draftof hartlepool - nth.nhs.uk · workforce – absence management, ensuring we have adequate...
TRANSCRIPT

Board of Directors Meeting
Thursday, 26 April 2018 at 1.00 pm
Boardroom
University Hospital of Hartlepool Draft
Glossary of Terms
Strategic Aims and Objectives
Strategic Aims
Putting Patients First – to create a patient centred organisational culture by engaging and enabling all staff to add value to the patient experience and demonstrated through patient safety, service quality and LEAN delivery.
Integrated Care Pathways – to develop and expand the portfolio of services to provide integrated care pathways for the people of Easington, Hartlepool, Sedgefield and Stockton providing equal access to acute care and care as close to home as possible in line with Momentum: Pathways to Healthcare.
Service Transformation – to improve and grow our healthcare services to continually review the needs of our healthcare community and transform services. In line with evidence based guidelines we will enhance quality, clinical effectiveness and patient experiences whilst improving clinical outcomes.
Manage our Relationships – to ensure our services, and the way we provide them, meet the needs of our patients, commissioners and other partners by proactively engaging with all appropriate stakeholders including our staff, through communications, engagement and partnership working.
Maintain Compliance and Performance – to maintain our performance and compliance with required standards and continually strive for excellence by good governance and operational effectiveness in all parts of our business.
Health and Wellbeing – to embrace the health and well being of the population we serve and ensure that the health needs of the people of Easington, Hartlepool, Sedgefield and Stockton are reflected and catered for in the commissioning of services from the Trust.
Strategic Objectives Maintain Compliance and Performance – assurance around compliance with standards, performance indicators and requirements within the Terms of Authorisation. Requirement to provide Board regulation and self certification on a quarterly and annual basis in accordance with Monitors Terms of Authorisation. Seasonal Pressures – requirement to ensure preparedness for seasonal winter pressures. Reduce Hospital Acquired Infections – supports the Trust’s key strategic theme of; Maintain Compliance and Performance with required standards and continually strive for excellence by good governance and operational effectiveness in all parts of the Trust business. Effective Board Governance – corporate oversight and scrutiny will continue to be provided by key management structures; 1. Board of Directors, 2. Executive Team, 3. Trust Directors Group. Training – ensuring the workforce is appropriately trained.
Draft
Workforce – absence management, ensuring we have adequate staffing levels that provide safe and effective care to our patients. Momentum – Pathways to Healthcare – delivery of a new healthcare system for the people of Easington, Hartlepool, Sedgefield and Stockton. Putting Patients First / Patient Safety – to create a patient-centred organisation by engaging and enabling staff to add value to the patient experience, demonstrated through patient safety, service quality and LEAN delivery. Finance – to maintain our performance and compliance with required standards and continually strive for excellence by good governance and operational effectiveness in all parts of our business.
Draft
PG/SH 19 April 2018 Dear Colleague A meeting of the Board of Directors will be held on Thursday, 26 April 2018 at 1:00 pm in the Boardroom, University Hospital of Hartlepool. Yours sincerely
Paul Garvin Chairman
Agenda
Led by
1. (1.00pm) Apologies for absence Chairman 2. (1.00pm) Declaration of Interest Chairman 3. (1.00pm) Minutes of the meeting held on, 29 March 2018 (enclosed) Chairman 4. (1.05pm) Matters Arising Chairman Items for Information 5. (1.10pm) Chairman’s Report (verbal) Chairman 6. (1.20pm) Chief Executive’s Report (enclosed) J Gillon 7. (1.30pm) Retrospective Approval of Documents Executed Under Seal J Gillon (enclosed) Quality 8. (1.30pm) Safety, Quality and Infection Prevention Report (enclosed) J Lane
Draft

Strategic Management 9. (1.40pm) Project Management and Improvement Office Update (enclosed) J Gillon 10. (1.50pm) Capital Programme Performance 2017/18 (enclosed) R Toole Performance Management 11. (2.00pm) Compliance and Performance Report (enclosed) L Taylor 12. (2.10pm) Finance and Contract Performance Report, R Toole as at 31 March 2018 (enclosed) 13. (2.20pm) Draft Revenue and Capital Budgets 2018/19 (enclosed) R Toole 14. (2.30pm) Carter Efficiency Metrics Update (verbal) L Taylor 15. (2.40pm) Integrated Compliance and Performance – L Taylor, Year-end report 2017/18 (enclosed) J Lane & A Sheppard
16. (2.50pm) NHS National Staff Survey Results 2017 (enclosed) A Sheppard Governance 17. (3.00pm) Learning from Deaths (enclosed) D Dwarakanath 18. (3.10pm) Any Other Notified Business Chairman Cyber Security Assessment Update (verbal) G Evans 19. Date of Next Meeting (Thursday, 24 May 2018, Boardroom, University Hospital of North Tees)
Draft
____________________ * voting member
North Tees and Hartlepool NHS Foundation Trust
Minutes of a meeting of the Board of Directors held on Thursday, 29 March 2018 at 1.00pm
at the University Hospital of North Tees Present: Paul Garvin, Chairman* Chairman Brian Dinsdale, Non-Executive Director* BD Rita Taylor, Non-Executive Director* RT Steve Hall, Non-Executive Director* SH Jonathan Erskine, Non-Executive Director* JE Kevin Robinson, Non-Executive Director* KR Julie Gillon, Chief Executive* CE Kevin Scollay, Deputy Director of Finance* DDoF Jane Metcalf, Deputy Medical Director* DMD Alan Sheppard, Director of Workforce DoW Julie Lane, Director of Nursing, Patient Safety and Quality* DoN,PS&Q Graham Evans, Chief Information and Technology Officer CI&TO Julie Parkes, Director of Operations DoO Lynne Taylor, Director of Performance and Planning DoP&P Barbara Bright, Company Secretary CS In attendance: Sarah Hutt, Assistant Company Secretary Bill Johnson, Hospital User Group Representative (HUG) John Edwards, Elected Governor for Stockton Eunice Huntington, Appointed Governor, Durham County Council BoD/3628 Apologies for Absence Apologies for Absence were reported from Deepak Dwarakanath, Medical Director and Robert Toole, Director of Finance. BoD/3629 Minutes of the meeting held on Thursday, 25 January 2018
Resolved: that, the minutes of the meeting held on Thursday, 25 January 2018 be confirmed as an accurate record.
BoD/3630 Declaration of Interests There were no declarations of interest on open agenda items. BoD/3631 Matters Arising There were no matters arising. BoD/3632 Chairman’s Report
a. Appointments The Chairman reported that since the last meeting Neil Atkinson had been appointed as the new Director of Finance. A start date was yet to be finalised.
Draft
2
b. Committee in Common
The Chairman reported that the Committee in Common had met on 19 February 2018. A blueprint document in respect of governance arrangements was being developed by the CE to be shared with the three trusts. Chairmanship of the Committee had transferred to Alan Downey, the newly appointed Chairman at South Tees Hospitals NHS Foundation Trust for 12 months.
c. Care Quality Commission Well-Led Visit
The Chairman placed on record his thanks to all members of staff for their efforts during the recent Care Quality Commission (CQC) inspection. The Trust had been rated as ‘Good’, which was an excellent achievement.
d. NHS Provider Chairs Meeting The Chairman reported that he had attended the recent NHS Providers Chairs and Chief Executives Meeting in London. The event had included discussions in respect of Integrated Care Systems and proposals for the Sustainability and Transformation Partnerships (STPs) to operate under 3 tiers: local organisations; groups of organisations and the wider STP system, or Integrated Care Systems as they would be known going forward.
e. Financial climate The Chairman reported that for the year ending 2017/18 nationally there was £778m of Sustainability and Transformation Funding unallocated; CCGs were £471m in deficit, and the provider sector was £1.28bn in deficit. Locally Hartlepool and Stockton-on-Tees (HAST) CCG was reporting a surplus of c.£8m. The average proposed cost reduction target for 2018/19 was 5.7%, and there were approximately 20% of trusts who had declared non-compliance against their individual control total, with another 29% undecided.
f. NHSI and NHS England The Chairman reported that there were proposals for increased joint working between NHS Improvement (NHSI) and NHS England (NHSE) to provide a more uniform platform to support the work of the Integrated Care Systems. The individual statutory entities would remain separate, however, there would be some areas of amalgamation and the regional structures would be revised accordingly.
Resolved: that, the information be noted.
BoD/3633 Chief Executive’s Report
a. Sustainability and Transformation Partnership (STPs) update
The CE provided an update in respect of the Sustainability and Transformation Partnership (STP) working. An oversight group had been established to deliver on the forward plan of the STP and to take forward governance arrangements. Capital bids submitted in respect of initiatives to support locality based services were being considered. A blue print of clinical services was being developed to ensure sustainable services for the future across the Tees Valley working in collaboration with the Trust, South Tees Hospitals NHS Foundation Trust and County Durham and Darlington NHS Foundation Trust, as part of the work of the Committee in Common. The CI&TO reported that a workshop had taken place recently to discuss the provision of
Draft
3
pathology services regionally, and that a bid was being put together to seek some pathology digital systems interoperability support. In addition, the CI&TO described aspects of the Global Digital Exemplar (GCE) programme which is continuing within the Trust.
b. Care Quality Commission
The CE reported that following an inspection by the Care Quality Commission (CQC) with both an unannounced inspection of services, and an announced Well Led inspection in November and December 2017 the Trust had been rated as ‘good’, which was an excellent achievement. Letters of congratulation had been received from HAST CCG and a number of Governors.
c. University of Sunderland School of Medicine
The CE reported that the University of Sunderland had been successful in its bid to open a new Medical School, one of five being opened nationally. The first cohort of students would be in September 2019, with the Trust offering 12 placements. The School would specialise in GP and Psychiatric training.
d. Kirkup Report
The CE reported that the Kirkup Report, which was published in February 2018 detailed the findings of an independent review following failings at Liverpool Community Health NHS Trust between 2010 and 2014. The conclusion noted that had there been earlier intervention avoidable harm that occurred to patients and staff across the Trust would have been reduced. In addition, the outcomes of an investigation by NHS Improvement regarding Wirral University Teaching Hospital NHS Foundation Trust had recently been published, following allegations by staff in respect of cultural, behavioural and governance issues. The Trust would review both reports and recommendations to understand any implications or impact for the future.
e. Fit and Proper Persons Test
The CE reported that the CQC had issued updated guidance in respect of the Fit and Proper Persons Test in January 2018. The guidance included a more detailed description of serious mismanagement and misconduct, and provided greater clarity regarding the obligations and responsibilities of those holding director roles. Following publication of the Kirkup Report a further review of the Fit and Proper Person test would be commissioned.
f. NTH Solutions The CE reported that on 1 March 2018 North Tees and Hartlepool Solutions LLP was formally launched, which was a wholly owned subsidiary of the Trust. The aim of the LLP was to reduce support service costs whilst providing sustainable, high quality and safe services. Staff from Estates and Facilities, and Procurement and Supplies transferred into the LLP with effect from the ‘go live’ date on 1 March.
g. Spring Statement
The CE reported that following the announcement of the Chancellor’s 2018 Spring Statement, no direct funding would be available for the NHS, however the Government was taking a balanced approach to reduce public sector debt whilst aiming to fund vital public services.
Draft
4
h. NHS 70th Celebrations
The CE reported on 5 July 2018 the NHS would be celebrating its 70th Anniversary. A wide range of celebrations were planned nationally, regionally and at individual organisations. The Trust was exploring a number of ideas and was approaching local companies regarding sponsorship to support the plans.
Resolved: that, the information be noted. BoD/3634 Retrospective Approval of Documents Executed Under Seal The CE requested retrospective approval for the sealing of the following documents:
Document Date Sealed By
Members Agreement relating to North Tees and Hartlepool Solutions LLP Between:
1) North Tees and Hartlepool NHS Foundation Trust 2) Northumbria Healthcare Facilities Management
And
3) North Tees and Hartlepool Solutions LLP
1 March 2018
Mr R Toole and Mr A Sheppard
Master Services Agreement Between:
1) North Tees and Hartlepool NHS Foundation Trust And 2) North Tees and Hartlepool Solutions LLP
1 March 2018
Mr R Toole and Mr A Sheppard
Resolved: that, the retrospective approval of the sealing of documents be
granted.
BoD/3635 Safety, Quality and Infection Prevention Report The DoN,PS&Q presented the Safety, Quality and Infection Prevention Report and drew members’ attention to the key points. There had been an increase in falls from 113 in January to 120 in February. The
increase was partly due to increased incident reporting following the Trust previously being noted as a low reporter. All falls were investigated and a full review had been undertaken in the areas of high incidence. There was no correlation in respect of staffing levels. New equipment continued to be piloted.
There had been a decrease in pressure ulcers from 28 in December to 26 in January, which were grade 2 and above. When benchmarked against April 2017 to January 2018 data, the Trust had experienced a total of 67 more pressure ulcers, 216 (April 2017 to January 2018) against 149 (April 2016 to January 2017). The increase was partly due to the increased acuity of patients and the introduction of the Safe Care Live
Draft
5
tool, providing real time data 3 times per day, which had assisted in the development of a benchmark. It was noted there had not been any increase in the deterioration of ulcers. A piece of work was being undertaken regionally regarding pressure ulcers and medical equipment.
The Trust had reported three cases of Clostridium Difficile (C-Diff) in January and two cases in February, taking the year to date total to 31, which exceeded the annual trajectory of 13 cases. The trajectory for 2018/19 was 12 cases. Antibiotic prescribing for a cohort of patients both in and out of hospital had been reviewed. It was noted that the method of reporting would change with effect from 2019/20 and would include 4 categories of reporting. The Trust would shadow report from 2018/19 in preparation.
There was zero cases of Trust-attributable MRSA in January and one case in February which was non-avoidable, and a full root cause analysis had been completed; one case of Trust-attributable MSSA in January and two cases in February; five cases of Trust-attributable E.coli in January and one case in February; six cases of Klebsiella species bacteraemia in January and one case in February, and one case of Pseudomonas aeruginosa bacteraemia in January and zero cases in February. The Trust was working regionally with Public Health England to reduce the instances of MSSA and E.coli and was on track to achieve a 14% reduction.
The overall hand hygiene compliance score remained unchanged in January and February at 97%, exceeding the Trust’s internal target of 95%.
The Trust’s latest HSMR value was 101.32 (January 2017 to December 2017), from the rebased 100.04 (December 2016 to November 2017). The latest SHMI value was 108.01 (July 2016 to June 2017) from the previous reported value of 109.07 (June 2016 to May 2017). Both values remained within the ‘as expected’ range. A slight increase in the HSMR was expected following the increased winter pressures during December and January and an increase in deaths nationally. All cases had been reviewed and there were no care related deaths.
The Trust had received 96 complaints in January and 79 in February, of which 15 (15.62%) and 19 (18.98%) respectively were Stage 3 – request for a written response. The Trust’s response rate for Stage 3 complaints was 100% in December and 82% for January.
The registered nurse fill rate remained consistently above 80% for both day and night duty, with all areas adhering to the red rules. There had been no never events.
There were a total of 13 Staff, Patient Experience and Quality Standards (SPEQS) visits undertaken in February with an overall score of 92.75%, which was a reduction from 94.02% in January. The mechanism to provide feedback to the Governors partaking in the inspections was being reviewed. The collection of data would be via tablets going forward to allow the information to be recorded whilst on the visit.
The number of Friends and Family returns that ‘Would Recommend’ the Trust increased to 95.76% in February from 95.36% in January, and the number that ‘Wouldn’t Recommend’ decreased to 0.85% in February from 1.07% in January.
The Trust remained under significant pressure with bed occupancy reporting at 92.71% in February, and consistently above the recommended 85% month on month during 2017.
Following a planned Well Led review by the CQC between 19 and 21 December 2017 and an unannounced inspection of key services in November as part of a new inspection regime the Trust was rated as ‘good’ across all five domains, which was an excellent result.
KR, Chair of the Infection Control Committee sought to understand the peaks in trust attributed C-Diff infections that were often seen during quarter 4, and sought clarity regarding the reduced trajectory for 2018/19. The DoN,PS&Q explained that peaks in infections during quarter 4 was likely due to high levels of activity in the organisation
Draft
6
preventing the full decant programme to be carried out. The annual trajectory was set nationally without provider involvement. RT, Chair of the Patient Safety and Quality Standards Committee welcomed the announcement that more training placements were to be made available to midwives, however, sought to understand how this would be possible with the number of births currently at the Trust. The DoN,PS&Q explained that the Trust was considering alternative ways to offer training for students, and was looking to increase its market share of births.
Resolved: (i) that, the content of the report be noted; and (ii) that, the work in relation to pressure ulcers and patient falls be noted;
and (iii) that, the work in relation to Clostridium Difficile be noted.
BoD/3636 Care Quality Commission Update The DoN,PS&Q reported that the Trust had been rated as ‘good’ following the Care Quality Commission’s ‘well-led’ review between 19-21 December and the unannounced inspection of key services in November. Outstanding practice was identified in Maternity Services in relation to training, and in the Emergency Department with staff going the extra mile for patients and families in their delivery of care and support. A number of areas for improvement were identified which included mandatory training compliance, maternity staffing and improvement to be noted in the Royal College of Emergency Medicine Audits. The final report was published on 14 March, and the improvement plan was being developed in readiness for submission by mid-April. There were two ‘must do’ areas which included the compliance of audits, and mental health assessments. In addition there were 11 ‘should do’ items. Quarterly engagement sessions at the Trust would re-commence to monitor progress against the Trust’s action plan.
Resolved: (i) that, the content of the report be noted; and (ii) that, the outcome rating of ‘good’ following the inspection be noted; and (iii) that, the areas of ‘outstanding’ practice in Maternity Service and the
Emergency Department be noted. BoD/3637 Trust Strategy Development – Progress Report The DoP&P provide an update regarding strategy development including the Annual Planning Business Cycle, the Clinical Services Strategy (CSS), the Corporate Strategy and the Delivering Productivity Programme (DPP). As part of future proofing healthcare provision a programme of ‘deep dive’ scrutiny sessions for current clinical services continued using the categorisation of Core, Outer Core and Vulnerable, to review potential re-design options and future viability including being reviewed by the Project Management Improvement Office (PMIO) structure. The Corporate Strategy continued to provide a strategic focus for the organisation and following a programme of engagement events had been embraced by staff at all levels with the four strategic objectives remaining widely visible across the Trust: Putting Patients First; Valuing our People; Health and Wellbeing, and Transforming our Services. There were currently eight work streams as part of the DPP, identifying areas for greater efficiency and productivity. The Trust’s Annual Business Planning Cycle which helped to shape the Trust’s Annual Operating Plan was now complete. The draft revised Annual Operating Plan was submitted on 8 March, with final version due for submission on 30 April.
Draft
7
Resolved: (i) that, the content of the report be noted; and (ii) that, the on-going work in respect of the Clinical Services Strategy and
the future viability of services be noted; and (iii) that, the progress to date with the Delivering Productivity Programme be
noted; and (iv) that, the positive influence of the Corporate Strategy on culture and
leadership throughout the Trust be noted; and (v) that, the progress to date of the Annual Operating Plan be noted.
BoD/3638 Senior Information Risk Owner (SIRO) Update The CI&TO provided an end of year update for 2017/18 as Senior Information Risk Owner (SIRO). In preparation for the new General Data Protection Regulations (GDPR) which commence on 25 May 2018 the Trust’s Information Governance policies were being reviewed to ensure they were compliant. Data protection was an element included in the new Care Quality Commission (CQC) inspection regime. To determine compliance with Information Governance (IG) requirements, three elements were measured: IG Training; Subject Access Requests, and IG Toolkit compliance. The Trust was forecasting compliance against the 95% threshold at year end for IG Training following a challenging year with the transfer of mandatory training onto the My ESR system. Subject Access Requests were completed, 97.5% within the required 40 day period, and the IG Toolkit compliance exceeded the 80% target. The overall number of IG risks was slightly reduced with 25 open risks compared to the previous year. All risks were reviewed, themed and where required corrective actions agreed. Risks were rated in 4 categories: high, moderate, low and very low. There was currently only one risk rated as high, which was in relation to staff data protection training compliance levels. This would be resolved by 31 March 2018. BD, Chair of the Audit Committee sought assurance regarding risk to the organisation in relation to the 20% non-compliance against the IG Toolkit. The CI&TO explained that it was not possible to eradicate all risk when dealing with people and paper records as elements of human error do occur, however, the number of incidents level 2 and above had greatly reduced from 13 in 2014/15, two in 2015/16 and one during 2017/18. The Chairman sought clarity regarding the Trust’s position in relation to Data Harvesting. The CI&TO confirmed that the Trust does not transfer such data off site and the database storing information is held on site. The CI&TO reported that in 2014 the Trust was ranked 121st nationally in respect of the Digital Maturity Index, however, the report for 2017 ranked the Trust as joint 1st, which was an excellent achievement. JE, Non-Executive Director enquired what the potential cost to the organisation would be in respect of patients being able to access medical records free of charge under the new GDPR rules. The CI&TO explained that it would place a large burden on the organisation, as currently only a small team manages the subject access request process and going forward requests of this nature require clinical oversight and turnaround times would be reduced. Organisations would be fined should breaches occur.
Resolved: (i) that, the content of the report be noted; and (ii) that, the current position in respect of Information Governance
compliance be noted; and (iii) that, the Trust’s Digital Maturing joint first position for 2017 be noted.
Draft
8
BoD/3639 Compliance and Performance Report The DoP&P presented the Compliance and Performance Report for the month of February against indicators from the Single Oversight Framework and foundation trust licence conditions. The Corporate Dashboard and reporting framework was reflective of both the mandatory performance frameworks for 2017/18 and additional internal reporting requirements, including the Lord Carter Model Hospital Review. The Trust achieved 97.63% for the four hour emergency care standard against 95%
target. This placed the Trust in first position nationally which was an excellent result. Overall A&E activity had increased by 84.2% and admissions had increased by 29.2%
compared to the same period the previous year. Overall Emergency activity saw a decrease of 9.34% compared to the same period the
previous year, which included 782 patients treated via Ambulatory Care, equating to 24.55% of the total emergency admissions.
Type 1 attendances to A&E reduced by 35.9% compared to the same period the previous year, with minor patients streamed to the Integrated Urgent Care Centre following its opening on 1 April 2017.
On aggregate there were 8,710 attendances to the Integrated Urgent Care Centres and 626 admissions, with 4,772 admissions and 351 admissions at the University Hospital of North Tees and 3,938 attendances, 275 admissions at the University Hospital of Hartlepool.
The Trust achieved 92.01% against the 92% for RTT standard with no over 52 weeks waits reported. An impact on performance was anticipated following planned reductions in elective activity during December and January and subsequent additional cancellations to absorb emergency pressures.
Occupancy levels remained high reporting at 92.71% despite the daily opening of resilience beds to a maximum peak of 48 to absorb the increased admissions. Occupancy levels consistently remained above the recommended 85% during the past two years, reflecting the system wide pressure. Delayed transfers of care (DTOC) reported at 2.31% which was an improved position on previous months and the lowest position year to date.
The Trust achieved against all the cancer standards in January (latest validated position), with exception of the 31 Day Subsequent Treatment reporting at 88.24% against the 94% target. The Trust achieved 90.70% against the 85% target for the 62 Day Referral to Treatment standard; nationally the average was 81%. Despite January’s position, there were still significant challenges to achieve the standard in part due to complex pathways and patient choice. The provisional position for February reported below the 85% standard, currently reporting below 80%, however the quarter position was expected to be improved. Work continued to improve pathway management.
Non-medical cancelled operations reported at 1.45% in February against the target of 0.80% as a result of elective procedures being cancelled due to continued seasonal pressures. No urgent procedures had been cancelled for a second time, all procedures had been re-scheduled.
The Trust continued to keep ambulance handover delays to a minimum despite the significant pressure on emergency care services with handover delays greater than 30 minutes reporting at 20, and delays greater than 60 minutes reporting at one case. In comparison the North East average handover greater than 30 minutes reported at 120 (range 48 – 301), the average handover greater than 60 minutes reporting at 15 (range 0 – 72). The Trust’s overall performance in February indicated 60.72% of ambulance handovers less than 15 minutes.
Focused work continued in respect of DNA rates and readmissions.
Draft

9
Operational efficiencies continued to be explored with the Delivering Productivity Programme (DPP), which was currently focusing on eight individual work streams.
KR, Chair of Infection Control Committee sought clarity regarding the Trust’s average waits in respect of the 18 week RTT target. The DoP&P reported that 75% of patients who had been cancelled were seen within 6-8 weeks, and only 11 patients out of the 139 total cancelled patients waited over 10 weeks for their operation to be reappointed. RT, Chair of Patient Safety and Quality Standards Committee sought assurance regarding what action was taken in relation to Stranded patients. The D&PP explained that Stranded patients were patients with lengths of stay greater than 7 days, and in addition there were Super stranded patients which were patients with lengths of stay over 21 days. Work continued to identify alternative pathways sooner where possible and the identification of patients who although not completely medically fit no longer required to be in an acute setting. It was noted that the majority of these patients were frail and elderly with complex care needs, and 15% of super stranded patients were aged over 90. It was noted that the Frailty work being undertaken front of house was having a positive impact on lengths of stay for patients including admission avoidance in some cases. BD, Chair of the Audit Committee sought clarity regarding the Trust’s A&E Time to initial Assessment for Ambulance handovers data. The DoP&P explained that the target represented the 95th upper centile. The average figure was much lower and placed in context the Trust’s performance against the standard. The Chairman expressed concern regarding the low theatre utilisation data in comparison to the high level of readmissions for both elective and non-elective patients, and requested a piece of work be undertaken with the findings to be reported to the Patient Safety and Quality Standards (PS and QS) Committee. SH, member of the PS and QS Committee reported that information regarding the delay of re-appointed patients was also being looked into at the request of the Committee.
Resolved: (i) that, the Corporate Dashboard and performance against the Single Oversight Framework and key national indicators be noted; and
(ii) that, the on-going operational performance and system risks be noted; and
(iii) that, the national position of first for the 4 hour emergency care standard in February be noted; and
(iv) that, the February position in respect of the 62 day referral to treatment cancer standard be noted;
(v) that, a piece of work in respect of theatre utilisation rates v readmission rates be reported to the Patient Safety and Quality Standards Committee.
BoD/3640 Financial Performance Report as at 28 February 2018 The DDoF presented the Financial Performance Report as at 28 February 2018, drawing members’ attention to the key highlights. The Trust had a Use of Resources (UoR) rating of 3. The Trust was reporting an in month deficit of £(0.539)m, which was £0.553m ahead of
plan, year to date there was a reported deficit of £(19.858)m, which was £(10.392)m behind plan. This position assumes non achievement of planned Sustainability and Transformation Funding (STF) income.
Draft
10
Income excluding STF was £24,704m, which was £1.336m ahead of plan, and year to date income was adverse by £3.871m largely due to reduced activity levels and increased readmission rates.
Pay expenditure was £0.192m ahead of plan in month, and £0.759m ahead of plan year to date. Agency expenditure for the year totalled £3.6m, and bank expenditure £3.9m. The expenditure was largely offset by significant underspends on substantive Nursing and Midwifery staff.
Non-pay expenditure was £1.052m adverse in month, and year to date £7.798m. The continued overspend on non-pay relates to undelivered CRT.
STF income was adverse by £(6.1)m. As the year to date financial target had not been met, no STF income was assumed to have been achieved.
Capital spend year to date was £11.3m with a further £3.5m committed against a forecast of £2.9m, therefore £0.6m would be carried forward to 2018/19. There would be underspend against plan due to delays with the Energy Centre project.
The cash balance at month 11 was £11.1m, a slight variation from plan which was being monitored closely.
BD, Chair of the Finance Committee commended the improvement in the run rate and substantial reduction in both agency and temporary staffing spend which contributed positively to pay expenditure. The area of focus needed to be non-pay expenditure.
Resolved: that, the financial position at Month 11 be noted. BoD/3641 Lord Carter Procurement Targets Update The DDoF provided an update in respect of progress against the Lord Carter operational performance and productivity metrics in relation to Procurement. In January 2017 a new tool was launched: the Purchase Price Index and Benchmarking Tool (PBIB Tool). NHS Improvement introduced targets for trusts to attain to. Trust related data from the PBIB was recently published, which cited the Trust as being one of eight organisations that weren’t compliant. The data was historic from December 2016. The Trust’s actual position showed the Trust was fully compliant for one of the metrics and marginally compliant (within 10%) for the two remaining metrics with targets. Although significant progress had been made during the last 12 months, work continued to ensure the Trust’s processes increasingly reflect the national methodology.
Resolved: that, the content of the report be noted.
BoD/3642 Workforce Report – Quarter 3: 2017/18 The DoW presented the Workforce Report – Quarter 3: 2017/18 and drew members’ attention to the key points. The sickness absence rate was 4.99%, an increase of 0.65% when compared to
Quarter 2, and the un-validated position showed an increase to 5.67% in January. The long term sickness absence rate for Quarter 3 showed an increase of 0.08% when compared to the same period the previous year. There were targeted interventions being undertaken in relation to sickness absence, and cultural behaviours were being reviewed.
The cost of sickness absence for Quarter 3 was £1,773,799, which was £162,533 higher than in Quarter 2. The top three reasons for absence remained as stress, muscuo-skeletal, and gastrointestinal.
The turnover rate for Quarter 3 was 12.90% (foundation doctors included), which was higher than the previous quarter. The Trust headcount increased by 19 to 5,628 in
Draft
11
Quarter 3 when compared to the baseline at the end of March 2017. There were 300 new starters to the Trust compared to 251 in Quarter 2.
Due to the Regional Streamlining Project a number of mandatory training topics had altered frequency requirements, to bring regional organisations mandatory training in line with each other, which created a drop in compliance in some areas. The current RAG Report was also being reviewed to be in line with the My ESR system competencies, which would create a drop in compliance for a brief period during the transition from one system to another.
Appraisal compliance was 77% for Quarter 3 against a target of 95%, which was a concern. This remained an area of focus, and regular reminders were sent to directorates by the Education Delivery Team.
National guidance indicated that it was not appropriate for a Freedom to Speak up Guardian to be employed within Human Resources, and it was therefore no longer appropriate for the DoW to fulfil this role. Approval had been granted for internal expressions of interest to be invited to undertake the role, with a Job Description and Advert issued. The new incumbent would be supported by the Employee Relation function and would report to the DoN,PS&Q. This was an important role, highlighted by the outcome of the Wirral Report which cited failures in culture and behaviours as being a key issue, and staff not feeling able to raise concerns.
The Annual NHS Staff Survey 2017 was carried out during Quarter 3, and the response rate was 51% against a target of 60%, and the national average response rate was 43%. A breakdown of the response rates by directorate was provided.
BD, Chair of the Audit and Finance Committees expressed concern regarding the rising cost of sickness absence to the organisation, and sought some assurance as to actions being taken to improve the situation, prompting discussion. The DoW reported that an Executive Team development session was scheduled to review sickness absence. JE, Non-Executive Director sought to understand the wide variation between response rates to the staff survey and were there any trends. The DoW explained that there were some trends of low reporting, however, it was noted that often the staff survey was viewed as a corporate tool preventing staff from responding, methods of improving this were being explored to increase feedback in future surveys. The Chairman queried the inclusion of staff from North Tees and Hartlepool Solutions LLP following its launch on 1 March for future surveys. The DoW explained that reporting would need be separate rather than collective.
Resolved: (i) that, the content of the report be noted; and (ii) that, the on-going work in relation to sickness absence be noted;
and (iii) that, the temporary drop in mandatory compliance due to the
Regional Streamlining Project and transition to the My ESR system. BoD/3643 Planning Guidance 2018/19 The DoP&P provided an overview of the Planning Guidance for 2018/19. A two year plan was submitted in December 2016. Planning Guidance for 2018/19 required providers and commissioners to refresh the original plan to reflect the revised financial, operational and quality deliverables. A draft plan was submitted on 8 March, with the final plan due for submission on 30 April 2018. The Trust had held a market place event on 15 March to showcase directorate business plans. The final submission was to be agreed at the Board Seminar on 19 April with approval at the Board of Directors meeting on 26 April.
Draft

12
Resolved: (i) that, the requirements of the Operational Planning Guidance 2018/19 and the impact on the Trust’s operational planning be noted; and
(ii) that, progress to date in respect of the Trust’s Draft Annual Operational Plan be noted.
BoD/3644 Guardian of Safe Working Hours Summary Report The DMD presented the Guardian of Safe Working Hours Summary Report for Quarter 3: 2017/18. Since commencement of the new contract for Doctors in Training in December 2016 a total of 54 exception reports had been received, and the areas of exceptional reporting were outlined which were mainly in Medicine. No fines had been imposed against the Trust, which was considered a low exceptional reporting organisation. Feedback from junior doctors was largely positive noting they felt able to raise concerns and felt supported.
Resolved: that, the content of the report be noted. BoD/3645 Any Other Notified Business
a. Healthcare User Group (HUG) Visits Bill Johnson, the Healthcare User Group (HUG) Representative reported that a rescheduled visit had taken place to the Short Stay Unit following a previous cancellation due to seasonal pressures. Feedback was neutral with no issues raised. A visit was also undertaken to the EAU, which despite being a busy ward received positive feedback from the patients. BoD/3646 Date and Time of Next Meeting
Resolved: that, the next meeting be held on Thursday, 26 April 2018 at 1.00pm in the Boardroom, University Hospital of Hartlepool.
BoD/3647 Exclusion of Press and Public
Resolved: that, representatives of the press and other members of the public be excluded for the remainder of the meeting having regard to the confidential nature of the business to be transacted, publicity on which would be prejudicial to the public interest (Section 1(2), Public Bodies (Admission to Meetings) Act 1960).
Signed: Date: The meeting closed at 2.40 pm. Draf
t
North Tees and Hartlepool NHS Foundation Trust
Meeting of the Board of Directors
26 April 2018
Report of the Interim Chief Executive
Strategic Aim (The full set of Trust Aims can be found at the beginning of the Board Reports) Putting Patients First; Valuing our People; Transforming our Services; Health and Wellbeing. 1. Introduction The Chief Executive’s Report provides information to the Board of Directors on key local, regional and national issues. 2. Key Issues and Planned Actions 2.1 Integrated Care System (formerly known as Sustainability and Transformation Partnership update) Progress continues to be made in relation to the Integrated Care System (ICS) with Alan Foster providing leadership on the planning to merge the three Cumbria and North East STPs and to ensure a new identity and focus. The Cumbria and North East Health Strategy Group met on Friday, 13 April 2018 where the focus was on Integrated Care Systems, population health management to support developments and engagement, Acute Care optimisation and Local Health and Care Record Exemplar status with regard to the Great North Care Record. Collaboration to sustain clinical services for the future with a focus on locality planning in the Tees Valley is still a priority for the Trust working closely with representatives from South Tees Hospitals NHS Foundation Trust and County Durham and Darlington NHS Foundation Trust. This is being progressed via the Committee in Common, which last met on 6 April 2018, with further meetings scheduled on a regular basis in 2018. 2.2 Secretary of State for Health and Social Care Jeremy Hunt, in a speech to Parliament on 30 March 2018, has outlined the 7 key principles that will guide the Government's thinking ahead of the social care green paper, to be published later in 2018. The Green Paper will be published before the summer and will be framed by thinking on the 7 principles that are set out below:
quality and safety embedded in service provision; whole-person, integrated care with the NHS and social care systems operating as one; the highest possible control given to those receiving support; a valued workforce; better practical support for families and carers; a sustainable funding model for social care supported by a diverse, vibrant and stable
market; and greater security for all – for those born or developing a care need early in life and for
those entering old age who do not know what their future care needs may be. 2.3 Local Elections: Purdah considerations for providers
Draft
2
Due to local elections taking place on 3 May 2018, the Board of Directors should be aware of the pre-election ‘purdah’ period. This is the period of time immediately before elections when announcements from and activities by public bodies which could influence or be seen to influence the election are restricted. This period is designed to avoid the actions of public bodies distracting from or having influence on election campaigns. The ‘purdah’ period typically will be six weeks before the election and NHS Providers have published national guidance for organisations.
2.4 National Pay Structure and Terms and Conditions The NHS Staff Council met on 21 March 2018, and formally signed off a framework agreement for the reform of the NHS pay structure and terms and conditions for all Agenda for Change staff. The NHS trade unions have set in motion a consultation period with their members on the proposed agreement. The assumption is therefore that any deal will move forward to implementation from July 2018, with backdating to April 2018. In brief, the proposed agreement would deliver: A three year fully funded pay deal covering 2018/19 - 2020/21, which would reform the pay
structure delivering fewer pay points, faster progression, and higher starting salaries, and award a 6.5% over the three years to the top of pay scales.
A new system of pay progression. A minimum rate in the NHS of £17,460 from 1 April 2018 – compliant with Living Wage
Foundation Living Wage, and the closure of Band 1. Terms and conditions improvements including enhanced shared parental leave, child
bereavement leave, and a national framework on buying and selling leave. Development of a joint programme of work to improve health and wellbeing to improve
attendance levels and reduce sickness absence. A commitment for the NHS Staff Council to negotiate a provision for apprenticeship pay,
and look at the scope for a national agreement on bank and agency working. The government has confirmed that additional money will be made available to fund the increased salary costs. NHS Improvement has confirmed that funding for the NHS Agenda for Change staff pay agreement will be provided direct to NHS organisations in 2018/19. An appropriate mechanism for distributing the funding in future years is currently being considered by NHS Improvement and NHS England. 2.5 Emergency Care Department The Trust remained one of the top performing NHS Trusts in the county for emergency care. In the latest figures published in March, the emergency care department was in second position nationally with 97.2% of patients treated or admitted within 4 hours. This was an outstanding achievement even with the significant challenges faced over the winter months and which have continued. The opening of the integrated urgent care service on both hospital sites, which has reached its 1 year anniversary, has undoubtedly contributed towards the success, with patients being treated in the right place at the right time. This is fantastic result for the front of house staff in the emergency and urgent care departments, and all staff across the Trust in the way we are treating patients, the new innovative ways that patients are being cared for and commitment from all to be the best. 2.6 Winter Pressures ‘listening’ event Following on from National ‘listening’ events the Trust will hold a local event on 18 April 2018, where the theme will be winter pressures; focussing on what we did well and how we can
Draft
3
improve for the future. The event will be an informal ‘drop in’ and include representatives from a range of key areas including:
Emergency care pathways Emergency planning Staffing Pharmacy Support staff (North Tees and Hartlepool Solutions) Bed management Occupational Health (Flu Campaign) Critical Care Out of hospital care
The purpose of the ‘listening’ event is to gather feedback and ideas from staff who have worked during the period of winter pressures in order to learn from their experiences, taking forward ideas and improvements for the future. 2.7 NHS Providers Policy update Phillippa Hentsch, Head of Analysis, NHS Providers visited the Executive Team, by invite, on 17 April 2018 to discuss the national perspective on current strategic policy issues affecting the NHS. This stimulated a great deal of debate and adds perspective to the challenges being experienced by the Trust and the development of the strategic direction. 2.8 Relaunch of smoke free agenda The Trust has already signed the national pledge to be smoke free by March 2019 and is working towards improving the smoke free status of both sites to improve the overall appearance and quality of the hospital environments. The Trust is aware that as well as dying prematurely, many of the conditions caused by smoking are chronic illnesses such as COPD (chronic obstructive pulmonary disorder), which can be debilitating for the sufferer and make it difficult to carry out day to day tasks. It is important therefore that the Trust makes a clear statement through its smoke free policy in support of lifestyles which maintain health and prevent unnecessary suffering. Changes to be made across the next 12 months include: All patients will be screened for tobacco dependence and all inpatients offered nicotine
replacement therapy; Nicotine replacement therapy will be stocked at ward level and easily obtained on site per
patient need; All smokers will be offered a referral to community stop smoking service who give specialist
advice and support; All staff will be trained in brief interventions for tobacco dependence; All staff who smoke will have access to stop smoking support through occupational health; Smoke free entrances and exits across both hospital sites will be promoted and enforced.
2.9 North Tees and Hartlepool Education Alliance A new programme which the Trust was commissioned to lead on to train staff in care homes has been shortlisted in the ‘Improving value in the care of frail older patients’ category at the Health Services Journal awards 2018. The programme is delivered through an alliance arrangement providing both registered and non-registered staff with training with the aim of providing the best possible care for older people, empowering staff to make confident and informed decisions to enable care to be delivered closer to home avoiding the need for unnecessary admission to hospital.
Draft
4
The package of training focuses on key areas of care including wellbeing of frail elderly; falls prevention; dementia awareness, delirium and person centred care; end of life care and is also supported by the implementation of digital technology. This is part of our clear strategy on improving and delivering a frailty model for the future. The winners will be announced on 7 June 2018. 3. Recommendations The Board of Directors is asked to note the content of this report. Julie Gillon Interim Chief Executive
Draft

North Tees and Hartlepool NHS Foundation Trust
Meeting of the Board of Directors
26 April 2018
Report of the Interim Chief Executive
Retrospective Approval of Documents Executed Under Seal Strategic Aim (The full set of Trust Aims can be found at the beginning of the Board Reports) Transforming our Services The following documents have been executed under the Common Seal of the Trust.
Document Date Sealed By
Litigation Funding Deed Between:
1) GVA Grimley Limited
And
2) North Tees and Hartlepool NHS Foundation Trust
9 February 2018
Mr R Toole In the presence of
Mrs B Bright
Facilities Agreement Between:
1) North Tees and Hartlepool NHS Foundation Trust And 2) North Tees and Hartlepool Solutions LLP
3 April 2018
Mr R Toole and Mr A Sheppard
Debenture Between: 1) North Tees and Hartlepool NHS Foundation Trust And 2) North Tees and Hartlepool Solutions LLP
3 April 2018
Mr R Toole and Mr A Sheppard
The Board is requested to grant retrospective approval for the sealing of these documents.
Julie Gillon Interim Chief Executive
Draft
1
North Tees and Hartlepool NHS Foundation Trust
Meeting of the Board of Directors
26 April 2018
Executive Summary
Safety, Quality and Infection Prevention Report
Report of the Director of Nursing, Patient Safety and Quality
Strategic Aim (The full set of Trust Aims can be found at the beginning of the Board Reports) Putting Patients First Strategic Objective (The full set of Trust Objectives can be found at the beginning of the Board Reports) Putting Patients First/Patient Safety 1 Introduction
1.1 The safety, quality and infection prevention report highlights aspects of patient safety
and experience along with the healthcare associated infection performance position and ongoing work.
2 Safe
2.1 Patient Falls, March 2018 (134) and the total for 2017-2018 (1,467).
2.2 Pressure Ulcers, February 2018 (23) and the total for 2017-2018 (227). 2.3 Clostridium difficile - The Trust is reporting four Trust attributed cases of Clostridium
difficile infections for March 2018, giving an end of year position of 35 trust attributed cases.
2.4 MRSA bacteraemia - The Trust is reporting no Trust attributed cases of MRSA bacteraemia for March 2018, giving an end of year position of 4 trust attributed cases.
2.5 MSSA bacteraemia - The Trust is reporting four Trust attributed cases of MSSA
bacteraemia for March 2018, giving an end of year position of 25 trust attributed cases. 2.6 E.coli bacteraemia - The Trust is reporting one Trust attributed cases of E.coli
infections for March 2018 and 43 cases for the full year which represents an improvement on the previous year.
2.7 Klebsiella species bacteraemia – The Trust is reporting two Trust attributed cases of
Klebsiella species bacteraemia for March 2018 and 29 cases for the full reporting year. 2.8 Pseudomonas aeruginosa bacteraemia – The Trust is reporting zero Trust
attributed case of Pseudomonas aeruginosa bacteraemia for March 2018 and 5 cases for the full reporting year.
2.9 Hand hygiene - The overall Trust compliance scores for hand hygiene was 98% for
March 2018, this exceeds the Trust internal target of 95%. Caring
Draft

2
2.10 The position for Friends and Family for ‘Would Recommend’ was 95.53% for March 2018; this has decreased from 95.76% in February 2018. The percentage of patients who stated they ‘Wouldn’t Recommend’ was 1.15% for March 2018; this has increased from 0.85% in February 2018.
3 Effective 3.1 The latest HSMR value is now 101.32 (January 2017 to December 2017) from the
rebased 100.04 (December 2016 to November 2017), this new value continues to remain inside the ‘as expected’ range; the national mean is 100. The Trust crude mortality rate for HSMR has increased to 3.44% from the rebased 3.39%.
3.2 The latest SHMI value is 105.91 (October 2016 to September 2017), this has decreased from the previously unreported value of 106.27 (September 2016 to August 2017), the value maintains the Trust in the ‘as expected’ range. The Trust crude mortality rate for SHMI is now 3.50%.
4 Responsive 4.1 The Trust received 66 complaints in March 2018, of which 8 were Stage 3 (request for
a written response) complaints (12.12%).
4.2 The Trust’s response rate for stage 3 complaints for February 2018 was 100%. 5 Well-Led
5.1 The registered nurse fill rate has consistently remained above 80% for both day and
night duty with all areas adhering to the red rules ensuring maintenance of safe staffing.
6 Quality Accounts 2017-18
6.1 The Trust annual Quality Accounts is currently out with all the required stakeholders,
the stakholders will provide their third pary statements based on the document by the end of April 2018.
6.2 PriceWaterhouseCoopers will be in the Trust late April/early May 2018 to audit the Quality Accounts document prior to its publication in June 2018.
7 Recommendation
7.1 The Board of Directors is asked to note the content of the report, the current
performance and work to continously improve.
7.2 The Board are asked to note the HSMR and SHMI values which contine to remain within the expected range.
Julie Lane Director of Nursing, Patient Safety and Quality
Draft
3
North Tees and Hartlepool NHS Foundation Trust
Meeting of the Board of Directors
26 April 2018
Safety, Quality and Infection Prevention Report
Report of the Director of Nursing, Patient Safety and Quality
1 Introduction/Background 1.1 The purpose of this report is to inform the Board of Directors of aspects of quality,
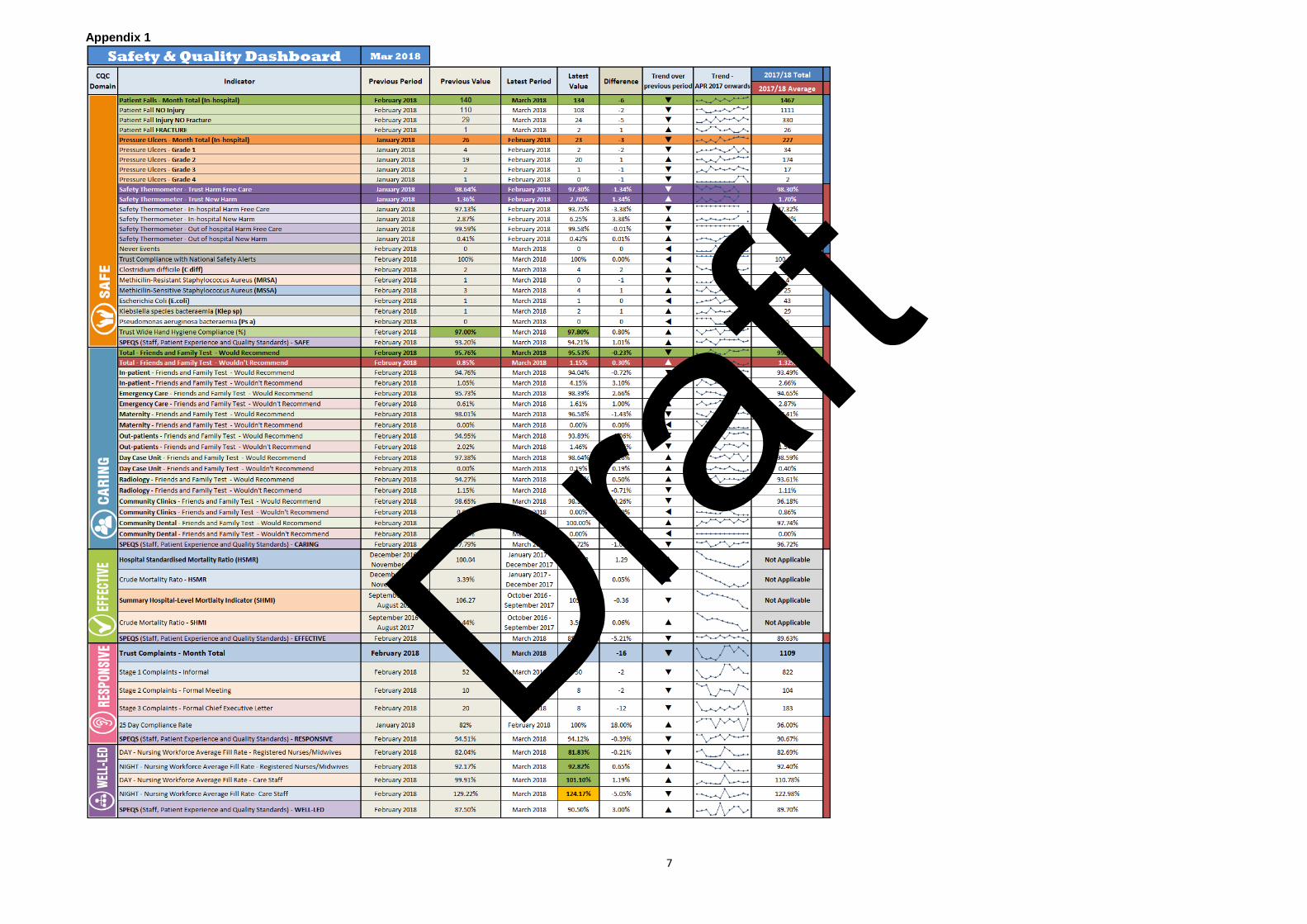
patient safety and experience along with healthcare associated infection performance. 1.2 The Trust Safety and Quality Dashboard (see appendix 1), utilises the CQC domains
of Safe, Caring, Effective, Responsive and Well-Led. The dashboard allows users, to see month on month trending. Safe
2 Falls data for 2017-18 – In-hospital (data to March 2018)
2.1 For the reporting period of March 2018 the Trust has seen 134 falls (108 falls with no Injury, 24 falls with injury no fracture and 2 falls with fracture).
2.2 When benchmarked against April 16 to March 2017 data, the Trust has experienced a total of 110 more falls, 1,467 (April 2017 to March 2018) against 1,357 (April 16 to March 2017).
2.3 Focused work has been undertaken by the lead nurse for unplanned care, due to the
rise in the overall number; areas for improvement have been identified with regard to assessment and onward referral.
3 Pressure Ulcers 2017-18 – In-hospital (data to February 2018)
3.1 For February 2018 the Trust experienced 23 pressure ulcers of which 21 were grade 2 and above, this has decreased from 22 in January 2018.
3.2 When benchmarked against April 2017 to February 2018 data, the Trust had
experienced a total of 54 more pressure ulcers, 227 (April 2017 to February 2018) against 173 (April 2016 to February 2017).
3.3 Work is being undertaken to identify any trends in pressure ulcer incidence. Revised
documentation has been developed and a new SSKIN daily care plan for pressure ulcer prevention has been rolled out across the Trust. Compliance is monitored bi-monthly by audit.
4 Never Events
4.1 There have been no never events in this reporting period.
5 Healthcare Acquired Infections (data up to March 2018)
5.1 Clostridium difficile - The Trust is reporting four Trust attributed cases of Clostridium
difficile infections for March 2018, compared with the previously reported two in
Draft
4
February 2018. This gives an end of year total of 35 Trust attributed cases. Although this exceeds the annual trajectory this does represent an improved position on the previous year. The Improvement Plan for 2018-19 is now under development with any incomplete actions being carried forward. The focus of the plan will again be getting the fundamentals of care right including hand hygiene, environmental cleanliness and antibiotic stewardship, plus continuing the collaborative work with partner organisations which commenced during 2017-18.
5.2 MRSA bacteraemia - The Trust is reporting no Trust attributed cases of MRSA bacteraemia for March 2018. This gives an end of year position of 4 Trust attributed cases. This is a deterioration in comparison with the previous year.
5.3 MSSA bacteraemia - The Trust is reporting four Trust attributed case of MSSA bacteraemia for March 2018 giving an end of year position of 25 Trust attributed cases. This is a deterioration in comparison with the previous year.
5.4 E.coli bacteraemia - The Trust is reporting one Trust attributed cases of E.coli infections for March 2018 and 43 cases for the full year which represents an improvement on the previous year.
5.5 Klebsiella species bacteraemia – The Trust is reporting two Trust attributed cases of Klebsiella species bacteraemia for March 2018 and 29 cases for the full reporting year
5.6 Pseudomonas aeruginosa bacteraemia – The Trust is reporting no Trust attributed case of Pseudomonas aeruginosa bacteraemia for March 2018 and 5 cases for the full reporting year.
5.7 Hand hygiene - The overall Trust compliance score for hand hygiene was 98% for March 2018, with a fully reporting year of 97%; this exceeds the Trust internal target of 95%.
Caring 6 Family and Friends Test (FFT) (data up to March 2018)
6.1 The position for Friends and Family for ‘Would Recommend’ was 95.53% for March 2018; this has decreased from 95.76% in February 2018. The percentage of patients who stated they ‘Wouldn’t Recommend’ was 1.15% for March 2018; this has increased from 0.85% in February 2018.
Effective
7 Mortality - Hospital Standardised Mortality Ratio (HSMR)
7.1 The latest HSMR value is now 101.32 (January 2017 to December 2017) from the rebased 100.04 (December 2016 to November 2017), this new value continues to remain inside the ‘as expected’ range; the national mean is 100.
7.2 The Trust crude mortality rate for HSMR has increased to 3.44% from the rebased 3.39%.
8 Mortality - Summary Hospital-Level Mortality Indicator (SHMI)
8.1 The latest SHMI value is 105.91 (October 2016 to September 2017), this has decreased from the previously unreported value of 106.27 (September 2016 to August 2017), the value maintains the Trust in the ‘as expected’ range.
Draft
5
8.2 The Trust crude mortality rate has increased to 3.50% (October 2016 to September 2017) from 3.44% (September 2016 to August 2017). Responsive
9 Trust complaints performance (data up to March 2018) 9.1 The Trust has continued to make improvements in complaint resolution. The
complainant is given three choices of how the complaint is dealt with including local resolution, formal meeting within the area or a written response from the Chief Executive
9.2 The Trust received 66 complaints in March 2018, of which 8 were Stage 3 (request for a written response) complaints (12.12%); this has decreased from the 82 complaints reported in February 2018, of which 20 were Stage 3 (request for a written response) complaints (24.39)%
9.3 For April 17 to March 2018 the Trust received 1,109 complaints. The spilt of all complaints are: Stage 1 – Informal 74.12%, Stage 2 – Formal meeting 9.38%, Stage 3 – written response from the Chief Executive 16.50%.
9.4 The Trust’s response rate for Stage 3 complaints was 100% for February 2018.
Well-Led
10 Nursing and Midwifery Workforce (data up to March 2018) 10.1 Registered Nurse/Midwife day shift fill rates across inpatient areas for the month of
March 2018 is 81.83% down from 82.04% in February 2018. The night duty fill rate for March 2018 is 92.82% up from 92.17% in February 2018.
10.2 Variances in percentage fill rates occur for a number of reasons including staff vacancies, sickness and maternity leave and in some areas higher than planned fill rates due to increased acuity and care needs of the patient group.
11 Staff, Patient Experience and Quality Standards (SPEQS) (data up to March 2018)
11.1 For the month of March 2018, there was a total of 16 SPEQS visits conducted (10 in-
patient and 6 Outpatient), with an overall SPEQS score of 91.33%, this has decreased from 92.75% in February 2018 where 14 visits were conducted (11 in-patient and 3 Outpatient).
11.2 Throughout the reporting period of 2017-18, there were a total of 144 visits undertaken, with the full year averages as follows:
• Safe 93.96% • Effective 89.63% • Caring 96.72% • Responsive 90.67% • Well-Led 89.70% • Commodes Clean 92.28% • Toilets Clean 97.21%
Draft

6
12 Quality Accounts 2017-18
12.1 The Trust annual Quality Accounts is currently out with all the required stakeholders,
who will provide their third pary statements by the end of April 2018. 12.2 The Trusts Quality Accounts will be audtied by PriceWaterhouseCoopers, this audit
will occur late April/early May 2018 prior to its publication in June 2018.
13 Trust Occupancy
13.1 The following table demonstrates the Trusts occupancy throughout the financial year, with the March 2018 occupancy reaching 90.74%.
2017-18 Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Target 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00%
Trust actual 89.47% 97.76% 89.20% 88.23% 92.45% 92.63% 87.90% 91.94% 94.19% 91.37% 92.71% 90.74%
13.1 The following table demonstrates the Trusts occupancy throughout the financial year
of 2016-2017 for comparison.
2016-17 Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Target 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00%
Trust actual 96.29% 96.68% 95.61% 95.18% 93.20% 96.19% 92.57% 94.22% 90.91% 94.23% 92.31% 85.51%
13.2 The following chart demonstrates the trend from April 2016
14 Recommendation 14.1 The Board of Directors is asked to note the content of the report, current
performance and work to continously improve
14.2 The Board are asked to note the HSMR and SHMI values which contine to remain within the expected range.
Julie Lane Director of Nursing, Patient Safety and Quality
Draft
7
Appendix 1
Draft
1
North Tees and Hartlepool NHS Foundation Trust
Board of Directors
26 April 2018
Project Management and Improvement Office Update
Report of the Chief Executive
Strategic objective: Transforming our services
Executive Summary
1. Introduction
1.1 The purpose of the paper is to update the Board of Directors of changes which have been made to date in relation to the role of the Project Management and Improvement Office (PMIO) that will serve to enhance the ownership and delivery of a portfolio of projects to improve efficiency, quality and contribute to the achievement of financial and operational stability.
2. Background
2.1 The Transformation Team, previously aligned strategically to Workforce and Organisation Development managed a number of service improvement and cost reduction projects.
2.2 Further schemes and pipeline schemes were identified at corporate and directorate level as part of the productivity and efficiency plans to deliver financial and operational stability.
2.3 Additional support was required to develop and progress these plans in a consistent manner with appropriate scrutiny and governance applied.
2.4 A review of the internal Transformation structure has been undertaken to develop a framework of improvement and appropriate oversight by an established Project Management and Improvement Office (PMIO). Executive sponsorship has transferred from the Director of Human Resources and Education to that of the Interim Chief Executive.
3. Current State
3.1 The PMIO’s main role is to monitor, manage and report on the progress of the Trusts cost improvement programme, this is done through maintenance of a project database which will capture the overarching financial plan and performance against delivery.
3.1 This database will be underpinned by a succinct plan for each project that identifies
milestones, key actions, individual’s responsibilities and risks. 4. Project Focus
4.1 Further efficiencies to support the recovery of the financial position have been identified using the Model Hospitals Opportunities Scanner.
4.2 A core element of this work will be associated with the development of a framework
of improvement through the Delivering Productivity Programme (DPP)
Draft

2
4.3. The Trust is being supported by NHSI, and other external bodies such as the Get it Right First Time (GIRFT) team, Calderdale and Huddersfield NHS Trust sharing best practice, and scoping further opportunities.
4.4 The Executive Team will exercise grip and control through a focused weekly meeting via the Executive Financial Management Group, and will hold individuals and project delivery to account through both day to day management and the governance infrastructure
5. Overarching Programme and Perspective Fit
5.1 The PMIO has an overarching view of all projects in order that links at strategic and system level can be identified. This supporting database will be underpinned by a succinct plan for each project that identifies interdependencies, milestones, key actions, responsibilities and risks.
5.2 Alongside internal Trust-wide plans, the PMIO will support the system-wide planning and delivery of transformation opportunities. A regular capacity and capability review will be undertaken to assess the required resource to support delivery.
6. Next Steps
• Continue to identify projected savings for each programme of work, supporting the Cost Improvement Plans for 2018/19 and overall delivery of financial stability
• Continue to monitor delivery through agreed governance structure • Expand on current savings opportunities with a specific focus on outpatients,
theatres, procurement and medicines management • Continue to work collaboratively to develop an integrated care system
reducing variation and duplication • Fully scope commercial opportunities
7. Recommendations
The Board of Directors is asked to:
• Note the robust PMIO structure and appropriate governance process and
approach to provide assurance to the Board of Directors with regard to capability and capacity to deliver key operational and financial projects linking into a tiered system approach to financial stability;
• Note the urgency of change and pace of intensity required to support the financial recovery and stability; and
• Note the requirement to provide a regular report to NHSI as part of the externally monitored financial recovery programme.
Julie Gillon Interim Chief Executive April 2018
Draft
1
North Tees and Hartlepool NHS Foundation Trust
Board of Directors
26 April 2018
Project Management and Improvement Office Update
Report of the Chief Executive
Strategic Aim and Objectives (the full set of Trust Aims can be found at the beginning of the Board of Directors Reports) Transforming our services
1. Introduction
1.1 The NHS is facing a number of challenges as it strives to meet the requirements of the Five Year Forward view. Demand for services is rising and the resources available to meet these demands are finite. Increasingly commissioners, NHS Trusts and health and social care systems are establishing Programme Management Offices to help them develop appropriate governance arrangements to support the development and delivery of change, cost improvement plans (CIPs) and efficiency gains.
1.2 The purpose of the paper is to update the Board of Directors of the changes which
have been made to date in relation to the role of the Project Management and Improvement Office (PMIO) that will serve to enhance the ownership and delivery of a portfolio of projects to improve efficiency, quality and contribute to the achievement of financial and operational stability.
2. Background
2.1 The Transformation Team, previously aligned strategically to Workforce and Organisation Development managed a number of service improvement and cost reduction projects. Further schemes and pipeline schemes were identified at corporate and directorate level as part of the productivity and efficiency plans to deliver financial and operational stability. Whilst it is recognised that not all schemes identified for 2017/18 were cash releasing the Trust agreed to develop a revised financial plan, in alignment with NHSI and using the Model Hospital ‘Opportunities Scanner’ to highlight and target key areas of potential savings. It was recognised that additional support was required to develop and progress these plans in a consistent manner with appropriate scrutiny and governance applied. As such a review of the internal Transformation structure took place with the aim to develop a framework of improvement and appropriate oversight by an established Project Management and Improvement Office (PMIO).
3. Current State
3.1 The PMIO’s main role is to monitor, manage and report on the progress of the Trusts cost improvement programme, this is done through maintenance of a project database which will capture the overarching financial plan and performance against delivery. This database will be underpinned by a succinct plan for each project that identifies milestones, key actions, individual’s responsibilities and risks. To ensure a standardised approach throughout the organisation a document portfolio has been developed to take the proposed schemes through the necessary approval processes (Project Initiation document (PID) Quality Impact Assessment (QIA) and risk register,
Draft
2
and to report on progress via the Executive Financial Management Group (EFMG). The ultimate goal of this programme approach is to realise outcomes and benefits which are in line with the organisations strategic direction. To achieve this, the programme has been designed as a structure created to coordinate, direct and oversee the delivery and implementation of projects.
3.3 The programme principles are to:
• Remain aligned and support the delivery of the corporate strategy. • Lead change. • Envision and communicate a clear and sustainable future. • Focus on benefits and threats to achievement. • Design and deliver a coherent capability. • Learn from experience. • Add value.
4. Project Focus
4.1 The Trust recognises the need to move at pace to deliver on further efficiencies to support recovery and stability of the financial position. In 2017/18 and going forward into 2018/19 and beyond a core element of this work is associated with the development of a framework of improvement through the Delivering Productivity Programme (DPP).
4.2 The Model Hospital Opportunities Scanner is an NHSI benchmarking tool that
identifies potential opportunities of variance within reference cost data and highlights where Trust’s costs for like for like activities exceeds the national average and quantifies the potential cost savings that could be realised if these above average costs were reduced. On using this benchmarking tool the Trust has been able to identify areas indicating a negative variance. These include the following areas;
• Corporate Services (including corporate overheads and administration) • Procurement • Obstetrics & Gynaecology • Paediatrics • Orthopaedics
4.3 The Trust has been supported in the initial stages by NHSI. The Trust is committed to working collaboratively with the NHSI team to ensure full delivery of the DPP programme. In addition the Getting It Right First Time (GIRFT) Programme has been adopted by the Trust to engage clinicians working in acute care to use their own data to accelerate the adoption of evidence based practice through peer to peer discussion and review. The priority areas and ensuing improvements will be pursued and supported by clinical and managerial leadership / ownership and a robust PMIO infrastructure, with GIRFT reviews and recommendations integrated into the work plans. The Trust is also working closely with Calderdale and Huddersfield NHS Trust and other partner agencies sharing best practice, and scoping further opportunities.
4.4 The Executive Team exercise control through a focused weekly meeting via the Executive Financial Management Group, whereby individuals and project delivery are held to account through both day to day management and the agreed PMIO governance infrastructure.
The PMIO sits within the overarching framework of wider transformation both internal
and systematic with a specific focus in these early days of internal stabilisation.
Draft
3
5. Project Development
5.1 Strategic leadership planning and challenge on matters of organisational change and service delivery occurs through the Project Management and Improvement Office with associated governance and scrutiny applied that will enable the Trust to achieve key programmes of work to support delivery of the financial plan and enable a sustainable operational, financial and quality position for the future. Clinical and operational buy in is critical to the success of this programme of work and as the PMIO has developed the process has been refined to clarify clinical ownership and responsibilities to ensure the required engagement is clear and unambiguous.
5.2 It has been acknowledged by the Executive Financial Management Group that robust challenge is necessary and wider corporate requirements must be taken into consideration. A review of the roles and responsibilities of the project team has recognised that Executive Sponsorship is essential and day to day project management should be led at directorate level by the appropriate Associate Director or General Manager (Delivery Manager) (Appendix 1).
Whilst project team responsibilities have been established they are developing into a form and embedded structure throughout the organisation and include:
5.2.1 Executive Sponsor.
• Accountable for the outcome • Chairing their Projects Board • Keeping senior stakeholders onside • Engaging with Users (also using Clinical Lead Influencer) • Removing roadblocks • Role modelling require behaviours
5.2.2 Delivery Manager (directorate led unless cross cutting)
• Ensuring plan is documented • Clear Milestones/Actions • Delivers to Schedule(Time), Quality and Budget • Setting up governance • Report and Escalate • Organising the change
5.2.3 Clinical lead
• Provide overall direction and assurance on clinical impact of project. • Contribute to project development and sign off from a clinical perspective. • Ongoing monitoring to ensure a clinically safe and appropriate approach to
project delivery promoting ownership and buy-in from clinical colleagues to achieve change
5.2.4 Finance Business Partner
• ensure projects are validated, collated and reported on • Establish benchmark opportunity and target financial value
5.2.5 Virtual Team
• Organisational Development, HR Business Partner, Service Improvement Leads and Business Intelligence) will be co-opted in as necessary to support delivery of projects.
Draft
4
• Specialist programme and project advice is given in areas such as business case development, risk management or benefits realisation. (NHSI and GIRFT teams)
5.2.6 PMIO
• Each project team will receive dedicated project management support with
the level of intensity determined by complexity and interdependency. 6. Governance Arrangements
6.1 Robust governance arrangements will be supported both internally and externally with overall accountability for strategic delivery and financial control remaining with the Board of Directors. (Appendix 2) The reporting structure includes;
• Detailed review of the PMIO work plan weekly to provide assurance that the
reporting of performance against delivery of the programme is robust. • Assurance from the Executive team that management action has been taken
regarding Cost Reduction performance. • Provide assurance that Cost Improvement Plans to support organisational
changes are being delivered through PMIO reports. • Review all significant financial risks identified on the portfolio tracker • Consideration of alternative projects of equal financial value should any
existing project indicate non delivery – supported by benchmarking and peer review reports
• A cycle of continuous scoping will identify portfolio choice where a project is not delivering
• Objective assurance of systems and procedures is independently audited by Audit One, reporting to the Audit Committee.
7. Overarching Programme and Perspective Fit
7.1 There are three main levels of planning that need to be considered to determine how Cost Improvement Plans (CIP) will be delivered from a transformational / trust wide level, a day to day operational level and a transactional perspective. The scope of each project considers the level of complexity and the impact on services including system wide involvement to support financial stability and ensure sustainable change is achieved (Appendix 3).
7.2 The PMIO has an overarching view of all projects in order that links at strategic and system level can be identified. This supporting database will be underpinned by a succinct plan for each project that identifies interdependencies, milestones, key actions, responsibilities and risks.
7.3 The project portfolio is updated weekly with a report produced for each project, to ensure sharing of requirements, targets, progress and delivery. This detailed review ensures appropriate stakeholder involvement and work with external and commissioning partners is undertaken as required.
7.4 The PMIO will ensure identification and management of risks/issues likely to impact progress and overall financial and non-financial objectives is established at an early
Draft
5
stage ensuring appropriate remedial action is taken and complete assessment of programme risks against time, quality, cost and impact is undertaken.
Alongside internal Trust-wide plans, the PMIO will support the system-wide planning and delivery of transformation opportunities. A regular capacity and capability review will be undertaken to assess the required resource to support delivery.
8. Financial Update
8.1 The overarching CIP consists of 3 internal programmes of work, CIP, DPP and Limited Liability Partnership which will be supplemented by system working across the Integrated Care System with other Trusts and partner organisations.
Given the current financial position, the challenge to achieve a stretch target of 4% of turnover remains. Directorates are currently working up plans to support the delivery of the target.
The Trust externally reported plan adjusts for risks associated with delivery and realism of achievement, whilst retaining the internal ambition required to deliver financial balance in broad terms.
9. Next Steps
Assurance around delivery of CIP is paramount and plans are currently being reviewed for level of risk and assurance to deliver. In addition, the PMIO and supporting infrastructure will:
• Continue to identify projected savings for each programme of work, supporting the Cost Improvement Plans for 2018/19 and overall delivery of financial stability
• Continue to monitor delivery through agreed governance structure • Expand on current savings opportunities with a specific focus on outpatients,
theatres, procurement and medicines management • Continue to work collaboratively to develop an integrated care system
reducing variation and duplication • Fully scope commercial opportunities
10. Summary 10.1 The purpose of the Trust’s PMIO is to ensure that there is an effective framework for
the management of the organisations Cost Improvement Plan, to ensure sustainable change is achieved and that benefits are identified, managed, monitored and ultimately realised in a timely manner.
10.2 The PMIO will ensure a consistent approach with the use of best practice project
management tools, clear guidance on planning requirements, clear roles and responsibilities and regular progress.
10.3 The PMIO will also ensure identification and management of risks/issues likely to
impact progress and that financial and non-financial objectives are established at an early stage ensuring appropriate remedial action is taken and complete assessment of programme risks against time, quality, cost and impact is undertaken.
10.4 The PMIO provides visibility of progress against targets, agreed milestones and
impact of slippage, driving timely decision making and unblocking of issues. Appropriate challenge, support and guidance is provided to directorate teams in
Draft
6
project development with ongoing facilitation and promotion of project management best practice across the organisation.
10.5 The PMIO has an overarching view of all projects therefore links at strategic level can
be identified and supported. 10.6 The PMIO will also support system-wide planning and delivery of transformational
opportunities; supported by appropriate resource review. 11. Recommendations
The Board of Directors is asked to:
• Note the robust PMIO structure and appropriate governance process and approach to provide assurance to the Board of Directors with regard to capability and capacity to deliver key operational and financial projects linking into a tiered system approach to financial stability;
• Note the urgency of change and pace of intensity required to support the financial recovery and stability; and
• Note the requirement to provide a regular report to NHSI as part of the externally monitored financial recovery programme.
Julie Gillon Interim Chief Executive
Draft
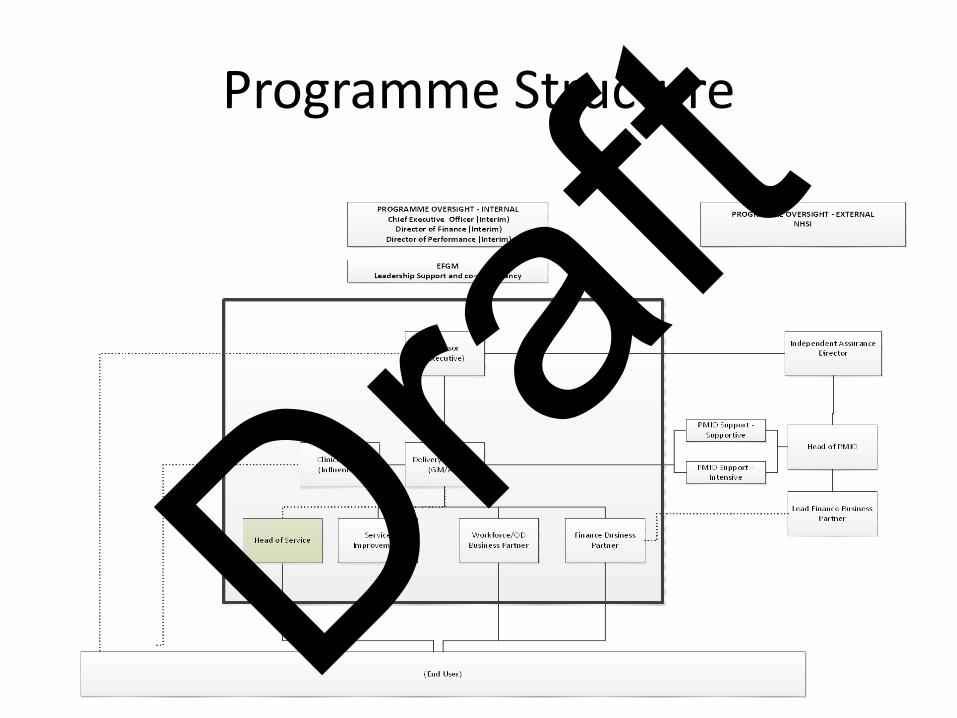
Programme Structure
Draft
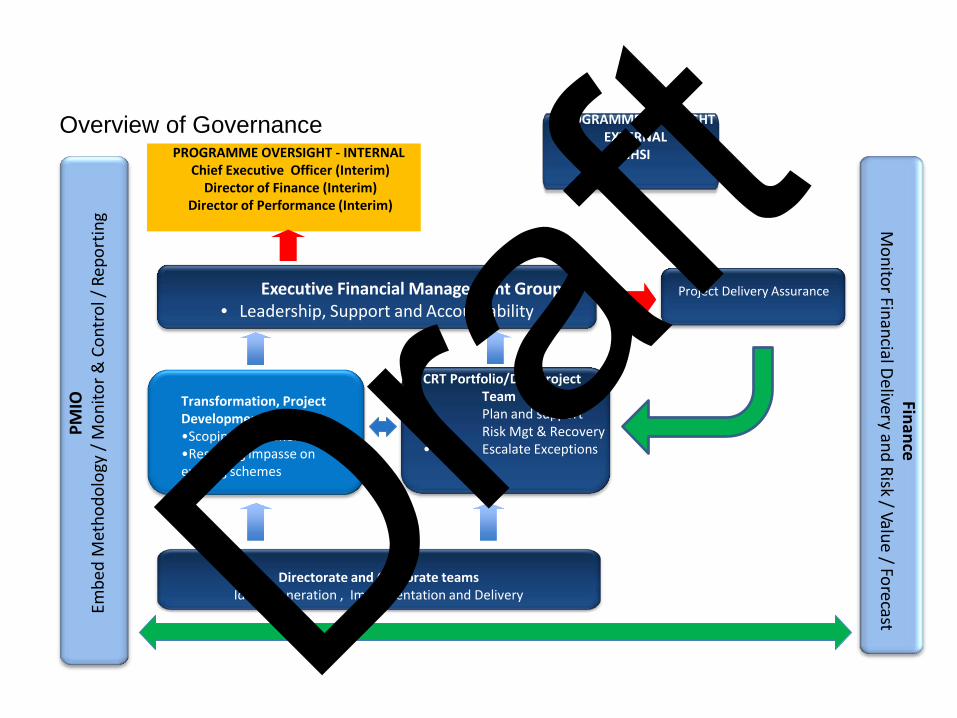
PM
IO
Embe
d M
etho
dolo
gy /
Mon
itor &
Con
trol
/ Re
port
ing
Executive Financial Management Group • Leadership, Support and Accountability
Project Delivery Assurance
CRT Portfolio/DPP Project Team
• Plan and support • Risk Mgt & Recovery • Escalate Exceptions
Transformation, Project Development, Recovery •Scoping new schemes •Resolving impasse on existing schemes
Directorate and Corporate teams Ideas generation , Implementation and Delivery
Finance M
onitor Financial Delivery and Risk / Value / Forecast
Overview of Governance PROGRAMME OVERSIGHT - INTERNAL
Chief Executive Officer (Interim) Director of Finance (Interim)
Director of Performance (Interim)
PROGRAMME OVERSIGHT EXTERNAL
NHSI
Draft
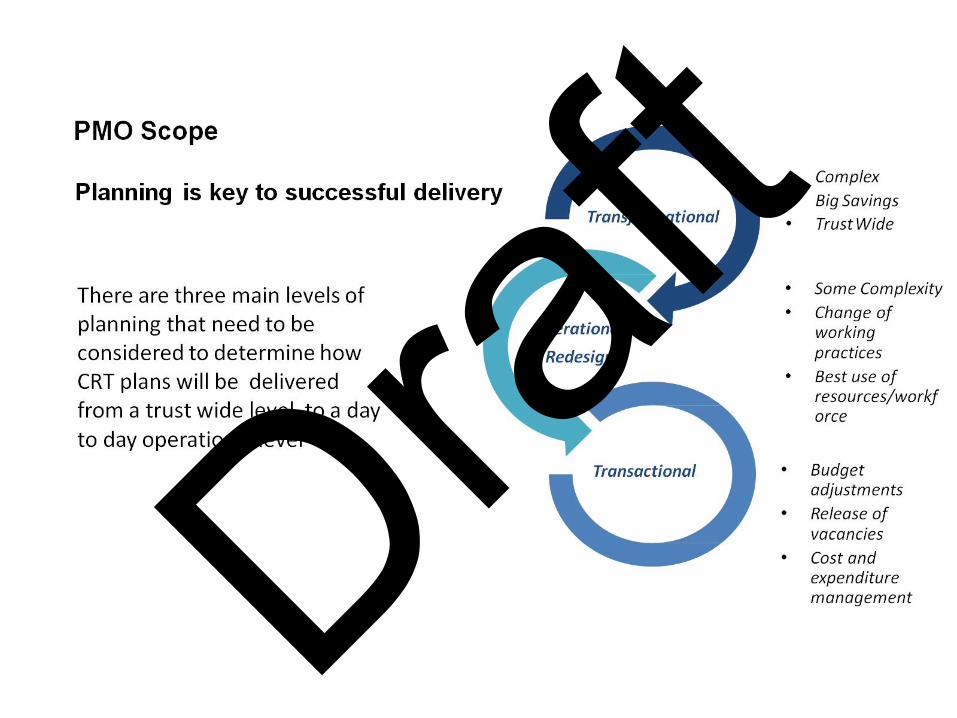
Draft
1
North Tees and Hartlepool NHS Foundation Trust
Meeting of the Board of Directors
26 April 2018
Executive Summary
Capital Programme Performance 2017/18
Report from the Managing Director, North Tees and Hartlepool Solutions LLP Presented by the Director of Finance (Interim)
Strategic Aim (The full set of Trust Aims can be found at the beginning of the Board Reports)
Manage our relationships
Strategic Objective (The full set of Trust Objectives can be found at the beginning of the Board Reports)
Finance
1. Introduction/Background 1.1 To provide an update as at 31 March 2018 (Quarter 4) on the progress of delivering
the 2017/18 capital programme. 2. Main content of report 2.1 The four work-streams of Medical Equipment, ICT, Service Development and Estates
Backlog Maintenance have performed as anticipated in Quarter 4. A narrative summary of each work-stream is shown in Appendix 1.
2.2 Significant work has been undertaken on the Major Engineering Infrastructure
Replacement Project and the programme of work has progressed well. There is currently a 12 week delay to the programme due to NG Bailey Limited changing their building sub-contractor. Work is underway to reduce this delay. However, this has had the effect of reducing the current financial year spend for the project although the overall cost of the project remains unaltered.
2.3 The replacement of the 2nd CT scanner on the UHNT site occurred during Quarter 4, it
was essential that this work took place due to the age of the machine and the end of the operational lease. Despite the winter pressures and with careful planning from the Radiology department, the 5 week programme of work was completed without detriment or delay to the delivery of patient services.
3. Conclusion/Summary
3.1 The significant elements of the programme to comment upon are:
Financial expenditure is not in-line with the anticipated annual programme. The Major
Engineering Infrastructure Replacement scheme is progressing well however, with 12 weeks allowable and recoverable delays due to NG Bailey Limited changing their building and civils sub-contractor. Efforts to reduce the delay have been applied. However, inclement weather during most of Quarter 4 has resulted in the programme continuing with the 12 week delay. This has had the effect of a variation to planned
Draft
2
phasing of work in progress milestone payments, reducing the current financial year spend for the project.
3.2 The overall financial summary for the period to 31 March 2018 is being finalised.
4. Recommendation 4.1 The Board is requested to receive this report and note the position on capital schemes. Prepared by Peter Mitchell Managing Director, North Tees and Hartlepool Solutions LLP Reviewed and Presented by R D Toole Director of Finance (Interim) Draf
t
3
North Tees and Hartlepool NHS Foundation Trust
Meeting of the Board of Directors
26 April 2018
Capital Programme Performance 2017/18
Report from the Managing Director, North Tees and Hartlepool Solutions LLP Presented by the Director of Finance (Interim)
1. Introduction 1.1 The 2017/18 capital programme allocation was agreed at £21.9m comprising £6.0m
internally generated depreciation, £14.7m advanced loan for the Major Engineering Infrastructure Replacement Scheme, £1m PDC for the Integrated Urgent Care Centres and £150K donated funds. The NHS Improvement Compliance Framework requires that a minimum of 85% and a maximum of 115% of the original capital allocation should be spent on a monthly basis. Only goods and services that have been received or invoiced may be counted as expenditure.
2. Key Issues & Planned Actions
2.1 The Major Engineering Infrastructure Replacement Scheme is progressing well and
costs remain below budget allocation. The first phase to construct and operationalise new electrical substations is complete. The second phase of work concerns the construction of a new energy centre. A recommendation was made to the Project Board in March 2017 to award the contract to NG Bailey Limited. Following expiry of the compulsory standstill period, NG Bailey Limited was appointed as principal contractor and construction work commenced in July 2017. Work is progressing with a 12 week delay due to NG Bailey Limited changing their building and civil works sub-contractor at a very early stage of the project. NG Bailey Limited continues to strive to reduce the overall time delay. However, difficult weather conditions during Q4 have prevented any progress in shortening the delay in the programme. This had had the effect of reducing the current financial year spend for the project.
Completion of the new energy centre is anticipated to be Autumn 2018, with de-
commissioning of the old boiler house and demolition of the old boiler house chimney anticipated to be completed by the end of March 2019. The anticipated combined During Q4 significant additional infrastructure business cases have been approved to renew the whole of the fire alarm system on the UHNT site and to undertake a major lift replacement programme, also on the UHNT site. Specifications have been written and an OJEU tender exercise undertaken for both projects. A contract evaluation and contract award for the fire alarm scheme has been completed and the evaluation of the lift tender and contract award sections, in particular, will be undertaken during Q1 2018-19.
2.2 During Q4 the CT scanner within the Radiology Department at UHNT was replaced. 2.3 The significant elements of the programme to comment upon are:
Financial expenditure was aligned to the annual programme and capital cash
flow projections/expenditure is behind plan in relation to the annual financial forecast.
Draft

4
Completed schemes have been achieved within the overall planned programme end timescales and budget allocations, with good outcomes and positive feedback.
3. Recommendation
3.1 The Board is requested to receive this report and note the position on capital schemes
up to 31 March 2018.
Prepared by Peter Mitchell Managing Director, North Tees and Hartlepool Solutions LLP Reviewed and Presented by R D Toole Director of Finance (Interim)
Draft

5
Appendix 1 - Work Stream Reports 1. Medical Equipment 1.1 31 replacement patient monitors have been received for both theatre sites. They have
been commissioned for use and training will start week commencing 9 April 2018. 1.2 A total of 12 invasive ventilators have now been commissioned. Of these, three are in
use in CCU and nine in the general medical wards, with staff training having been completed.
1.3 Two replacement cardiac pacemakers, which are used to stabilise heart rhythms, have been purchased for use in the cardio respiratory department.
1.4 A replacement diathermy has been purchased for the Colposcopy clinic at Hartlepool to replace the existing machine that has failed.
2. Information Communication & Technology 2.1 The Capital ICT allocation for 2017/18 was used this financial year to improve / replace
current wired and wireless networks to enable the Trust to offer improved services to patients.
2.2 As part of the wireless upgrade, it was the aim of the Trust to offer free patient and
guest Wi-Fi for other visiting NHS staff. The work to enable this is complete and we are currently trialling its use within the Education department for student access. It is planned to “roll out” the free patient Wi-Fi by the end of Q1 financial year 2018/19.
2.3 The internal video conferencing systems are undergoing testing with the aim of “going
live” by the end of April 2018. This will allow multi endpoint connection to a video call system for single user (with video phone or desk based alternative) or room based such as the boardrooms both internally and externally (via the Jabber guest application). ICT staff are currently working with Neo natal Consultants, who work between the Trust and South Tees Hospitals NHS Foundation Trust, to set up a system where they can carry out video conference calls between sites.
3. Digital Strategy – Electronic Patient Record 3.1 Good progress was achieved within this period. Both contractual milestone payments
5a and 5b have been met, and this links to the delivery of the Theatre module within TrakCare and subsequent payments released during Q3 and Q4 2017/18 respectively.
3.2 The workflow within TrakCare Accident &Emergency has been updated to allow for the
collection and submission of the new emergency dataset. This went live Q4 2017/18 with full support given from the EPR team to ensure a smooth transition for staff.
3.3 Nurses on Ward 33 have recently undertaken a trial of the new electronic handover
available within TrakCare that removes the paper-based process completely. The trial has been successful and resulted in the ward continuing to work paper-free. A wider roll out is now being planned for all other in-patient wards.
3.4 In Q4 2017/18, the Trust commenced with the roll out of TrakCare‟s electronic
prescribing and administration system on Ward 42. This is now used across two wards with the third ward planned to go live on 10 April 2018. The transition from paper to an electronic process has been successful due to the support provided by clinical teams, pharmacy and ward staff. The full roll out across all in-patient wards is expected to complete by Q3 2018/19. This development fulfils the next contractual payment milestones, which will be released Q1 2018/19.
Draft
6
To facilitate clinical staff in the management of patient care at the bedside, investment
has been made in 65 new versatile EPMA carts, encompassing 22” „all in one‟ PCs together with a further 60 versatile carts with built in PCs known as „WoWs‟ (workstations on wheels). Staff trialling the new cart have given positive feedback, highlighting how responsive and quick it is to retrieve information electronically.
3.5 NT&HFT were successful in being awarded Global Digital Exemplar (Fast Follower)
funds following submission of its funding agreement. This funding will be delivered in four milestone payments; the first „on-boarding‟ payment of £1.1m was drawn down March 2018. There are a number of identified deliverables that need to be complete in order to meet the next milestone. The governance for the GDE FF programme is being established, with the inaugural meeting set for May 2018.
3.6 The Trust has hosted two formal site visits under InterSystem‟s Client Reference
Program, both of which attracts service credits to the Trust that can be used against future implementations of TrakCare releases or specific developments.
3.7 In February 2018, the latest Clinical Digital Maturity index report was published by
Digital Health Intelligence. This has seen the Trust ranked joint 1st in the NHS provider sector in England, when this position is compared to the 15th position reported in 2016 and the joint 21st position reported in 2014 the increased maturity results demonstrate a significant improvement, and is testament to the strategic vision and associated investments being made and is a credit to all the hard work that has been carried out across the Trust in using digital technology to support patient care.
3.8 Health Call – Further progress has been made around this NHS Collaboration of which
the Trust is a key member. The second Board of Directors Meeting was held on Monday 26 March, together with an engagement event, aimed at improving the understanding of Healthcall by clinical leaders, and at the way in which the platform can be used across service developments. An internal HealthCall development group is currently being established to identify which pathways of care will benefit from this technology to support pathways of care.
4. Service Developments 4.1 The Electronic Document Management (EDM) department at UHH was relocated from
the 4th Floor of the main ward block to be co-located with the medical records department on the lower ground floor. This has enabled improved communication between the respective teams and reduces logistical issues of transporting patient notes around the building. This freed up space and allowed the expansion of the successful Single Point of Access (SPA) service, further improving the discharge process.
4.2 High level planning and feasibility work was undertaken to support future business
cases for:- Improvements to the Chemotherapy department at UHNT. Installation of a pharmacy robot within the main Pharmacy department UHNT. The addition of a 5th Endoscopy treatment room at UHNT. Additional accommodation to support the surgical breast service within the
Breast Screening service. A Third CT scanner on the UHNT site with options for locations within the
Ultrasound department and adjacent to Rapid Assessment. To provide a Mental Health assessment room within UHNT A&E.
Draft
7
5. Estates Programme 5.1 Energy Centre Replacement
NG Bailey Limited (NGB) decided to replace its building sub-contractor. Interserve Limited is now carrying out the major excavations, civil works and building elements of the project. Work commenced on site in September 2017. A revised detailed project plan has been developed by NG Bailey Limited to take into account this change of building sub-contractor. The project is progressing to the revised programme, which is anticipated to cause a delay of up to 12 weeks against the original project completion date. NG Bailey Limited is striving to mitigate this overall programme delay. However, weather conditions continued to hamper progress on site during Q4 and the site was closed on safety grounds from 27th February 2018 to 2nd March 2018 due to very heavy snow. The overall risks of delay due to the weather are anticipated to reduce in Q1 2018/19. The current anticipated completion date is 30th October 2018.
The overall major infrastructure replacement project costs are anticipated to be £22.5m with a worst case projection of £23m against a DH approved OBC cost plan of £26m, although funding was limited to £25m.
On site, the work progresses with a significant milestone being achieved on the 28th March 2018, when 300 cubic metres of concrete was poured over a 10 hour period to form the ground floor slab of the new energy centre. The steel frame for the building will be built from this base. The construction of the steel frame is anticipated to commence on the 16th April 2018.
Internally within the hospital, work continues to prepare for migration of the departmental electricity supplies from the old substations to the new substations. The containment, cabling and bus bar installation within these locations will continue to progress with installation completion anticipated during Q1 of 2018/19. This work will enable the electrical changeovers that are anticipated to take place over the summer and towards the end of the project once the new emergency generators have been commissioned. A detailed planning process involving clinical and ICT colleagues is now underway to establish the most appropriate changeover sequence that will transfer every electrical supply in the hospital from the old substations to the new substations to minimise disruption to clinical services. Each department will experience a 4 hour interruption of their non-essential electrical supply, and at a later date a 4 hour interruption to their essential supply. Once the detailed electrical changeover sequence has been fully developed, the plans will be submitted to the Project Board for approval to proceed.
Monthly video and photographic drone images showing the progress on site continue to been uploaded to the Trust Twitter and Facebook accounts and within communication messages. NG Bailey Limited has arranged a quarterly letter drop to provide our potentially affected local neighbours with a point of contact for any issues that are raised during the works. All monthly payment valuations are independently validated and certified by Currie and Brown Limited who are filling the role of Cost Advisor to the Trust on this project.
5.2 Backlog maintenance
Draft
8
5.2.1 The UHNT fire alarm replacement project was approved to proceed at the Capital Management Group in January 2018 and, after an OJEU compliant procurement process, a contract has been awarded. The detailed design is anticipated to take place during Q1 2018/19 and work will commence on site to coincide with the ward decant programme. The project is anticipated to take 2 years to complete.
5.2.2 The UHNT lift replacement project was also approved to proceed at the Capital
Management Group in January 2018. An OJEU compliant procurement process is underway. Tender responses have been received from 3 bidders. A round of clarification questions is currently underway and it is anticipated that the contract will be awarded in Q1 of 2018/19. The scope of works includes two bed evacuation lifts within the Tower block. The project is planned to be spread over 3 years.
5.2.3 The end of life CT scanner has been replaced. During the down time the room
has been refurbished to improve the patient environment. 5.2.4 A fire compartmentation survey has been commissioned for the UHNT site to
check compliance and facilitate prioritisation of improvement works. The survey work is anticipated to be complete during Q1 of 2018/19.
Draft

1
North Tees and Hartlepool NHS Foundation Trust
Meeting of the Board of Directors
26 April 2018
Executive Summary
Compliance and Performance Report
Report of the Interim Director of Planning and Performance
Strategic Aim (The full set of Trust Aims can be found at the beginning of the Board Reports) Putting Patients First 1. Introduction/ Purpose
1.1 The Compliance and Performance Report highlights performance against a range of indicators against the Single Oversight Framework (SOF) and the Foundation Trust terms of licence for the month of March and Q4 (Q4) 2017/18. The Corporate Dashboard and reporting framework reflects both the mandatory performance frameworks for 2017/18 and the additional internal reporting requirements, including the Lord Carter Model Hospital review and key objectives.
1.2 This report must be read in conjunction with the additional information as detailed in
the Safety, Quality and Infection Prevention Performance Report, the Human Resources (HR) Report and the Finance and Contract Report.
2. Key Highlights/ Issues/ Risks
2.1 The Trust’s Integrated Urgent and Emergency Care service reported 97.18% against the four hour standard for the month of March and 97.03% for Q4. The Trust’s performance has remained within or above the national average, reporting 2nd position nationally and first regionally. Full details are described in section 3 of the main report.
2.2 On aggregate, the overall A&E activity (Type 1 and Type 3) during Q4 indicates the
Trust has seen a net increase of 91.46% (n=19,391) compared to the same period last year, with admissions increasing by 31.41% (n=1539).
2.3 The Trust has reported 92.82% against the 92% RTT standard for the month of March
and 92.63% for Q4 period. 2.4 The Trust under-achieved against the Cancer 62 day urgent referral to treatment
standard in February, reporting at 73.17% against the 85% standard. This is a disappointing position, with a considerable drop in performance against the January position of 90.70%. All other cancer standards where achieved. In comparison, the Northern England Cancer Alliance (NCA) reported 84.66% against the target of 85%, with the national position reporting an average of 80.8%. See main report for details.
2.5 The Trust achieved against the 99% Diagnostic standard for March and the quarter,
reporting at 99.62% and 99.60 respectively.
Draft
2
2.6 In March non-medical cancelled operations reported at 0.47% (n=16) below the target of 0.80%. This is an improved position following a difficult start to the quarter, which felt the impact of seasonal pressures and the national directive to reduce non urgent elective lists. No ‘urgent’ procedures had been cancelled for a second time.
2.7 The Trust has performed relatively well against key operational efficiency measures, however with DNA rates and Readmission rates are reporting above target. Further work is on-going to improve efficiencies supported by the Delivering Productivity Programme.
3. Key Challenges 3.1 Continuous and sustainable achievement of key access standards across elective,
emergency and cancer pathways, alongside a number of variables outside of the control of the Trust within the context of system pressures and financial constraints.
3.2 Delivery against the Lord Carter operational efficiency recommendations and
associated cash releasing savings. 4. Conclusion 4.1 The Trust has performed relatively well against the majority of key operational
standards during March and Q4, despite the considerable challenges associated with on-going operational, clinical, financial and system wide pressures. The Trust continues to develop the performance reporting framework to ensure it meets the needs of both corporate and directorate level delivery, reflecting the multiple internal and external performance requirements.
4.2 Whilst the Trust has robust governance processes in place for the monitoring and
management of all performance standards there is recognition that current pressures across the whole health economy may ultimately impact on consistent and sustainable delivery, therefore presents an on-going risk.
5. Recommendations
5.1 The Board of Directors is asked to note:
The detail in the Corporate Dashboard and performance against the Single Oversight Framework requirements and the key national indicators.
Review of the Trust’s SOF segmentation, linked to the governance measures and triggers for concern and current financial performance.
The on-going operational performance and system risks to regulatory key performance indicators and the intense mitigation work that is being taken forward to address these going forward.
The due diligence in assessing on-going compliance across both current and new performance requirements, as illustrated in regular seminars and committee discussions.
Lynne Taylor Interim Director of Planning and Performance
Draft
1
North Tees and Hartlepool NHS Foundation Trust
Meeting of the Board of Directors
26 April 2018
Compliance and Performance Report
Report of the Interim Director of Planning and Performance
1. Introduction/ Purpose 1.1 The Compliance and Performance Report highlights performance against a range of
indicators against the Single Oversight Framework (SOF) and the Foundation Trust terms of licence for the month of March and Quarter 4 (Q4) 2017/18. The Corporate Dashboard and reporting framework reflects both the mandatory performance frameworks for 2017/18 and the additional internal reporting requirements, including the Lord Carter Model Hospital review and key objectives.
1.2 This report must be read in conjunction with the additional information as detailed in the Safety, Quality and Infection Prevention Performance Report, the Human Resources (HR) Report and the Finance and Contract Report. This report will concentrate on the operational performance only.
1.3 Appendix 1 illustrates the trend and variance analysis against targets/trajectory
profiles; with due consideration given to both positive and negative variances and progress against monthly, annual and in year improvement targets. Appendix 2 illustrates a high level view of the Corporate Dashboard and progress against key performance indicators. Appendix 3 illustrates the Single Oversight Framework (SOF) and the triggers of governance concern.
2. Performance Context 2.1 The Trust’s Integrated Urgent and Emergency Care service reported 97.18% against
the four hour standard for the month of March and 97.03% for Q4. Full details are described in section 3.
2.2 Emergency Activity (including GPs) across the organisation has seen a slight
decrease of 1.22% (n=137) in Q4 compared to the same time last year.
2.3 The overall emergency activity in Q4 included 2589 patients who were treated via Ambulatory Care, equating to 23.31% of the total emergency admissions.
2.4 Whilst A&E saw a decrease in Type 1 attendances of 33.76% (n=5636) during Q4,
in comparison with the same time last year, this is in the main due to the opening of the Integrated Urgent Care Services which has reduced the number of minor patients attending the Type 1 A&E department. The Integrated Urgent Care Services activity in Q4 reported 16,071 attendances at the North Tees site, including 1105 admissions, with the Hartlepool site reporting 13,467 attendances and 819 admissions (aggregate 29,538 attendances; 1924 admissions).
2.5 Therefore on aggregate, the overall A&E activity (Type 1 and Type 3) during Q4
indicates the Trust has seen a net increase of 91.46% (n=19,391) compared to the same period last year, with admissions increasing by 31.41% (n=1539).
2.6 The Trust is committed to sustainable achievement and continuous improvement
against all access targets. Mitigation plans are in place where appropriate to manage
Draft
2
the position in line with set targets and to provide assurance with regard to remedial action and on-going improvement.
3. Compliance Indicators 3.1 Referral to Treatment (RTT) Pathways
3.1.1 The Trust has reported 92.82% against the 92% RTT standard for the month of
March and 92.63% for Q4 period. 3.1.2 National RTT data, February position (latest published data) indicated the Trust
performed above the national average which reported at 87.90%. See Appendix 1, ‘Index 5 - Benchmarking’.
3.1.3 Median and 92nd percentile waits have remained relatively consistent and within
target, reporting lower than the national average, demonstrating that more patients are generally waiting less than 18 weeks.
3.1.4 The Trust reported no over 52 week waits. 3.1.5 The Trust recognises that the planned reduction in elective activity over the winter
months, with the need to cancel further routine electives to absorb emergency pressures, has had a significant impact on RTT performance which continued throughout Q4. A full recovery plan has been implemented, including additional in-week and weekend sessions. Median and 92nd percentile waits have remained relatively consistent and within target, reporting lower than the national average, demonstrating that more patients are generally waiting less than 18 weeks.
3.2 Emergency Care Standards 3.2.1 The Trust’s Integrated Urgent and Emergency Care service reported 97.18% against
the four hour standard for the month of March and 97.03% for Q4. 3.2.2 The NHS England published statistical report for the A&E 4 hour standard indicates
that only 9 out of the 137 acute providers with a Type 1 A&E department achieved the standard in March 2018.
3.2.3 Appendix 1 ‘Index 5’ reports that, as such, the England average reported at 84.6% in
March, below the 95% standard, with the North East position reporting at 91.5%, with only two regional Trust achieving the standard.
3.2.4 Whilst A&E saw a decrease in Type 1 attendances of 33.76% (n=5636) during Q4,
comparison with the same time last year, this is in the main due to the opening of the Integrated Urgent Care Services which has reduced the number of minor patients attending the Type 1 A&E department. The Integrated Urgent Care Services activity in Q4 reported 16,071 attendances at the North Tees site, including 1105 admissions, with the Hartlepool site reporting 13,467 attendances and 819 admissions (aggregate 29,538 attendances; 1924 admissions).
3.2.5 Therefore on aggregate, the overall A&E activity (Type 1 and Type 3) during Q4
indicates the Trust has seen a net increase of 91.46% (n=19,391) compared to the same period last year, with admissions increasing by 31.41% (n=1539).
3.2.6 The Trust achieved 99.92% (Q4) compliance against the 2 hour Integrated Urgent
Care standard “once clinically streamed, patients to be treated within 2 hours”, which is an excellent achievement within the fourth quarter of the new service going live. Split by site, Hartlepool achieved 99.51% and North Tees achieved 98.63%.
Draft
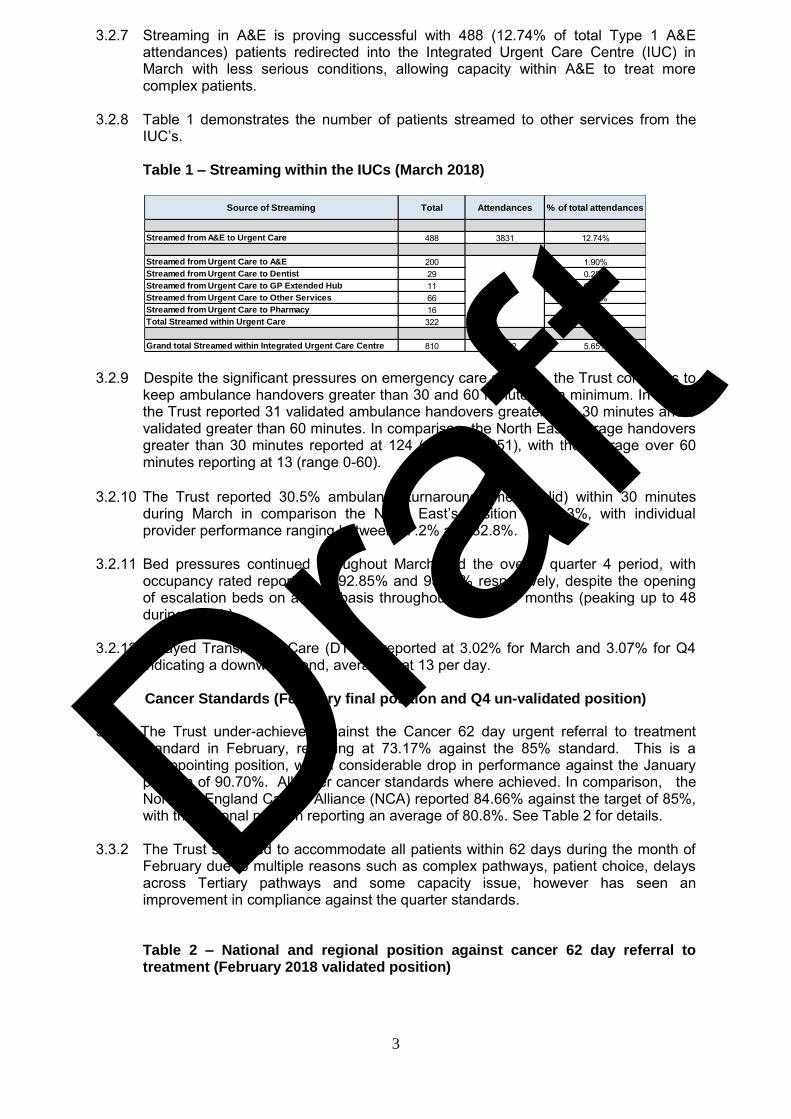
3
3.2.7 Streaming in A&E is proving successful with 488 (12.74% of total Type 1 A&E attendances) patients redirected into the Integrated Urgent Care Centre (IUC) in March with less serious conditions, allowing capacity within A&E to treat more complex patients.
3.2.8 Table 1 demonstrates the number of patients streamed to other services from the
IUC’s.
Table 1 – Streaming within the IUCs (March 2018)
3.2.9 Despite the significant pressures on emergency care services, the Trust continues to
keep ambulance handovers greater than 30 and 60 minutes to a minimum. In March the Trust reported 31 validated ambulance handovers greater than 30 minutes and 0 validated greater than 60 minutes. In comparison, the North East average handovers greater than 30 minutes reported at 124 (range 49-251), with the average over 60 minutes reporting at 13 (range 0-60).
3.2.10 The Trust reported 30.5% ambulance turnaround times (valid) within 30 minutes
during March in comparison the North East’s position at 26.3%, with individual provider performance ranging between 17.2% and 32.8%.
3.2.11 Bed pressures continued throughout March and the overall quarter 4 period, with
occupancy rated reporting at 92.85% and 93.32% respectively, despite the opening of escalation beds on a daily basis throughout the winter months (peaking up to 48 during March).
3.2.12 Delayed Transfers of Care (DTOC) reported at 3.02% for March and 3.07% for Q4 indicating a downward trend, averaging at 13 per day.
3.3 Cancer Standards (February final position and Q4 un-validated position)
3.3.1 The Trust under-achieved against the Cancer 62 day urgent referral to treatment standard in February, reporting at 73.17% against the 85% standard. This is a disappointing position, with a considerable drop in performance against the January position of 90.70%. All other cancer standards where achieved. In comparison, the Northern England Cancer Alliance (NCA) reported 84.66% against the target of 85%, with the national position reporting an average of 80.8%. See Table 2 for details.
3.3.2 The Trust struggled to accommodate all patients within 62 days during the month of
February due to multiple reasons such as complex pathways, patient choice, delays across Tertiary pathways and some capacity issue, however has seen an improvement in compliance against the quarter standards.
Table 2 – National and regional position against cancer 62 day referral to treatment (February 2018 validated position)
Source of Streaming Total Attendances % of total attendances
Streamed from A&E to Urgent Care 488 3831 12.74%
Streamed from Urgent Care to A&E 200 1.90%Streamed from Urgent Care to Dentist 29 0.28%Streamed from Urgent Care to GP Extended Hub 11 0.10%Streamed from Urgent Care to Other Services 66 0.63%Streamed from Urgent Care to Pharmacy 16 0.15%Total Streamed within Urgent Care 322 3.07%
Grand total Streamed within Integrated Urgent Care Centre 810 14332 5.65%
10501
Draft
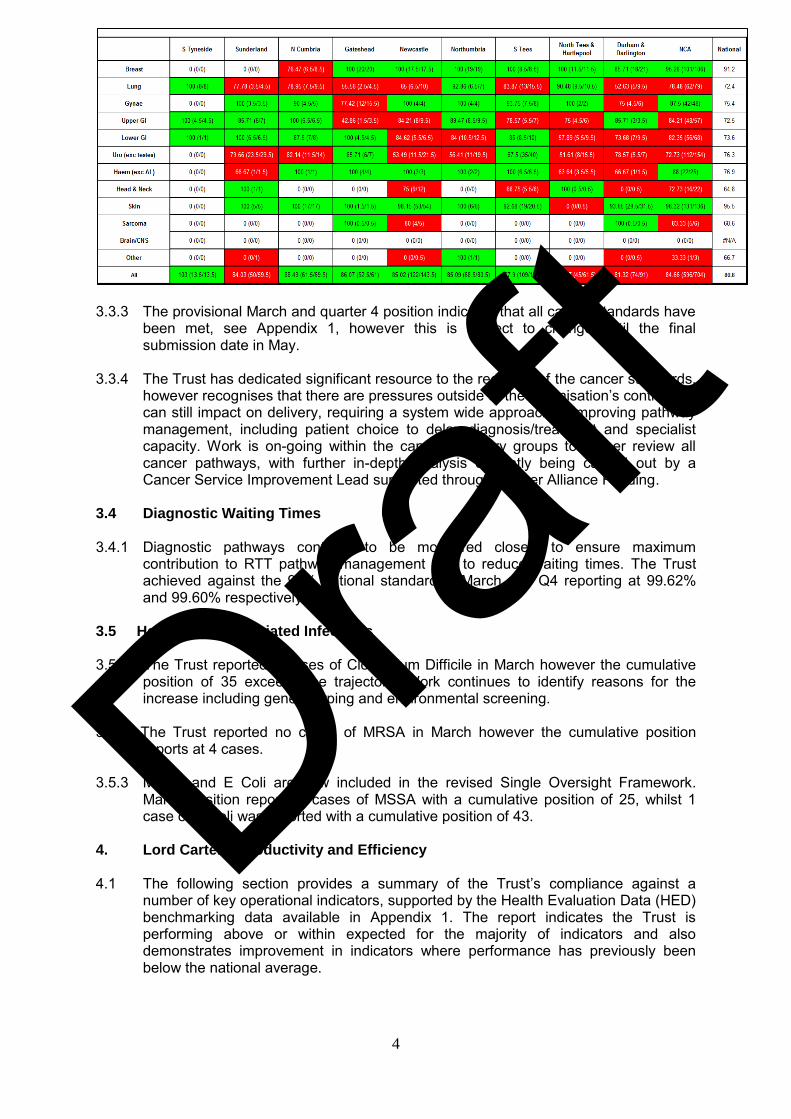
4
3.3.3 The provisional March and quarter 4 position indicates that all cancer standards have
been met, see Appendix 1, however this is subject to change until the final submission date in May.
3.3.4 The Trust has dedicated significant resource to the recovery of the cancer standards,
however recognises that there are pressures outside of the organisation’s control that can still impact on delivery, requiring a system wide approach to improving pathway management, including patient choice to delay diagnosis/treatment and specialist capacity. Work is on-going within the cancer recovery groups to further review all cancer pathways, with further in-depth analysis currently being carried out by a Cancer Service Improvement Lead supported through Cancer Alliance Funding.
3.4 Diagnostic Waiting Times 3.4.1 Diagnostic pathways continue to be monitored closely to ensure maximum
contribution to RTT pathway management and to reduce waiting times. The Trust achieved against the 99% national standard in March and Q4 reporting at 99.62% and 99.60% respectively.
3.5 Health Care Associated Infections 3.5.1 The Trust reported 4 cases of Clostridium Difficile in March however the cumulative
position of 35 exceeds the trajectory. Work continues to identify reasons for the increase including genetic typing and environmental screening.
3.5.2 The Trust reported no cases of MRSA in March however the cumulative position
reports at 4 cases. 3.5.3 MSSA and E Coli are now included in the revised Single Oversight Framework.
March position reports 4 cases of MSSA with a cumulative position of 25, whilst 1 case of E Coli was reported with a cumulative position of 43.
4. Lord Carter – Productivity and Efficiency 4.1 The following section provides a summary of the Trust’s compliance against a
number of key operational indicators, supported by the Health Evaluation Data (HED) benchmarking data available in Appendix 1. The report indicates the Trust is performing above or within expected for the majority of indicators and also demonstrates improvement in indicators where performance has previously been below the national average.
Draft
5
4.1 Outpatient Attendance Indicators 4.1.1 The aggregate New to Review ratios reported at 1.24 in February (latest available
position), showing a positive performance against the current target of 1.45. 4.1.2 The Trust’s performance against ‘New’ Outpatient DNA rates reported above the
agreed target of 5.40%, at 8.92% with ‘Review’ DNA rates reporting at 11.39% against the 9% target, however with further work on-going across directorates as part of the Lord Carter work to deliver additional improvements.
4.1.3 A focussed piece of work will include further assessment of the number of review
appointments carried out within both consultant and nurse led clinics, with the aim to reduce avoidable face to face reviews wherever possible, releasing clinical capacity and improving productivity.
4.2. E-Booking (ASIs) 4.2.1 Latest available data for February 2018 indicates the Trust reported within the 4%
target, at 2.60% for E-Referrals, Appointment Slot Issues (ASIs). In comparison, the regional position reported at 12%, with the national position reporting at 19%. The Trust reported in 15th position nationally. In line with the NHS Digital requirements, the Trust has fully implemented E-Referrals which went live from 1st March 2018, ahead of the National contract deadline of October 2018.
4.3 Cancelled Operations 4.3.1 In March non-medical cancelled operations reported at 0.47% (n=16) below the
target of 0.80%. This is an improved position following a difficult start to the quarter, which felt the impact of seasonal pressures and the national directive to reduce non urgent elective lists. No ‘urgent’ procedures had been cancelled for a second time.
4.4 Readmissions
4.4.1 The Trust is currently reporting emergency readmission rates at 11.18% post emergency admission, with the internal target set at 9.73%, and 3.23% post elective admission, set against a zero tolerance (January 2018 position, latest available data). The aggregate emergency readmission rate reports at 7.78% against the internal stretch target of 7.70% (based on peer average and year on year improvement).
4.4.2 The Trust recognises readmissions as an area requiring further work, in line with
national drivers to reduce avoidable admissions. The reasons for readmissions are regularly audited to establish a root cause and establish if alternative management may have prevented admission and also if the readmission was related to the original admission, therefore un-avoidable. This process is under review with a view to provide deeper analysis, review pathways and develop service redesign were appropriate.
4.4.3 Service development initiatives already established include ‘Hospital at Home’, which
has a proven track record of preventing admissions for those patients suffering from chronic respiratory problems, and Elective Care’s review of Ward 4’s capacity to allow direct access to review post-operative patients and reduce the need to admit as an emergency admission onto base wards. Future developments include a frailty co-ordinator based within A&E and community matrons to visit care home residents.
4.4.4 Table 3 provides an overview of the top 10 reasons for readmission based on April to
January data, however noting the readmitting conditions may not be related to the original admission diagnosis.
Draft

6
Table 3: Top 10 Re-admitting Diagnosis
4.4.5 In general, the Trust has demonstrated a relatively positive position against its overall
operational efficiency performance indicators, which is attributed to the constant effort by service lines and clinical teams to improve quality, efficiency and patient safety and experience.
4.5 Theatre Utilisation
4.5.1 Theatre utilisation is currently under review through a dedicated Delivering Productivity Programme, which includes workstreams across session scheduling, cancellations on the day/DNAs, conversions to day surgery, additional utilisation of Hartlepool site, theatre session flow, stock control and analytics, noting further work is required on the data reporting following the movement to Trakcare.
4.5.2 There is little up to date benchmarking data available to monitor the Trust’s position
against, however internal improvement targets will be set to monitor improvement in productivity.
6 Community Information Dataset (CIDS) 6.1 Performance indicators for Community Services, with data completeness used as a
measure for the three elements of Referral to Treatment (RTT), referral information and treatment activity information, with a target of 50% completeness.
6.2 February position (latest available data) indicates the Trust has achieved all three
CIDs targets for the period, reporting 96.56% against RTT data, 95.96% for Referral data and 95.70% against the activity data. A target of 50% is set for all three indicators.
7. Contract Key Performance Indicators 7.1 The Trust agreed a significant number of key performance measures for 2017/18
within the NHS standard and local contract negotiations. In line with the NHS England Commissioning Board structure, these are reported to multiple commissioning bodies including:
Clinical Commissioning Groups Area Team Local Authority Specialist Commissioning Public Health
7.2 The KPIs cover quality requirements across both acute and community services, with
financial penalties attached against non-compliance. The Trust reports performance to the commissioners on a monthly basis.
Post Emergency admission% of
Readmissions
Number of
Readmissions Post Elective admission% of
Readmissions
Number of
Readmissions
Lobar, Atypical or Viral Pneumonia 6.50% 252 Non-Malignant Gastrointestinal Tract Disorders 6.03% 67
Chronic Obstructive Pulmonary Disease or Bronchitis 5.65% 219 Infections or Other Complications of Procedures 4.50% 50
Non-Malignant Gastrointestinal Tract Disorders 5.27% 204 Sepsis 4.23% 47
Unspecified Chest Pain 4.47% 173 Abdominal Pain 4.23% 47
Sepsis 4.31% 167 Non-Malignant, Hepatobiliary or Pancreatic Disorders 3.42% 38
Non-Malignant, Hepatobiliary or Pancreatic Disorders 3.54% 137 Kidney or Urinary Tract Infections 3.06% 34
Abdominal pain 3.25% 126 Lobar, Atypical or Viral Pneumonia 2.97% 33
Skin Disorders 2.94% 114 Skin disorder/procedure 2.70% 30
Kidney or Urinary Tract Infections 2.92% 113 Chest pain 2.16% 24
Heart Failure or Shock 2.12% 82 COPD or Bronchitis 1.98% 22
Top 10 Total 40.97% 1587 Top 10 Total 35.28% 392
Total Readmissions 3874 1111
Draft
7
7.3 The Trust performed relatively well across the majority of the contract KPIs during Q4. The main areas of pressure are reflective of the Trust’s overall position on key STP access targets including cancer waits and specialty level RTT performance.
7.4 Performance against the contract KPIs for all commissioners are available via a link
within the Corporate Dashboard. 8. NHS Improvement (NHSI) 8.1 Single Oversight Framework (SOF) - Segmentation
8.1 Whilst reporting mechanisms have not been confirmed by NHSI, the expectation is
that all Trusts will continue to be rated in this vein. The Trust currently remains in Segment 2.
8.2 The Sustainability and Transformation Funding (STF) conditions for 2017/18 relate to
achievement of the control total, however with 30% allocated to performance related delivery of the 4 hour standard (15%) and Primary Care Streaming (15%), subject to the overall control total being met. Performance against STF can be found in ‘Index 7’.
9. Conclusion/Summary
9.1 The Trust has performed relatively well against the majority of key operational standards during March and Quarter 4, despite the considerable challenges associated with on-going operational, clinical, financial and system wide pressures. The Trust continues to develop the performance reporting framework to ensure it meets the needs of both corporate and directorate level delivery, reflecting the multiple internal and external performance requirements.
9.2 Whilst the Trust has robust governance processes in place for the monitoring and
management of all performance standards there is recognition that current pressures across the whole health economy may ultimately impact on consistent delivery, therefore presents an on-going risk.
9.3 This risk is outlined within the Trust’s Risk Register and Board Assurance
Framework, with supporting mitigation and recovery plans, alongside internal and external governance assurance processes.
10. Recommendations 10.1 The Board of Directors is asked to note:
The detail in the Corporate Dashboard and performance against the Single Oversight Framework requirements and the key national indicators for March and Quarter 4 2017/18.
Review of the Trust’s SOF segmentation, linked to the governance measures and triggers for concern and current financial performance.
The on-going operational performance and system risks to regulatory key performance indicators and the intense mitigation work that is being taken forward to address these going forward.
The due diligence in assessing on-going compliance across both current and new performance requirements, as illustrated in the regular seminars and committee discussions.
Lynne Taylor Interim Director of Planning and Performance
Draft
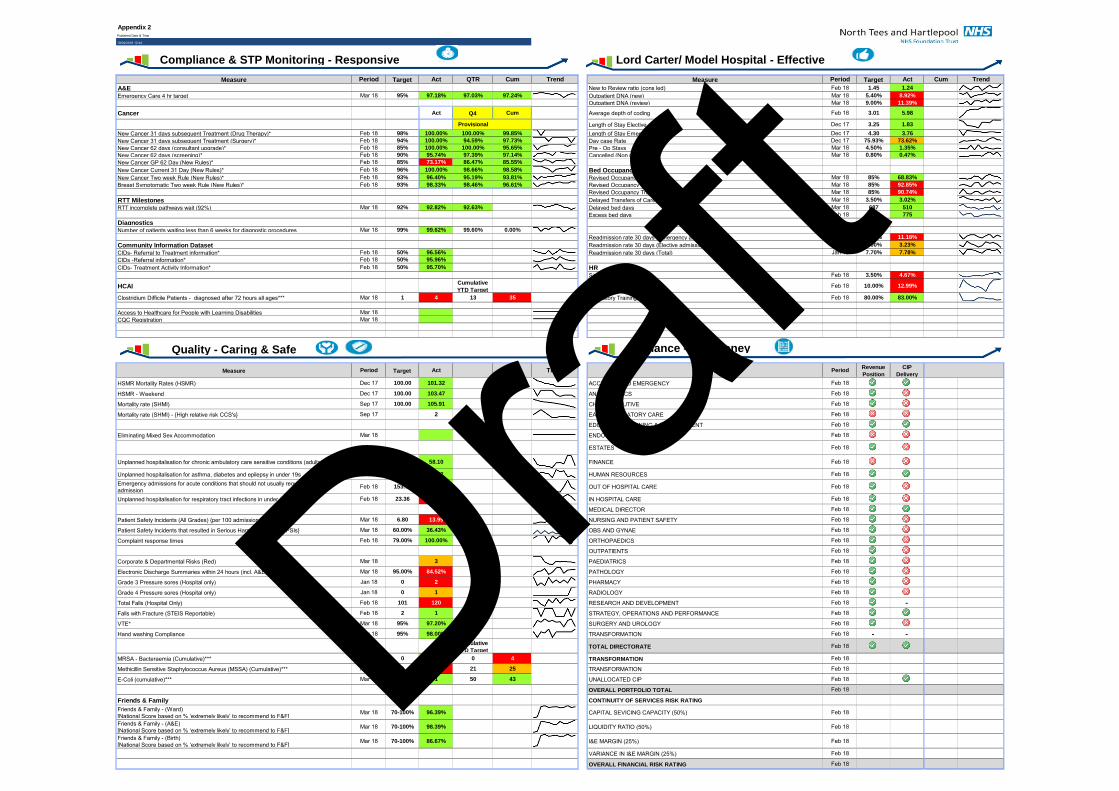
Appendix 2Published Date & Time
19/04/2018 12:44
Measure Period Target Act QTR Cum Trend Measure Period Target Act Cum Trend
A&E New to Review ratio (cons led) Feb 18 1.45 1.24
Emergency Care 4 hr target Mar 18 95% 97.18% 97.03% 97.24% Outpatient DNA (new) Mar 18 5.40% 8.92%
Outpatient DNA (review) Mar 18 9.00% 11.39%
Cancer Act Q4 Cum Average depth of coding Feb 18 3.01 5.98
Provisional Length of Stay Elective Dec 17 3.25 1.83
New Cancer 31 days subsequent Treatment (Drug Therapy)* Feb 18 98% 100.00% 100.00% 99.85% Length of Stay Emergency Dec 17 4.30 3.76
New Cancer 31 days subsequent Treatment (Surgery)* Feb 18 94% 100.00% 94.59% 97.73% Day case Rate Dec 17 75.93% 73.62%
New Cancer 62 days (consultant upgrade)* Feb 18 85% 100.00% 100.00% 95.65% Pre - Op Stays Mar 18 4.50% 1.35%
New Cancer 62 days (screening)* Feb 18 90% 95.74% 97.39% 97.14% Cancelled (Non medical) Mar 18 0.80% 0.47%
New Cancer GP 62 Day (New Rules)* Feb 18 85% 73.17% 86.47% 85.55%
New Cancer Current 31 Day (New Rules)* Feb 18 96% 100.00% 98.66% 98.58% Bed Occupancy New Cancer Two week Rule (New Rules)* Feb 18 93% 96.40% 95.19% 93.81% Revised Occupancy Hartlepool Mar 18 85% 68.83%
Breast Symptomatic Two week Rule (New Rules)* Feb 18 93% 98.33% 98.46% 96.61% Revised Occupancy North Tees Mar 18 85% 92.85%
Revised Occupancy Trust Mar 18 85% 90.74%
RTT Milestones Delayed Transfers of Care Mar 18 3.50% 3.02%
RTT incomplete pathways wait (92%) Mar 18 92% 92.82% 92.63% 0.00% Delayed bed days Mar 18 687 510
Excess bed days Feb 18 1534 775
DiagnosticsNumber of patients waiting less than 6 weeks for diagnostic procedures Mar 18 99% 99.62% 99.60% 0.00%
Readmission rate 30 days (Emergency admission) Jan 18 9.73% 11.18%
Community Information Dataset Readmission rate 30 days (Elective admission) Jan 18 0.00% 3.23%
CIDs- Referral to Treatment information* Feb 18 50% 96.56% Readmission rate 30 days (Total) Jan 18 7.70% 7.78%
CIDs -Referral information* Feb 18 50% 95.96%
CIDs- Treatment Activity Information* Feb 18 50% 95.70% HRSickness absence % * Feb 18 3.50% 4.67%
HCAICumulative
YTD TargetStaff turnover ratio Feb 18 10.00% 12.99%
Clostridium Difficile Patients - diagnosed after 72 hours all ages*** Mar 18 1 4 13 35 Mandatory Training Compliance Feb 18 80.00% 83.00%
Access to Healthcare for People with Learning Disabilities Mar 18 0.00%
CQC Registration Mar 18 0.00%
Measure Period Target Act Cum Trend Measure PeriodRevenue
Position
CIP
Delivery
HSMR Mortality Rates (HSMR) Dec 17 100.00 101.32 ACCIDENT AND EMERGENCY Feb 18
HSMR - Weekend Dec 17 100.00 103.47 ANAESTHETICS Feb 18
Mortality rate (SHMI) Sep 17 100.00 105.91 CHIEF EXECUTIVE Feb 18
Mortality rate (SHMI) - {High relative risk CCS's} Sep 17 2 EAU & AMBULATORY CARE Feb 18
EDUCATION,LEARNING & DEVELOPMENT Feb 18
Eliminating Mixed Sex Accommodation Mar 18 0 0.00% ENDOSCOPY Feb 18
ESTATES Feb 18
Unplanned hospitalisation for chronic ambulatory care sensitive conditions (adults) Feb 18 75.10 58.10 FINANCE Feb 18
Unplanned hospitalisation for asthma, diabetes and epilepsy in under 19s Feb 18 22.25 11.12 HUMAN RESOURCES Feb 18Emergency admissions for acute conditions that should not usually require hospital admission
Feb 18 153.70 149.30 OUT OF HOSPITAL CARE Feb 18
Unplanned hospitalisation for respiratory tract infections in under 19s Feb 18 23.36 26.70 IN HOSPITAL CARE Feb 18
MEDICAL DIRECTOR Feb 18
Patient Safety Incidents (All Grades) {per 100 admissions} Mar 18 6.80 13.99 NURSING AND PATIENT SAFETY Feb 18
Patient Safety Incidents that resulted in Serious Harm - {% of total PSIs} Mar 18 60.00% 36.43% OBS AND GYNAE Feb 18
Complaint response times Feb 18 79.00% 100.00% ORTHOPAEDICS Feb 18
OUTPATIENTS Feb 18
Corporate & Departmental Risks (Red) Mar 18 3 PAEDIATRICS Feb 18
Electronic Discharge Summaries within 24 hours (incl. A&E) Mar 18 95.00% 84.52% PATHOLOGY Feb 18
Grade 3 Pressure sores (Hospital only) Jan 18 0 2 PHARMACY Feb 18
Grade 4 Pressure sores (Hospital only) Jan 18 0 1 RADIOLOGY Feb 18
Total Falls (Hospital Only) Feb 18 101 120 RESEARCH AND DEVELOPMENT Feb 18 -Falls with Fracture (STEIS Reportable) Feb 18 2 1 STRATEGY, OPERATIONS AND PERFORMANCE Feb 18
VTE* Mar 18 95% 97.20% SURGERY AND UROLOGY Feb 18
Hand washing Compliance Mar 18 95% 98.00% TRANSFORMATION Feb 18 - -Cumulative
YTD TargetTOTAL DIRECTORATE Feb 18
MRSA - Bacteraemia (Cumulative)*** Mar 18 0 0 0 4 TRANSFORMATION Feb 18
Methicillin Sensitive Staphylococcus Aureus (MSSA) (Cumulative)*** Mar 18 0 4 21 25 TRANSFORMATION Feb 18
E-Coli (cumulative)*** Mar 18 4 1 50 43 UNALLOCATED CIP Feb 18 -OVERALL PORTFOLIO TOTAL Feb 18
Friends & Family CONTINUITY OF SERVICES RISK RATING
Friends & Family - (Ward)[National Score based on % ‘extremely likely’ to recommend to F&F]
Mar 18 70-100% 96.39% CAPITAL SEVICING CAPACITY (50%) Feb 18
Friends & Family - (A&E)[National Score based on % ‘extremely likely’ to recommend to F&F]
Mar 18 70-100% 98.39% LIQUIDITY RATIO (50%) Feb 18
Friends & Family - (Birth)[National Score based on % ‘extremely likely’ to recommend to F&F]
Mar 18 70-100% 86.67% I&E MARGIN (25%) Feb 18
VARIANCE IN I&E MARGIN (25%) Feb 18
OVERALL FINANCIAL RISK RATING Feb 18
Compliance & STP Monitoring - Responsive Lord Carter/ Model Hospital - Effective
Finance - Our Money Quality - Caring & Safe
Draft
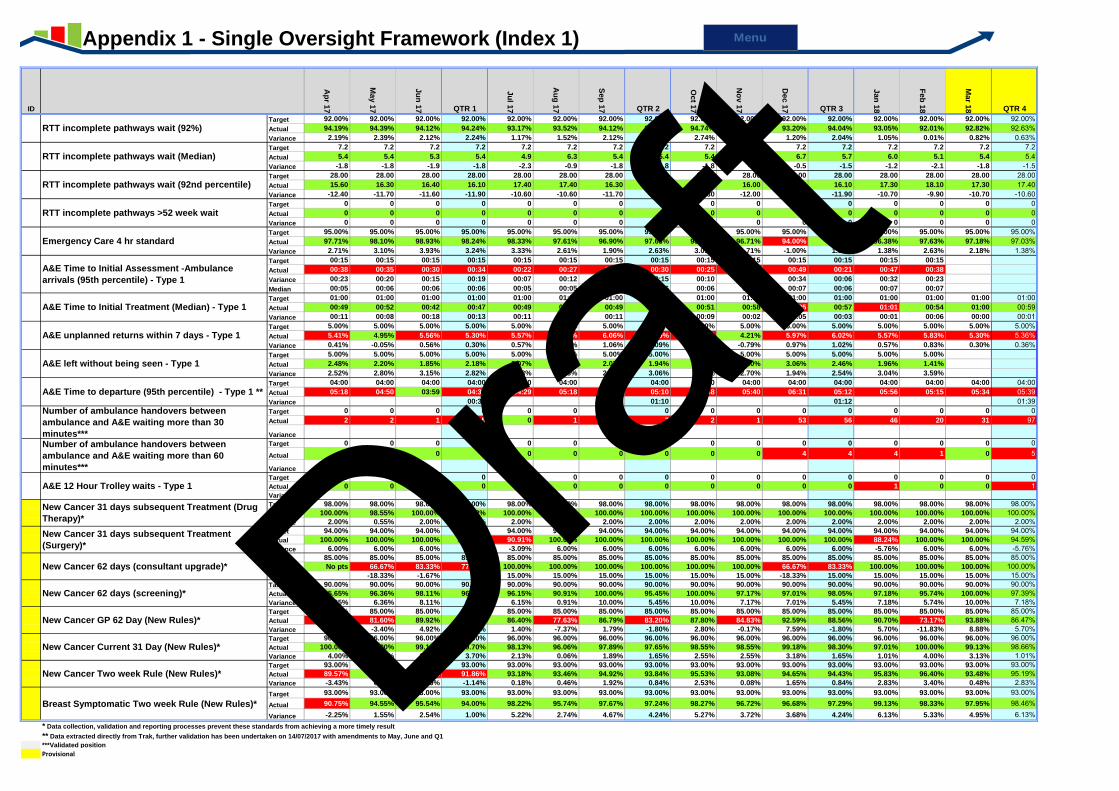
ID
Ap
r 17
May 1
7
Ju
n 1
7 QTR 1
Ju
l 17
Au
g 1
7
Sep
17 QTR 2
Oct 1
7
No
v 1
7
Dec 1
7 QTR 3
Jan
18
Feb
18
Mar 1
8 QTR 4
Target 92.00% 92.00% 92.00% 92.00% 92.00% 92.00% 92.00% 92.00% 92.00% 92.00% 92.00% 92.00% 92.00% 92.00% 92.00% 92.00%Actual 94.19% 94.39% 94.12% 94.24% 93.17% 93.52% 94.12% 93.61% 94.74% 94.20% 93.20% 94.04% 93.05% 92.01% 92.82% 92.63%Variance 2.19% 2.39% 2.12% 2.24% 1.17% 1.52% 2.12% 1.61% 2.74% 2.20% 1.20% 2.04% 1.05% 0.01% 0.82% 0.63%Target 7.2 7.2 7.2 7.2 7.2 7.2 7.2 7.2 7.2 7.2 7.2 7.2 7.2 7.2 7.2 7.2Actual 5.4 5.4 5.3 5.4 4.9 6.3 5.4 5.4 5.4 5.4 6.7 5.7 6.0 5.1 5.4 5.4Variance -1.8 -1.8 -1.9 -1.8 -2.3 -0.9 -1.8 -1.8 -1.8 -1.8 -0.5 -1.5 -1.2 -2.1 -1.8 -1.5Target 28.00 28.00 28.00 28.00 28.00 28.00 28.00 28.00 28.00 28.00 28.00 28.00 28.00 28.00 28.00 28.00Actual 15.60 16.30 16.40 16.10 17.40 17.40 16.30 17.00 15.70 16.00 17.00 16.10 17.30 18.10 17.30 17.40Variance -12.40 -11.70 -11.60 -11.90 -10.60 -10.60 -11.70 -11.00 -12.30 -12.00 -11.00 -11.90 -10.70 -9.90 -10.70 -10.60Target 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0Actual 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0Variance 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0Target 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00%Actual 97.71% 98.10% 98.93% 98.24% 98.33% 97.61% 96.90% 97.63% 98.09% 96.71% 94.00% 96.18% 96.38% 97.63% 97.18% 97.03%Variance 2.71% 3.10% 3.93% 3.24% 3.33% 2.61% 1.90% 2.63% 3.09% 1.71% -1.00% 1.18% 1.38% 2.63% 2.18% 1.38%
T00 Target 00:15 00:15 00:15 00:15 00:15 00:15 00:15 00:15 00:15 00:15 00:15 00:15 00:15 00:15
Actual 00:38 00:35 00:30 00:34 00:22 00:27 00:39 00:30 00:25 00:23 00:49 00:21 00:47 00:38
Variance 00:23 00:20 00:15 00:19 00:07 00:12 00:24 00:15 00:10 00:08 00:34 00:06 00:32 00:23
Median 00:05 00:06 00:06 00:06 00:05 00:05 00:07 00:06 00:06 00:06 00:07 00:06 00:07 00:07
T00 Target 01:00 01:00 01:00 01:00 01:00 01:00 01:00 01:00 01:00 01:00 01:00 01:00 01:00 01:00 01:00 01:00Actual 00:49 00:52 00:42 00:47 00:49 00:48 00:49 00:49 00:51 00:58 01:05 00:57 01:01 00:54 01:00 00:59Variance 00:11 00:08 00:18 00:13 00:11 00:12 00:11 00:11 00:09 00:02 00:05 00:03 00:01 00:06 00:00 00:01
T00 Target 5.00% 5.00% 5.00% 5.00% 5.00% 5.00% 5.00% 5.00% 5.00% 5.00% 5.00% 5.00% 5.00% 5.00% 5.00% 5.00%Actual 5.41% 4.95% 5.56% 5.30% 5.57% 6.67% 6.06% 6.09% 6.36% 4.21% 5.97% 6.02% 5.57% 5.83% 5.30% 5.36%Variance 0.41% -0.05% 0.56% 0.30% 0.57% 1.67% 1.06% 1.09% 1.36% -0.79% 0.97% 1.02% 0.57% 0.83% 0.30% 0.36%
T00 Target 5.00% 5.00% 5.00% 5.00% 5.00% 5.00% 5.00% 5.00% 5.00% 5.00% 5.00% 5.00% 5.00% 5.00%
Actual 2.48% 2.20% 1.85% 2.18% 2.07% 1.67% 2.07% 1.94% 1.62% 2.30% 3.06% 2.46% 1.96% 1.41%
Variance 2.52% 2.80% 3.15% 2.82% 2.93% 3.33% 2.93% 3.06% 3.38% 2.70% 1.94% 2.54% 3.04% 3.59%
T01 Target 04:00 04:00 04:00 04:00 04:00 04:00 04:00 04:00 04:00 04:00 04:00 04:00 04:00 04:00 04:00 04:00Actual 05:18 04:50 03:59 04:30 04:29 05:18 05:26 05:10 04:48 05:40 06:31 05:12 05:56 05:15 05:34 05:39Variance 00:30 01:10 01:12 01:39
T02 Target 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0Actual 2 2 1 5 0 1 6 7 2 1 53 56 46 20 31 97
Variance
T02 Target 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
Actual 0 0 0 0 0 0 0 0 0 0 4 4 4 1 0 5
Variance
T01 Target 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0Actual 0 0 0 0 0 0 0 0 0 0 0 0 1 0 0 1Variance
T00 Target 98.00% 98.00% 98.00% 98.00% 98.00% 98.00% 98.00% 98.00% 98.00% 98.00% 98.00% 98.00% 98.00% 98.00% 98.00% 98.00%Actual 100.00% 98.55% 100.00% 99.42% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00%Variance 2.00% 0.55% 2.00% 1.42% 2.00% 2.00% 2.00% 2.00% 2.00% 2.00% 2.00% 2.00% 2.00% 2.00% 2.00% 2.00%
T00 Target 94.00% 94.00% 94.00% 94.00% 94.00% 94.00% 94.00% 94.00% 94.00% 94.00% 94.00% 94.00% 94.00% 94.00% 94.00% 94.00%Actual 100.00% 100.00% 100.00% 100.00% 90.91% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 88.24% 100.00% 100.00% 94.59%Variance 6.00% 6.00% 6.00% 6.00% -3.09% 6.00% 6.00% 6.00% 6.00% 6.00% 6.00% 6.00% -5.76% 6.00% 6.00% -5.76%
T00 Target 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00%Actual No pts 66.67% 83.33% 77.78% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 66.67% 83.33% 100.00% 100.00% 100.00% 100.00%Variance -18.33% -1.67% 15.00% 15.00% 15.00% 15.00% 15.00% 15.00% -18.33% 15.00% 15.00% 15.00% 15.00% 15.00%
T00 Target 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00%Actual 95.65% 96.36% 98.11% 96.61% 96.15% 90.91% 100.00% 95.45% 100.00% 97.17% 97.01% 98.05% 97.18% 95.74% 100.00% 97.39%Variance 5.65% 6.36% 8.11% 6.61% 6.15% 0.91% 10.00% 5.45% 10.00% 7.17% 7.01% 5.45% 7.18% 5.74% 10.00% 7.18%
T00 Target 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00%Actual 84.69% 81.60% 89.92% 85.51% 86.40% 77.63% 86.79% 83.20% 87.80% 84.83% 92.59% 88.56% 90.70% 73.17% 93.88% 86.47%Variance -0.31% -3.40% 4.92% 0.51% 1.40% -7.37% 1.79% -1.80% 2.80% -0.17% 7.59% -1.80% 5.70% -11.83% 8.88% 5.70%
T00 Target 96.00% 96.00% 96.00% 96.00% 96.00% 96.00% 96.00% 96.00% 96.00% 96.00% 96.00% 96.00% 96.00% 96.00% 96.00% 96.00%Actual 100.00% 100.00% 99.11% 99.70% 98.13% 96.06% 97.89% 97.65% 98.55% 98.55% 99.18% 98.30% 97.01% 100.00% 99.13% 98.66%Variance 4.00% 4.00% 3.11% 3.70% 2.13% 0.06% 1.89% 1.65% 2.55% 2.55% 3.18% 1.65% 1.01% 4.00% 3.13% 1.01%
T00 Target 93.00% 93.00% 93.00% 93.00% 93.00% 93.00% 93.00% 93.00% 93.00% 93.00% 93.00% 93.00% 93.00% 93.00% 93.00% 93.00%Actual 89.57% 93.08% 92.61% 91.86% 93.18% 93.46% 94.92% 93.84% 95.53% 93.08% 94.65% 94.43% 95.83% 96.40% 93.48% 95.19%Variance -3.43% 0.08% -0.39% -1.14% 0.18% 0.46% 1.92% 0.84% 2.53% 0.08% 1.65% 0.84% 2.83% 3.40% 0.48% 2.83%
T00 Target 93.00% 93.00% 93.00% 93.00% 93.00% 93.00% 93.00% 93.00% 93.00% 93.00% 93.00% 93.00% 93.00% 93.00% 93.00% 93.00%
Actual 90.75% 94.55% 95.54% 94.00% 98.22% 95.74% 97.67% 97.24% 98.27% 96.72% 96.68% 97.29% 99.13% 98.33% 97.95% 98.46%
Variance -2.25% 1.55% 2.54% 1.00% 5.22% 2.74% 4.67% 4.24% 5.27% 3.72% 3.68% 4.24% 6.13% 5.33% 4.95% 6.13%* Data collection, validation and reporting processes prevent these standards from achieving a more timely result
** Data extracted directly from Trak, further validation has been undertaken on 14/07/2017 with amendments to May, June and Q1
***Validated position
Provisional
T00
12RTT incomplete pathways wait (92%)
T00
80RTT incomplete pathways wait (Median)
A&E left without being seen - Type 1
T00
83RTT incomplete pathways wait (92nd percentile)
T01
15RTT incomplete pathways >52 week wait
T00
01Emergency Care 4 hr standard
A&E Time to Initial Assessment -Ambulance
arrivals (95th percentile) - Type 1
A&E Time to Initial Treatment (Median) - Type 1
A&E unplanned returns within 7 days - Type 1
Breast Symptomatic Two week Rule (New Rules)*
A&E Time to departure (95th percentile) - Type 1 **
Number of ambulance handovers between
ambulance and A&E waiting more than 30
minutes***Number of ambulance handovers between
ambulance and A&E waiting more than 60
minutes***
A&E 12 Hour Trolley waits - Type 1
New Cancer 31 days subsequent Treatment (Drug
Therapy)*
New Cancer 31 days subsequent Treatment
(Surgery)*
New Cancer 62 days (consultant upgrade)*
New Cancer 62 days (screening)*
New Cancer GP 62 Day (New Rules)*
New Cancer Current 31 Day (New Rules)*
New Cancer Two week Rule (New Rules)*
Appendix 1 - Single Oversight Framework (Index 1) Menu
Draft
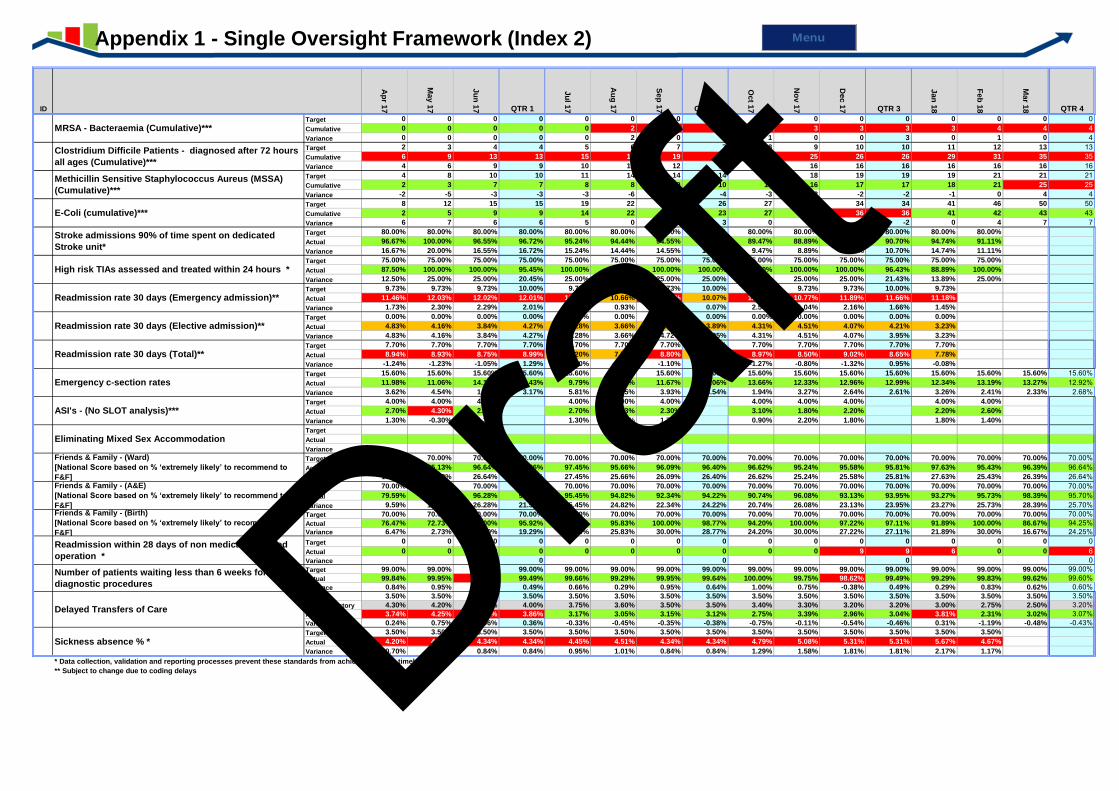
ID
Ap
r 17
May 1
7
Ju
n 1
7 QTR 1
Ju
l 17
Au
g 1
7
Sep
17 QTR 2
Oct 1
7
No
v 1
7
Dec 1
7 QTR 3
Jan
18
Feb
18
Mar 1
8 QTR 4
Target 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0Cumulative 0 0 0 0 0 2 2 2 3 3 3 3 3 4 4 4Variance 0 0 0 0 0 2 0 2 1 0 0 3 0 1 0 4Target 2 3 4 4 5 6 7 7 8 9 10 10 11 12 13 13Cumulative 6 9 13 13 15 19 19 19 20 25 26 26 29 31 35 35Variance 4 6 9 9 10 13 12 12 12 16 16 16 16 16 16 16Target 4 8 10 10 11 14 14 14 16 18 19 19 19 21 21 21Cumulative 2 3 7 7 8 8 10 10 13 16 17 17 18 21 25 25Variance -2 -5 -3 -3 -3 -6 -4 -4 -3 -2 -2 -2 -1 0 4 4Target 8 12 15 15 19 22 26 26 27 33 34 34 41 46 50 50Cumulative 2 5 9 9 14 22 23 23 27 33 36 36 41 42 43 43Variance 6 7 6 6 5 0 3 3 0 0 -2 -2 0 4 7 7Target 80.00% 80.00% 80.00% 80.00% 80.00% 80.00% 80.00% 80.00% 80.00% 80.00% 80.00% 80.00% 80.00% 80.00%
Actual 96.67% 100.00% 96.55% 96.72% 95.24% 94.44% 94.55% 94.70% 89.47% 88.89% 93.48% 90.70% 94.74% 91.11%
Variance 16.67% 20.00% 16.55% 16.72% 15.24% 14.44% 14.55% 14.70% 9.47% 8.89% 13.48% 10.70% 14.74% 11.11%
Target 75.00% 75.00% 75.00% 75.00% 75.00% 75.00% 75.00% 75.00% 75.00% 75.00% 75.00% 75.00% 75.00% 75.00%
Actual 87.50% 100.00% 100.00% 95.45% 100.00% 75.00% 100.00% 100.00% 90.00% 100.00% 100.00% 96.43% 88.89% 100.00%
Variance 12.50% 25.00% 25.00% 20.45% 25.00% 0.00% 25.00% 25.00% 15.00% 25.00% 25.00% 21.43% 13.89% 25.00%
Target 9.73% 9.73% 9.73% 10.00% 9.73% 9.73% 9.73% 10.00% 9.73% 9.73% 9.73% 10.00% 9.73%
Actual 11.46% 12.03% 12.02% 12.01% 11.07% 10.66% 11.57% 10.07% 12.27% 10.77% 11.89% 11.66% 11.18%
Variance 1.73% 2.30% 2.29% 2.01% 1.34% 0.93% 1.84% 0.07% 2.54% 1.04% 2.16% 1.66% 1.45%
Target 0.00% 0.00% 0.00% 0.00% 0.00% 0.00% 0.00% 0.00% 0.00% 0.00% 0.00% 0.00% 0.00%
Actual 4.83% 4.16% 3.84% 4.27% 3.28% 3.66% 4.72% 3.89% 4.31% 4.51% 4.07% 4.21% 3.23%
Variance 4.83% 4.16% 3.84% 4.27% 3.28% 3.66% 4.72% 3.95% 4.31% 4.51% 4.07% 3.95% 3.23%
Target 7.70% 7.70% 7.70% 7.70% 7.70% 7.70% 7.70% 7.70% 7.70% 7.70% 7.70% 7.70% 7.70%
Actual 8.94% 8.93% 8.75% 8.99% 8.20% 7.77% 8.80% 8.26% 8.97% 8.50% 9.02% 8.65% 7.78%
Variance -1.24% -1.23% -1.05% 1.29% -0.50% -0.07% -1.10% 0.56% -1.27% -0.80% -1.32% 0.95% -0.08%
Target 15.60% 15.60% 15.60% 15.60% 15.60% 15.60% 15.60% 15.60% 15.60% 15.60% 15.60% 15.60% 15.60% 15.60% 15.60% 15.60%Actual 11.98% 11.06% 14.17% 12.43% 9.79% 14.85% 11.67% 12.06% 13.66% 12.33% 12.96% 12.99% 12.34% 13.19% 13.27% 12.92%Variance 3.62% 4.54% 1.43% 3.17% 5.81% 0.75% 3.93% 3.54% 1.94% 3.27% 2.64% 2.61% 3.26% 2.41% 2.33% 2.68%Target 4.00% 4.00% 4.00% 4.00% 4.00% 4.00% 4.00% 4.00% 4.00% 4.00% 4.00%
Actual 2.70% 4.30% 2.70% 2.70% 3.33% 2.30% 3.10% 1.80% 2.20% 2.20% 2.60%
Variance 1.30% -0.30% 1.30% 1.30% 0.67% 1.70% 0.90% 2.20% 1.80% 1.80% 1.40%
Target
Actual 0.00% 0.00% 0.00% 0.00% 0.00% 0.00% 0.00% 0.00% 0.00% 0.00% 0.00% 0.00% 0.00% 0.00% 0.00% 0.00%Variance
Target 70.00% 70.00% 70.00% 70.00% 70.00% 70.00% 70.00% 70.00% 70.00% 70.00% 70.00% 70.00% 70.00% 70.00% 70.00% 70.00%Actual 83.78% 85.13% 96.64% 96.36% 97.45% 95.66% 96.09% 96.40% 96.62% 95.24% 95.58% 95.81% 97.63% 95.43% 96.39% 96.64%Variance 13.78% 15.13% 26.64% 22.20% 27.45% 25.66% 26.09% 26.40% 26.62% 25.24% 25.58% 25.81% 27.63% 25.43% 26.39% 26.64%Target 70.00% 70.00% 70.00% 70.00% 70.00% 70.00% 70.00% 70.00% 70.00% 70.00% 70.00% 70.00% 70.00% 70.00% 70.00% 70.00%Actual 79.59% 81.05% 96.28% 94.88% 95.45% 94.82% 92.34% 94.22% 90.74% 96.08% 93.13% 93.95% 93.27% 95.73% 98.39% 95.70%Variance 9.59% 11.05% 26.28% 21.57% 25.45% 24.82% 22.34% 24.22% 20.74% 26.08% 23.13% 23.95% 23.27% 25.73% 28.39% 25.70%Target 70.00% 70.00% 70.00% 70.00% 70.00% 70.00% 70.00% 70.00% 70.00% 70.00% 70.00% 70.00% 70.00% 70.00% 70.00% 70.00%Actual 76.47% 72.73% 100.00% 95.92% 100.00% 95.83% 100.00% 98.77% 94.20% 100.00% 97.22% 97.11% 91.89% 100.00% 86.67% 94.25%Variance 6.47% 2.73% 30.00% 19.29% 30.00% 25.83% 30.00% 28.77% 24.20% 30.00% 27.22% 27.11% 21.89% 30.00% 16.67% 24.25%Target 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0Actual 0 0 0 0 0 0 0 0 0 0 9 9 6 0 0 6Variance 0 0 0 0Target 99.00% 99.00% 99.00% 99.00% 99.00% 99.00% 99.00% 99.00% 99.00% 99.00% 99.00% 99.00% 99.00% 99.00% 99.00% 99.00%Actual 99.84% 99.95% 98.76% 99.49% 99.66% 99.29% 99.95% 99.64% 100.00% 99.75% 98.62% 99.49% 99.29% 99.83% 99.62% 99.60%Variance 0.84% 0.95% -0.24% 0.49% 0.66% 0.29% 0.95% 0.64% 1.00% 0.75% -0.38% 0.49% 0.29% 0.83% 0.62% 0.60%Target 3.50% 3.50% 3.50% 3.50% 3.50% 3.50% 3.50% 3.50% 3.50% 3.50% 3.50% 3.50% 3.50% 3.50% 3.50% 3.50%NHSI Trajectory 4.30% 4.20% 4.00% 4.00% 3.75% 3.60% 3.50% 3.50% 3.40% 3.30% 3.20% 3.20% 3.00% 2.75% 2.50% 3.20%Actual 3.74% 4.25% 3.56% 3.86% 3.17% 3.05% 3.15% 3.12% 2.75% 3.39% 2.96% 3.04% 3.81% 2.31% 3.02% 3.07%Variance 0.24% 0.75% 0.06% 0.36% -0.33% -0.45% -0.35% -0.38% -0.75% -0.11% -0.54% -0.46% 0.31% -1.19% -0.48% -0.43%Target 3.50% 3.50% 3.50% 3.50% 3.50% 3.50% 3.50% 3.50% 3.50% 3.50% 3.50% 3.50% 3.50% 3.50%
Actual 4.20% 4.07% 4.34% 4.34% 4.45% 4.51% 4.34% 4.34% 4.79% 5.08% 5.31% 5.31% 5.67% 4.67%
Variance 0.70% 0.57% 0.84% 0.84% 0.95% 1.01% 0.84% 0.84% 1.29% 1.58% 1.81% 1.81% 2.17% 1.17%
* Data collection, validation and reporting processes prevent these standards from achieving a more timely result
** Subject to change due to coding delays
T00
16MRSA - Bacteraemia (Cumulative)***
T00
17
Clostridium Difficile Patients - diagnosed after 72 hours
all ages (Cumulative)***
T00
37
Methicillin Sensitive Staphylococcus Aureus (MSSA)
(Cumulative)***
T00
38E-Coli (cumulative)***
T00
93
Stroke admissions 90% of time spent on dedicated
Stroke unit*
T00
94High risk TIAs assessed and treated within 24 hours *
T00
25Readmission rate 30 days (Emergency admission)**
T00
26Readmission rate 30 days (Elective admission)**
T01
19Readmission rate 30 days (Total)**
T02
08Emergency c-section rates
T00
95ASI's - (No SLOT analysis)***
T00
18Eliminating Mixed Sex Accommodation
T01
21
Friends & Family - (Ward)
[National Score based on % ‘extremely likely’ to recommend to
F&F]
T01
22
Friends & Family - (A&E)
[National Score based on % ‘extremely likely’ to recommend to
F&F]
T01
23
Friends & Family - (Birth)
[National Score based on % ‘extremely likely’ to recommend to
F&F]
T01
00
Readmission within 28 days of non medical cancelled
operation *
T01
16
Number of patients waiting less than 6 weeks for
diagnostic procedures
T00
74Sickness absence % *
T01
03Delayed Transfers of Care
Appendix 1 - Single Oversight Framework (Index 2)
Menu
Draft
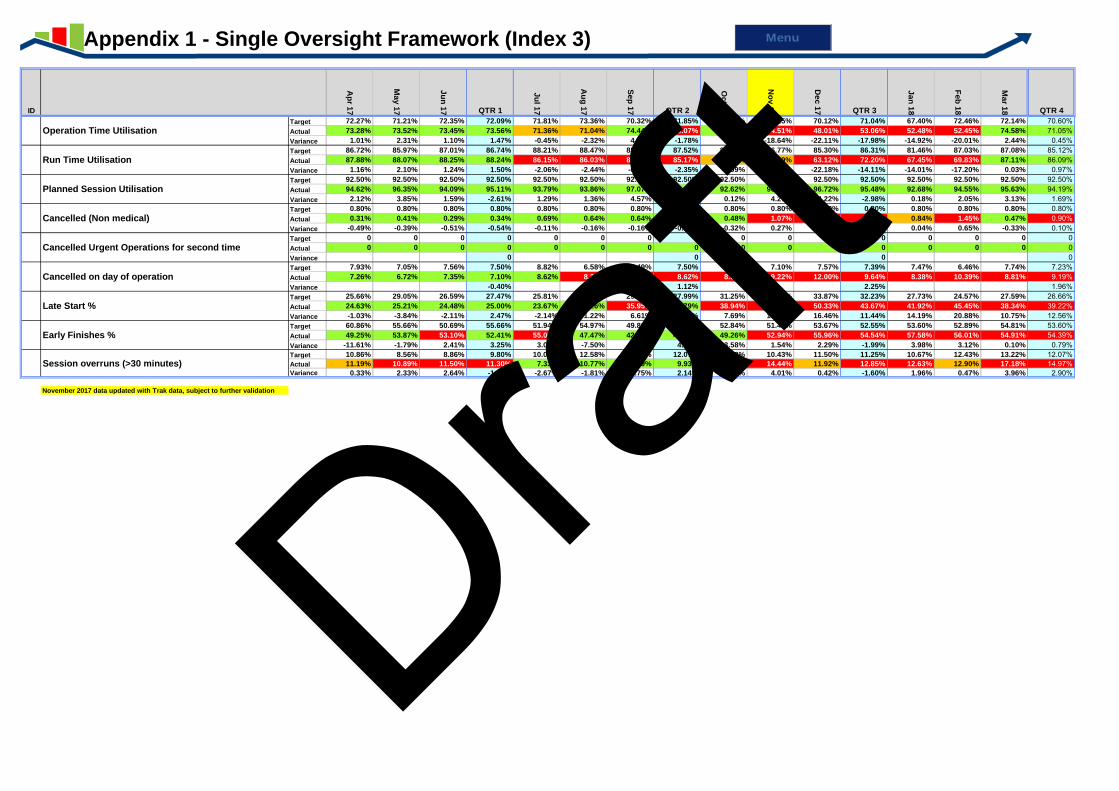
ID
Ap
r 17
Ma
y 1
7
Ju
n 1
7 QTR 1
Ju
l 17
Au
g 1
7
Se
p 1
7 QTR 2
Oc
t 17
No
v 1
7
Dec
17 QTR 3
Ja
n 1
8
Fe
b 1
8
Ma
r 18 QTR 4
Target 72.27% 71.21% 72.35% 72.09% 71.81% 73.36% 70.32% 71.85% 72.40% 73.15% 70.12% 71.04% 67.40% 72.46% 72.14% 70.60%Actual 73.28% 73.52% 73.45% 73.56% 71.36% 71.04% 74.44% 70.07% 74.60% 54.51% 48.01% 53.06% 52.48% 52.45% 74.58% 71.05%Variance 1.01% 2.31% 1.10% 1.47% -0.45% -2.32% 4.12% -1.78% 2.20% -18.64% -22.11% -17.98% -14.92% -20.01% 2.44% 0.45%Target 86.72% 85.97% 87.01% 86.74% 88.21% 88.47% 85.78% 87.52% 86.57% 86.77% 85.30% 86.31% 81.46% 87.03% 87.08% 85.12%Actual 87.88% 88.07% 88.25% 88.24% 86.15% 86.03% 85.37% 85.17% 86.48% 82.29% 63.12% 72.20% 67.45% 69.83% 87.11% 86.09%Variance 1.16% 2.10% 1.24% 1.50% -2.06% -2.44% -0.41% -2.35% -0.09% -4.48% -22.18% -14.11% -14.01% -17.20% 0.03% 0.97%Target 92.50% 92.50% 92.50% 92.50% 92.50% 92.50% 92.50% 92.50% 92.50% 92.50% 92.50% 92.50% 92.50% 92.50% 92.50% 92.50%Actual 94.62% 96.35% 94.09% 95.11% 93.79% 93.86% 97.07% 94.96% 92.62% 96.77% 96.72% 95.48% 92.68% 94.55% 95.63% 94.19%Variance 2.12% 3.85% 1.59% -2.61% 1.29% 1.36% 4.57% -2.46% 0.12% 4.27% 4.22% -2.98% 0.18% 2.05% 3.13% 1.69%Target 0.80% 0.80% 0.80% 0.80% 0.80% 0.80% 0.80% 0.80% 0.80% 0.80% 0.80% 0.80% 0.80% 0.80% 0.80% 0.80%Actual 0.31% 0.41% 0.29% 0.34% 0.69% 0.64% 0.64% 0.66% 0.48% 1.07% 1.46% 0.98% 0.84% 1.45% 0.47% 0.90%Variance -0.49% -0.39% -0.51% -0.54% -0.11% -0.16% -0.16% -0.14% -0.32% 0.27% 0.66% 0.18% 0.04% 0.65% -0.33% 0.10%Target 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0Actual 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0Variance 0 0 0 0Target 7.93% 7.05% 7.56% 7.50% 8.82% 6.58% 7.49% 7.50% 7.55% 7.10% 7.57% 7.39% 7.47% 6.46% 7.74% 7.23%Actual 7.26% 6.72% 7.35% 7.10% 8.62% 8.23% 8.91% 8.62% 8.30% 9.22% 12.00% 9.64% 8.38% 10.39% 8.81% 9.19%Variance -0.40% 1.12% 2.25% 1.96%Target 25.66% 29.05% 26.59% 27.47% 25.81% 27.48% 29.34% 27.99% 31.25% 31.81% 33.87% 32.23% 27.73% 24.57% 27.59% 26.66%Actual 24.63% 25.21% 24.48% 25.00% 23.67% 26.26% 35.95% 27.79% 38.94% 42.25% 50.33% 43.67% 41.92% 45.45% 38.34% 39.22%Variance -1.03% -3.84% -2.11% 2.47% -2.14% -1.22% 6.61% 0.20% 7.69% 10.44% 16.46% 11.44% 14.19% 20.88% 10.75% 12.56%Target 60.86% 55.66% 50.69% 55.66% 51.94% 54.97% 49.86% 52.65% 52.84% 51.40% 53.67% 52.55% 53.60% 52.89% 54.81% 53.60%Actual 49.25% 53.87% 53.10% 52.41% 55.00% 47.47% 42.14% 48.57% 49.26% 52.94% 55.96% 54.54% 57.58% 56.01% 54.91% 54.39%Variance -11.61% -1.79% 2.41% 3.25% 3.06% -7.50% -7.72% 4.08% -3.58% 1.54% 2.29% -1.99% 3.98% 3.12% 0.10% 0.79%Target 10.86% 8.56% 8.86% 9.80% 10.00% 12.58% 12.54% 12.07% 11.93% 10.43% 11.50% 11.25% 10.67% 12.43% 13.22% 12.07%Actual 11.19% 10.89% 11.50% 11.30% 7.33% 10.77% 11.79% 9.93% 14.75% 14.44% 11.92% 12.85% 12.63% 12.90% 17.18% 14.97%Variance 0.33% 2.33% 2.64% -1.50% -2.67% -1.81% -0.75% 2.14% 2.82% 4.01% 0.42% -1.60% 1.96% 0.47% 3.96% 2.90%
Theatre data from Sep-17 unvalidated, because of system changeover from Theatreman to TrakCare
November 2017 data updated with Trak data, subject to further validation
T00
67Operation Time Utilisation
T00
68Run Time Utilisation
T01
82Planned Session Utilisation
T00
71Cancelled (Non medical)
T01
18Cancelled Urgent Operations for second time
T00
70Cancelled on day of operation
T00
64Late Start %
T00
65Early Finishes %
T00
66Session overruns (>30 minutes)
Appendix 1 - Single Oversight Framework (Index 3)
Menu
Draft

ID
Ap
r 17
Ma
y 1
7
Ju
n 1
7 QTR 1
Ju
l 17
Au
g 1
7
Se
p 1
7 QTR 2
Oc
t 17
No
v 1
7
Dec
17 QTR 3
Ja
n 1
8
Fe
b 1
8
Ma
r 18 QTR 4
Target 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00%Actual 100.21% 99.87% 99.72% 99.94% 100.29% 99.93% 99.88% 100.03% 100.27% 100.23% 98.35% 99.67% 98.42% 98.24% 98.42% 98.36%Variance 5.21% 4.87% 4.72% 4.94% 5.29% 4.93% 4.88% 5.03% 5.27% 5.23% 3.35% 4.67% 3.42% 3.24% 3.42% 3.36%
Target 17.00% 17.00% 17.00% 17.00% 17.00% 17.00% 17.00% 17.00% 17.00% 17.00% 17.00% 17.00% 17.00% 17.00% 17.00% 17.00%
Actual 26.11% 18.08% 22.90% 22.35% 21.98% 22.12% 16.94% 21.76% 21.71% 17.02% 12.62% 17.24% 23.59% 20.54% 22.71% 21.62%
Variance 9.11% 1.08% 5.90% 5.35% 4.98% 5.12% -0.06% 4.76% 4.71% 0.02% -4.38% 0.24% 6.59% 3.54% 5.71% 4.62%Target 93.50% 93.50% 93.50% 93.50% 93.50% 93.50% 93.50% 95.00% 93.50% 93.50% 93.50% 95.00% 93.50% 93.50% 93.50% 95.00%Actual 93.00% 100.00% 100.00% 97.56% 98.60% 100.00% 100.00% 99.54% 100.00% 96.82% 95.40% 97.50% 99.00% 100.00% 98.80% 97.50%Variance -0.50% 6.50% 6.50% 5.10% 6.50% 6.50% 4.54% 6.50% 3.32% 1.90% 2.50% 5.50% 6.50% 5.30% 2.50%Target 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00%Actual 83.19% 78.65% 74.57% 78.30% 69.29% 71.04% 70.49% 70.34% 72.09% 95.68% 98.15% 88.72% 94.90% 97.76% 85.95% 93.43%Variance -6.81% -11.35% -15.43% -11.70% -20.71% -18.96% -19.51% -19.66% -17.91% 5.68% 8.15% -1.28% 4.90% 7.76% -4.05% 3.43%Target 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00%
Actual 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 99.46% 99.85% 100.00% 99.66%
Variance 5.00% 5.00% 5.00% 5.00% 5.00% 5.00% 5.00% 5.00% 5.00% 4.46% 5.00% 5.00% 4.66% 0.00%
Target 18.30 18.30 18.30 18.3 18.30 18.30 18.30 18.3 18.30 18.30 18.30 18.3 18.30 18.30
Actual 4.00 4.00 4.00 4.00 5.00 5.00 4.00 4.00 4.00 2.00 5.00 4.00 4.00 4.00
Variance -14.30 -14.30 -14.30 14.3 -13.30 -13.30 -14.30 14.3 -14.30 -16.30 -13.30 14.3 -14.30 -14.30
Target 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00%
Actual 96.82% 96.42% 95.98% 96.42% 97.48% 95.74% 96.70% 96.65% 97.97% 96.92% 96.77% 97.26% 96.59% 96.56%
Variance 46.82% 46.42% 45.98% 46.42% 47.48% 45.74% 46.70% 46.65% 47.97% 46.92% 46.77% 46.65% 46.59% 46.56%
Target 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00%
Actual 95.56% 95.73% 96.51% 95.96% 96.75% 97.38% 96.35% 96.85% 97.81% 96.82% 96.22% 96.98% 95.98% 95.96%
Variance 45.56% 45.73% 46.51% 45.96% 46.75% 47.38% 46.35% 46.85% 47.81% 46.82% 46.22% 46.85% 45.98% 45.96%
Target 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00%
Actual 97.25% 94.74% 95.28% 95.70% 95.65% 95.83% 95.01% 95.50% 97.61% 95.48% 95.00% 96.06% 94.81% 95.70%
Variance 47.25% 44.74% 45.28% 45.70% 45.65% 45.83% 45.01% 45.50% 47.61% 45.48% 45.00% 45.50% 44.81% 45.70%
Target 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00%
Actual 97.25% 94.74% 95.28% 95.22% 95.65% 95.83% 95.01% 95.50% 97.61% 95.48% 95.00% 96.06% 94.81% 95.70%
Variance 47.25% 44.74% 45.28% 45.22% 45.65% 45.83% 45.01% 45.50% 47.61% 45.48% 45.00% 46.06% 44.81% 45.70%
Target 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00%
Actual 86.62% 86.17% 83.33% 86.10% 88.79% 86.72% 80.00% 85.03% 84.82% 84.51% 85.71% 85.07% 86.02% 85.71%
Variance 36.62% 36.17% 33.33% 36.10% 38.79% 36.72% 30.00% 35.03% 34.82% 34.51% 35.71% 35.07% 36.02% 35.71%
* Data collection, validation and reporting processes prevent these standards from achieving a more timely result
** Percentage greater than 100% possible, when total number of appointments offered exceeds the number of patients (please note September and Qtr 2 position updated)
T01
11Diabetic Retinopathy Screening **
T01
84
TCS 19 - % of Community Patients that have had an
unplanned admission LOS <=2 days (Defined set of
conditions)
T01
85
TCS 24 - % of Patients achieving improvement using a
EQ5 validated assessment tool
T01
86
TCS 35 - % of standard wheelchair referrals completed
within five days
T00
84
The % patients treated within 18 weeks of referral to
audiology (Hpool site)
T00
85Audiology non admitted wait (92nd percentile)
T00
13CIDs- Referral to Treatment information*
T00
14CIDs -Referral information*
T00
15CIDs- Treatment Activity Information*
T01
05Patient Identifier Indicator *
T01
06End of Life measure *
Appendix 1 - Out of Hospital Monitoring Framework (Index 4)
Menu
Draft
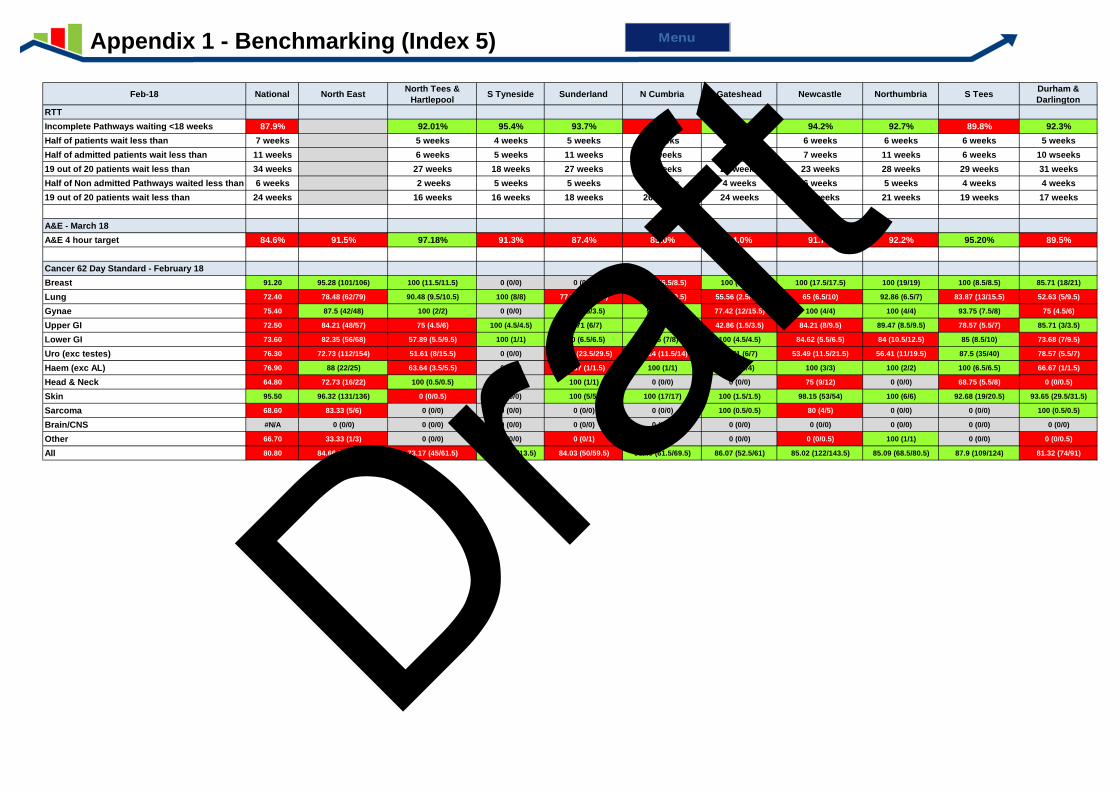
Feb-18 National North EastNorth Tees &
HartlepoolS Tyneside Sunderland N Cumbria Gateshead Newcastle Northumbria S Tees
Durham &
Darlington
RTT
Incomplete Pathways waiting <18 weeks 87.9% 92.01% 95.4% 93.7% 85.1% 93.7% 94.2% 92.7% 89.8% 92.3%
Half of patients wait less than 7 weeks 5 weeks 4 weeks 5 weeks 9 weeks 6 weeks 6 weeks 6 weeks 6 weeks 5 weeks
Half of admitted patients wait less than 11 weeks 6 weeks 5 weeks 11 weeks 14 weeks 13 weeks 7 weeks 11 weeks 6 weeks 10 wseeks
19 out of 20 patients wait less than 34 weeks 27 weeks 18 weeks 27 weeks 43 weeks 28 weeks 23 weeks 28 weeks 29 weeks 31 weeks
Half of Non admitted Pathways waited less than 6 weeks 2 weeks 5 weeks 5 weeks 7 weeks 4 weeks 6 weeks 5 weeks 4 weeks 4 weeks
19 out of 20 patients wait less than 24 weeks 16 weeks 16 weeks 18 weeks 26 weeks 24 weeks 18 weeks 21 weeks 19 weeks 17 weeks
A&E - March 18
A&E 4 hour target 84.6% 91.5% 97.18% 91.3% 87.4% 85.0% 94.0% 91.7% 92.2% 95.20% 89.5%
Cancer 62 Day Standard - February 18
Breast 91.20 95.28 (101/106) 100 (11.5/11.5) 0 (0/0) 0 (0/0) 76.47 (6.5/8.5) 100 (20/20) 100 (17.5/17.5) 100 (19/19) 100 (8.5/8.5) 85.71 (18/21)
Lung 72.40 78.48 (62/79) 90.48 (9.5/10.5) 100 (8/8) 77.78 (3.5/4.5) 78.95 (7.5/9.5) 55.56 (2.5/4.5) 65 (6.5/10) 92.86 (6.5/7) 83.87 (13/15.5) 52.63 (5/9.5)
Gynae 75.40 87.5 (42/48) 100 (2/2) 0 (0/0) 100 (3.5/3.5) 90 (4.5/5) 77.42 (12/15.5) 100 (4/4) 100 (4/4) 93.75 (7.5/8) 75 (4.5/6)
Upper GI 72.50 84.21 (48/57) 75 (4.5/6) 100 (4.5/4.5) 85.71 (6/7) 100 (6.5/6.5) 42.86 (1.5/3.5) 84.21 (8/9.5) 89.47 (8.5/9.5) 78.57 (5.5/7) 85.71 (3/3.5)
Lower GI 73.60 82.35 (56/68) 57.89 (5.5/9.5) 100 (1/1) 100 (6.5/6.5) 87.5 (7/8) 100 (4.5/4.5) 84.62 (5.5/6.5) 84 (10.5/12.5) 85 (8.5/10) 73.68 (7/9.5)
Uro (exc testes) 76.30 72.73 (112/154) 51.61 (8/15.5) 0 (0/0) 79.66 (23.5/29.5) 82.14 (11.5/14) 85.71 (6/7) 53.49 (11.5/21.5) 56.41 (11/19.5) 87.5 (35/40) 78.57 (5.5/7)
Haem (exc AL) 76.90 88 (22/25) 63.64 (3.5/5.5) 0 (0/0) 66.67 (1/1.5) 100 (1/1) 100 (4/4) 100 (3/3) 100 (2/2) 100 (6.5/6.5) 66.67 (1/1.5)
Head & Neck 64.80 72.73 (16/22) 100 (0.5/0.5) 0 (0/0) 100 (1/1) 0 (0/0) 0 (0/0) 75 (9/12) 0 (0/0) 68.75 (5.5/8) 0 (0/0.5)
Skin 95.50 96.32 (131/136) 0 (0/0.5) 0 (0/0) 100 (5/5) 100 (17/17) 100 (1.5/1.5) 98.15 (53/54) 100 (6/6) 92.68 (19/20.5) 93.65 (29.5/31.5)
Sarcoma 68.60 83.33 (5/6) 0 (0/0) 0 (0/0) 0 (0/0) 0 (0/0) 100 (0.5/0.5) 80 (4/5) 0 (0/0) 0 (0/0) 100 (0.5/0.5)
Brain/CNS #N/A 0 (0/0) 0 (0/0) 0 (0/0) 0 (0/0) 0 (0/0) 0 (0/0) 0 (0/0) 0 (0/0) 0 (0/0) 0 (0/0)
Other 66.70 33.33 (1/3) 0 (0/0) 0 (0/0) 0 (0/1) 0 (0/0) 0 (0/0) 0 (0/0.5) 100 (1/1) 0 (0/0) 0 (0/0.5)
All 80.80 84.66 (596/704) 73.17 (45/61.5) 100 (13.5/13.5) 84.03 (50/59.5) 88.49 (61.5/69.5) 86.07 (52.5/61) 85.02 (122/143.5) 85.09 (68.5/80.5) 87.9 (109/124) 81.32 (74/91)
Appendix 1 - Benchmarking (Index 5) Menu
Draft
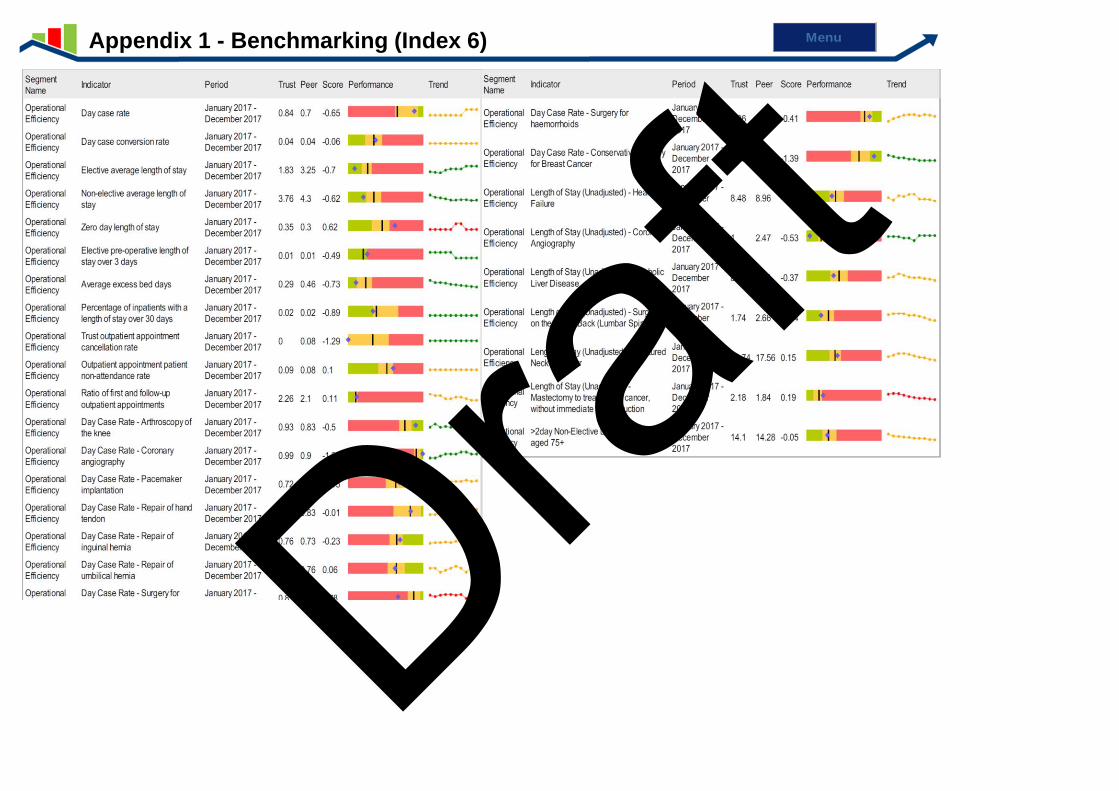
Appendix 1 - Benchmarking (Index 6) Menu
Draft
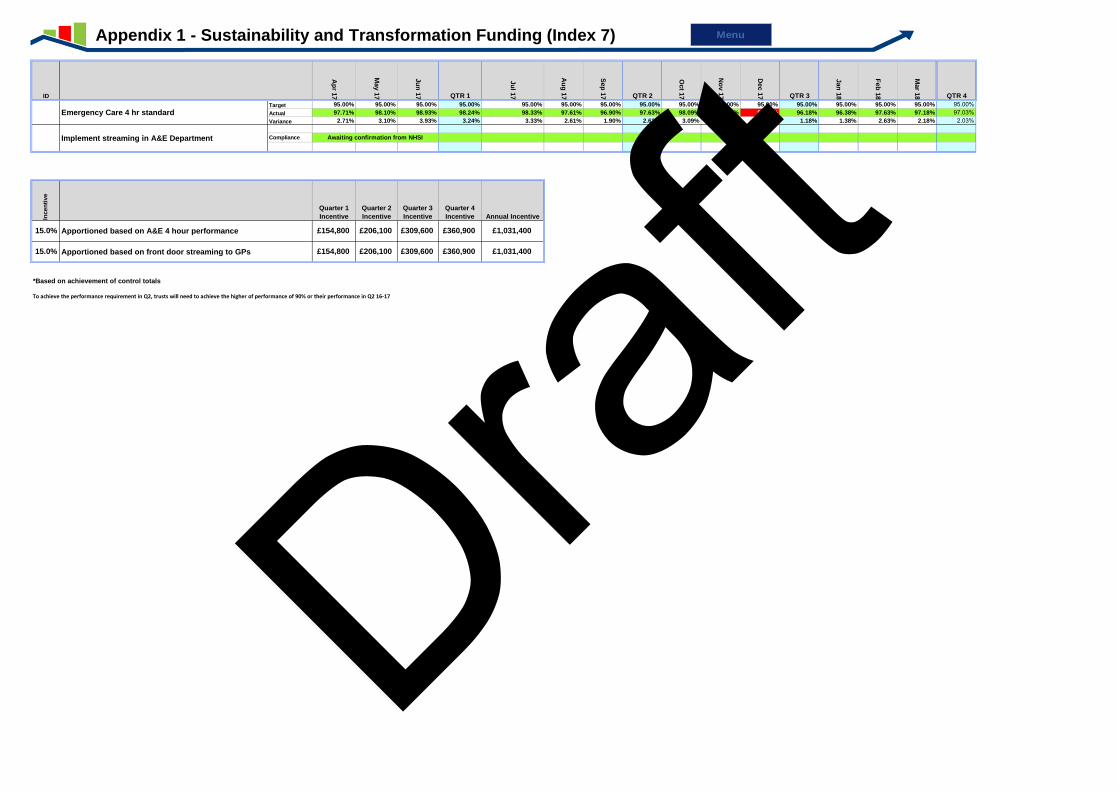
ID
Ap
r 17
May 1
7
Ju
n 1
7 QTR 1
Ju
l 17
Au
g 1
7
Sep
17 QTR 2
Oct 1
7
No
v 1
7
Dec 1
7 QTR 3
Jan
18
Feb
18
Mar 1
8 QTR 4
Target 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00%Actual 97.71% 98.10% 98.93% 98.24% 98.33% 97.61% 96.90% 97.63% 98.09% 96.71% 94.00% 96.18% 96.38% 97.63% 97.18% 97.03%Variance 2.71% 3.10% 3.93% 3.24% 3.33% 2.61% 1.90% 2.63% 3.09% 1.71% -1.00% 1.18% 1.38% 2.63% 2.18% 2.03%Target
Compliance
Variance
Incen
tive
Quarter 1
Incentive
Quarter 2
Incentive
Quarter 3
Incentive
Quarter 4
Incentive Annual Incentive
*Based on achievement of control totals
To achieve the performance requirement in Q2, trusts will need to achieve the higher of performance of 90% or their performance in Q2 16-17
Awaiting confirmation from NHSI
T0001 Emergency Care 4 hr standard
T0211 Implement streaming in A&E Department
£1,031,400
15.0% Apportioned based on front door streaming to GPs £154,800 £206,100 £309,600 £360,900 £1,031,400
15.0% Apportioned based on A&E 4 hour performance £154,800 £206,100 £309,600 £360,900
Appendix 1 - Sustainability and Transformation Funding (Index 7) Menu
Draft
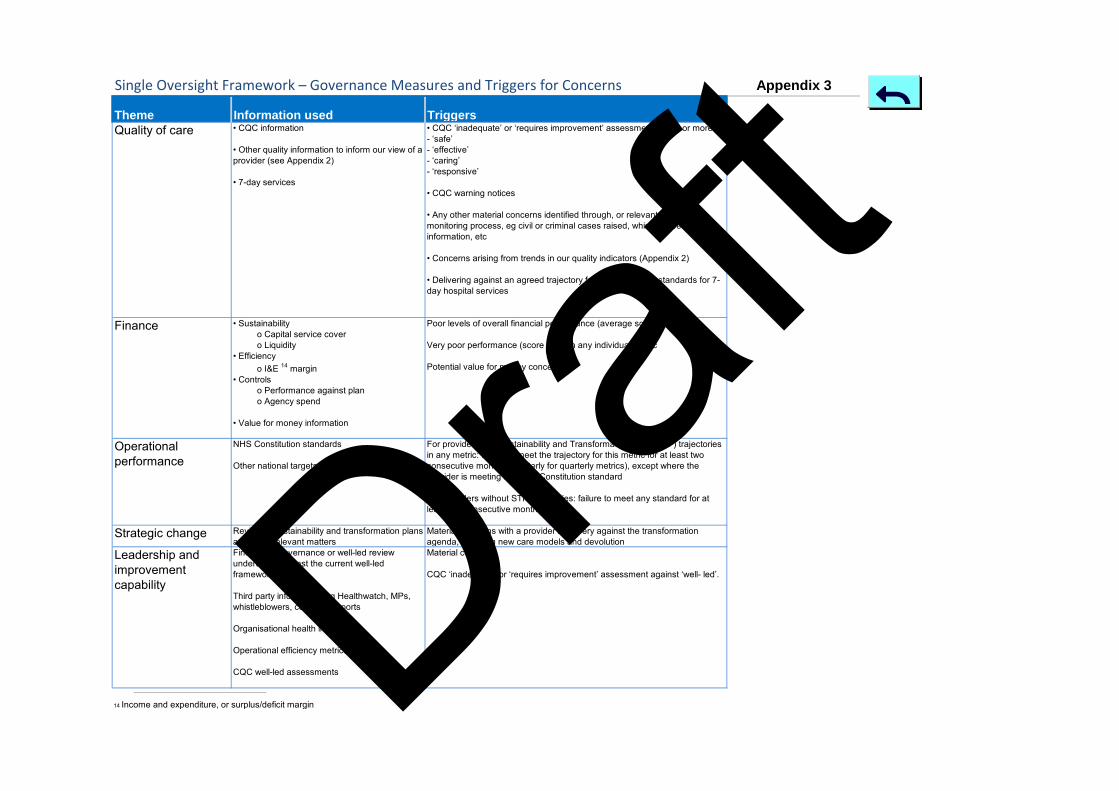
Single Oversight Framework – Governance Measures and Triggers for Concerns
Theme Information used Triggers
Quality of care • CQC information
• Other quality information to inform our view of a
provider (see Appendix 2)
• 7-day services
• CQC ‘inadequate’ or ‘requires improvement’ assessment in one or more of:
- ‘safe’
- ‘effective’
- ‘caring’
- ‘responsive’
• CQC warning notices
• Any other material concerns identified through, or relevant to, CQC’s
monitoring process, eg civil or criminal cases raised, whistleblower information, etc
• Concerns arising from trends in our quality indicators (Appendix 2)
• Delivering against an agreed trajectory for the four priority standards for 7-
day hospital services
Finance • Sustainability
o Capital service cover o Liquidity• Efficiency
o I&E 14 margin• Controls
o Performance against plan o Agency spend
• Value for money information
Poor levels of overall financial performance (average score of 3 or 4)
Very poor performance (score of 4) in any individual metric
Potential value for money concerns
Operational performance
NHS Constitution standards
Other national targets and standards
For providers with Sustainability and Transformation Fund (STF) trajectories in any metric: failure to meet the trajectory for this metric for at least two consecutive months (quarterly for quarterly metrics), except where the provider is meeting the NHS Constitution standard
For providers without STF trajectories: failure to meet any standard for at least two consecutive months
Strategic change Review of sustainability and transformation plans and other relevant matters
Material concerns with a provider’s delivery against the transformation
agenda, including new care models and devolutionLeadership and improvement capability
Findings of governance or well-led review undertaken against the current well-led framework
Third party information, eg Healthwatch, MPs, whistleblowers, coroners’ reports
Organisational health indicators
Operational efficiency metrics
CQC well-led assessments
Material concerns
CQC ‘inadequate’ or ‘requires improvement’ assessment against ‘well- led’.
14 Income and expenditure, or surplus/deficit margin
Appendix 3
Draft

1
North Tees and Hartlepool NHS Foundation Trust
Meeting of the Board of Directors
26 April 2018
Executive Summary
Month 12 Financial Performance Report - 31 March 2018
Report of the Director of Finance (Interim) Strategic Aim (The full set of Trust Aims can be found at the beginning of the Board Reports) Transforming our Services
1. Introduction 1.1 This report outlines the draft Group financial performance for March 2018 (Month 12).
The figures included in this report are draft and therefore subject to validation and audit. They may change before draft submission of the accounts on 24 April 2018.
2. Key Issues & Planned Actions
Statement of Comprehensive Income (SoCI) - Group Position
Reporting period: 1st April 2017 to 31st March 2018
Current Month Actual
(£'000s) YTD Actual
(£'000s)
Income 21,154 278,730
Pay Expenditure 16,865 201,094
Operating Non Pay Expenditure 9,224 79,567
Passthrough Drugs and devices 1,157 14,746
Total Operating Expenditure 27,246 295,407
EBITDA (6,092) (16,677)
Interest, Depreciation, PDC 3,811 13,160
Surplus/Deficit before STF (9,903) (29,837)
STF 0 0
Surplus/Deficit after STF (9,903) (29,837)
Draft
2
2.1 The Group’s Month 12 March position is a deficit of £(29.8)m. This position is draft at
time of writing and is consistent with how the Trust is measured against its financial performance targets (i.e. Control Total). This compares to a control total (excluding STF) of £(3.9)m deficit – £(25.9)m adverse variance from plan. This is in line with the expected position for the 2017/18 year end.
2.2 The Trust position includes a number of non-recurrent items which have been
reported to Finance Committee, which masks the underlying position. The items include 2016/17 contract settlement (c£2.1m adverse impact), stock write downs of c£(2.3)m – adverse impact and additional depreciation of c£(3)m relating to asset classification and Trakcare.
2.3 This position is consolidated to include positions for the Trust subsidiaries – Optimus
and North Tees and Hartlepool Solutions LLP (NTS). NTS has reported a £0.7m profit – principally because items purchased relating to the FT contract are lower than expected. Optimus has generated a £54k deficit.
Operating Income (excluding STF)
2.4 Income has continued to perform in line with forecast for 2017/18. The year-end positions agreed with commissioners have been reflected in this position.
2.5 The income position has deteriorated as the impact of the 2016/17 contract
settlement has been reflected in the Month 12 position. This impact is c£(2.1)m adverse and is non recurrent in nature. This impact was expected and is in line with previously briefed expectations.
Expenditure - Pay 2.6 Pay expenditure continues to perform in line with previous months, demonstrating
that pay costs have been contained throughout the winter period. 2.7 These costs include accruals for NHSP agency and bank staff, a small movement for
annual leave accruals and overtime and enhancements incurred in March 2018, but expected to be paid in April 2018.
Expenditure – Non-Pay 2.8 Non pay costs have demonstrated a significant increase in Month 12. Significant
levels of stock write downs £(2.3)m have adversely affected the financial position in 2017/18 non recurrently.
STF Income 2.9 As the year to date financial target has not been met no STF income is assumed to
have been achieved.
Impairments 2.10 The Trust financial position reported above is consistent with how it is
measured against its control total by its regulator, NHS Improvement. This methodology excludes technical impairments.
Draft
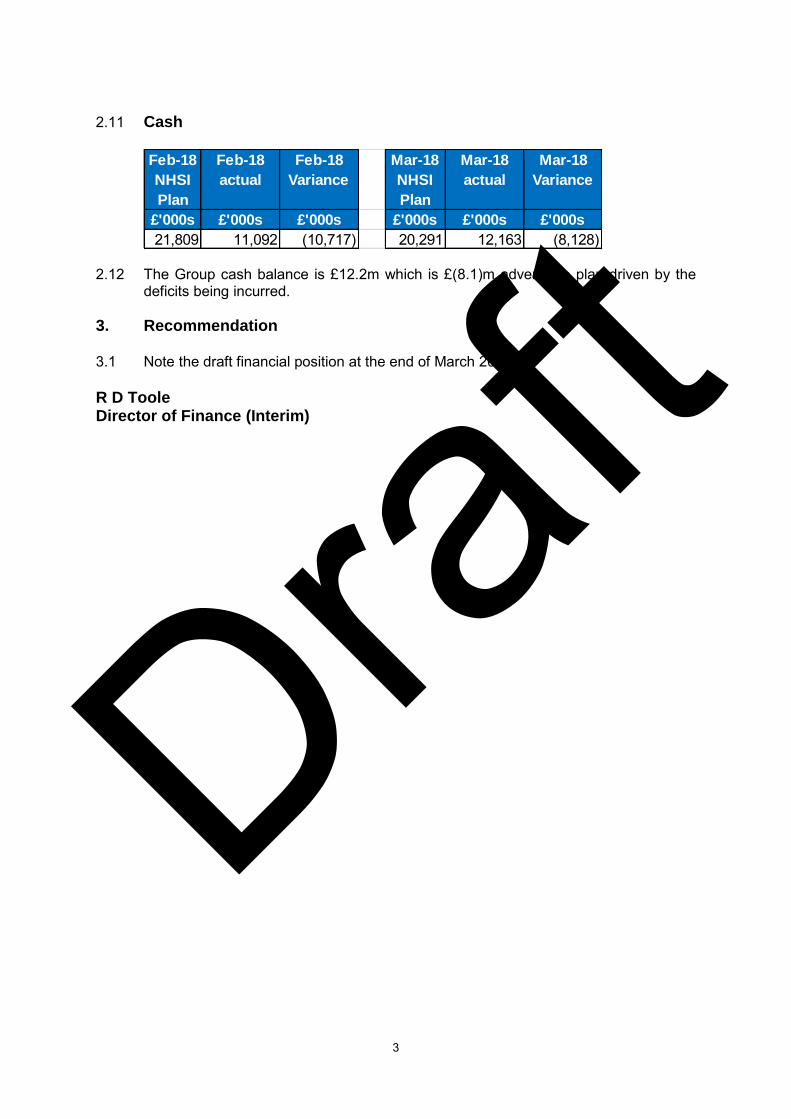
3
2.11 Cash
2.12 The Group cash balance is £12.2m which is £(8.1)m adverse to plan driven by the
deficits being incurred. 3. Recommendation 3.1 Note the draft financial position at the end of March 2018. R D Toole Director of Finance (Interim)
Feb-18
NHSI
Plan
Feb-18
actual
Feb-18
Variance
Mar-18
NHSI
Plan
Mar-18
actual
Mar-18
Variance
£'000s £'000s £'000s £'000s £'000s £'000s
21,809 11,092 (10,717) 20,291 12,163 (8,128)
Draft
1
North Tees and Hartlepool NHS Foundation Trust
Meeting of the Board of Directors
26 April 2018
Executive Summary
Draft Revenue and Capital Budgets - 2018/19
Report of the Director of Finance (Interim)
Strategic Aim (The full set of Trust Aims can be found at the beginning of the Board Reports). Maintain Compliance and Performance
Strategic Objective (The full set of Trust Objectives can be found at the beginning of the Board Reports). Finance
1. Introduction
1.1 The purpose of this report is to present to the Board of Directors the proposedrevenue and capital budgets for 2018/19, previously discussed at Board Seminars.
2. Key Issues & Planned Actions
2.1 The report outlines:
The approach and principles to planning for the 2018/19 financial year The proposed revenue budgets for 2018/19 and LLP Unitary Payment. The 5 year Capital Plan
2.2 Overall approach has been to set realistic and achievable, but challenging financial targets. Budgets have been set based on current run rates. As such „budget slack‟ has been removed e.g. posts held in 2017/18.
Actual contracted workforce as at January 2018 plus committed appointments –with sense check for safe (red rules) ward staffing levels
Pay contingency of 0.5% for essential recruitment (c.£1m) Pay 2.1% assumed, Non-Pay inflation at 2.1% (NHSI have advised to use these
assumptions rather than any assessment of the potential impact of 2018/19nationally proposed pay awards
Non-Pay & Directorate income – based on normalised 2017/18 FOT at M9 Contract income – based on agreed contracts - normalised, realistic forecast
outturn Adjusted for decommissioned services (0-19 Service) Cost reduction targets at challenging though “expected” levels (4%)
Committed, unavoidable pressures funded (Microsoft licences / LLP Start-up)
2.3 The Trust has agreed an alternative contracting methodology for 2018/19 with its main commissioners. This approach is intended to align incentives within the local health economy whilst providing stability from a planning perspective.
Draft

2
2.4 The Trust budget includes the planned Unitary Payment to North Tees and Hartlepool Solutions LLP. This payment is based on version 15 of the financial model and is £42.8m. There are several items to work through on budgeted items within the LLP. Specifically these are;
Recurrent Procurement Budgets are to be resolved due to challenges with theBuying / Contract Management and especially the Materials Managementfunction. (c.£50k)
Some estates staff are budgeted for within both the capital plan and therevenue budgets (hence double-count – more than offsets procurement)
The value of Non-Pay being purchased by the LLP was lower than planned atMonth 12 2017/18. Work will continue to maximise the opportunities for LLPand Group with novated contracts.
2.5 The enhanced stability provided by the agreed healthcare contracts allows the Trust to focus more clearly on management of its cost base. The Trust plan includes an £11.2m CIP assumption which delivers a £(24)m deficit plan. The Trust recognises the risks associated with CIP delivery and remains committed to improving financial performance – as such it has set a stretch internal target to support delivery.
2.6 Global Trust budgets for 2018/19 will therefore be as follows;
Global Trust Budget Pre CIP
(£m)
CIP (£m) Global Trust Budgets after CIP
(£m)
Income 281.2 0.4 281.6 Pay (208.7) 5.0 (203.7) Non Pay (107.7) 5.8 (101.9) Total Surplus/(Deficit)
(35.2m) 11.2 (24.0)
3. Recommendation
3.1 The Board of Directors is requested to receive the report and approve the 2018/19 revenue and capital budgets and Unitary Payment to the LLP as detailed.
Robert D Toole Director of Finance (Interim) Draf
t
North Tees and Hartlepool NHS Foundation Trust
Meeting of the Board of Directors
26 April 2018
Executive Summary
Integrated Compliance and Performance - Year End Report 2017/18
Report of the Director of Performance and Planning, Director of Nursing, Patient Safety and Quality and Director of Workforce
Strategic Aim (The full set of Trust Aims can be found at the beginning of the Board Reports) Putting Patients First; Valuing our People 1. Introduction/ Purpose
1.1 This report highlights an integrated summary of key achievements and exceptions
against standards included in the NHS Improvement (NHSI) Single Oversight Framework, Sustainability and Transformation Plan (STP), NHS Outcomes Framework and Core National and Local Standards for year end 2017/18.
1.2 It comprises a year-end summary report including Compliance and Performance,
Quality, Finance and Workforce as the Board has received in-year detailed reports, with a summary of key areas of action for this year.
2. Performance Overview
2.1 The Trust has performed relatively well against national and local key indicators
throughout 2017/18 despite considerable challenges associated with on-going operational, clinical, financial and system wide pressures.
2.2 Additional emergency demand resulted in an extremely pressured winter period, with significant surges in activity and high bed occupancy rates on both base wards and critical care, which necessitated cancellation of multiple elective procedures outside the planned reduction in elective activity, compounded by the national directives to cancel all routine elective waiting lists over the January period.
2.3 Despite the significant financial pressures, the Trust has continued to deliver against
its key operational and quality standards, gaining the revised CQC rating of ‘Good’ in year.
2.4 This report indicates the Trust has performed above or within expected for the
majority of indicators and also demonstrates improvements in indicators where performance has previously been below the national average, as outlined in Appendix 1 within the main report.
3. Conclusion/Summary
3.1 The Trust has performed relatively well against the majority of key operational
national and local standards throughout 2017/18, despite the considerable
Draft
challenges associated with on-going operational, clinical, financial and system wide pressures. The Trust continues to develop the performance reporting framework to ensure it meets the needs of both corporate and directorate level delivery, reflecting the multiple internal and external performance requirements.
4. Recommendations
The Board of Directors is asked to note:
The relatively positive performance against the key operational, quality and workforce standards during 2017/18, despite the significant pressures experienced during the winter period;
the on-going work to improve performance and productivity within the current financial framework;
the significant achievement of the improved CQC rating of ‘Good’ in year, an indication of the on-going dedication of all staff to deliver safe, quality, patient centred care.
Lynne Taylor, Interim Director of Planning and Performance Julie Lane, Director of Nursing and Infection Prevention and Control Alan Sheppard, Interim Director of Workforce
Draft
1
North Tees and Hartlepool NHS Foundation Trust
Meeting of the Board of Directors
26 April 2018
Integrated Compliance and Performance - Year End Report 2017/18
Report of the Director of Performance and Planning, Director of Nursing,
Patient Safety and Quality and Director of Workforce
1. Introduction/ Purpose
1.1 This report highlights an integrated summary of key achievements and exceptions against standards included in the NHS Improvement (NHSI) Single Oversight Framework, Sustainability and Transformation Plan (STP), NHS Outcomes Framework and Core National and Local Standards for year end 2017/18.
1.2 It comprises a year-end summary report including Compliance and Performance,
Quality, Finance and Workforce as the Board has received in-year detailed reports, with a summary of key areas of action for this year.
1.3 Appendix 1 details compliance and performance against all key national and local
standards. 2. Performance Overview 2.1 The Trust has performed relatively well against national and local key indicators
throughout 2017/18 despite considerable challenges associated with on-going operational, clinical, financial and system wide pressures.
2.2 Additional emergency demand resulted in an extremely pressured winter period, with significant surges in activity and high bed occupancy rates on both base wards and critical care, which necessitated cancellation of multiple elective procedures outside the planned reduction in elective activity, compounded by the national directives to cancel all routine elective waiting lists over the January period.
2.3 Despite the significant financial pressures, the Trust has continued to deliver against
its key operational and quality standards, gaining the revised CQC rating of ‘Good’ in year.
2.4 This report indicates the Trust has performed above or within expected for the
majority of indicators and also demonstrates improvements in indicators where performance has previously been below the national average, as outlined in Appendix 1.
2.5 The NHSI Model Hospital dashboard has made a number of updates in year to
include additional reports across specialties and directorates, which have been utilised to identify efficiency and productivity opportunities. The Trust has embraced Lord Carter’s recommendations and continues to explore productivity, quality, efficiency and responsiveness, to provide a clearer view of improvement opportunities through the ‘Delivering Productivity Programme’.
2.6 NHS Improvement has recognised, on the whole, the excellent performance of the
Trust with regard to quality of care, operations and change although work and regular meetings continue. This coupled with the achievements outlined and recognised by the CQC, when the Trust received a rating of ‘Good’, is testament to the dedication of
Draft

2
the organisation and strengthens the Trust’s credibility in meeting the challenges
moving forward into 2018/19. 2.7 The Trust is delighted with the success of the Integrated Urgent Care Centre which
has seen sustained achievement of the four hour standard throughout the year, reporting a year end performance of 97.24%, an increase of 3.01% compared to 2016/17, evidencing the improved emergency patient pathways that have been implemented.
2.8 Delivery against the 62 day referral to treatment cancer standard has been a
challenge, with varied performance throughout the year, impacted on by a number of variables including patient choice, complex pathways, capacity and system wide issues. Despite these challenges, the aggregate provisional year end position indicates the Trust has achieved against all cancer standards for 2017/18 and has, in the main, remained above the national and regional position in year.
2.9 As outlined in section 2.2, seasonal challenges impacted on the management of the
referral to treatment standard, however despite these pressures achieved 93.63% for the aggregate year-end position. No patients waited more than 52 weeks in comparison to the national position which reported 2,236 patients waiting greater than 52 weeks (validated data February 2018).
2.10 The Trust achieved against the 99% Diagnostic national standard reporting a year
end average of 99.55%. Diagnostic pathways continue to be monitored closely to ensure maximum contribution to RTT pathway management and to reduce waiting times.
2.11 Delayed Transfers of Care (DTOC) have reported in a favourable position with a
gradual reduction noted throughout the year. The focus going into 2018/19 will concentrate on ‘stranded patients’ (LOS>7 days) with the aim to further reduce overall bed occupancy and overall discharge processes. The Trust also recognises readmissions as an area requiring further work, in line with national drivers to reduce avoidable admissions.
2.12 Performance against indicators for Community Services has remained compliant
throughout 2017/18 with a positive year end position against all indicators. 2.13 The end of year performance against the operational efficiency metrics indicate the
Outpatient DNAs and Readmission rates continue to report above the internal targets. There will be further focussed review of these areas during 2018/19, supported through the directorate DPP projects, including standardised audits of the readmissions to understand the avoidable and unavoidable split, with recovery plans developed to deliver pathway improvements.
2.14 During 2017-18 the Trust experienced a total of 1,467 falls, of which 26 falls where
with a fracture. The total number of falls has increased by 110 against 2016-17, where the Trust had 1,357 falls of which 20 falls resulted with fracture.
2.15 During April 2017 to February 2018, the Trust experienced a total of 227 in-hospital
pressure ulcers of which 2 were Grade 4. This is an increase of 54 pressure ulcers against April 2016 to February 2017.
2.16 The Trust is reporting 35 Trust attributed cases of Clostridium Difficile infections at
the end of 2017-18. Although this exceeds the annual trajectory of 13 this does represent an improved position on the previous year. The Trust reported 4 Trust attributed cases of MRSA bacteraemia in 2017-18 which unfortunately is deterioration in comparison with the previous year.
Draft
3
2.17 The Improvement Plan for 2018-19 is now under development with any incomplete actions being carried forward. The focus of the plan will again be getting the fundamentals of care right including hand hygiene, environmental cleanliness and antibiotic stewardship, plus continuing the collaborative work with partner organisations that commenced during 2017-18.
2.18 The Trust reported 25 Trust attributed cases of MSSA bacteraemia in 2017/18 and 43 Trust attributed cases of E.coli.
2.19 The latest HSMR value is currently reporting at 101.32 (January 2017 to December
2017). This value continues to remain inside the ‘as expected’ range (the national mean is 100). The Trust crude mortality rate for HSMR is 3.44%. The latest SHMI value is 105.91 (October 2016 to September 2017) and this value maintains the Trust in the ‘as expected’ range.
2.20 The Trust saw a reduction in stage 3 formal complaints in 2017/18 compared to the
previous year and responded well with compliance within 25 working days.
2.21 The Trust has maintained performance in respect of the workforce indicators. 2.22 The sickness absence data is the year to date figure (up to 28 February 2018) and is
reported as 4.53%, a reduction of 0.46% when compared to the previous year (4.99%), however outside the 3.5% target.
2.23 The Trust’s Turnover rate at the end of 2017/18 is 14.80% (including foundation
doctors) and against a target of 10.50%. This is an increase of 2.97% when compared to the baseline of 31 March 2017; however this is attributed to the transfer of the Estates & Facilities and Supplies & Procurement services to a wholly owned subsidiary company on 1 March 2018. This is due to the historically low turnover rate of the staff who have transferred to the LLP, which has previously resulted in a lower overall turnover rate for the Trust.
2.24 The Trust headcount at the end of 2017/18 is reported as 625 less than as at the
baseline of 31 March 2017. 2.25 The Staff Friends and Family Test for Quarter 4 2017/18 reported that 73% (n=45) of
staff would recommend the Trust as a place to receive care or treatment, and 57% (n=35) of staff would recommend the Trust as a place to work, recognising the low number of overall returns (n=62). To improve staff feedback, the staff section of the Staff and Patient Experience Survey (SPECs) will now include the Friend and Family Test questions.
2.26 The Staff Engagement Score as reported by the annual NHS Staff Survey (2017) is
3.81 out of a total score of 5. There has been a steady increase in the engagement score over the previous years, which is in recognition of the impact of the enhanced engagement activities which have taken place.
3. Conclusion/Summary
3.1 The Trust has performed relatively well against the majority of key operational national and local standards throughout 2017/18, despite the considerable challenges associated with on-going operational, clinical, financial and system wide pressures. The Trust continues to develop the performance reporting framework to ensure it meets the needs of both corporate and directorate level delivery, reflecting the multiple internal and external performance requirements.
Draft
4
4. Recommendations
The Board of Directors is asked to note:
The relatively positive performance against the key operational, quality and workforce standards during 2017/18, despite the significant pressures experienced during the winter period;
the on-going work to improve performance and productivity within the current financial framework;
the significant achievement of the improved CQC rating of ‘Good’ in year, an indication of the on-going dedication of all staff to deliver safe, quality, patient centred care.
Lynne Taylor, Interim Director of Planning and Performance Julie Lane, Director of Nursing and Infection Prevention and Control Alan Sheppard, Interim Director Workforce
Draft
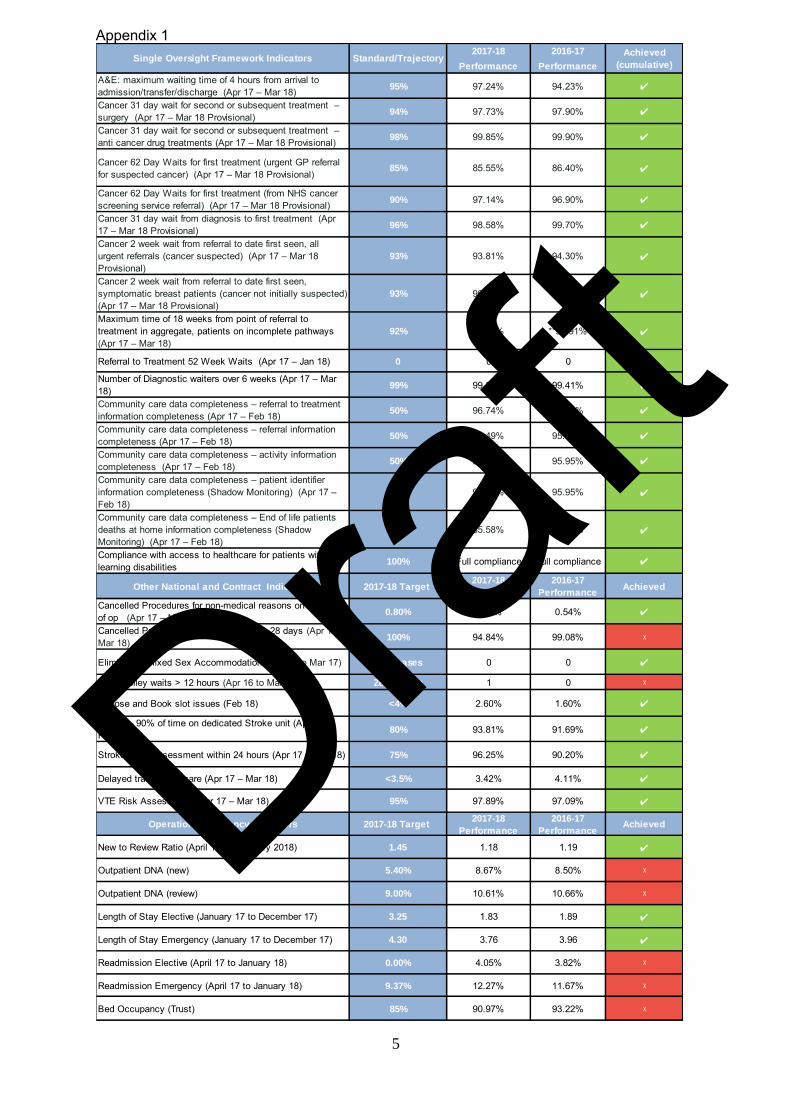
5
Appendix 1
2017-18 2016-17
Performance Performance
A&E: maximum waiting time of 4 hours from arrival to admission/transfer/discharge (Apr 17 – Mar 18)
95% 97.24% 94.23% ✔
Cancer 31 day wait for second or subsequent treatment –
surgery (Apr 17 – Mar 18 Provisional)94% 97.73% 97.90% ✔
Cancer 31 day wait for second or subsequent treatment –
anti cancer drug treatments (Apr 17 – Mar 18 Provisional)98% 99.85% 99.90% ✔
Cancer 62 Day Waits for first treatment (urgent GP referral for suspected cancer) (Apr 17 – Mar 18 Provisional)
85% 85.55% 86.40% ✔
Cancer 62 Day Waits for first treatment (from NHS cancer screening service referral) (Apr 17 – Mar 18 Provisional)
90% 97.14% 96.90% ✔
Cancer 31 day wait from diagnosis to first treatment (Apr 17 – Mar 18 Provisional)
96% 98.58% 99.70% ✔
Cancer 2 week wait from referral to date first seen, all urgent referrals (cancer suspected) (Apr 17 – Mar 18
Provisional)93% 93.81% 94.30% ✔
Cancer 2 week wait from referral to date first seen, symptomatic breast patients (cancer not initially suspected) (Apr 17 – Mar 18 Provisional)
93% 96.61% 96.90% ✔
Maximum time of 18 weeks from point of referral to treatment in aggregate, patients on incomplete pathways (Apr 17 – Mar 18)
92% 93.63% **92.91% ✔
Referral to Treatment 52 Week Waits (Apr 17 – Jan 18) 0 0 0 ✔
Number of Diagnostic waiters over 6 weeks (Apr 17 – Mar
18) 99% 99.56% 99.41% ✔
Community care data completeness – referral to treatment
information completeness (Apr 17 – Feb 18)50% 96.74% 97.45% ✔
Community care data completeness – referral information
completeness (Apr 17 – Feb 18)50% 96.49% 95.88% ✔
Community care data completeness – activity information
completeness (Apr 17 – Feb 18)50% 95.66% 95.95% ✔
Community care data completeness – patient identifier
information completeness (Shadow Monitoring) (Apr 17 –
Feb 18)50% 95.66% 95.95% ✔
Community care data completeness – End of life patients
deaths at home information completeness (Shadow Monitoring) (Apr 17 – Feb 18)
50% 85.58% 86.62% ✔
Compliance with access to healthcare for patients with learning disabilities 100% Full compliance Full compliance ✔
Other National and Contract Indicators 2017-18 Target 2017-18
Performance
2016-17
PerformanceAchieved
Cancelled Procedures for non-medical reasons on the day of op (Apr 17 – Mar 18)
0.80% 0.72% 0.54% ✔
Cancelled Procedures reappointed within 28 days (Apr 17 to Mar 18) 100% 94.84% 99.08% ᵡ
Eliminating Mixed Sex Accommodation (Apr 16 to Mar 17) Zero cases 0 0 ✔
A&E Trolley waits > 12 hours (Apr 16 to Mar 17) Zero cases 1 0 ᵡ
Choose and Book slot issues (Feb 18) <4% 2.60% 1.60% ✔
Stroke – 90% of time on dedicated Stroke unit (Apr 17 –
Feb 18) 80% 93.81% 91.69% ✔
Stroke – TIA assessment within 24 hours (Apr 17 – Feb 18) 75% 96.25% 90.20% ✔
Delayed transfers of care (Apr 17 – Mar 18) <3.5% 3.42% 4.11% ✔
VTE Risk Assessment (Apr 17 – Mar 18) 95% 97.89% 97.09% ✔
Operational Efficiency Indicators 2017-18 Target 2017-18
Performance
2016-17
PerformanceAchieved
New to Review Ratio (April 17 to February 2018) 1.45 1.18 1.19 ✔
Outpatient DNA (new) 5.40% 8.67% 8.50% ᵡ
Outpatient DNA (review) 9.00% 10.61% 10.66% ᵡ
Length of Stay Elective (January 17 to December 17) 3.25 1.83 1.89 ✔
Length of Stay Emergency (January 17 to December 17) 4.30 3.76 3.96 ✔
Readmission Elective (April 17 to January 18) 0.00% 4.05% 3.82% ᵡ
Readmission Emergency (April 17 to January 18) 9.37% 12.27% 11.67% ᵡ
Bed Occupancy (Trust) 85% 90.97% 93.22% ᵡ
Single Oversight Framework Indicators Standard/TrajectoryAchieved
(cumulative)
Draft
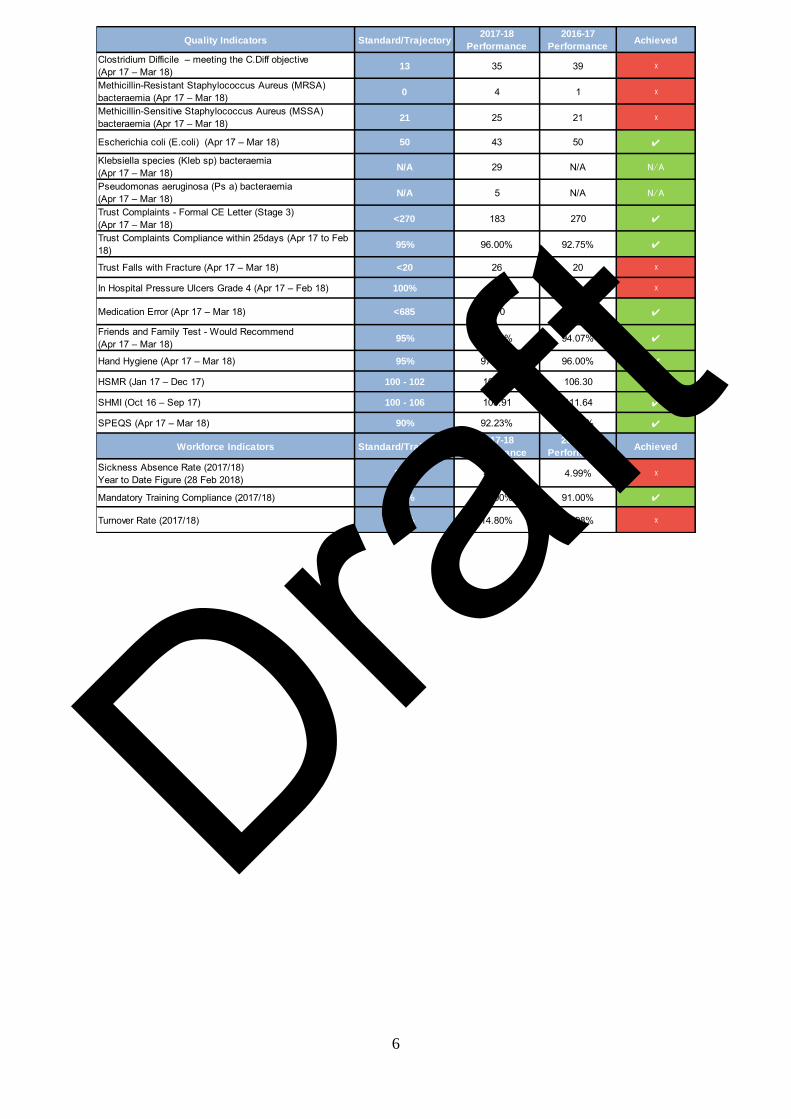
6
Quality Indicators Standard/Trajectory2017-18
Performance
2016-17
PerformanceAchieved
Clostridium Difficile – meeting the C.Diff objective
(Apr 17 – Mar 18)13 35 39 ᵡ
Methicillin-Resistant Staphylococcus Aureus (MRSA) bacteraemia (Apr 17 – Mar 18)
0 4 1 ᵡ
Methicillin-Sensitive Staphylococcus Aureus (MSSA) bacteraemia (Apr 17 – Mar 18)
21 25 21 ᵡ
Escherichia coli (E.coli) (Apr 17 – Mar 18) 50 43 50 ✔
Klebsiella species (Kleb sp) bacteraemia (Apr 17 – Mar 18)
N/A 29 N/A N/A
Pseudomonas aeruginosa (Ps a) bacteraemia (Apr 17 – Mar 18)
N/A 5 N/A N/A
Trust Complaints - Formal CE Letter (Stage 3)(Apr 17 – Mar 18)
<270 183 270 ✔
Trust Complaints Compliance within 25days (Apr 17 to Feb 18) 95% 96.00% 92.75% ✔
Trust Falls with Fracture (Apr 17 – Mar 18) <20 26 20 ᵡ
In Hospital Pressure Ulcers Grade 4 (Apr 17 – Feb 18) 100% 2 1 ᵡ
Medication Error (Apr 17 – Mar 18) <685 670 685 ✔
Friends and Family Test - Would Recommend(Apr 17 – Mar 18)
95% 95.10% 94.07% ✔
Hand Hygiene (Apr 17 – Mar 18) 95% 97.00% 96.00% ✔
HSMR (Jan 17 – Dec 17) 100 - 102 101.32 106.30 ✔
SHMI (Oct 16 – Sep 17) 100 - 106 105.91 111.64 ✔
SPEQS (Apr 17 – Mar 18) 90% 92.23% 88.43% ✔
Workforce Indicators Standard/Trajectory2017-18
Performance
2016-17
PerformanceAchieved
Sickness Absence Rate (2017/18) Year to Date Figure (28 Feb 2018)
3.5% 4.53% 4.99% ᵡ
Mandatory Training Compliance (2017/18) 80% 84.00% 91.00% ✔
Turnover Rate (2017/18) 11% 14.80% 11.98% ᵡ
Draft
1
North Tees & Hartlepool NHS Foundation Trust
Meeting of the Board of Directors
26 April 2018
Executive Summary
NHS National Staff Survey Results 2017
Report of the Director of Workforce (Interim) Strategic Aim (The full set of Trust Aims can be found at the beginning of the Board Reports) Valuing our People; Health and Wellbeing. 1. Introduction This report provides detail relating to the 2017 staff survey results; specifically in relation to how the Trust compares to similar Trusts nationally; highlighting good practice and areas where focus may be required. From a sample of 1250 people 620 surveys were completed. This equates to a response rate of 51% which is above average when compared to similar Trusts nationally (43%). It is positive to note that out of the 32 key findings contained within that report the Trust rated better than average in 17 of them and average in a further 10. The remaining 5 were ranked as worse than average. 2. Summary of Key Findings 2.1 Top Scores The Trust’s five top scores in the 2017 Staff Survey were in the following key findings:
People believing that the organisation provides equal opportunities for career progression or promotion (higher the better)
People working extra hours (lower the better) People feeling satisfied with the quality of work and care they are able to
deliver (higher the better) People reporting violence (higher the better) People witnessing potentially harmful errors, near misses or incidents (lower
the better) 2.2 Bottom Scores The Trust’s five bottom scores were in the following key findings:
People experiencing physical violence from patients, relatives or public (lower the better)
Draft
2
People experiencing physical violence from staff (lower the better) Number of people appraised (higher the better) People experiencing harassment, bullying or abuse from patients, relatives or
the public (lower the better) Number of staff agreeing that their role makes a difference to patients/service
users (higher the better) 3. Recommendation The Board are asked to note the contents of this report. Alan Sheppard Director of Workforce (Interim)
Draft
3
North Tees and Hartlepool NHS Foundation Trust
Meeting of the Board of Directors
26 April 2018
NHS National Staff Survey Results 2017
Report of the Director of Workforce (Interim)
1. Introduction This report provides detail relating to the 2017 staff survey results; specifically in relation to the benchmarked report produced by Picker on behalf of the Department of Health. These reports provide the Trust with a national view on the staff survey responses and highlights good practice and areas where focus may be required when compared against other similar Trusts. Out of a sample of 1250 people 620 surveys were completed. This equates to a response rate of 51% which is above average when compared to similar Trusts nationally (43%). 2. Trust Results 2017 It is positive to note that of the 32 key findings contained within the Trust benchmarked report the Trust rated better than average in 17 and average in a further 10. The remaining 5 were ranked as worse than average. The survey responses are arranged under 10 themes this year:
Staff Engagement Appraisals & support for development Equality and diversity Errors and incidents Health and wellbeing Working patterns Job satisfaction Managers Patient care and experience Violence, harassment and bullying
2.1 Staff Engagement This indicator concerns the ability of staff to contribute to improvements at work; willingness to recommend the Trust as a place to work or receive treatment and the extent to which staff feel motivated and engaged in their work. The Trust score of 3.81 (out of 5) was relatively static when looking at the 2016 engagement score and was average when compared to other similar Trusts.
2014 2015 2016 2017
3.64 3.75 3.82 3.81
Draft
4
Although there is static position this year it is positive to note a steady and sustained improvement in the Trust engagement score over previous years which is a reflection on the activities developed and implemented with the 4 key priority areas in mind:
Increasing compliance and quality of performance appraisals across the Trust;
Ensuring all staff know how they can / do make positive impact on patient care;
Recognising and celebrating good practice; Communicate the strategic vision and the part we all play in making the vision
a reality.
2.2 Appraisal & support for development It is positive to note that the Trust saw an improvement in the quality of non-mandatory training, learning or development; which was a bottom ranked score in 2016. A response of 4.11 (out of 5) was rated as above average when compared to other similar Trusts. However, despite seeing an increase in relation to the percentage of staff having an appraisal over the last 12 months (from 74% to 77%), this was rated below average when compared to other similar Trusts and is one of the Trust bottom 5 scores. 2.3 Equality and diversity The Trust has seen a 2% improvement in the percentage of staff believing that the Trust provides equal opportunities for career progression or promotion; rating better than average nationally (93% compared to a national average of 85%). 2.4 Errors and incidents Responses to 3 of the 4 key findings in this section were rated as better than average. The Trust had less people than average witnessing potentially harmful errors, near misses or incidents (25% compared to 29% national average); more people than average reporting potentially harmful errors, near misses or incidents (92% against a national average of 91%) and more people than average telling the Trust that the procedures for reporting such incidents are fair and effective (3.80 out of 5 against a national average of 3.73). 2.5 Health and wellbeing It is positive to note that the Trust rated as above average in all aspects of the health and wellbeing section of the survey when compared to other similar Trusts. However, when reviewing the annual comparison of Trust scores, there was an increase of 3% (to 34%) in the percentage of staff feeling unwell due to work related stress and an increase of 1% (to 52%) in the number of staff attending work despite feeling unwell due to pressure from their manager, colleague or themselves. 2.6 Working patterns The Trust was better than average when considering opportunities for flexible working patterns (54% against a national average of 51%) and the low numbers of staff working extra hours (63% compared to a national average of 71%).
Draft
5
2.7 Job satisfaction The Trust scored well compared to other similar Trust when considering themes linked to job satisfaction; particularly the number of staff that would recommend the Trust as a place to work or receive treatment. This was particularly noticeable in the responses linked to staff working extra hours which decreased from 65% to 63% this year. However, there was a decrease of 2% from last year in relation to staff feeling able to contribute towards improvements at work (from 72% to 70%). 2.8 Managers Whilst rating better than average on recognition and value of staff by managers and the Trust, there was a slight deterioration in the annual score from last year (from 3.53 to 3.51 out of 5). 2.9 Patient care and experience The Trust rated better than average in 2 of the 3 elements included in this section. This considers people being satisfied with the quality of work and care they are able to give 4.05 out of 5 against a national average of 3.90) and the effective use of feedback from patients (3.76 against a national average of 3.69). However, the Trust rated worse than average in relation to people believing that their role makes a difference to patients / service users, having seen a 3% decline from the 2016 results (from 92% to 89%). 2.10 Violence, harassment and bullying Responses received in this section were mixed. It is important to note that any case of this nature is unacceptable and the Trust exercises a zero tolerance to this behaviour. This report however considers how the Trust fared compared to others nationally. Of the 6 key findings contained within this section of the report, the Trust ranked worse than average in 3; staff experiencing physical violence from patients, relatives or the public, staff experiencing physical violence from staff and staff experiencing harassment, bullying or abuse from patients, relatives or the public in the last 12 months. The Trust ranked better than average to the key finding relating to staff reporting their experience of violence. When considering the Trust annual comparison of responses, this shows a positive trend in relation to physical violence from patients, relatives or the public, despite being ranked as worse than average against other Trusts (from 19% to 15%). This is also true of the key finding linked to staff experiencing physical violence from staff (from 3% to 2%). 3. Positive scores The areas where the Trust compares most favourably when compared with other similar Trusts are:
Draft

6
3.1 Percentage of staff working extra hours (lower the better) 2017 2016 2017 average Similar Trust best
score 63% 65% 71% 63%
3.2 Percentage of staff believing that the organisation provides equal
opportunities for career progression or promotion (higher the better) 2017 2016 2017 average Similar Trust best
score 93% 91% 85% 93%
3.3 Staff satisfaction with the quality of work and care they are able to deliver (higher the better) 2017 2016 2017 average Similar Trust best
score 4.05 4.01 3.90 4.16
3.4 Percentage of staff witnessing potentially harmful errors, near misses or
incidents in the last month (lower the better) 2017 2016 2017 average Similar Trust best
score 25% 25% 29% 22%
3.5 Percentage of staff reporting most recent experience of violence (higher
the better) 2017 2016 2017 average Similar Trust best
score 75% 81% 67% 82%
4. Negative scores The areas where the Trust compares least favourably with other similar Trusts are: 4.1 Percentage of staff appraised in the last 12 months (higher the better) 2017 2016 2017 average Similar Trust best
score 77% 74% 86% 95%
4.2 People experiencing harassment, bullying or abuse from patients,
relatives or the public in the last 12 months (lower the better) 2017 2016 2017 average Similar Trust best
score 30% 28% 27% 19%
4.3 Percentage of staff experiencing physical violence from staff in the last
12 months (lower the better)
Draft
7
2017 2016 2017 average Similar Trust best score
2% 3% 2% 1% 4.4 Percentage of staff experiencing physical violence from patients, relatives or the public in the last 12 months (lower the better) 2017 2016 2017 average Similar Trust best
score 15% 19% 14% 9%
4.5 Percentage of staff agreeing that their role makes a difference to
patients/service users (higher the better) 2017 2016 2017 average Similar Trust best
score 89% 92% 90% 93%
5. Significant Changes The Trust has not seen any significant changes in any of the key findings from last years’ survey; whether that is positive or negative. 6. Taking things forward It is encouraging to note there are a number of positive trends apparent from the staff survey results this year. There has been a significant rise in engagement activity over the past year which appears to be reflected in the staff survey results. It is accepted that such activities take time to embed and have a positive influence on the culture of an organisation; however it is anticipated that this will continue over the next year, improving overall engagement and as a result be reflected in the 2018 survey results. Results are being analysed via the Trust culture group with input from staff and staff side representatives across the Trust regarding priorities and making continuous improvements. This will be included within the staff survey action plan, which will be monitored through the culture group and reported to the Workforce Committee It is important to note that the staff survey results are not considered in isolation, but form part of the wider engagement agenda. This ensures appropriate trend analysis takes place with any actions reflecting this analysis. 6.1 Working with directorates The Employee Relations team are working with Directorates across the Trust in relation to their local staff survey results; providing support and guidance in relation to the development of local action plans. These action plans will be monitored through the Deputy Executive Team meeting and reported to the Workforce Committee. The analysis of local reports includes exemplar practices to ensure Trust wide learning and sharing good practice in areas where results were less positive. It is also vital that specific areas of concern are focused upon which will be picked up during the Heat Map related activity that is currently in place through the Quality Reference Groups with individual areas.
Draft

8
6.2 Feedback It is important that the results from the survey are shared widely with staff; providing all with the opportunity to provide their view and thoughts on the results and how things could be improved; including working with staff side colleagues. Feeding back to staff is a vital part of engagement and the Trust is developing alternative and innovative ways of feeding what ‘we said, we did’ back to staff. It is anticipated that this will have a positive impact on the response rate for the 2018 survey. 7. Recommendation The Trust Board is requested to note the content of this paper; noting in particular the on-going activity relating to analysing and action planning going forward. Alan Sheppard Director of Workforce (Interim)
Draft

1
North Tees and Hartlepool NHS Foundation Trust
Meeting of the Board of Directors
26 April 2018
Executive Summary
Learning from Deaths Report
Report of the Medical Director
Strategic Aim Putting Patients First
Strategic Objective Putting Patients First / Patient Safety
1. Introduction
1.1 In March 2017, the National Quality Board (NQB) published national guidance “Learning from Deaths: A Framework for NHS Trust and NHS Foundation Trusts on Identifying, Reporting, Investigating and Learning from Deaths in Care”. The guidance provides requirements for Trusts to implement as a minimum in order ensure there is a focused approach towards responding to and learning from deaths of patients in our care.
1.2 This report provides details of the numbers of deaths that have occurred in the Trust since April 2017. It also provides the current position in relation to mortality case reviews that have been undertaken in relation to compulsory requirements in line with the Trust policy alongside additional reviews that have been undertaken.
1.3 The information presented in this report includes an overview of learning to date, including positive findings as well as areas that have been identified for further development.
2. Key Issues & Planned Actions
2.1 The Trusts HSMR value in the latest period has increased to 101.32, the SHMI is currently 105.91, both have now been within the expected range for 6 or more consecutive quarters.
2.2 Of the compulsory case reviews identified in the Trusts policy 70% have been reviewed to date; the pending reviews are those which have primarily been identified over quarter 4. Updates on pending reviews will be provided in future reports. Overall to date in 2017-18 the Trust has reviewed 22% of all deaths.
2.3 13 cases were identified as serious incidents, prior to case review. Of these, 7 have been reviewed and 2 were identified as being avoidable. There are a further 6 cases where the investigations are ongoing and updates will be provided in the next report.
2.4 The Trust is continuing to work in close in partnership with Primary Care, Local Authorities, CCGs and a number of other external stakeholders in order to identify where strategic changes can be initiated to support planning and the provision of end of life care across all areas of health and social care.
2.5 The Bereavement survey and the resultant reviews have identified cases where there has been excellent care provision, but has also highlighted some areas for learning that are being analysed.
2.6 There are small numbers of deaths in Trust for children, patients with learning difficulties and significant mental health problems. The reviews undertaken to date show that in the majority of
Draft

2
these cases there is evidence of safe, effective and responsive care provision; where there has been concerns identified these have been investigated in full.
2.7 There are areas where continued improvements are needed; these have been identified and each has ongoing monitoring in place. The Trust Outcome, Performance, Delivery Operational Group and the Patient Safety and Quality Standards Committee seek further assurance in relation to these areas in line with their terms of reference.
3. Recommendations
3.1 The Board of Directors are asked to note the content of this report and the information provided in relation to the reduction in the Trusts mortality rates.
3.2 The Board are asked to note the on-going work programme to maintain the mortality rates within the expected range for the organisation.
Dr D Dwarakanath
Medical Director
Draft
3
North Tees and Hartlepool NHS Foundation Trust Meeting of the Board of Directors
26 April 2018
Learning from Deaths Report
Report of the Medical Director
1. Introduction/Background
1.1 In March 2017, the National Quality Board (NQB) published national guidance “Learning from Deaths: A Framework for NHS Trust and NHS Foundation Trusts on Identifying, Reporting, Investigating and Learning from Deaths in Care”. The guidance provide requirements for Trust to implement as a minimum in order ensure there is a focused approach towards responding to and learning from deaths of patients in our care.
1.2 The Trust strives to improve the care provided to all of our patients; the overall aim is to identify, understand and implement improvements where any issues are related to the provision of safe and effective quality care. It is considered that if such safety and quality improvements are initiated effectively and embedded, then the mortality statistics will naturally show improvement.
1.3 The information presented in this report provides an overview of learning from deaths that has been obtained from mortality reviews undertaken by the Trust. The Trust policy identifies some key areas where all deaths will be reviewed and also identifies additional randomly selected cases will also be included in the review process. Some compulsory review areas have small numbers; therefore learning is presented as a summation of all reviews to reduce the risk of identifying cases directly.
2. Mortality Data
2.1 Information related to mortality is gathered from data provided routinely by the Trust to a national system where all hospital episode statistics (HES Data) is collated. Hospital Standardised Mortality Ratio (HSMR) examines information covering 56 diagnostic groups that are identified as accounting for 80% of hospital deaths nationally.
This information is used to calculate an overall HSMR taking into account, gender of the patient, age, how the patient was admitted (emergency or elective), levels of deprivation, how many times they have been admitted as an emergency in the last year, if palliative care was provided and various details relating to presenting complaint on admission.
2.2 This calculation is undertaken nationally and provides the Trusts overall HSMR. The latest HSMR value is 101.32 (January 2017 to December 2017) an increase from 99.52 (October 2016 to September 2017) that was in the previous report. This reflects the impact of increased mortalities during December 2017 and it is anticipated the Trust may see a further small increase when data from January 2018 is included. This new value continues to remain inside the „as expected‟ range for the 8th consecutive quarter.
2.3 The Trust currently resides 64th from the 137 Trusts, nationally, on its HSMR value.
2.4 The Summary Hospital-level Mortality Indicator (SHMI) is a ratio between the number of actual (observed) deaths to the “expected” number of deaths for an individual Trust, including deaths in hospital and up to 30 days following discharge. The ratio is calculated with consideration of gender, age, admission method, admissions in the last year and diagnosis being treated for the last admission.
Draft
4
2.5 The ratio is calculated nationally and provides the trusts overall SHMI. The latest SHMI value is 105.91 (October 2016 to September 2017), this has decreased from a value of 108.01 (July 2016 to June 2017), the value maintains the Trust in the „as expected‟ range for the 6th consecutive quarter.
2.6 The Trust has improved from the highest SHMI value in the country, to the 39th highest.
3. Mortality reviews
3.1 The Trust uses an electronic system to record mortality case reviews that are undertaken; this system is also used by other trusts in the region and is based on the “PRISM” methodology, one of the review tools recommended in the national guidance. This is a structured review of a case record, carried out by clinicians not involved in the patient‟s care, to determine whether there were any problems in care. Case record review is undertaken routinely to learn and improve in the absence of any concerns, with all directorates undertaking their own specialty based mortality and morbidity meetings. This is because it can help identify issues where there are no initial concerns. It is also used where concerns exist, such as when bereaved families or members of staff raise issues about care.
3.2 The Trust policy identifies that all in-patient deaths and those in the Accident and Emergency department are included in the scope of the mortality reviews. Since April 2017 the Trust has reported the following deaths:
3.3 The Trust policy identifies specific cases where a compulsory review is required; these include:
• Where requests are made by families to undertake a case review.
• Where staff request a case review.
• All deaths in the Intensive Care Unit (ICU).
• All deaths linked to complaints about significant concerns in relation to clinical care.
• All deaths linked to Serious Incident investigations.
• All deaths where the patient was admitted for elective treatment.
Compulsory case reviews are also undertaken for the following cases, which are linked to specific national review processes, some of these reviews are not yet recorded in the Trust mortality system and this is an area of ongoing development:
• All deaths where a patient has a registered Learning Disability (LD) – in conjunction withthe Learning Disability Mortality Review Programme (LeDER).
• All maternal deaths – in conjunction with M-BRRACE-UK.
• All deaths where the patient has a severe mental illness – in conjunction with localMental Health Trusts as required.
Draft
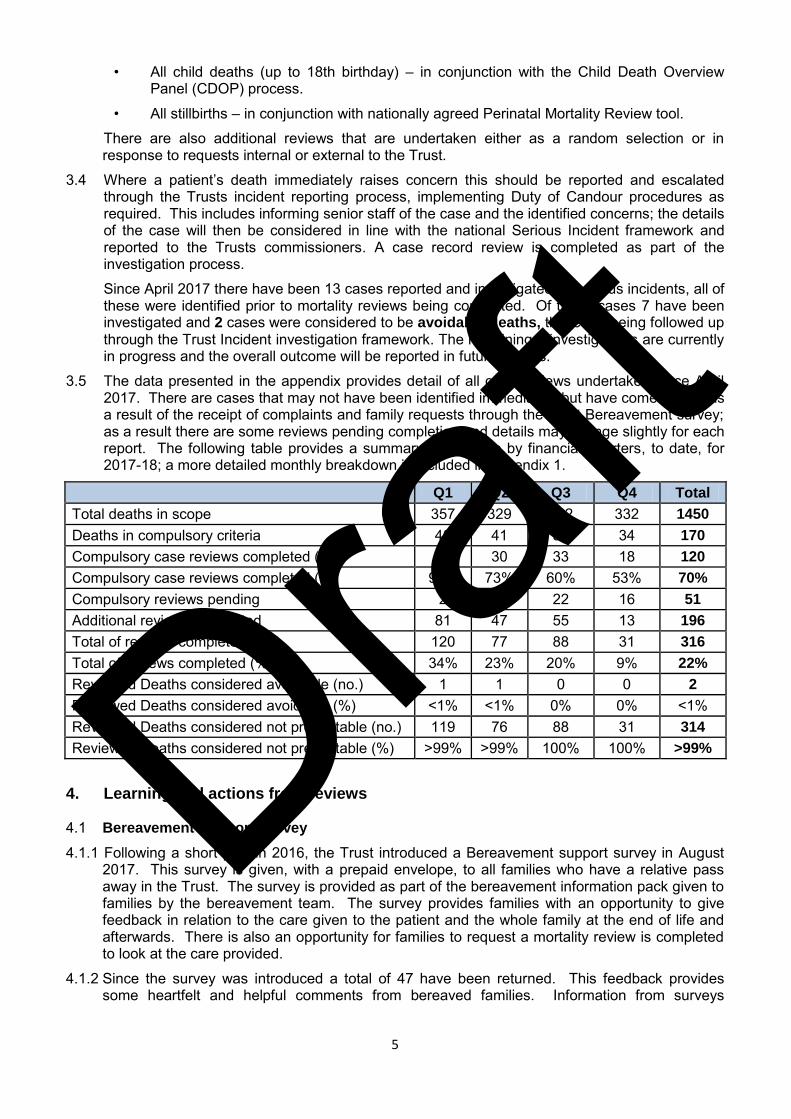
5
• All child deaths (up to 18th birthday) – in conjunction with the Child Death OverviewPanel (CDOP) process.
• All stillbirths – in conjunction with nationally agreed Perinatal Mortality Review tool.
There are also additional reviews that are undertaken either as a random selection or in response to requests internal or external to the Trust.
3.4 Where a patient‟s death immediately raises concern this should be reported and escalated through the Trusts incident reporting process, implementing Duty of Candour procedures as required. This includes informing senior staff of the case and the identified concerns; the details of the case will then be considered in line with the national Serious Incident framework and reported to the Trusts commissioners. A case record review is completed as part of the investigation process.
Since April 2017 there have been 13 cases reported and investigated as serious incidents, all of these were identified prior to mortality reviews being completed. Of these cases 7 have been investigated and 2 cases were considered to be avoidable deaths, these are being followed up through the Trust Incident investigation framework. The remaining 6 investigations are currently in progress and the overall outcome will be reported in future reports.
3.5 The data presented in the appendix provides detail of all case reviews undertaken since April 2017. There are cases that may not have been identified immediately but have come to light as a result of the receipt of complaints and family requests through the Trust Bereavement survey; as a result there are some reviews pending completion and details may change slightly for each report. The following table provides a summary of the data by financial quarters, to date, for 2017-18; a more detailed monthly breakdown is included in appendix 1.
Q1 Q2 Q3 Q4 Total
Total deaths in scope 357 329 432 332 1450
Deaths in compulsory criteria 40 41 55 34 170
Compulsory case reviews completed (no.) 39 30 33 18 120
Compulsory case reviews completed (%) 95% 73% 60% 53% 70%
Compulsory reviews pending 2 11 22 16 51
Additional reviews completed 81 47 55 13 196
Total of reviews completed (no.) 120 77 88 31 316
Total of reviews completed (%) 34% 23% 20% 9% 22%
Reviewed Deaths considered avoidable (no.) 1 1 0 0 2
Reviewed Deaths considered avoidable (%) <1% <1% 0% 0% <1% Reviewed Deaths considered not preventable (no.) 119 76 88 31 314
Reviewed Deaths considered not preventable (%) >99% >99% 100% 100% >99%
4. Learning and actions from reviews
4.1 Bereavement Support Survey
4.1.1 Following a short pilot in 2016, the Trust introduced a Bereavement support survey in August 2017. This survey is given, with a prepaid envelope, to all families who have a relative pass away in the Trust. The survey is provided as part of the bereavement information pack given to families by the bereavement team. The survey provides families with an opportunity to give feedback in relation to the care given to the patient and the whole family at the end of life and afterwards. There is also an opportunity for families to request a mortality review is completed to look at the care provided.
4.1.2 Since the survey was introduced a total of 47 have been returned. This feedback provides some heartfelt and helpful comments from bereaved families. Information from surveys
Draft

6
returned to date has been shared with relevant teams as it is received. Currently all information received is being collated and an overall summary will be prepared and shared with the relevant groups of teams. Areas of focus for improvement will be identified and an improvement plan initiated.
4.1.3 The Bereavement team are committed to ensuring those they care for are given the highest quality of experience at such a sad time. The team are always happy to improve their service and the survey has highlighted issues which they are hoping will be resolved with the actions taken in response to them. The team have summarised some of the learning and actions taken:
The survey highlighted that some who responded felt property was not returned in adignified manner. As a result the team have approached the Trusts charitable funds and asuccessful bid for “dignity bags” was approved, the bags have now been purchased. Theteam are currently looking at a ward level “bereavement pack” that can be given to families/carers at the time of death, this pack will include the updated bereavement booklet, a dignitybag so relatives can gather belongings of the deceased and some other items to aid andsupport at the time of the death. The Bereavement team are working collaboratively withthe End of Life Care Team and are hoping to pilot this project on 3 wards, in the firstinstance, as part of “Dying Matters” awareness week 14th – 18th May 2018 (see section4.5.1 below for further details about this initiative).
A survey responder stated that they were upset at not being able to register a patient‟sdeath due to their relationship status as a partner not being legally recognised in the sameway as a civil or married partner or a blood relative. This was also included in a complaintreceived into the Trust. The Bereavement team have approached the local Registrars teamand a mutual agreement has been made to be sensitive to the relationship status ofpartners. Wherever legally possible as a team they will explore whether a partner couldregister in another qualifying status, for example as a person present at death. The team arein the process of updating the bereavement booklet with this information.
A responder stated they were given incorrect information over an appointment time toregister a death. Although the team could not find how the miscommunication occurred, allstaff booking appointment times with families have been asked to repeat appointment timesback to the bereaved to ensure effective communication, at such a time of distress, can beconfirmed.
4.1.4 As a result of returned surveys there have been 11 requests made for Mortality reviews to be undertaken; all are included within the compulsory reviews outlined in section 3.5 above. Out of these eleven requests, there were 6 requests made where only positive feedback has been given about the care provided to the patient at the end of their life. The other 5 surveys include negative and also some positive feedback; all have been reviewed by the relevant clinical teams and the concerns raised have been addressed directly with the families involved. The content of the feedback will be included in the analysis to be undertaken as described earlier.
4.1.5 The format of this survey has been shared with other Trusts in the north east region following interest in this approach when discussed at the Regional Mortality Review Group.
4.2 Learning disability reviews
4.2.1 As a result of the Trust undertaking LeDER reviews several areas of positive practice have been identified:
Good use of hospital passport, with an understanding of reasonable adjustments to careand recognition of patient deterioration with appropriate actions taken.
Good communication with carers and family has been evident with an emphasis ofworking together in the best interest of the patient.
The care towards the end of life for patient has been exemplary.
Draft
7
4.2.2 The reviews completed by the Trust in relation to patients with learning disabilities form part of a wider multiagency review linking with all services who provided care to the patient. From the reviews undertaken this quarter the Trust has identified the following:
A review raised the issue of long standing health risks and how these are managed. Ahealth risk (obesity) was identified early in the patient‟s life, however there is noevidence of how this was managed or if this was raised with the patient. The patientdied due to complications associated with obesity and anaesthetic. This will bereviewed by the multiagency team to ascertain if this was identified and discussed withpatient by another agency involved in care.
The management of long term health issues and how they are coordinated in thecommunity by involved agencies is a key point; this is to be discussed with themultiagency team at the planned shared case review.
A lack of awareness in relation to an emergency health care plan led to an inappropriatestay in the intensive care unit, although this has not yet gone to multiagency review, ithas raised questions of how and where an emergency health care plan should becommunicated.
4.3 Severe Mental illness
4.3.1 The definition in relation to the cases to be reviewed is yet to be agreed nationally. The Trust has worked in partnership with the main local Mental Health Trust in relation to identifying patient who have died whilst receiving care from both organisations. As both Trusts are required to undertake mortality reviews it will be effective to share the overall findings and learning. Currently there are very low numbers of patients in this group, for this Trust; however as this partnership working develops further there are certain to be shared improvements that can be made and reported in future reports.
4.4 Child Deaths
4.4.1 The numbers of deaths in children in the Trust has remained low during quarter 4.
4.4.2 All child deaths are subject to a nationally agreed review process; reviews of cases are undertaken in the Trust using a multidisciplinary process and this provides information into an overarching multiagency group to ensure that learning is shared across all areas. Where a death occurs in the Neonatal Unit the internal Trust review includes an independent clinician from an adjacent Trust. The review process for child deaths can take up to 6 months to fully complete, report findings and lessons learned.
4.4.3 Of the child deaths reviewed to date in 2017 none have been identified as avoidable and overall good care has been provided in all cases whether this was in Accident and Emergency Department or in the Neonatal Unit.
4.4.4 Deaths in the Neonatal Unit are in general unexpected and unpredictable; however it is important to have access to as much information as possible if a death does occur. When a baby requires early transfer to the Neonatal Unit it is important that the placenta (afterbirth) is examined closely in the laboratory as it can provide vital information. There have been occasions following a death when the placenta was found not to have been examined in such a way and this may have helped the overall review of the case. As a result of this posters have been developed to provide a prompt to midwifery staff to send placentae to be examined in the laboratory if a baby is transferred immediately after its birth to the Neonatal Unit.
4.4.5 The Neonatal team have also identified that following the death of a baby, families do not want a post mortem to be undertaken. The information provided through a post mortem examination can provide invaluable insight into what problems had led to the baby‟s death; if the post mortem is not performed then it is often difficult to provide a full explanation to families. The Neonatal team recognise how difficult it is for families to make such decisions at such a traumatic time; as a result they are examining different approaches towards how staff approach the discussions in relation to post mortems. As deaths are thank fully rare it will be difficult to
Draft
8
assess the impact of this work within a short period, however progress will be reported in future reports.
4.5 End of Life Care
4.5.1 The Trust has been working collaboratively with external organisations as part a national initiative “Dying Matters”. Dying Matters is a coalition of 32,000 members across England and Wales which aims to help people talk more openly about dying, death and bereavement, and to make plans for the end of life. Dying Matters week will run from 14-20 May and aims to raise awareness of the support available to people who need it.
This will involve a fundamental change in society in which dying, death and bereavement will be seen and accepted as the natural part of everybody‟s life cycle. Changes in the way society views dying and death have impacted on the experience of people who are dying and bereaved. A general lack of openness has affected the quality and range of support and care services available to patients and families. It has also affected our ability to die where or how we would wish.
The Dying Matters Coalition is working to address this by encouraging people to talk about their wishes towards the end of their lives, including where they want to die and their funeral plans with friends, family and loved ones.
It is important that the Trust, as an organisation, supports this initiative to get the conversation started and where patients are nearing their end of life; they die as they may have wished.
4.5.2 The Trust are committed to the use of the Amber Care Bundle and its implementation across the organisation, with the project continuing across medical wards currently. The Amber Care Bundle looks to support patients who are unstable, with a limited recovery and have a risk of dying on their admission despite active treatment. By using the Amber Care Bundle, there should be greater opportunity to provide Advance Care Planning and enable patients to achieve their preferred place of care or death.
4.5.3 As a result of learning from deaths and case reviews, Palliative & End of Life Care across the organisation is becoming part of a national project run by Care Opinion and Hospice UK. The 2 year project will look at promoting patients, families and carers to share their stories through the „Care Opinion‟ platform, promoting greater feedback and service development with stories of Palliative & End of Life Care at the heart of our learning, development and delivery of care. The impact of this work will be reported in future reports.
5. Conclusion/Summary
5.1 The Trusts HSMR value in the latest period has increased to 101.32, the SHMI is currently 105.91, both have now been within the expected range for 6 or more consecutive quarters.
5.2 Of the compulsory case reviews identified in the Trusts policy 70% have been reviewed to date; the pending reviews are those which have primarily been identified over quarter 4. Updates on pending reviews will be provided in future reports. Overall to date in 2017-18 the Trust has reviewed 22% of all deaths.
5.3 13 cases were identified as serious incidents, prior to case review. Of these, 7 have been reviewed and 2 were identified as being avoidable. There are a further 6 cases where the investigations are ongoing and updates will be provided in the next report.
5.4 The Trust is continuing to work in close in partnership with Primary Care, Local Authorities, CCGs and a number of other external stakeholders in order to identify where strategic changes can be initiated to support planning and the provision of end of life care across all areas of health and social care.
Draft

9
5.5 The Bereavement survey and the resultant reviews have identified cases where there has been excellent care provision, but has also highlighted some areas for learning that are being analysed.
5.6 There are small numbers of deaths in Trust for children, patients with learning difficulties and significant mental health problems. The reviews undertaken to date show that in the majority of these cases there is evidence of safe, effective and responsive care provision; where there has been concerns identified these have been investigated in full.
5.7 There are areas where continued improvements are needed; these have been identified and each has ongoing monitoring in place. The Trust Outcome, Performance, Delivery Operational Group and the Patient Safety and Quality Standards Committee seek further assurance in relation to these areas in line with their terms of reference.
6. Recommendations
6.1 The Board of Directors are asked to note the content of this report and the information provided in relation to the reduction in the Trusts mortality rates.
6.2 The Board are asked to note the on-going work programme to maintain the mortality rates within the expected range for the organisation.
Dr D Dwarakanath Medical Director
Draft
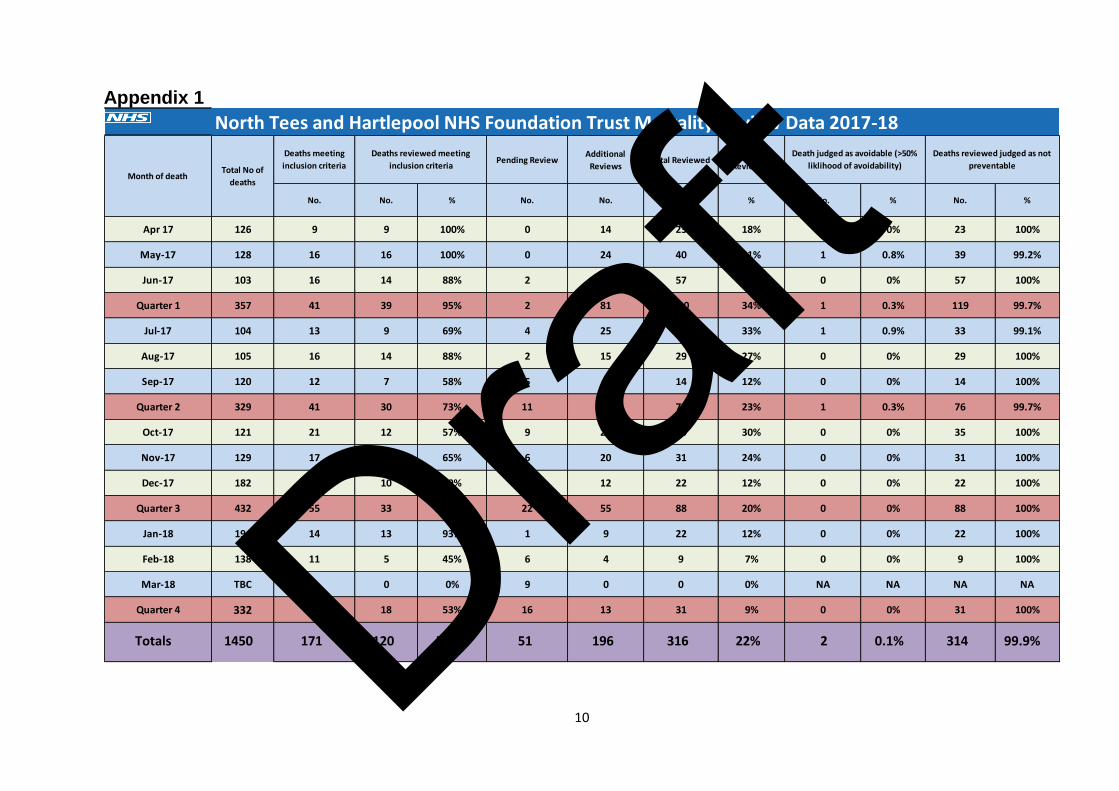
10
Appendix 1
Pending ReviewAdditional
ReviewsTotal Reviewed
Overall %
Reviewed
No. No. No. No. % No. % No. %
Apr 17 9 0 14 23 18% 0 0% 23 100%
May-17 16 0 24 40 31% 1 0.8% 39 99.2%
Jun-17 14 2 43 57 55% 0 0% 57 100%
Quarter 1 39 2 81 120 34% 1 0.3% 119 99.7%
Jul-17 9 4 25 34 33% 1 0.9% 33 99.1%
Aug-17 14 2 15 29 27% 0 0% 29 100%
Sep-17 7 5 7 14 12% 0 0% 14 100%
Quarter 2 30 11 47 77 23% 1 0.3% 76 99.7%
Oct-17 12 9 23 35 30% 0 0% 35 100%
Nov-17 11 6 20 31 24% 0 0% 31 100%
Dec-17 10 7 12 22 12% 0 0% 22 100%
Quarter 3 33 22 55 88 20% 0 0% 88 100%
Jan-18 13 1 9 22 12% 0 0% 22 100%
Feb-18 5 6 4 9 7% 0 0% 9 100%
Mar-18 0 9 0 0 0% NA NA NA NA
Quarter 4 18 16 13 31 9% 0 0% 31 100%
Totals 120 51 196 316 22% 2 0.1% 314 99.9%
103
Deaths reviewed meeting
inclusion criteria
%
100%
100%
North Tees and Hartlepool NHS Foundation Trust Mortality Review Data 2017-18
Month of deathTotal No of
deaths
126
128
194
138
TBC
332
357
329
432
104
105
120
121
129
182
Deaths meeting
inclusion criteria
No.
9
16
16
11
9
171
34
1450
41
41
55
59%
93%
17
17
14
13
16
12
21
Death judged as avoidable (>50%
liklihood of avoidability)
Deaths reviewed judged as not
preventable
70%
95%
73%
60%
53%
88%
69%
88%
58%
57%
65%
45%
0%Draft