% of subjects with H. pylori and 24% without H. pylori had dyspepsia (P > O. 50). The seroprevalence of H. pylori was also similar among the different categories of dyspepsia. We conclude that infection with H. pylori is not associated with abdominal complaints in otherwise healthy subjects.
KEY WORDS: aspirin; functional dyspepsia; Hel icobacterpy lor i ; irritable bowel syndrome.
Symptoms of upper gastrointestinal distress are among the most frequent complaints seen by phy- sicians in Western countries (1-4). Even though there is evidence that disturbed motility and percep- tion occur in some patients with functional dyspep-
Manuscript received February 10, 1993; revised manuscript received August 19, 1993; accepted September 7, 1993.
From the Division of Gastroenterology, University of Essen, Germany; Department of Transfusion Medicine, University of Essen, Germany; and University of Sydney, Sydney, Australia.
Supported by a grant from Deutsche Forschungsgemeinschaft, grant number Ho 1193/3-1. Parts of this study were presented at the Annual Meeting of the American Gastroenterological Asso- ciation in Boston, May 1993 and published as an abstract (Gas- troenterology 104:A102, 1993).
Address for reprint requests: Dr. Gerald Holtmann, Univer- sity of Essen, Department of Internal Medicine, Division of Gastroenterology, Hufelandstr. 55, 45122 Essen, Germany.
1090
sia (5, 6), the pathophysiology is very poorly under- stood. One potential pathogenic factor is histological gastritis, but the relationship between dyspeptic symptoms and gastritis has remained controversial for years (7).
It is now accepted that chronic gastritis is usually due to infection with Helicobacterpylori (8-11). In previous studies, the prevalence rate of infection with H. pylori in patients with functional dyspepsia has approached 50% (12-20) although infection is also common in asymptomatic persons (10). If H. pylori plays a pathogenic role in functional dyspep- sia, there should be an association between dyspep- sia and H. pylori. However, data on the relationship between specific upper abdominal symptoms and
Digestive Diseases and Sciences, Vol. 39, No. 5 (May 1994) 0163-21 t6/94/0500-109(007,00/0 © 1994 Plenum Publishing Corporation
DYSPEPSIA AND H. pylori
H. pylori remains conflicting, with some studies reporting a positive association (17-19, 21) and oth- ers failing to confirm any link (13, 15, 20, 22-24). Such disparate results could have arisen for meth- odological reasons. In particular, selection bias may be important, as most of the studies have dealt only with patients who by definition have sought health care. Because health care seeking behavior in pa- tients with functional bowel disease is influenced by social and psychological factors (25, 26) and be- cause those who present are just a small proportion of subjects with dyspepsia (4), the results of outpa- tient studies are likely to be biased. Furthermore, previous studies have often not controlled for po- tential confounding variables such as age or social status, which are linked to H. pytori (27). Another limitation may have been the lack of adequate cat- egorization of symptoms. Patients with dyspepsia can be subdivided into subgroups based on the symptoms that predominate (28, 29). Dyspepsia cat- egories include dysmotility-like, ulcer-like, reflux- like, and nonspecific dyspepsia, and it has been proposed that these subgroups reflect entities with different pathophysiologies (28). Whether H. pylori is associated with any particular dyspepsia symp- tom subgroup in the general (nonpatient) population is unknown.
We, therefore, aimed to estimate the prevalence of dyspeptic symptoms in healthy blood donors and evaluate the association of symptoms with the pres- ence of H. pylori antibodies. To test the hypothesis that the different symptom subgroups identify dis- tinct underlying pathophysiological disturbances, the association between specific categories of dys- pepsia and H. pylori serology was also investigated. We postulated that ulcer-like dyspepsia, but not the other symptom subgroups, would be associated with H. pylori infection because this infection is strongly linked to the pathogenesis of chronic pep- tic ulceration (30). To control for other possible confounders, the association between dyspeptic symptoms and potential risk factors other than H. pylori, namely smoking, alcohol consumption, and analgesic use, were also studied.
MATERIALS AND METHODS
Subjects. The study protocol was approved by the Institutional Review Board of the University of Essen. During a four-week period, 180 consecutive healthy per- sons who volunteered to provide a blood donation were included in the study. After giving informed consent, all volunteers underwent a physical examination and labora-
tory screening (sedimentation rate, red and white blood count, transaminases, gamma glutamyltransferase, hepa- titis B and C antibodies, and HIV antibodies). In addition 10 cc of blood was taken for the determination of Heli- cobacterpylori antibodies (ELIAS, Freiburg, Germany). The preparation of the antigen used for this commercially available assay was performed according to the method described by Blaser and Duncan (31). Previous studies have shown that the serodiagnosis of H. pylori is highly sensitive and specific; serodiagnosis is one of the gold standard tests for identifying H. pylori infection (32). Compared with the combination of CLO-testing, histol- ogy and microbiological culture, sensitivity and specific- ity of the present assay were 93% and 88%, respectively in a study population of 40 patients tested in our labora- tory.
During the six-week study period, all subjects eligible for a blood donation were asked to participate in the study. Four subjects did not qualify for a blood donation (one volunteer had undergone orthopedic surgery within the last six months, in one volunteer transaminases were elevated, and two volunteers had been visiting tropical areas in the six months prior to the study). Furthermore, three subjects refused to participate in the study, and one subject with a history of duodenal ulcer disease with dyspeptic symptoms was excluded since peptic ulcer was not ruled out as a cause of symptoms. In contrast, five subjects with a history of a peptic ulcer more than five years ago but without evidence of current organic disease were included. Therefore, out of a population of 188 subjects, data from 180 subjects (95.7%) were available for further analyses.
Assessment of Abdominal Symptoms. A German version of the previously validated Bowel Disease Questionnaire [BDQ, (33)] was given to all study participants. It was completed prior to the physical examination. The German version of the questionnaire has been shown to be easily understandable and completed by a German-speaking population in pretesting the instrument. Furthermore, to confirm the reliability of this instrument, 40 subjects from the study population were also asked to complete it on two separate occasions. The median time between com- pletion of the surveys was 60 days (range 14-90). The percent agreement observed and the kappa statistic for each symptom item was calculated (34). The English version, used in previous studies (4), has been shown to have adequate content as well as predictive and construct validity for the measurement of gastrointestinal tract symptoms (33).
Selection of Questionnaire Items. Standardized criteria were utilized for the categorization of symptoms based on previous studies (4, 29). Briefly, subjects who reported pain centered in the upper abdomen during the previous year were classified as having dyspepsia; those with pain more than six times during the last year were considered to have frequent dyspepsia (3). The subjects were also categorized into one of the following symptom groups based on their responses on the BDQ:
Category 1, ulcer-like symptoms, included subjects with upper abdominal pain and at least two of the follow- ing symptoms (4, 28, 29, 35, 36): (a) pain often relieved by food (>25% of the time); (b) pain often relieved by ant-
Digestive Diseases and Sciences, Vol. 39, No. 5 (May 1994) 1091
HOLTMANN ET AL
acids; (c) pain often before meals or when hungry; (d) periodic pain (periods of at least one month without pain, with periods in between of weeks to month when there is pain); and/or (e) night pain (waking the subject from sleep).
Category 2, dysmotility-like dyspepsia (4, 28, 29, 35), included subjects with upper abdominal pain and at least three or more of the following symptoms suggesting gas- tric stasis or upper intestinal dysmotility: (a) nausea or vomiting once a month or more; (b) abdominal bloating and visible distension, often; (c) anorexia or weight loss (>3.5 kg); (d) pain often aggravated by food or milk; (e) pain often after meals; and/or (f) pain often relieved by belching.
Category 3, reflux-like dyspepsia (4, 28, 29, 35), in- cluded subjects who had upper abdominal pain associated by one or more of the following symptoms: (a) heartburn at least once a week or more; and/or (b) acid regurgitation once a week or more.
Category 4, nonspecific dyspepsia (4, 35), included subjects with upper abdominal pain that did not fit into categories 1, 2, or 3.
Symptoms Compatible with Irritable Bowel Syndrome (IBS). Lower abdominal pain often relieved by defecation and/or looser or more frequent stools at its onset was classified as colonic pain; this type of pain was considered to be characteristic of IBS, based on the modified Rome criteria for IBS (4, 35). IBS was also considered to be present if three or more of the following symptoms that define a chronic but irregular disturbance of defecation were reported: (a) altered stool frequency (>3 stools daily and/or <3 stools weekly, often); (b) altered stool form (hard and/or loose or watery, often); (c) altered stool passage (straining and/or a feeling of incomplete evacua- tion and/or urgency often), and (d) mucus per rectum. These symptoms also comprise part of the Rome criteria for IBS.
Other Potential Risk Factors. Socioeconomic status was graded 1-4 based on the educational level achieved (with- out formal degree; up to 10 years of school education; more than 10 years of school education; or university degree). Marital status, employment status, a past history of peptic ulcer disease, a history of abdominal pain as a child, a history of abdominal surgery, and physician visits in the previous year were obtained from the responses to the questionnaire. In addition, the frequency and severity of 12 extraintestinal complaints were measured including headache, eye pain when reading, backpain, and stiffness (36). Smoking, high alcohol consumption (defined as more than six glasses of alcoholic beverages per week, eg, six glasses of German beer or wine per week), and use of analgesics (eg, aspirin or paracetamol) were also as- sessed. The sociodemographic characteristics of the study population are summarized in Table 1.
Statistical Analyses. Prevalence rates and the respective 95% confidence intervals were calculated (36-38). Non- parametric tests were used for comparisons. Logistic regression analysis was utilized to determine the associ- ation between H. pylori seroprevalence (adjusting for age, gender, and socioeconomic status based on educa- tional level) and dyspeptic symptoms or categories of dyspeptic symptoms. Similarly, the association between
TABLE l. SOCIODEMOGRAPHIC CHARACTERISTICS OF STUDY POPULATION (N = 180)
Age, years [mean (std, range)] 32.3 (10.5, 18-62) Gender, male (N, %) 106, 58.9 Marital status (%)
Single 51.7 Married/partnership 44.5 Divorced/separated 2.2 Widowed 1.7
Educational level (%) Without formal degree 3.8 Up to 10 years of school 42.4 More than 10 years of school 37.9 University degree 15.9
Working (%) Employed/own business 80.0 Unemployed 10.0 Retired 2.8 Housewife 7.2
H. pylori and age, frequent alcohol consumption, smok- ing, and intake of analgesics was evaluated using logistic regression. Risk factors were coded as present or absent (39). All P values calculated were two-tailed; an et level of 5% was considered significant. Statistical analyses were performed using the Statistical Analysis System [SAS Institute Release 6.04 (40)].
RESULTS
Gastrointestinal Symptoms. S y m p t o m s repor ted by men and women in the s tudy populat ion are summar ized in Table 2. A total of 65 of the 180 heal thy blood donors (36.1%, 95% CI 29.1-43.1) repor ted abdominal pain or discomfort in the prior 12 months . For ty- four persons (24.4%, 95% CI 18.2-30.7) repor ted dyspeps ia and 27 (15.0%, 95% CI 9.8-20.2%) had frequent dyspepsia . Significant differences in the f requency of dyspept ic s y m p t o m s among men and w o m e n were not found, and the f requency of dyspeps ia did not va ry significantly with age.
Of the 46 s y m p t o m items, all were significantly reliable and mos t quest ions produced good to ex- cellent agreement in the 40 subjects tested. The median kappa statistic for the s y m p t o m items was 0.72 (interquartile range 0.48-1.0).
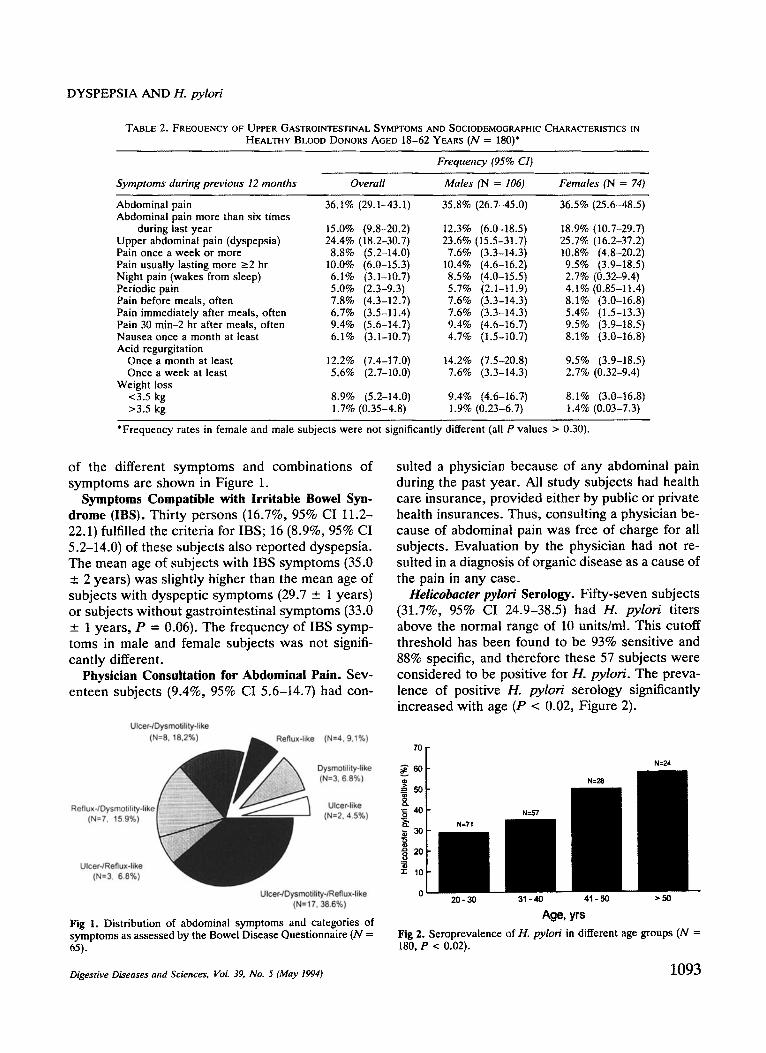
Subgroups of Dyspepsia. Dysmoti l i ty-l ike symp- toms were repor ted by 19.4% (95% CI 13.7-25.2), reflux-like s y m p t o m s by 17.2% (95% CI 11.7-22.7) and ulcer-like s y m p t o m s by 16.7% (95% CI 11.2- 22.1) of subjects with dyspepsia . H o w e v e r , only 19.4% (95% CI 13.7-25.2) of subjects could be clas- sified into one ca tegory of s y m p t o m s alone; all other persons repor ted s y m p t o m s compat ib le with two or more subgroups of dyspepsia . The f requency
1092 Digestive Diseases and Sciences, Vol. 39, No. 5 (May 1994)
D Y S P E P S I A A N D 1-1. py lor i
TABLE 2. FREQUENCY OF UPPER GASTROINTESTINAL SYMPTOMS AND SOCIODEMOGRAPHIC CHARACTERISTICS IN HEALTHY BLOOD DONORS AGED 18-62 YEARS (N = 180)*
Symptoms during previous 12 months Overall
Frequency (95% CI)
Males (N = 106) Females (N = 74)
Abdominal pain 36.1% (29.1-43.1) 35.8% (26.7-45.0) 36.5% (25.6-48.5) Abdominal pain more than six times
during last year 15.0% (9.8-20.2) 12.3% (6.0-18.5) 18.9% (10.7-29.7) Upper abdominal pain (dyspepsia) 24.4% (18.2-30.7) 23.6% (15.5-31.7) 25.7% (16.2-37.2) Pain once a week or more 8.8% (5.2-14.0) 7.6% (3.3-14.3) 10.8% (4.8-20.2) Pain usually lasting more >--2 hr 10.0% (6.0-15.3) 10.4% (4.6-16.2) 9.5% (3.9-18.5) Night pain (wakes from sleep) 6.1% (3.1-10.7) 8.5% (4.0-15.5) 2.7% (0.32-9.4) Periodic pain 5.0% (2.3-9.3) 5.7% (2.1-t 1.9) 4. I% (0.85-11.4) Pain before meals, often 7.8% (4.3-12.7) 7.6% (3.3-14.3) 8.1% (3.0-16.8) Pain immediately after meals, often 6.7% (3.5-11.4) 7.6% (3.3-14.3) 5.4% (1.5-13.3) Pain 30 min-2 hr after meals, often 9.4% (5.6-14.7) 9.4% (4.6-16.7) 9.5% (3.9-18.5) Nausea once a month at least 6.1% (3.1-10.7) 4.7% (1.5-10.7) 8.1% (3.0-16.8) Acid regurgitation
Once a month at least 12.2% (7.4-17.0) 14.2% (7.5-20.8) 9.5% (3.9-18.5) Once a week at least 5.6% (2.7-10.0) 7.6% (3.3-14.3) 2.7% (0.32-9.4)
Weight loss <3.5kg 8.9% (5.2-14.0) 9.4% (4.6-16.7) 8.1% (3.0-16.8) >3.5 kg 1.7% (0.35-4.8) 1.9% (0.23-6.7) 1.4% (0.03-7.3)
*Frequency rates in female and male subjects were not significantly different (all P values > 0.30).
of the different symptoms and combinations of symptoms are shown in Figure 1.
Symptoms Compatible with Irritable Bowel Syn- drome (IBS). Thirty persons (16.7%, 95% CI 11.2- 22.1) fulfilled the criteria for IBS; 16 (8.9%, 95% CI 5.2-14.0) of these subjects also reported dyspepsia. The mean age of subjects with IBS symptoms (35.0 _+ 2 years) was slightly higher than the mean age of subjects with dyspeptic symptoms (29.7 --- 1 years) or subjects without gastrointestinal symptoms (33.0 _-. 1 years, P = 0.06). The frequency of IBS symp- toms in male and female subjects was not signifi- cantly different.
Physician Consultation for Abdominal Pain. Sev- enteen subjects (9.4%, 95% CI 5.6-14.7) had con-
Ulcer-/Dysmotility-like (t~ . . . . . . . . . . . . . ~, (N=4, 9,1%)
Dysmotility-like (N=3. 6.8%)
Reflux4Dysmotility-like Ulcer-like (N=7, 15.9%) (N=2.4.5%)
UIcer4Reflux-like (N=3, 6.8%)
Ulcer4Dysmotility-/Reflux-like (N=17, 36,6%)
Fig 1. Distr ibution of abdominal symptoms and categories of symptoms as assessed by the Bowel Disease Questionnaire (N = 65).
suited a physician because of any abdominal pain during the past year. All study subjects had health care insurance, provided either by public or private health insurances. Thus, consulting a physician be- cause of abdominal pain was free of charge for all subjects. Evaluation by the physician had not re- sulted in a diagnosis of organic disease as a cause of the pain in any case.
Helicobacter pylori Serology. Fifty-seven subjects (31.7%, 95% CI 24.9-38.5) had H. pylori titers above the normal range of 10 units/ml. This cutoff threshold has been found to be 93% sensitive and 88% specific, and therefore these 57 subjects were considered to be positive for H. pylori. The preva- lence of positive H. pylori serology significantly increased with age (P < 0.02, Figure 2).
7O
60
,-= 50
.o~ 40
~ z o
20
i 1o
o 20-30 31-40 41-50 >50
Age, yrs Fig 2. Seroprevalence of H. p y l o r i in different age groups (N = 180, P < 0.02).
Digestive Diseases and Sciences, VoL 39, No. 5 (May 1994) 1093
H O L T M A N N ET A L
TABLE 3. FREQUENCY OF UPPER GASTROINTESTINAL SYMPTOMS IN PATIENTS WITH AND WITHOUT POSITIVE n. pylori SEROLOGY
Symptoms during previous 12 months
Frequency (95% CI)
H. pylori negative H. pylori positive (N = 123) (N = 57) P value
Abdominal pain Abdominal pain more than six times during last year Upper abdominal pain (dyspepsia) Pain once a week or more Pain usually lasting more ~2 hr Pain severity moderate or worse Night pain (wakes from sleep)
Periodic pain Pain before meals, often Pain immediately after meals, often
Pain 30 min-2 hr after meals, often Pain relieved by food Pain aggravated by food/milk Pain aggravated by alcohol Pain relieved by antacids Nausea once a month at least Abdominal pain Acid regurgitation
Once a month at least Once a week at least
Weight loss <3.5 kg >3.5 kg
39.0% (30.4-47.6) 29.8% (18.4-43.4) 14.6% (8.4-20.9) 15.8% (7.5-27.9) 23.6% (16.1-31.1) 26.3% (I5.5-39.7) 8.1% (4.0-14.4) 10.5% (4.0-21.5) 9.8% (5.2-16.4) 10.5% (4.0-21.5)
29.3% (21.2-37.3) 24.6% (14.1-37.8) 5.7% (2.3-11.4) 7.0% (2.0-17.0)
4.9% (1.8-10.3) 5.3% (1.1-14.6) 8.9% (4.6-15.4) 5.3% (1.1-14.6) 6.5% (2.9-12.4) 7.0% (2.0-17.0)
0.23 0.92 0.56 0.19 0.26 0.6 0.75 0.44 0.91 0.39 0.75 0.74
8.9% (4.6-15.4) 10.5% (4.0-21.5) 11.4% (5.8-17.0) 10.5% (4.0-21.5) 0.87 13.0% (7.1-19.0) 5.3% (1.1-14.6) 0.12 7.3% (3.4-13.4) 7.0% (2.0-17.0) 0.96
12.2% (6.4-18.0) 10.5% (4.0-21.5) 0.58 7.3% (3.4-13.4) 3.5% (0.43-12.1) 0.20
39.0% (30.4-47.6) 29.8% (18.4-43.4) 0.23
12.2% (6.4-18.0) 12.3% (5.1-23.7) 0.83 5.7% (2.3-11.4) 5.3% (1.1-14.6) 0.83
8.9% (4.6-15.4) 8.8% (2.9-19.3) 0.49 2.4% (0.5-7.0) 0% 0.49
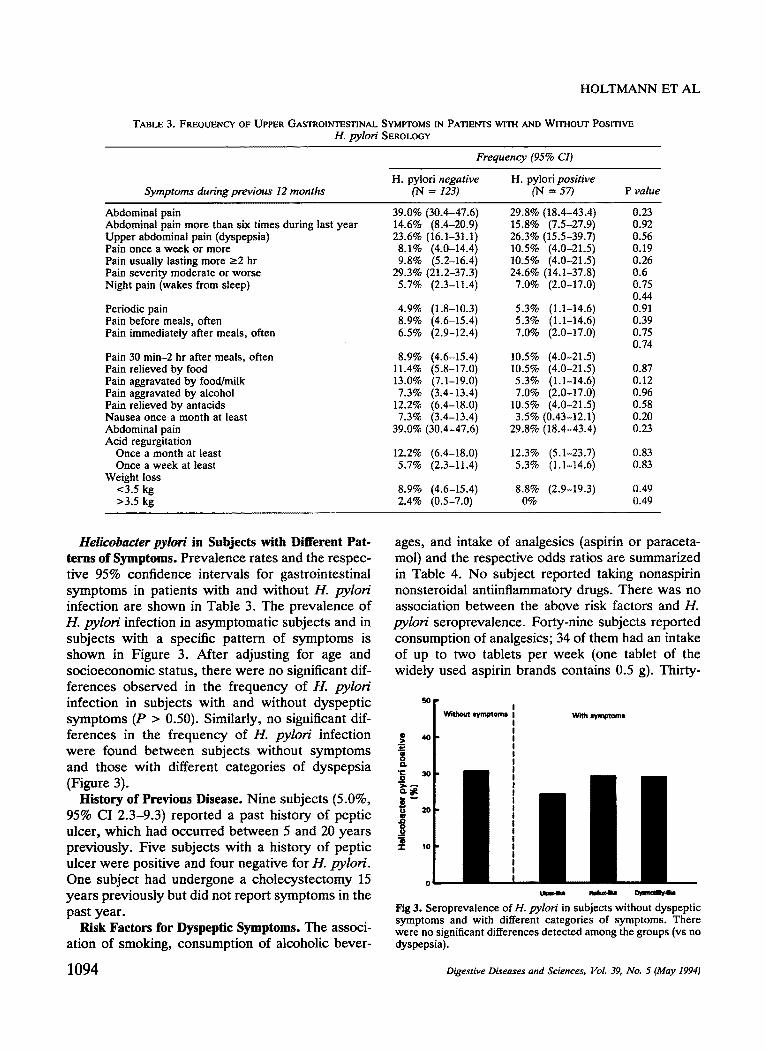
Helicobacter pylori in Subjects with Different Pat- terns of Symptoms. Prevalence rates and the respec- tive 95% confidence intervals for gastrointestinal symptoms in patients with and without 1-1. pylori infection are shown in Table 3. The prevalence of H. pylori infection in asymptomatic subjects and in subjects with a specific pattern of symptoms is shown in Figure 3. After adjusting for age and socioeconomic status, there were no significant dif- ferences observed in the frequency of H. pylori infection in subjects with and without dyspeptic symptoms (P > 0.50). Similarly, no significant dif- ferences in the frequency of H. pylori infection were found between subjects without symptoms and those with different categories of dyspepsia (Figure 3).
History of Previous Disease. Nine subjects (5.0%, 95% CI 2.3-9.3) reported a past history of peptic ulcer, which had occurred between 5 and 20 years previously. Five subjects with a history of peptic ulcer were positive and four negative for H. pylori. One subject had undergone a cholecystectomy 15 years previously but did not report symptoms in the past year.
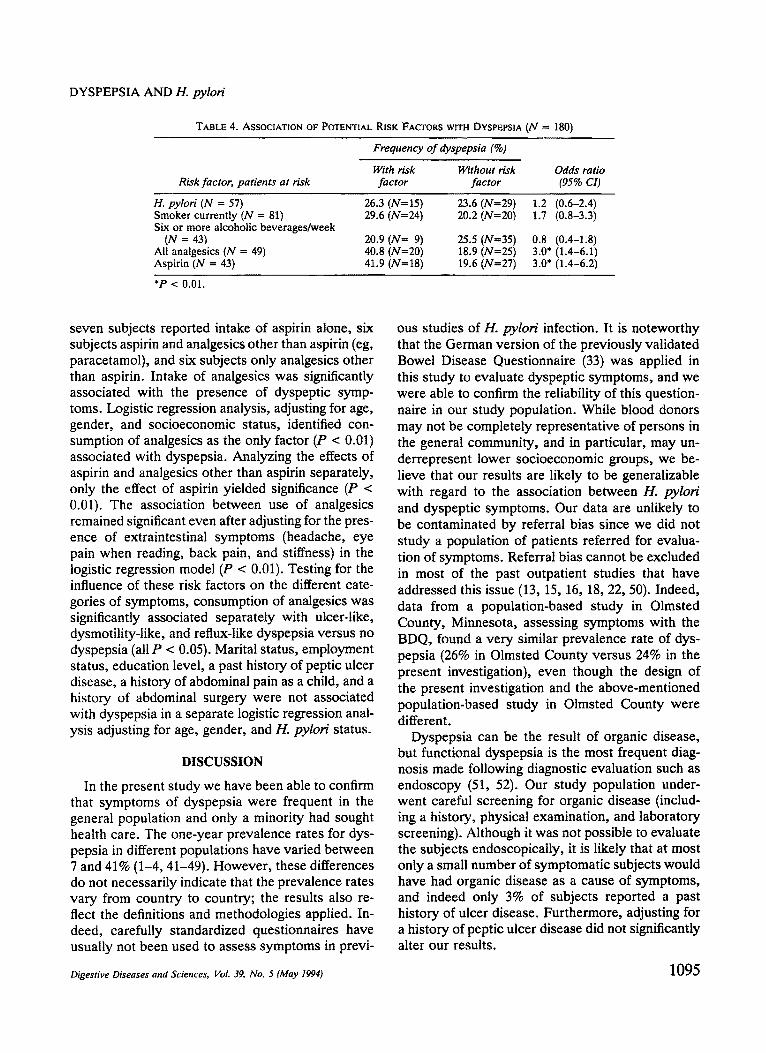
Risk Factors for Dyspeptic Symptoms. The associ- ation of smoking, consumption of alcoholic bever-
ages, and intake of analgesics (aspirin or paraceta- mol) and the respective odds ratios are summarized in Table 4. No subject reported taking nonaspirin nonsteroidal antiinflammatory drugs. There was no association between the above risk factors and H. pylori seroprevalence. Forty-nine subjects reported consumption of analgesics; 34 of them had an intake of up to two tablets per week (one tablet of the widely used aspirin brands contains 0.5 g). Thirty-
g i . 0
.Q 0 o
T
50 I ~V'I~Ui i~rrl~om|
F 4O
3O
20
10
With ~mptaml
0 L~w~ke R m ~
Fig 3. Seroprevalence of H. pylori in subjects without dyspeptic symptoms and with different categories of symptoms. There were no significant differences detected among the groups (vs no dyspepsia).
1094 Digestive Diseases and Sciences, VoL 39, No. 5 (May 1994)
DYSPEPSIA AND H. pylori
TABLE 4. ASSOCIATION OF POTENTIAL RISK FACTORS WITH DYSPEPSIA (N = 180)
Risk factor, patients at risk
Frequency of dyspepsia (%)
With risk Without risk Odds ratio factor factor (95% CI)
H. pylori (N = 57) 26.3 (N=15) 23.6 (N=29) 1.2 (0.6-2.4) Smoker currently (N = 81) 29.6 (N=24) 20.2 (N=20) 1.7 (0.8-3.3) Six or more alcoholic beverages/week
(N = 43) 20.9 (iV= 9) 25.5 (N=35) 0.8 (0.4-1.8) All analgesics (N = 49) 40.8 (N=20) 18.9 (N=25) 3.0* (1.4-6.1) Aspirin (N = 43) 41.9 (N=lS) 19.6 (N=27) 3.0* (1.4-6.2)
*P < 0.01.
seven subjects reported intake of aspirin alone, six subjects aspirin and analgesics other than aspirin (eg, paracetamol), and six subjects only analgesics other than aspirin. Intake of analgesics was significantly associated with the presence of dyspeptic symp- toms. Logistic regression analysis, adjusting for age, gender, and socioeconomic status, identified con- sumption of analgesics as the only factor (P < 0.01) associated with dyspepsia. Analyzing the effects of aspirin and analgesics other than aspirin separately, only the effect of aspirin yielded significance (P < 0.01). The association between use of analgesics remained significant even after adjusting for the pres- ence of extraintestinal symptoms (headache, eye pain when reading, back pain, and stiffness) in the logistic regression model (P < 0.01). Testing for the influence of these risk factors on the different cate- gories of symptoms, consumption of analgesics was significantly associated separately with ulcer-like, dysmotility-like, and reflux-like dyspepsia versus no dyspepsia (all P < 0.05). Marital status, employment status, education level, a past history of peptic ulcer disease, a history of abdominal pain as a child, and a history of abdominal surgery were not associated with dyspepsia in a separate logistic regression anal- ysis adjusting for age, gender, and H. pylori status.
DISCUSSION
In the present study we have been able to confirm that symptoms of dyspepsia were frequent in the general population and only a minority had sought health care. The one-year prevalence rates for dys- pepsia in different populations have varied between 7 and 41% (1-4, 41-49). However, these differences do not necessarily indicate that the prevalence rates vary from country to country; the results also re- flect the definitions and methodologies applied. In- deed, carefully standardized questionnaires have usually not been used to assess symptoms in previ-
ous studies of H. pylori infection. It is noteworthy that the German version of the previously validated Bowel Disease Questionnaire (33) was applied in this study to evaluate dyspeptic symptoms, and we were able to confirm the reliability of this question- naire in our study population. While blood donors may not be completely representative of persons in the general community, and in particular, may un- derrepresent lower socioeconomic groups, we be- lieve that our results are likely to be generalizable with regard to the association between H. pylori and dyspeptic symptoms. Our data are unlikely to be contaminated by referral bias since we did not study a population of patients referred for evalua- tion of symptoms. Referral bias cannot be excluded in most of the past outpatient studies that have addressed this issue (13, 15, 16, 18, 22, 50). Indeed, data from a population-based study in Olmsted County, Minnesota, assessing symptoms with the BDQ, found a very similar prevalence rate of dys- pepsia (26% in Olmsted County versus 24% in the present investigation), even though the design of the present investigation and the above-mentioned population-based study in Olmsted County were different.
Dyspepsia can be the result of organic disease, but functional dyspepsia is the most frequent diag- nosis made following diagnostic evaluation such as endoscopy (51, 52). Our study population under- went careful screening for organic disease (includ- ing a history, physical examination, and laboratory screening). Although it was not possible to evaluate the subjects endoscopically, it is likely that at most only a small number of symptomatic subjects would have had organic disease as a cause of symptoms, and indeed only 3% of subjects reported a past history of ulcer disease. Furthermore, adjusting for a history of peptic ulcer disease did not significantly alter our results.
Digestive Diseases and Sciences, Vol. 39, No. 5 (May 1994) 1095
HOLTMANN ET AL
The etiology of functional dyspepsia is largely unknown and there is ongoing debate about the underlying pathophysiology. One possible patho- genic mechanism is mucosal inflammation. There is convincing evidence that infection with 1"1. pylori is the commonest cause of chronic nonspecific gastri- tis, and it is strongly linked to the pathophysiology of chronic duodenal ulceration (17, 53). Earlier studies have reported that H. pylori infection was more frequent in patients with functional dyspepsia than in asymptomatic healthy controls, so it has been suggested that infection with H. pylori might be a cause of functional dyspepsia (54-56). Shall- cross et al, for example, found that 1-1. pylori infec- tion was significantly more common in dyspeptic patients below the age of 30 and between 40 and 49 years of age compared to healthy blood donors (54), but patients and controls in this study probably came from different socioeconomic groups, which could account for the findings. Our results suggest that H. pylori is not an important risk factor for dyspepsia in the community.
Functional dyspepsia is probably a heteroge- neous disorder and therefore H. pylori infection might be a causal factor only in a subgroup of patients, but previous studies have yielded conflict- ing results. Thus, Marshall and Warren showed an association between H. pylori and burping (17), while other studies have found an association of H. pylori with postprandial bloating (19), regurgitation, or epigastric pain or burning (18). In contrast, sev- eral studies could not find any specific symptom that was associated with H. pylori infection in out- patients (13, 15, 20, 22-24). In the present study of a nonpatient population, we could not detect an association between any individual symptoms and H. pylori. While it has been argued that there might be a defined pattern of symptoms that is due to H. pylori (28, 29), our results demonstrate that neither the pattern of symptoms nor individual symptoms are associated with H. pylori infection. In particu- lar, our hypothesis that ulcer-like pain would be linked to H. pylori was not substantiated.
Some randomized placebo-controlled trials with bismuth and antibiotics have shown a reduction of symptoms following active treatment, with clear- ance of 1-1. pylori and histological improvement be- ing associated with a significant decrease in symp- toms (57, 58). However , the methodological limitations of these studies have been considerable (59). Indeed, improvement of symptoms was ob- served even in patients without 1-1. pylori infection
before treatment and in patients in whom suppres- sion of H. pylori was not successful (60-62), while other trials have not been able to demonstrate any significant symptom improvement (~i3, 64). Simi- larly, eradication of H. pylori was not associated with improvement of symptoms immediately after completion of therapy in patients with functional dyspepsia (64). Thus, any beneficial effect of an- ti-H. pylori therapy may be independent of the suppression or eradication of H. pylori.
We did find a significant association between the intake of analgesics (aspirin but not other sub- stances) and dyspepsia. Aspirin has been linked to dyspepsia in controlled trials where large doses have been taken (65). The majority of subjects in this study had a consumption of less than 1 g of aspirin per week, but this small dose of aspirin was still associated with dyspepsia, even adjusting for possible confounders such as headache, back pain, and stiffness. We believe that the reporting of med- ication usage by our study subjects is likely to be accurate. Government regulations in Germany de- mand that blood donors do not take any medication 14 days prior to blood donation. All subjects who volunteer to give a blood donation have to sign a document stating that they have complied with this regulation. In addition, random drug screening is performed to help enforce this regulation. While our data may suggest that even low doses of aspirin can be associated with dyspepsia, how many of our cases had (undiagnosed) peptic ulcer disease from aspirin use that could explain this finding is un- known. Moreover, subjects with dyspeptic symp- toms might have taken aspirin to self-treat their abdominal pain or nongastrointestinal complains. Thus there are at least three potential explanations for the association between dyspepsia and the con- sumption of aspirin: (1) low dose aspirin causes dyspepsia (eg, by causing ulceration), (2) a disorder (eg, headache) is linked to both dyspepsia and as- pirin ingestion, or (3) aspirin is taken to try to relieve dyspepsia. The association between low- dose consumption of aspirin and dyspepsia needs further investigation.
In conclusion, there does not appear to be an association between H. pylori and dyspeptic symp- toms or dyspepsia subgroups in subjects from the community who attend for blood donation. Our results suggest that H. pylori is unlikely to be im- portant in the pathophysiology of dyspepsia.
1096 Digestive Diseases and Sciences, VoL 39, No. 5 (May 1994)
DYSPEPSIA AND H. pylori
A C K N O W L E D G M E N T S
The skillful assistance of Ms. J. Hiiber and Ms. S. Garthmann is greatly appreciated. The authors thank Ms. H. Lax, Department of Medical Statistics, Universi ty of Essen, for assistance with the statistical analyses and J. Bartel, MD, Praxis fiir Labormedizin, Heidelberg, for measuring H. pylori antibodies. The authors are indebted to staff, technicians, and nurses of the department of transfusion medicine for their support .
R E F E R E N C E S
1. Tibblin G: Introduction to the epidemiology of dyspepsia. Stand J Gastroenterot Suppl 109:29-33, 1985
2. Jones RH, Lydeard S: Prevalence of symptoms of dyspepsia in the community. Br Med J 298:30-32, 1989
3. Thompson WG, Heaton KW: Functional bowel disorders in apparently healthy people. Gastroenterology 79:283-288, 1980
4. Talley N J, Zinsmeister AR, Schleck CD, Melton I~: Dys- pepsia and dyspepsia subgroups: A population-based study. Gastroenterology 102:1259-1268, 1992
5. Talley NJ, Phillips SF: Non-ulcer dyspepsia: Potential causes and pathophysiology. Ann Intern Med 108:865-879, 1988
6. Holtmann G, Goebell H: Ursachen der funktionellen Dys- pepsie. Dtsch Med Wochenschr 117:1029-1034, 1992
7. Talley NJ: Chronic (non-specific) gastritis. Dig Dis Sci 347:61-75, 1989
8. Morris A, Nicholson G: Ingestion of campylobacter pylori- dis causing gastritis and raised fasting pH. Am J Gastroen- terol 82:192-199, 1987
9. Blaser MJ: Hypotheses on the pathogeneses and natural history of Helicobacter pylori-induced inflammation. Gas- troenterology 102:720-727, 1992
10. Dooley CP, Cohen H, Fitzgibbons P, Bauer M, Appleman MD, Perez-Perez G J, Blaser MJ: Prevalence of Helicobacter pylori and histologic gastritis in asymptomatic persons. N Engl J Med 321:1562-1566, 1989
11. Blaser M J: Gastric Campylobacter-tike organisms, gastritis, and peptic ulcer disease. Gastroenterology 93:371-383, 1987
12. Andersen LP, Elsborg L, Justesen T: Campylobacterpylori in peptic ulcer disease. III. Symptoms and paraclinical and epidemiologic findings. Scand J Gastroenterol 23:347-350, 1988
13. B6rsch G, Schmidt G, Wegener M, Sandmann M, Adamek R, Leverkus F, Reitemeyer E: Campylobacterpylori: Pro- spective analysis of clinical and histological factors associ- ated with colonization of the upper gastrointestinal tract. Eur J Clin Invest 18:133-138, 1988
14. Collins JS, Knill-Jones RP, Sloan JM, Watt PCH, Hamilton PW, Crean GP, Love AHG: Comparison of symptoms be- tween non-ulcer dyspepsia patients positive and negative for C. pylori using a single bias computer system for history taking. Klin Wochenschr 67(suppl 18):11-12, 1989
15. Guerre J, Berthe Y, Chaussade S, Merite F, Gaudric M, Tulliez M, Deslignieres S, Zone A: Has Campylobacter pylori gastritis a specific clinical symptomatology. Klin Wochenschr 67(suppl 18):25-26, 1989
16. Loffeld RJ, Potters HV, Arends JW, Stobberingh E, Flen- drig JA, van Spreeuwel JP: Campylobacter associated gas-
tritis in patients with non-ulcer dyspepsia. J Clin Pathol 41:85-88, 1988
17. Marshall BJ, Warren JR: Unidentified curved bacilli in the stomach of patients with gastritis and peptic ulceration. Lancet 1:1311-1315, 1984
18. Rathbone BJ, Wyatt J, Heatley RV: Symptomatology in C. pylori positive and negative nonulcer dyspepsia, Gut 29:A1473, 1988
19. Rokkas T, Pursey C, Uzoechina E, Dorrington L, Simmons NA, Filipe MI, Sladen GE: Campylobacterpylori and non- ulcer dyspepsia. Am J Gastroenterol 82:1149-1152, 1987 Sobala GM, Dixon MF, Axon ATR: H. pylon is not associ- ated with a distinct dyspeptic syndrome. Gut 30:A733, 1989 Landini MP, Varoli O, Tucci A, Paparo GF, Corinaldesi R, Zoccoli G, Lalli AA, La Plata M: Antibodies to Campylo- bacterpylori in patients with idiopathic dyspepsia. Microbi- ologica 12:181-188, 1989
22. Collins JS, Knill Jones RP, Sloan JM, Hamilton PW, Watt PC, Crean GP, Love AH: A comparison of symptoms be- tween non-ulcer dyspepsia patients positive and negative for Helicobacterpytori. Ulster Med J 60:21-27, 1991
23. Goh KL, Parasakthi N, Peh SC, Wong NW, Lo YL, Puthu- cheary SD: Helicobacterpylori infection and non-ulcer dys- pepsia: The effect of treatment with colloidal bismuth sub- citrate. Stand J Gastroenterol 26:1123-1131, 1991
24. Strauss RM, Wang TC, Kelsey PB, Campton CC, Ferraro MT, Perez-Perez G, Blaser M J: Association of Helicobacter pylori infection with dyspeptic symptoms in patients under- going gastroduodenoscopy. Am J Med 89:464-469, 1990
25. Talley NJ, Phillips SF, Bruce B, Twomey CK, Zinsmeister AR, Melton I~ III: Relation among personality and symp- toms on nonulcer dyspepsia and the irritable bowel syn- drome. Gastroenterology 99:327-333, 1990
26. Whitehead WE, Bosmajian L, Zorderman AB, Costa PT, Schuster MM: Symptoms of psychologic distress associated with irritable bowel syndrome. Comparison of community and medical clinic samples. Gastroenterology 95:709-714, 1988
27. Sitas F, Forman D, Yarnell JWG, Burr ML, Elwood PC, Pedley S, Marks KJ: Helicobacterpylori rates in relation to age and social class in a population of Welsh men. Gut 32:25-28, 1991
28. Colin-Jones DG, Bloom B, Bodemar G, Crean G, Freston J, Gigler R, Malagelada J, Nyr6n O, Petersen H, Piper D: Management of dyspepsia: report of a working party. Lancet 1:576-579, 1988
29. Talley NJ, Colin-Jones D, Koch KL, Koch M, Nyr6n O, Stanghellini V: Functional dyspepsia: A classification with guidelines for diagnosis and management. Gastroenterol Int 4:145-160, 1991
30. Petersen WL: Helicobacterpylori and peptic ulcer disease. N Engl J Med 324:1043-1048, 1991
31. Blaser MJ, Duncan DJ: Human serum antibody response to Campylobacter jejuni infection as measured in an enzyme linked immunoabsorbent assay. Infect Immun 33:292-298, 1984
32. Talley N J, Newell DG, Ormand JE, Carpenter HA, Wilson WR, Zinsmeister AR, Perez-Perez GI, Blaser M J: Serodiag- nosis of Helicobacterpyloti: Comparison of enzyme-linked immunosorbent assay. J Clin Microbiol 29:1635-1639, 1991
33. Talley N J, Phillips SF, Melton J, Wiltgen C, Zinsmeister
20.
21.
Digestive Diseases and Sciences, Vol. 39, No. 5 (May 1994) 1097
HOLTMANN ET AL
AR: A patient questionnaire to identify bowel disease. Ann Intern Med 111:671-674, 1989
34. Koran LM: The reliability of clinical methods, data and judgments. N Engl J Med 293:642-646, 1975
35. Drossman DA, Thompson WG, Talley NJ, Funch-Jensen P, Janssens J, Whitehead WE: Identification of subgroups of functional gastrointestinal disorders. Gastroenterology 3:159-172, 1990
36. Talley N J, Piper DW: Comparison of the clinical features and illness behaviour of patients presenting with dyspepsia of unknown cause (essential dyspepsia) and organic disease. Aust NZ J Med 16:352-359, 1986
37. Fleiss JL: Statistical Methods for Rates and Proportions. New York, Wiley, 1981, pp 29-30
38. Gardner M, Altman DG: Calculating confidence intervals for proportions and their differences. In Statistics with Confi- dence-Confidence Intervals and Statistical Guidelines. Gardner M, Altman DG (eds). London, 1991, pp 28-33
39. Atkinson AC: A note on the generalized information crite- rion for choice of a model. Biomet 67:413-418, 1980
40. SAS Institute Inc. SAS/STAT User's Guide, Release 6.03. Cary, North Carolina, SAS Institute, 1988
41. Banke L: Ulcumygdommers epidemiologi. Kobenhavn, F.A.D.L.'s Forlag, 1975
42. Hollnagel H, Norrelund N, Larsen S: Marve-tarmsymp- tomer blandt 40-arige i Glostrup: En epidemiologisk under- sogelse. Ugeskr Laeg 1982;144:267-273
43. Johnsen R, Straume B, Forde OH: Peptic ulcer and non- ulcer dyspepsia--a disease and a disorder. Scand J Prim Health Care 6:239-243, 1988
44. Harrison JD, Morris DL: Dyspepsia in coalminers and the general population: A comparative study. Br J Ind Med 46:428-429, 1989
45. Holcombe C, Omotara BA, Padonu MK, Bassi AP: The prevalence of symptoms of dyspepsia in north eastern Nige- ria. A random community based survey. Trop Geogr Med 43:209-214, 1991
46. Ahmed N, Malur PR, Sankapal MN, Nagalotimath S J: Prev- alence of Carnpylobacterpylori in non-ulcerative dyspepsia. Indian J Pathol Microbiol 34:247-252, 1991
47. Metcalf R, Youngs GR: Prevalence of symptoms of dyspep- sia. BMJ 298:526-527, 1989
48. Jones R, Lydeard S: Prevalence of symptoms of dyspepsia in the community. BMJ 298:30-32, 1989
49. Weir RD, Backett EM: Studies of the epidemiology of peptic ulcer in a rural community: Prevalence and natural history of dyspepsia and peptic ulcer. Gut 9:75-83, 1968
50. Bernersen B, Johnsen R, Bostad L, Straume B, Sommer AI, Burhol PG: Is Heticobacterpylori the cause of dyspepsia? BMJ 304:1276-1279, 1992
51. Richter JE: Dyspepsia: Organic causes and differential char- acteristics from functional dyspepsia. Scand J Gastroenterol Suppl 182:11-16, 1991
52. Klauser AG, Voderholzer WA, Knesewitsch PA, Schindel- beck NE, Mtiller-Lissner SA: What is behind dyspepsia. Gastroenterology 100:A458, 1991
53. Blum AL, Armstrong D, Damman H, Fischer M, Greiner L, Haase W, Hogeboom-Verdegal A, Liszkay M, Stolte M, Sulser H, Simon B, Talicomp Study Group: The effect of Helicobacter pylori on the healing and relapse of duodenal ulcer. Gastroenterology 98:A22, 1990
54. Shallcross TMJ, Rathbone BJ, Heatley RV: Campylobacter pylori and non-ulcer dyspepsia. In Campylobacterpylori and Gastroduodenal Disease. Rathbone R J, Heatly RV (eds). Oxford, Blackwell Scientific, 1989, pp 155-166
55. Pettross CW, Appleman MD, Cohen H, Valenzuela JE, Chandrasoma P, Laine LA: Prevalence of Campylobacter pylori and association with antral mucosal histology in sub- jects with and without gastrointestinal symptoms. Dig Dis Sci 33:649-653, 1988
56. Rauws EA, Langenberg W, Houthoff HJ, Zanen HC, Tytgat GN: Campylobacter pyloridis-associated chronic active an- tral gastritis. A prospective study of its prevalence and the effects of antibacterial and antiulcer treatment. Gastroenter- ology 94:33-40, 1988
57. Lambert JR, Dunn K, Borromeo M, Korman MG, Hansky J: Campylobacterpylon---a role in non-ulcer dyspepsia? Scand J Gastroenterol Suppl 160:7-13, 1989
58. Glupczynski Y, Burette A, Labbe M, Deprez C, De Reuck M, Deltenre M: Campylobacterpylori-associated gastritis: A double-blind placebo-controlled trial with amoxycillin. Am J Gastroenterol 83:365-372, 1988
59. Talley NJ: Drug treatment of functional dyspepsia. Scand J Gastroenterot Suppl 182:47-60, 1991
60. Vaira D, Holton J, Aintey C, Falzon M, Osborn J, D'Anna L, Romanos A, Chandrakumaran K, McNeil I: Double blind trial of colloidal bismuth subcitrate versus placebo in Heli- cobacter pylori positive patients with non-ulcer dyspepsia. Ital J Gastroenterol 24:400-404, 1992
61. Rokkas T, Pursey C, Uzoechina E, Dorrington L, Simmons NA, Filipe MI, Sladen GE: Non-ulcer dyspepsia and short term De-Nol therapy: A placebo controlled trial with partic- ular reference to the role of Campylobacter pylori. Gut 29:1386-1391, 1988
62. Dill S, Payne-James JJ, Misiewicz J J, Grimble GK, McSwig- gan D, Pathak K, Wood AJ, Scrimgeous CM, Rennie MJ: Evaluation of the 13C-urea breath test in the detection of Helicobacterpylori and in monitoring the effect of tripotas- sium dicitrobismuthate in non ulcer dyspepsia. Gut 31:1237- 1241, 1990
63. McNulty CA, Gearty JC, Crump B, Davis M, Donovan IA, Melikian V, Lister DM, Wise R: Campylobacter pyloridis and associated gastritis: investigator blind, placebo con- trolled trial of bismuth salicylate and erythromycin ethylsuc- cinate. Br Med J (Clin Res Ed) 293:645-649, 1986
64. Patchett S, Beattie S, Leen E, Keane C, O'Morain C: Eradicating Helicobacterpylori and symptoms of non-ulcer dyspepsia. BMJ 303:1238-1240, 1991
65. Steering Committee of the Physicians' Health Study Group: Final report on the aspirin component of the ongoing physi- cians' health study. N Engl J Med 321:129-135, 1989
1098 Digestive Diseases and Sciences, Vol. 39, No. 5 (May 1994)