Download - Validacion Escala HPQ

Psychological Reporis, 2003,92,723-734. O Psycholog~cal Rcpom 2003
VALIDATION OF THE HEALTH PERCEPTIONS QUESTIONNAIRE FOR AN OLDER MEXICAN POPULATION '
PETER E. BEAMAN SANDFU REYES-FRAUSTO
Deparfmertf of Sorial Sciertcer Lo~(~hborough University
Center for Research LI Social Policy Loughborough University
CARMEN GARCIA-PENA
Medical Research Co-ordination IMSS-Mexico City
Summay.-The objective was to translate, adapt, and validate the Health Percep- tions Questionnaire for use on an older Mexican popularion. After translating and pretesting, three items were eliminated and answers were dichotomised. In the scale, 24 items were used to interview a representative sample OF 4,966 respondents. Internal consistency was .91. Principal components analysis for categorical data gave Four sirni- lar factors to those reported in the original version. Scoring was made by weighting items, using (A) homogeneous values (1 or 2) or (B) factor loadings (0-1.0). Scoring A is proposed for clinical settings or research since no daerences were Found and this procedure is easier to compute. Objective health indicators such as chronic dis- eases, depression, incontinence, death during Follow up, and disability were associated with the self-perception of health measured with the revised version.
The unmet health needs of an increasing number of older people shows (Reyes-Frausto, 2001) that the current medical model is not sufficient for un- derstanding and attending to their complexity. The first h i ta t ion is the con- ceptualization of health dominant in western cultures (Sidell, 1995), where people are classified as dl if demonstrable by signs, symptoms, or the clinical laboratory. A more complex concept of health, a state of complete physical, social and mental well-being (WHO, 1946), has been proposed but it in- cludes aspects related with health but not necessarily about health itself (Si- dell, 1995). Over recent years there has been a move towards a more social model of health, which seems to be more appropriate to understand older people's health needs. In this model, adverse effects on physical and psycho- logical well-being are considered as a function of the interaction of the phys- ical and social environment in which people live and age (Thompson, Itzin, & Abendstern, 1990; Sidell, 1995).
A second limitation is the meaning of health. For the older population (Sidell, 1995), this includes having no disease, having physical energy, being
-- - -
'This research was carried out at the Medical Research Unit on A eing, IMSS-QuerCtaro, Mexico. Address enquiries to Perer Beaman, Departmcnr of Social eciences, Loughborough University, Loughborough, Leicestershire LEI1 3TU, UK or e-mail ([email protected]).
724 P. E. BEAMAN, ET AL.
able to do things, and f eehg good. In the medically oriented model the focus is on the first meaning, even when aspects of well-being and social interaction have been considered relevant in medical care (McHorney, 1997).
Health perceptions are subjective and judgmental processes that involve a person's own feelings, ideas, and beliefs about his health (Connelly, Philbrick, Smith, Kaiser, & Wymer, 1989; Cleary, 1997). However, associa- tions with other objective health indicators such as depression (Connelly, et al., 1989; Mder, Parads, Houck, Mazumdar, Ellen, Dew, & Reynolds, 19961, number of chronic dseases (Connelly, et a/., 19891, dependency (Fo- ley, Branch, Madans, Brock, Guralnlk, & Withams, 1990; Whittle & Golden- berg, 1996; Hkbert, Brayne, & Spiegelhalter, 1999), incontinence (Johnson, Kmcade, Bernard, Bushby-Whitehead, Herz-Picciotto, & Defriese, 1998), and mortality (Mossey & Shapiro, 1982; Foley, et a/., 1990; Menec, Chipper- field, & Perry, 1999) have been reported. Ln that sense, health perceptions are considered an evaluation of the overall health and a good complement for the comprehensive evaluation of patients in the clinical setting.
Measures of health perceptions have had an uneven development (Jette, Cumrnings, Brock, Crispin, & Naessens, 1981). Previous researchers have used the isolated typical statement, "how would you rate your health?" (Krause & Jay, 1994; Musick, 1996; Shmueli, 1999), and with that question they have reached conclusions even when the meaning of the question could vary according to people's characteristics (Krause &Jay, 1994). Others have used scales vahdated for different groups of the population without follow- ing a strict evaluation of their appropriateness. Finally, some researchers have decided to construct scales because those available did not cover as- pects or questions they wished to evaluate (Streiner & Norman, 1989). How- ever, some of the scales have neither a conceptual basis nor validation.
The Health Perceptions Questionnaire, developed by Ware, Wright, and Synder in 1974, validated two years later (Ware, 1976), and tested in the RAND Health Insurance Study (Ware, Davies-Avery, & Donald, 1978; Brook, Ware, Davies-Avery, Stewart, Donald, Rogers, Wdbams, &Johnston, 1979) fits within the framework of the Health Beliefs Model (Jette, et al., 1981), includes the concept of positive health (McHorney, 1997), and has been reported as reliable and valid (Bell & Femea, 1983; McDowell & Newell, 1996). Items from Ware's original work have been included in the General Health Rating Index (Read, Quinn, & Hoefer, 1987) and in the Medical Outcomes Study (McDowell & Newell, 1996) and derived Short Forms (Ware, 1993). The questionnaire has been used to evaluate percep- tions of health in adult population (Connelly, et al . , 1989; Peterson & Wil- son, 1996; Welsh, Thompson, & Long-Krug, 1999), to evaluate the parents' perceptions of their children's health (Bush, 1997), and adapted to evaluate children's health status directly (Eisen, Ware, Donald, & Brook, 1979).
OLDER MEXICANS' HEALTH PERCEPTIONS 725
In Mexico, there is some experience evaluating self-perception among older people (Alvarez & Brown, 1983; CONAPO, 1994); however, these scales were used without appropriate validation. The objective in this study was to translate, adapt, and vahdate the Health Perceptions Questionnaire for use with older Mexicans.
Translation and Adupration of the Health Percep~ions Questionnaire Twenty-seven items from the health perceptions subscales of the Health
Perceptions Questionnaire (McDowell & Newell, 1996) were translated and backtranslated (English-Spanish-English) (Brislin, 1970; Streiner & Norman, 1989) for use on a Mexican elderly population (used by permission granted by the Oxford University Press, 1nc.~1996). A committee (Brislm, 1970) of three b h g u a l medical researchers reviewed versions both in the target and the source language. Once no changes in meaning in the version in Spanish were found, a pretest (Brislin, 1970) was carried out to identlfy difficulties wth the words used. After the pretest some of the words were modified and the new version was reviewed again. The new version was used in a pilot test with 50 elderly people not included in the sample. On this basis, three items were excluded, since it was clear that they were not understood at all. Then the final questionnaire included 24 items that covered Ware's six health perception subscales. The original Likert-type 5-point scale was changed to a dichotomized 'Yes' or 'NO' response. The 'Don't know' answer was included as an alternative to the other options, but whenever participants selected this option the case was excluded.
Data Collection Elderly people were interviewed at home. The interviewer had to ex-
plain the objective of the project and ask for permission to apply the h i - Mental State Examination (MMSE) before receiving full consent to proceed with the interview (Reyes-Frausto, 2001). Only subjects who obtained 24 points or more on the Mini-Mental State Examination participated in this study.
The interviewer was guided by a highly structured. questionnaire that included measurements of elderly people's health status together with their use of health services and other health inhcators. This group of older peo- ple were followed-up over 405 days on the average (Reyes-Frausto, 2001), and some variables related to the uthzation of services and needs during that period were used as objective measures of health to compare with the results in the scale.
Sample Interviewed respondents (N=5,492) constituted a representative popu-
726 P. E. BEAMAN, ET AL.
lation (Reyes-Frausto, 2001) of those living in Mexico City and covered by the Mexican Institute of Social Security (IMSS) (Garcia-Pefia, Hernhndez- Leyva, Anzures-Carro, & Reyes-Frausto, 1999). Only 4,966 of the 5,492 cases were used given missing values, deaths, or cognitive problems (Reyes- Frausto, 2001). Of the population 61% were women, 62% were living as a couple, and 60% had their own income although for most it was minimum wage. Ln all, 77% had received formal education, but 28% only had three years in elementary school. Of the subjects 32% were between 60 and 64 years old, 27% between 65 and 69, 20% between 70 and 74, 12% between 75 and 79, and 9% were 80 years old or over.
Data Analysis SPSS Version 10 was used in the analysis (NoruSis, 1994). Scores on
some items were reversed to give the same direction to all the categories (a higher score was given to the most positive perception of health). Internal consistency was evaluated using Cronbach alpha. Principal components anal- ysis for categorical data was used to reduce the number of variables to a more simply interpreted group of conceptually related factors (Meulman, 1997). Criteria for accepting a reasonable number of factors were an eigen- value greater than 1 and identhing a conceptual aspect of the various dimensions of the 'health perception'.
The scoring process was made in two different ways, (A) giving the same weight to each question ('2' for the positive direction and '1' for the negative) and (B) using the loading value to weigh the positive answer and 'a zero' value for the negative answer. Ln both forms values were added to get a total score. The maximum score was divided by four using quartiles as the cut-off point to create the categories of very poor, poor, well, and very well.
To evaluate the stabhty of the scale, 25% of the cases were evaluated again two months later. A Pearson correlation between scores in the first and second evaluations was calculated.
The association between the self-perception of health and other objec- tive indicators such as acute and chronic diseases, depression, impairment (hearing or vision) or incontinence, disability [dependency in at least one of the activities of dady living (ADL)], cutting down on activities, death at fol- low-up, or health services uthzation was evaluated by x2.
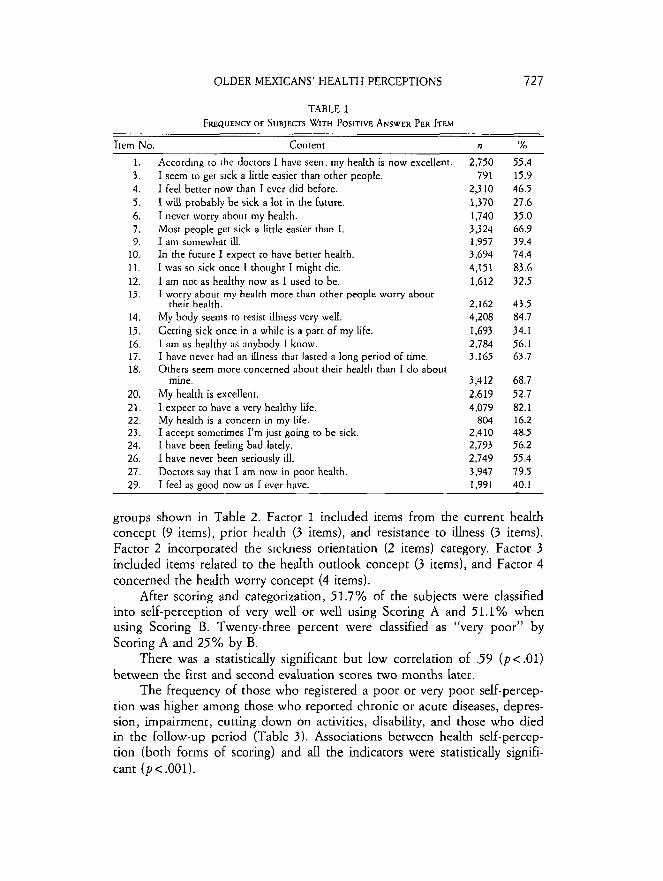
RESULTS Table 1 shows the frequency of the positive perception per item. Items
14, 21, and 27 had the highest proportion of older people with a positive perception while Items 3 , 5 , and 22 had the lowest.
The alpha score derived from the principal components analysis for cat- egorical data with 24 items was .91. Variables reduction resulted in the four
OLDER MEXICANS' HEALTH PERCEPTIONS
TABLE 1 FREQUENCY OF SUBJECTS WITH POSITIVE ANSWER PER ITEM
Item No. Content n YO A c c o r d ~ n ~ ro h e doctors I have seen, my health is now excellent. I seem ro ger s ~ c k a little easier than other people. I feel better now than I ever did before. I will probably be sick a lot in the future. I never worry about my health. Most people get sick a little easier than I. I an1 somewhat ill. In the future I expect to have better health. I was so sick once I thought I might die. I am not as healthy now as I used to be. I worry about my health more than other people worry about
their health. My body seems to resist ~llness very well. Getting sick once in a while is a part of my life. I am as healthy as anybody I know. I have never had an illness that lasted a long period of time. Others seem more concerned about their health than I do about
mme. My health is excellent. I expect to have a very healthy Life. My healcb is a concern in my Ue. I accept sometimes I'm just going to be sick. I have been Feehng bad lately. I have never been seriously LU. Doctors say that I am now in poor health. I feel as eood now as I ever have.
groups shown in Table 2. Factor 1 included items from the current health concept (9 items), prior health (3 items), and resistance to illness (3 items). Factor 2 incorporated the s~ckness orientation (2 items) category. Factor 3 included items related to the health outlook concept (3 items), and Factor 4 concerned the health worry concept (4 items).
After scoring and categorization, 51.7% of the subjects were classified into self-perception of very well or well using Scoring A and 51.1% when using Scoring B. Twenty-three percent were classified as "very poor" by Scoring A and 25% by B.
There was a statistically significant but low correlation of .59 (pc.01) between the first and second evaluation scores two months later.
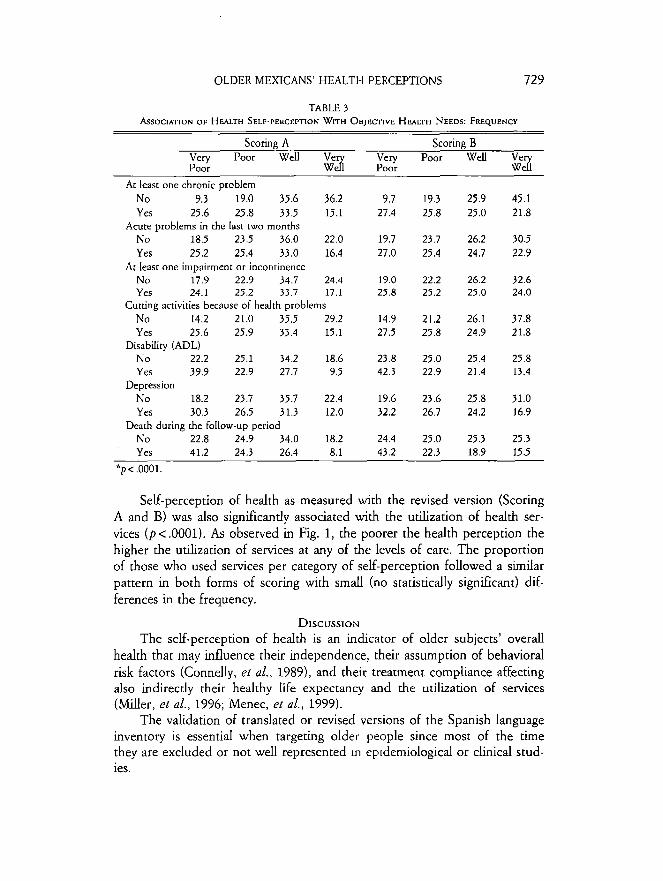
The frequency of those who registered a poor or very poor self-percep- tion was higher among those who reported chronic or acute diseases, depres- sion, impairment, cutting down on activities, disabhty, and those who died in the follow-up period (Table 3 ) . Associations between health self-percep- tion (both forms of scoring) and all the indicators were statistically signifi- cant ( p < .001).
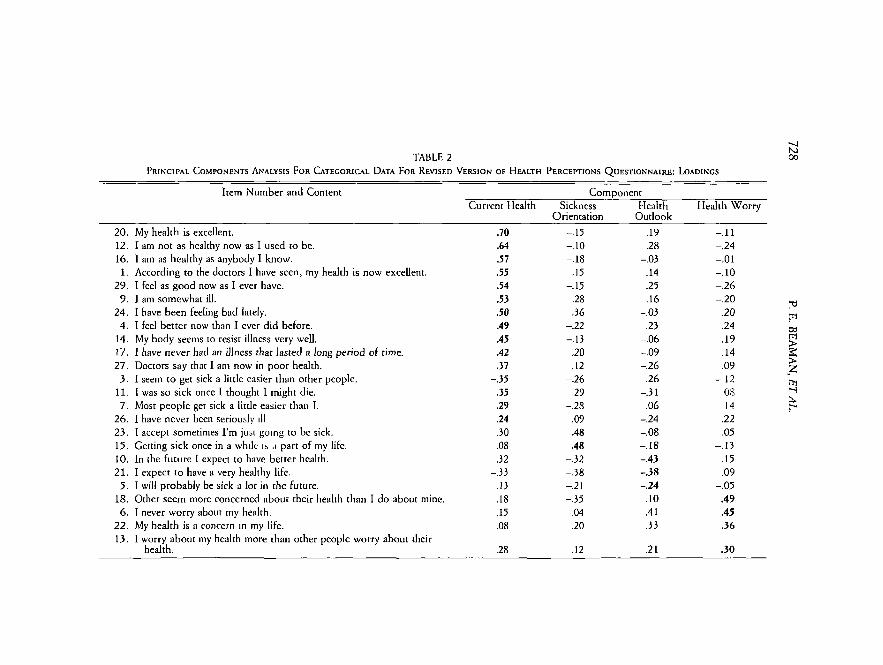
TABLE 2 P R ~ N C ~ P A L COMPONENTS ANALYSIS FOR CATEGORICAL DATA FOR REVISED VERSION OF HFALTH PERCEPTIONS QUESTIONNAIRE: LOADINGS
Item Number and Content C o m ~ o n e n t Current Health Sickness Health Health Worry
Orientation Outlook
20. My health is excellent. 12. I am not as hcalthy now as I used to be. 16. I am as healthy as anybody I know. 1. According to the doctors I have scen, my health is now excellent.
29. I feel as good now as I ever have. 9 . I am somewhat ill.
24. I have been feeling bad lately. 4 . I feel better now than I ever did before.
14. My body seems to resist ilhess very well. 17. I have never had an illness that lasted a long period of time. 27. Doctors say that I am now in poor health.
3 . I seem to get sick a little easier than other people. 11. 1 was so sick once I thought I might die. 7. Most people get sick a little easier than I.
26. I have never been seriously d 23. I accept sometimes I'm just going to bc sick. 15. Getting sick once in a wh~le I > ,I part of my life. 10. In the future 1 expect to have better health. 2 1. 1 expect to have a very healthy life.
5 . I will probably be sick a lot in the future. 18. Other seem more concerned about their health than I do about mine. 6 . I never worry about my health.
22. My health is a concern in my life. 13. I worry about my health more than other people worry about their
health.
OLDER MEXICANS' HEALTH PERCEPTIONS 729
TABLE 3 ASSOCIAT~ON OF HEALTH SELF-PERCEPTION WITH OBJECTIVE HFALTH NEEDS: FREQUENCY
- - ~ ~
Scoring A Scoring B Very Poor Well Very Poor Well Poor b Poor
At least one chronic problem No 9.3 19.0 35.6 36.2 9.7 Yes 25.6 25.8 33.5 15.1 27.4
Acute problems in the last two months No 18.5 23.5 36.0 22.0 19.7 Yes 25.2 25.4 33.0 16.4 27.0
At least one impairment or incontinence No 17.9 22.9 34.7 24.4 19.0 Yes 24.1 25.2 33.7 17.1 25.8
Cutting activities because of health problems No 14.2 21.0 35.5 29.2 14.9 Yes 25.6 25.9 33.4 15.1 27.5
Disability (ADL) No 22.2 25.1 34.2 18.6 23.8 Yes 39.9 22.9 27.7 9.5 42.3
Depression No 18.2 23.7 35.7 22.4 19.6 Yes 30.3 26.5 31.3 12.0 32.2
Death during the EoUow-up period No 22.8 24.9 34.0 18.2 24.4 Yes 41.2 24.3 26.4 8.1 43.2
* p < ,0001.
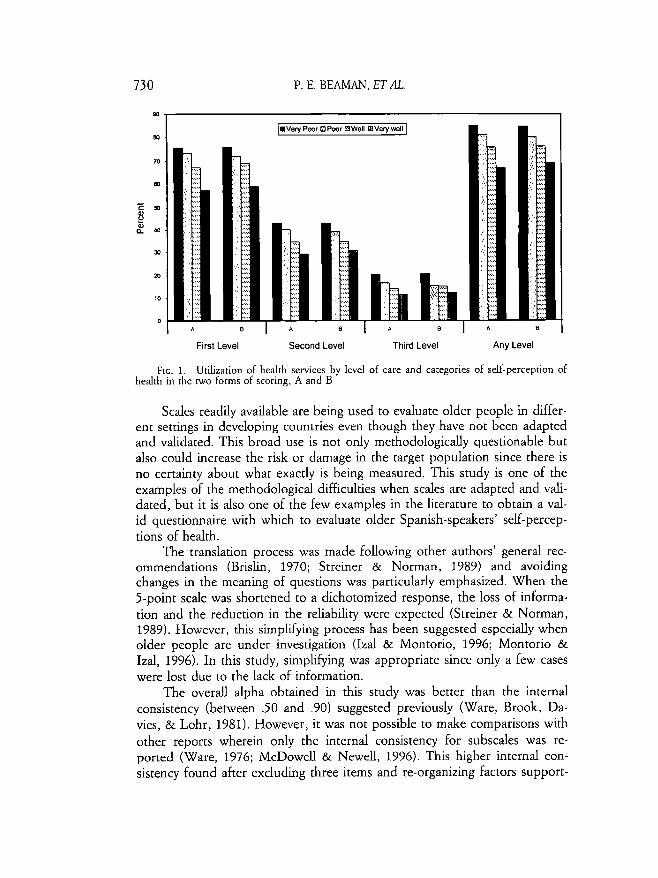
Self-perception of health as measured with the revised version (Scoring A and B) was also significantly associated with the utilization of health ser- vices ( p < .0001). As observed in Fig. 1, the poorer the health perception the higher the udzation of services at any of the levels of care. The proportion of those who used services per category of self-perception followed a similar pattern in both forms of scoring with small (no statistically significant) dif- ferences in the frequency.
DISCUSSION The self-perception of health is an indlcator of older subjects' overall
health that may influence their independence, their assumption of behavioral risk factors (Connelly, et al., 1989), and their treatment compliance affecting also indirectly their healthy life expectancy and the utilization of services (Miller, et al., 1996; Menec, et al., 1999).
The validation of translated or revised versions of the Spanish language inventory is essential when targeting older people since most of the time they are excluded or not well represented m ep~demiological or clinical stud- ies.
730 P. E. BEAMAN, E T A .
First Level Second Level Third Level Any Level
FIG. 1. Utilization of health services by level of care and categories of self-perceprion of health in h e two forms of scoring, A and B
Scales readily available are being used to evaluate older people in differ- ent settings in developing countries even though they have not been adapted and vahdated. This broad use is not only methodologicaUy questionable but also could increase the risk or damage in the target population since there is no certainty about what exactly is being measured. This study is one of the examples of the methodological difficulties when scales are adapted and vali- dated, but it is also one of the few examples in the literature to obtain a val- id questionnaire with which to evaluate older Spanish-speakers' self-percep- tions of health.
The translation process was made following other authors' general rec- ommendations (Brislin, 1970; Streiner & Norman, 1989) and avoiding changes in the meaning of questions was particularly emphasized. When the 5-point scale was shortened to a dichotomized response, the loss of informa- tion and the reduction in the reliabhty were expected (Streiner & Norman, 1989). However, this simphfying process has been suggested especially when older people are under investigation (Izal & Montorio, 1996; Montorio & Izal, 1996). In this study, sirnplkying was appropriate since only a few cases were lost due to the lack of information.
The overall alpha obtained in this study was better than the internal consistency (between .50 and .90) suggested previously (Ware, Brook, Da- vies, & Lohr, 1981). However, it was not possible to make comparisons with other reports wherein only the internal consistency for subscales was re- ported (Ware, 1976; McDoweU & Newell, 1996). This higher internal con- sistency found after excluding three items and re-organizing factors support-
OLDER MEXICANS' HEALTH PERCEPTIONS 73 1
ed not only the reconceptualization proposed in this study but also the sig- nificance of this shorter verison.
The stability of the scale after two months is comparable to that re- ported by Ware for the original subscales, and it is slightly lower than that reported for the General Health Rating Index after one year (Ware, 1976; McDowell & Newell, 1996). Rapid changes in the elderly population's health status could explain this lower stability. Then, we would recommend using a shorter period for evaluating the stabdity but a period of at least two months to find observable changes in the self-perception of health in this popula- tion.
Concepts integrated in the perception of health of this older Mexican population were very similar to those originally reported (Ware, et al., 1974; Ware, 1976). The concept of 'current health' is clearly identified as the first factor of our study and accounts for 11.8% of the total variance. This sug- gests that older people are very aware of the importance of their present health (Read, et al., 1987). In this revised verison, the current health con- cept included items from prior health and resistance to illness. Frequent and rapid changes observed in older people's health status could explain why they interpreted past health or resistance as part of their present health con- cept. The second, third, and fourth factors were similar to the subscales reported by Ware, et al.
The external vahdation achieved by comparing with objective indicators of health reinforces the conclusion that health perception is being measured since a higher proportion of people in the negative extreme in each variable were classified in the poor or very poor category and the opposite. Some subjects had a very positive opinion about their health even when they were ill, impaired, or disabled but also the opposite was noted (Connelly, et al., 1989). The psychological process of acceptance and adaptation to the sick role after a period of time could explain the first perception. The poor or very poor self-perception of health among those who did not report a very specific problem could have two different explanations-the under-dagnosis of some chronic problems (Garcia-Peiia, Thorogood, Reyes, Salmeron, & Duran, 2001) and the lack of analysis of all the possible permutations in health needs (one person could have diabetes but not disab~li t~ or impair- ments, while another impairment but not other chronic problems or dis- abhty, and another could have all of them, etc.) among older people. Those with supposed better health conditions and a negative self-perception should be targeted by health programs to assess the current real health status since the association of that self-perception and other negative outcomes has been demonstrated (Miller, et al. , 1996; Whittle & Goldenberg, 1996).
The association of self-perception and the utilization of health services has been reported by Connelly, et al. (19891, but as we said before, the per-
732 P. E. BEAMAN, ET AL.
ception is only one of the factors influencing health behavior (Jette, et al., 1981). Objective health indicators among older people determine health self- perception and drectly or indirectly influence the decision to request me&- cal care. Even with this limitation, as an overall indicator of health, this scale could help clinicians prevent or diagnose early complications of existmg problems by targeting those with poor or very poor self-perception. In con- sequence, reducing health needs could reduce the utilization of other more complex services or levels of care.
Both forms of scoring are equally valuable for classdymg health percep- tions. Using the simplest procedure (Scoring A) could facilitate its use in dif- ferent health settings since this does not require a weighted chart derived from the principal components analysis for categorical data.
Other researchers have attempted to uulize and validate parts of the Health Perceptions Questionnaire (Bell & Femea, 1983; Bentzen & Chris- tiansen, 1993, 1995; Bush, 1997), but this is the first time that it has been selected for vahdation and use in Mexico so no other comparisons are possi- ble.
In conclusion the Health Perceptions Questionnaire-Revised is valid for evaluating self-perceptions of health among older Spanish speakers and could be used as a complement to the physical examination (Applegate, Blass, &
W&arns, 1990) during the comprehensive geriatric evaluation.
REFERENCES
ALVAREZ, R., &BROWN. M. J. (1983) Encuesta de 1as necesidades de 10s ancianos en Mexico. Salud PJblica de Mixico, 25, 21-75.
APPLEGATE. W. B., BUSS, W. B., &WILLIAMS, T. F. (1990) Instruments for the functional assess- ment of older patients. The New England Journal of Medicine, 322, 1207-1214.
BELL, C. E., & FEMEA. I? L. (1983) A corn arative analysis of the health beliefs of older black males and females. The Associalion o r ~ l a c k Nursing Faculty Journal, 4, 66-69.
BENTZEN, N., &CHRISTIANSEN. T. (1993) Current health as a eneral indicator: I. Evaluation of scaling properties. Scandinavian Journal of Primary ~ e a l t ! Care, 11, 207-210.
BENTZEN, N.. &CHIUSTIANSEN, T (1995) Current health as a general indicator: I. Evaluation of reliability and validity. Scanditzavian Journal of Primary Health Care, 13, 21-25.
BWSLIN, R. W. (1970) Back-translation for cross-cultural research. Journal of Cross-Cultural Psychology, 1, 185-216.
BROOK, R. H., WARE, I. E., DAWES-AVERY, A,, STWART, A. L., DONALD, C. A,, ROGERS, W. H., WILLIAMS, K. N., &JOHNSTON, S. A. (1979) Conceplzia~iution and measzrrement for adults in the health insurance study. Vol. VIII. Overview. Santa Monica, CA: Rand. (Publication No. R-1987/8-HEW)
BUSH, M. R. (1997) Lduence of health locus of control and parental health perceptions on follow-through with school nurse referrals. lsmes in Comprehensive Pediatric Nursing, 20, 175-182.
CLFARY, I? D. (1997) Subjective and objective measures of health: which is better when? Jour- nal of Health Services Research Policy, 2, 3-4.
CONNELLY, J. E., PHILBRICK, J . T., SMITH, G. R., KAISER, D. L., &WYMER, A. (1989) Health er ceptions of primary care patients and the influence on health care utilization. ~ e & a i Care, 27, s99-s109.
CONSEJO NACIONAL DE POBUCION (CONAPO). (1994) Enmesta nacional sobre la sociodemogri- fica del envejecimiento en Mixico. Database produced by the National Council of Popula- uon in Mexico.
OLDER MEXICANS' HEALTH PERCEPTIONS ,733
EISEN, M., WARE, R., DONND, C. A., &BROOK, R. H. (1979) Measuring components of chil- dren's h e a l ~ s t a t u s . Medical Care, 17, 902.921.
F o ~ c r , D. J., BRANCH, L. G.. ~ ~ A D A N S , J. H., BROCK, D. B., GURMNIK, J . M., &WILLIAMS, T. F. (1990) Physical €unction. In J. C. Cornoni-Huntley, R. R Huncley, & J. J. Feldman (Eds.), Heakh status and wellbeing of the elderly: national heahh and nutrifion examina- tion survey: I. Epidemiological follow-up study. New York: Oxford Univer. Press. Pp. 221- 236.
GARC~A-PESA, C., HERN~NDEZ-LCNA, B., A N Z U R E S - ~ R O . R, &&s-FRAUSTO, S. (1999) Devel- o ment and validation of an inventory to measure satisfaction of users of family medicine Lies in Mexico. Psychological Reports, 84, 677-685.
GARC~A-PEP~A, C., THOROGOOD, M., h, S., SALMERON, I., &DURAN, C. (2001) The prevalence and treatment of h pertension in elderly eople in the Mexican Institute of Social Secur- ity in Mexico. Sal 8ublica de Mexico ( ~ n ~ i s h ) , 43, 415-420.
H~BERT, R., BRAYNE, C., &SPIEGELHALTER, 0. (1999) Factors associated with functional decline and improvement in very elderly community-dwelling population. American Journal of Epidemiology, 150, 501-510.
I x , M., & MONTORIO, 1. (1996) Adaptacibn en nuestro medio de la escala de depresi6n geriicrica (GDS) en distintos sub roupos: residentes en la comunidad y asistentes a hos- pitales de dia. Reuista de ~ e r o n t o l ~ i a , 6, 329-337.
JETE, A. M., CUMMINGS, K. M., BROCK, B. M., CRISPIN, l?, &NAESSENS, J. (1981) The structure and reliability of health belief indices. Health Seruices Research, 16, 81-98.
JOHNSON, T. M., KINCADE, J. E., BERNARD, S. L., BUSHBY-WHITEHEAD, J., HERTZ-PICCIOTTO, I., & DEFRIESE, G. (1998) The association of urinary incontinence with poor self-rated health. The Journal of the American Geriatrics Society, 46, 693-699.
KRAUSE, N. M.. &JAY, G. M. (1994) What do global self-rated health items measure? Medical Care. 32. 930-942. , .
MCDOWELL, I., & NEWELL, C. (1996) Measuring health: a guide to rating scales and question- naires. (2nd ed.) Oxford, UK: Oxford Univer. Press.
M c H o m n , C. k (1997) Generic health measurement: past accomplishments and a measure- ment paradigm for the 21st century. Annals oflnternal Medicine, 127, s743-s750.
MENEC, V. H., CHIPPERFIELD, J. H., &PERRY, R P. (1999) Self-perception of health: a prospec- tive analysis of mortahty, control and health. lournal of Gerontology, 54B, 85-93.
MEULMAN, J . J. (1997) Optimal scaling methods for multivanate calegorical data analysis. (SPSS White Paper) Chicago, IL: SPSS, Inc. Pp. 1-19.
MCLLER, M., PARADIS, C., HOUCK, P.. MAZUMDAR, S., ELLEN, F.. DEW, M. A,, & REYNOLDS, C. (1996) Changes in perceived health status of depressed elderly patients treated until re- mission. American Journal of Psychiatry, 153, 1350-1352.
MONTORIO, I., & IZAL, M. (1996) The Geriatric Depression Scale: a review of its development and uudity. International Psychogeriatrics, 8, 103 - 112.
MOSSEY, 1. M., & SHAPIRO, E. A. (1982) Predictor of mortality among the elderly. American Journal of Public Heakh, 72, 800-808.
MUSICK, M. A. (1996) Religion and subjective health among black and white elders. Journal of Health and Social Behavior, 37, 221-237.
NORUSIS, M. J. (1994) SPSS Professional Statistics 6.1. Chicago, IL: SPSS, Inc. PETERSON, M., &WILSON, J. (1996) ob satishction and perceptions of health. Journal of Ocni-
pational 6 Environmental Med?cihe, 38, 891-898. READ, J. L., QUINN, R. J., & HOEFER, M. A. (1987) Measuring overall health: an evaluation of
three important approaches. Journal of Chronic Disease, 40, s7-21. REYES-FRAUSTO, S. (2001) Population ageing in the Mexican Institute of Soriol Security: economic
and heakh police implications. Mexico City: IMSS-Mexican Foundation €or Health. SHMUEU, A. (1999) Subjective health status and health values in the general population. Medi-
cal Dension Making, 9, 122-127. SIDELL, M. (1995) Heakh in old age: myfh, mystery and management. London, UK: Open Uni-
ver. Press. STEINER, L., &NORMAN. G. R. (1989) Health measurement scales: a practical guide to their de-
velopment and nse. Oxford, U K : Oxford Univer. Press. THOMPSON, I?, ITZIN, C., & ENDS STERN, M. (1990) I don't feel old: the experience of later liJe.
Oxford, UK: Oxford Univer. Press.
734 P. E. BEAMAN, ET AL
WARE, J. E., JR. (1976) Scales for measuring general health perceprions. Health Seruices Research, 11, 396-415.
WARE, 1. E.. JR. (1993) SF-36 Health Szrruey, manual and i~~terpretatiotz guide. Boston, MA: The Health Institute.
WARE, 1. E., JR., BROOK, R. H., DAVIS, A. R., & LOHR, K. N. (1981) Choosing measures of health status for individuals in general populations. American Journal ofPublic Healfh, 7 1 , 620-625.
WARE, J. E., JR. , DAVIES-AVERY, A,, &DONALD, C. A. (1978) Conceptuofization and measurement of health for adrrlts in the heolfh insurance strrdy. Vol. V. General health perceptions. Santa Monica, CA: Rand. (Publication R-198715-HEW)
WARE, J . E., JR., WRIGHT, W. R., & SYNDER, M. K. (19741 Measures of percepiiotrs rcgard~r~~ health status: preliminary Jirzditrgs as to scale reliability, validity and administra!ior~ proce- dures. (PB-242-7263 Springfield, VA: National Technical Service.
WELSH, C. H . T H O ~ ~ P C O W . K . & LONG-KRUG. S. (1999) Evaluation of patient-perceived health status us~ng the M c J ~ c d Outcomes Survey Short-Form 36 in an intensive care unit popu- lation. Cr~/rcol Cure !\lcdlcine, 27, 1466-1471.
WH~TTLE, H., &GOLDI:NBERG. D. (1996) Functional health status and instrument activities of daily living performance in non-inscitutionalized elde1.1y people. ,Totima1 of Advanced A1urs- ine. 23. 220-227.
.2. ,
WORLD HEALTH ORGANIZATION (WHO). (1946) Constitution of the \Y'orld Health Organizafion. Geneva, Switz.: WHO.
Accepted Febnrary 12, 2003







