
A d a anaesth. scand. 1977, 21, 240-244
Peroperative Arterial Blood Pressure Control in Ophthalmological Anaesthesia RAIMO PIHLAJANIEMI and JYRKI HELVE Departments of Anaesthesia and Ophthalmology, Oulu University Central Hospital, Oulu, Finland
The effects were studied of a standardised general anacsthcsia on mean arterial blood pressure, rentral venous pressure, blood gas values and the course of cataract operations. The material consisted of 20 unselected senile rataract operations, thc mcan age of the patients being 71.3 years. The arterial blood pressure was con- tinuously checked, using an intra-arterial cannula. In order to avoid vitreous loss, the blood pressure was successfully kept optimally low during the extraction of the lens. No vitreous problems were noted. The oxygenation and ventilation of the patients were sufficient during anaesthesia and immediately postoperatively.
Received 18 August, accefited for publication 31 August 1976
Between September 1969 and December 1971, practically all adult cataracts at our clinic were operated on under local anaes- thesia. Of these 250 cases, 6% had vitreous loss. These cataract operations and any sub- sequent operations were performed by both resident and attending surgeons.
After January 1973, practically all adult cataracts were operated on under general anaesthesia. In the first 114 cataract opera- tions carried out under general anaesthesia, no vitreous loss was found. But then our anaesthetist, who had worked continuously with ophthalmologists, was moved to another department, and his place was taken by various colleagues. During this time the frequency of vitreous loss in cataract surgery returned to the 6% level, although the method of anaesthesia remained the same. The basic problem seemed to be that the anaesthesia was too light. In situations in which the iris- lens diaphragm was protruding upwards, the level of arterial blood pressure was often clearly higher than earlier measurements had shown. It has been noted in the literature that lowering of arterial blood pressure, in con- junction with sufficient oxygenation and hyperventilation, reduces the intraocular
pressure (EDRIDGE 1963, ADAMS & BARNET'I. 1966, GENBE & v. GRAEFES 1974).
The purpose of this study is to determine how the mean arterial pressure can be con- trolled in routine cataract operations by using a standardised anaesthesia. Special emphasis was laid on active lowering of the arterial blood pressure by deepening the anaesthesia before the extraction of the lens.
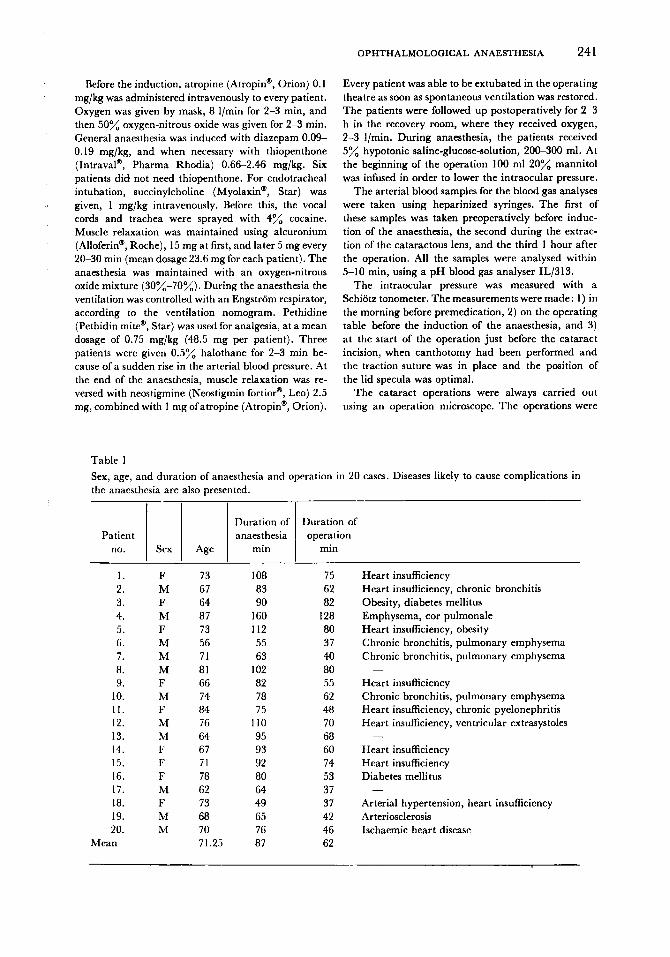
MATERIAL AND METHODS The material for this study consisted of 20 unselected patients, 11 men and 9 women with scnilc cataracts. The patients' consent was obtained. The operation was performed under general anaesthesia, and diseases complicating the anaesthesia were noted preoperatively in 17 cases. The mean age of the patients was 71.3 years, with a minimum of 56 and a maximum of 87 years. The mean duration of the operation was 61.8 min and that of the anaesthesia was 86.6 min (Table I ) . None of the cataracts was hypermature. One patient had well-controlled glaucoma simplex.
Diazepam (Diapam@', Orion) was given as premedi- cation, 10 mg orally 1-2 h before the anaesthesia. The right radial artery and basilica1 vein werc cannulatrd in the operating theatre for continuous measurement\ of the arterial blood pressure and the central venous pressure. The pulse wave and the electrocardiogram were checked continuously. An intravenous cannula was used for injection and fluid therapy.
OPHTHALMOLOGICAL ANAESTHESIA 24 1
Patient no. Sex Age
Before the induction, atropine (Atropin", Orion) 0.1 mg/kg was administered intravenously to every patient. Oxygen was given by mask, 8 l/min for 2-3 min, and then 50% oxygen-nitrous oxide was given for 2-3 min. General anaesthesia was induced with diazepam 0.09- 0.19 mg/kg, and when necessary with thiopenthone (Intraval", Pharma Rhodia) 0.66-2.46 mg/kg. Six patients did not need thiopenthone. For endotracheal intubation, succinylcholine (Myolaxin@, Star) was given, 1 mg/kg intravenously. Before this, the vocal cords and trachea were sprayed with 4% cocaine. Muscle relaxation was maintained using alcuronium (Alloferin@, Roche), 15 mg at first, and later 5 mg every 20-30 min (mean dosage 23.6 mg for each patient). The anaesthesia was maintained with an oxygen-nitrous oxide mixture (30%-70%). During the anaesthesia the ventilation was controlled with an Engstrom respirator, according to the ventilation nomogram. Pethidine (Pethidin mite@, Star) was used for analgesia, at a mean dosage of 0.75 mg/kg (48.5 mg per patient). Three patients were given 0.5% halothane for 2-3 min be- cause of a sudden rise in the arterial blood pressure. At the end of the anaesthesia, muscle relaxation was re- versed with neostigmine (Neostigmin fortior@, Leo) 2.5 mg, combined with 1 mg ofatropine (Atropin", Orion).
Duration of Duration of anaesthesia operation
min min
Every patient was able to be extubated in the operating theatre as soon as spontaneous ventilation was restored. The patients were followed up postoperatively for 2-3 h in the recovery room, where they received oxygen, 2-3 I/min. During anaesthesia, the patients received 5% hypotonic saline-glucose-solution, 200-300 ml. At the beginning of the operation 100 ml 20% mannitol was infused in order to lower the intraocular pressure.
The arterial blood samples for the blood gas analyses were taken using heparinized syringes. The first of these samples was taken preoperatively before induc- tion of the anaesthesia, the second during the extrac- tion of the cataractous lens, and the third 1 hour after the operation. All the samples were analysed within 5-10 min, using a pH blood gas analyser IL/313.
The intraocular pressure was measured with a Schiotz tonometer. The measurements were made: 1) in the morning before premedication, 2) on the operating table before the induction of the anaesthesia, and 3) a t the start of the operation just before the cataract incision, when canthotomy had been performed and the traction suture was in place and the position of the lid specula was optimal.
The cataract operations were always carried out using an operation microscope. The operations were
242 R . PIHLAJANIEMI AND J . HELVE
I P
performed by seven ophthalmologists, of whom four were residents and three were attending surgeons. The incision was made corneally in every case. Alfa-chymo- trypsin was used in only four cases. Iridectomy was per- formed in every case. The lens was always extracted using a cryopencil, and the iris was dilated by means of surgical sponges. The corneal wound was sutured using 8-0 silk sutures. The following stages of the opera- tion were recorded : intubation, canthotomy, traction suture, incision, iridotomy, dilatation of the sphincter, extraction of the lens and suturation of the operation wound.
I intubation d t i o n Iridtomy Extrkdion End of
Wtum the operation
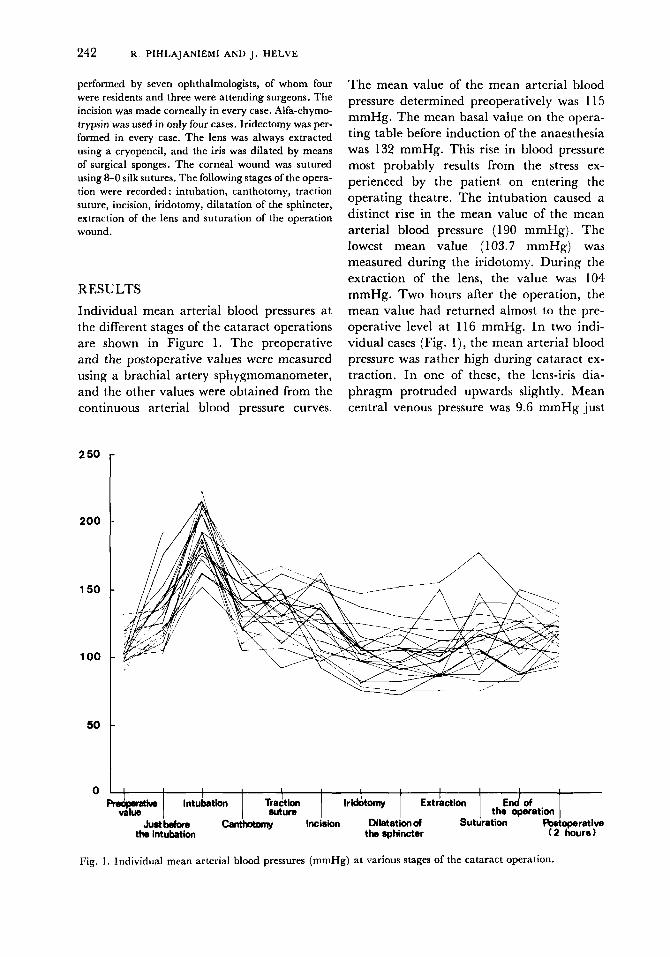
RESULTS Individual mean arterial blood pressures at the different stages of the cataract operations are shown in Figure 1. The preoperative and the postoperative values were measured using a brachial artery sphygmomanometer, and the other values were obtained from the continuous arterial blood pressure curves.
2 50
200
150
100
50
0
The mean value of the mean arterial blood pressure determined preoperatively was 1 15 mmHg. The mean basal value on the opera- ting table before induction of the anaesthesia was 132 mmHg. This rise in blood pressure most probably results from the stress ex- perienced by the patient on entering the operating theatre. The intubation caused a distinct rise in the mean value of the mean arterial blood pressure (190 mmHg). The lowest mean value (103.7 mmHg) was measured during the iridotomy. During the extraction of the lens, the value was 104 mmHg. Two hours after the operation, the mean value had returned almost to the pre- operative level at 116 mmHg. In two indi- vidual cases (Fig. l ) , the mean arterial blood pressure was rather high during cataract ex- traction. In one of these, the lens-iris dia- phragm protruded upwards slightly. Mean central venous pressure was 9.6 mmHg just
Fig. 1. Individual mean arterial blood pressures (mmHg) at various stages of the cataract operation.
OPHTHALMOLOGICAL ANAESTHESIA 243
Preoperative value
Value during the extraction of the Value 1 hour
lens postoperatively
PH
Pace, range
kPa range BE mmol/l range
kPa range Pao,
7.41
5.4 4.3-8.0
+ 1.6
11.3
7.26-7.48
-8.0-+ 12.6
6.5-19.1
7.42
5.0 7.33-7.49
4.0-6.9 - 0.4
- 6.O-+4.5 16.2
6.7-22.7
7.38
2.8-7.2
7.3 1-7.58 5.6
- 1 . 1 -4.8-+3.0
15.1 6.5-22.3
before the induction of anaesthesia, and in- creased to 14.6 mmHg during intubation. Thereafter the CVP values were quite stable at 10.9-12.2 mmHg.
The intraocular pressures were (mean and s.d.) 14.6 mmHgk3.3 in the morning before premedication, 14.9 mmHgf4.8 on the operating table before induction of the anaesthesia, and 14.8 mmHgk5.3 just before the cataract incision. Thus the mild rise in mean arterial blood pressure on the operating table had no influence on the mean value of the intraocular pressure.
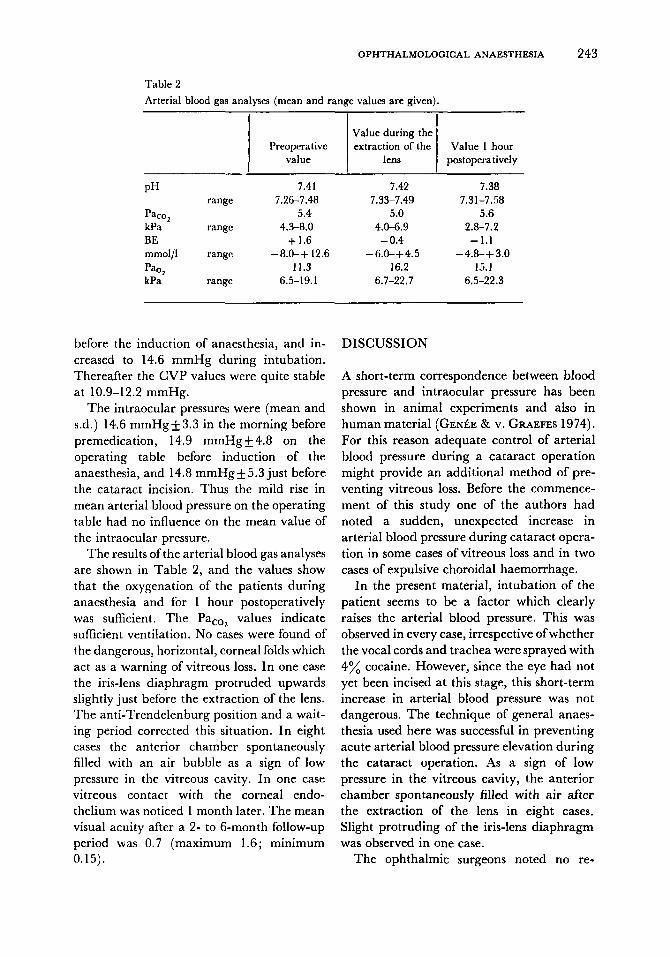
The results of the arterial blood gas analyses are shown in Table 2, and the values show that the oxygenation of the patients during anaesthesia and for 1 hour postoperatively was sufficient. The PacOl values indicate sufficient ventilation. No cases were found of the dangerous, horizontal, corneal folds which act as a warning of vitreous loss. In one case the iris-lens diaphragm protruded upwards slightly just before the extraction of the lens. The anti-Trendelenburg position and a wait- ing period corrected this situation. In eight cases the anterior chamber spontaneously filled with an air bubble as a sign of low pressure in the vitreous cavity. In one case vitreous contact with the corneal endo- thelium was noticed 1 month later. The mean visual acuity after a 2- to 6-month follow-up period was 0.7 (maximum 1.6; minimum 0.15).
DISCUSSION
A short-term correspondence between blood pressure and intraocular pressure has been shown in animal experiments and also in human material ( G E N ~ ~ E & v. GRAEFES 1974). For this reason adequate control of arterial blood pressure during a cataract operation might provide an additional method of pre- venting vitreous loss. Before the commence- ment of this study one of the authors had noted a sudden, unexpected increase in arterial blood pressure during cataract opera- tion in some cases of vitreous loss and in two cases of expulsive choroidal haemorrhage.
In the present material, intubation of the patient seems to be a factor which clearly raises the arterial blood pressure. This was observed in every case, irrespective of whether the vocal cords and trachea were sprayed with 4% cocaine. However, since the eye had not yet been incised at this stage, this short-term increase in arterial blood pressure was not dangerous. The technique of general anaes- thesia used here was successful in preventing acute arterial blood pressure elevation during the cataract operation. As a sign of low pressure in the vitreous cavity, the anterior chamber spontaneously filled with air after the extraction of the lens in eight cases. Slight protruding of the iris-lens diaphragm was observed in one case.
The ophthalmic surgeons noted no re-

244 R . PIHLAJANIEMI AND J . HELVE
actions in any of the patients, and the stable central venous pressure values support this view. An acute increase in the central venous pressure most probably raises the volume of the choroidal and orbital venous plexus.
These undesirable factors, which reduce the volume of the vitreous cavity, were avoided in at least 19 of the 20 cases in this study. When a patient is operated on under local anaesthesia using an operating micro- scope, the lengthy and delicate operation quite often causes some restlessness. An optimal local anaesthesia technique cannot prevent move- ments or coughing in the patient, for example. Continuous control of the arterial blood pressure is, of course, unnecessary as a clinical routine. The experiences of about 500 cataract operations performed under general anaes- thesia since January 1973, and the informa- tion provided by the present study, lead us to recommend measuring of blood pressure relatively often during the critical stages of the cataract operation. If an increase is noted in the arterial blood pressure, it should be
actively lowered by deepening the anaes- thesia. Only after this, can the lens be safely extracted. If general anaesthesia is used, i t seems to be very beneficial to work with an anaesthetist who has a profound knowledge of all the special problems involved in ophthal- mic surgery.
REFERENCES ADAMS, A. K. & BARNETT, K. C. (1966) Anaesthesia
and intraocular pressure. Anaesthesia 21, 202. EDRIDCE, A. (1963) Anaesthetic aspects of hypotension
in eye surgery. Proc. TOY. Soc. Med, 56, 985. G E N ~ E , E. & v. GRAEPES, A. (1974) Manornetrische
Untersuchungen iiber die Abhangigkeit des Augenin- nendruckes vom allgemeinen Kreislaufverhalten unter besonderer Berucksichtigung des Glauko- mauges. Arch. Klin. Exk. Ophthal. 190, 109.
Address:
Raimo Pihlajaniemi, M.D. Department of Anaesthesia Oulu University Central Hospital Oulu Finland







