www.interdigest.ch
PD Dr. Daniel Bimmler
Wenn es prolabiert:(Rektum-)Prolaps oder Hämorrhoiden ?(Handout)
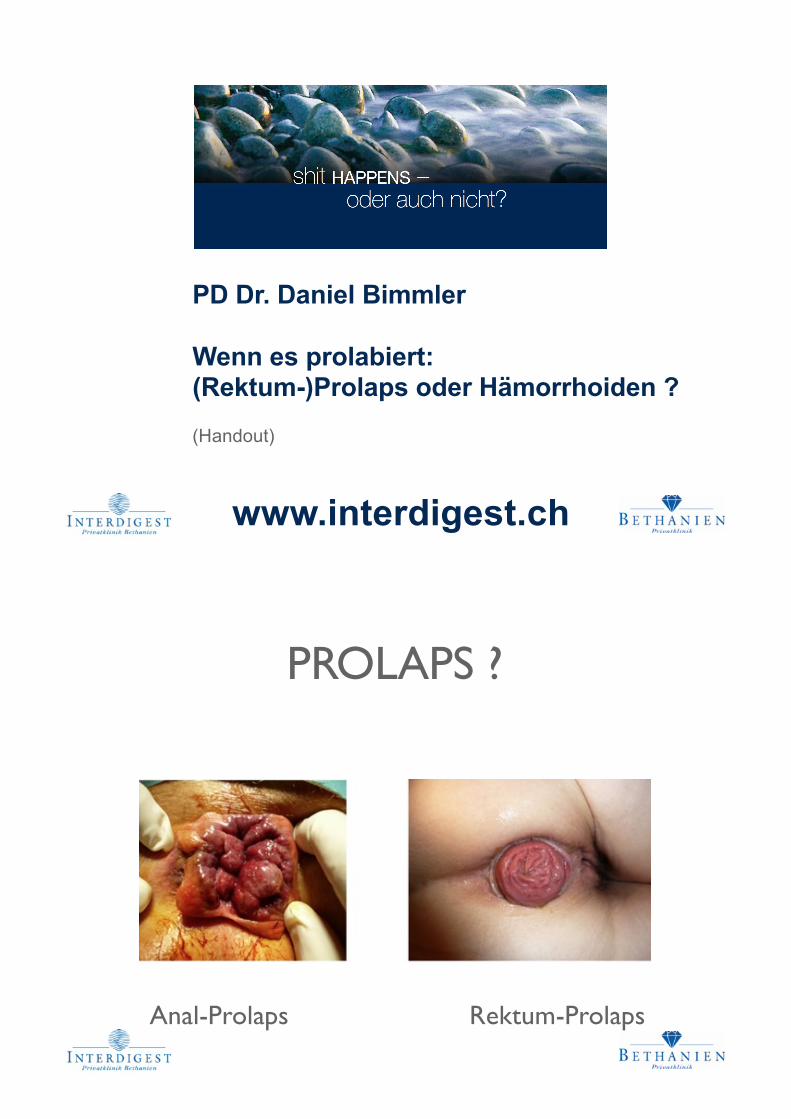
Anal-Prolaps Rektum-Prolaps
PROLAPS ?
Pressen
Prolaps
Inkontinenz
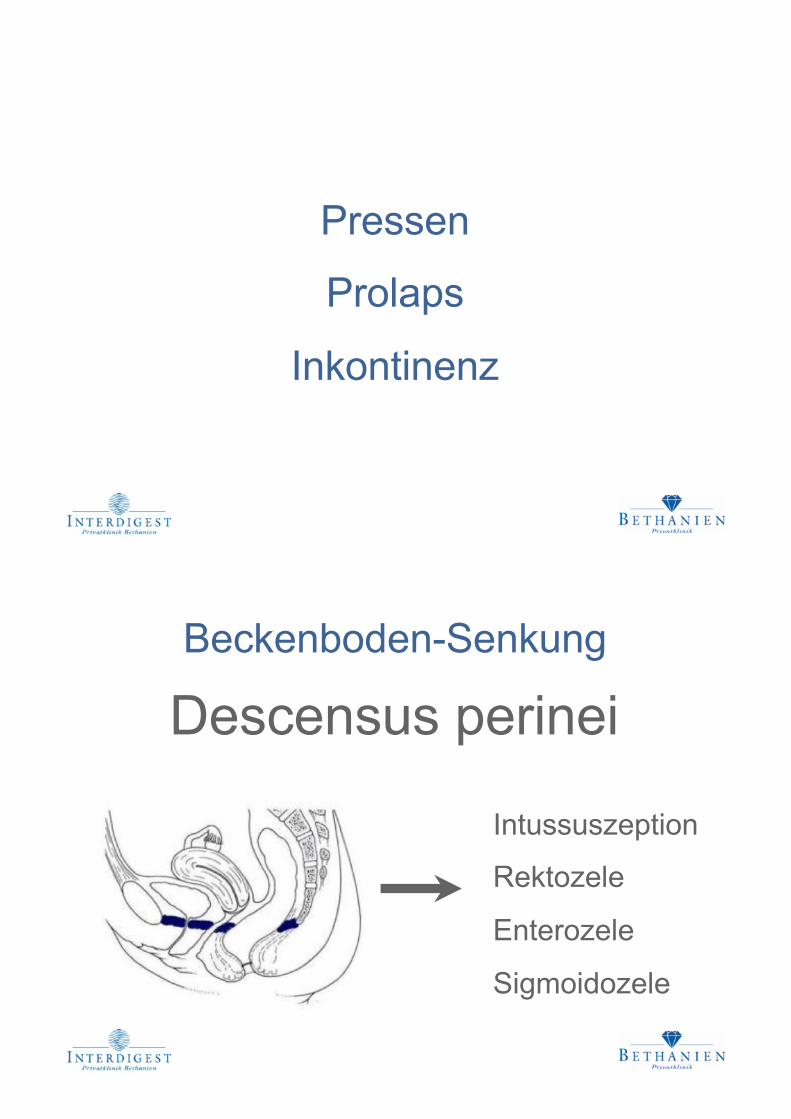
Beckenboden-Senkung
Descensus perinei
Intussuszeption
Rektozele
Enterozele
Sigmoidozele
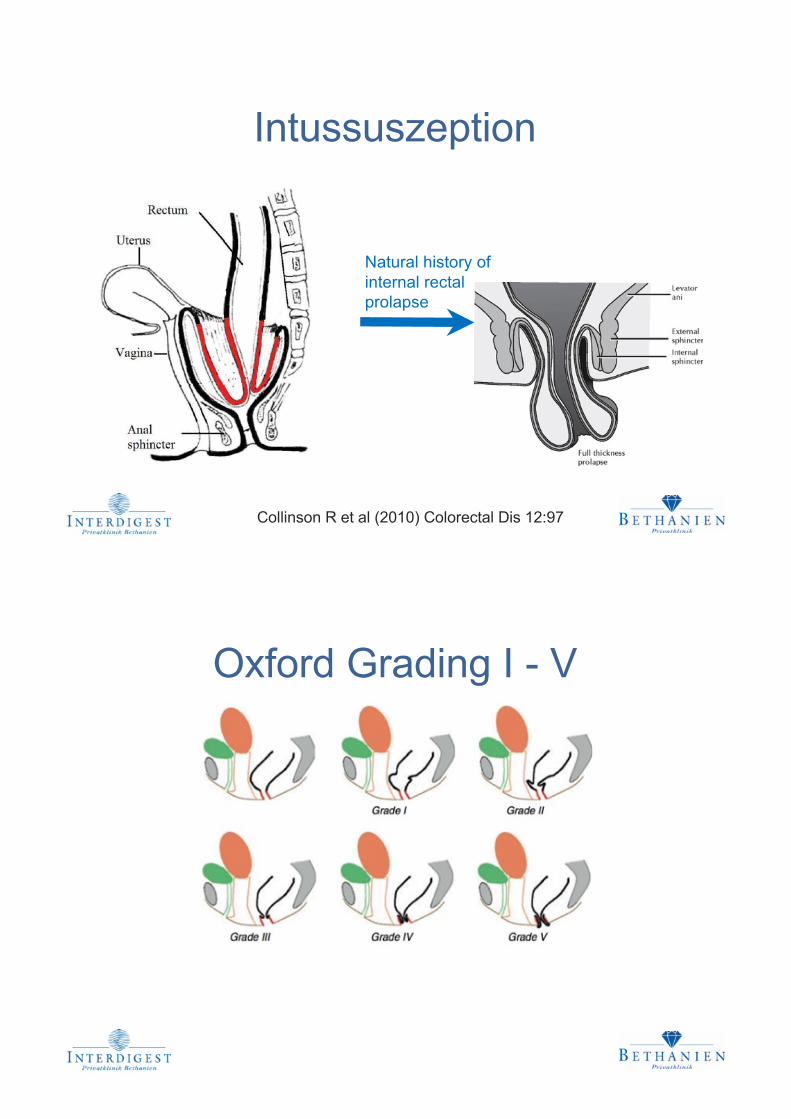
Intussuszeption
Collinson R et al (2010) Colorectal Dis 12:97
Natural history of internal rectal prolapse
Oxford Grading I - V
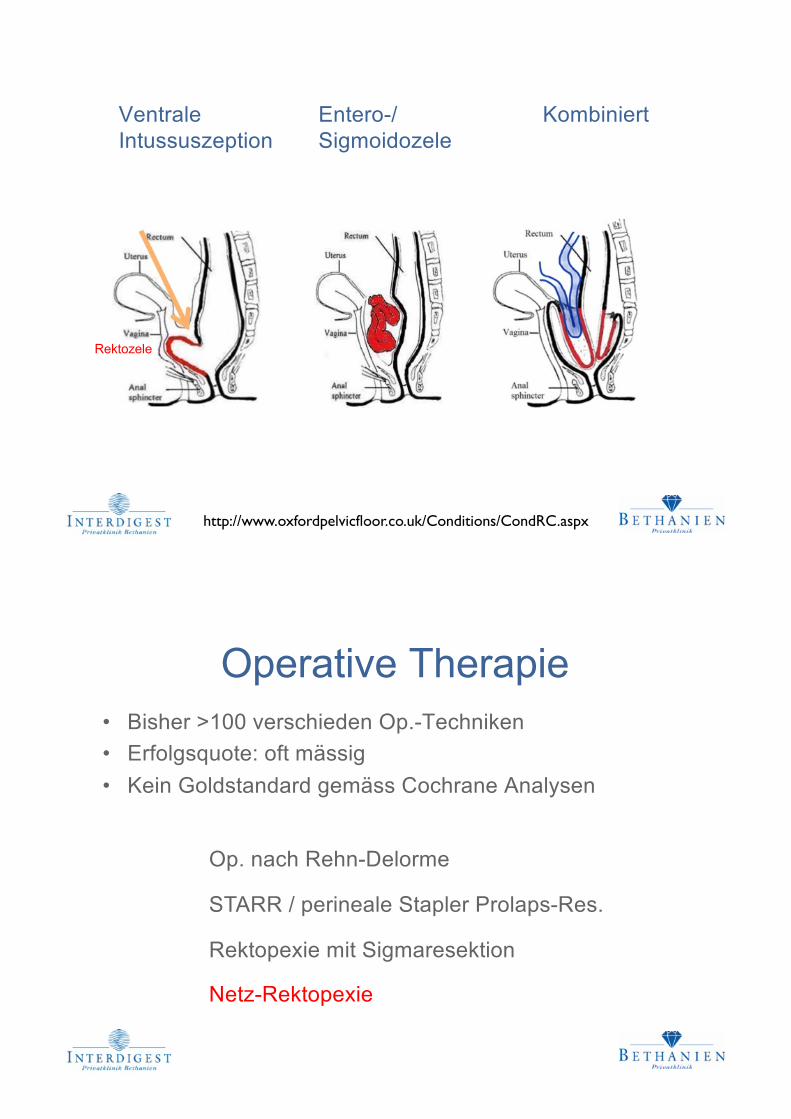
http://www.oxfordpelvicfloor.co.uk/Conditions/CondRC.aspx
Rektozele
Ventrale Entero-/ KombiniertIntussuszeption Sigmoidozele
Operative Therapie• Bisher >100 verschieden Op.-Techniken• Erfolgsquote: oft mässig• Kein Goldstandard gemäss Cochrane Analysen
Op. nach Rehn-Delorme
STARR / perineale Stapler Prolaps-Res.
Rektopexie mit Sigmaresektion
Netz-Rektopexie
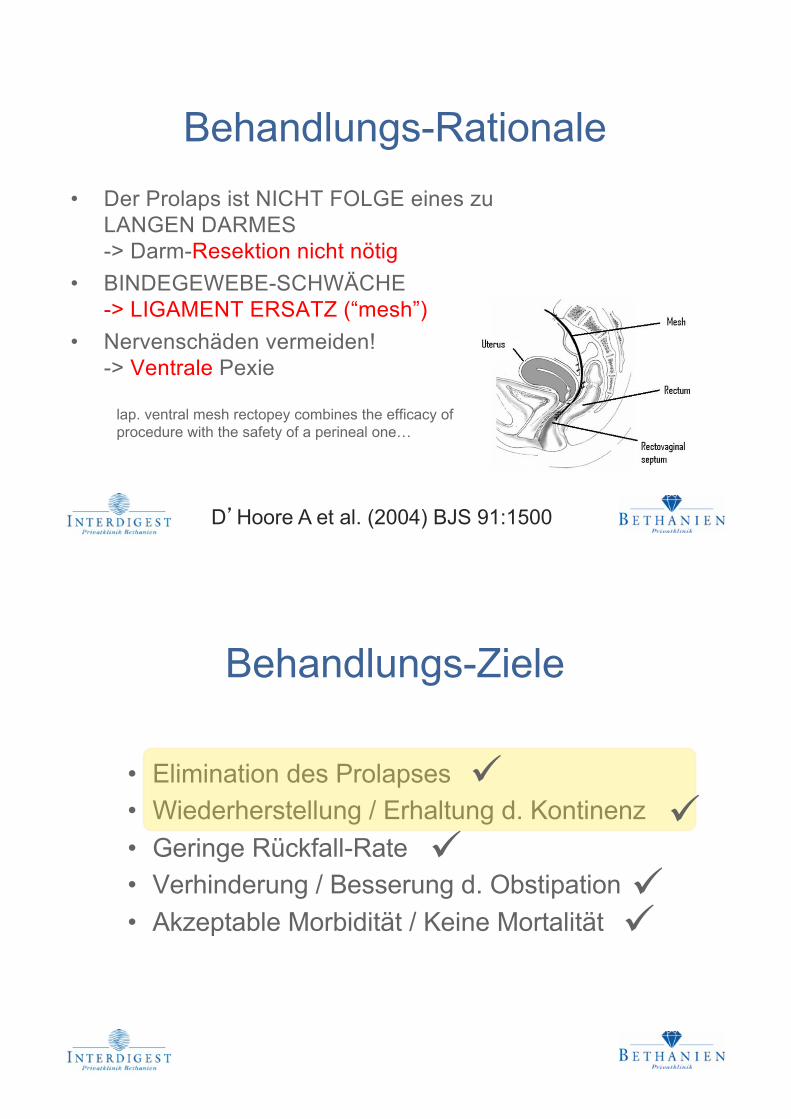
Behandlungs-Rationale• Der Prolaps ist NICHT FOLGE eines zu
LANGEN DARMES-> Darm-Resektion nicht nötig
• BINDEGEWEBE-SCHWÄCHE-> LIGAMENT ERSATZ (“mesh”)
• Nervenschäden vermeiden!-> Ventrale Pexie
lap. ventral mesh rectopey combines the efficacy of an abdominal procedure with the safety of a perineal one…
D�Hoore A et al. (2004) BJS 91:1500
Behandlungs-Ziele
• Elimination des Prolapses• Wiederherstellung / Erhaltung d. Kontinenz• Geringe Rückfall-Rate• Verhinderung / Besserung d. Obstipation• Akzeptable Morbidität / Keine Mortalität
üü
üüü
Epidemiologie Rektumprolaps
Prävalenz in der adulten Bevölkerung:
0.25 - 0.42%
>65 J: 1%
W >>> M
Kairaluma et al (2005) Scan J Surg 94:207
Patient selection ?
Anamnese !!!
Untersuchung !!Zusatz-Abklärungen !
Stuhl-Verlust?Stuhl-Schmieren?Zurückhalten von Wind?

Colorectal Dis 2010;12
Resultate der laparoskop. ventralen Netz-Rektopexie:
Wijffels N et al (2011) Colorectal Dis 13:561
FDA public health notification: serious complications associated with transvaginal
placement of surgical mesh …
Regulatory warning regarding the use of synthetic mesh
in repairing pelvic organ prolapse
Daniel & Schultz: www.fda.gov/medicaldevices/safety/alertsandnotices/ (July 2012)
J Gastrointest Surg 2012;16:622
Case-matched series of a non-cross-linked biologic versus non-absorbable mesh in LVR
Comparable results
Biologic mesh almost completely degraded by 12 months, replaced by collagen, extracellular matrix and neovascularization -> no later complications expected
Ogilvie, Stevenson & Powar; Int J Colorectal Dis 2014;29:1477
Evans Ch et al. Dis Colon Rectum 2015;58:799
Prospective data2203 patients, 93% femaleSynthetic mesh (80%)Biological prosthesis (20%)
Mortality 0.1% (sepsis after bowel perforation)Nonmesh complication rate: 11%Mesh erosion (vaginal & rectal): 2%(2.4% synthetic, 0.7% biological)Stitch sinuses (Ethibond sutures?)
Dis Colon Rectum 2015;58:799
Recommendations:
Absorbable sutures
Polypropylene mesh instead of polyester
Biological grafts in younger patients and in risk situations
Eigene Resultate LVMR
• 47 Pat., w; 47-88j.(69j.); f-u 2-48 Mo
• 36x R-Prolaps (77%)
• Im Beckenbereich voroperiert: 38 P (80%)
• St. n. Hysterektomie: 25 P (53%)
• 23x TiMesh light; 1x ohne Impl.; 23x Biodesign
Eigene Resultate LVMR
geringfügige Morbidität in 17%
1x Harnverhalt1x HWI bei suprapubischem Kath.1x Epistaxis (vorbestehendes Problem)1x mech. Subileus, kons. Th.1x sacrococcygeale Sz., kons. Th.1x Sz anorektal -> HAL im Verlauf1x PONV1x rezid. reaktive Depression (wenige Wochen)
Eigene Resultate LVMR
Intraoperative Komplikationen (4%):
1x Verzicht auf TiMesh-Netzeinlage:
klinisch stumme Anastomosen-Insuffizienz bei St. n.
PSP / STARR
1x intraop. Läsion im Bereich Kolpotomie-Narbe bei
St. n. vag. Hyst. & St. n. Kolpoperineoplastik:
Biodesign-Implantation
Spät-Komplikation (2%):
1x TiMesh-Netz-Erosion rektal
im Verlauf 2x transanal op.
Restitutio ad integrum
1 Rezidiv (2%)
LVMR: effektive und risikoarmeOperation mit guten Resultaten bzgl.
Prolaps-KorrekturKontinenzObstipation
Rückfall-RisikoMorbidität
LVMR ist auch beim alten Menschen eine valable Alternative zur transanalen Op.







