Prof. Silvio Tatti MD, MSc, Phd, FACOGPast President IFCPC
Hospital de Clínicas “José de San Martín” University of Buenos Aires
Professor Silvio Tatti Past President IFCPC
Introduction and Update of the new
IFCPC nomenclature
Presented at the 7th world congress of the IFCPC in Rome, Italy in 1990. Developed by a Nomenclature Committee headed by Adolf Stafl
Jim Bentley - Canada
Jacob Bornstein - Israel
Peter Bosze – Hungary
Frank Girardi – Austria
Hope Haefner - USA
Michael Menton – Germany
Myriam Perrota – Argentina/
Walter Prendiville – Ireland
Peter Russell - Australia
Mario Sideri – Italy
Bjorn Strander – Sweden
Aureli Torne – Spain
Patrick Walker – UK
Silvio Tatti – Argentina
IFCPC board
4º IFCPC Nomenclature - 2011
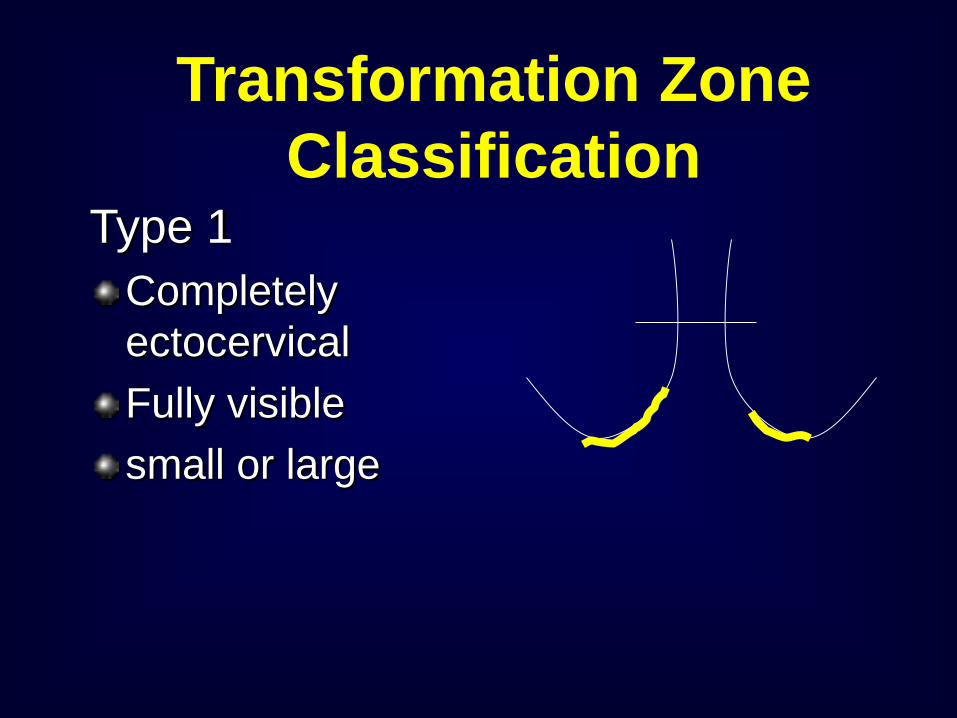
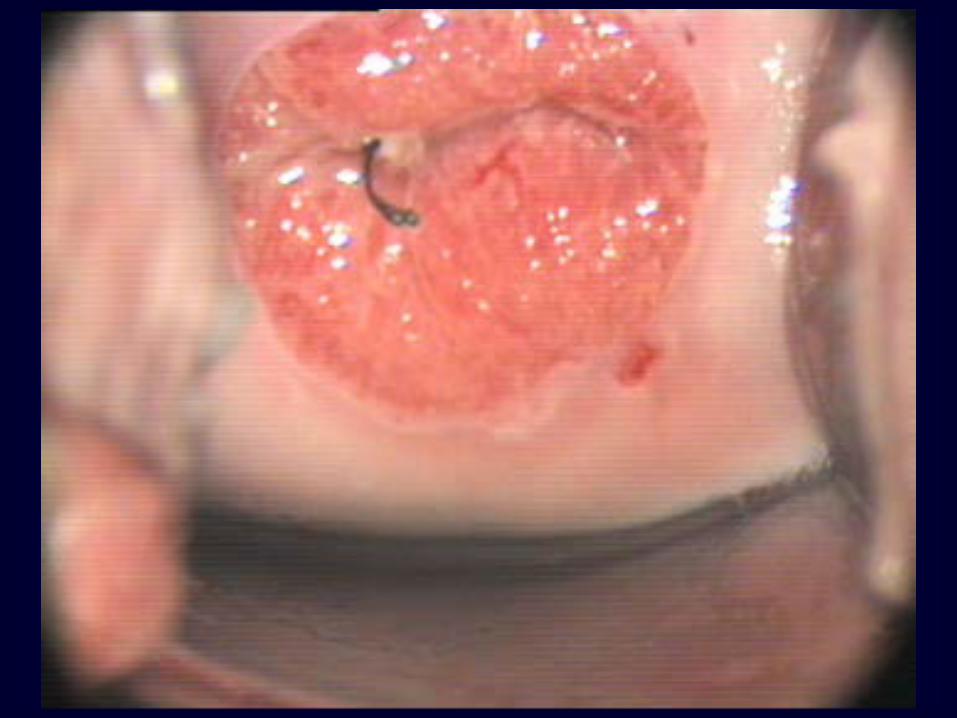
Type 1Completely ectocervicalFully visiblesmall or large
Transformation Zone Classification
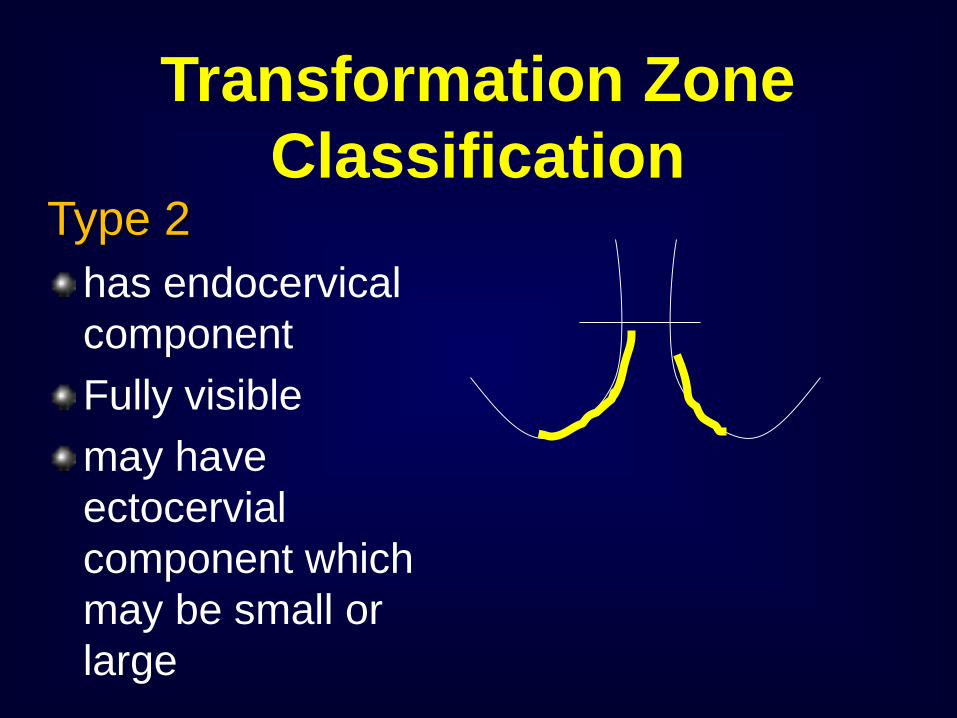
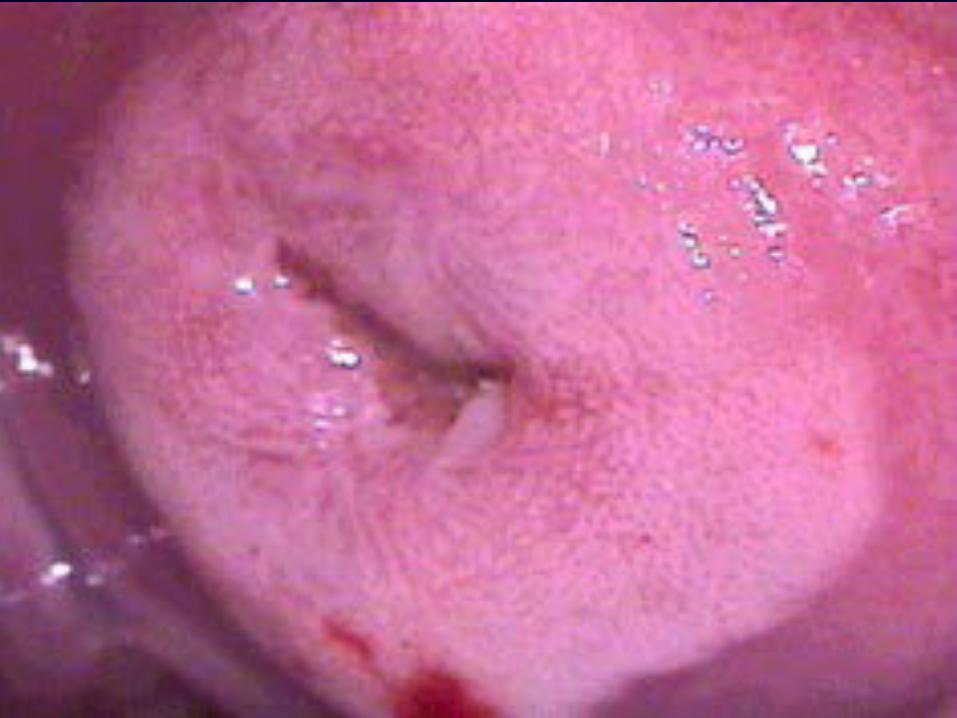
Type 2has endocervical componentFully visiblemay have ectocervial component which may be small or large
Transformation Zone Classification
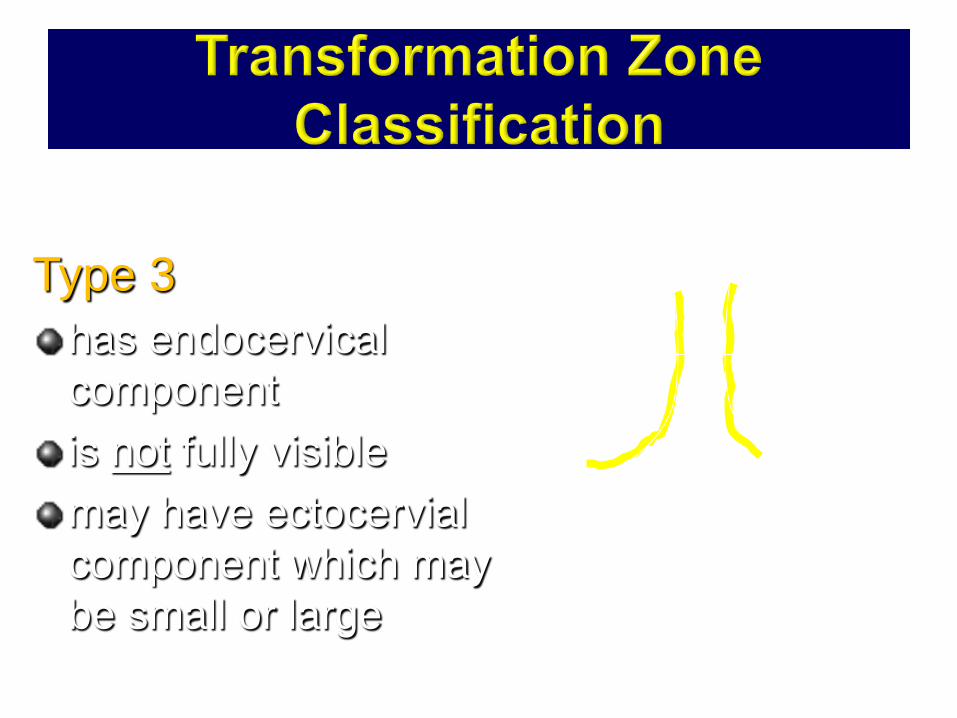
Type 3has endocervical componentis not fully visiblemay have ectocervial component which may be small or large

To avoid using “conization”, “cone biopsy” “Big loop excision”, “small loop excision”
To educate ourselves with the current understanding of how extensive an excision should be done
2011 IFCPC colposcopic terminology - addendum
Excision treatment types
Why do we need a nomenclature of excision treatment types?
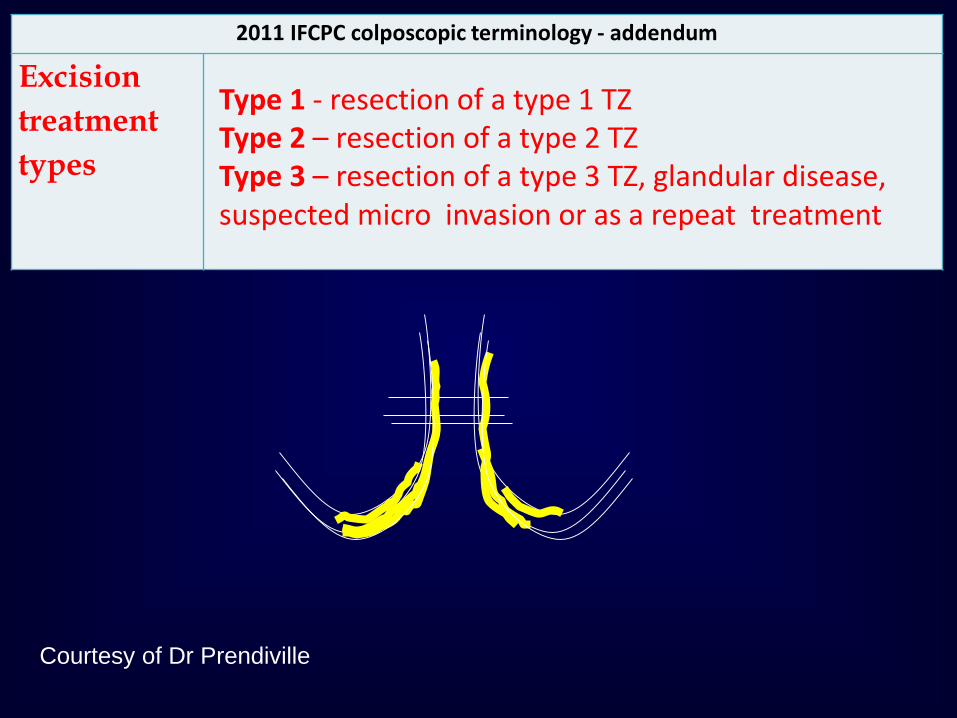
2011 IFCPC colposcopic terminology - addendum
Excision treatment types
Type 1 - resection of a type 1 TZ Type 2 – resection of a type 2 TZType 3 – resection of a type 3 TZ, glandular disease, suspected micro invasion or as a repeat treatment
Courtesy of Dr Prendiville
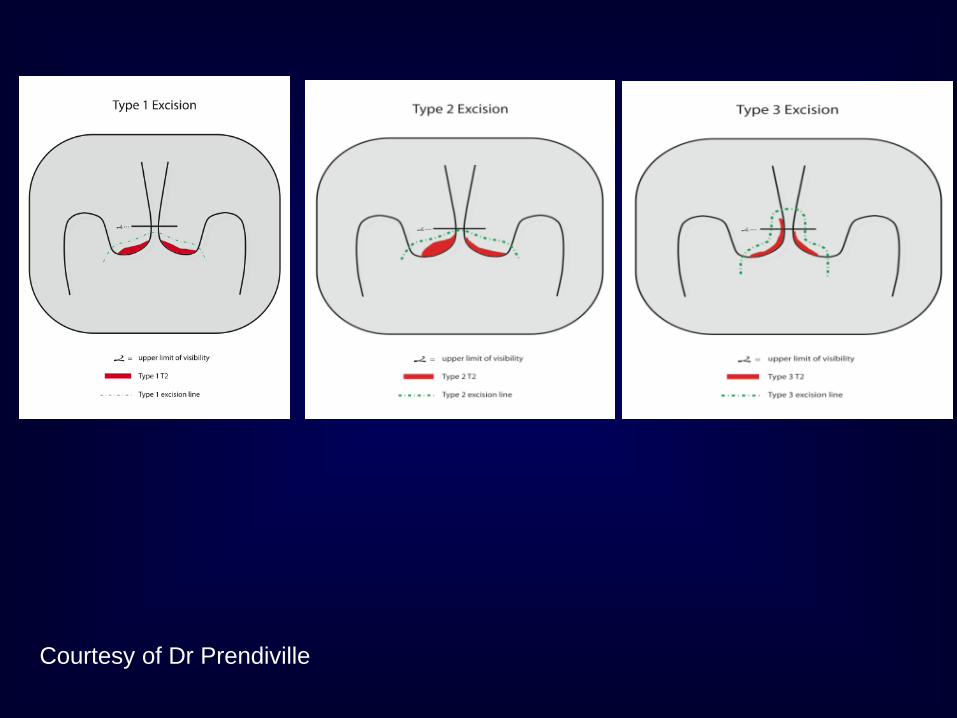
Courtesy of Dr Prendiville
Why do we need a nomenclature of the size of the excised specimen?
The dimensions of the excised specimen are significant to future pregnancy outcome: Systematic reviews documented an increase in pre-term delivery with an increase in the size of the excised specimen
Studies sometimes used : “cone height”, “cone depth“, etc.
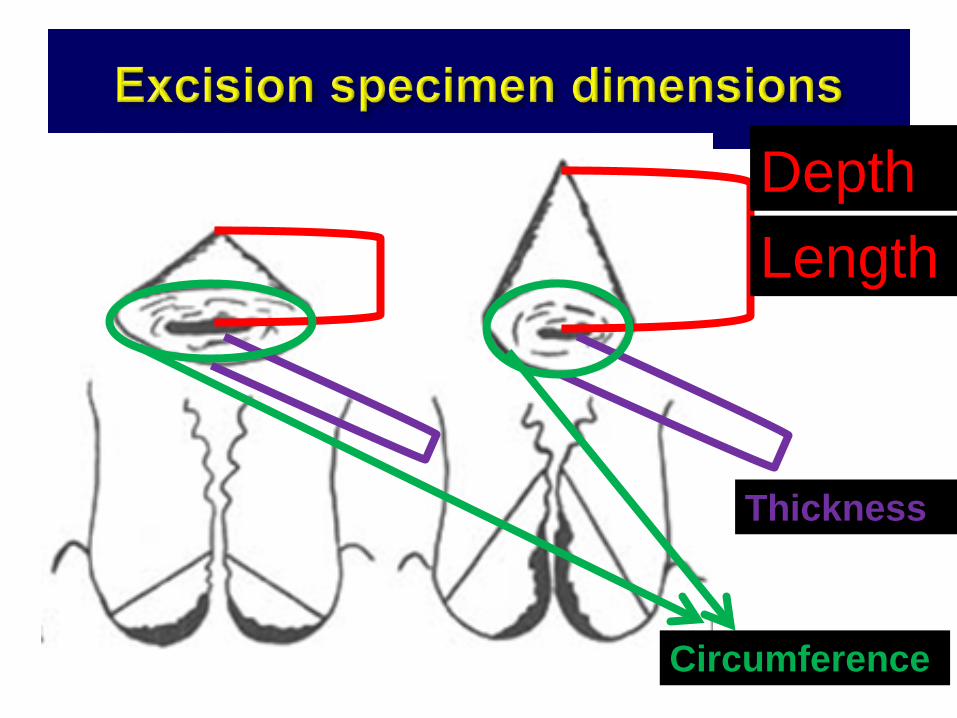
Length
Thickness
Circumference
HeightDepth
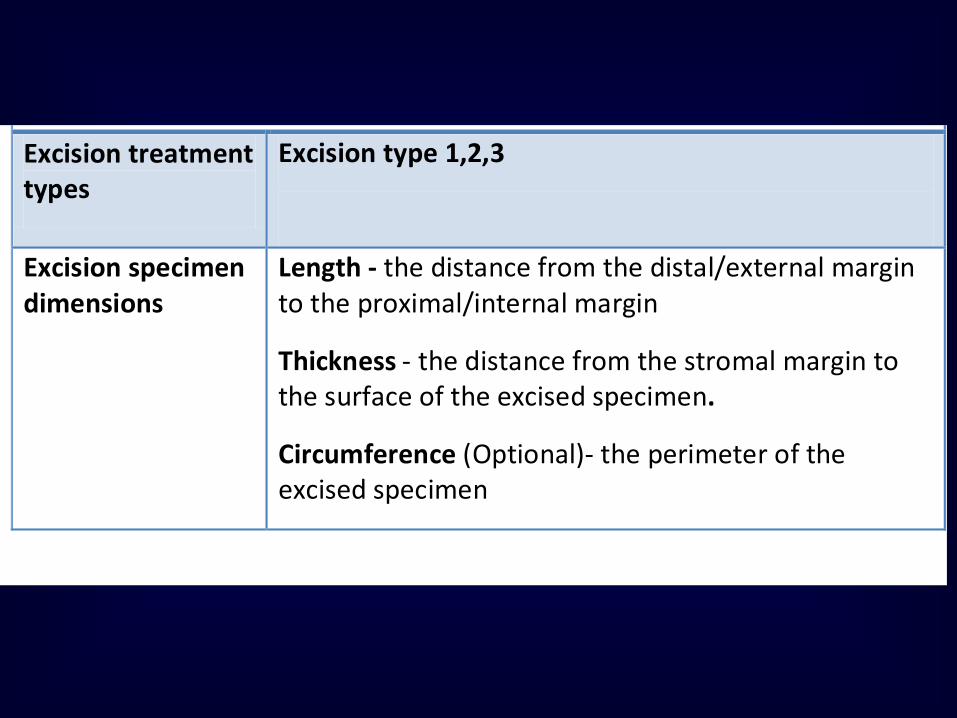
Excision type 1,2,3
Excision treatment types
Length - the distance from the distal/external margin to the proximal/internal margin
Thickness - the distance from the stromal margin to the surface of the excised specimen.
Circumference (Optional)- the perimeter of the excised specimen
Excision specimen dimensions

Terminology : 3 fundamental principles
1.Communicate clinically relevant information from the laboratory to the patient’s health care provider.2.Uniform and reasonably reproducibleacross different pathologists and laboratories and also flexible enough to be adapted in a wide variety of lab settings and geographic locations3.Reflect the most current understanding of the disease process
These principles were adopted by the LAST Project
Robert J. Kurman, MD Forward to the Bethesda Atlas, 2nd edition
What is LAST?
A unified histopathological nomenclature Use a single set of diagnostic term It is recommended for all HPV-associated
preinvasive squamous lesions of the lower anogenital tract (LAT).
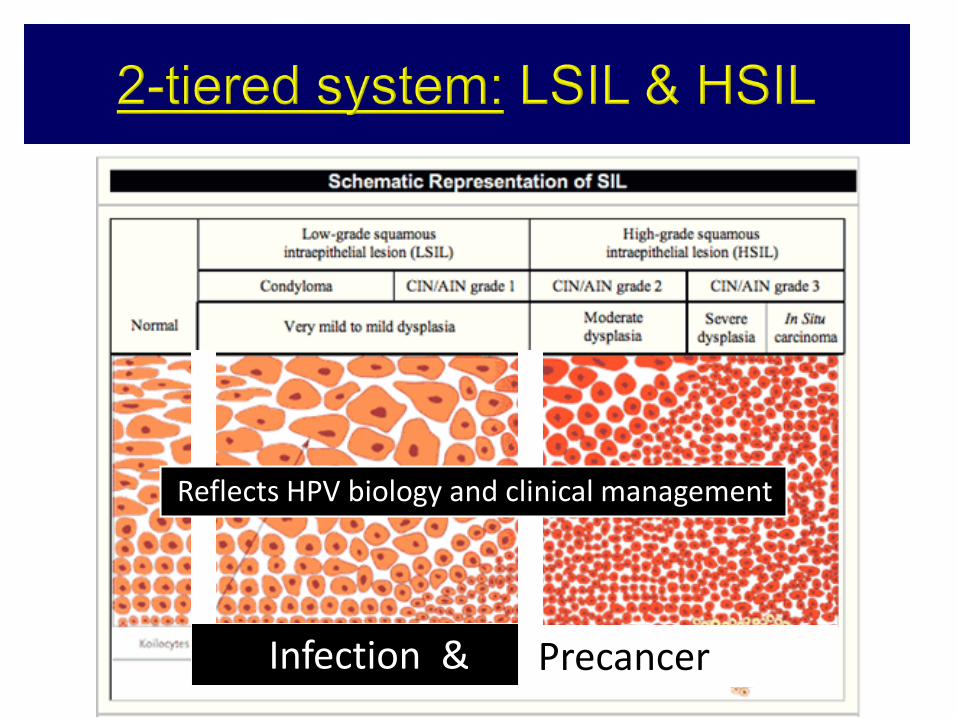
PrecancerInfection &
Reflects HPV biology and clinical management
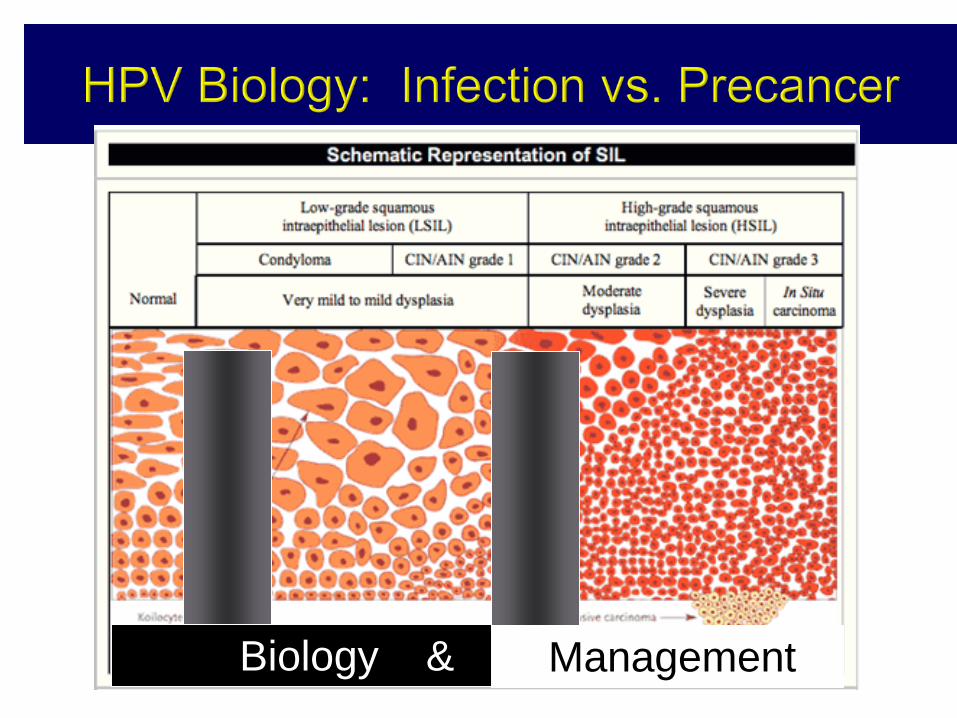
Management Biology &
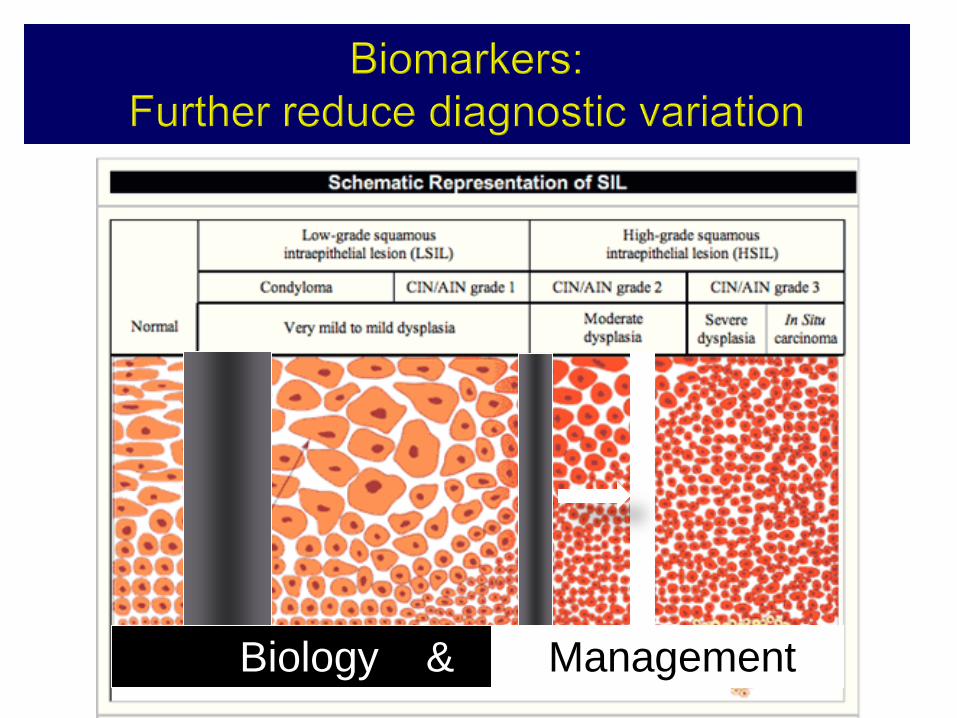
Biology & Management
The difficulty of pathologists (H E) is to interpretate –IN2 lesions
The interobserver agreement for CIN 2 is Benign Kappa 0.52 CIN1 Kappa 0.24 CIN2 Kappa 0.20 CIN3+ Kappa 0.61
Robertson et al. J Clin Pathol 1989;42:231-8.
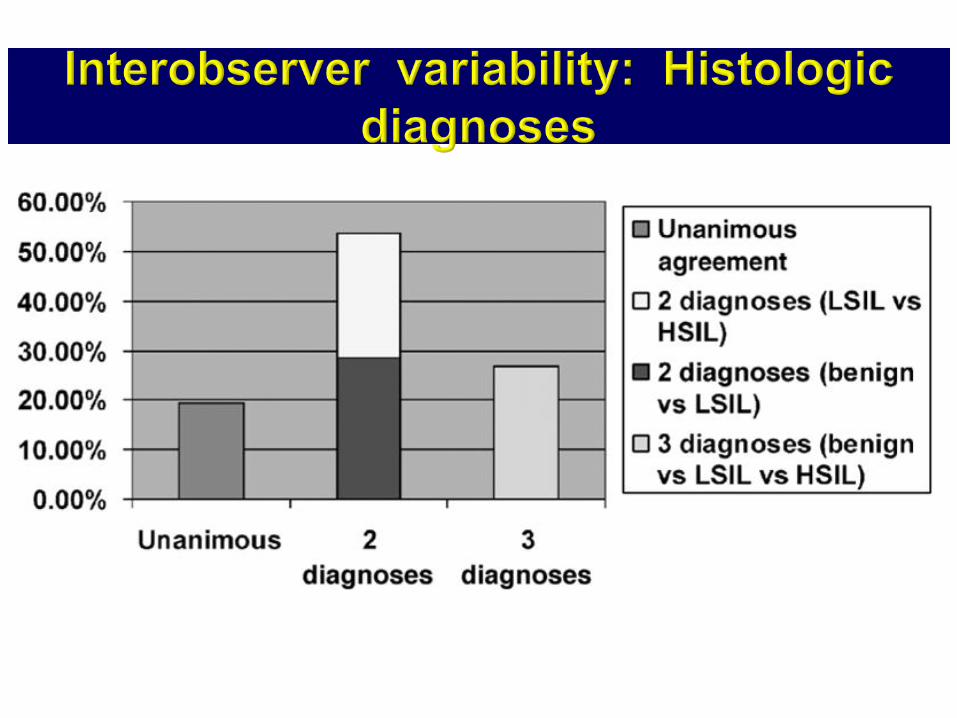
Distribution of 56 cases according to number of different diagnoses – by 22 pathologists From: Ceballos KM: Int J Gynecol Pathol, Volume 27(1).January 2008.101-107
Teresa Darragh MD
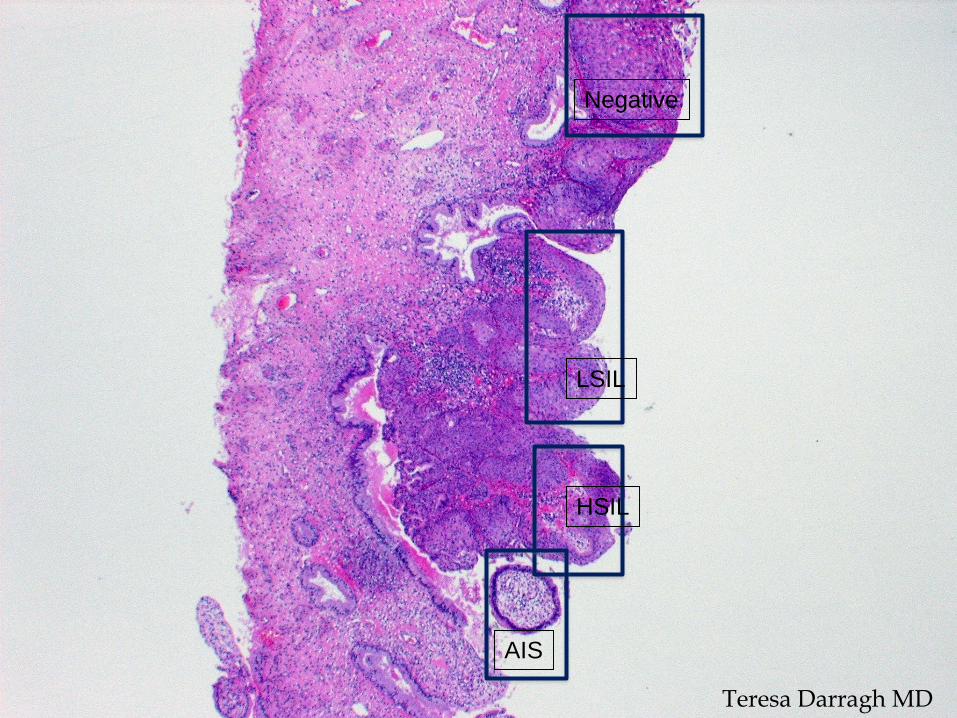
Negative
LSIL
HSIL
AIS
Teresa Darragh MD
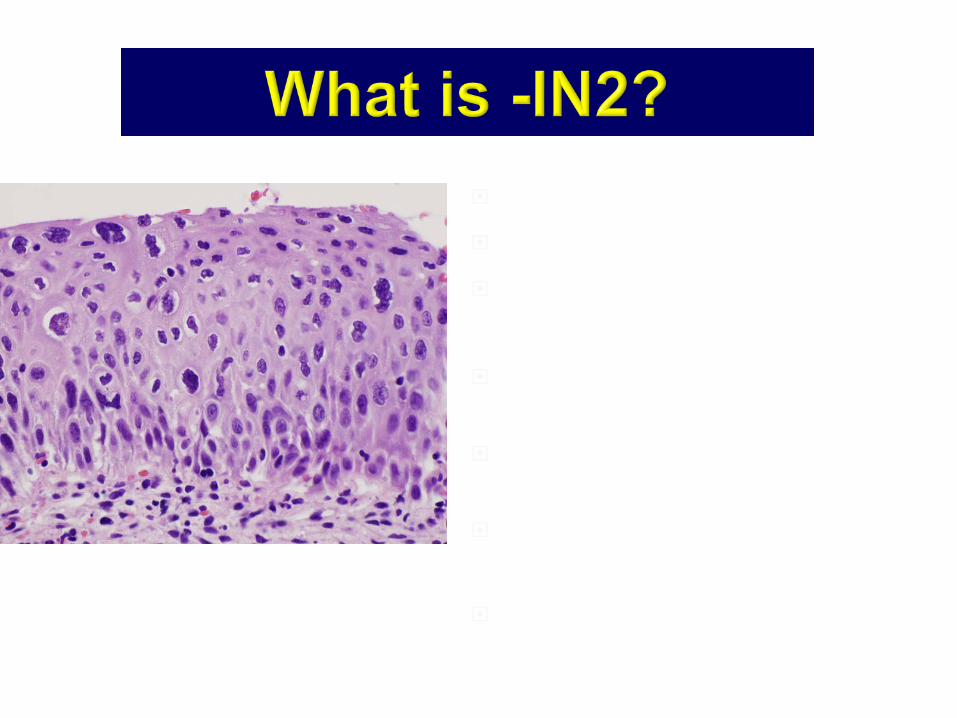
A Distinct Biologic Stage? Ugly Looking CIN1? Not So Ugly CIN3?
An equivocation that is NOT reproducible
A representation of incomplete sampling
~2/3s HSIL; ~1/3 LSIL
A management safety net?Does not reflect our current understanding:
infection vs. precancerTeresa Darragh MD

CIN 2
LSIL
HSIL
P16-
P16+
LAST terminology for the cervix, vulva and
vagina
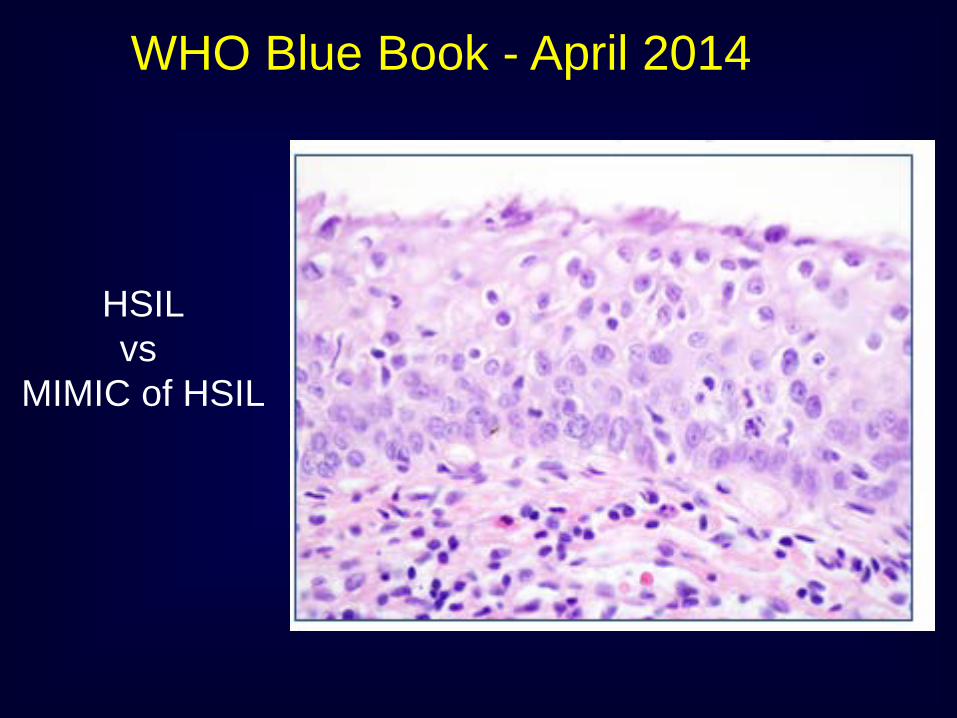
WHO Blue Book - April 2014
HSILvs
MIMIC of HSIL
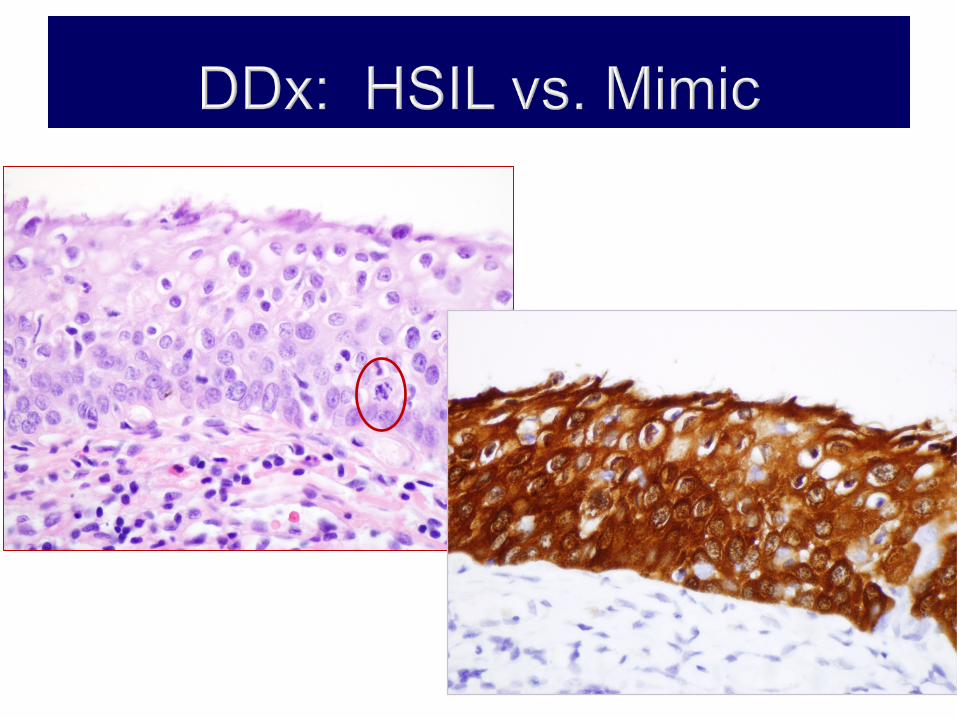
p16 positive = HSILTeresa Darragh MD
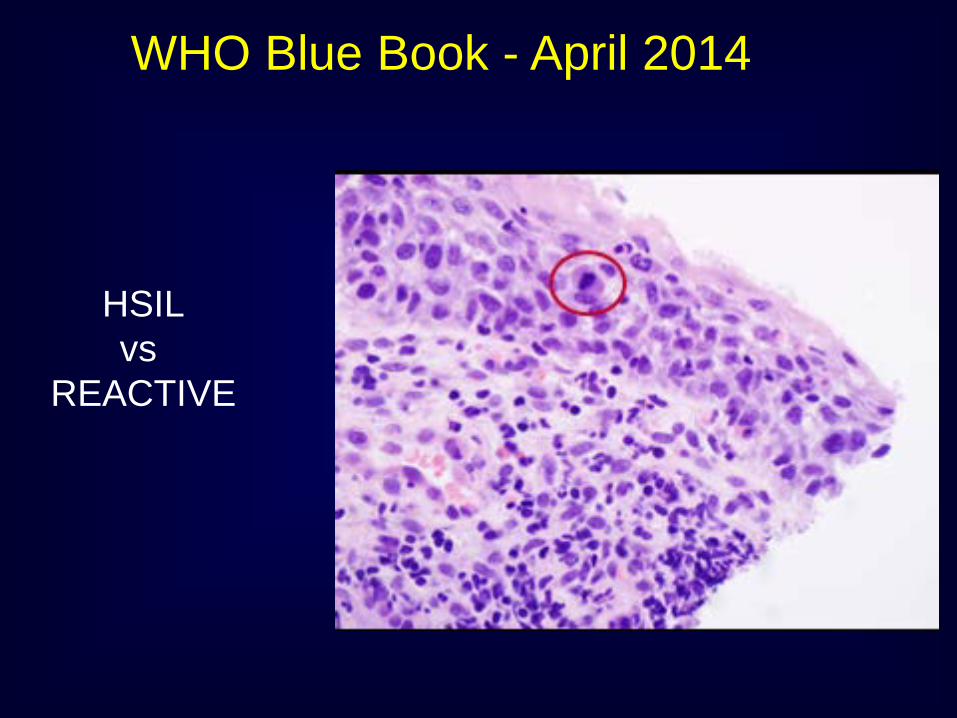
WHO Blue Book - April 2014
HSILvs
REACTIVE
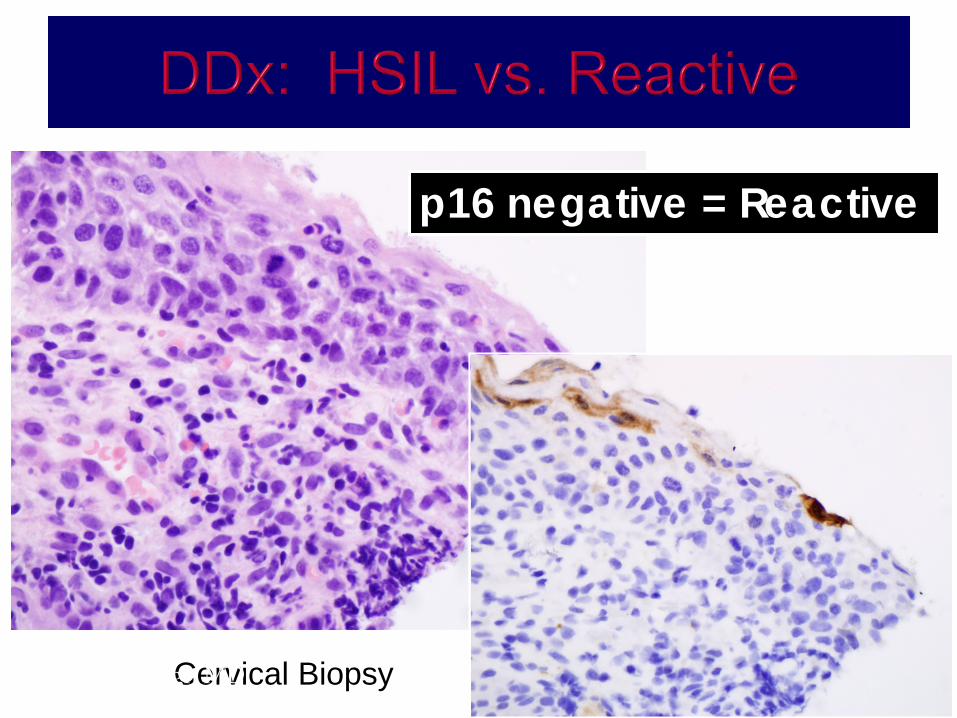
p16 negative = Reactive
Cervical BiopsyTeresa Darragh MD
LAST Recommendations
The morphology suggest HSIL vs mimic a precancer lesion
The morphology suggest CIN 2 and we need to apply p16 to define if this is HSIL or LSIL
To define a disagreement in between two patholgists. One think it is a –IN2 and the other –IN3
Do not recommend the use of p16 in a define –IN1, -IN or Cervical cancer
Conclusions
In the near future the implementation of preventive HPV vaccines in adolescents will produce changes in frequency of HPV lesions in this population and in screening methods (use of molecular tests).
Special Circumstances
The morphology suggests LGSIL, but the cytology results ASC-H, ACG or ASC-US/VPH+16








